Embed Size (px)
Citation preview
1 3
Arch Gynecol ObstetDOI 10.1007/s00404-014-3233-5
GynecOlOGIc OncOlOGy
Follow‑up of probably benign lesions in non‑screening breast diagnostics
Smaragda Kapsimalakou · Annika Waldmann · Alexander Katalinic · Isabell Grande‑Nagel · Dorothea Fischer · Joerg Barkhausen · Florian M. Vogt
Received: 19 September 2013 / Accepted: 24 March 2014 © Springer-Verlag Berlin Heidelberg 2014
size was 13.8 ± 6.3 mm. The cancer detection ratio in these cases was 18.7/1,000.Conclusions The amount of detected tumors at follow-up of women with preceding BI-RADS 3 equates the associ-ated potential of malignancy.
Keywords Surveillance · BI-RADS 3 · QuaMaDi · Breast cancer detection
AbbreviationsBI-RADS Breast imaging reporting and data systemAcR American college of RadiologyRBcP Regional breast care projectADH Atypical ductal hyperplasialIn lobular intra-epithelial neoplasiaQuaMaDi local quality-assured breast diagnostics
program
Introduction
Mammography is definitely one of the most demand-ing radiological procedures, with direct impact on patient management. examinations graded as BI-RADS 1 or 2 according to the American college of Radiology’s Breast Imaging Report and Data System, do not require any addi-tional tests, whereas lesions characterized as BI-RADS 4 or 5 are referred for surgical or imaging-guided core biopsy.
However, some lesions cannot easily be assigned to one of these groups, and may be graded as BI-RADS 3, indicat-ing ‘probably benign findings’ [1, 2] with a very low prob-ability of malignancy. For those lesions, periodic imaging is recommended as the preferred alternative to immediate open surgical or imaging-guided core biopsy.
Abstract Purpose Our study addresses at the benefit of surveil-lance of probably benign lesions, detected outside mammo-graphic screening, during a 3-year period.Methods 28,588 women (mean age 57 ± 12 years) were examined. Two independent radiologists read the mammo-gram as well as the supplemented ultrasound (in case of breast density AcR type 3 and 4). In the case of discord-ance a third expert considered whether further examination was indicated or not.Results 3,266 diagnostic procedures ended with BI-RADS 3 result and 2,512 (76.9 %) women underwent a follow-up examination. 295 (11.7 %) of them received assessment examination (imaging and/or biopsy) and 37 (12.5 %) (none of them palpable) ended with BI-RADS 6. This equals a tumor detection rate of 14.7/1,000. The ratio in situ:invasive was 7:10 (1:1.43) and the mean size was 11.1 ± 4.51 mm. In the total cohort, 536 carcinomas ended with BI-RADS 6 of them 17 % were in situ and 83 % were invasive breast cancers (ratio in situ:invasive 1:4.99), mean
S. Kapsimalakou · I. Grande-nagel · J. Barkhausen · F. M. Vogt (*) clinic for Radiology and nuclear Medicine, University clinic of Schleswig-Holstein, campus luebeck, Ratzeburger Allee 160 (Haus 40), 23538 lübeck, Germanye-mail: [email protected]
A. Waldmann · A. Katalinic Institute of clinical epidemiology, University clinic of Schleswig-Holstein, Ratzeburger Allee 160 (Haus 50), 23538 lübeck, Germany
D. Fischer clinic for Gynecology and Obstetrics, University clinic of Schleswig-Holstein, Ratzeburger Allee 160 (Haus 12,16), 23538 lübeck, Germany

Arch Gynecol Obstet
1 3
Although BI-RADS 3 lesions remain a matter of debate, the management is justified by the demonstration that: (a) lesions meeting the BI-RADS 3 criteria have a very low likelihood of malignancy; (b) imaging surveillance will identify all malignant lesions by progression and (c) the vast majority of cancers initially considered to be most likely benign will still be diagnosed early in their course resulting in a favorable prognosis [4, 7].
Initial studies demonstrated that the percentage of examinations graded as BI-RADS 3 is highly variable, reaching up to 14 % of all examinations. To reduce the number of short-term follow-up examinations, several articles recommended using the BI-RADS 3 category only after thorough evaluation with mammography and ultrasound.
The majority of studies published on BI-RADS 3 lesions focused on screening mammograms targeted at asymptomatic women in this age group. In a recent study Baum et al. analyzed more than 47,000 screening mam-mograms. Of those 1,114 (2.3 %) were assigned to the BI-RADS 3 category. About 70 % of the patients were compliant and returned for short-term follow-up and the overall tumor detection rate either after additional workup or the next regular screening examination was 0.8 %. How-ever, women outside this age range or with breast cancer-related symptoms are not eligible and approximately 75 % of all breast cancer cases are diagnosed outside of screen-ing programs.
Some years ago, the process-orientated and compre-hensive quality-assured mammographic diagnosis pro-ject, the so-called QuaMaDi project, was implemented in Schleswig–Holstein to improve the standard of breast cancer diagnosis in indication-based mammography in a decentralized healthcare setting. This program is aimed at high standard mammography in symptomatic women at any age and in women with increased risk for breast cancer (i.e., personal history of breast or ovarian cancer, positive family anamnesis for breast cancer), who are not eligible for systematic mammography screening. The Qua-MaDi program includes blinded double readings and expert arbitration reading of mammograms and expert follow-up of suspicious lesions in one of four participating breast centers.
In our study, we analyzed BI-RADS 3 lesions in symp-tomatic patients and women at an increased risk for breast cancer, examined in this local quality-assured breast diag-nostics program. We aimed to determine (a) the frequency of BI-RADS 3 lesions; (b) the compliance of the patients with follow-up recommendations and (c) the frequency and stages of malignancies compared to the entire cohort included in the program and to reported results in a regular screening setting.
Materials and methods
Quality-assured mamma-diagnostics: QuaMaDi
Quality-assured mamma-diagnostics (QuaMaDi) was started in the here documented area in the middle of 2005 and aims at quality-assured mammography in symptomatic women of any age, in women with high risk for breast can-cer or history of breast cancer irrespective of the women’s age and in asymptomatic women older than 70 years who are not eligible for systematic mammography screening [13–17].
High risk was defined as known family history of breast cancer and/or ovarian cancer.
