Embed Size (px)
Citation preview

FOCUS ON
THE AUSTRIAN
W UND
ASSOCIATION
Volume 12Number 1January 2012
Published byEuropeanWound ManagementAssociation

EWMA Council
The EWMA JournalISSN number: 1609-2759
Volume 12, No 1, January, 2012
Electronic Supplement January 2012www.ewma.org
The Journal of the EuropeanWound Management Association
Published three times a year
Editorial BoardSue Bale, UK, Editor
Jan Apelqvist, SwedenMartin Koschnick, Germany
Zena Moore, IrelandMarco Romanelli, Italy
Rytis Rimdeika, LithuaniaJosé Verdú Soriano, Spain
Rita Gaspar Videira, Portugal Salla Seppänen, Finland
EWMA web sitewww.ewma.org
Editorial Officeplease contact:
EWMA SecretariatNordre fasanvej 113
2000 Frederiksberg, Denmark.Tel: (+45) 7020 0305Fax: (+45) 7020 0315
Layout:Birgitte Clematide
Printed by:CS Grafisk A/S, Denmark
Copies printed: 11,000
Prices:The EWMA Journal is distributed
in hard copies to members as part of their EWMA membership.
EWMA also shares the vision of an “open access” philosophy,
which means that the journal is freely available online.
Individual subscription per issue: 7.50€
Libraries and institutions per issue: 25€
The next issue will be published in May 2012. Prospective material for
publication must be with the editors as soon as possible and no later
than March 1st 2012.
The contents of articles and letters inEWMA Journal do not necessarily reflect
the opinions of the Editors or the European Wound Management Association.
All scientific articles are peer reviewed by EWMA Scientific Review Panel.
Copyright of all published materialand illustrations is the property of
the European Wound ManagementAssociation. However, provided prior
written consent for their reproduction, including parallel publishing
(e.g. via repository), obtained from EWMA via the Editorial Board of the Journal,
and proper acknowledgement and printed, such permission will normally
be readily granted. Requests to reproduce material should state
where material is to be published, and, if it is abstracted, summarised,
or abbreviated, then the proposed new text should be sent to the
EWMA Journal Editor for final approval.
All issues of EWMA Journal are CINAHL listed.
CO-OPERATING ORGANISATIONS’ BOARD
Christian Thyse, AFISCeP.be
Tommaso Bianchi, AISLeC
Roberto Cassino, AIUC
Aníbal Justiniano, APTFeridas
Gerald Zöch, AWA
Jan Vandeputte, BEFEWO
Vladislav Hristov, BWA
Els Jonckheere, CNC
Milada Francu, CSLR
Dubravko Huljev, CWA
Martin Koschnick, DGfW
Bo Jørgensen, DSFS
Anna Hjerppe, FWCS
Pedro Pacheco, GAIF
J. Javier Soldevilla, GNEAUPP
Christian Münter, ICW
Aleksandra Kuspelo, LBAA
Susan Knight, LUF
Kestutis Maslauskas, LWMA
Corinne Ward, MASC
Hunyadi János, MSKT
Suzana Nikolovska, MWMA
Alison Johnstone, NATVNS
Kristin Bergersen, NIFS
Louk van Doorn, NOVW
Arkadiusz Jawien, PWMA
Severin Läuchli, SAfW (DE)
Hubert Vuagnat, SAfW (FR)
Goran D. Lazovic, SAWMA
Mária Hok, SEBINKO
Sylvie Meaume, SFFPC
Christina Lindholm, SSIS
Jozefa Košková, SSOOR
Leonid Rubanov, STW (Belarus)
Guðbjörg Pálsdóttir, SUMS
Javorca Delic, SWHS
Magnus Löndahl, SWHS
Andrea Nelson, TVS
Jasmina Begic-Rahic, URuBiH
Borys Datsenko, UWTO
Barbara E. den Boogert-Ruimschotel, V&VN
Georgina Gethin, WMAI
Skender Zatriqi, WMAK
Nada Kecelj Leskovec, WMAS
Bülent Erdogan, WMAT
Paulo Jorge Pereira Alves, Portugal
Caroline Amery, UK
Michelle Briggs, UK
Stephen Britland, UK
Mark Collier, UK
Rose Cooper, UK
B. E. den Boogert-Ruimschotel, Netherlands
Javorka Delic, Serbia
Corrado Maria Durante, Italy
Bulent Erdogan, Turkey
Madeleine Flanagan, UK Milada Francu, Czech Republic
Peter Franks, UK
Francisco P. García-Fernández, Spain
Luc Gryson, Belgium
Marcus Gürgen, Norway
Eskild W. Henneberg, Denmark
Alison Hopkins, UK
Gabriela Hösl, Austria
Dubravko Huljev, Croatia
Gerrolt Jukema, Netherlands
Nada Kecelj, Slovenia
Klaus Kirketerp-Møller, Denmark
Karsten Knobloch, Germany
Zoltán Kökény, Hungary
Severin Läuchli, Schwitzerland
Maarten J. Lubbers, Netherlands
Sylvie Maume, France
EWMA JOURNAL SCIENTIFIC REVIEW PANEL
Patricia PriceSecretary
Gerrolt JukemaRecorder
Jan ApelqvistPresident
Zena MooreImmediate Past President
Corrado M. DuranteTreasurer
Mark CollierBarbara E. den Boogert-Ruimschotel
Paulo Alves Javorka Delic
Robert StrohalRytis RimdeikaElia Ricci Salla Seppänen José Verdú Soriano
Dubravko Huljev Martin KoschnickLuc Gryson Sebastian ProbstNada Kecelj-LeskovecEskild Winther Henneberg
Christian Münter, Germany
Andrea Nelson, UK
Pedro L. Pancorbo-Hidalgo, Spain Hugo Partsch, Austria
Patricia Price, UK
Sebastian Probst, Schwitzerland
Rytis Rimdeika, Lithuania
Zbigniew Rybak, Poland
Salla Seppänen, Finland
Robert Strohal, Austria
Carolyn Wyndham-White, Switzerland
Gerald Zöch, Austria
Sue BaleSecretary
2

Volume 12Number 1January 2012Published byEuropean
Wound ManagementAssociation
FOCUS ONTHE AUSTRIAN W UND ASSOCIATION
ELECTRONIC SUPPLEMENT
ELECTRONIC SUPPLEMENT January 2012
WWW.EWMA.ORG
The January edition of the EWMA Journal Electronic Supplement includes articles with news from EWMA Cooperating Organisations. All organisations have been invited to contribute with information about their organisation, its recent activities, research projects and meetings, as well as their political and scientific involve-ment in wound care on a national level. ContentsItalian Nurses’ Cutaneous Wounds Association AISLeC Italian Association for the Study of Cutaneous Ulcers AUIC Croatian Wound Association CWA Lithuanian Wound Management Association LWMA The Hungarian Wound-management Association MSKT The National Association of Tissue Viability Nurses, Scotland NATVNS Swiss Association for Wound Care SAfW Tissue Viability Society TVS Association for Wound Management of Bosnia and Herzegovina URuBiHWound Management Association of Ireland WMAI Wound Management Association of Turkey WMAT
Science, Practice and Education
Organisations
EBWM
EWMA
5 EditorialJan Apelqvist
7 How to rate the wound debridement trauma? Jan Stryja
14 Ensuring equitable wound management education within the Australian contextJan Rice
18 Low wound prevalence and cost burden: The impact of a multidisciplinary wound specialist teamAlison Hopkins, Fran Worboys, John Posnett
18 The results of a comprehensive wound audit in a UK primary care trustAlison Hopkins, Fran Worboys
21 Pressure ulcer programme of research – PURPOSE Nixon J, Wilson L.M, Coleman S, Gorecki C, Muir D, Pinkney L, Keen J, Briggs M, McGinnis E, Stubbs N, Dealey C, Nelson A
27 The skin’s own bacteria may aggravate inflammatory and occlusive changes in atherosclerotic arteries of lower limbsWaldemar L. Olszewski, Piotr Andziak, M. Moscicka-Wesolowska,Bozenna Interewicz, Ewa Swoboda, Ewa Stelmach
33 Problem with the post burn wound pain: Chronic profilesLaima Juozapaviciene, Rytis Rimdeika, Aurika Karbonskiene
40 Abstracts of recent Cochrane reviewsSally Bell-Syer
42 EWMA Journal Previous Issues and other Journals
44 The Austrian Wound Association AWAArja Riegler, Franz Trautinger
46 The Amputation Register Project by the Austrian Society of Surgery and the Austrian Wound AssociationGerald Zöch
48 Diabetic Foot Activities in AustriaJan Apelqvist, Thomas Pieber, Gerald Zöch
50 Wound care in Russia and Neighbouring Countries: Symposium at EWMA 2012 and other activitiesRytis Rimdeika, Robert Strohal
51 Meeting with MEP Vittorio Prodi
52 Pisa International Diabetic Foot Course 2011Alberto Piaggesi
54-56 Book ReviewSue Bale, Salla Seppänen
58 The EWMA Master Course 2011Zena Moore
60 Conference Report: Leg Ulcer & Compression SeminarsFinn Gottrup, Hugo Partsch
62 EWMA Corporate Sponsors
63 EWMA Activities Update
64 Conference Calendar
66 The 14th EPUAP Annual Meeting in Porto PortugalMichael Clark
68 SAfW – 13th Symposium on Modern Wound TherapySeverin Läuchli, Jürg Hafner
70 Overview on WAWLC activities during 2011David Keast
72 WMAI – Building the Future of Wound Care 15th Anniversary ConferenceGeorgina Gethin
74 Cooperating Organisations
75 International Partner Organisations
75 Associated Organisations 3

Wound Management T +44 (0) 1482 225181 www.smith-nephew.com/woundSmith & Nephew F +44 (0) 1482 328326Medical Ltd ™Trademark of Smith & Nephew101 Hessle Road © Smith & Nephew August 2011Hull HU3 2BN 30626UK
If society fails to meet its growing healthcare costs, future generations will pick up the bill. We cannot let that happen.For patients. For budgets. For today.™

Editorial
I would like to begin this editorial by wishing you all a peaceful and successful 2012. 2012 will be my first full year as the president of
EWMA. In this position I succeed the previous president of EWMA, Zena Moore. I would like to take this opportunity to thank Zena Moore for all her hard work and great efforts to define and develop EWMA during her presidential period.
In previous years, EWMA has, amongst other things, focused on: n Further developing wound management
education in Europe by taking steps towards establishing a wound care teacher network and new educational initiatives.
n Raising awareness of the true burden of wounds to patients, and to EU Healthcare systems, in order to improve patient out-comes, by approaching the EU Parliament in collaboration with the Eucomed Advanced Wound Care Sector Group.
n Supporting the development of better evidence in wound care. The EWMA Patient Outcome is currently working on a set of study protocol templates, based on the rec-ommendations on use of outcome measures (published in 2010), offering guidelines for good wound care study practice.
n Increasing collaboration with other interna-tional societies involved in wound manage-ment or related areas.
My period as EWMA President will run from 2011 to 2013. During these years, I will support the continuation of all the valuable initiatives that have been started in the previous years. Additionally, during my presidency, my contribution to the continuous development of EWMA will include the following main objec-tives: n To develop, implement and advocate for the
use of multidisciplinary treatment guidelines, based on the existing evidence.
n To advocate for an holistic approach to treat-ment, in particular with regards to recognising the value of the patient as an active partner.
n To contribute to the recognition of health economics and organisation of care as a tool to improve management and care.
n To advocate for the recognition of the industry as an owner of valid information, experience and skills which give grounds for inviting wound care companies to act as potential partners in the efforts to improve management and care.
The multidisciplinary approach to wound man-agement is essential for successful wound manage-ment. Despite this, the understanding of the benefits of multidisciplinary wound management still needs to be fully understood and approved in many treatment settings around Europe. This lack of understanding may have a significant impact on the life of the patient, leading to problems, for example foot amputations, which could have been avoided.
Taking the financial crisis and increased ageing population into account, the focus on health economy is becoming an increasingly important part of all discussions about treatment structures. This underlines the need to focus on health economy in all wound care studies produced in the future, to provide the information needed for policy makers and administrators to understand the impact of wounds on the health care system.
To solve these challenges, we need all relevant partners to contribute and collaborate. This includes the wound care industry as well as patients and clinicians working within wound management all over Europe.
We are looking forward to an exiting 2012-2013. Currently we are racing to meet the many challenges facing the European and global health system. We are sure that EWMA will be successful in contributing to some of the solutions.
Jan Apelqvist, EWMA President
EWMA Journal 2012 vol 12 no 1 5

A chronic wound with EPA has a 90% probability it won’t heal1
28% of non healing wounds have EPA1
There are no visual cues to detect EPA2,3
References1. Serena T. et al. Protease activity levels associated with healing status of chronic wounds. Poster, Wounds UK 2011.2. Snyder R. et al. A survey: The importance of proteases in wound healing and wound assessment. Poster, Wounds UK 2011.3. International consensus. The role of proteases in wound diagnostics. An expert working group review. London: Wounds International, 2011.SYS/GBI/748
/1211
UNTIL NOWFor more information, contact us on [email protected]
or visit our website www.systagenix.com

Science, Practice and Education
Jan Stryja, M.D.
Centre of Vascular and Mini-invasive Surgery, Podlesi Hospital, Trinec, Czech Republic
Contact: [email protected]
Conflict of interest: none
Key words: debridement, hydrosurgery, sharp debridement, wound trauma
ABSTRACTBackground: The positive influence of debri-dement on wound healing has been described in a number of clinical studies. To remove the necrosis, foreign material, and the damaged tissues from the surface of the wound we can use different methods and techniques. Me-chanical debridement is fast and effective, but its usage is connected with many problems and disadvantages (damaging the underlying structures of the wound surface with a con-sequent deterioration of tissue nourishment, acute wound pain, bleeding etc.).Methods and materials: In our study, we monitored the extent of wound surface dam-age during the mechanical debridement on the model of a surgical wound. To remove the necrosis we used a scalpel, surgical scis-sors, electro-cautery and a water-jet hand-piece. Tested tissue samples were sent to the coroner’s office for histological analysis and assessment of the level of wound surface dam-age after debridement. To assess the degree of wound trauma we have created a special scoring system based on the presence of 6 microscopic markers on the tissue sample surface. This scoring system consists of three degrees of wound surface damage, indicating the range of tissue trauma. Results: We observed the smallest tissue trauma in a group treated with the hydro-surgery debridement technique. The gravest tissue trauma signs were in a group debrided with scissors. These results were validated by statistical analysis. Conclusion: Our study demonstrates that the hydrosurgery debridement method is safer than other mechanical debridement methods.
INTRODUCTIONDebridement is an essential part of the acute and chronic wound healing process. Properly conducted debridement reduces bacterial and toxic bio-burden, reduces wound exudate and odour and speeds up the healing process. The positive influence of debridement on wound healing has been described in a number of clinical studies. Necrosis and tissue debris on the surface of the wound can mechanically interfere with the healing process. This devitalized tissue is also the source of odour and can increase the risk of bacte-rial colonization, critical colonization and the devel-opment of wound infection1. Necrosis slows down wound contraction, increases the inflammatory re-sponse of the organism as a result of inflammatory mediators and cytokine release. In 1996, Steed de-scribed the acceleration of the healing process after surgical debridement of the chronic wound in patients with diabetic foot syndrome in a comparative study2.
We can use different methods and techniques to remove the necrosis, foreign material and the damaged tissue from the surface of a wound. Optimal debride-ment is quick and simple; it effectively removes the damaged tissue, is cheap, considerate of the healthy tissue and the area around the wound. Mechanical debridement removes the affected tissue using surgical procedures and instruments. It is generally fast and easy to apply. Its disadvantage however is a higher risk of damaging the underlying structures of the wound surface (so called over-excision) with a consequent deterioration of tissue nourishment and a negative impact on the healing process. Sharp debridement may also be complicated by acute wound pain, bleed-ing from the wound surface and following haemostatic interventions with subsequent secondary damage of the wound bed.
Minimising trauma of the deeper structures on the surface of the wound provides the conditions for reducing the inflammatory phase and thus accelerates the healing of the wound itself. In contrast, extensive debridement trauma interferes with wound vitality by increasing the risk of tissue ischaemia on the wound. This often leads to a deepening of the necrosis. Previ-
How to rate the wound debridement trauma?
Presented at the EWMA 2010 Conference
Genva, Switzerland
EWMA Journal 2012 vol 12 no 1 7

