Embed Size (px)
Citation preview

Tishk International University
Science Faculty
Medical Analysis Department
Pathology
Fourth Grade- Spring Semester 2020-2021
Dr. Jalal A. Jalal Assistant Professor of
Pathology
Neoplasia- 3, Epidemiology
of Cancer

EPIDEMIOLOGY
Cancer Incidence:
2

1. Geographic and Environmental Variables
3

Occupational Cancers
• Arsenic : Lung, skin, Angiosarcoma.
• Asbestos: Lung, mesothelioma;
• Benzene: Leukemia, Hodgkin lymphoma.
• Beryllium: Lung
• Cadmium: Prostate
• Chromium: Lung
• Ethylene oxide: Leukemia
• Nickel: Nose, lung
• Radon: Lung
• Vinyl chloride: Angiosarcoma, liver
4

2. Age
• In general, the frequency of cancer increases with
age.
• Most cancer mortality occurs between ages 55
and 75 years.
• Cancer causes about 10% of all deaths among
children younger than 15 years.
• The major lethal cancers in children are
leukemia,
tumors of the central nervous system,
lymphomas,
soft tissue sarcomas, and
bone sarcomas.5

3. Heredity
• Evidence now indicates that for many types ofcancer, there exist not only environmentalinfluences but also hereditary predispositions.
• In summary, about 5% to 10% of all human
cancers are categorized under hereditary forms
of cancer.
6

4. Acquired Preneoplastic Disorders
certain clinical conditions are well-recognizedpredispositions to the development of malignantneoplasia and are referred to as preneoplasticdisorders.1. Chronic skin fistula or a longstanding-unhealedskin wound may lead to Squamous cell carcinoma.2. Cirrhosis of the liver may lead to Hepatocellular
carcinoma.3. Atypical endometrial hyperplasia; may lead toEndometrial carcinoma.4. Dysplastic bronchial mucosa of habitual cigarettesmokers may lead to Bronchogenic carcinoma.
7

5. Chronic atrophic gastritis e.g., gastric carcinoma
in pernicious anemia or following long-standing
Helicobacter pylori infection.
6. Chronic ulcerative colitis (e.g., an increased
incidence of colorectal carcinoma in long-standing
disease).
7. Leukoplakia of the oral cavity (e.g., increased risk
of squamous cell carcinoma).
8. Villous adenomas of the colon (e.g., high risk of
transformation to colorectal carcinoma).
8

CARCINOGENESIS:
THE MOLECULAR BASIS OF CANCER
• Nonlethal genetic damage lies at the heart ofcarcinogenesis.
• Such genetic damage (or mutation) may beacquired by the action of environmental agents,such as chemicals, radiation, or viruses, or it maybe inherited in the germ line.
• The genetic hypothesis of cancer implies that atumor mass results from the clonal expansion ofa single progenitor cell that has incurred geneticdamage (i.e., tumors are monoclonal).
9

Four classes of normal regulatory genes are the
principal targets of genetic damage:
1. Growth-promoting proto-oncogenes,
2. Growth-inhibiting tumor suppressor genes,
3. Genes that regulate programmed cell death-
apoptosis
4. Genes involved in DNA repair.
10

• Mutant alleles of proto-oncogenes are called
oncogenes.
• They are considered dominant because
mutation of a single allele can lead to cellular
transformation.
• In contrast, typically both normal alleles of
tumor suppressor genes must be damaged for
transformation to occur, so this family of genes
is sometimes referred to as recessive
oncogenes.

• Genes that regulate apoptosis may be dominant,
as are proto-oncogenes, or they may behave as
tumor suppressor genes.
• DNA repair genes affect cell proliferation or
survival indirectly by influencing the ability of the
organism to repair nonlethal damage in other
genes, including proto-oncogenes, tumor
suppressor genes, and genes that regulate
apoptosis.
•
12

• A disability in the DNA repair genes can
predispose cells to widespread mutations in the
genome and thus to neoplastic transformation.
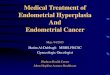
• Carcinogenesis is a multistep process at both
the phenotypic and the genetic levels, resulting
from the accumulation of multiple mutations.
• malignant neoplasms have several phenotypic
attributes, such as excessive growth, local
invasiveness, and the ability to metastases.

• It is well established that over a period of time,many tumors become more aggressive andacquire greater malignant potential.
• This phenomenon is referred to as tumorprogression.
• Even though most malignant tumors aremonoclonal in origin, by the time they becomeclinically evident, their constituent cells areextremely heterogeneous.
14

• tumor progression and associatedheterogeneity most likely result from multiplemutations that accumulate independently indifferent cells, generating subclones withdifferent characteristics.

16

17

30