CBE results of: Nipple discharge, no palpable mass Asymmetric thickening/nodularity Skin Changes (Peau d’ orange, Erythema,
Nipple Excoriation, Scaling/Eczema) Dominant Mass ? Unilateral Breast Pain Mammogram results of ACR 0 – Assessment Incomplete ACR 4 – Suspicious Abnormality, ACR 5 – Highly Suggestive of Malignancy
Abnormal CBE Results
Nipple Discharge Third most common breast complaint by
women seeking medical attention after lumps and breast pain
During breast self exam, fluid may be expressed from the breasts of 50% to 60% of Caucasian and African-American women and 40% of Asian-American women
Nipple Discharge cont. Palpation of the nipple in a woman who
does not have a history of persistent spontaneous nipple discharge - not recommended
Rationale: Non-spontaneous nipple discharge is a normal physiological phenomenon and of no clinical consequence
Infections (E.g. abscess) should be treated with incision and drainage or repeated aspiration if needed (consider antibiotics)
Nipple Discharge is of Concern if it is:
Blood stained, serosanguinous, serous (watery) with a red, pink, or brown color, or clear
90% of bloody discharges are intraductal papillomas; 10% are breast cancers)
appears spontaneously without squeezing the nipple
persistent on one side only (unilateral) a fluid other than breast milk
Presenter
Presentation Notes
Rust colored nipple discharge implies blood in the secretions from the gland and ducts of the breast. Bloody discharge is worrisome for basically two conditions: intraductal papilloma (about 90% of bloody nipple discharge) and intraductal or other types of breast cancer (about 10% of bloody nipple discharge). Rarely it can indicate other benign or inflammatory conditions but intraductal papilloma and cancer are the main two to rule in or rule out. Almost always, a rust colored or bloody nipple discharge come from only one of the breast ducts. A ductogram is an xray procedure in which a very small, blunt-ended plastic tube is placed in the nipple duct that is producing the discharge in order to inject dye and see if there is a papilloma in the duct.
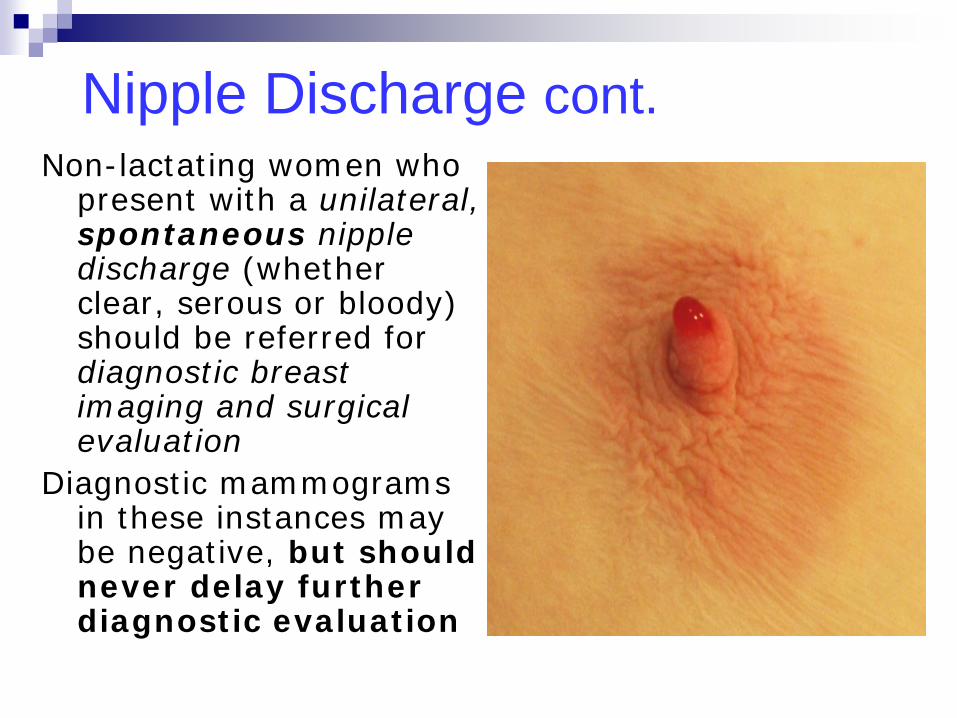
Nipple Discharge cont. Non-lactating women who
present with a unilateral, spontaneous nipple discharge (whether clear, serous or bloody) should be referred for diagnostic breast imaging and surgical evaluation
Diagnostic mammograms in these instances may be negative, but should never delay further diagnostic evaluation
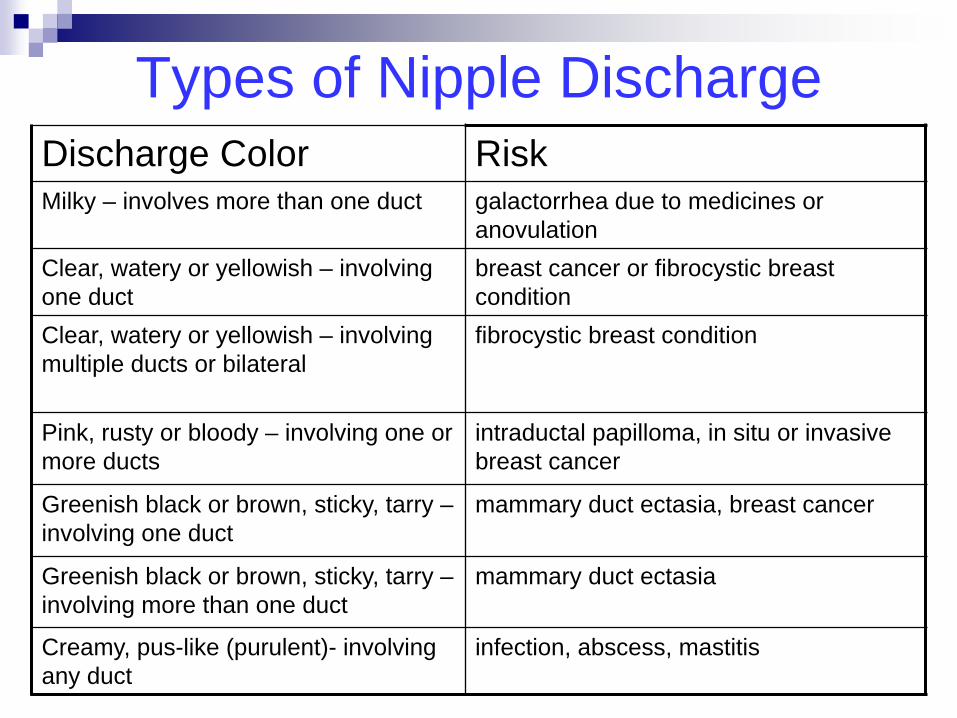
Types of Nipple Discharge Discharge Color Risk Milky – involves more than one duct galactorrhea due to medicines or
anovulation Clear, watery or yellowish – involving one duct
breast cancer or fibrocystic breast condition
Clear, watery or yellowish – involving multiple ducts or bilateral
fibrocystic breast condition
Pink, rusty or bloody – involving one or more ducts
intraductal papilloma, in situ or invasive breast cancer
Greenish black or brown, sticky, tarry – involving one duct
mammary duct ectasia, breast cancer
Greenish black or brown, sticky, tarry – involving more than one duct
mammary duct ectasia
Creamy, pus-like (purulent)- involving any duct
infection, abscess, mastitis
Nipple Discharge Follow-up CBE: Identify color/consistency of discharge Mammogram: If a suspicious mass together
with nipple discharge present – refer for additional imaging? and surgical consult
Further Diagnostic Tests: --Ductogram/Galactogram – not a
reimbursable BCCCP code. --Contact NC – may map procedure to a
BCCCP CPT code. Evaluated on a case by case basis.
Presenter
Presentation Notes
Galactography involves the retrograde injection of water-soluble radiopaque contrast material into a discharging duct with subsequent mammographic imaging. adjunctive imaging and biopsy as necessary. If these tests are negative and show no malignancy, nipple smear should be evaluated. Galactography is not indicated unless the nipple discharge is spontaneous, unilateral, and expressed from a single pore. If discharge cannot be expressed at the time of galactography, the affected duct cannot be identified or cannulated. Some papillomas are near the nipple and are large enough to be felt. In these cases, a needle biopsy can be done to test for malignancy or diagnose papilloma. In some cases, a galactogram (also called a ductogram) is performed to aid in diagnosing the cause of an abnormal nipple discharge such as intraductal papilloma. However, a ductogram that does not show an abnormality does not exclude the fact that a significant lesion may be present.
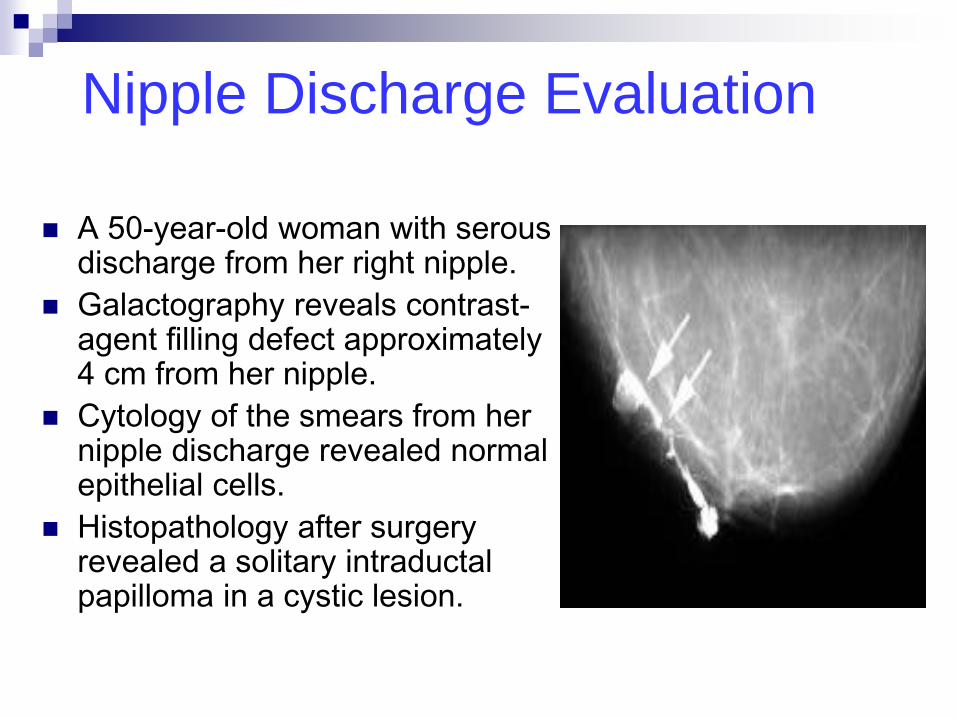
Nipple Discharge Evaluation
A 50-year-old woman with serous discharge from her right nipple.
Galactography reveals contrast-agent filling defect approximately 4 cm from her nipple.
Cytology of the smears from her nipple discharge revealed normal epithelial cells.
Histopathology after surgery revealed a solitary intraductal papilloma in a cystic lesion.