ously published experimental studies (Tenenhaus, 2007) indicate that treatment of the wound by hydrosurgery debridement is considerate and helpful3,4,5,6.
Aim of the study: A study comparing the effect of 4 dif-ferent types of debridement on the tissue has not been published yet. This study measured the histological qual-ity of the tissue samples‘ resection areas while conducting different debridement techniques. The aim of this experi-ment was to assess the degree of soft tissue trauma using 4 different methods of mechanical debridement and to de-scribe their impact using soft tissue microscopic imagery.
MATERIALS AND METHODSStatistical power analysis for a four groups study was per-formed in advance to determine the minimal number or samples needed (Power and Sample Size Programme, t-test). We took into consideration: a=0.008, b=0.80, SD=1.0, accounting for the score difference of 1 point. To prove the statistically significant difference of 1 point it was necessary to have 26 sections in each group of the study. We fulfilled this requirement very well (n=32).
Methodology: The experiment was designed as a pro-spective, blinded, comparative study. We biopsied 64 and investigated 128 tissue sample slices taken from 16 patients indicated for necrectomy (hospitalized in the surgical de-partment, Podlesí Hospital, Trinec). All these patients were treated for peripheral artery disease with a mani-festation of chronic critical limb ischaemia. The inclu-sion criterion for monitoring the patient was presence of a lower limb ulcer indicated for necrectomy. Debriding the surface and edges of the wound was carried out “lege artis” as a planned operation in the operating-theatre using the appropriate anaesthetic. The tissue samples were divided into 4 groups (n=32) and then debrided by scalpel, surgi-cal scissors, electro-cautery and hydrosurgery handpiece.
Methods: Each tissue sample was a section consisting of skin and subcutaneous tissue, approximately 1 cubic cm, harvested from the edge of the debrided wound. Then the sections were removed and marked:n Tissue sample “S” – surgical debridement by scalpel
(32 sections in total) n Tissue sample “V” – using the Versajet hydrosurgery
device (water-jet intensity 6, 32 sections in total)n Tissue sample “E” – debridement carried out by the
electro-cautery cut (type ERBE ICC 300, wattage 150 W), (32 sections in total),
n Tissue sample “N” – surgical debridement carried out with scissors (32 sections in total).
Each tissue sample contained skin, subcutaneous tissue or deep fascia (depending to the local anatomical op-tions). We obtained a maximum of 8 samples within one procedure (and one patient). The specimens had been marked with stitches in the operating room to define their topographical location, then preserved in a fixing solu-tion (formalin), and sent to the biopsy lab in the Nový Jiˇín Hospital. Pathologist Dr. Ivan Ferák prepared and subsequently evaluated all specimens here. Two different histological slices from the resection areas (marked with India ink) were made from each tissue sample (from dif-ferent parts of the tested wound). In every group (S, V, E, N) we had 16 processed tissue preparations and 32 edge-oriented sections.
We used Tenenhaus’s clinical study from 20073 to find the basic information on how to evaluate the his-topathological results. Tenenhaus prospectively studied the versatility of the water-jet instrument for the treat-ment of deep face and neck burns. First he debrided tis-sue with this instrument and then measured the depth of debridement using micrometry via light microscopy (the thickness of the debrided tissue was determined). Deb-ridement performed with settings 7 and 8 removed the dermis to a thickness of 80 to 100 microns. The ex vivo results demonstrated that it is possible to precisely select and adjust the desired debridement depth (according to the tissue type).
We decided to create our own scoring system (TDD – tissue damage degree) for describing the histopathological changes and quantifying soft tissue bruising. The micro-scopic image was used to determine the score – grade I, II and III. The pathologist focused on 6 touchstones in the histological evaluation of the sections:1. degree of tissue damage (including injury depth)
(less than 0.5 mm, more than 0.5 mm),2. microscopically visible differences between the
margins of the tested wound (present/absent), 3. disintegrated or crushed tissue on the wound surface
(present/absent), 4. presence of secondary necrosis (consequence of
debridement procedure) (present/absent), 5. presence of haematomas at the test sample edge
(present/absent)6. disrupted blood vessels in the skin and subcutaneous
tissue (present/absent).
The presence of each of the pathological-anatomical phe-nomena mentioned above has been valued at 1 point. The microscopic structure evaluation was carried out “blindly”, the pathologist didn’t know what evaluation technique had been applied by the clinician. Examined tissue samples were rated from 1 to 6 points.
EWMA Journal 2012 vol 12 no 1 8

Science, Practice and Education
Histopathological processing: Two slices, coloured by default with hematoxylin and eosin, were prepared from each tissue sample at the Department of Pathology. The presence of the colonies of bacteria penetrating into the wound after debridement was evaluated by a pathologist using direct microscopy. Bacteria were detected on the sur-face of the wound in only 1 case. Statistically, this marker was not significant. As the most common tissue damage marker the pathologist recorded a soft tissue crushing (115 sections), microscopic margin differences (96 sections) and deep tissue damage (more than 0.5 mm) – (81 sections). He described 40 sections with haematomas at the sample edges; disrupted blood vessels were present in 29 sections. Secondary necrosis on the wound surface was present in 14 sections. Distribution of the observed markers frequency is shown in table No. 1 and graph No. 1.
The first wound trauma degree (straight edge without any cracks or other signs of bruising) is illustrated in fig. 1. This category contains samples with a total of 1 or 2 points. Slight differences between the wound margins and smaller fissures are typical features of the second wound trauma degree (see fig. 2.), the samples reached the score
sum of 3 and 4 points. Extensive tissue contusion, large cracks and disruptions are characteristics of the third wound trauma degree (see fig. 3 and 4). We included samples with a score of 5 and 6 points here. Our local Ethics Committee considered a proposal for this experi-ment and approved it.
RESULTSThe results of our study are shown in table No. 2 and graph No. 2. The most frequent tissue damage degree (TDD) in group “V” (hydro-surgery technique) was TDD I (22, i.e. 69%). In group “N” (debrided with scissors) we found TDD III to be the most frequent one (15, i.e. 47%) and in group “E” (treated with electro-cautery) it was TDD II (22, i.e. 69%). In group “S” (sharp debride-ment with scalpel) we have seen an equal incidence of the most frequent TDDs I and II (15 and 15, i.e. together 93%).
We carried out the statistical analysis (Statistica soft-ware, version 9) of the results using M-L Chi-square test.
TDD marker incidence
disintegrated or crushed tissue on the wound surface 115
microscopic inequality margin of the tested wound 96
degree of tissue damage (including injury depth) above 0.5 mm 81
presence of haematomas 40
disrupted blood vessels 29
presence of secondary necrosis 14
Table 1 and graph 1:Histo-pathological touchstones foud in the evaluation of all the sections:
Technique (p=0.00000) TDD I TDD II TDD III sum
V (water-jet) 22 8 2 n=32
N (scissors) 7 10 15 n=32
E (electro-cautery) 8 22 2 n=32
S (scalpel) 15 15 2 n=32
Table 2 and graph 2:Tissue damage degree (TDD) representation in each group of debridement
EWMA Journal 2012 vol 12 no 1 9

Science, Practice and Education
First, we analysed the distribution of TDD in the whole observation. We found a statistically significant difference between the TDD I, II and III (p = 0.0000) and also be-tween the group with minimal tissue damage (TDD I) and the rest of the cohort (p = 0,00023) and between the maxi-mum damage grade (TDD III) and the rest (0,00001), see table and graph 3a, 3b. Each group is unique and can be used to describe the properties of the whole group.
The best results (the lowest occurrence of trauma markers), are achieved with the water-jet hydrosurgery technique (69%) and scalpel debridement (47%). In con-trast, the greatest incidence of grade III trauma (the most severe signs of tissue trauma) were found in the group of tissue samples treated with scissors, method N (47%). A statistically significant difference in results was confirmed between the groups “V” and “N” (p=0.00005), “V” and “E” (P=0.00112), “N” and “S” (p=0.00049) and “N” and “E” (p=0.00035). Statistical analysis didn’t prove the sta-tistically significant difference in wound trauma between the group “E” versus “S” (p=0.17404) and “V” versus “S” (p=0.17404).
To establish a ranking of all the tested techniques we can calculate the average TDD (ATDD ) score, which takes into account not only the layout in each of the stages I-III, but also the significance of histopathological changes when assessing the impact of the relevant debri-dement technology on wound healing. According to this ATDD score, the best results (the least severe trauma) were achieved by group “V”, followed by groups “S” and “E”. The worst results (the heaviest histopathological changes on the surface due to wound trauma) were observed in group “N” (see table and graph No. 4).
DISCUSSIONWe observed 64 soft tissue specimens debrided with 4 different surgical techniques in our experimental study. When planning the study we decided to make 2 independ-ent histological sections from each tissue block to utilize the clinical material effectively. Thanks to this, we were able to increase the number of histological findings in
Figure 3: The third wound trauma degree (deep crack) Figure 4: The third wound trauma degree (disrupted tissue)
Figure 1: The first degree of tissue damage (straight edge without any cracks)
Figure 2: The second wound trauma degree (small fissure)
EWMA Journal 2012 vol 12 no 1 10

Technique (p=0.00023) TDD I TDD II + TDD III sum
V (water-jet) 22 10 n=32
N (scissors) 7 25 n=32
E (electro-cautery) 8 24 n=32
S (scalpel) 15 17 n=32
Technique (p=0.00001) TDD I + TDD II TDD III sum
V (water-jet) 30 2 n=32
N (scissors) 17 15 n=32
E (electro-cautery) 30 2 n=32
S (scalpel) 30 2 n=32
Table 3a and graph 3a:Minimal tissue damage (TDD I) versus medium and heavy tissue damage degrees (TDD II + TDD III) representation for each group of debridement
Table 3b and graph 3b:Heavy tissue damage (TDD III) versus medium and light tissue damage degrees (TDD I + TDD II) representation for each group of debridement
Technique TDD gr I score
TDD gr II score
TDD gr III score ATDD
n=32 coef = 1 coef = 2 coef= 3 /n
V (water-jet) 22 16 6 44 1,375
N (scissors) 7 20 45 72 2,25
E (electro-cautery) 8 44 6 58 1,813
S (scalpel) 15 30 6 51 1,594
Table 4 and graph 4:The average TDD score (ATDD)
each group. As all our patients had been given the same main diagnosis (peripheral artery disease) and we did not perform long-term observation, we decided not to con-nect the results of debridement to the patients’ datasets.
Tenenhaus et al., 20073 published a special scale for rating the results of the debridement depth using water-jet. They worked with macroscopic and microscopic features on debrided skin in patients with burns. For our work, we preferred the histological examination of the sections. There was a risk of erroneous subjective evaluation, but we defined 6 marks of trauma before and with this purpose we tested the histological image of all the slices. It could
be problematic to define the acute wound trauma on the microscopic level and strictly objective methods measuring the wound trauma are also rare. We tried to eliminate this source of mistakes by blinding the evaluation process of the microscopic views and by increasing the number of markers focused on. The original scoring scale was devel-oped for the final rating of wound trauma. It consists of only 3 stages because more stages would divide the tested samples into many smaller groups with problematic statis-tical evaluation. It made the final evaluation more simple.
The secondary necrosis on the wound surface after debridement could be connected with unsatisfactory de-
EWMA Journal 2012 vol 12 no 1 11

bridement or the application of electro-cautery. After de-bridement, we tried to leave the wound sample without macroscopically visible persisting necrosis. In the end, the total number of secondary necroses was low in monitored groups and it seemed to be expedient to define only three tissue damage degrees.
The statistical analysis proved our earlier clinical ex-perience, that scalpels allow for the more perfect incision resulting in quick and high-quality healing than scissors or electro-cautery. Water-jet debridement produced very similar results to the scalpel treatment. Both methods, hydrosurgery and electro-cautery, are dependent on set-ting the proper grade of output according to the type of tissue treated. It was done according to the manufacturer’s recommendations and our clinical practice. The technical conditions while debriding the wound were the same in all cases. The statistical analysis of ATDD was problematic but calculating the average value of tissue damage degree for each group approximately described the impact of deb-ridement on the wound and proved that scissors produced the least acceptable results. The assessment tool used in the study had a certain limitation caused by a possible subjec-tive evaluation mistake on the part of the pathologist. It is very difficult to find quantifiable features in evaluating the histological sections but the pathologists are well trained to cope with this. Our pathologist was an experienced doctor with clinical practice of more than 20 years.
To minimise the subjective point of view and personal influence we used sample blinding and the results were statistically analyzed.
CONCLUSIONSIn our opinion, we can consider the water-jet debridement to be safe and “mini-invasive”. It causes less trauma and produces better results at microscopic evaluation level than conventional surgical debridement techniques: scalpel, electro-cautery and scissors. m
AcknowledgementsI would like to acknowledge Prof. Dr. R. Staffa’s support in planning the study and Dr. I. Ferak’s help in the evaluation of microscopic sections.
References
1. Gray, D., White, R. J., Cooper, P. The wound healing continuum. British Journal of Community Nursing 7, 12, Supl 3: 15-19, 2002.
2. Steed DL, Donohoe D, Webster MW, Lindsley L. Effect of extensive debridement and treatment on the healing of diabetic foot ulcers. Diabetic Ulcer Study Group. J Am Coll Surg 1996;183:61-4.
3. Tenenhaus M., Bhavsar D, Rennekampff H. Treatment of deep partial thickness and indeterminate depth facial burn wounds with water-jet debridement and a biosynthetic dressing. Injury, Int. J. Care Injured (2007) 38S, S38-S44
4. Granick MS, Posnett J, Jacoby M, Noruthun S, Ganchi PA, Datiashvili RO. Efficiency and cost-effectiveness of a high powered parallel waterjet for wound debridement. Wound Repair Regen. 2006; 14: 394-397.
5. Mosti G, Iabichella ML, Picerni P, Magliaro A, Mattaliano V. The debridement of hard to heal leg ulcers by means of a new device based on Fluidjet technology. Int Wound J. 2005 Dec;2(4):307-14.
6. Tortella, B. J. Traumatic and Chronic Wound Debridement With A Novel Fluidjet Device: The VersaJet Hydrosurgery System. Wound Management, Smith and Nephew, 2004.
7. Webb, L. X., Smith, T. L., Morykwas, M. J. A Pilot Study of Two Techniques for Wound Debridement. Wound Management, Smith and Nephew, 2004.
Science, Practice and Education
Become a Member of EWMAMake a difference in clinical practice
Benefits of your EWMA Membership:n You make a difference in clinical practice within wound management in Europen Right to vote and stand for EWMA Counciln EWMA Journal send directly to you three times a yearn EWMA news and statements send directly to youn A discount on your registration fee for EWMA Conferencesn Right to apply for EWMA travel grantsn Yearly membership fee € 25n Yearly membership fee for members of cooperating organisations € 10
Please register as a EWMA member at WWW.EWMA.ORG
EWMA SecretariatNordre Fasanvej 113,2000 Frederiksberg,DenmarkTel: +45 7020 0305Fax: +45 7020 [email protected]
EWMA Journal 2012 vol 12 no 1 12

An all-in-one wound careportfolio doesnot exist
www.coloplast.com
The Coloplast logo is a registered trademark of Coloplast A/S. © 2011-12. All rights reserved Coloplast A/S, 3050 Humlebæk, Denmark.
Superior
absorption for
non-infected
wounds*
Superior
absorption for
infected
wounds
Superior
absorption for
painful
wounds
After 30 years in wound care, we at Coloplast
believe that absorption is the key to better healing.
Our Biatain portfolio offers a diverse range of
wound dressings that provide superior absorption
for faster healing of non-infected, infected and
painful wounds. Biatain – superior absorption for
faster healing.
Biatain® – the simple choice
Biatain
Silicone with
Barrier-Free
Foam™
Biatain
Silicone Ag
with Barrier-Free
Foam™
Biatain
Ibu**
Biatain® – superior absorption for faster healing
* Can also be used on infected and painful wounds, but be sure to address these conditions by other means.
** First, treat the underlying possible causes of pain, e.g. infection or uncontrolled oedema.

Jan Rice, RN,
Mast. Wound Care (Monash University),
FAWMA
Coordinator: Wound EducationWorld of Wounds
La Trobe University
Correspondance:[email protected]
Conflict of interest: none
ABSTRACTAim: Wound management education within the Australian context is ad hoc and varies in structure and content. This project aimed to develop a pro-gressive system of wound management education that could be accessed by all health professionals of varying skill levels taking them to a higher level as they became more proficient with new knowledge and skills.Method: An education programme comprising a variety of modes and durations was developed over the past three years. Participants were able to select from seminars, short courses, and Masters Award programmes. Education was provided by videoconferencing, facility-based sessions, web-based tutorials and institution-based workshops. Each education session was specifically designed to meet the needs of the broad spectrum of partici-pants, ranging from surgical registrars through to the Personal Care Attendants (PCAs). To ensure participants’ knowledge continued, the “Friends of WoW” programme was developed. “Friends” are able to seek clinical consultation, be involved in product evaluation and access specific education materials provided by the website. Results: Since its inception, 7800 participants have undertaken the education programme; nurs-es (70%), personal care attendants (20%), allied health (10%), government/corporate (5%), indig-enous health care workers (3%) and medical staff (2%). There has been a 33% growth in numbers each year with 22% of those undertaking the short programmes progressing through to the longer programmes. Currently, there are 505 Friends of WoW. Conclusions: The challenges of providing education to a variety of health care professionals within Aus-tralia require innovative educational programmes. The programmes developed by the LaTrobe Uni-versity World of Wounds have demonstrated an effective model for overcoming these challenges. Some participants have progressed through the vari-ous programmes to become key wound clinicians in metropolitan and rural/remote settings.
INTRODUCTIONThe Australian Wound Management Associa-tion (AWMA) began in 1993 with a meeting of interested participants drawn from all states and territories, in Perth Western Australia. The attendees to this meeting voted to establish the association with a view to acting as a source for dissemination of wound knowledge through a bi-annual conference hosted in a different state or territory each time. The establishment of the association is seen by many as the beginning of modern wound management concepts within Australia.
Those practicing as wound educators or wound nurse consultants would therefore see Australia as coming in a little late. Winter1 pub-lished his well known moist wound healing the-ory in 1962 and education about the theory and the new concepts was slow to begin. Since 1993 AWMA has held conferences in Perth, Sydney, Melbourne, Darwin, Adelaide, Hobart, Bris-bane and Canberra. Our European counterparts may think this is not something to highlight however the size of Australia is one barrier that needs to be overcome in order to work together as one nation on a common problem.
AUSTRALIAN STATISTICS2 n Land mass-7.7 million square kilometres
(sq km)n There are some 12,000 islandsn The land area of Australia is almost as
great as that of the United States of Amer-ica (excluding Alaska), about 50% greater than Europe (excluding the former USSR) and 32 times greater than the United Kingdom
n Australia is the lowest, flattest and, apart from Antarctica, the driest of the conti-nents
n The age of landforms in Australia is gener-ally measured in many millions of years
Ensuring equitable wound management education within the Australian context
Short paper EWMA 2011
Brussels · Belgium
EWMA Journal 2012 vol 12 no 1 14