Inclusion criteria
1. Symptomatic women independent of age with clinical findings including unilateral mastodynia, tenderness, induration, palpable mass, nipple secretion, lymph node and/or breast enlargement, nipple changes such as retraction or ulceration and dermal changes such as inflammation or ulceration.
2. Women with increased risk of breast cancer, i.e., women with a history of breast cancer or ovarian can-cer or with a family history of breast cancer and/or ovarial cancer.
3. History of hormonal replacement therapy more than 5 years.
4. Women younger than 50 meeting one of the inclusion criteria 1–4.
5. Women older than 70 years who are not eligible for systematic mammography screening.
Asymptomatic women between 50 and 70 years old were not investigated as they participated in the local mam-mography screening program.
QuaMaDi procedure
The process starts with the patient’s visit to the gynecolo-gist, who is qualified and authorized to participate in the QuaMaDi project. All patients referred for mammography were asked to participate in the program and gave a writ-ten informed consent prior to the examinations. In cases of dense breast tissue (AcR type 3 or 4) or suspicious lesions at mammography (BI-RADS 3, 4 and 5), an additional ultrasound examination is performed. The images are then sent to a second radiologist, who performs an independent second reading. In cases of disagreement or in cases of sus-picion of malignancy (BI-RADS 4, 5) all images are sent to the Breast Reference centre for a third expert reading.

Arch Gynecol Obstet
1 3
The third expert reading at the Breast centre may lead to the following results: either a final diagnosis is possible based on all documented images or further assessment is needed, e.g., clinical examination, additional mammo-graphic views (SenOGRAPHe DMR+, Ge Medical System) and/or ultrasound (Applio XU, Toshiba Medical Systems, Japan). In cases of suspicion of malignancy, his-tological clarification is performed.
On all stages of the QuaMaDi procedure physicians report findings and conducted diagnostics on standardized report forms (paper based). All forms are sent to the Insti-tute of cancer epidemiology in luebeck, Germany, where all data are first entered into an electronic database, then checked for plausibility, and finally linked via probabilistic record linkage resulting in a dataset for each women that depicts her way through the QuaMaDi program (gynecolo-gist, radiologist first and second reading, expert reading and expert follow-up if necessary). The final administra-tive dataset of the QuaMaDi program is used for quality assurance feedback reporting routinely. After request the Institute of cancer epidemiology provides an anonymized extract of the dataset, which can be used for health care research (as done here).
Study population
QuaMaDi is implemented in the existing structure of the decentralized healthcare system in Schleswig–Holstein, Germany. To date, in eastern Schleswig–Holstein 71 gynecologists and 64 radiologists, one specialized breast cancer center, the regional Association of Statutory Health Insurance Physicians of Schleswig–Holstein (KVSH) and various statutory health insurance companies are involved. Participation for physicians and breast cancer centers is regulated by written contract. Women who are members of a statutory health insurance company are eligible to take part in the project.
Breast imaging reporting and data system
The BI-RADS lexicon provides a dictionary of terms to use when describing lesions seen on mammography [1, 11]. A variety of mammographic findings are interpreted as prob-ably benign—BI-RADS 3 lesions. The three most com-mon such findings are: (a) non-calcified solid masses with a round, oval or gently lobular contour and margins that are predominantly circumscribed; (b) clustered tiny calcifica-tions (if fine-detail images portray the calcified particles to be round or oval); and (c) focal asymmetric densities (with-out associated calcifications or architectural distortion) [3, 4, 12].
lesions were interpreted as probably benign (BI-RADS 3) at ultrasound if a solid oval, round or lobulated (less than
three gentle lobulation) mass presented with sharp margins more than 70 % of their circumference and hypoechoic to heterogeneous echotexture.
Follow-up protocols
A first examination with negative results was defined as one with a BI-RADS category 1 or 2 interpretation. These patients received a recommendation to undergo 24-month follow-up in case of a void family history of breast or ovar-ian cancer and 12-month follow-up if history of breast can-cer or a positive family history was known.
Patients with BI-RADS category 3 results after first assessment received typical recommendation to undergo 6-month follow-up breast imaging (clinical examination, mammography and eventually ultrasound) over the course of 2 or 3 years, in order to prove the lesion’s stability in size and morphology.
All follow-up examinations were arranged orally with-out any written invitation and the participation is voluntary for the QuaMaDi patients.
Statistics
For statistical analysis SPSS (Version 17) was used.Data were extracted from the administrative QuaMaDi
data set from 2006 to 2008 and provided as an SPSS file. For descriptive statistics, we used absolute and relative fre-quencies for qualitative data and mean values with standard deviations (SD) and medians plus ranges for quantitative data. cancer detection rates per 1,000 women were com-puted by dividing the number of cancer findings by the number of women in a defined group and multiplying it by 1,000.
For subgroup analyses women were grouped according to their final QuaMaDi result of each diagnostic procedure (BI-RADS 1 or 2 vs. 3 vs. 4 or 5).
Odds ratios and 95 % confidence intervals of predic-tors for a tumor finding at follow-up examination were computed with logistic regression, in which the variables age (continuous variable), actual clinical findings, preced-ing clIS/ADH, history of breast cancer, family history of breast cancer, hormone therapy, asymmetry, mass, calcifi-cation (each yes/no) were included as predictors. History of ovarian cancer was not included in the logistic regres-sion models due to the small number of patients with this characteristic.