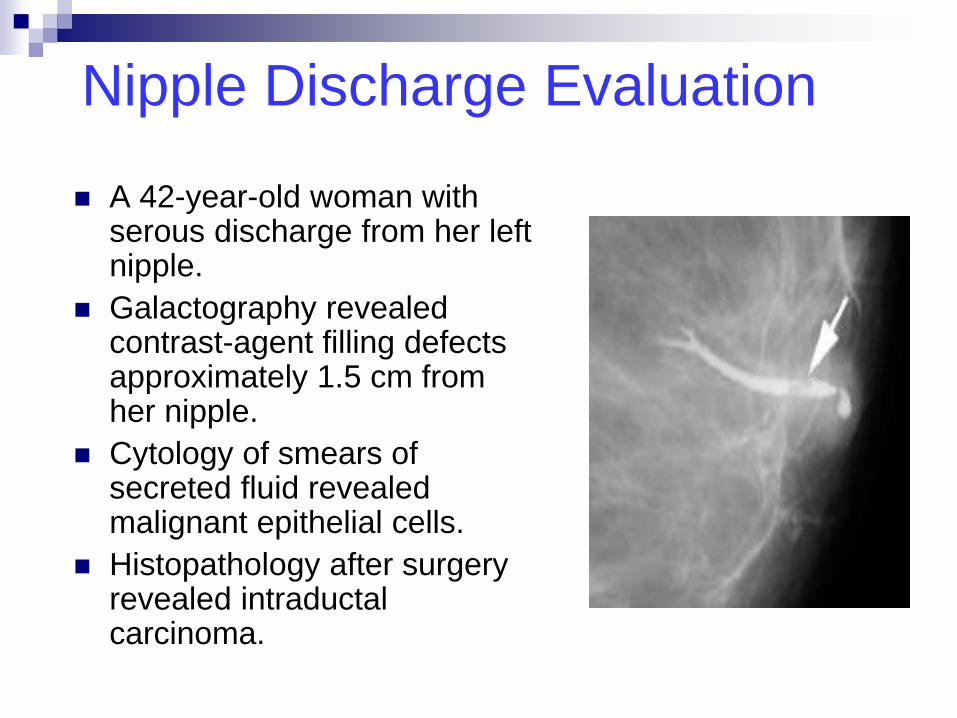
Nipple Discharge Evaluation
A 42-year-old woman with serous discharge from her left nipple.
Galactography revealed contrast-agent filling defects approximately 1.5 cm from her nipple.
Cytology of smears of secreted fluid revealed malignant epithelial cells.
Histopathology after surgery revealed intraductal carcinoma.
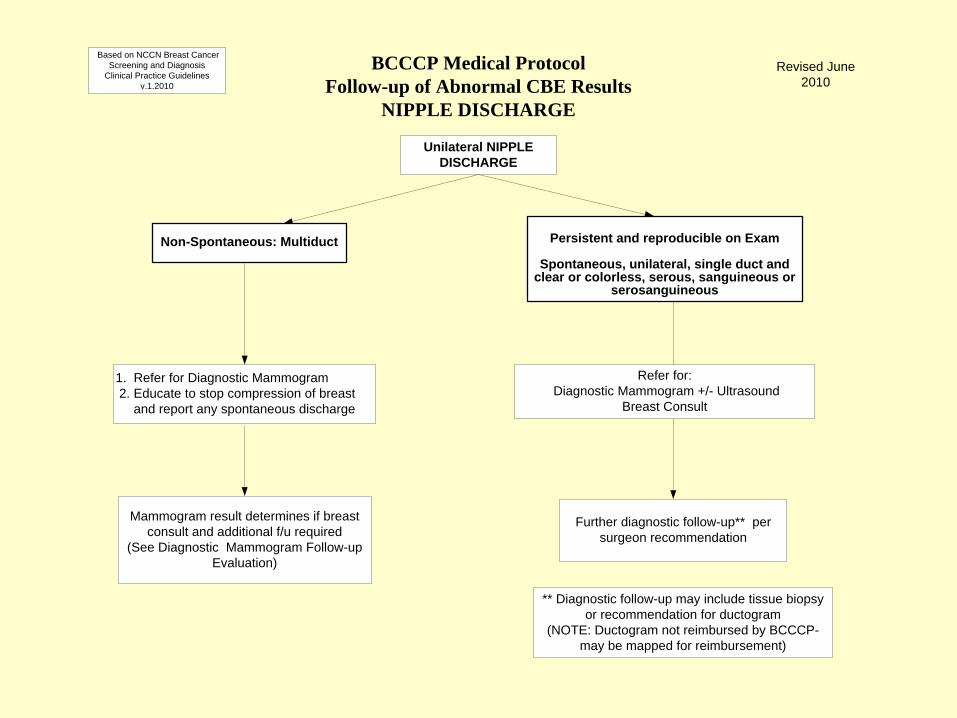
Non-Spontaneous: Multiduct
1. Refer for Diagnostic Mammogram 2. Educate to stop compression of breast and report any spontaneous discharge
Persistent and reproducible on Exam
Spontaneous, unilateral, single duct and
clear or colorless, serous, sanguineous or serosanguineous
Refer for: Diagnostic Mammogram +/- Ultrasound
Breast Consult
Mammogram result determines if breast consult and additional f/u required
(See Diagnostic Mammogram Follow-up Evaluation)
Further diagnostic follow-up** per surgeon recommendation
BCCCP Medical ProtocolFollow-up of Abnormal CBE Results
NIPPLE DISCHARGE
Based on NCCN Breast Cancer Screening and Diagnosis
Clinical Practice Guidelines v.1.2010
Revised June 2010
Unilateral NIPPLE DISCHARGE
** Diagnostic follow-up may include tissue biopsy or recommendation for ductogram
(NOTE: Ductogram not reimbursed by BCCCP- may be mapped for reimbursement)
Abnormal CBE Findings Asymmetrical Thickening vs.
Breast Mass Despite widespread use of screening
mammography, breast cancer presents as a palpable mass in the majority of cases
4:1 prevalence of benign breast mass compared to malignant
Variation in breast tissue nodularity among pre and post menopausal women is considerable
Presenter
Presentation Notes
Breast Mass or Asymmetrical Thickening (When is a Lump Just a Lump?): Despite the widespread use of screening mammography, breast cancer presents as a palpable mass in the majority of the cases. The prevalence of benign breast masses compared to those of malignant masses is at least four-to-one (4:1). The normal physiology of breast tissue is one of nodularity. The variation in tissue is in part determined by menstrual phase of the cycle; the vessels and stromal tissue become engorged during the luteal phase, resulting in increased nodularity. However, the variation in breast tissue nodularity among both premenopausal and postmenopausal women is considerable and must be recognized. The most difficult aspect of the CBE is deciding whether to regard an area of concern as part of the normal, physiologic nodularity or as a dominant mass. Distinguishing between benign disease and malignancy can be challenging. Making this distinction demands that the clinician strike a balance between the goal of high-quality, cost-effective care that maximizes the timely diagnosis of malignancy and efforts to avoid unnecessary surgical biopsy. In a 1995 study by the Physician’s Insurers Association of America, failure to diagnose breast cancer was shown to be the most common reason for malpractice litigation. In the same study, breast cancer claims accounted for the highest amount of claim dollars paid. The most common error made by physicians in these cases was to discount either the patient’s or their own findings of a palpable abnormality on CBE. Physiologic nodularity often is referred to as fibrocystic breast disease. However, this designation is incorrect. Such nodularity is, in fact, physiologic. Thus, the issue is not one of treatment. Instead, it is how to best follow patients with dense and nodular breast tissue so as to maintain high sensitivity without sacrificing specificity in the clinical breast examination. Documenting the areas of nodularity is critical to the clinician’s ability to follow differences in the examination over time. Re-examination during the follicular phase can often clarify findings in premenopausal women. Although data have not conclusively shown any benefit of caffeine elimination, some isolated small studies have shown that a caffeine-free diet can reduce clinically palpable breast findings. Repeating the examination several months after a decrease in caffeine consumption can provide additional reassurance of the benign nature of clinically palpable findings if they can be documented as decreasing in size. Lack of adherence to breast self-examination is in part related to anxiety that can arise because of this nodularity. Reviewing the finding of nodularity provides women with information and reassurance about what they are finding on their own, which will be of value for their own examinations. For patients with normal breast cancer risk, annual examination by a health care provider is recommended. For women who have a high risk of breast cancer and extensive nodularity on CBE, examinations every six months by a health care provider may be of benefit in detecting new findings, although this has not been studied.
Asymmetrical Thickening or Lump
Challenge to clinicians: Is the area of concern
part of the normal physiologic nodularity of the breast or is it a dominant mass?
Physiologic nodularity is often referred to as fibrocystic disease - designation is incorrect
Such nodularity is, in fact, physiologic. - the issue is not one of treatment but of follow-up monitoring
Breast consult to decide if immediate or short-term follow-up required.
Presenter
Presentation Notes
Breast Mass or Asymmetrical Thickening (When is a Lump Just a Lump?): Physiologic nodularity often is referred to as fibrocystic breast disease. However, this designation is incorrect. Although data have not conclusively shown any benefit of caffeine elimination, some isolated small studies have shown that a caffeine-free diet can reduce clinically palpable breast findings. Repeating the examination several months after a decrease in caffeine consumption can provide additional reassurance of the benign nature of clinically palpable findings if they can be documented as decreasing in size. Lack of adherence to breast self-examination is in part related to anxiety that can arise because of this nodularity. Reviewing the finding of nodularity provides women with information and reassurance about what they are finding on their own, which will be of value for their own examinations. For patients with normal breast cancer risk, annual examination by a health care provider is recommended. For women who have a high risk of breast cancer and extensive nodularity on CBE, examinations every six months by a health care provider may be of benefit in detecting new findings, although this has not been studied.