n Total population 2010 – 22,328.80n Life expectancy for males – 79.2 years in 2008 and
79.3 years in 2009n Life expectancy for females – 83.7 years in 2008 and
83.9 years in 2009n 1.8% of total 2010 population were aged over
85yearsn Cancer, heart disease and disease of the respiratory
system were the leading cause of deaths in 2010
and practice of wound management4. Associate Professor Michael Woodward also found that some wound practices requested or performed by geriatricians were unconven-tional or lacked a sound knowledge basis5. With a strong suspicion and some publication-based research it was clear that wound education programmes were needed in order for Australia to catch up with the rest of the world.
Since 1993 and the ongoing AWMA conferences the various states and territories also continued to provide edu-cational opportunities to clinicians who were developing their skills in wound management. Apart from company sponsored educational sessions there were few independent educational opportunities because those with the knowl-edge and ability to present sessions, generally hold full-time positions within their hospitals or organisations so any education they perform outside of work is generally done in their own time at their own costs.
WHy WOW?There have been only a few independent organisations set up to provide this much needed wound education; the most renowned being the Wound Foundation of Aus-tralia (WFA) 1994-2007. World of Wounds (WoW) was established in 2008 to provide non-award education to clinicians who were seeking the knowledge without the stressful assessment of a full academic programme. Some universities have masters programmes specifically dedicat-ed to wound management or where wound management is a major focus, however these are usually quite expensive and for many the challenge of academia is too daunting.
The programmes offered by WoW have covered the following subject matter areas:n Anatomy and physiology of healingn Pertinent factors affecting healing and other factors
to be consideredn Tissue recognition and setting aims for the various
types of tissue present within the woundn Wound care products and devices in both the
pharmacological and functionality stylesn Skin tears – prevention, classification, management
and ongoing preventionn Ambulatory burns – prevention, classification,
management and residual, if any, scar managementn Surgical wound dehiscence – looking at root causes
and problem solving with these causes in mindn Pressure injury – prevention, classification, manage-
ment and ongoing preventionn Ulceration of lower legs – prevention, classification,
management and ongoing prevention
MEDICAL & NURSING TRAININGThere are 13 schools of nursing within universities in Australia – details of these can be found at www.austral-ian-universities.com/schools/nursing. More recently other recognised education providers – Technical and Further Education (TAFE) institutions – have commenced small intakes of students onto their new Diploma in Nursing courses offering more of a clinical focus than a theoretical one to encourage more students into nursing. We, like many other countries, face a shortage of nurses3. The con-stant dilemma of ensuring that the training offered meets the clinical demands in an ever changing environment is faced by both the universities and the other education providers.
Curricula generally contain core subjects of patho-physiology, pharmacology and health assessment. Sadly wound management has taken a back step in many schools – not unlike that in medical schools. The North American Academy of Wound Technology, (NAAWT), which is a collaboration of international multidisciplinary experts, makes clear reference to the fact that physicians receive lit-tle if any education throughout their training in the theory
Australia by scale with Europe overlaid.
Science, Practice and Education
EWMA Journal 2012 vol 12 no 1 15

Science, Practice and Education
n Foot ulceration – the high risk foot, pre-vention, classification, management and ongoing care requirements
n Unusual wounds – skin cancers, inflam-matory ulcers, rare skin infections, radia-tion damage
n Resources available to assist in ongoing learning
Whilst WoW does have a planned annual pro-gramme which is available for viewing on the website www.worldofwounds.com, 50% of the work performed by the staff of WoW is by in-vitation. This aspect is seen as absolutely essen-tial; Australia being such a large country many participants are unable to be spared from their workplace for extended periods so by sending the trainer to the area, a variety of health clinicians can often be educated in the different forums. For example an invitation to speak to staff working in an aged care facility in a rural setting can be followed by an education session in the early evening for visiting community nurses and then an evening session for general practitioners and their nursing staff. Each session ranges from 1.5 - 2 hours and the subject matter areas will have been selected by the organisation making the request, usually based on re-cent events which may have driven their quest for further knowledge on the topic.
LEVELS OF TRAINING AND FOR WHOM?If asked to provide a one hour training session to Personal Care Assistants the instruction is given using only a white-board and highlighting the principles of wound care then further developing these in response to the participants answers to questions asked -this is a very interactive session and usual feedback gains 8/10 with notions such as –“now know the importance of feeding and good nutrition,” or “know not to rub skin dry, rather pat”.
For visiting community nurses who are time poor, and must be ‘Jacks of all trades” the invitation usually states specifically the topic on which they wish to be educated. A request for information on long standing lower leg ulcera-tion would enable the presenter to focus on the following – do they understand the pathophysiology, do they have access to a vascular surgeon, do they have access to good compression therapy methods? The access to a vascular surgeon in remote areas (sometimes only monthly) may result in long delays in consultation, so it is often necessary to help them establish relationships with the surgeons. Our email consultation services fill the void between the surgeon and the service provider and so provide much needed support.
I have also suggested that they invite the visiting vas-cular surgeon to meet with them for 30 minutes to discuss how he/she would like to receive referrals and when is the referral appropriate and/or inappropriate. Setting up good relationships is important in remote and rural areas; WoW offers to help with this and empowers the nurses with clinical reasoning rather than emotional bluff. Hav-ing the experienced practicing clinician /educator reinforce their understanding in wound healing and the various options for management adds strength to the learning and knowledge gained.
VIDEOCONFERENCING Where there have been clusters of interested parties a vide-oconference session has been run to deal with a specific topic, e.g. a new born baby with Epidermolysis Bullosa (EB). This rare condition would usually require the baby to be nursed in a large metropolitan hospital – often requiring air ambulance transfer and much stress and anxiety. If the doctors have deemed that the baby will most likely die within a few weeks, then the trauma of transferring can be too great, so the support of local staff is paramount. The videoconferencing session to support the community nurses providing care to the baby and family is seen as invaluable according to their feedback. This service is provided by a flexible learning unit within a larger training facility and thus remains independent but clinically focused.
States and territories and Country where WoW conducted wound educational training.
EWMA Journal 2012 vol 12 no 1 16

WOW ADMINISTRATIONWoW is administered under the umbrella of the Faculty of Health Sciences, School of Nursing and Midwifery, La Trobe University. The staff however is totally independent and was employed on the proviso that they were to be of no additional cost to the university, and, as such, are self funded. This allows for a not-for-profit ethos. Whilst this is not totally correct, the fees paid for the WoW education are well below that which one would pay if undertaking a full course within the university. This suits most clinicians who are in reality just wanting to gain more knowledge in order to work more effectively with better outcomes for those afflicted with slow to heal wounds.
All associated travel costs are met by the requesting or-ganisation and this is put into the initial planning budget so that when added to the tutorial fee, the actual par-ticipant costs will usually be less expensive than sending one or two staff members to a metropolitan training pro-gramme. This way more people may receive the training in order to disseminate the knowledge across the region and thus provide continuity of care.
SUMMARyWounds cover the entire health care spectrum. Wound training and education is limited in most medical and nursing schools. In general most health professionals gath-er their knowledge ‘on the job’. This can be both good and bad depending on the clinician and their continued profes-sional development learning. Products, devices and other approaches change. University education and other award training programmes can be expensive and often out of reach to the ‘average’ health care professional whose main aim is to improve skills in one particular area or aspect relevant to a local issue or concern. WoW has managed to have the flexibility to support the ongoing learning of these clinicians by providing education packages through multiple delivery modes such as face to face-programmes, whole days or short in-service sessions, videoconferencing and email consultations. m
References
1. Winter,G. Formation of a scab and the rate of epithelialisation of superficial wounds in the skin of the young domestic pig. Nature 1962; 193: 293–34
2. Australian Bureau of Statistics (homepage on the internet). National Statistics. Available from: www.abs.gov.au/ accessed November 12th 2012, last updated 29th November 2011
3. Jackson,D., Mannix,J. & Daly, J. Nursing staff shortages: Issues in Australian residential aged care. The Australian Journal of Advanced Nursing 2003; 1: 42-45
4. North American Academy of wound Technology (homepage on the internet). Available from: http://awt.vulnus.org/?page_id=4
5. Woodward, M. Wound management by aged care experts. Primary Intention. 2002; 2:70-76
ATMOS NPWT
With the next generation of the ATMOS S 041 Wound you get a solution for sensor-controlled wound drainage at a fair price!
Please ask for further information.
N E W Now with intermittent function
S i l e n t . G e n t l e . P o w e r f u l .
ATMOS MedizinTechnik GmbH & Co. KG Ludwig-Kegel-Str. 12, 14-16, 18 79853 Lenzkirch / GermanyTel: +49 7653 689-374 | Fax: +49 7653 [email protected] | www.atmosmed.comEWMA Journal 2012 vol 12 no 1

LOW WOUND PREVALENCE AND COST BURDEN: THE IMPACT OF A MULTIDISCIPLINARY WOUND SPECIALIST TEAM
Alison Hopkins, MSc, RGN, DN Cert
Fran Worboys, BSc Hons, RGN, DN Dip, Dip NursingEast London Wound Healing Centre (Since November 1st known as Accelerate CIC), Tower Hamlets, London UK
John Posnett, Heron Evidence Investment
Aim: A wound prevalence audit was undertaken within Tower Hamlets PCT in September 2009. As part of the analysis, it was important to trans-late this data into the economic burden to the PCT and discuss the findings in relation to the service model of the multidisciplinary wound care team.
Methods: A comprehensive wound prevalence au-dit in 2009 revealed a low wound prevalence of 1.2 per 1000 residents in a UK primary care trust. Additional data was captured on wound duration, nursing time, frequency of dressing, products used and travel time. This enabled a cost to be attrib-uted to the wound prevalence data.
Results: The economic analysis of this audit re-vealed that the cost burden attributed to wound care provision within this trust was significantly less than published studies (£1.14m per 100,000 vs £2.03m1), despite a more costly specialist team. The multidisciplinary wound care team is larger than would be expected in a population of 240,000 and includes specialists from nurs-ing with sessional time from podiatry, derma-tology and plastic surgery. The cost burden was attributed to nursing time (51%), dressings and bandages (16%), Specialist service (11%) and in-patient care (22%).
Early wound referral is encouraged so that ef-fective care can be implemented promptly. The team also has a heightened focus on leg ulceration of all types, the importance of gait management and efficacy of compression therapy. The data re-vealed high usage of compression therapy: 94% in venous or mixed ulceration demonstrating good tolerance to therapy. It is noteworthy that venous ulceration was significantly lower than published studies at 1.14 per 1000 residents. When reflect-ing on the specialist model and early interven-tion employed, the data revealed that 41% of all
patients with wounds, and 82% of venous ulcers patients, being known to the specialist service.
Conclusions: The specialist model employed within this UK primary care trust appears to have impacted on wound prevalence and the associ-ated cost burden. The multidisciplinary teams approach over the last 15 years has been towards early intervention thereby preventing chronicity and the most costly of patient groups, especially venous ulcer prevalence.
Specialist teams are assumed to be a costly extra to the healthcare system and to be reserved for the most complex of patients. Anecdotally it appears that many specialist posts are being lost as healthcare is rationed in the UK. This survey reveals a saving of over £2m to the Primary Care Trust when compared to comparable audits of a similar population. It is hoped that the outcomes of this audit will offer hope to other teams striving to demonstrate their worth.
1. Vowden K and Vowden P (2009) A survey of wound care provision within one English health care district. Journal Tissue Viability 18, 2-6
THE RESULTS OF A COMPREHENSIVE WOUND AUDIT IN A UK PRIMARY CARE TRUST
Alison Hopkins, MSc, RGN, DN Cert
Fran Worboys, BSc Hons, RGN, DN Dip, Dip NursingEast London Wound Healing Centre [Since November 1st known as Accelerate CIC], Tower Hamlets, London UK
Aim: The Tissue Viability services from Tower Hamlets PCT and Barts and the London NHS Trust undertook a wound prevalence audit to as-certain the extent of the wound caseload across all services and the cost burden to the local health economy. This short paper presents the data for Tower Hamlets residents only, identifying wheth-er they had a presented with a wound as an in-patient or being managed in community services.
Methods: A comprehensive wound prevalence audit was undertaken in September 2009. A tool used within published studies1 was utilized to en-able comparisons to be made as the districts had
Extended Abstracts EWMA 2011
Brussels · Belgium
Alison Hopkins,MSc, RGN, DN Cert
Correspondance:alison.hopkins@
acceleratecic.com
Conflict of interest: none
EWMA Journal 2012 vol 12 no 1 18

Science, Practice and Education
some similarities. Locally trained auditors captured data from district nursing, in-patients, GP Practices, Nursing Homes and other community services. Auditors went out to all services so that no reliance was placed in survey returns, thus ensuring robust capture of data. This was also checked against data from other sources. Data was analysed and an economic analysis was performed. A pa-tient survey captured patient experience and their views on quality of care and their involvement in care planning.
Results: 297 residents had wounds giving a prevalence of 1.2 per 1000 with an average of 1.31 wounds each. 52 patients were being managed within acute services, the remainder within a variety of community settings. 51% of patients had their wound for less than 3 months and 20% for longer than a year (Figure 1). Venous ulcer prevalence was lower than expected at 0.14 per 1000; studies report an incidence of circa 0.39 per 1000. Pressure ulcers were 12% of the total.
The majority of patients were managed within district nursing, whilst practices nurses saw patients with acute wounds of short duration. Quality indicators for assess-ment and management were satisfactory or good: 75% of patients had a documented pain assessment (Figure 2), 88% of patients with venous ulcers had a Doppler and were in compression therapy (Figure 3) and 90% of patients with pressure ulcers had specialist equipment. Documentation of risk assessment needed to be improved.
The patient survey revealed high scores in areas of confidence in care, pain management and the use of their opinion in care planning.
It was interesting to note that 41% of all patients with wounds were known to the specialist service: 82% of ve-nous ulcers, 65% of all foot and leg ulcers and 62% of pressure ulcers and all the grade 4 ulcers (Figure 4)
Conclusions: The wound prevalence of 1,2 per 1000 was lower than other published studies which range from 2.78-3.261,2. It appears that being a resident in this trust reduces their risk of having a non-healing wound. The younger and ethnically diverse population may contribute to this, as well as having an established specialist team that promotes early intervention thereby preventing the chronic wound.
As a specialist service we believe this reflects the referral pathway that encourages early referral and the specialist service philosophy of a zero tolerance to wounds. There is close engagement with services that manage any patients with wounds that are not progressing. There is the ex-pectation that this service would be closely involved with all wounds that are not showing signs of healing within 3 weeks of initiating treatment. The results of this survey demonstrate that the audit tool can be replicated in other trusts so that robust comparisons can be made. m
1. Vowden K and Vowden P (2009) A survey of wound care provision within one English health care district. Journal Tissue Viability 18, 2-6
2. Drew P, Posnett J, Rusling L (2007) The cost of wound care for a local population in England. Int Wound Journal 4,2 149-155
Figure 1
Figure 3
Figure 2
Figure 4
EWMA Journal 2012 vol 12 no 1 19

9503
170
0411
e
“ For faster healing and a balanced wound situation …”
accelerates wound healing process of problem wounds.
binds factors that inhibit wound healing
protects growth factors
stimulates fresh tissue growth
is fully absorbable
Suprasorb® C
Aseptic collagen sponge
Lohmann & Rauscher
www.Lohmann-Rauscher.com

BACKGROUNDGood quality information regarding the extent of the problem faced by patients suffering with pressure ulcer(s) is very limited. Important issues like pain and quality of life have not been fully explored and current risk assessment tools used in clinical practice have limitations in their ability to identify individuals at risk of pressure ulceration.
A collaborative academic/clinical group, lead by Professor Jane Nixon, was successful in gain-ing UK National Institute for Health Research (NIHR) funding of £2 million, to support a five year Pressure UlceR Programme Of reSEarch (PURPOSE). The collaboration includes clinical and academic partnerships for programme leader-ship and the involvement of over 40 NHS acute and community centres throughout England in the delivery and patient recruitment for the pro-gramme. The programme is also supported by a Steering Committee with International and Eu-ropean Pressure Ulcer Advisory Panel (EPUAP) representation.
PURPOSE aims to reduce the impact of pressure ulcers (PUs) on patients through:1. Early identification of patients at risk of PUs
and improved identification and investiga-tion of patients at risk of progression to se-vere PUs
2. The development of methods to capture patient-reported outcomes including health-related quality of life (HRQoL) and health utilities for routine clinical use and in clini-cal trials.
Objectives follow sequentially, addressing the research gaps identified and their subsequent ap-plication to practice.
Theme 1 Risk Assessment1. Determine the extent of pain suffering and its
role as a predictor of PU development.2. Identify individual and organisational fac-
tors which contribute to the development of severe PUs and develop a critical incident/adult neglect investigation methodology for the review.
3. Agree a PU Risk Factor Minimum Data Set and use this to underpin the develop-ment, implementation and evaluation of an evidence-based risk assessment framework including safety flagging to guide decision making about risk of superficial PUs and risk of progression to severe PUs.
Theme 2 Patient Reported Outcomes4. Determine outcomes important to patients
who develop PUs and develop a psychomet-rically rigorous, patient-reported outcome measure that is reliable and valid, and suit-able for use in the NHS.
5. Assess the value patients place on the preven-tion of PUs and develop a rigorous health utility measure.
OVERVIEW The PURPOSE programme comprises six indi-vidual research studies and two distinct themes, each one will be described in turn (Figure 1).
Nixon J, Wilson L.M, Coleman S, Gorecki C, Muir D, Pinkney L, Keen J, Briggs M, McGinnis E, Stubbs N, Dealey C, Nelson A
on behalf of the Purpose team.
Contact:[email protected]
Conflict of interest: none
Science, Practice and Education
Pressure ulcer programme of research – PURPOSE
EWMA Journal 2012 vol 12 no 1 21