Results
From January 2006 until December 2008, the participat-ing gynecologists initiated 28,558 diagnostic processes, of
Arch Gynecol Obstet
1 3
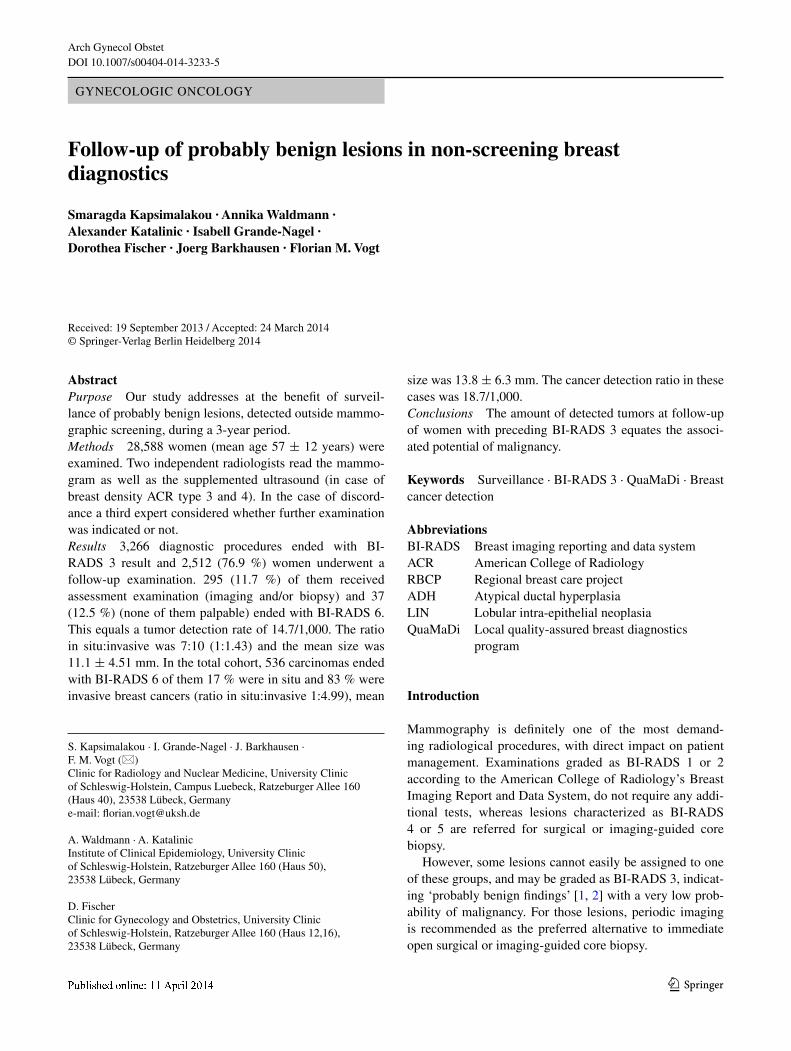
which 3,266 cases (10.7 %) ended with a BI-RADS 3 result, 24,310 with a BI-RADS 1 or 2 result (85.1 %) and 982 (4.2 %) with a BI-RADS 4 or 5 result. The demographic and clinical data of our study population as well as of the patients classified as BI-RADS category 3 and BI-RADS category 1 or 2, respectively, are described in Table 1.
In the total cohort of 28,558 diagnostic examinations 982 had a BI-RADS 4 or 5 finding after double reading of images. Among these women 536 BI-RADS 6 lesion were detected. The ratio of in situ:invasive was 1:4.99, respec-tively. Taking into account all cancers, 16.7 % were in situ and 83.3 % were invasive breast cancers. The mean size was 13.8 ± 6.3 mm [median (range) 13 (3–44 mm)]. The
cancer detection rate in the total cohort was 18.7/1,000. logistic regression showed that—in this group—the find-ing of a mass at initial examination significantly declines the risk to develop a tumor after the initial BI-RADS 4 or 5 finding by 73 %.
Palpable nodes
In the entire cohort of 28,558 women, 1,795 women had palpable nodes.
Of those 1,033 women with BI-RADS category 1 or 2 findings, 362 women with BI-RADS 3 findings and 400 women with BI-RADS 4 or 5 findings.
Table 1 Basic demographic and clinical data of total study population as well as of the patients classified as BI-RADS 3
a Actual clinical findings include mastodynia, induration, palpable lump/finding, nipple secretion/discharge, lymph node enlargement, nipple alterations such as inversion and cutaneous/dermal alteration such as ulcus, redness, etcb numbers are persons with finding classified BI-RADS 3 or higherc Percentages refer to persons with actual clinical findings
All diagnostic procedures (n = 28,558)
BI-RADS category 3 (n = 3,266)
BI-RADS category 1 or 2 (n = 24,310)
BI-RADS category 4 or 5 (n = 982)
Age
Mean and SD 57.3 ± 12.3 55.2 ± 12.2 57.5 ± 12.3 61.3 ± 13.1
Median and range 57 (19–94) 54 (22–91) 58 (19–94) 63 (22–91)
Age groups (years)
<50 9,092 (31.8 %) 1,249 (38.2 %) 7,627 (31.4 %) 216 (22.0 %)
50–69 13,783 (48.3 %) 1,498 (45.9 %) 11,807 (48.6 %) 478 (48.7 %)
≥70 5,683 (19.9 %) 519 (15.9 %) 4,876 (20.1 %) 288 (29.3)
cRF gynecologist
Actual clinical findingsa,c 10,754 (37.7 %) 1,415 (43.4 %) 8,735 (35.9 %) 604 (61.5 %)
Mastodynia (present)c 6,343 (58.9 %) 710 (50.2 %) 5,491 (62.9 %) 142 (14.5 %)