Asymmetrical Thickening or Lump
Providers need to decide how to best follow patients with dense and nodular breast tissue so as to maintain high sensitivity without sacrificing specificity in the clinical breast examination
Reassuring women about what they are finding on their own may alleviate some of the anxiety
For patients with normal breast cancer risk, annual examination by a health care provider is recommended
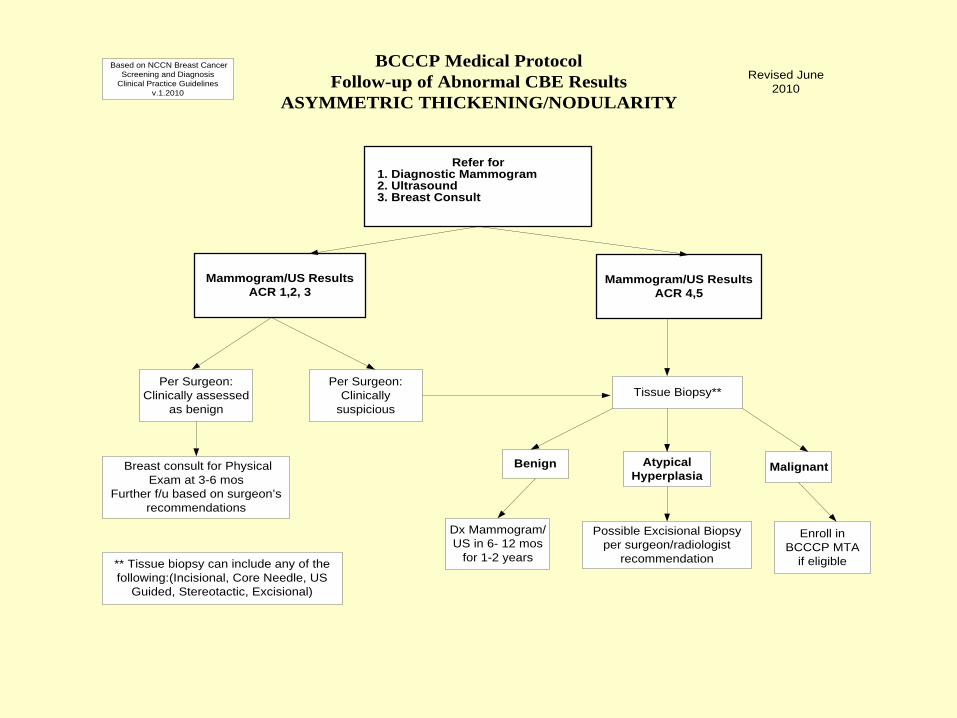
Refer for 1. Diagnostic Mammogram 2. Ultrasound 3. Breast Consult
Mammogram/US ResultsACR 1,2, 3
Breast consult for PhysicalExam at 3-6 mos
Further f/u based on surgeon’srecommendations
Per Surgeon:Clinically assessed
as benignTissue Biopsy**
Mammogram/US ResultsACR 4,5
BCCCP Medical ProtocolFollow-up of Abnormal CBE Results
ASYMMETRIC THICKENING/NODULARITY
Based on NCCN Breast CancerScreening and Diagnosis
Clinical Practice Guidelinesv.1.2010
Revised June2010
Per Surgeon:Clinically
suspicious
Benign AtypicalHyperplasia
Malignant
Dx Mammogram/US in 6- 12 mos
for 1-2 years
Possible Excisional Biopsyper surgeon/radiologist
recommendation
Enroll inBCCCP MTA
if eligible** Tissue biopsy can include any of thefollowing:(Incisional, Core Needle, US
Guided, Stereotactic, Excisional)
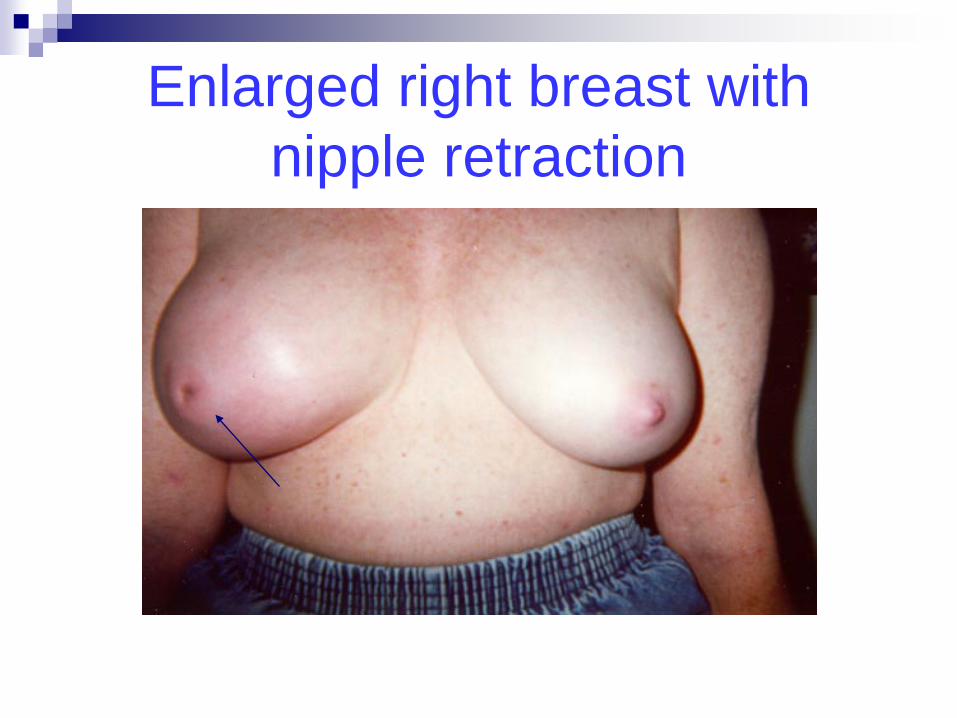
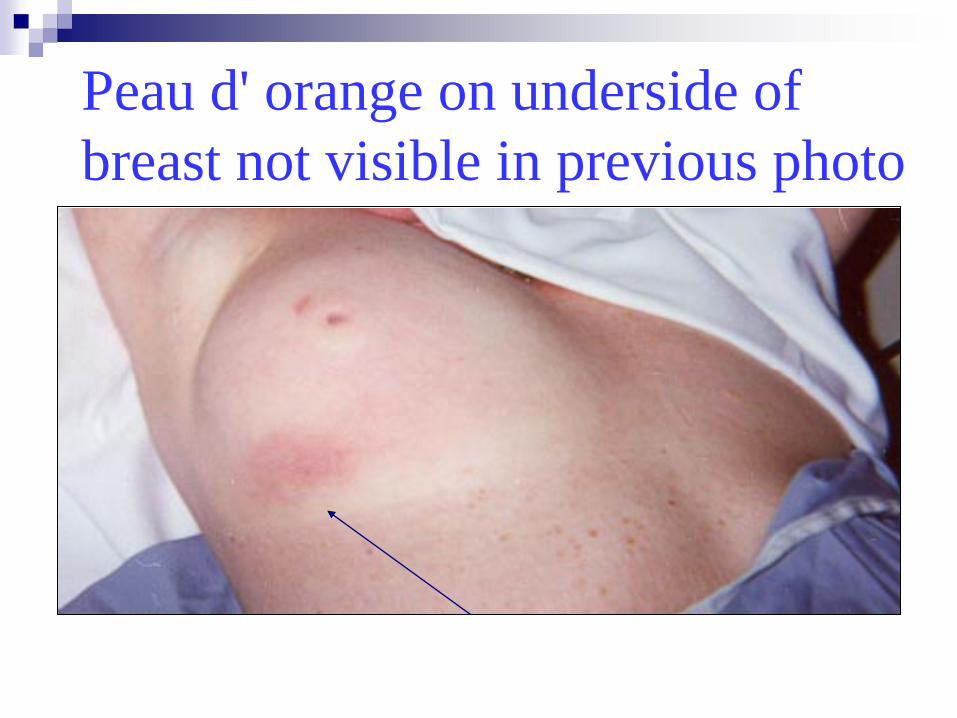
Nipple retraction • Cancer until proven otherwise! • Suggests retroareolar mass Peau d'orange • Breast skin dotted like the skin of an orange • Very ominous sign – carcinoma when present
over a lump; suggests lymph node involvement
Abnormal CBE Results Skin Changes (Red Flags)
Paget’s Disease of the Nipple • Skin Retraction • Skin Dimpling/Puckering (skin pulled in by an
underlying carcinoma) Breast Erythema • In non-lactating women: Ominous if
persistent mastitis greater than 2 weeks; suggests inflammatory carcinoma
• In elderly women: erythema with ulceration may suggest neglected carcinoma
Visible lump • May be due to cysts, giant fibroadenoma,
carcinoma
Skin Changes (Red Flags)
Enlarged right breast with nipple retraction
Peau d' orange on underside of breast not visible in previous photo
Paget’s Disease of the Nipple
Breast Erythema: Inflammatory Carcinoma
Skin Changes – Follow-Up Diagnostic work-up for any unilateral breast skin
changes or nipple retraction An inflammatory appearance of the breast in any
woman older than 40 should be considered inflammatory breast cancer until proven otherwise
Bilateral diagnostic mammography is the first line of investigation - should be followed by a surgical consultation and a biopsy of the breast and skin.
? Possible infection vs. cancer
Subtle skin changes (rash, scaliness) Refer to surgeon (unless NP can prescribe
antibiotics) Re-evaluate after antibiotics completed If not resolved, refer for diagnostic work-up
to rule out cancer
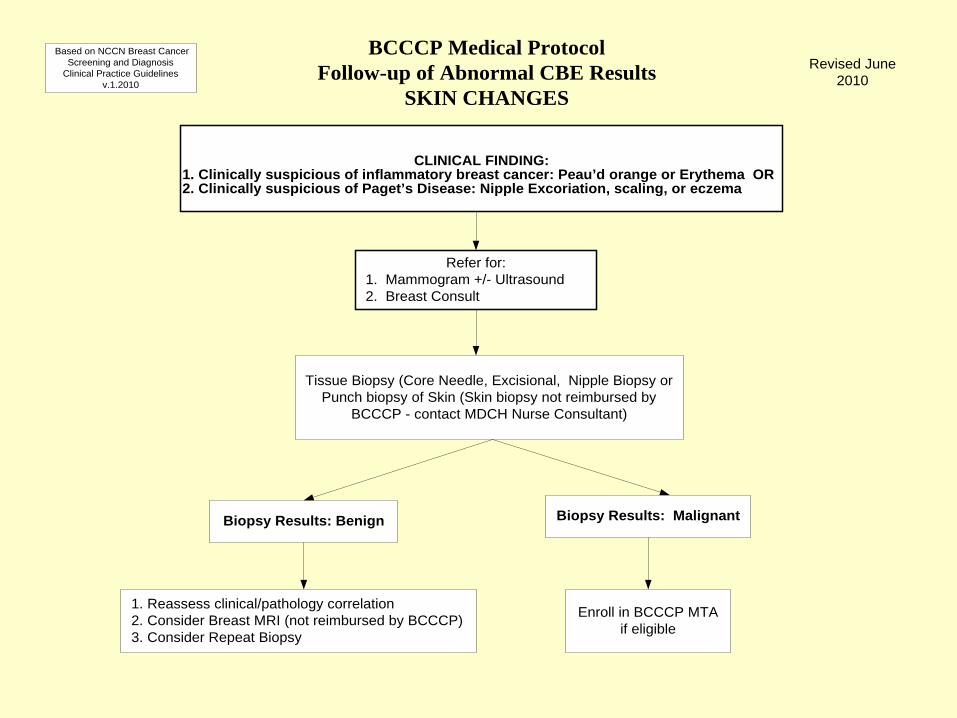
CLINICAL FINDING:1. Clinically suspicious of inflammatory breast cancer: Peau’d orange or Erythema OR2. Clinically suspicious of Paget’s Disease: Nipple Excoriation, scaling, or eczema
Refer for: 1. Mammogram +/- Ultrasound 2. Breast Consult
Enroll in BCCCP MTAif eligible
Tissue Biopsy (Core Needle, Excisional, Nipple Biopsy orPunch biopsy of Skin (Skin biopsy not reimbursed by
BCCCP - contact MDCH Nurse Consultant)
Biopsy Results: Benign
1. Reassess clinical/pathology correlation 2. Consider Breast MRI (not reimbursed by BCCCP) 3. Consider Repeat Biopsy
Biopsy Results: Malignant
BCCCP Medical ProtocolFollow-up of Abnormal CBE Results
SKIN CHANGES
Based on NCCN Breast CancerScreening and Diagnosis
Clinical Practice Guidelinesv.1.2010
Revised June2010
Abnormal CBE Findings Breast Mass
Characteristics of Malignant CBE Findings True masses are generally: • asymmetrical in relation to the other breast • distinct from the surrounding tissues • are three dimensional Cancerous mass: • may be firm • have attachments to skin or deep fascia with dimpling or nipple retraction
Presenter
Presentation Notes
True masses are generally asymmetrical in relation to the other breast, distinct from the surrounding tissues, and three dimensional . A typical cancer may be firm, have indistinct borders, and have attachments to the skin or deep fascia with dimpling or nipple retraction. Benign lesions typically have discrete, well defined margins and are mobile. Cysts can be difficult to distinguish by palpation from solid masses. In one study only 58% of 66 palpable cysts were correctly identified by physical examination. Significant disagreement among experienced examiners may occur. In another study, four surgeons performed physical examination independently and agreed on the need for biopsy of only 73% of 15 masses subsequently proven malignant. Because many breast masses may not exhibit distinctive physical findings, an imaging evaluation is necessary in almost all cases to characterize the palpable lesion and screen the remainder of each breast for additional lesions. Unfortunately not all palpable breast masses will be visualized with conventional imaging techniques. In the Breast Cancer Detection Demonstration Project (BCDDP) which began in 1970, nine percent (9%) of the cancers were found by CBE alone. With improvement in imaging methods since the BCDDP, this percentage should be considerably less. Nevertheless, a negative imaging evaluation should never overrule a strongly suspicious finding on physical examination or visa versa. Based upon the clinician’s interpretation of the findings, a diagnostic mammogram may be ordered instead of a screening mammogram for these women. Women who present with symptoms may need further tests to identify if the problem might indicate the presence of breast cancer. When a patient presents with signs or symptoms, the clinician should ask specific questions to determine the exact type of symptoms the woman has. Answers to these questions help guide the clinician in determining follow-up diagnostic testing. Breast cancers present clinically in considerably varied ways. If a mass is found, it is important to consider relevant clinical factors, such as patient age, menstrual cycle (and whether there are changes in symptoms associated with the cycle), hormone use, trauma, duration, changes over time, and individual risk factors. Breast disorders that require further diagnostic work-up include: breast pain; a mass or asymmetrical thickening, nipple discharge, and observed skin, or nipple changes.
