Embed Size (px)
Citation preview

Thomas Z, Abbas T, Sasson SBradford Royal Infirmary, Bradford
Insert your Logos
BACKGROUND
•Endometrial hyperplasia is a pathological
condition characterised by hyperplastic changes in
the endometrial glandular and stromal structures
lining the uterine cavity
•The revised 2014 World health organization ( WHO
)classification separates endometrial hyperplasia
into two groups : 1) hyperplasia without atypia and
2) atypical hyperplasia
•Endometrial hyperplasia with atypia is a significant
clinical concern as it can have concurrent or be a
precursor of endometrial cancer
•Accurate diagnosis is essential for optimal
management of patients and reversion to normal
endometrium is the key with meticulous follow up
•It is often associated with multiple identifiable risk
factors and treatment should also aim to modify
and monitor these factors .
•We have audited our practice on the follow up of
endometrial hyperplasia in a large District General
Hospital.
OBJECTIVES
•The aim was to evaluate the follow -up
management options given to patients diagnosed
with endometrial hyperplasia
•Treatment effectiveness - regression, relapse and
progression were assessed
•The necessity for a separate pipelle clinic for
endometrial hyperplasia follow ups was also
evaluated.
•The list of follow ups from the hysteroscopy clinic
over a year (Aug 2017-18)was obtained and
retrospective analysis of electronic records for 44
patients performed
•The RCOG/BSGE Green -top Guideline for
Endometrial Hyperplasia was used as the standard .
RESULTS
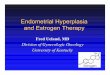
•68%(30/44) were managed with intrauterine
progestogen (LNG-IUS),25%(11/44) had oral
progestogen and 7% declined treatment and chose
observation alone
•The interval for the first repeat sample for both
groups was a mean of 8.6 months
•8 patients had more than 3 repeat samples,which
predated the RCOG/BSGE Guideline on
Hyperplasia.
•30%(13/44) patients had a hysteroscopy at this
follow up visit due to irregular bleeding .The
majority 86%(38/44)had an adequate sample
noting progesterone effect in 73%(32/44)
RECOMMENDATIONS
REFERENCES
RESULTS
•The majority of patients were aged between 46-65
years, 82%(26/33)were multiparous.75%(33/44) were
post-menopausal .
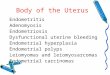
•The body mass index(BMI)data was available for 26
patients, of which 65%(16/26) were of BMI >35
•Other risk factors were evaluated,one patient had
polycystic ovarian syndrome(PCOS )and no patients
were on hormone replacement therapy(HRT) or
tamoxifen
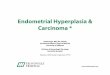
•At first diagnosis,77%(34/44)were endometrial
hyperplasia without atypia and 23%(10/44) had
hyperplasia with mild focal/focal atypia
• Raised BMI is an important risk factor for endometrial
hyperplasia ,documentation was available in only 26
patients. 61.5%(16/26) of them had BMI >35.
•The mean interval for the first repeat biopsy was
approximately 8.6 months for all hyperplasias detected.
This was against the standard of 3 months for atypia and
6 months for those without atypia after treatment .
•18% (8/44)of hyperplasia diagnosed was within a polyp,
only 37.5% (3/8)had follow up hysteroscopy.
Follow up of Endometrial Hyperplasia and treatment effect in a large
District General Hospital
16
10
18
BMI
>35
<35
No data
34
6
4
Histology at first diagnosis
Hyperplasia
without
atypia
Hyerplasia
with mild
focal atypia
Hperplasia
with focal
typia
ENDOMETRIAL POLYPS-18%(8/44)OF HYPERPLASIA
71% had BMI >35
50% had focal atypia
75% accepted IUS,25%had oral progestogen as treatment
37.5%had follow up hysteroscopy100% regression in follow up
FOCAL ATYPICAL
HYPERPLASIA -23%
(10/44) OF
HYPERPLASIA
20% had
BMI>35
50% identified
in polyps
70% accepted
IUS,30% had oral
progesterone as
treatment
20% had follow
up hysteroscopy
100% regression
in follow up
30
11
3
0
5
10
15
20
25
30
35
1 2 3 4
IUS
Oral
Progestogen
Observation
Of the 8 patients with endometrial hyperplasia
identified in a polyp,only 37.5%(3/8) had a follow
up hysteroscopy
Looking at treatment effect,100% had regression,
one patient (2.3%) had relapse who was then
treated with intrauterine progestogen and the
repeat biopsy was negative.There was no disease
progression.
CONCLUSIONS
•Clear documentation of BMI is essential
•On adherence with the RCOG guidelines,strict
follow up protocols have to be considered
•Endometrial hyperplasia with focal atypia is a
grey area and treatment has to be
individualised
•Considering focal atypical hyperplasia follow
up,hysteroscopy can be put into practice
•Hyperplasia was detected in 44 patients in this
period.Setting up a separate pipelle clinic could
free up some hysteroscopy slots.This requires
prior triage to ensure no abnormal bleeding
and for previous atypia to have hysteroscopy
slots
•To write up a local Guideline for Endometrial
Hyperplasia – and re audit practice
•Management of Endometrial Hyperplasia,Green-top Guideline No 67 RCOG/BSGE joint Guideline/February 2016
•Commission of the Gynaecological Oncology working Group (AGO).New WHO classification of Endometrial Hyperplasias.Emons et al .GeburtshilfeFrauenheilkd.2015;75(2):135-136
•Hysteroscopic Resection in Fertility Sparing Surgery for Atypical Hyperplasia and Endometrial Cancer:Safety and Efficacy.De Marzi P et al.Jminim Invasive Gynaecol.2015Nov-Dec;22(7):1178-82
•Prediction of Relapse After Therapy Withdrawal in Women with Endometrial Hyperplasia:A long term follow up study.Stetten ET et al.AnticancerRes.2017May;37(5):2529-2536
RISK FACTORS FOR ENDOMETRIAL HYPERPLASIA• Obesity • Diabetes and hypertension• Polycystic ovarian syndrome(PCOS)• Nulliparity• Hormone replacement therapy and
tamoxifen• Lynch syndrome
![Endometrium presentation - Dr Wright[1] · Endometrial Hyperplasia Simple hyperplasia Complex hyperplasia (adenomatous) Simple atypical hyperplasia ... Progression of Hyperplasia](https://img.pdfslide.us/doc/110x75/5b8a421e7f8b9a50388bc13d/endometrium-presentation-dr-wright1-endometrial-hyperplasia-simple-hyperplasia.jpg)