Mastopathy 3,426 (31.8 %) 535 (37.8 %) 2,793 (32.0 %) 98 (10 %)
Palpable nodes 1,795 (16.7 %) 362 (25.6 %) 1,033 (11.8 %) 400 (40.7 %)
Asymmetry 251 (2.3 %) 30 (2.1 %) 188 (2.1 %) 33 (3.3 %)
Skin changes 406 (3.8 %) 64 (4.5 %) 257 (2.9 %) 95 (9.7 %)
Secretion 146 (1.4 %) 16 (1.1 %) 97 (1.1 %) 23 (2.3 %)
Palpable lymph nodes 273 (2.5 %) 31 (2.2 %) 188 (2.1 %) 35 (5.4 %)
Preceding clIS/ADH 79 (0.3 %) 10 (0.3 %) 64 (0.3 %) 5 (0.5 %)
History of breast cancer 5,343 (18.7 %) 553 (16.9 %) 4,636 (19.1 %) 154 (15.7 %)
Family history of breast cancer
10,994 (38.5 %) 1,113 (34.1 %) 9,641 (39.7 %) 240 (24.4 %)
Receive breast cancer aftercare
265 (0.9 %) 43 (1.3 %) 216 (0.9 %) 6 (0.6 %)
History of ovarian cancer 20 (0.1 %) 4 (0.1 %) 15 (0.1 %) 1 (0.1 %)
Hormone replacement therapy (HRT) ≥5 years
4,432/25,309 (17.5 %) 530/2,880 (18.4 %) 3,772/21,546 (17.5 %) 5/883 (0.6 %)
Follow-up examination 1,920 (6.7 %) 682 (20.9 %) 1,166 (4.8 %) 72 (7.3 %)
cRF radiologist (1)/(2)b
Mass 3,067 (10.7 %) 1,147 (35.1 %) 1,345 (5.5 %) 452 (46.6 %)
Microcalcification 1,835 (6.4 %) 1,016 (31.1 %) 523 (2.1 %) 215 (21.9 %)
Asymmetry 946 (3.3 %) 273 (8.4 %) 534 (2.2 %) 67 (6.8 %)
Arch Gynecol Obstet
1 3
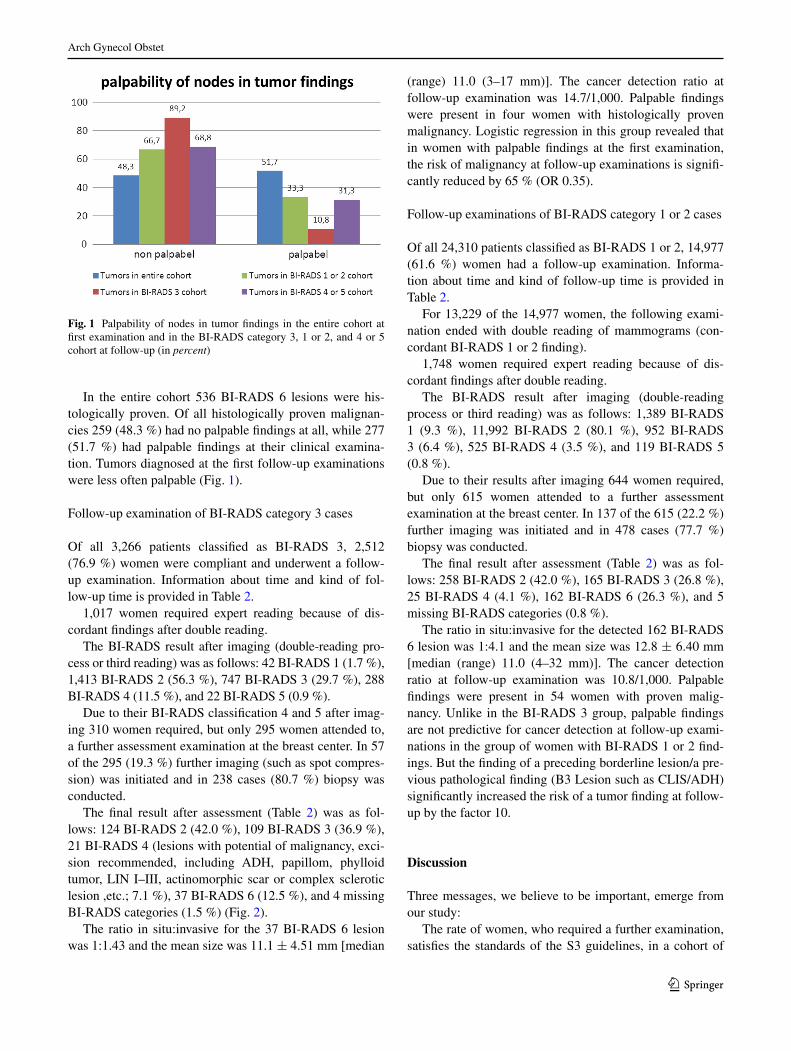
In the entire cohort 536 BI-RADS 6 lesions were his-tologically proven. Of all histologically proven malignan-cies 259 (48.3 %) had no palpable findings at all, while 277 (51.7 %) had palpable findings at their clinical examina-tion. Tumors diagnosed at the first follow-up examinations were less often palpable (Fig. 1).
Follow-up examination of BI-RADS category 3 cases
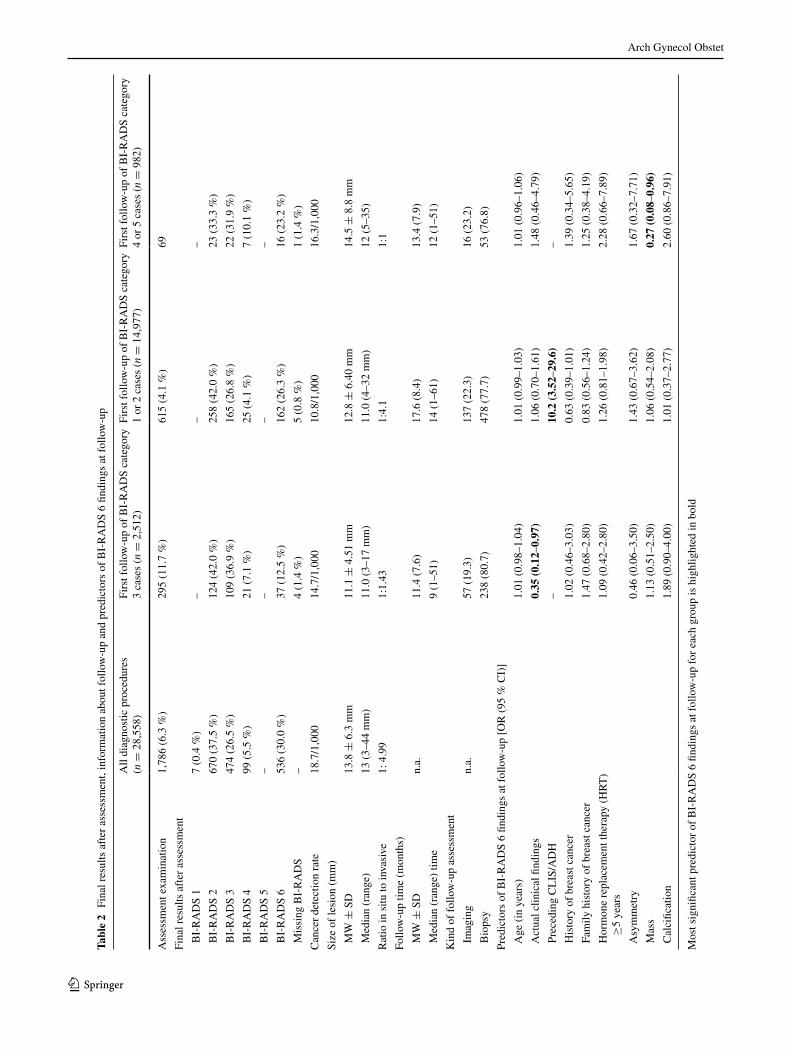
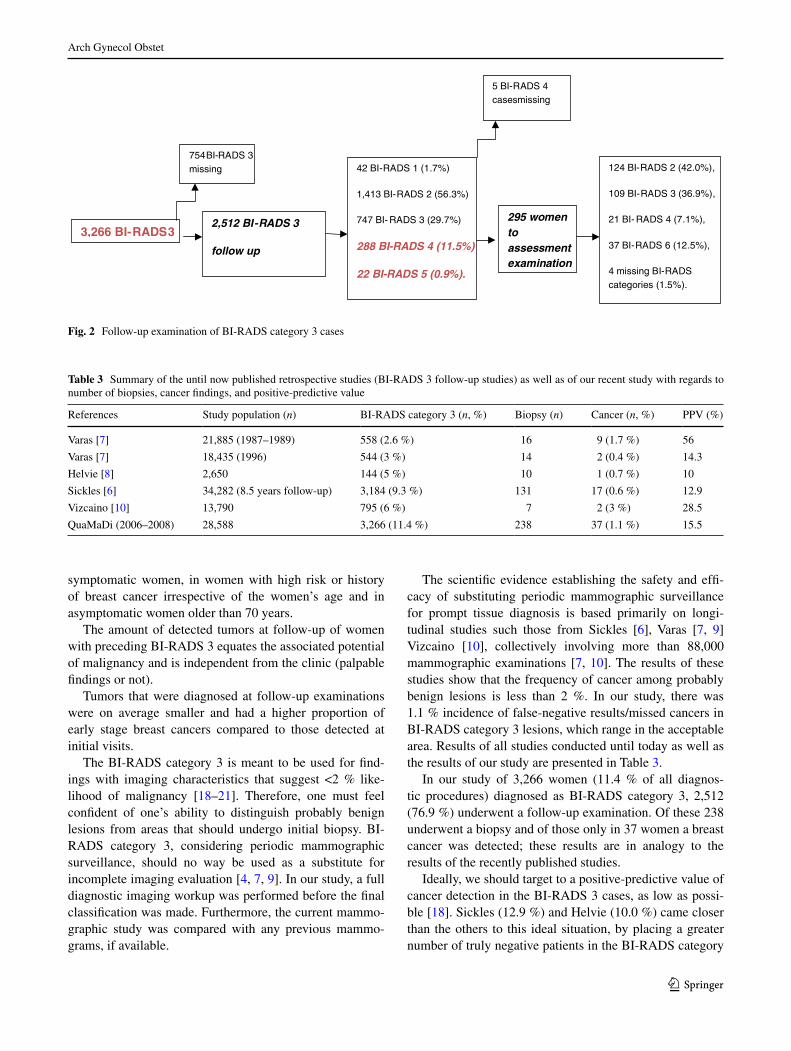
Of all 3,266 patients classified as BI-RADS 3, 2,512 (76.9 %) women were compliant and underwent a follow-up examination. Information about time and kind of fol-low-up time is provided in Table 2.
1,017 women required expert reading because of dis-cordant findings after double reading.
The BI-RADS result after imaging (double-reading pro-cess or third reading) was as follows: 42 BI-RADS 1 (1.7 %), 1,413 BI-RADS 2 (56.3 %), 747 BI-RADS 3 (29.7 %), 288 BI-RADS 4 (11.5 %), and 22 BI-RADS 5 (0.9 %).
Due to their BI-RADS classification 4 and 5 after imag-ing 310 women required, but only 295 women attended to, a further assessment examination at the breast center. In 57 of the 295 (19.3 %) further imaging (such as spot compres-sion) was initiated and in 238 cases (80.7 %) biopsy was conducted.