Benign CBE Findings
Characteristics of Benign Lesions • Have discrete, well defined margins • Are generally mobile NOTE: • DO NOT rely on palpation alone to determine a
malignant from benign mass • Full diagnostic work-up is required to confirm
malignant from bengn mass
Presenter
Presentation Notes
Because many breast masses may not exhibit distinctive physical findings, an imaging evaluation is necessary in almost all cases to characterize the palpable lesion and screen the remainder of each breast for additional lesions. Unfortunately not all palpable breast masses will be visualized with conventional imaging techniques. In the Breast Cancer Detection Demonstration Project (BCDDP) which began in 1970, nine percent (9%) of the cancers were found by CBE alone. With improvement in imaging methods since the BCDDP, this percentage should be considerably less. Nevertheless, a negative imaging evaluation should never overrule a strongly suspicious finding on physical examination or visa versa. Based upon the clinician’s interpretation of the findings, a diagnostic mammogram may be ordered instead of a screening mammogram for these women. Women who present with symptoms may need further tests to identify if the problem might indicate the presence of breast cancer. When a patient presents with signs or symptoms, the clinician should ask specific questions to determine the exact type of symptoms the woman has. Answers to these questions help guide the clinician in determining follow-up diagnostic testing. Breast cancers present clinically in considerably varied ways. If a mass is found, it is important to consider relevant clinical factors, such as patient age, menstrual cycle (and whether there are changes in symptoms associated with the cycle), hormone use, trauma, duration, changes over time, and individual risk factors. Breast disorders that require further diagnostic work-up include: breast pain; a mass or asymmetrical thickening, nipple discharge, and observed skin, or nipple changes.
Abnormal CBE Findings Cysts vs. solid masses
• Cysts can be difficult to distinguish by palpation from
solid masses • Studies show equivocal results -- In one study, 58% of 66 palpable cysts were correctly
identified by physical examination -- In a second study, 4 surgeons performed physical
exams independently – they agreed on the need for biopsy in 73% of 15 masses subsequently proven malignant
An imaging evaluation is necessary in almost all cases to
characterize the type of lesion
Presenter
Presentation Notes
Cysts can be difficult to distinguish by palpation from solid masses. In one study only 58% of 66 palpable cysts were correctly identified by physical examination. Significant disagreement among experienced examiners may occur. In another study, four surgeons performed physical examination independently and agreed on the need for biopsy of only 73% of 15 masses subsequently proven malignant. Because many breast masses may not exhibit distinctive physical findings, an imaging evaluation is necessary in almost all cases to characterize the palpable lesion and screen the remainder of each breast for additional lesions. Unfortunately not all palpable breast masses will be visualized with conventional imaging techniques. In the Breast Cancer Detection Demonstration Project (BCDDP) which began in 1970, nine percent (9%) of the cancers were found by CBE alone. With improvement in imaging methods since the BCDDP, this percentage should be considerably less. Nevertheless, a negative imaging evaluation should never overrule a strongly suspicious finding on physical examination or visa versa. Based upon the clinician’s interpretation of the findings, a diagnostic mammogram may be ordered instead of a screening mammogram for these women. Women who present with symptoms may need further tests to identify if the problem might indicate the presence of breast cancer. When a patient presents with signs or symptoms, the clinician should ask specific questions to determine the exact type of symptoms the woman has. Answers to these questions help guide the clinician in determining follow-up diagnostic testing. Breast cancers present clinically in considerably varied ways. If a mass is found, it is important to consider relevant clinical factors, such as patient age, menstrual cycle (and whether there are changes in symptoms associated with the cycle), hormone use, trauma, duration, changes over time, and individual risk factors. Breast disorders that require further diagnostic work-up include: breast pain; a mass or asymmetrical thickening, nipple discharge, and observed skin, or nipple changes.
Drawbacks of Imaging for Breast Abnormalities
Not all palpable breast masses will be visualized with conventional imaging techniques
Breast Cancer Detection Demonstration Project (BCDDP), which began in 1970, found 9% of cancers by CBE alone – this % is now less due to improvements in imaging technology
A NEGATIVE MAMMOGRAM SHOULD NEVER
OVERRULE A STRONGLY SUSPICIOUS FINDING ON PHYSICAL EXAM– FURTHER FOLLOW-UP IS REQUIRED BEYOND THE MAMMOGRAM
Presenter
Presentation Notes
Because many breast masses may not exhibit distinctive physical findings, an imaging evaluation is necessary in almost all cases to characterize the palpable lesion and screen the remainder of each breast for additional lesions. Unfortunately not all palpable breast masses will be visualized with conventional imaging techniques. In the Breast Cancer Detection Demonstration Project (BCDDP) which began in 1970, nine percent (9%) of the cancers were found by CBE alone. With improvement in imaging methods since the BCDDP, this percentage should be considerably less. Nevertheless, a negative imaging evaluation should never overrule a strongly suspicious finding on physical examination or visa versa.
Abnormal CBE Findings Clinical management
of breast mass Breast cancers present clinically in varied ways When a mass is found consider the following:
Patient age, menstrual cycle (and whether the change in symptoms are associated with the cycle), hormone use, trauma, durations, changes over time, individual risk factors, & presence of mass in one breast or both breasts
Presenter
Presentation Notes
Breast cancers present clinically in considerably varied ways. If a mass is found, it is important to consider relevant clinical factors, such as patient age, menstrual cycle (and whether there are changes in symptoms associated with the cycle), hormone use, trauma, duration, changes over time, and individual risk factors. Breast disorders that require further diagnostic work-up include: breast pain; a mass or asymmetrical thickening, nipple discharge, and observed skin, or nipple changes.
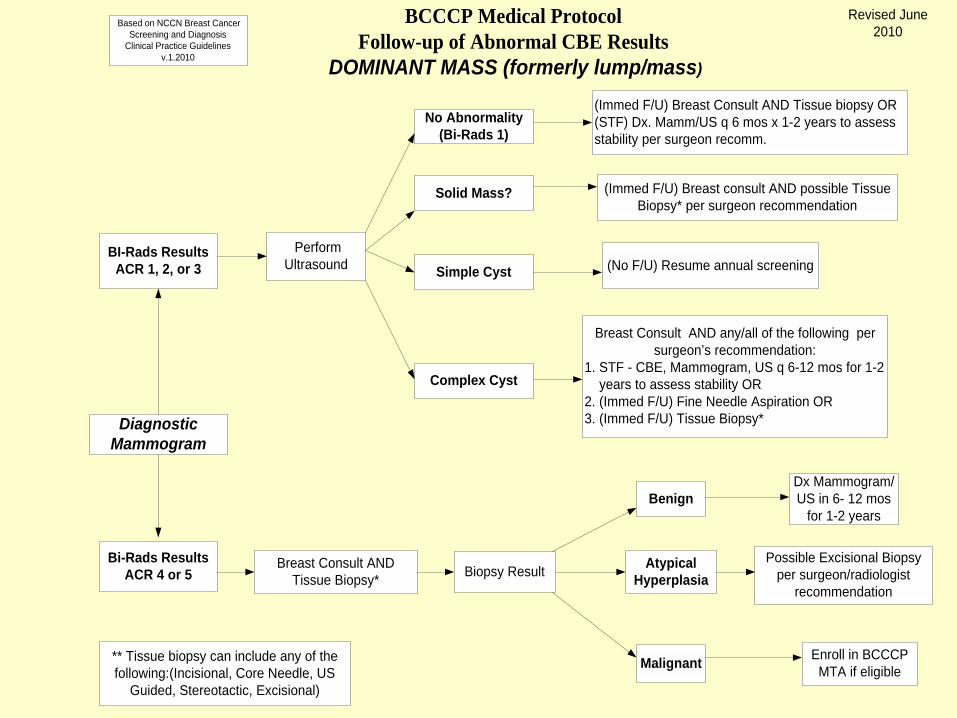
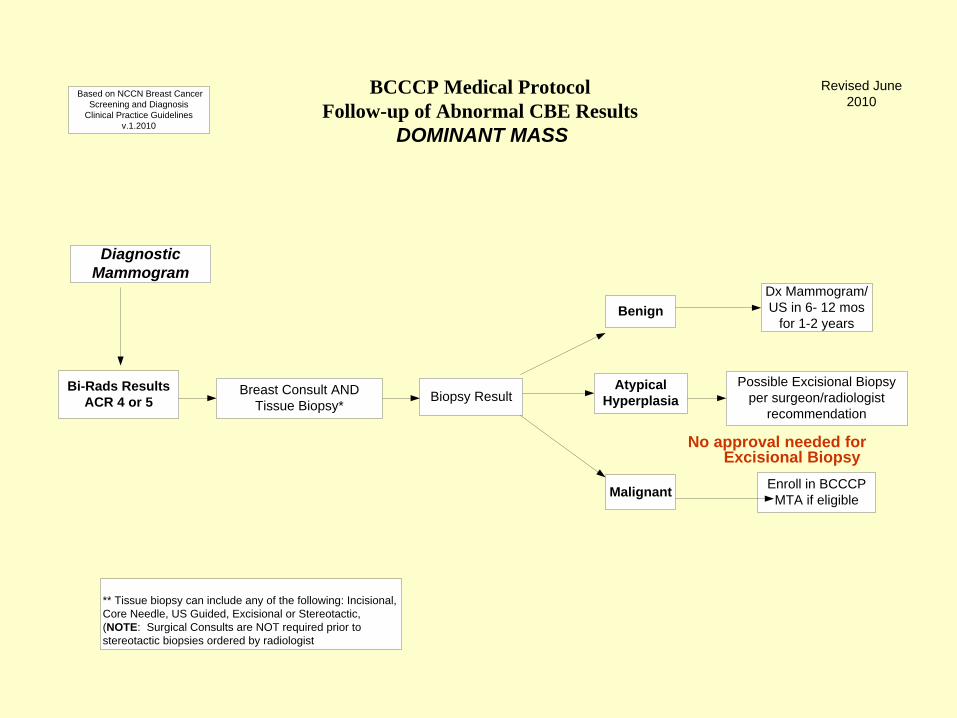
BCCCP Medical ProtocolFollow-up of Abnormal CBE Results
DOMINANT MASS (formerly lump/mass)
DiagnosticMammogram
BI-Rads ResultsACR 1, 2, or 3
Bi-Rads ResultsACR 4 or 5
PerformUltrasound
No Abnormality(Bi-Rads 1)
(Immed F/U) Breast Consult AND Tissue biopsy OR(STF) Dx. Mamm/US q 6 mos x 1-2 years to assessstability per surgeon recomm.
Solid Mass?