THEME 1: RISK ASSESSMENT Risk assessment practices have not been updated for dec-ades. They are a basic screening tool, but have been evalu-ated as diagnostic instruments and their validity is variable. Recent work makes it timely to reshape risk assessment practice. However, prior to implementation, we will con-sider two research gaps, the role of pain as a PU predictor, and individual and organisational factors which lead to severe PUs. This work will then inform the development of an evidence-based minimum data set to standardise documentation of key risk factors and underpin risk as-sessment.
Study 1. Pain Pain is often a significant and disabling symptom for those with pressure ulcers (PUs). A systematic review of health related quality of life in patients with pressure ulcers (PUs) identified that patients’ reports of localised skin pain asso-ciated with early PU development are ignored, but limited prospective data suggested it may be predictive of PUs4. Integrating pain assessment and management into PU prevention and management may lead to better outcomes.
Establishing the extent and type of pain is important to guide clinical practice. There are essentially two types of pain: nociceptive pain resulting from the inflammatory response, and neuropathic pain occurring as a result of nerve damage or tissue ischaemia; both types of pain can occur during pressure ulcer development. The objective of study 1, therefore, is to determine the extent of pain suffering and its role as a predictor of PU development. Two integrated studies are being undertaken to explore pain and PUs as follows.
Pain PrevalenceThe aims of the pain prevalence study were to: n determine the prevalence of localised PU pain in
‘pressure areas’.n assess the type and severity of localised PU pain in
‘pressure areas’ in patients with clinically assessed normal skin and Grade 1-U PUs
n explore the association between pain and skin clas-sification.
We undertook pain prevalence surveys in three acute NHS Trusts and two Community NHS Trusts in the UK. By piggy-backing pain questions onto the routine annual PU prevalence audits, anonymised individual patient data was recorded by a ward nurse. In addition to the standard PU data, patients were asked two questions relating to local-ised skin pain to establish PU pain prevalence. Where pain was indicated, consenting patients underwent a detailed pain and skin assessment using:1. numerical rating scale2. an adapted Leeds Assessment of Neuropathic
Symptoms and Signs (LANSS) Pain Scale3. Skin assessment using EPUAP classification.
Pain Cohort This study aims to explore the role of pain as an early predictor of Category 2 PU development. We are cur-rently undertaking a prospective cohort study with 30 days follow-up, in acute and community NHS Trusts, involving 632 patients at high-risk of PU development.
This study started in December 2009 and will end recruitment in December 2011. Results will be analysed and published in 2012.
Study 2. Severe PU Study. There is suggestive evidence that some severe pressure ulcers occur due to the organisation of care surrounding patients. However, there are no studies which have ad-dressed this problem systematically. Risk factor studies fail to recruit enough patients who develop severe pressure ulcers. Local investigation of severe pressure ulcers is not standardised and learning is not shared across the NHS. There is a need to undertake primary research and use the findings to improve the risk assessment framework which is being developed locally.
The Severe PU study is multi-centre and based in acute and community settings in the north of England, and
Figure 1
Science, Practice and Education
EWMA Journal 2012 vol 12 no 1 22

focuses on links between severe pressure ulcers and patient safety. The study reviews patients with severe pressure ulcers retrospectively through their care path-ways, focusing on the organisation of care and how this may have influenced the development of their pressure ulcers.
The aims of this study are i) to find causal explanations for severe pressure ulcers and ii) to produce findings which can be generalised to all patients who develop severe pressure ulcers. It has been designed to:n provide better methods for reviewing severe
pressure ulcers n contribute to tools (i.e. a risk assessment frame-
work and a clinical incident review tool) to aid better understanding and prevention of an actual severe pressure ulcer in daily practice.
n disseminate recommendations for multi-agency service improvements aimed at promoting patient safety, reducing system failures for patients and risk of NHS prosecution
The study is a novel retrospective case study design, using primarily qualitative methods. This type of study has rarely been applied in health care. It has more often been used in high risk industries to look at safety inci-dents; however the design has resonance with inquiries into clinical incidents such as the Bristol Royal Infir-mary Inquiry (2001). In addition to talking to patients about their experiences, the study includes talking to other people involved in a patient’s care pathway, such as informal and professional carers, nurses, and other relevant people, gaining their personal experience of the development of the severe pressure ulcer. This process involves systematically searching relevant health care documentation, and with the aid of a narrative chro-nology, compiling all evidence to produce a ‘coherent account’ of what happened to each patient involved in our study. Cases are then analysed.
Results will be analysed and presented in 2012
Study 3. PU Risk Assessment Framework (PURAF)This study aims to develop an evidence-based Pressure Ulcer Risk Assessment Framework (PURAF) for use in clinical practice and agree a Pressure Ulcer Minimum Data Set (PU-MDS) to facilitate comparison of patient groups.
We will utilise structured consensus methods com-prising a nominal group of international PU experts and a wider participant Delphi group of other experts in the field, as well clinical users, to facilitate the de-velopment of a PURAF and PUMDS to meet the re-
10th Scientific Meeting of the
Diabetic Foot Study Groupof the EASD
28-30 September 2012
Berlin-Potsdam, Germany
www.dfsg.org
Conference theme
Advancementof knowledgeon all aspects ofdiabetic foot care
Main subjects during conference: Epidemiology Basicandclinicalscience Diagnostics Classification Footclinics Biomechanics,Osteoarthropathy Orthopaedicsurgery Infection Revascularisation Uraemia Woundhealing/outcome
EWMA Journal 2012 vol 12 no 1

We developed the PU-QOL instrument to measure PU symptoms and HRQL outcomes in people with PUs on the basis of a conceptual framework of HRQL developed from a systematic review, patient interviews and clini-cal expertise. These three sources were used to generate an exhaustive item pool which was subsequently used to produce a draft version of the PU-QOL instrument. A multidisciplinary group of clinical and health outcome methodology experts evaluated the draft version, which was then pre-tested using mixed methods. Psychometric evaluation was undertaken in two parts: 1) Item reduc-tion on the basis of PU-QOL instrument data from 227 patients with PUs and 2) formal psychometric evaluation using both classical and Rasch methods on the basis of PU-QOL instrument data from 231 patients with PUs.
The final PU-QOL instrument consists of 10 validated scales to measure PU symptoms (pain, exudate, odour), physical functioning (sleep, movement and mobility, daily activities, vitality); psychological well-being (emotional well-being, self-consciousness and appearance); and so-cial participation. Scale scores are generated by summing items. High scores indicate greater patient bother. The PU-QOL is intended as an administered instrument and patients rate the amount of bother attributed (e.g. “During the past week, how much have you been bothered by…?”) on a three-point response scale (e.g. 0=not at all – 2=a lot). We chose a recall period of the past-week on clinical grounds; as changes in PU severity and symptomology generally occur over days, a longer recall period would risk missing changes relevant to HRQL.
This work is complete and results papers will be pub-lished in 2012.
Study 5. Health Utility Measure Study (PUQOLY) aims to develop health economic tools to ensure appropriate allocation of PU prevention and management resources. The protocol for this study is currently being developed and results will be published in 2013.
PURSUN – The Pressure Ulcer Research Service User Network for the UKPatient and Public Involvement (PPI) is an important part of the programme and the team works closely with the Pressure Ulcer Research Service User Network UK (PURSUN UK). For more information about PURSUN UK contact Delia Muir ([email protected]). m
AcknowledgementsThis publication presents independent research commissioned by the National Institute for Health Research (NIHR) under the Programme Grants for Applied Research programme (RP-PG-0407-10056).
quirements of clinical practice. We will also consult with PURSUN (Pressure Ulcer Research Service User Network (see below)) to explore the acceptability of proposed risk assessment elements with patients and carers. The work is underpinned by a PU risk factor systematic review and emerging evidence from the other PURPOSE studies (Figure 2).
This study is ongoing and results of this work will be presented and published in 2012/13.
THEME 2: QUALITy OF LIFE There is no formal method for assessing need or evaluat-ing outcomes from the patient’s perspective. Therefore, clinical decision making is usually based upon opinion. The development of a reliable and valid patient reported outcome measure will provide a rigorous tool for assessing needs and evaluating patients’ self reports of the outcomes of PU treatments. In addition, we need to provide the evidence base necessary to establish the value of improve-ments in PU prevention and management to ensure appro-priate funding of effective interventions within the NHS.
Study 4. PU Quality of Life (PUQOL) Assessments of health outcomes are increasingly included in clinical trials, with patient-reported outcomes (PROs) now an integral aspect of patient care, policy decision-making and healthcare delivery. With International con-sensus for use of scientifically robust and responsive PRO instruments in routine clinical practice and research, the careful stepwise construction of PRO instruments, based on current detailed guidelines, is a must. Currently no PRO instruments are available to assess the impact of pres-sure ulcers (PUs) on health-related quality of life (HRQL).
Figure 2
Science, Practice and Education
EWMA Journal 2012 vol 12 no 1 24

helps healing.

Customisable wound healing with all the right pieces.V.A.C.Ulta™ Therapy System
NOTE: Specific indications, contraindications, warnings, precautions and safety information exist for KCI products and therapies. Please consult a physician and product instructions for use prior to application.
© 2011 KCI Licensing, Inc. All Rights Reserved. All trademarks designated herein are proprietary to KCI Licensing, Inc, its affiliates and/or licensors. This material is intended for healthcare professionals only. DSL#xx-xxxx.EMEA.CS (12/11)

Science, Practice and Education
Waldemar L. Olszewski1,3
Piotr Andziak1,2 M. Moscicka-Wesolowska1
Bozenna Interewicz1
Ewa Swoboda4 Ewa Stelmach1,4
1Department of Surgical Research and Transplant-ology, Medical Research Center, Polish Academy of Sciences, Warsaw, Poland
2Department of General and Vascular Surgery, Central Clinical Hospital, Ministry of Internal Affairs, Warsaw, Poland
3Department of Gastro-enterological Surgery and Transplantation, Central Clinical Hospital, Ministry of Internal Affairs, Warsaw, Poland
4Department of Clinical Microbiology, Warsaw Medical University, Warsaw, Poland
Correspondence:[email protected]
Key words: atherosclerosis, femoral artery, inflam-mation, bacteria, bacterial DNA
ABSTRACTLower limb ischemia is not infrequently accompa-nied by toe necrosis. The question arises whether this is only the consequence of lack of arterial perfusion or in addition infection of ischemic tis-sues. So far, not much attention has been attached to the patient’s own limb skin and deep tissue’s bacterial flora, activated in ischemic tissues. This flora may enhance the inflammatory and throm-botic process in the atherosclerotic arteries. Aim: To identify microbial cells and their DNA in perivascular tissues and arterial walls of ischemic lower limbs. Methods: Bacterial cultures and PCR method for detection of 16s RNA and immunohistopatho-logical staining for identification of immune cells infiltrating vascular bundles.Results: a) specimens of atherosclerotic calf and femoral arteries contained bacterial isolates and/or their DNA, whereas, in control normal ca-daveric organ donors’ limb arteries or patients’ carotid arteries and aorta bacteria they were de-tected only sporadically, b) lower limb lymphatics contained bacterial cells in 76% of specimens, whereas controls only in 10%, c) isolates from limb arteries and lymphatics belonged in major-ity to the coagulase-negative staphylococci and S.aureus, however, other highly pathogenic strains were also detected and d) immunohistopathologi-cal evaluation arterial walls and periarterial tissue showed dense focal infiltrates of granulocytes and macrophages.Conclusions: Own bacterial isolates can be re-sponsible for dense neutrophil and macrophage inflitrates of atherosclerotic walls and periarterial tissue in lower limbs and this aggravates ischemic changes.
INTRODUCTIONMultiple studies were carried out on Chlamydia, Helicobacter, Herpes and dental bacteria’s’ role in atherosclerosis(1-5). So far, not much atten-tion has been attached to patients’ own bacterial foot and calf bacteria activated in ischemic tis-sues. They may enhance the inflammatory and thrombotic processes in the atherosclerotic arter-ies. This especially applies to the arteries of lower limbs with a dramatically higher exposure to en-vironmental bacterial stress than arteries of other body regions(6). Foot and leg skin is inhabited by a number of bacterial strains not encountered in other body regions(7, 8). They belong to the skin saprophytic flora and in particular to the coagula-se-negative Staphylococci(9). There are also highly pathogenic bacteria originating from the anal and perineal regions floating down on epidermal scales and colonising foot skin. Microbes may penetrate epidermis upon even minor injuries infecting limb vascular bundles either directly or through the lymphatics draining foot skin accompanying large blood vessels(10, 11).
The question arises whether infection of lower limb arteries by foot and calf bacteria may aggra-vate the inflammatory and occlusive atheromatous changes and act as a secondary destructive factor. Moreover, the question is whether these bacterial strains may be the causative factor of infective complications after arterial grafting(12, 13, 14).
We investigated the atherosclerotic tibial, pop-liteal and femoral arterial walls harvested from the amputated ischemic limbs for presence of (i) bacterial cells and (ii) their DNA, with use of broad- range PCR targeting conserved region 16s RNA of nosocomial microbes. The findings were compared with those obtained from normal arteries harvested from organ donors. The con-trol material consisted also of carotid plaques and punch fragments of thoracic aorta obtained dur-ing CABG operation. Moreover, bacteriological
The skin’s own bacteria may aggravate inflammatory and occlusive changes in atherosclerotic arteries of lower limbs
EWMA Journal 2012 vol 12 no 1 27

findings were correlated with the immunohistochemical changes in the arterial wall and periarterial tissue.
MATERIAL AND METHODS
Patients:Investigations were carried out in one study with three control groups. Group I comprised 50 patients, age range 55 to 76 years (mean 64), 15 females and 35 males, with atherosclerosis of lower limb arteries causing chronic ex-acerbated foot ischemia. Thirty-two patients had intracta-ble ischemic foot pain and in 18 patients necrosis of toes was in an initial stage. Obstruction of superficial femoral, popliteal and calf arteries was diagnosed on arteriography. In all patients the arteriographic image precluded recon-structive operation and amputation was performed below the knee or in the mid-thigh. Fragments of arteries were harvested. All patients received wide-spectrum antibiotics for at least seven days before amputation. Excluded were patients with overt diabetes. In Group II normal lower limb arterial fragments were obtained from 25 cadaveric organ donors. In Group III 50 atherosclerotic plaques with media and partial adventitia were obtained from carotid arteries by thromboendarterectomy. In Group IV, punch fragments of aorta at the site of coronary artery bypass graft were taken from 100 patients with CAD. Approval to conduct this study was obtained from the Warsaw Uni-versity medical ethics committee.
Harvesting of material:Fragments of posterior tibial, popliteal and/or femoral artery, and calf lymphatic vessels were harvested in the operating room from the stumps of amputated lower legs and thighs, immediately after the operation. In the control groups fragments of femoral artery, lymphatic vessels, ca-rotid plaques and punch fragments of aorta were collected.
Bacteriological culture media:The following media were used: Hemoline liquid medium (Biomerieux), Columbia blood agar base enriched with 5% sterile defibrinated sheep blood, MacConkey’s agar, Chapman’s agar, Sabouraud’s agar (malt agar), and brain heart infusion (BHI) (all from Difco, Detroit, MI).
Identification of bacterial strains:The cultures were incubated at 37oC and examined at 24 and 48 hours for aerobic bacterial growth. Isolates were identified by standard procedures using the Analytical Profile Identification (API) System (Biomerieux). Aerobic Cocci of the Micrococcaccae family were identified using the API- Staph system. Bacteria of Streptococcaccae family were identified with API 20 Strep. Members of the genus
Corynebacterium (gram-positive coryneform and pleo-morphic rods) were identified with API Coryne. Gram-negative rods were identified using API 20E. Gram-pos-itive spore-forming Bacilli (Bacillus spp.) were identified by evaluating the fermentation of sugars or polyalcohols. The sensitivity of isolated bacterial strains to antibiotics was examined using the ATB system (Biomerieux).
Identification of bacterial DNA:Bacterial 16s RNA. The PCR amplification was per-formed with primers for gene fragment coding bacterial 16s RNA: 5’AGTTTGATCCTGGCTCAG 3’ forward and 5’GGACTACCAGGGTATCTAAT 3’ reverse to detect any bacterial strain..
Antibodies and immunohistochemical procedures for atherosclerotic changes:
The following specific antibodies purchased from Dako (Glostrup, Denmark), (antigen specificity, clone number and working dilution in parentheses) were used: HLA DR (MHC class II, CD68 (mostly macrophages, EMB11, 1/50), CD3 (T lymphocytes), CD4 (helper cells), CD8 (cytoxic cells), CD68 (macrophages), CD14 (monocytes), CD11a and CD11c (adhesion molecule, leukocytes, dendritic cells), neutrophil elastase (NP57, 1/100), cytokine IL8, macrophage inflammatory protein MIP1, and macrophage chemoattracting protein MCP1. The antibodies against LYVE-1 antigen located on lym-phatic endothelial cells were obtained from Relia Tech (Braunschweig, Germany). The sections were examined microscopically and photographs were taken using an Ol-ympus Camera Microimage System.
Analysis of infiltrating cell density:The evaluated areas were cross sections of arterial wall and adjacent tissue, plaque shoulders with media. The density of infiltrating cells was evaluated using the following score: + = up to 25 cells, ++ = 25 to 50 cells, +++ = above 50 cells accumulating focally. Means from 3-5 infiltrating foci were calculated. All specimens were evaluated microscopi-cally by two independent investigators.
Data statistical evaluation:The frequency of bacterial isolates was presented in %. The differences in frequency between sites of bacteria location were evaluated using chi square method with significance level at p<0.05. The Monte Carlo exact test was used to investigate the significance of differences in the mean densities of infiltrates between the groups. A p-value <0.05 was considered statistically significant.
EWMA Journal 2012 vol 12 no 1 28