The final result after assessment (Table 2) was as fol-lows: 124 BI-RADS 2 (42.0 %), 109 BI-RADS 3 (36.9 %), 21 BI-RADS 4 (lesions with potential of malignancy, exci-sion recommended, including ADH, papillom, phylloid tumor, lIn I–III, actinomorphic scar or complex sclerotic lesion ,etc.; 7.1 %), 37 BI-RADS 6 (12.5 %), and 4 missing BI-RADS categories (1.5 %) (Fig. 2).
The ratio in situ:invasive for the 37 BI-RADS 6 lesion was 1:1.43 and the mean size was 11.1 ± 4.51 mm [median
(range) 11.0 (3–17 mm)]. The cancer detection ratio at follow-up examination was 14.7/1,000. Palpable findings were present in four women with histologically proven malignancy. logistic regression in this group revealed that in women with palpable findings at the first examination, the risk of malignancy at follow-up examinations is signifi-cantly reduced by 65 % (OR 0.35).
Follow-up examinations of BI-RADS category 1 or 2 cases
Of all 24,310 patients classified as BI-RADS 1 or 2, 14,977 (61.6 %) women had a follow-up examination. Informa-tion about time and kind of follow-up time is provided in Table 2.
For 13,229 of the 14,977 women, the following exami-nation ended with double reading of mammograms (con-cordant BI-RADS 1 or 2 finding).
1,748 women required expert reading because of dis-cordant findings after double reading.
The BI-RADS result after imaging (double-reading process or third reading) was as follows: 1,389 BI-RADS 1 (9.3 %), 11,992 BI-RADS 2 (80.1 %), 952 BI-RADS 3 (6.4 %), 525 BI-RADS 4 (3.5 %), and 119 BI-RADS 5 (0.8 %).
Due to their results after imaging 644 women required, but only 615 women attended to a further assessment examination at the breast center. In 137 of the 615 (22.2 %) further imaging was initiated and in 478 cases (77.7 %) biopsy was conducted.
The final result after assessment (Table 2) was as fol-lows: 258 BI-RADS 2 (42.0 %), 165 BI-RADS 3 (26.8 %), 25 BI-RADS 4 (4.1 %), 162 BI-RADS 6 (26.3 %), and 5 missing BI-RADS categories (0.8 %).
The ratio in situ:invasive for the detected 162 BI-RADS 6 lesion was 1:4.1 and the mean size was 12.8 ± 6.40 mm [median (range) 11.0 (4–32 mm)]. The cancer detection ratio at follow-up examination was 10.8/1,000. Palpable findings were present in 54 women with proven malig-nancy. Unlike in the BI-RADS 3 group, palpable findings are not predictive for cancer detection at follow-up exami-nations in the group of women with BI-RADS 1 or 2 find-ings. But the finding of a preceding borderline lesion/a pre-vious pathological finding (B3 lesion such as clIS/ADH) significantly increased the risk of a tumor finding at follow-up by the factor 10.