Simple Cyst
(Immed F/U) Breast consult AND possible TissueBiopsy* per surgeon recommendation
Breast Consult AND any/all of the following persurgeon’s recommendation:
1. STF - CBE, Mammogram, US q 6-12 mos for 1-2 years to assess stability OR2. (Immed F/U) Fine Needle Aspiration OR3. (Immed F/U) Tissue Biopsy*
Complex Cyst
(No F/U) Resume annual screening
Breast Consult ANDTissue Biopsy*
BenignDx Mammogram/US in 6- 12 mos
for 1-2 years
Biopsy Result AtypicalHyperplasia
Malignant
Possible Excisional Biopsyper surgeon/radiologist
recommendation
Enroll in BCCCPMTA if eligible
** Tissue biopsy can include any of thefollowing:(Incisional, Core Needle, US
Guided, Stereotactic, Excisional)
Based on NCCN Breast CancerScreening and Diagnosis
Clinical Practice Guidelinesv.1.2010
Revised June2010
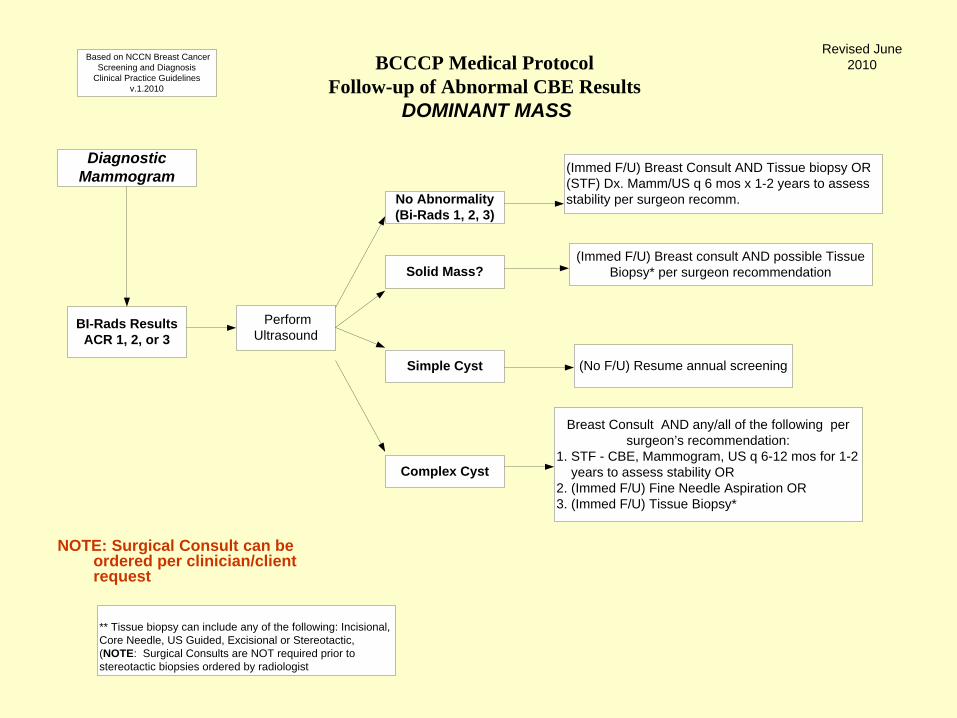
BCCCP Medical ProtocolFollow-up of Abnormal CBE Results
DOMINANT MASS
Diagnostic Mammogram
BI-Rads ResultsACR 1, 2, or 3
Perform Ultrasound
No Abnormality (Bi-Rads 1, 2, 3)
(Immed F/U) Breast Consult AND Tissue biopsy OR (STF) Dx. Mamm/US q 6 mos x 1-2 years to assess stability per surgeon recomm.
Solid Mass?
Simple Cyst
(Immed F/U) Breast consult AND possible Tissue Biopsy* per surgeon recommendation
Breast Consult AND any/all of the following per surgeon’s recommendation:
1. STF - CBE, Mammogram, US q 6-12 mos for 1-2 years to assess stability OR2. (Immed F/U) Fine Needle Aspiration OR3. (Immed F/U) Tissue Biopsy*
Complex Cyst
(No F/U) Resume annual screening
** Tissue biopsy can include any of the following: Incisional, Core Needle, US Guided, Excisional or Stereotactic, (NOTE: Surgical Consults are NOT required prior to stereotactic biopsies ordered by radiologist
Based on NCCN Breast Cancer Screening and Diagnosis
Clinical Practice Guidelines v.1.2010
Revised June 2010
NOTE: Surgical Consult can be ordered per clinician/client request
CBE Result: Dominant Mass (Coded as Abnormality/Rule Out Cancer)
IF the Mammogram AND Ultrasound Results are ANY combination of ACR 1, 2, OR 3
Refer for Follow-up Surgical Consult AND Possible Tissue Biopsy (per surgeon’s
recommendation) OR 6 month follow-up Diagnostic Mammogram*
and/or Ultrasound* along with Surgical Consult* *BCCCP will reimburse
CBE Result: Dominant Mass (Coded as Abnormality/Rule Out Cancer)
IF the Mammogram Result is ACR 1, 2, OR 3 AND Ultrasound Result shows SOLID mass
Refer for Follow-up Surgical Consult AND/OR Tissue Biopsy (per radiologist’s OR
surgeon’s recommendation)
CBE Result: Dominant Mass (Coded as Abnormality/Rule Out Cancer)
IF the Mammogram Result is ACR 1, 2, OR 3 AND Ultrasound Result shows SIMPLE CYST No Follow-up Required NOTE: If cyst painful may refer to surgeon to perform
FNA Post FNA mammogram/US will be reimbursed to
determine if cyst refilled
CBE Result: Dominant Mass (Coded as Abnormality/Rule Out Cancer)
IF the Mammogram Result is ACR 1, 2, OR 3 AND Ultrasound Result shows COMPLEX CYST Refer for Follow-up Surgical Consult AND any/all of the following per surgeon’s
recommendation: Fine Needle Aspiration* AND/OR Tissue Biopsy* OR CBE, and/or Mammogram, and/or Ultrasound in 6 months
to assess stability OR NOTE: *BCCCP will reimburse consult post aspiration/
biopsy to assess stability of cyst
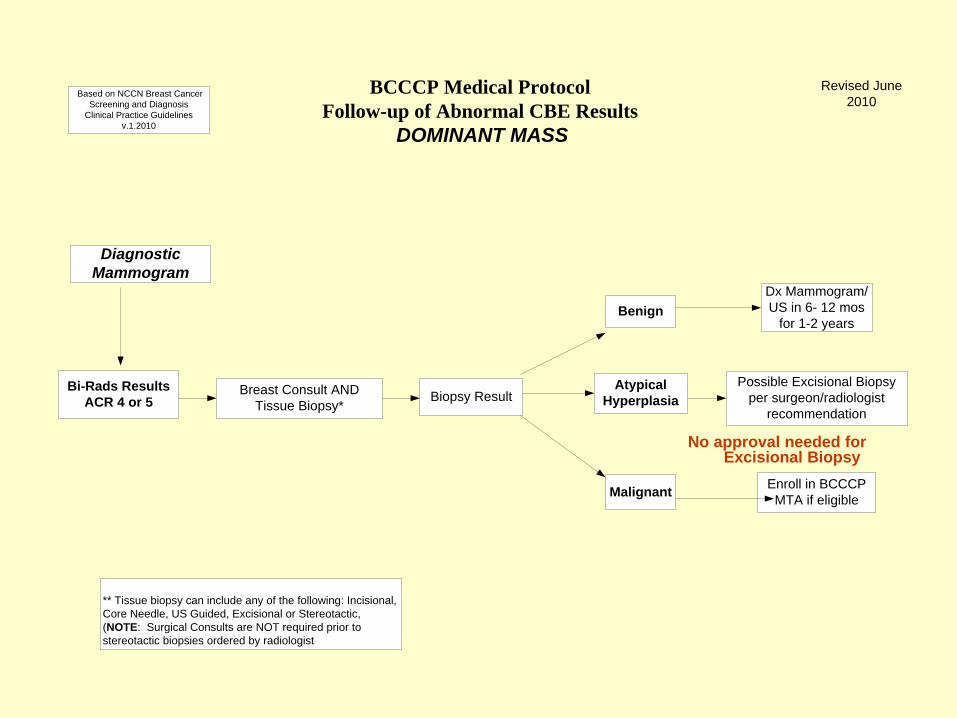
BCCCP Medical ProtocolFollow-up of Abnormal CBE Results
DOMINANT MASS
Diagnostic Mammogram
Bi-Rads ResultsACR 4 or 5
Breast Consult AND Tissue Biopsy*
BenignDx Mammogram/US in 6- 12 mos
for 1-2 years
Biopsy ResultAtypical
Hyperplasia
Malignant
Possible Excisional Biopsy per surgeon/radiologist
recommendation
Enroll in BCCCP MTA if eligible
** Tissue biopsy can include any of the following: Incisional, Core Needle, US Guided, Excisional or Stereotactic, (NOTE: Surgical Consults are NOT required prior to stereotactic biopsies ordered by radiologist
Based on NCCN Breast Cancer Screening and Diagnosis
Clinical Practice Guidelines v.1.2010
Revised June 2010
No approval needed for Excisional Biopsy
Pre/post Biopsy Questions (Contact NC for guidance)
Abscess post biopsy (Will reimburse for surgeon’s f/u visits; cannot reimburse
for I & D or antibiotics) Lymph node biopsy (If to r/o breast cancer, can map lymph node biopsy to
BCCCP code; cannot reimburse if to r/o anything unrelated to breast cancer)
Atypical hyperplasia – (Can reimburse for Excisional biopsy and 6 month f/u
mammogram/surgical consult; cannot reimburse for oncology referral or chemoprevention therapy)
Follow-up of Breast Pain
Most common breast complaint Etiology is unclear – most commonly occurs 1
week prior to menses and in some women on HRT
Causes worry and anxiety about breast cancer (Among women with breast pain who have a
normal CBE and radiologic studies, cancer will be found in about 0.5% upon f/u)
Presenter
Presentation Notes
Breast Pain: Breast pain is the most common breast complaint, and it should be taken seriously. In one large survey, 66 percent of women reported it. Unfortunately, the etiology is often unclear. Breast pain is usually hormonally related in that it occurs commonly 1 week prior to menses and in some women taking hormone replacement therapy. When women present with breast pain, clinicians should take a thorough medical history and conduct a physical exam to determine the cause of the pain. Breast pain is a symptom that can cause anxiety and worry about breast cancer. When patients present with breast pain, health care providers should ask questions to determine the following: · Location and duration of the pain; · Whether the pain is unilateral or bilateral; · Patient-ranked degree of discomfort (on a 10-point scale); · Whether the pain is cyclic, whether it changes with the patient’s menstrual cycle, and, if appropriate, whether it is related to hormone replacement therapy; and · Whether the pain has altered the patient’s lifestyle (e.g., whether it has interfered with exercise, hugs, sexual activity, or sleep). Among those women presenting with breast pain who have a normal CBE and radiologic studies, cancer will be found in about 0.5 percent upon follow-up. Women with persistent mastalgia should have three- to six-month follow-up exams. Once breast cancer has been ruled out, it is important to communicate to the woman that mastalgia is very common. Occasionally, substituting a more supportive brassiere, lowering the dose of estrogen, or substituting a different form of estrogen can be helpful. In women unrelieved by these measures, drug intervention (i.e., evening primrose oil, danazol, or bromocriptine) can be useful. Cyclic pain is more responsive than non-cyclic pain.
Breast Pain Follow-up cont.
HCP should determine the cause of pain Location and duration of the pain Unilateral or bilateral Patient ranked discomfort (scale 1-10) Whether the pain is cyclic, changes with
menstrual cycle or related to HRT Whether the pain has altered patient’s lifestyle
(interfered with exercise, hugs, sexual activity, sleep)
Presenter
Presentation Notes
Breast Pain: Breast pain is the most common breast complaint, and it should be taken seriously. In one large survey, 66 percent of women reported it. Unfortunately, the etiology is often unclear. Breast pain is usually hormonally related in that it occurs commonly 1 week prior to menses and in some women taking hormone replacement therapy. When women present with breast pain, clinicians should take a thorough medical history and conduct a physical exam to determine the cause of the pain. Breast pain is a symptom that can cause anxiety and worry about breast cancer. When patients present with breast pain, health care providers should ask questions to determine the following: · Location and duration of the pain; · Whether the pain is unilateral or bilateral; · Patient-ranked degree of discomfort (on a 10-point scale); · Whether the pain is cyclic, whether it changes with the patient’s menstrual cycle, and, if appropriate, whether it is related to hormone replacement therapy; and · Whether the pain has altered the patient’s lifestyle (e.g., whether it has interfered with exercise, hugs, sexual activity, or sleep). Among those women presenting with breast pain who have a normal CBE and radiologic studies, cancer will be found in about 0.5 percent upon follow-up. Women with persistent mastalgia should have three- to six-month follow-up exams. Once breast cancer has been ruled out, it is important to communicate to the woman that mastalgia is very common. Occasionally, substituting a more supportive brassiere, lowering the dose of estrogen, or substituting a different form of estrogen can be helpful. In women unrelieved by these measures, drug intervention (i.e., evening primrose oil, danazol, or bromocriptine) can be useful. Cyclic pain is more responsive than non-cyclic pain.