Science, Practice and Education
RESULTS
Bacterial isolates in arterial walls:In the 50 ischemic limbs specimens of tibial and popliteal arteries 58.6% contained bacterial cells and in femoral arteries it was 33.8%. In the control, healthy femoral ar-teries microbial cells were isolated in just 11% (p<0.05). Lower limb lymphatics contained bacterial cells in 76%, whereas in the control they were only in 10% (Fig.1). In the carotid arteries microbes were detected in 4% and in the aortic wall in 0.7%. The difference between limb and carotid arteries and aorta was significant at p<0.001.
The isolates in limb arteries belonged, in the major-ity, to the coagulase-negative staphylococci and S.aureus. The highly pathogenic Enterococcus, Proteus, Pseudomonas, Micrococcus, Klebsiella, Enterobacter, Serratia, Acinetobacter and Citrobacter were also found. In 25 control specimens obtained from the femoral artery bacterial cells were found only sporadically. The gram-positive bacteria were sen-sitive to all antibiotics but penicillin. Enterococcus was mostly sensitive to vancomycin.
Bacterial isolates in limb lymphatics:Bacterial isolates from lymphatic vessels of ischemic limbs belonged mostly to S. epidermidis and S. aureus. Less com-mon were Enterococcus, Pseudomonas and E.coli. Normal lymphatics contained S. epidermidis. Bacterial isolates were sensitive to all antibiotics but penicillin and meticillin.
Microbial DNA in arterial wall:Out of the 50 samples of tibial, popliteal and femoral arteries the 16s RNA gene was detected in 70%. In 25 normal femoral arteries 16s RNA was detected in 21%. In 50 samples of atherosclerotic carotid plaques the 16s RNA gene was found in 29%. Of the total number of 100 aortic wall biopsies, the 16s RNA gene was found in 32%.
Comparison of frequency of bacterial isolates and DNA:Evidently higher frequency of detected bacterial DNA than of bacterial isolates was noted in the calf and femoral arterial walls (p>0.05). In 50 samples of atherosclerotic carotid plaques the 16s RNA gene was found in 29% and bacterial cells in 4% (p<0.05). Of the total number of 100 aortic wall biopsies, the 16s RNA gene was found in 32% and bacterial isolates in 0.7% (p<0.05).
Immunohistochemical findings:The density of infiltrating cells in the limb arterial walls and carotid plaque shoulders and media was similar, ex-cept that granulocytes were more frequently seen in tibial arteries. The HLA DR, CD 68, and CD14 cells as well as neutrophils formed in limb adventitia and periarterial tissue dense focal infiltrates (+++). Although the structure of plaques was similar in the limb and carotid arteries, the parietal thrombi were evidently more common in tibial and popliteal arteries. There were multiple macrophages
Fig. 1. The frequency rate and names of bacterial strains on skin, in vascular bundles of calf and thigh, muscles and lymphatics. In pa-rentheses normal values (details in results)
EWMA Journal 2012 vol 12 no 1 29

and granulocytes in the thrombi. Most dense infiltrates of granulocytes and macrophages were seen in tibial veins accompanying arteries. Multiple lymphatics, a possible microbial conduit from the foot, were located between arteries and veins.
DISCUSSIONThere is a plethora of articles on the role of infective fac-tor in the pathogenesis of atherosclerosis in the coronary, carotid and subclavian arteries and thoracic and abdominal aorta, however, only a few papers are dealing with the iden-tification of bacterial cells or their DNA in arteries of lower limbs and their effect on the arterial wall(6). The presence of CP (Chlamydia pneumonia), HP (Helicobacter pylori), CMV (Cytomegalovirus) and HSV (Herpes simplex virus) as well as odontopathogens Porphyromonas gingivalis and Streptococcus sanguis in atherosclerotic plaques of coro-nary and carotid arteries and aortic wall has been widely documented both using PCR and serological methods(1-5). Mixed infections consisting of the by us detected microbes and those multiple microorganism described in the litera-ture should be taken into consideration in understanding of the development of inflammatory and occlusive changes in arteries and their neighbouring tissues(15-17).
Human skin of all regions has been considered to har-bor a complex microbial ecosystem, with transient, short-term resident and long-term resident biota, based on the consistency with which they are isolated. Staphylococcus, Micrococcus, Corynebacterium, Brevibacteria, Propionibac-teria, and Acinetobacter species are, among others, regu-larly cultivated from normal skin. Staphylococcus aureus, Streptococcus pyogenes, and Pseudomonas aeruginosa may be transient colonisers, especially in pathological condi-tions(7,8,9).
Lower limbs are exposed to specific bacterial phe-notypes originating from the environment and perineal and anal regions. Their soft tissues are considered to be immune to colonisation in the process of “physiological” penetration of microorganisms through the normal sole skin, as well as during multiple foot epidermal abrasions or micro-injuries. Few penetrating microbes are transported away from the ports of entry via lymphatics to the lymph nodes. The low “bacterial load” transported in this fashion is clinically hardly recognisable. Bacteriological culture of harvested lymph in normal individuals allows identifica-tion of microorganisms in lower limb lymph in around 5-10%(10). Since limb deep lymphatics are running in a close proximity to the veins and arteries and the lymphatic endothelium has the ability to transports particles ad- and abluminally, there exists a possibility for infecting arterial wall at the predisposed sites. The lymph microbes may be highly pathogenic in limb ischemia and add to the already existing inflammatory changes.
In our studies, the high prevalence of isolates in tibial, popliteal and femoral arterial walls and concomitant occlu-sion of the arterial lumen with thrombi raises the question as to whether these microbes may be an additional patho-genic factor responsible for inflammatory and ischemic changes. Bacterial isolates were practically detected only in lower limb arteries and adjacent tissues. Also the 16s RNA was detected at higher level in limb arteries than in the controls. Higher level of bacterial DNA than of live bacterial cells is the result of retention of the genetic mate-rial of dead bacteria in the tissues and macrophages. The density of macrophage and leukocyte infiltrates in limb arterial walls was higher than in carotid arteries and there were also parietal or lumen occluding thrombi.
Taken together, we conclude that bacteria such as Staphylococci and other foot colonising microbes may have a secondary destructive effect on the arterial wall in ischemia. Their presence may have an additional impact on the infective complications after arterial bypass proce-dures. m
AcknowledgementsThis study was carried out with support from the Ministry of Science and Higher Education nr 2 PO5D 032 30
REFERENCES
1. Ross R: Atherosclerosis – an inflammatory disease. N Engl J Med 1999; 340:115-126.
2. Muhlestein JB: Chronic infection and coronary artery disease. Med Clin North Am 2000;84:123-148.
3. Kol A, Libby P: Molecular mediators of arterial inflammation. A role for microbial products? Am Heart J 1999;138:450-452.
4. Gaydos CA, Quinn TC: The role of Chlamydia pneumoniae in cardiovascular disease. Adv Intern Med 2000;45:139-173.
5. Nieto FJ: Infections and atherosclerosis: new clues from an old hypothesis? Am J Epidemiol 1998;148:937-58.
6. Mayr M, Kiechl S, Willeit J, Wick G, Xu G: Infections, immunity, and atherosclerosis. Circulation 2000;102:833-83.
7. Costello EK, Lauber ChL, Hamady M, Fierer N, Gordon JI, Knight R: Bacterial community variation in human body habitats across space and time. Science 2009; 326:1694-97.
8. Zhan Gao, Chi-hong Tseng, Zhiheng Pei, Blaser MJ.: Molecular analysis of human forearm superficial skin bacterial biota. PNAS 2007; 104: 2927–2932.
9. Kloos WE., Musselwhite MS.: Distribution and persistence of staphylococcus and micrococcus species and other aerobic bacteria on human skin. Applied Microbiology 1975; 30:381-395.
10. Olszewski WL, Jamal S, Manokaran G: Bacteriological studies of skin, tissue fluid, lymph, and lymph nodes in patients with lymphoedema. Am J Trop Med Hyg 1997;57:7-15.
11. Kung Wang, DeChang-Wang, Y, Yong Qian Feng, Xian Feng Leng: Lymph invasion route of bacteria and endotoxin and CD4+/CD8+ T cells ratio changes of draining lymph node of burn infection wound. Burnes 2008; 34: 234-240.
12. Lalka SG., Malone JM., Fisher Jr. DF., Bernhard VM., Sullivan D, Stoeckelmann D, Bergstrom RF.: Efficacy of prophylactic antibiotics in vascular surgery: An arterial wall microbiologic and pharmacokinetic perspective. J Vasc Surg 1989;10:501-10.
13. Malone JM., Lalka SG., Mclntyre KE., Bernhard VM., Pabst TS.: The necessity for long-term antibiotic with positive arterial wall cultures therapy. J Vasc Surg 1988;8:262-7.
14. Macbeth GA, Rubin JR., Mclntyre KE., Goldstone Jr.J, Malone JM.: The relevance of arterial wall microbiology to the treatment of prosthetic graft infections: Graft infection vs. arterial infection. J Vasc Surg 1984; 1:750-756.
15. Szczesny G., Interewicz B., Swoboda-Kopec E., Olszewski WL., Górecki A., Wasilews-ki P.: Bacteriology of callus of closed fractures of tibia and femur. J Trauma 2008; 65(4):837-842.
16. Wakefield TW., Pierson CL., Sehaberg D R., Messina LM., Lindenauer SM, Greenfield Lazar J., Zelenock GB., Stanley JC.: Artery, periarterial adipose tissue, and blood microbiology during vascular reconstructive surgery.: Perioperative and early postoperative observations. J Vasc Surg 1990;11:624-8.
17. Ploeg A, Lange C, Lardenoye JW, Breslau P. Nosocomial Infections after peripheral arterial bypass surgery. World J Surg 2007; 31:1687-1692.
Science, Practice and Education
EWMA Journal 2012 vol 12 no 1 30

New
Tried. True. Trusted.TM powered by
STRENGTH • ABSORBENCY • CONFIDENCE
Hydrofiber® dressing with strengthening fiber
More to love about AQUACEL® dressingsNEW AQUACEL® EXTRA™ dressing:• 9x stronger1a
• 39% more absorbent1a
• Manages a wide range of exudate levels
AQUACEL® DressingsTRIED. TRUE. TRUSTED.TM
To find out more about AQUACEL® EXTRA™ dressing, please visit www.convatec.com
aAs compared to original AQUACEL® dressing.Reference: 1. Preliminary assessment of the physical properties of AQUACEL® EXTRATM and AQUACEL® Dressings. Scientific Background Report. WHRI3461 TA214. 2011, Data on File, ConvaTec Inc.
AQUACEL and Hydrofiber are registered trademarks of ConvaTec Inc. AQUACEL EXTRA and Tried. True. Trusted. are trademarks of ConvaTec Inc. © 2011 ConvaTec Inc. AP-011601-MM [AM/EM]

Pain is bad, but unnecessary pain is even worse. Safetac® technology is less painful
to the wound and patient than any traditional advanced adhesive1. It doesn’t strip skin at
dressing changes2. It doesn’t stick to the moist wound bed3. Safetac technology also seals the
wound margins, protecting healthy tissue around the wound against maceration. With Safetac,
there’s no reason a dressing change should be more painful for anyone. Give your patients
more reason to smile. Reduce the pain at dressing changes with Safetac technology.
For more information about Safetac technology, please visit www.molnlycke.com
1. White R., Wounds UK 2008; Vol 4, No 1 2. Dykes PJ et al. Journal of Wound Care 2001: 10: 7-10 3. White R. Evidence for atraumatic soft silicone wound dressing use. Wounds UK 2005; 1 (3): 104-109. 3. White R. Evidence for atraumatic soft silicone wound dressing use. Wounds UK 2005; 1 (3): 104-109.
The Mölnlycke Health Care name and logo, Safetac®, Mepilex® wound dressings and Mepitel® are registered trademarks of Mölnlycke Health Care AB.Mölnlycke Health Care AB (publ.), Box 13080, SE-402 52 Göteborg, Sweden. Phone + 46 31 722 30 00. www.molnlycke.com
Patented Safetac® technology is available exclusively on Mepilex® wound dressings, Mepitel® and other selected Mölnlycke Health Care dressings.
Put a smile on withSafetac® technology

ABSTRACTKey words: Burn, pain, quality of life.The aim of study: To investigate chronic pain in burn survivors in the six months after injury in terms of incidence, quantitative and qualitative characteristics and health-related quality of life.Methods: A cross sectional study carried out in Kaunas medical hospital in Lithuania. Standard Questionnaires were sent by email to burn vic-tims treated in a single burn unit during period of 01/06/2008– 30/04/2009. Results: Response rate was 36.7%. Of those who responded, 68.2% of patients indicated that they are suffering from varied intensity of pain at the site of the burn and those patients who had ex-perienced wound infection in the acute trauma period, indicated a higher NAS score (p=0.03). Of our patients, 86.3% responded on the emotional scale: one quarter (25%) were fearful and one-third (33.3%) found the pain tiring. In addition, 84.38% of patients marked on the neuropathic pain scales: hot burning 36.4%, gnawing 29.5%, (p=0.01). A large percentage of patients, 70.4%, stated that social relationships were affected and limited by their poor physical well-being and emotional problems and 43.2% of patients also said that post-burn pain limited their usual daily activity.Conclusions: More than 60% of burn survivors experience chronic pain at the burn site and 50% in donor sites six months after injury. The inten-sity of chronic pain correlates with the wound infection rate during the acute period. Quality of life in patients experiencing post-burn pain is poor because of disrupted physical well-being, general health status and chronic pain.
INTRODUCTIONAbout 7000 people experience burn injuries in Lithuania every year. Over 1500 of them are ad-mitted to hospitals and about 400 victims of inju-ries are treated in specialised burn centres1. Stand-ard burn wounds’ care involves a series of daily, aggressive procedures that stimulate nociceptive afferent fibres days, weeks, or months following initial injury. Severe burns are among the most painful, devastating, sudden and unpredictable forms of trauma, which affect the victims both physically and psychologically2. Burn pain is not a single entity but involves several components, which cause the most severe and prolonged types of pain3. Most patients with burns experience a profound impairment in chronic pain and quality of life (QOL)4.
Chronic pain has been identified as a signifi-cant problem following a burn injury even many years after burn recovery. In studies, prevalence of chronic pain has been shown to be high, with esti-mates ranging from one quarter to over a third of burn patients reporting chronic pain. Choiniere et al. (1991) found that 35% of the patients (n=104) still complained of chronic pain one year or more after the burn injury5. In a study by Malefant, performed one year or more after burn trauma, 36.4% of the participants complained of pain and 71.2% of paresthetic sensations6. In addi-tion, 52% of respondents (Phoenix Society for Burn Survivors) reported ongoing burn-related pain 12 years after their injuries (n=348, 24% response rate)7. The co-occurrence of pain and depression represents an even greater risk of reduced physi-cal functioning over time among burn survivors (n=122)8.
The aim of the studyTo investigate chronic pain in burn survivors six months following injury: its incidence, quantita-tive and qualitative characteristics and impact on health-related quality of life and daily activity.
Laima Juozapaviciene1 MD
Rytis Rimdeika2
MD, PhD, Professor of Plastic Surgery
Aurika Karbonskiene3
MD, PhD, Associate Professor of Anesthesiology
1Dpt. of Anestesiology, Lithuanian University of Health Sciences, Kaunas, Lithuania
2Department of Plastic and Reconstructive Surgery
3Department of Anesthesio logy,University Hospital Kauno Klinikos, Lithuanian University of Health Sciences
Correspondence: [email protected]
Conflict of interest: none
Problem with the post burn wound pain: Chronic profiles
Science, Practice and Education
EWMA Journal 2012 vol 12 no 1 33

METHODSA cross-sectional study was carried out at a major terti-ary care hospital in 2009. Standard questionnaires were mailed to burn victims treated in a single burn unit during period of 01/06/2008 - 30/04/2009 more than six months following their burn injury.
General demographic information (age, gender, edu-cation, place of residence, occupation and marital status), burn-related information (depth and extent of burn, loca-tion of burn and cause of burn), burn care and therapy-related information (information about type and number of surgical interventions, and complications such as wound infection, pneumonia, etc.) were obtained from medical notes and questionnaires. Burn pain intensity was meas-ured by a numerical rating scale (NRS).
The quantitative characteristics of chronic burn-related pain were obtained by using the Standard McGill Pain Questionnaire (Lithuanian version), a validated instru-ment widely employed in many clinical studies of pain. It consists of 54 descriptors from which the patient selected those that best described his/her pain. The adjectives, scaled according to relative intensity within each category, are grouped into three major classes which measure the sensory, emotional and evaluative dimensions of the pain experience.
Medical Outcomes Study 36-Item Short Form Ques-tionnaire (SF-36) was used for this study. The SF-36 describes outcomes in terms of eight separate subscales: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health. It also produces two summary scores: the physical component summary (PCS) and the mental com-ponent summary (MCS). All items in the SF-36 were scored on a Likert 5 grade scale: 4=extreme, 3=quite a bit,
2=moderate, 1=a little bit and 0=none at all. The overall scoring of the test was calculated on the sum of the scores in each item divided by the total number of items and expressed in percentages (%). This percentage refers to the degree of alteration of quality of life estimated by the questionnaire for a particular patient with 100% being the maximum alteration and 0% being the minimum.
Statistical analysisData entry and analysis were performed using the Statisti-cal Package for Social Sciences version 13.0 (SPSS, Inc., Chicago, IL, USA). The qualitative data were presented as numbers, percentages and as mean (x–), with standard deviation (SD) for quantitative variables. The internal con-sistency of SF-36 subscales was assessed with Cronbach’s alpha (a) coefficients with the questionnaire being reliable if Cronbach’s a value >0.7. The P value of <0.05 shows a significant result. All correlations were reported in terms of Pearson’s coefficient of correlation (r) with corresponding 95% confidence intervals (95% CI’s) and upper (UCL) and lower (LCL) confidence limits where appropriate.
EthicsThe study was carried out in compliance with the Helsinki Declaration and approved by the local ethics committee (Kaunas Regional Committee of Biomedical Research, nr BE-2-77).
RESULTSQuestionnaires were mailed to 120 patients and 44 responses were received (response rate – 36.7%). De-mographic and medical characteristics are presented in Table 1. The majority of patients suffered thermal mixed
Figure 1. Pain in burn site six months after injury Figure 2. Wound infection in acute trauma period and post recovery NRS score
EWMA Journal 2012 vol 12 no 1 34