Discussion
Three messages, we believe to be important, emerge from our study:
The rate of women, who required a further examination, satisfies the standards of the S3 guidelines, in a cohort of
Fig. 1 Palpability of nodes in tumor findings in the entire cohort at first examination and in the BI-RADS category 3, 1 or 2, and 4 or 5 cohort at follow-up (in percent)
Arch Gynecol Obstet
1 3
Tabl
e 2
Fin
al r
esul
ts a
fter
ass
essm
ent,
info
rmat
ion
abou
t fol
low
-up
and
pred
icto
rs o
f B
I-R
AD
S 6
findi
ngs
at f
ollo
w-u
p
Mos
t sig
nific
ant p
redi
ctor
of
BI-
RA
DS
6 fin
ding
s at
fol
low
-up
for
each
gro
up is
hig
hlig
hted
in b
old
All
diag
nost
ic p
roce
dure
s (n
= 2
8,55
8)Fi
rst f
ollo
w-u
p of
BI-
RA
DS
cate
gory
3
case
s (n
= 2
,512
)Fi
rst f
ollo
w-u
p of
BI-
RA
DS
cate
gory
1
or 2
cas
es (
n =
14,
977)
Firs
t fol
low
-up
of B
I-R
AD
S ca
tego
ry
4 or
5 c
ases
(n
= 9
82)
Ass
essm
ent e
xam
inat
ion
1,78
6 (6
.3 %
)29
5 (1
1.7
%)
615
(4.1
%)
69
Fina
l res
ults
aft
er a
sses
smen
t
BI-
RA
DS
17
(0.4
%)
––
–
BI-
RA
DS
267
0 (3
7.5
%)
124
(42.
0 %
)25
8 (4
2.0
%)
23 (
33.3
%)
BI-
RA
DS
347
4 (2
6.5
%)
109
(36.
9 %
)16
5 (2
6.8
%)
22 (
31.9
%)
BI-
RA
DS
499
(5.
5 %
)21
(7.
1 %
)25
(4.
1 %
)7
(10.
1 %
)
BI-
RA
DS
5–
––
–
BI-
RA
DS
653
6 (3
0.0
%)
37 (
12.5
%)
162
(26.
3 %
)16
(23
.2 %
)
Mis
sing
BI-
RA
DS
–4
(1.4
%)
5 (0
.8 %
)1
(1.4
%)
can
cer
dete
ctio
n ra
te18
.7/1
,000
14.7
/1,0
0010
.8/1
,000
16.3
/1,0
00
Size
of
lesi
on (
mm
)
MW
± S
D13
.8 ±
6.3
mm
11.1
± 4
.51
mm
12.8
± 6
.40
mm
14.5
± 8
.8 m
m
Med
ian
(ran
ge)
13 (
3–44
mm
)11
.0 (
3–17
mm
)11
.0 (
4–32
mm
)12
(5–
35)
Rat
io in
situ
to in
vasi
ve1:
4.9
91:
1.43
1:4.
11:
1
Follo
w-u
p tim
e (m
onth
s)
MW
± S
Dn.
a.11
.4 (
7.6)
17.6
(8.
4)13
.4 (
7.9)
Med
ian
(ran
ge)
time
9 (1
–51)
14 (
1–61
)12
(1–
51)
Kin
d of
fol
low
-up
asse
ssm
ent
Im
agin
gn.
a.57
(19
.3)
137
(22.
3)16
(23
.2)
Bio
psy
238
(80.
7)47
8 (7
7.7)
53 (
76.8
)
Pred
icto
rs o
f B
I-R
AD
S 6
findi
ngs
at f
ollo
w-u
p [O
R (
95 %
cI)
]
Age
(in
yea
rs)
1.01
(0.
98–1
.04)
1.01
(0.
99–1
.03)
1.01
(0.
96–1
.06)
Act
ual c
linic
al fi
ndin
gs0.
35 (
0.12
–0.9
7)1.
06 (
0.70
–1.6
1)1.
48 (
0.46
–4.7
9)
Pre
cedi
ng c
lIS
/AD
H–
10.2
(3.
52–2
9.6)
–
His
tory
of
brea
st c
ance
r1.
02 (
0.46
–3.0
3)0.
63 (
0.39
–1.0
1)1.
39 (
0.34
–5.6
5)
Fam
ily h
isto
ry o
f br
east
can
cer
1.47
(0.
68–2
.80)
0.83
(0.
56–1
.24)
1.25
(0.
38–4
.19)
Hor
mon
e re
plac
emen
t the
rapy
(H
RT
) ≥
5 ye
ars
1.09
(0.
42–2
.80)
1.26
(0.
81–1
.98)
2.28
(0.
66–7
.89)
Asy
mm
etry
0.46
(0.
06–3
.50)
1.43
(0.
67–3
.62)
1.67
(0.
32–7
.71)
Mas
s1.
13 (
0.51
–2.5
0)1.
06 (
0.54
–2.0
8)0.
27 (
0.08
–0.9
6)
cal
cific
atio
n1.
89 (
0.90
–4.0
0)1.
01 (
0.37
–2.7
7)2.
60 (
0.86
–7.9
1)
Arch Gynecol Obstet
1 3
symptomatic women, in women with high risk or history of breast cancer irrespective of the women’s age and in asymptomatic women older than 70 years.
The amount of detected tumors at follow-up of women with preceding BI-RADS 3 equates the associated potential of malignancy and is independent from the clinic (palpable findings or not).
Tumors that were diagnosed at follow-up examinations were on average smaller and had a higher proportion of early stage breast cancers compared to those detected at initial visits.
The BI-RADS category 3 is meant to be used for find-ings with imaging characteristics that suggest <2 % like-lihood of malignancy [18–21]. Therefore, one must feel confident of one’s ability to distinguish probably benign lesions from areas that should undergo initial biopsy. BI-RADS category 3, considering periodic mammographic surveillance, should no way be used as a substitute for incomplete imaging evaluation [4, 7, 9]. In our study, a full diagnostic imaging workup was performed before the final classification was made. Furthermore, the current mammo-graphic study was compared with any previous mammo-grams, if available.