Common cause of pain Fibrocystic Breast Condition
Occurs from changes in the glandular and stromal tissues of the breast
Changes are related to a woman’s menstrual cycle and the hormones, estrogen and progesterone
Women with fibrocystic breasts often have bilateral cyclic breast pain or tenderness that coincides with their menstrual cycles
Presenter
Presentation Notes
Symptoms of fibrocystic breasts include: cysts (fluid-filled sacs) fibrosis (formation of scar-like connective tissue) lumpiness areas of thickening tenderness pain The degree to which women experience these symptoms varies significantly. Some women with fibrocystic breasts only experience mild breast pain and may not be able to feel any breast lumps when performing breast self-exams. Other women with fibrocystic breasts may experience more severe breast pain or tenderness and may feel multiple lumps in their breasts. Most fibrocystic breast lumps are found in the upper, outer quadrant of the breasts (near the axilla, armpit, region), although these lumps can occur anywhere in the breasts. Fibrocystic breast lumps tend to be smooth, rounded, and mobile (not attached to other breast tissue), though some fibrocystic tissue may have a thickened, irregular feel. The lumps or irregularities associated with fibrocystic breasts are often tender to touch and may increase or decrease in size during the menstrual cycle. What is Fibrocystic Breast Disease? In the past, many physicians have referred to fibrocystic breasts, or lumpy breasts, as "fibrocystic breast disease." This term is misleading because fibrocystic breast condition is not a disease at all. Rather, it is a common, non-cancerous breast condition that affects over half of all women at some point in their lives. Today, most physicians refer to this condition as "fibrocystic breast condition" or "fibrocystic breast change." Other terms that may be used to describe the condition include "cystic disease," "chronic cystic mastitis," or "mammary dysplasia." In fact, since fibrocystic breasts are so common among women during their reproductive years, some physicians do not even like to label the symptoms as a "condition." They believe that these women simply have lumpier and more tender breasts than others. What Causes Fibrocystic Breasts? How Are Fibrocystic Breasts Diagnosed? Fibrocystic breasts are often first noticed by the woman, and further investigated by her physician. Breast tenderness, pain, and/or lumpiness are common indicators of fibrocystic breasts, especially when they coincide with menstruation. Often, fibrocystic breasts will be diagnosed with a physician-performed clinical breast exam alone. While having fibrocystic breasts is usually not a risk factor for breast cancer, the condition can sometimes make breast cancer more difficult to detect. Therefore, in some cases, breast imaging exams, such as mammography or ultrasound, will need to be performed on women who show symptoms of fibrocystic breasts. However, screening mammography may be more difficult to perform on women with fibrocystic breasts because the breast density associated with fibrocystic breasts may eclipse breast cancer on the mammogram film. In some cases, additional mammography or ultrasound imaging, followed by fine needle aspiration or biopsy, will be performed on women with fibrocystic breasts to determine whether breast cancer is present. Fine needle aspiration (to drain large, painful cysts) may also be performed by a physician help relieve some of the more severe symptoms of fibrocystic breast condition. How Are Fibrocystic Breasts Treated? Often, physicians may recommend that the symptoms of fibrocystic breasts be treated with self-care. Depending on the individual situation, several measures may be recommended to relieve the symptoms of fibrocystic breasts. For instance, women may wish to wear extra support (athletic type) bras to help hold the breasts closer to the chest wall, which may provide some symptomatic relief. Extra support bras are especially important for large breasted women and may provide relief when breasts are full and tense with fluid. Physicians will often recommend that a support bra be worn both during the day and at night, especially during times of the woman’s menstrual cycle when the breasts are most tender. In addition, certain vitamins (particularly vitamin E, vitamin B6, or niacin) or herbal supplements such as evening primrose oil may help alleviate the symptoms of fibrocystic breasts by reducing inflammation and fluid retention. It is important that these supplements be used according to directions and that women avoid megadoses since serious side effects may occur from incorrect use. Some women also find that reducing their caffeine intake by avoiding coffee, tea, chocolate, and soft drinks decreases water retention and breast discomfort. However, this is a controversial topic among healthcare professionals because studies linking breast pain and caffeine have been inconsistent. In 1978, a study revealed that patients who took oral contraceptives were less likely to have fibrocystic breasts. The study has since been reconfirmed several times, though some health care professionals (and women) do not believe oral contraception has any significant effect on treating fibrocystic breasts. If fibrocystic breast pain is severe and interferes with a woman’s daily activities, further treatment may be necessary. Diuretics, substances that encourage the excretion of excess fluid from the body in the form of urine (which may in turn reduce tissue swelling and pain) are usually reserved for women who experience non-cyclical breast pain, but may be used to alleviate the symptoms of fibrocystic breast condition in some cases. The release of fluid in the body can help decrease breast pain and swelling. Additional drug treatments for severe breast pain include: bromocriptine (brand name, Parlodel) danazol (brand name, Danocrine) Bromocriptine and danazol both relieve cyclical breast pain by blocking estrogen and progesterone. However, these drugs may cause serious side effects in some women. Bromocriptine is poorly tolerated by many patients; side effects include nausea, dizziness, and fertility problems. Side effects of danazol may include weight gain, amenorrhea (absence of menstruation), and masculinization (such as extra facial hair) when given high doses. Other drugs, such as tamoxifen (brand name, Nolvadex) or goserelin (brand name, Zoladex) have been shown to have some effect on cyclical breast pain; however, these drugs are currently only approved for use in the United Kingdom for treating severe fibrocystic breast pain. Treatment of Fibrocystic Breasts May Include: Wearing extra support bras Avoiding caffeine (controversial recommendation) Taking oral contraceptives (controversial recommendation) Taking over-the-counter medications such as aspirin, acetaminophen or Motrin Maintaining a low fat diet rich in fruits, vegetables, and grains Applying heat to the breasts Reducing salt intake Taking diuretics Taking vitamin E, vitamin B6, niacin, or other vitamins Taking prescription drugs such as bromocriptine or danazol Surgically removing breast lumps
Fibrocystic Breast Condition cont.
Most fibrocystic breast lumps are found in the upper, outer quadrant of the breasts (near the axilla, armpit, region), although these lumps can occur anywhere in the breasts
Fibrocystic breast lumps tend to be smooth, rounded, and mobile (not attached to other breast tissue), though some fibrocystic tissue may have a thickened, irregular feel
Fibrocystic lumps or irregularities are often tender to touch and may increase or decrease in size during the menstrual cycle
Fibrocystic Breast Condition Symptoms of fibrocystic breasts include: cysts , fibrosis, lumpiness, areas of
thickening, tenderness, and pain Fibrocystic breasts are not risk factors for
breast cancer, but it can make breast cancer more difficult to detect
Screening mammograms may be more difficult to perform because the breast density associated with fibrocystic breasts may eclipse breast cancer on the mammogram
Additional imaging, biopsy, cyst aspiration may be needed
Presenter
Presentation Notes