2nd and 3rd degree burns covering 10-30% of total body surface area.
Of the 44 respondents, 68.2% of patients indicated that they are suffering from varied intensity of pain at the site of the burn constantly or once every day (Figure 1), but only 36.7% of them are taking analgesics. Sever-ity (depth and size) and cause (scalding, electrical, etc.) of burn trauma did not have any significant influence on chronic pain intensity. However, patients having ex-perienced wound infection in the acute trauma period indicated higher pain intensity. The intensity of chronic pain directly correlated with the infection of wound dur-ing the initial treatment period; NRS at rest (mean pain intensity±SD) 5.6±1.9 versus 1.9±1.6 (p=0.008, r=0.396) and NRS on movement 6.6±1.3 versus 3.4±1.7 (p=0.029, r=0.329), (Figure 2).
In addition, 51.6% of patients experience pain in skin donor site at six months post injury (mild pain indicated 29%, moderate 12.9%, severe 9.7% of patients).
Standard McGill Pain Questionnaires (Lithuanian version) were used for qualitative assessment of chronic pain manifestation. In these questionnaires, 86.3% of our patients indicated the emotional components of their pain: one quarter – fearful and one-third – tiring. Regarding the sensory components of pain, 84.38% of patients identi-fied descriptors of neuropathic pain such as hot burning (36.4%); gnawing – (29.5%) and tingling or `pins and needles` (20.5%) (Figures 3 and 4).
Medical Outcomes Study 36-Item Short Form Ques-tionnaires (SF-36) demonstrated good internal consistency (Cronbach’s a=0.7-0.9) among six subscales, except role limitations due to emotional problems subscale (a=0.69) and mental health subscale (a=0.6). Test-retest reliability coefficients ranged from 0.67 to 0.92.
Figure 3. Qualitative characteristics of chronic burn wound pain: sensory components (Standard McGill Pain Questionnaires (Lithuanian version))
Figure 4. Qualitative characteristics of chronic burn wound pain: emotional components (Standard McGill Pain Questionnaires (Lithuanian version))
Table 1. Summary demographic and medical information
Characteristics Number (percentage)
Demographic variables
Mean age at time of burn (SD) 51,3±16,8
Min-max 21-82
Men/women 30/14
Educational level
University 4 (9%)
High school 2 (4.5%)
Professional school 15 (34%)
Secondary 12 (27%)
Elementary 11 (25%)
Aetiology of burn
Flame and scalds 39 (89.7%)
Chemical 2 (4.5%)
Electrical 3 (6.8%)
Burn size (Total body surface area)
<10% 15 (34%)
11-30% 21 (47.7%)
31-50% 6 (13.6%)
>50% 2 (4.5%)
Degree of burns
Mixed 1st and 2nd degree 7 (15%)
Mixed 2nd and 3rd degree 23 (52.2%)
3rd degree 14 (31.8%)
Necrectomia/skin grafts
Yes 31 (70.5%)
No 13 (29.5%)
Length of hospital stay
<1 month 14 (31.8%)
>1 month 21 (47.7)
>2 month 6 (13.6%)
>3 month 3 (6.8%)
Science, Practice and Education
EWMA Journal 2012 vol 12 no 1 35

In the General Health subscale (a=0.76) 21 (48%) patients noted that their health is fair and 4 (10%) noted it as poor. Only 5 (12%) of burn survivors mentioned that their health at the moment of survey was excellent.
The Physical Functioning (Cronbach’s a=0.79) scale results showed 41% of respondents were limited a lot in vigorous activities (such as running, lifting heavy objects, participating in strenuous sports), 25% in moderate activi-ties (such as moving a table, pushing a vacuum cleaner, bowling, or playing golf), 25% in bathing or dressing, and 14% walking several hundred yards (Figure 5).
The Role Physical scale (Cronbach’s a=0.71) which measures how much health interferes with the ability to perform daily activities and normal work showed that more than a half (59%) of respondents had difficulties in working at their usual job during the recent four weeks.
About 57% of patients were limited in the kind of work they could do. (Figure 6).
The Bodily Pain subscale (Cronbach’s a=0.9) showed than 75% of patients suffered varied intensity of pain in the burn site during the recent four weeks. Also 43 (2%) of patients noted that post-burn pain was limiting their usual daily activity during the recent weeks; 20 (5%+) identified moderate limitation and 15 (9%+) identified quite a bit while 6 (8%) identified extreme limitation.
Social Functioning subscale (Cronbach’s a=0.72) re-sults reported that only 29, (5%), of respondents did not have any physical health or emotional problems interfering with social activities (like visiting friends, relatives, etc.) while 70 (4%) of patients were limited in social relation-ships due to poor well-being and emotional problems (Figure 7).
Figure 6. Role physical subscale
Figure 5. Physical functioning subscale: physical activity
EWMA Journal 2012 vol 12 no 1 36

DISCUSSIONChronic pain has been identified as a significant problem many years after burn recovery9. Our results show that chronic pain associated with burn trauma is a common problem even at the sixth month after the original injury. Pain experienced during acute post-burn hospitalisation has been well documented but subsequent pain has re-ceived little attention7. Choiniere et al. have presented prevalence data and quantitative descriptions of altered tactile, thermal, and pain sensibility in a cohort of adult patients with and without chronic pain after treatment. Their former patients had burns averaging 20% of total body surface. Of the 236 subjects, 86 (36%) reported pain one year or more after injury. The presence of pain cor-related with the severity of burns5,6. In the Dauber et al study, 52% of patients reported pain 12 years after injury. This finding may be explained by severity of burn injury (59% of patients suffered second plus third-degree burns)7. In our study the majority of patients (84%) had deep burns (second plus third-degree or third-degree) and 68.2% of patients reported chronic pain, but the degree of burns did not have any significant influence on chronic pain intensity for our patients. We found that patients with wound in-fections in the acute trauma period indicated higher NRS points post burn. There might be several causes of this finding – frequent wound debridement, dressing changes and strenuous physical and occupational therapy that re-quire manipulation of already inflamed tissue may contrib-ute to increase pain and inflammation in burn wounds9. This patient group often suffers unbearable pain that is difficult to control in the acute period. Although nocicep-tion and peripheral hyperalgesia are considered the major causes of burn pain, mechanisms like central hyperalgesia and neuropathic pain are important components not only in acute settings but after hospitalisation as well10.
The results of the current study indicate that about 51% patients felt pain in skin donor site six months post injury. According to Malenfant et al. the presence of this type of problem in burn patients is not surprising when one considers the nature of injury which damages underly-ing nerve structures, the kind of surgery carried out (skin grafting) and possible problems of the scarring process. Skin grafts and wound healing processes, which can affect the quality of reinnervation, along with the formation of hypertrophic scars may also account for diminished sen-sory function or appearance of some abnormal sensations6.
The present study was designed to provide data on the quantitative characteristics of burn-related chronic pain. It is important to mention that chronic burn-related pain has multidimensional faces; sensory and emotional com-ponents were noted together. Most subjects’ descriptions of the pain are consistent with the character of neuro-pathic pain. In the authors’ experience, this pain is often a significant complaint at long-term follow-up and affects the patients’ quality of life11,12. Our observational find-ings are in agreement with those presented in literature. However, literature is sparse on the topic of neuropathic pain in burn injury. In two studies examining a total of 534 burn patients, 71% and 82% reported paraesthetic sensations and 36% and 34% reported pain in the site of the burn scar5,6. Wong et al. found that pain experienced by burn survivors after wound healing had characteristics of neuropathic pain. Burn survivors described a change in the character of the pain they experience following wound healing. This pain had similar characteristics to the neuro-pathic pain that has been described in diabetic patients and in post-herpetic neuralgia13. Scheider et colleagues men-tioned that the first complaint of neuropathic-like symp-toms was at 4.3±0.5 months after injury and symptoms persisted for 13.1±2.2 months after injury11. An increased understanding of the physiological mechanisms underly-ing burn injuries will hopefully contribute to improving current analgesic practices and to the prevention and/or treatment of chronic sensory problems in burn patients13.
Patients’ quality of life is an increasingly important outcome measure in medicine and health care. Quality of life as an outcome variable is making a transition from a ‘biomedical model’ of health to one that incorporates the psychosocial aspects of disease4. In our study we in-vestigated the impact of chronic pain on health-related quality of life and daily activity. Determination of quality of life is often measured using the Burns Specific Health Scale (BSHS) or Quality of Life Questionnaire (QLQ). We used Medical Outcomes Study 36-Item Short Form Questionnaires (SF-36) for this study because SF-36 is more sensitive of the role physical, bodily pain, social func-tioning and role emotional subscales than the BSHS-B in burn patient population14. Baker et al. noted that physical
Figure 7. Social functioning subscale
Science, Practice and Education
EWMA Journal 2012 vol 12 no 1 37

functioning is represented more completely in the SF-3615. Based on the present study findings, it is concluded that burns affect patients’ overall quality of life. Burns also have a negative effect on most dimensions of quality of life including physical well-being, psychological health and bodily pain. Similar findings are reported by Ull-rich and colleagues: pain may contribute independently to compromised physical functioning8. These findings were supported by Kildal et al., who examined the health status in Swedish burn patients and found that the greatest negative impact on health and thereby the lowest mean domain scores were seen in the domains of heat sensitiv-ity, work and body image16. Further, Salvador et al., who examined the QOL of Spanish burn patients, found that burns represent a major problem with regards to impact on QOL and overall psychological health4,17.
CONCLUSIONThe study demonstrates that more than 60% of burn sur-vivors experience chronic pain in burn and 50% in donor sites six months after injury. The results indicate that the intensity of chronic pain correlates with the wound infec-tion rate during the acute period. Quality of life in patients experiencing post-burn pain is poor because of disrupted physical well-being, general health status and chronic pain. Mixed sensory-emotional components were indicated with chronic post-burn pain. m
References
1. Health Information Centre of Institute of Hygiene. Health Statistics of Lithuania 2009. www.hi.lt
2. Locar Z, Bras M, Mickovic V. The relationships between burn pain, anxiety and depression. Coll Antropol 2006;30(2):319-25.
3. Choiniere M. Burn pain: A unique challenge. Pain – Clinical Updates. International Association for Study of Pain IX, 2001.
4. Elsherbiny E, Salem M, El-Sabagh A. Quality of life of adult patients with severe burns. Burns 2011;37:776-89.
5. Choiniere M, Melzack R, Papillon J. Pain and paraesthesia in patients with healed burns: an exploratory study. J Pain Symptom Manage 1991;6(7):437-44.
6. Malenfant A, Forget R, Papillon J, Amsel R, Frigon JY, Choiniere M. Prevalence and characteristics of chronic sensory problems in burn patients. Pain 1996;67(2-3):493–500.
7. Dauber A, Osgood PF, Breslau AJ. Chronic persistent pain after severe burns: Survey of 358 burn survivors. Pain Medicine 2002;3:6-17.
8. Ullrich Ph, Askay Sh, Patterson R. Pain, Depression, and Physical Functioning Following Burn Injury Rehabil Psychol. 2009 May; 54(2): 211-216.
9. Gretchen J. Summer, Kathleen A Puntillo et al. Burn injury pain: The Continuing Challenge. The Journal of Pain 2007;8(7):533-548.
10. Cuignet O, Pirson J, Soudon O, Zizi M. Effects of gabapentin on morphine consumption and pain in severely burned patients. Burns 2007;33: 81-86.
11. Schneider J, Harris N, El Shami A. A descriptive review of neuropathic-like pain after burn injury. Journal of Burn Care Research 2006;27(4):525-28.
12. Coderre T, Choiniere M. Neuronal plasticity associated with burn injury and its relevance for perception and management of pain in burn patients. Pain Res Manage 2000;5(3):205-13.
13. Wong L, Turner L. Treatment of post-burn neuropathic pain: evaluation of pregabalin. Burn 2011;36:769-72.
14. Edgar D, Dawson A, Hankey G. Demonstration of the validity of the SF-36 for measurement of the temporal recovery of quality of life outcomes in burns survivors. Burn 2010;36:1013-20.
15. Baker Ch, Rosenberg M, Mossberg K. Relationships between the Quality of Life Questionnaire (QLQ) and SF-36 among young adults burned as children. Burns 2008;34:1163-68.
16. Kildal M, Andersson G, Gerdin B. Health status in Swedish burn patients. Assess-ment and utilizing three variants of the Burn Specific Health Scale. J Int Soc Burns Injury 2002;28(7):639-45.
17. Salvador-Snaz J, Scanchez J, Rodriguez-Marin J. Quality of life of the Spanish burn patient. J Int Soc Burn Injuries 1999;25:593-8.
Science, Practice and Education

Treatment of Venous Leg Ulcersin a new light.
Cutimed®
Discover an innovative rangeof wound management, medi-cal skin care and compressionproducts which reliably coverall stages of wound healing.Especially developed for the
successful treatment of chronic,difficult-to-heal-wounds, suchas venous leg ulcers, ourrange offers a complete selec-tion of effective and patient-friendly products.
On request, we will provide youwith further information onindications and treatmentoptions. Contact us: www.cutimed.com
A D VA N C E D W O U N D C A R E
Cutimed® PROTECT Cutimed® Sorbact® Cutimed® Siltec JOBST® Comprifore JOBST® UlcerCARE
Int_EWMA_AZ_RZ_Cutimed_advert 15.04.11 09:46 Seite 1

ABSTRACTS OF RECENT COCHRANE REVIEWS
Sally Bell-Syer, MSc
Managing Editor Cochrane Wounds Group
Department of Health Sciences
University of YorkUnited Kingdom
Conflict of interest: none
Publication in The Cochrane Library Issue 12, 2011
Infection control strategies for preventing the transmission of meticillin-resistant Staphylococcus aureus (MRSA) in nursing homes for older peopleCarmel Hughes, Michael Smith, Michael Tunney, Marie C BradleyCitation example: Hughes C, Smith M, Tunney M, Bra-dley MC. Infection control strategies for preventing the transmission of meticillin-resistant Staphylococcus aureus (MRSA) in nursing homes for older people. Cochrane Database of Systematic Reviews 2008, Issue 1 . Art. No.: CD006354. DOI: 10.1002/14651858.CD006354.pub2 . Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
ABSTRACTBackground: Nursing homes for older people provide an environment likely to promote the acquisition and spread of meticillin-resistant Staphylococcus aureus (MRSA), putting residents at increased risk of colonisa-tion and infection. It is recognised that infection pre-vention and control strategies are important in prevent-ing and controlling MRSA transmission.
Objectives: To determine the effects of infection pre-vention and control strategies for preventing the trans-mission of MRSA in nursing homes for older people.
Search methods: We searched the Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library 2011, Issue 2), the Cochrane Wounds Group Specialised Register (searched May 27th, 2011). We also searched Ovid MEDLINE (from 1950 to April Week 2 2011), OVID MEDLINE (In-process and Other Non-Indexed Citations, April 26th 2011) Ovid EMBASE (1980 to 2011 Week 16), EBSCO CINAHL (1982 to April 21st 2011), DARE (1992 to 2011, week 16), Web of Science (1981 to May 2011), and the Health Tech-nology Assessment (HTA) website (1988 to May 2011). Research in progress was sought through Current Clini-cal Trials (www.controlled-trials.com), Medical Research Council Research portfolio, and HSRPRoj (current USA projects).
Selection criteria: All randomised and controlled clini-cal trials, controlled before and after studies and inter-rupted time series studies of infection prevention and
control interventions in nursing homes for older people were eligible for inclusion.
Data collection and analysis: Two review authors inde-pendently reviewed the results of the searches. Another review author appraised identified papers and under-took data extraction which was checked by a second review author.
Main results: For this second update only one study was identified, therefore it was not possible to under-take a meta-analysis. A cluster randomised controlled trial in 32 nursing homes evaluated the effect of an infection control education and training programme on MRSA prevalence. The primary outcome was MRSA prevalence in residents and staff, and a change in infection control audit scores which measured adher-ence to infection control standards. At the end of the 12 month study, there was no change in MRSA preva-lence between intervention and control sites, while mean infection control audit scores were significantly higher in the intervention homes compared with con-trol homes.
Authors’ conclusions: There is a lack of research eval-uating the effects on MRSA transmission of infection prevention and control strategies in nursing homes. Rigorous studies should be conducted in nursing homes, to test interventions that have been specifically designed for this unique environment.
Plain language summary: Infection control strategies for preventing the spread of meticillin-resistant Sta-phylococcus aureus (MRSA) in nursing homes for older peopleMRSA is a bacterium that can cause infection in people, particularly those who are in hospital. MRSA is now becoming a problem for older people (residents) who live in nursing homes. Nursing homes are ideal places for MRSA to spread: the residents live close to each other, many have a number of medical conditions and may receive several prescriptions for antibiotics, and some may have pressure sores and medical devices such as catheters. All of these factors increase the risk of residents getting MRSA, and so increase their risk of dying. Many different ways of preventing the spread of MRSA have been studied, particularly in hospitals; however, we found only one study that looked at whether an infection control education and training programme influenced the spread of MRSA in nursing homes for older people. This study showed there was
EWMA Journal 2012 vol 12 no 1 40