The scientific evidence establishing the safety and effi-cacy of substituting periodic mammographic surveillance for prompt tissue diagnosis is based primarily on longi-tudinal studies such those from Sickles [6], Varas [7, 9] Vizcaino [10], collectively involving more than 88,000 mammographic examinations [7, 10]. The results of these studies show that the frequency of cancer among probably benign lesions is less than 2 %. In our study, there was 1.1 % incidence of false-negative results/missed cancers in BI-RADS category 3 lesions, which range in the acceptable area. Results of all studies conducted until today as well as the results of our study are presented in Table 3.
In our study of 3,266 women (11.4 % of all diagnos-tic procedures) diagnosed as BI-RADS category 3, 2,512 (76.9 %) underwent a follow-up examination. Of these 238 underwent a biopsy and of those only in 37 women a breast cancer was detected; these results are in analogy to the results of the recently published studies.
Ideally, we should target to a positive-predictive value of cancer detection in the BI-RADS 3 cases, as low as possi-ble [18]. Sickles (12.9 %) and Helvie (10.0 %) came closer than the others to this ideal situation, by placing a greater number of truly negative patients in the BI-RADS category
3,266 BI-RADS 32,512 BI-RADS 3
follow up
754BI-RADS 3 missing 42 BI-RADS 1 (1.7%)
1,413 BI-RADS 2 (56.3%)
747 BI- RADS 3 (29.7%)
288 BI-RADS 4 (11.5%)
22 BI-RADS 5 (0.9%).
295 women to assessment examination
124 BI-RADS 2 (42.0%),
109 BI-RADS 3 (36.9%),
21 BI- RADS 4 (7.1%),
37 BI-RADS 6 (12.5%),
4 missing BI-RADS categories (1.5%).
5 BI-RADS 4 cases missing
Fig. 2 Follow-up examination of BI-RADS category 3 cases
Table 3 Summary of the until now published retrospective studies (BI-RADS 3 follow-up studies) as well as of our recent study with regards to number of biopsies, cancer findings, and positive-predictive value
References Study population (n) BI-RADS category 3 (n, %) Biopsy (n) cancer (n, %) PPV (%)
Varas [7] 21,885 (1987–1989) 558 (2.6 %) 16 9 (1.7 %) 56
Varas [7] 18,435 (1996) 544 (3 %) 14 2 (0.4 %) 14.3
Helvie [8] 2,650 144 (5 %) 10 1 (0.7 %) 10
Sickles [6] 34,282 (8.5 years follow-up) 3,184 (9.3 %) 131 17 (0.6 %) 12.9
Vizcaino [10] 13,790 795 (6 %) 7 2 (3 %) 28.5
QuaMaDi (2006–2008) 28,588 3,266 (11.4 %) 238 37 (1.1 %) 15.5

Arch Gynecol Obstet
1 3
3 [6, 9]. The positive-predictive value in our study (15.5 %) was a little bit higher compared to above studies (Table 3).
Most likely all of these malignancies would have prob-ably been discovered at the first examinations if all BI-RADS 3 findings would have underwent a biopsy. Recom-mending a follow-up examination for these cases increases the cost of mammography as well as the risk that malignan-cies will be probably discovered at a slightly more advanced stage. On the contrary, tumors that were diagnosed in our study at follow-up examinations were on average smaller (11.1 ± 4.51 vs. 13.8 ± 6.3 mm) and had a higher propor-tion of early stage breast cancers (in situ:invasive 1:1.43 vs. 1:4.99) compared to those at initial visits. From the above results, we believe that recommendation of a follow-up examination after 6 months seems to be a feasible and suf-ficient way to detect cancer in BI-RADS 3 cases in a timely manner since the ratio of in situ:invasive breast cancer is higher compared to the ratio detected by BI-RADS 4 and 5 cases, respectively.
The majority (2,904/3,266, 89 %) of our procedures classified as BI-RADS 3 had non-palpable findings at all. Within the BI-RADS 3 category the 33 detected tumors belong predominantly to the group of non-palpable find-ings while only 4 cases of proven malignancy were docu-mented prior as palpable findings. These results strengthen the fact, that BI-RADS 3 lesions are principally probably benign non-palpable lesions.
However, in the total collective of 28,588 procedures 536 histologically proven tumors were found. Of those, 259 (48.3 %) had no palpable findings at all, whereas 277 (51.7 %) had palpable findings. The majority of the his-tologically proven malignancies were judged as palpa-ble findings in the clinical examination, which might be explained by the fact that the participants of QuaMaDi are predominantly symptomatic women.
There are more factors that make surveillance an attrac-tive alternative to tissue diagnosis in the management of probably benign lesions. The positive-predictive value of biopsy will be increased because of a substantial reduc-tion in the number of interventional procedures that pro-duce benign results. In addition, surveillance is associated with reduced morbidity, especially when compared to open surgical biopsy but also, measurably, when compared to percutaneous imaging-guided tissue sampling [4–6]. Fur-thermore, the cost for health insurances will decrease sub-stantially, because the costs of diagnostic examinations usually are much lower than that of imaging-guided inter-ventional procedures or operating procedures.
Despite the advantages afforded by periodic mammo-graphic surveillance, the recommendation for 6-month follow-up is being made less frequently nowadays than it was 10 years before [4]. Since the cost for diagnos-tic imaging examinations are much lower than those for
imaging-guided interventional procedures, the use of sur-veillance, instead of biopsy should be increased. QuaMaDi argues for widespread adoption of periodic mammographic surveillance for probably benign lesions, which in view of the recent results is reasonable.
However, encouraging 6-month follow-up, according to mammography screening physicians, is unnecessarily anxi-ety provoking. Particularly, a patient with a recommenda-tion for 6-month follow-up can comply or not comply, seek a second opinion elsewhere, decide never to have another mammogram, or insists on resolution by means of biopsy [19, 20].
In our study, comparatively, 23 % of all the BI-RADS category 3 cases underwent their initial follow-up else-where, or not at all. compliance with the entire proposed follow-up protocol occurred in 77 % of our patients, rela-tive high for a decentralized health care system with a large geographical territory, like QuaMaDi (higher as in the 50 % compliance in the Sickle’s study and as in the 71 % compli-ance in the study of Baum et al. [6, 21]). Furthermore, the interval time for follow-up examination in our study ranged between 3 and 17 months expressing the patient’s individ-ual compliance with the follow-up examinations.