The degree to which women experience these symptoms varies significantly. Some women with fibrocystic breasts only experience mild breast pain and may not be able to feel any breast lumps when performing breast self-exams. Other women with fibrocystic breasts may experience more severe breast pain or tenderness and may feel multiple lumps in their breasts. Most fibrocystic breast lumps are found in the upper, outer quadrant of the breasts (near the axilla, armpit, region), although these lumps can occur anywhere in the breasts. Fibrocystic breast lumps tend to be smooth, rounded, and mobile (not attached to other breast tissue), though some fibrocystic tissue may have a thickened, irregular feel. The lumps or irregularities associated with fibrocystic breasts are often tender to touch and may increase or decrease in size during the menstrual cycle. What is Fibrocystic Breast Disease? In the past, many physicians have referred to fibrocystic breasts, or lumpy breasts, as "fibrocystic breast disease." This term is misleading because fibrocystic breast condition is not a disease at all. Rather, it is a common, non-cancerous breast condition that affects over half of all women at some point in their lives. Today, most physicians refer to this condition as "fibrocystic breast condition" or "fibrocystic breast change." Other terms that may be used to describe the condition include "cystic disease," "chronic cystic mastitis," or "mammary dysplasia." In fact, since fibrocystic breasts are so common among women during their reproductive years, some physicians do not even like to label the symptoms as a "condition." They believe that these women simply have lumpier and more tender breasts than others. What Causes Fibrocystic Breasts? How Are Fibrocystic Breasts Diagnosed? Fibrocystic breasts are often first noticed by the woman, and further investigated by her physician. Breast tenderness, pain, and/or lumpiness are common indicators of fibrocystic breasts, especially when they coincide with menstruation. Often, fibrocystic breasts will be diagnosed with a physician-performed clinical breast exam alone. While having fibrocystic breasts is usually not a risk factor for breast cancer, the condition can sometimes make breast cancer more difficult to detect. Therefore, in some cases, breast imaging exams, such as mammography or ultrasound, will need to be performed on women who show symptoms of fibrocystic breasts. However, screening mammography may be more difficult to perform on women with fibrocystic breasts because the breast density associated with fibrocystic breasts may eclipse breast cancer on the mammogram film. In some cases, additional mammography or ultrasound imaging, followed by fine needle aspiration or biopsy, will be performed on women with fibrocystic breasts to determine whether breast cancer is present. Fine needle aspiration (to drain large, painful cysts) may also be performed by a physician help relieve some of the more severe symptoms of fibrocystic breast condition. How Are Fibrocystic Breasts Treated? Often, physicians may recommend that the symptoms of fibrocystic breasts be treated with self-care. Depending on the individual situation, several measures may be recommended to relieve the symptoms of fibrocystic breasts. For instance, women may wish to wear extra support (athletic type) bras to help hold the breasts closer to the chest wall, which may provide some symptomatic relief. Extra support bras are especially important for large breasted women and may provide relief when breasts are full and tense with fluid. Physicians will often recommend that a support bra be worn both during the day and at night, especially during times of the woman’s menstrual cycle when the breasts are most tender. In addition, certain vitamins (particularly vitamin E, vitamin B6, or niacin) or herbal supplements such as evening primrose oil may help alleviate the symptoms of fibrocystic breasts by reducing inflammation and fluid retention. It is important that these supplements be used according to directions and that women avoid megadoses since serious side effects may occur from incorrect use. Some women also find that reducing their caffeine intake by avoiding coffee, tea, chocolate, and soft drinks decreases water retention and breast discomfort. However, this is a controversial topic among healthcare professionals because studies linking breast pain and caffeine have been inconsistent. In 1978, a study revealed that patients who took oral contraceptives were less likely to have fibrocystic breasts. The study has since been reconfirmed several times, though some health care professionals (and women) do not believe oral contraception has any significant effect on treating fibrocystic breasts. If fibrocystic breast pain is severe and interferes with a woman’s daily activities, further treatment may be necessary. Diuretics, substances that encourage the excretion of excess fluid from the body in the form of urine (which may in turn reduce tissue swelling and pain) are usually reserved for women who experience non-cyclical breast pain, but may be used to alleviate the symptoms of fibrocystic breast condition in some cases. The release of fluid in the body can help decrease breast pain and swelling. Additional drug treatments for severe breast pain include: bromocriptine (brand name, Parlodel) danazol (brand name, Danocrine) Bromocriptine and danazol both relieve cyclical breast pain by blocking estrogen and progesterone. However, these drugs may cause serious side effects in some women. Bromocriptine is poorly tolerated by many patients; side effects include nausea, dizziness, and fertility problems. Side effects of danazol may include weight gain, amenorrhea (absence of menstruation), and masculinization (such as extra facial hair) when given high doses. Other drugs, such as tamoxifen (brand name, Nolvadex) or goserelin (brand name, Zoladex) have been shown to have some effect on cyclical breast pain; however, these drugs are currently only approved for use in the United Kingdom for treating severe fibrocystic breast pain. Treatment of Fibrocystic Breasts May Include: Wearing extra support bras Avoiding caffeine (controversial recommendation) Taking oral contraceptives (controversial recommendation) Taking over-the-counter medications such as aspirin, acetaminophen or Motrin Maintaining a low fat diet rich in fruits, vegetables, and grains Applying heat to the breasts Reducing salt intake Taking diuretics Taking vitamin E, vitamin B6, niacin, or other vitamins Taking prescription drugs such as bromocriptine or danazol Surgically removing breast lumps
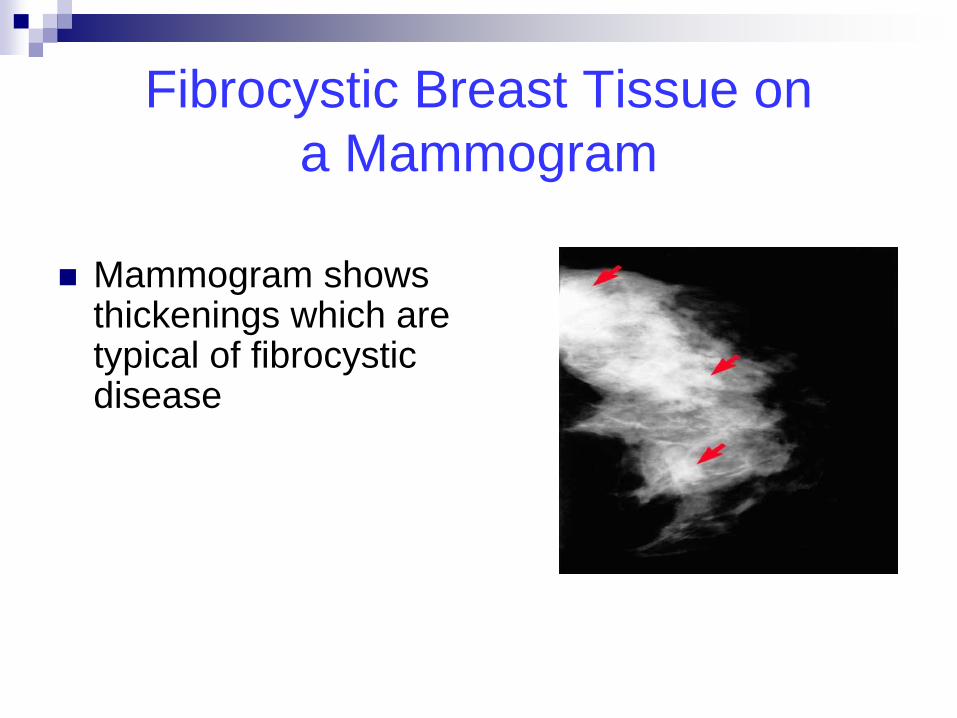
Fibrocystic Breast Tissue on a Mammogram
Mammogram shows
thickenings which are typical of fibrocystic disease
Breast Pain: Is a referral needed? Ask the client the following questions: Unilateral vs. bilateral? Cyclic vs non-cyclic? Constant vs. intermittent? Persists daily for more than a couple of weeks Localized to one specific area of breast (not
related to injury) Getting worse over time Interferes with daily activities If Breast Pain meets above criteria - refer for
breast consult
Follow-up of Breast Pain unrelated to cancer dx
Inform the woman that mastalgia is very common
Interventions to use: substituting a more supportive bra, lowering/changing estrogen dose, decreasing caffeine intake, ? Drug intervention I.e. evening primrose oil, danazol, bromocriptine, vitamin therapy I.e. Vitamin E (800u), Vitamin B6 or niacin
Cyclic pain is more responsive than non-cyclic pain
Presenter
Presentation Notes
Women with persistent mastalgia should have three- to six-month follow-up exams. Once breast cancer has been ruled out, it is important to communicate to the woman that mastalgia is very common. Occasionally, substituting a more supportive brassiere, lowering the dose of estrogen, or substituting a different form of estrogen can be helpful. In women unrelieved by these measures, drug intervention (i.e., evening primrose oil, danazol, or bromocriptine) can be useful. Cyclic pain is more responsive than non-cyclic pain.
Finding has < 2% risk of malignancy; not expected to change over f/u interval but radiologist wants to establish its stability
3 findings classified as probably benign: -- non-calcified mass -- focal asymmetry -- cluster of round calcifications Majority of findings can be managed through
initial STF (6 mos) up to 2 years (monitor closely as f/u often coincides with annual screening
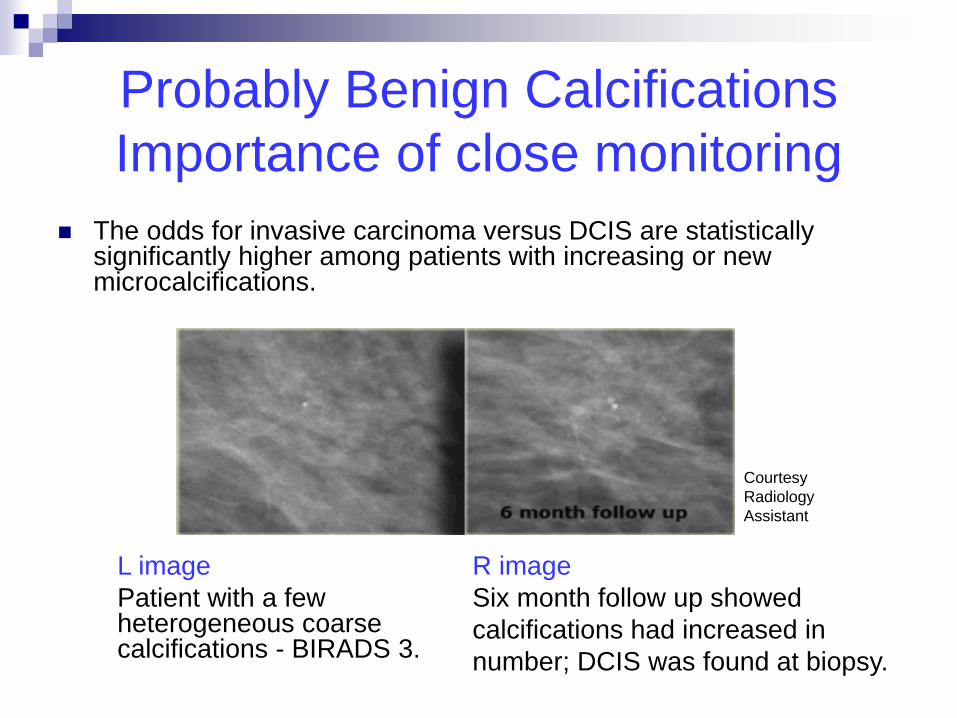
Probably Benign Calcifications Importance of close monitoring
The odds for invasive carcinoma versus DCIS are statistically significantly higher among patients with increasing or new microcalcifications.
L image Patient with a few
heterogeneous coarse calcifications - BIRADS 3.
R image Six month follow up showed calcifications had increased in number; DCIS was found at biopsy.
Courtesy Radiology Assistant
Mammogram Result: ACR 0: Assessment Incomplete-
Need Additional Imaging Evaluation
Additional imaging evaluation may include: spot compression, magnification, special magnification views, and/or ultrasound
Further follow-up beyond second imaging depends on final mammogram results
Mammogram Result: ACR 4: Suspicious Abnormality
Reserved for findings that do not have classic appearance of malignancy but have a wide probability of malignancy > than ACR 3 findings
Follow-up recommended based on
appearance/characteristics of findings Surgeon may choose to monitor as short-
term follow-up
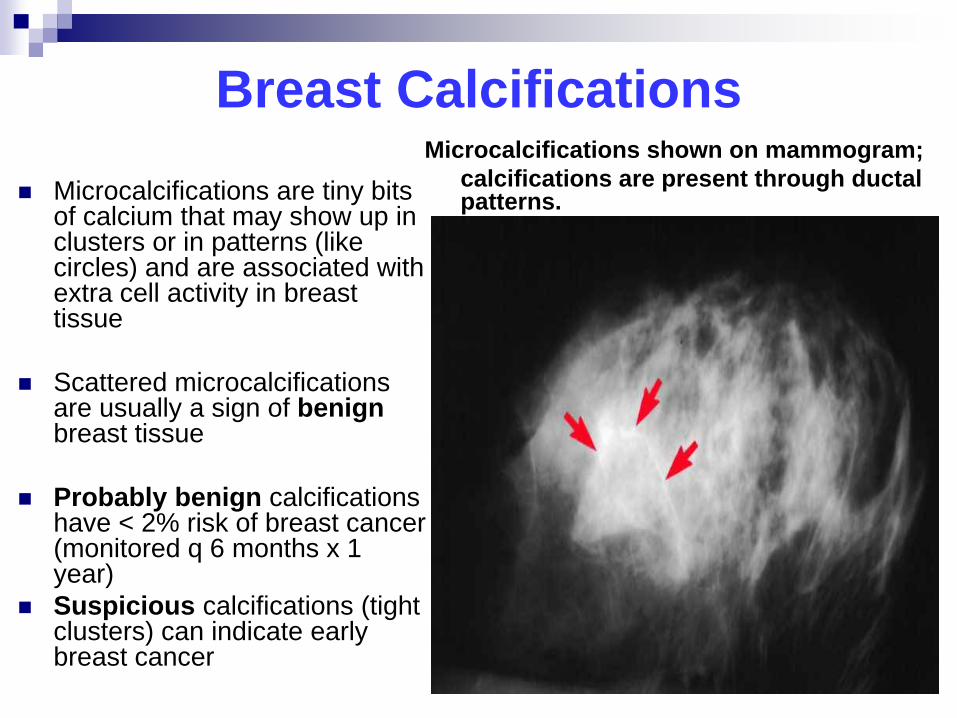
Breast Calcifications
Microcalcifications are tiny bits of calcium that may show up in clusters or in patterns (like circles) and are associated with extra cell activity in breast tissue
Scattered microcalcifications
are usually a sign of benign breast tissue
Probably benign calcifications
have < 2% risk of breast cancer (monitored q 6 months x 1 year)
Suspicious calcifications (tight clusters) can indicate early breast cancer
Microcalcifications shown on mammogram; calcifications are present through ductal
patterns.
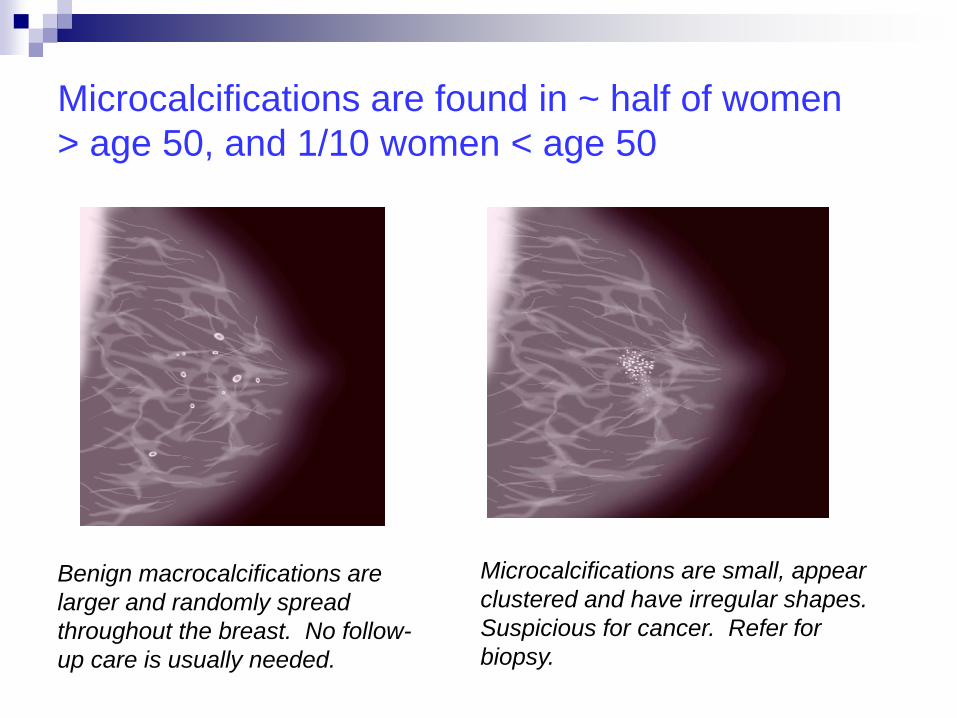
Microcalcifications are found in ~ half of women > age 50, and 1/10 women < age 50
Benign macrocalcifications are larger and randomly spread throughout the breast. No follow-up care is usually needed.