EBWM
no difference between the group that was involved in the pro-gramme and the comparison group which continued with their normal practice.Although there is some evidence for techniques that work well to prevent the spread of MRSA in hospital, it is not clear if these approaches will work in nursing homes for older people. Further research is needed to establish what will work in nursing homes.
Support surfaces for treating pressure ulcersElizabeth McInnes, Jo C Dumville, Asmara Jammali-Blasi, Sally EM Bell-Syer Citation: McInnes E, Dumville JC, Jammali-Blasi A, Bell-Syer SEM. Support surfaces for treating pressure ulcers. Cochrane Database of Systematic Reviews, Issue . Art. No.: . DOI: .Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
ABSTRACTBackground: Pressure ulcers are treated by reducing pressure on the areas of damaged skin. Special support surfaces (including beds, mattresses and cushions) designed to redistribute pres-sure, are widely used as treatments. The relative effects of differ-ent support surfaces are unclear.
Objectives: To assess the effects of pressure-relieving support surfaces in the treatment of pressure ulcers.
Search methods: We searched: The Cochrane Wounds Group Specialised Register (searched 15 July 2011); The Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2011, Issue 3); Ovid MEDLINE (2007 to July Week 1 2011); Ovid MEDLINE (In-Process & Other Non-Indexed Cita-tions, July 14, 2011); Ovid EMBASE (2007 to 2011 Week 27); EBSCO CINAHL (2007 to 14 July 2011). The reference sections of included studies were also searched.
Selection criteria: We included published or unpublished ran-domised controlled trials (RCTs), that assessed the effects of support surfaces for treating pressure ulcers, in any patient group or setting, that reported an objective measure of wound healing.
Data collection and analysis: Data extraction and assessment of risk of bias were performed independently by two review authors. Trials with similar patients, comparisons and outcomes were considered for pooled analysis. Where pooling was inap-propriate the results of the trials were reported narratively. Where possible, the risk ratio or mean difference was calculated for the results of individual studies.
Main results: We identified 18 trials of support surfaces for pres-sure ulcer treatment, involving 1309 participants with samples sizes that ranged from 14 to 160. Of three trials comparing air-fluidized devices with conventional therapy, two reported signifi-cant reductions in pressure ulcer size associated with air-fluidized devices. Due to lack of reported variance data we could not rep-licate the analyses. In relation to three of the trials that reported significant reductions in pressure ulcer size favouring low air loss devices compared with foam alternatives, we found no signifi-cant differences. A small trial found that sheepskin placed under
the legs significantly reduced redness and similarly a small sub-group analysis favoured a profiling bed compared with a stand-ard bed in terms of the healing of existing grade 1 pressure ulcers. Poor reporting, clinical heterogeneity, lack of variance data and methodological limitations in the eligible trials meant that no pooled comparisons were undertaken.
Authors’ conclusionsThere is no conclusive evidence about the superiority of any sup-port surface for the treatment of existing pressure ulcers. Meth-odological issues included variations in outcomes measured, sample sizes and comparison groups. Many studies had small sample sizes and often there was inadequate description of the intervention, standard care and co-interventions. Individual study results were often inadequately reported, with failure to report variance data common, thus hindering the calculation of mean differences. Some studies did not report P values when reporting on differences in outcomes. In addition, the age of some trials (some being 20 years old), means that other technologies may have superseded those investigated. Further and rigorous studies are required to address these concerns and to improve the evidence base before firm conclu-sions can be drawn about the most effective support surfaces to treat pressure ulcers.
Plain language summary: Support surfaces for treating pressure ulcersPressure ulcers (also called pressure sores, decubitus ulcers and bed sores) are ulcers on the skin caused by pressure or rubbing at the weight-bearing, bony points of immobilised people (such as hips, heels and elbows). Different support surfaces (e.g. beds, mattresses, mattress overlays and cushions) aim to relieve pres-sure, and are used to cushion vulnerable parts of the body and distribute the surface pressure more evenly. Support surfaces are used alongside other treatments such as wound dressings to treat pressure ulcers and this review has reviewed studies that compared different types of support sur-face. Low-tech support surfaces included foam filled mattresses, fluid-filled mattresses, bead-filled mattresses, air-filled mat-tresses and alternative foam mattresses and overlays. High-tech support surfaces included mattresses and overlays that are elec-trically powered to alternate the pressure within the surface, beds that are powered to have air mechanically circulated within them and low-air-loss beds that contain warm air moving within pockets inside the bed. Other support surfaces included sheep-skins, cushions and operating table overlays. We are unable to draw any firm conclusions about the rela-tive effects of support surfaces for treating pressure ulcers because the evidence base is weak. Current trials have failed to provide robust evidence due to small sample sizes, poor report-ing of results and poor quality of study conduct and design. Further rigorously conducted research into the use of support surfaces for treating pressure ulcer surfaces is required. m
Use the EWMA Journal to profile your company
Deadline for advertising in the May 2012 issue is 1 March 2012
EWMA Journal 2012 vol 12 no 1 41

EWMA Journal Previous Issues
The EWMA Journals can be downloaded free of charge from www.ewma.org
Other JournalsThe section on International Journals is part of EWMA’s attempt to exchange information on wound healing in a broad perspective.
Helcos, vol. 22, no. 3, 2011
Hyperoxygenated fatty acid efectiveness in the prevention of the vascular ulcersVives Sanchez E, et al.Dystrophic calcification in leg ulcersChaverri-Fierro D, et al.Quality of life and healing in patients with venous ulcers of etiology. Validation of Charing Cross Venous Ulcer Questionnaire, Spanish version (CCVUQ-e) and the Pressure Ulcer Scale for Healing, Spanish version (PUSH-e). Preliminaty resultsGonzalez-Conseugra RV, et al.Transforming cavity wound care with Hidrofiber® technology ribbon dressingsSegovia-Gomez T, et al.
Spanish
Haava, no. 4, 2011www.shhy.fi
Skin Diseases with Ulceration Sanna PoikonenSkin Sarcoidosis – Ethiology of woundAnna Hjerppe Vasculitis and SkinJussi LiippoRare Bacterial Infections of SkinSakari VuorinenSystemic sklerossi – skleroderma Riitta LuosujärviEpidermolysis bullosa – rare, genetic blister disease of skinKaisa Tasanen-MäättäA Wounded young LadySanna KujalaWound Management of Necrotic FascitisHelvi HietanenCorticosteroid emulsions in the treatment of wound patient Sirpa Paananen
Finnish
Volume 10, no 3, October 2010
Rationale for compression in leg ulcers with mixed, arterial and venous aetiologyHugo PartschPressure ulcers in Belgian hospitals: What do nurses know and how do they feel about prevention?D. Beeckman, T. Defloor, L. Schoonhoven, K. Vanderwee Nutritional Supplement is Associated with a Reduction in Healing Time and Improvement of Fat Free Body Mass in Patients with Diabetic Foot UlcersP. Tatti, A.E. Barber, P. di Mauro, L. MasselliChronic wounds, non-healing wounds or a possible alternative?M. BriggsSilver-impregnated dressings reduce wound closure time in marsupialized pilonidal sinusA. Koyuncu, H. Karadaˇ, A. Kurt, C. Aydin, O. TopcuVenous leg ulcer patients with low ABPIs: How much pressure is safe and tolerable?J. Schuren, A. Vos, J.O. Allen,Adherence to leg ulcer treatment: Changes associated with a nursing intervention for community care settingsA. Van Hecke, M. Grypdonck, H. Beele, K. Vanderwee, T. DefloorA Social Model for Lower Limb Care: The Lindsay Leg Club ModelM. Clark
Acta Vulnologica, vol. 9, no 3, 2011www.vulnologia.it
Nutritional treatment in patients with pressure ulcersBenati G., et al.Home care treatment for chronic skin wounds: A controlled study of treatment with advanced dressings alone versus combination negative pressure therapy and advanced dressingsOrsatti V., et al.Management and treatment of pressure ulcers in hospitalized neurological patients and ambulatory patientsFamà F., et al.Efficacy of 0.05% sodium hypochlorite isotonic solution versus 10% povidone-iodine in postoperative wound cleaning and disinfectionDi Vita F., et al.
Italian
Volume 11, no 1, January 2011
Who will take onAli Barutcu, Aydin O. Enver, Top Husamettin, Violeta Zatrigi Diabetic foot ulcer pain: The hidden burdenSarah E Bradbury, Patricia E PriceThe reconstructive clockwork as a 21st century concept in wound surgeryKarsten Knobloch, Peter M. VogtAnaemia in patients with chronic woundsLotte M. Vestergaard, Isa Jensen, Knud Yderstraede A survey of the provision of education in wound management to undergraduate nursing studentsZena Moore, Eric ClarkeCaring for Patients with Hard-to-Heal Wounds – Homecare Nurses’ NarrativesCamilla Eskilsson
Volume 11, no 2, May 2011
The fight against biofilm infections: Do we have the knowledge and means?Klaus Kirketerp-Møller, Thomas Bjarnsholt, Trine R. ThomsenBiofilms in wounds: An unsolved problem?António Pedro FonsecaDiabetic foot ulcer pain: The hidden burdenSarah E Bradbury, Patricia E PriceTopical negative pressure in the treatment of deep sternal infection following cardiac surgery: Five year results of first-line application protocolMartin ŠimekWounds Research for Patient Benefit: A five year programme of research in wound careKaren Lamb, Nikki Stubbs, Jo Dumville, Nicky Cullum
Volume 11, no 3, October 2011
Challenges facing district nurses in the prevention of pressure ulcersLynne Watret Clinical application of stem cells in wound healing: A near future?Benoit I HendrickxUnderstanding the Patient Experience: Does empowerment link to clinical practice?Patricia PriceThe Influence of Egyptian Propolis on Induced Burn Wound Healing in Diabetic Rats – Antibacterial MechanismEmad T. Ahmed, Osama M. Abo-Salem, Ali OsmanPURSUN UK: The Pressure Ulcer Research Service User Network for the UKDelia MuirPerspective of the European Patients’ Forum Developing CollaborationNicola Bedlington
Advances in Skin & Wound Care, vol. 25, no 1, 2012www.aswcjournal.com
Eradication of Methicillin-Resistant Staphylococcus aureus in Pressure Ulcers Comparing a Polyhexanide-Containing Cellulose Dressing with Polyhexanide Swabs in a Prospective Randomized StudyT. Wild, et al.Systematic Review and Meta-analysis on the Use of Honey to Protect from the Effects of Radiation-Induced Oral MucositisJ. J. Song, P. Twumasi-Ankrah, R. SalcidoEstimates of Evaporation Rates from Wounds for Various Dressings/Support Surface CombinationsC. Lachenbruch, C. VanGildeExploring the Effects of Pain and Stress on Wound HealingK. Y.Woo
English
EWMA Journal 2012 vol 12 no 1 42

EWMA
Wounds, vol. 24, no 1, 2012 www.woundsresearch.com
Benchmarking Chronic Wound Healing OutcomesLaura L. BoltonWound Care Outcomes and Associated Cost Among Patients Treated in U.S. Outpatient Wound Centers: Data From the U.S. Wound RegistryC. E. Fife, M. J. Carter, David Walker, Brett ThomsonProducing Precise Outcomes in Randomized Controlled Trials and Clinical StudiesFinn Gottrup, Jan Apelqvist, Patricia Price Diagnostic Dilemmas: Malignant Melanoma Misdiagnosed as a Diabetic Leg Ulcer – A Case Report and ReviewAlper Ata, Ayse Polat, Faith Tanrıverdi, Ali Arıcan
English
Wund Management, vol. 6, no 1, 2012 English abstracts are available from www.mhp-verlag.de
Self management of patients – theoretical background D. von Siebenthal „Giving patients a voice“ – leg clubs®: the organizational implementation of self management in wound care A. Uschok … to regain hope … – a case studyC. Settelen, B. Egger, I. A. Frei Self-Management – Only the informed patient can actively support his own care and treatmentM. Manteufel, C. Hampel-Kalthoff Integration of measures for promoting self-care competency in everyday life – Compromises as the key to successK. Lustig
German
Wound Repair and Regeneration, vol. 20, no 1, 2012 www.wiley.com
Benefit evaluation in the therapy of chronic wounds from the patients’ perspective –development and validation of a new methodMatthias Augustin, et al.Tissue-engineered provisional matrix as a novel approach to enhance diabetic wound healingSwathi Balaji, et al.Early and late calcium waves during wound healing in corneal endothelial cellsSilvia Chifflet, et al.Tumor necrosis factor-alpha (TNF-a) is a therapeutic target for impaired cutaneous wound healingGillian S. Ashcroft, et al.
English
Wounds (SÅR) vol. 19, no 4, 2011www.saar.dkManaging pain and stress by wound treatmentClifford Richardson, Dominic UptonMethods for cleaning and debridement of wounds – experiences with Debrisoft®
Wilja Dam, Connie Winther, Gitte Susanne RasmussenTesting heel relievement DecuheelSusan Bermark, Britt WahlersDiabetes Café – Group Guidance of diabetic patients and relativesCharlotte Brink Andersen
Scandinavian
Journal of Wound Care, vol. 21, no 1, 2012www.journalofwoundcare.com
Optimum microcurrent stimulation intensity for galvanotaxis in human fibroblastsM. Sugimoto, et al.Comparison of PHMB-containing dressing and silver dress-ings in patients with critically colonised or locally infected woundsT. Eberlein, et al.An open label non-comparative case series on the efficacy of an enzyme alginogelC.M. DuranteClinimetrics of tristimulus colourimeters in scar assessment: a review of evidenceH.G. JonesCryoglobulinaemic leg ulcers associated with transient ischaemic attackAltunay, B. Ates, G. Atis, O. Ton
English
Phlebologie, no 6, 2011www.schattauer.de
Chronical wound managementH. Diener and K. Herberger, M. Augustin, ES DebusNew multi-resistant bacteria in wound careS. Reich-Schupke; M. StückerOrganizational structures of modern wound care Institutional structures of modern wound careH. Diener and K. Herberger, A. Larena-Avellaneda, A. Kieback, M. Radtke, M. Augustin, P. Pohlenz and R. Schmelzle, ES DebusRefractory leg ulcers et pedis with grotesque deformityH.-J. Hermann, A. Hermann, P. Waldhausen“3D image” for determination of lower leg volume compared to water plethysmography S. Kauder, A. Strolin, A. Adamczyk, M. Krug, H.-M. HaefnerEulogy for Ratschow MedalE. RabeSkin, veins, and legsHAM NeumannSurgical Lymphology. Part 4: Preparation of the paradigm shift in secondary LyphödemM. Cornely
English
Journal of Tissue Viability, vol. 21, no 1, 2012www.journaloftissueviability.com
Reflections of a Challenging yearDan BaderWhat influences the impact of pressure ulcers on health-related quality of life? A qualitative patient-focused exploration of contributory factorsGorecki C.The value of frozen section biopsy in diagnosing necrotizing fasciitis: Proposal of a new grading systemStegeman Sylvia A.Iterative Design And Testing Of A Hand-Held, Non-Contact Wound Measurement Device.Sprigle StephenA Simple Stochastic Model To Explain The Sigmoid Nature Of The Strain-Time Cellular Tolerance CurveGefen Amit
English
NTVW vol. 6, no 12, 2011www.ntvw.nl
SpearPoints in Woundcare.1st National Dutch Multidicsiplinary congres for Woundcare professionals
Cick/off multi center study new treatment for patients with extreme lymphedema, using short stretch bandages and tubular under padding, first poster presentation EWMA 2011
Woundcare Center Evean essential for the direction of care
Prevention of incontinence related dermatitis
Dutch
Lietuvos chirurgija, vol.9, no 4, 2011www.chirurgija.lt
Sensitized treatment and diagnostics of advanced breast cancerBloznelyte-Plesniene L, et al.Breast preserving surgery and results of combined treatmentOstapenko V, et al.Laparoscopic colon cancer surgery in elderly patientsMiliauskas P, et al.Hand-assisted laparoscopic colorectal surgery via transumbilical incisionBrazyte V, et al.Preemptive analgesia in colorectal surgeryTikuisis R, et al.The value of autofluorescence bronchoscopy in the diagnosis of early lung cancerZaremba S, et al.
Lithuanian
International Wound Journal, vol. 8, no 6, 2011www.wiley.com
Antimicrobial sutures and prevention of surgical site infection: Assessment of the safety of the antiseptic triclosanD. Leaper, et al.Diabetic foot infections: Microbiological aspects, current and future antibiotic therapy focusing on methicillin-resistantStaphylococcus aureusA. Ambrosch, et al.Prevention of pressure ulcer: Interaction of body characteristics and different mattressesT. Moysidis, et al.The experience of patients with lymphoedema undergoing a period of compression bandaging in the UK and Canada using the 3M™ Coban™ 2 compression systemPA. Morgan, et al.
English
EWMA Journal 2012 vol 12 no 1 43