It is important to remember that stability of a finding at a 6-month follow-up cannot be used to reassure a patient that the mass is benign [4, 19, 22]. Only after 2 or 3 years of surveillance certainty of benignity is high. The patients must be informed that it is the length of surveillance that increases confidence in benignity, not the initial follow-up examination. If there is an abnormal finding in the first follow-up examination, biopsy is recommended. If biopsy is not indicated, the patients should be followed up annu-ally thereafter for 2 or 3 years [4]. Therefore, periodic sur-veillance will be effective only if there is a high degree of acceptance and compliance with follow-up recommenda-tions [23].
In the three groups of our participants different factors were predictive for a tumor finding at the first follow-up examination. For women of the BI-RADS 3 group that had palpable findings at the first examination the risk of malig-nancy at follow-up examinations was reduced by 65 %. This is due to the fact that many palpable lesions are classi-fied as BI-RADS 3 lesion according to its ambiguous char-acteristics on additional performed ultrasound, i.e., hem-orrhagic cyst, fibroadenoma or focal fibrocystic changes, although having a very low probability of malignancy.
In women of the BI-RADS 4 or 5 groups with a palpable mass at initial examination (and subsequent assessment) the risk for a cancer finding at follow-up examination declined by 73 %. Histological clarification of a clinically palpable and mammographic suspicious opacity in the first assess-ment examination seems to decline the risk of developing a breast cancer until follow-up examination significantly.

Arch Gynecol Obstet
1 3
logistic regression models revealed only in the group of women with BI-RADS 1 and 2 findings at initial exami-nation a factor that increased the risk for a tumor finding at the follow-up examination by a factor of 10: a previ-ous pathological finding (B3 lesion such as clIS, ADH). Therefore, our study confirms the well-known risk factor of a previous pathological finding for breast cancer.
Conclusion
Surveillance confirms the nature of breast lesions consid-ered probably benign and permits the detection of a small but relevant number of breast cancers at an early tumor stage and small size, resulting in better prognosis and qual-ity of life also in a cohort outside of systematic mammo-graphic screening.
Acknowledgments First of all, we want to thank the patients for their participation in QuaMaDi program and for their compliance to the periodic surveillance examinations. This publication is a team-work of 250 people (including doctors and medical staff, as well as the personnel of the Institute of cancer epidemiology of the Univer-sity of lübeck), who are involved in QuaMaDi project in Schleswig–Holstein. We also thank the participating health care insurance com-panies, the Ministry of Social Affairs and Health and the Deutsche Krebshilfe e. V., who have financed the program.
Conflict of interest none.
References
1. American college of Radiology (1998) Breast imaging reporting and data system (BI-RADS), 3rd edn. American college of Radi-ology, Raston, pp 94–95
2. lehman c, Holt S, Peacock S, White e, Urban n (2002) Use of the American college of radiology BI-RADS guidelines by com-munity radiologists: concordance of assessments and recommen-dations assigned to screening mammograms. AJR 179:15–20
3. caplan lS, Blackman D, nadel M, Monticciolo Dl (1999) cod-ing mammograms using the classification ‘probably benign find-ing: short interval follow-up suggested’. AJR 172:339–342
4. Sickles eA (1999) Probably benign breast lesions: when should follow-up be recommended and what is the optimal follow-up protocol? Radiology 213:11–14
5. Sickles eA (1995) Management of probably benign breast lesions. Radiol clin north Am 33:1123–1130
6. Sickles eA (1991) Periodic mammographic follow-up of prob-ably benign lesions: results in 3,184 consecutive cases. Radiology 179:463–468
7. Varas X, leborgne F, leborgne JH (1992) non palpable, prob-ably benign lesions: role of follow-up mammography. Radiology 184:409–414
8. Helvie MA, Pennes DR, Rebner M, Adler DD (1991) Mammo-graphic follow-up of low-suspicion lesions: compliance rate and diagnostic yield. Radiology 178:155–158
9. Varas X, leborgne JH, leborgne F, Mezzera J, Jaumandreu S, leborgne F (2002) Revisiting the mammographic follow-up of BI:RADS category 3 lesions. AJR 179:691–695
10. Vizcaíno I, Gadea l, Andreo l, Salas D, Ruiz-Perales F, cue-nas D, Herranz c, Bueno F, Screening Program Working Group (2001) Short-term follow-up results in 795 nonpalpable probably benign lesions detected at screening mammography. Radiology 219:475–483
11. Burnside eS, Sickles eA, Bassett lW et al (2009) The AcR BI-RADS® experience: learning from history. J Am coll Radiol 6:851–860
12. Adler DD, Helvie MA, Ikeda DM (1990) nonpalpable probably benign breast lesions: follow-up strategies after initial detection on mammography. AJR 155:1195–1201
13. eUReF european Guidelines for Quality Assurance in Mammog-raphy Screening (2001). european commission, luxembourg
14. eUReF european Guidelines for Quality Assurance in Mam-mography Screening and Diagnosis (2006). european commis-sion, luxembourg
15. Katalinic A, Bartel c, Raspe H, Shreer I (2007) Beyond mam-mography screening: quality assurance in breast cancer diagnosis (The QuaMaDi Project). Br J cancer 96:157–161
16. Schreer I, Katalinic A (2007) Is high quality breast imaging and diagnosis possible in a decentralized system?. The QuaMaDi pro-ject. Breast care 2:20–24
17. Albert U-S, Altland H, Duda V et al (2008) Summary of the updated stage 3 guideline for early detection of breast cancer in Germany 2008. Fortschr Röntgenstr 180:455–465
18. D’Orsi cJ (1992) To follow or not to follow, that is the question. Radiology 184:306
19. Rubin e (1999) Six-month follow-up: an alternative view (view-point). Radiology 213:15–18
20. Hall FM (2002) Malignancy in BI-RADS category 3 mammo-graphic lesions (letter). Radiology 225:918–920
21. Baum JK, Hanna lG, Acharyya S, Mahoney Mc, conant eF, Basset lW, Pisano eD (2011) Use of BI-RADS 3 probably benign category in the American college of radiology imaging network digital mammographic imaging screening trial. Radiol-ogy 260(1):61–67
22. Meyer Je, Kopans DB (1981) Stability of a mammographic mass: a false sense of security. AJR 137:595–598
23. liberman l, la Trenta lR, Dershaw DD, Abramson AF, Mor-ris eA, cohen MA, Rosen PP, Borgen PI (1997) Impact of core biopsy on the surgical management of impalpable breast cancer. AJR 168:495–499