Microcalcifications are small, appear clustered and have irregular shapes. Suspicious for cancer. Refer for biopsy.
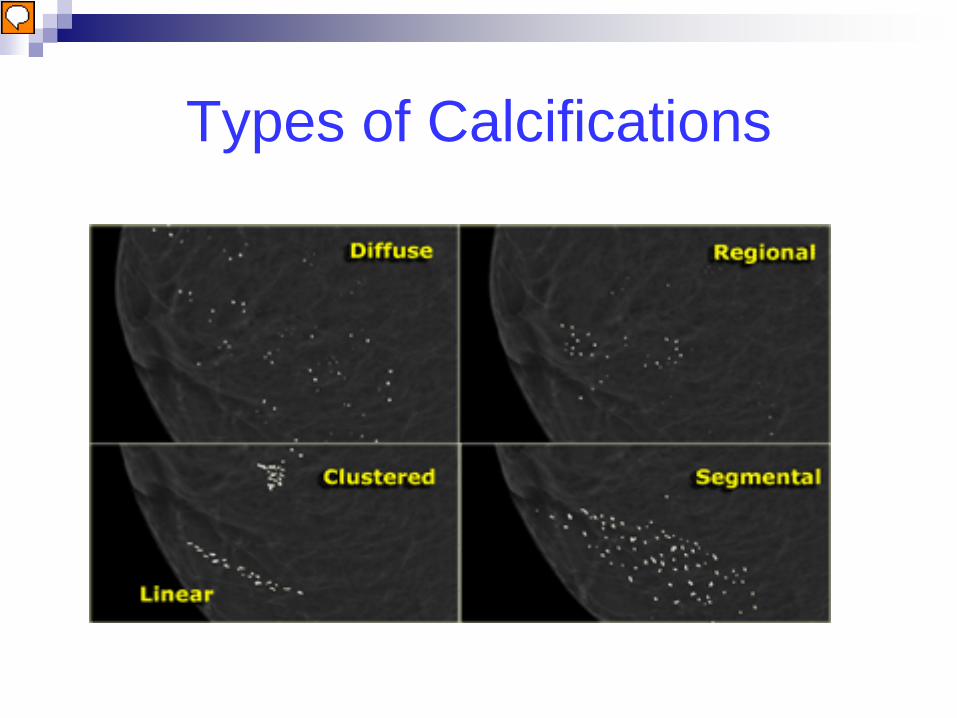
Types of Calcifications
Presenter
Presentation Notes
Radiology assistant Distribution In the BI-RADS atlas the following descriptions are given for the distribution of calcifications (1) : Diffuse or Scattered: diffuse calcifications may be scattered calcifications or multiple similar appearing clusters of calcifications throughout the whole breast. Regional: scattered in a larger volume (> 2 cc) of breast tissue and not in the expected ductal distribution. Clustered : at least 5 calcifications occupy a small volume of tissue (< 1 cc). Linear: calcifications arrayed in a line, which suggests deposits in a duct. Segmental: calcium deposits in ducts and branches of a segment or lobe.
Mammogram Abnormality
ACR 5: Highly Suggestive of Malignancy High probability (> 95%) of being cancer Type of biopsy performed depends on
lesion identified More than one biopsy may be performed
and/or combined with sentinel node imaging or delayed after neoadjuvant chemotherapy
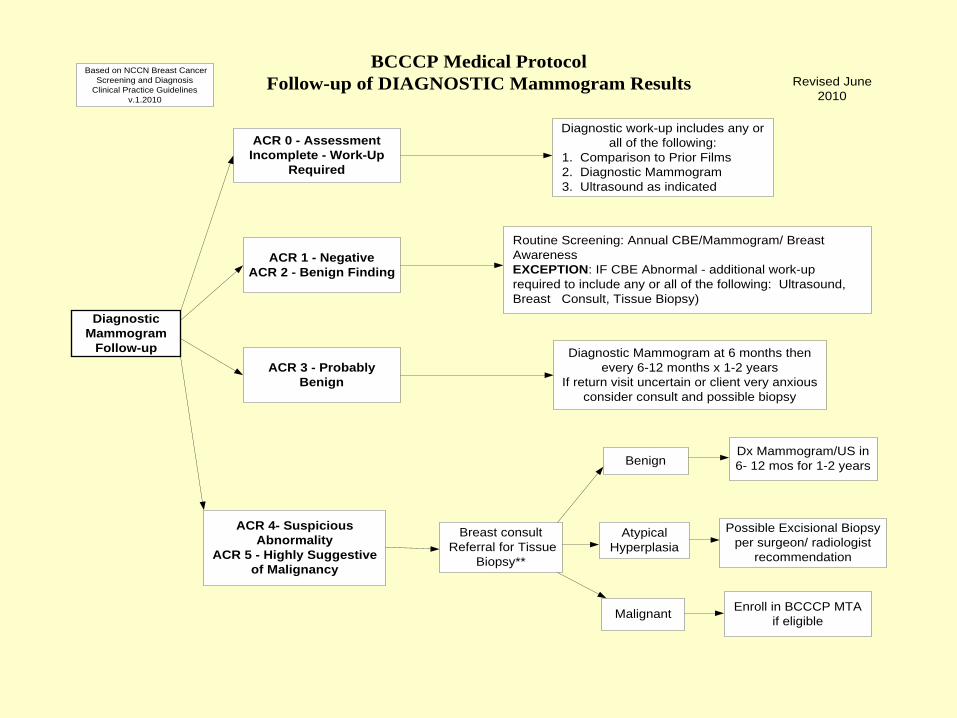
DiagnosticMammogram
Follow-up
Enroll in BCCCP MTAif eligible
ACR 0 - AssessmentIncomplete - Work-Up
Required
Routine Screening: Annual CBE/Mammogram/ Breast Awareness EXCEPTION: IF CBE Abnormal - additional work-up required to include any or all of the following: Ultrasound, Breast Consult, Tissue Biopsy)
ACR 3 - ProbablyBenign
ACR 4- SuspiciousAbnormality
ACR 5 - Highly Suggestiveof Malignancy
Diagnostic work-up includes any orall of the following:
1. Comparison to Prior Films 2. Diagnostic Mammogram 3. Ultrasound as indicated
ACR 1 - NegativeACR 2 - Benign Finding
Diagnostic Mammogram at 6 months thenevery 6-12 months x 1-2 years
If return visit uncertain or client very anxiousconsider consult and possible biopsy
Breast consult Referral for Tissue
Biopsy**
Benign
AtypicalHyperplasia
Possible Excisional Biopsyper surgeon/ radiologist
recommendation
Malignant
Dx Mammogram/US in6- 12 mos for 1-2 years
BCCCP Medical ProtocolFollow-up of DIAGNOSTIC Mammogram Results
Based on NCCN Breast CancerScreening and Diagnosis
Clinical Practice Guidelinesv.1.2010
Revised June2010
Case Study # 1
CBE Result: Probably Benign Screening Mammogram Result – ACR 0 Diagnostic Mammogram Result – ACR 0 Ultrasound confirms complex cyst. Next steps?
Presenter
Presentation Notes
Surgical consult
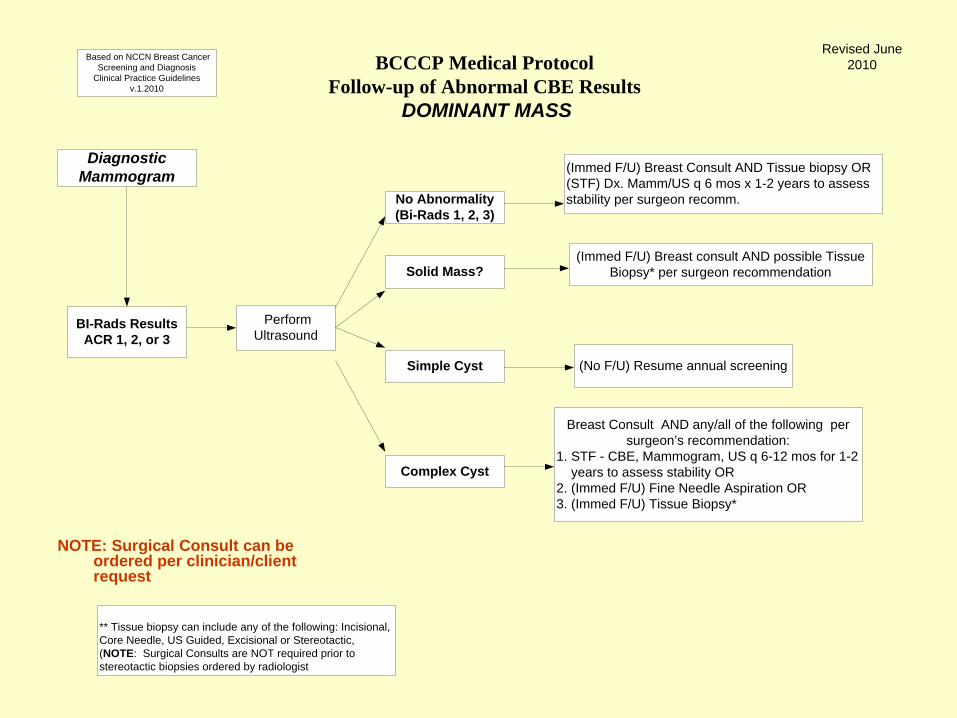
BCCCP Medical ProtocolFollow-up of Abnormal CBE Results
DOMINANT MASS
Diagnostic Mammogram
BI-Rads ResultsACR 1, 2, or 3
Perform Ultrasound
No Abnormality (Bi-Rads 1, 2, 3)
(Immed F/U) Breast Consult AND Tissue biopsy OR (STF) Dx. Mamm/US q 6 mos x 1-2 years to assess stability per surgeon recomm.
Solid Mass?
Simple Cyst
(Immed F/U) Breast consult AND possible Tissue Biopsy* per surgeon recommendation
Breast Consult AND any/all of the following per surgeon’s recommendation:
1. STF - CBE, Mammogram, US q 6-12 mos for 1-2 years to assess stability OR2. (Immed F/U) Fine Needle Aspiration OR3. (Immed F/U) Tissue Biopsy*
Complex Cyst
(No F/U) Resume annual screening
** Tissue biopsy can include any of the following: Incisional, Core Needle, US Guided, Excisional or Stereotactic, (NOTE: Surgical Consults are NOT required prior to stereotactic biopsies ordered by radiologist
Based on NCCN Breast Cancer Screening and Diagnosis
Clinical Practice Guidelines v.1.2010
Revised June 2010
NOTE: Surgical Consult can be ordered per clinician/client request
Case Study # 2 CBE – not performed Mammogram performed at Screening Fair;
Result: ACR 0 Referred to BCCCP Diagnostic Mammogram Result: - L breast – ACR 2 - simple or complicated
cysts without suspicious masses - R breast ACR 4 - solid nodule 10 o clock
appears suspicious Next Steps
Presenter
Presentation Notes
OK
BCCCP Medical ProtocolFollow-up of Abnormal CBE Results
DOMINANT MASS
Diagnostic Mammogram
Bi-Rads ResultsACR 4 or 5
Breast Consult AND Tissue Biopsy*
BenignDx Mammogram/US in 6- 12 mos
for 1-2 years
Biopsy ResultAtypical
Hyperplasia
Malignant
Possible Excisional Biopsy per surgeon/radiologist
recommendation
Enroll in BCCCP MTA if eligible
** Tissue biopsy can include any of the following: Incisional, Core Needle, US Guided, Excisional or Stereotactic, (NOTE: Surgical Consults are NOT required prior to stereotactic biopsies ordered by radiologist
Based on NCCN Breast Cancer Screening and Diagnosis