Franz Trautinger
President of the Austrian Wound
Association (AWA)
The Austrian Wound Association AWA was founded in 1998 and is a non-profit asso-ciation active in the field of wound treat-
ment. It is composed of members from both the medical and nursing sector (241 members, 127 from nursing, 111 doctors, 3 from other sectors; 13 contributing members and one corresponding member: Finn Gottrup).
AWA wants to promote scientific research and in-formation exchange in the field of modern wound treatment. Treatment options for acute and chronic wounds of any cause are to be researched and developed further. The AWA considers it its duty to strive for improved cooperation between medical and nursing treatment. Innovative de-velopments and new treatment methods should therefore bene fit patients quicker.
It is the association’s aim, besides informing and advising doctors and nursing staff, to provide the general public with a better understanding of the possibility of active and preventive measures in wound treatment. Information events and train-ing initiatives for healthcare personnel are used to pass on knowledge to specialists and laymen.
AWA see the key points of their activity as being:n Support of scientific research in the field of
wound treatment (annual two-day congress with a prize ceremony)
n Communication of new findings, discoveries and developments in wound treatment (e.g. EWMA project on Diabetic Foot Syndrome, seminar on venous ulcers and on compres-sion therapy)
n Public relations through press conferences, this year’s focus is on amputation. Announcement of the AWA press prize, to be awarded for the first time this year, should give due credit to the importance of medical press reports on the topic of wound healing.
n Cooperation with industry in the further development of wound care products
n Networking with associated organisations in Austria involved in wound management, with the aim of achieving a stronger, single voice in national and international issues, whilst respecting special or regional concerns and responsibilities.
n Advanced and specialist training for doctors and nursing staff as well as for interested groups (§64 “Wound management“ ad-vanced and specialist training course organ-ised by the Hospitals Association together with the AWA, for nursing staff and doctors from all sectors; recently also ÖÄK (Austrian Medical Association) certificate for medical wound treatment in cooperation with the Austrian Academy of Physicians).
n Establishment of standards/guidelines in wound treatment (e.g. guidelines for venous ulcers)
n Promotion of awareness of preventive and active wound treatment measures
To fulfil this goal on a global level, AWA cooperates with national and international part-ner associations. We believe that fostering interdisciplinary col-laboration to deliver optimum patient care and state-of-the-art treatment will significantly im-prove patients’ quality of life and simultaneously help to contain costs. m
The Austrian Wound Association
EWMA 2012
23-25 May
ienna
EWMA
AWA
Arja Riegler
Vice President of the Austrian Wound
Association (AWA)
www.a-w-a.at
EWMA Journal 2012 vol 12 no 1 44

ienna · Austria · Österreich
Organised by the European Wound Management Association in cooperation with Die Österreichische Gesellschaft für Wundbehandlung AWA (Austrian Wound Association)
Organisiert von: der Europäischen Wound Management Organisation in Zusammenarbeit mit der Österreichische Gesellschaft für Wundbehandlung, AWA
WWW.EWMA.ORG / EWMA2012
22nd Conference of the European Wound Management Association22. Kongress der European Wound Management Association
EWMA 201223-25 May / Mai · 2012
Bilingual:
English & German
Zweisprachig:
Englisch & Deutsch
WOUND HEALING – DIFFERENT PERSPECTIVES, ONE GOAL
WUNDHEILUNG – UNTERSCHIEDLICHE PERSPEKTIVEN, EIN ZIEL
Early registration deadline 15 March 2012. For more information about the programme, registration etc. please visit www.ewma2012.org

Summary: The Austrian Society of Surgery, in cooperation with the Austrian Wound Association (AWA) is creating a register in which all major amputations are recorded throughout Austria. It is primarily intended for quality assurance purposes and is not just urgently necessary for collecting data on the actual situation but should also be the basis for creating clinical pathways or algorithms for the indication of major amputations. It would also be an ideal tool for harmonising and ensuring rehabilita-tion after leg amputation. Key words: Amputation register – Diabetic Foot Syndrome – major amputation – peripheral vascular disease
WHy DO WE NEED AN AMPUTATION REGISTER?For patients with Diabetic Foot Syndrome (DFS) and/or peripheral vascular disease (PVD), the mortality rate after major amputation of a lower extremity is around 30%. Suitable measures such as revascularization or limb-saving surgical pro-cedures can reduce this figure. The number of major amputations in Austria rose by 10.62 % between 2002 and 2006, which corresponds with an increase in the amputation rate from 29 to 32 amputations per 100,000 general population. In absolute figures this represents an increase from 2316 to 2562 amputations per year. These figures are based on those provided by “Statistik Austria“, an independent, non-profit seeking Federal Insti-tution with public rights, responsible for official statistics tasks in Austria such as census, collection, analysis and publication of official statistics1. So-called “individual medical services”: lower limb amputation – knee disarticulation – upper limb amputation were used as a reference. Diagnos-tic classification is not possible as this does not appear in the statistics. Furthermore, figures can only be recorded for operations and not for pa-tients, as “reamputation” is not recorded either. Approximately 60%, i.e. 19 amputations/100,000 general population, could be patients with DFS. In Germany, this patient population is thought to be 32/100,000 general population, compared to 6-11/100,000 general population for the whole of
the UK. Neither of these two countries has precise data available, but also only estimated values2.
As the data provided by Statistik Austria sheds no light on the cause, underlying illness, length of stay etc., a nationwide register in Austria could in the first instance collect data on the actual situ-ation. Valid data for patients with DFS could thus be available for the first time. One of the goals of the St Vincent Declaration signed in 1989 was to reduce the amputation rate by 50% for DFS. This has not yet been demonstrably achieved as concrete figures are still missing. Austria co-signed this declaration of intent at that time. In Austria, special wound and foot out-patient clinics have only been set-up in a few individual departments compared to other EU countries. In the Austrian state of Styria, a disease manage-ment programme: Therapie Aktiv – Diabetes im Griff (Active therapy – Diabetes under control) has been implemented since 2009 under which foot out-patient clinics have been set-up in sev-eral hospital departments in Styria since Novem-ber 2009.3 Data or results are not yet available. Patients with problematic wounds are primarily treated in hospital out-patient clinics which are not specially equipped and are externally largely looked after by independent carers.
Interdisciplinary work groups have been estab-lished in many operative areas and their action has contributed to quality improvement through the use of multi-modular therapy concepts. By way of example, the set-up of a multi-disciplinary tumour board should be mentioned here, as is already standard in all specialist centres.
Multidisciplinary cooperation in vascular medicine, in the treatment of Diabetic Foot Syn-drome (DFS) or chronic wounds has led to qual-ity improvement and a considerable reduction in amputation rates in the institutions where it has been implemented so far4. A register has existed in Denmark since 1972 and one is currently being established in Germany5,6.
Gerald ZöchUniv. Prof. Dr.
Plastic, Reconstructive and Aesthetic Surgeon
Austrian Society of Surgery (OGC) and
Austrian Wound Association (AWA)
EWMA Congress President
2012
The Amputation Register Project by the Austrian Society of Surgery and the Austrian Wound AssociationEWMA 2012
23-25 May
ienna
EWMA Journal 2012 vol 12 no 1 46

In Austria, vascular care in general and vascular sur-gery treatment in particular are currently only limited to a few centres. The development of centres with a high number of cases and thus improved results is to be gener-ally welcomed. This makes it possible to combine what is feasible and reasonable. Vascular care in this country is deficient in two areas: there is a lack of therapeutic valence, but what is even worse, is that reasonable and established procedures – both endovascular and open surgical proce-dures – are frequently not even offered to patients. This is mainly due to a lack of knowledge and awareness of the possibilities available.
CURRENT SITUATION:Each medical society in Austria (surgery, plastic surgery, orthopaedics and AWA) has delegated an authorised rep-resentative. This board has defined targets and drafted a model as a basis for documentation. The first meetings have already been held with representatives from the qual-ity assurance department of the Austrian Federal Ministry of Health. The data collected from the respective hospital departments is to be stored centrally, together with in-dividual service coding so that they can be linked. The institution responsible for centralised data collection has the necessary special data protection programmes. Analysis can then be anonymous.
CONCLUSION:The declared target remains quality management or rather assurance. Collection of data, which is relevant to health policy (e.g. use of preventive medical check-ups, diabetes education courses etc.), and the effects on the care situa-tion in Austria (how many care cases could be avoided?) would make it possible to answer several health econom-ics questions. It is not merely a matter of reducing the amputation rate but also of ensuring patients’ quality of life after an unavoidable amputation. Establishment of an amputation register for Austria would offer the unique possibility of recording the actual situation with major amputations and the reasons which have led to them.
The patient’s outcome after the loss of a limb could also simultaneously be recorded. The actual requirement and the related potential with regard to the reduction of major amputations in Austria could thus be evaluated.
The introduction of a special amputation register would therefore primarily serve quality assurance. It would be the basis for creating clinical pathways or algorithms for the indication of major amputations. m
References
1. www.statistik.at
2. Greiteman B, Bork H, Brückner L, Hrsg., Rehabilitation Amputierter. Stuttgart: Genter 2002
3. http://diabetes.therapie-aktiv.at
4. Deutsche Gesellschaft für Gefäßchirurgie. Leitlinie zur amputationsbedrohten Extremität. Deutscher Ärzteverlag Köln, 1998
5. Ebskov B: The Danish amputation register 1972-1984. Prost Orth Int; 1986
6. Tigges W, Debus ES: Zweitmeinung und Amputationsregister – Instrumente für eine Reduktion der Majoramputationen in Deutschland?. WundM 2009
EWMA
To request a free sample, demo DVD, or CD please visit
www.heelift.com/j
Anatomy of a Heelift®
Extended stitching along top rim supports the forefoot
Ventilation holes allow added air circulation
Affixed pad lifts the leg to suspend the heel
Available in smooth and convoluted foam interiors
Tricot covered stiffener maintains the boot’s structure while the friction-free material allows the boot to easily slide across bed sheets
Soft adjustable straps secure the boot in place
Beveled fixed pad reduces pressure on calf
Heelift® Patent No. 5,449,339 & 7,458,948. © 2012, DM Systems, Inc. All rights reserved. EWMA
Designed for the prevention and treatment
of heel pressure ulcers.
• Forefoot support to prevent foot drop
• Three sizes to ensure a proper fit
• Washable/autoclavable
The soft foam design and spare elevation pad make it easy to
customize the Heelift to meet a patient’s unique needs.
• Relieve pressure on the Achilles tendon or ankle
• Control hip rotation
DARCO (Europe) GmbH
Gewerbegebiet 18, 82399 RaistingTelefon +49 (0) 8807.9228-0Fax +49 (0) [email protected]
Global:Europe:1316 Sherman Ave. Evanston IL 60201Phone +1 847 328 9540Fax +1 847 328 [email protected]

BACKGROUNDVarious studies conclude that if diabetic foot patients receive early and appropriate treatment, amputation rates are reduced, life expectancy prolonged and long term health care spending reduced. Basic principles of “best practice” diabet-ic foot care related to prevention, education and treatment are well described in the international guidelines on the diabetic foot (The IWGDF con-sensus guidelines – latest updated 2011).
However, examples on national implementa-tion of the guidelines in Austria are few and ac-cess to “best practice” standards of care remains a challenge for many diabetic foot patients. The first step towards implementation of “best prac-tice” care standards in Austria is to identify the implementation barriers and concurrently ensure that policy makers and politicians recognise and agree to overcome these barriers.
THE PROJECT The “Austrian Diabetic Foot Project” is being planned by AWA (Austrian Wound Association) and EWMA who, in collaboration with local and international diabetic foot experts, will work ac-tively for national implementation of the diabetic foot consensus guidelines.
This will be done through supporting and initiating a series of analyses highlighting the po-tential benefits of implementing nationwide “best practice” standards of care and identifying current implementation barriers. To achieve real impact these activities will be combined with targeted policy level advocacy initiatives.
Ultimately the Austrian Diabetic Foot Project will contribute to system level initiatives towards establishing a sufficient number of multidiscipli-nary diabetic foot clinics, ensuring that diabetic foot clinical guidelines and standardised referral guidelines are made available and that reimburse-ment supporting diabetic foot care is being pro-vided.
THE AUSTRIAN DIABETIC FOOT SyMPOSIUM DURING EWMA 2012One of the advocacy activities being planned is a ½-day symposium during the EWMA confer-ence, scheduled to take place on Thursday 24 May 2012.
Here, the current treatment situation in Aus-tria will be described and the benefits in terms of achieving better treatment outcomes and health economic savings if multidisciplinary treatment structures, as recommended in the international consensus guidelines, are being implemented will be highlighted.
On this occasion central stakeholders from patient organisations as well as policymakers and politicians, will be invited to take part in a panel discussion aiming to discuss how current obsta-cles for implementation of “best practice” care can be removed and pointing out future strate-gies towards achieving better standards of care for diabetic foot patients in Austria.
Participation requires as a minimum a full day conference registration; further information and registration at the conference web pagewww.ewma2012.org
PROJECT COLLABORATORS, TIMEFRAME AND FINANCING In addition to representatives of AWA and EWMA, the Austrian Diabetic Foot Project steer-ing group integrates highly respected Austrian and international experts on the diabetic foot repre-senting groups such as the Diabetic Foot Study Group (DFSG) and the International Working Group on the Diabetic Foot (IWGDF). This ensures that the project has access to a valuable combination of strong international experience as well as thorough insight in the Austrian con-textual setting.
The project is planned to be carried out in 2012 with financing currently being sought from Austrian funding sources as well as from unre-stricted educational grants from industry partners. m
Prof. Dr. Gerald Zöch Generalsekretär AWA
Prof. Dr. Thomas PieberAustrian representative
in the IWGDF
Dr. Jan Apelqvist EWMA President
EWMA 2012
23-25 May
iennaDiabetic Foot Activities in Austria
EWMA
EWMA Journal 2012 vol 12 no 1 48

Are You Doing Everything
You Can For Your Patients?
Heal Chronic Wounds - Completely.
For more information or to schedule your evaluation visit us at www.aotinc.net or email us at [email protected]
w w w . a o t i n c . n e t
Greater than 80% Wound Closure Rate Unprecedented closure rates in various stage 2, 3 and 4 wounds.
Stimulates Angiogenesis and Collagen ProductionSignificantly increases indigenous growth factors stimulating angiogenesis, capillary budding and collagen production.
Infection ControlEffectively eliminates wound pathogens including; Staphylo-coccus Aurous, Streptococci, Pseudomonas Aeruginosa and MRSA.
Significant Pain ReductionRapid reduction in wound related pain by over 75% within 3-4 weeks of commencing treatment.
Non Invasive Safe TherapyEasily applied and integrated into any Acute, Long Term and Home Care setting.
Cost Savings Less labor intensive and less costly then Negative Pressure Wound Therapy (NPWT). The ability to reduce healing times and complications can lead to significant cost savings.

Since the EWMA 2009 Helsinki conference, EWMA has actively supported the estab-lishment of wound care societies in Russia
and in the neighbouring countries of Belarus and Ukraine, where Russian is also widely spoken. The national processes taking place have so far led to the establishment of wound care associations in both Belarus and Ukraine and in Russia creation of an association is currently underway.
At the request of the EWMA Council, since 2009 Rytis Rimdeika has undertaken the role of EWMA representative in contact with the new associations.
RUSSIAN SyMPOSIUM AT EWMA 2012 VIENNADuring the 2012 Vienna conference, EWMA and the Austrian Wound Association (AWA) will offer a Russian Symposium with simultaneous Russian and English translation.
The full-day symposium on Wednesday 23 May 2012 will pay specific attention to Russian speaking physicians, specialist nurses and other persons interested in wound care.
The symposium offers high level scientific presentations, networking and possibilities for exchange of experiences and evaluation of clini-cal practices. For a list of the symposium scientific committee and the preliminary programme please see below.
Further, on Thursday 24 May 2012, selected key sessions and satellite symposia of the EWMA Conference will also offer simultaneous transla-tion from English into Russian and German.
Registration for the symposium is open through the www.ewma2012.org website, where the final programme of the Russian Symposium will also be available.
OTHER EWMA ACTIVITIES IN SUPPORT OF THE WOUND CARE ASSOCIATIONS IN THE REGIONEWMA continues its activities in support of the emerging wound associations in Russia, Belarus and Ukraine with the objective of contributing to raising awareness with physicians, nurses, de-cision-makers and the general population of the problem of chronic wounds and the treatment practices available.
Rytis Rimdeika, MD PhD
Member of the EWMA Council,
President of Lithuanian Wound Management Association (LWMA)
Robert Strohal MD, Ass. Professor
Member of the EWMA Council,
Vice-President of Austrian Wound
Association (AWA)
Russian Spoken Symposium:
Symposium at EWMA 2012 and other activitiesEWMA 2012
23-25 May
ienna
23 May 201212:30-15:.00 Theoretical session:
Specific topic of relevance in particular to clinicians from Belarus, Russia and Ukraine
15:00-15:30 Coffee Break15:30-16:30 Theoretical session:
– Evidence based knowledge in Wound Care– How to make a Poster and Oral Presentation
16:45-18:00 Theoretical session: Specific topic of relevance in particular to clinicians from Belarus, Russia and Ukraine
18:00-19:00 Round table discussion19:00-19:30 Networking event
24 May 2012Selected sessions on Thursday 24 May will offer simultaneous translation English/German/Russian
Russian Symposium Scientific Committee
Rytis Rimdeika (EWMA), Chair
Robert Strohal (EWMA), Chair
A. G. Baindurashvili (Russia)
A. A. Alekseev (Russia) P. G. Kozinets (Ukraine)
L. Rubanov (Belarus) O. Stasevich (Belarus)
E. J. Fistal (Ukraine)
RUSSIAN SyMPOSIUM AT EWMA 2012 VIENNA · PRELIMINARy PROGRAMME
EWMA Journal 2012 vol 12 no 1 50

Since 2009 EWMA has been represent-ed at the national conferences of the Soci-ety for the Treatment of Wounds (STW) Belarus (March 2010 and 2011), and the Ukraine Wound Treatment Organisation (UWTO) (November 2010 and Septem-ber 2011). Likewise, key representatives of the associations in Belarus and Ukraine have participated in the EWMA confer-ences in 2010 and 2011.
Both associations are now registered as EWMA Cooperating Organisations and have, as such, access to organisational support and advice from EWMA, whose representatives maintain a continuous con-tact with key clinical stakeholders in the countries in the region.
FUTURE PERSPECTIVESBased on the experience from the Russian Symposium now being planned EWMA will consider also holding a Russian Sym-posium during the EWMA 2013 Copen-hagen conference.
Further, in 2012, an attempt will be made to secure financial support for wound care association development in the region from the Nordic Council of Ministries’ “Support Programme for NGOs in the Baltic Sea Region”.
From the long term prospective, EWMA will continue to work with the new as-sociations in establishing activities which will emphasise the importance of wound care, and wound care organisations in the region.
Such activities could include participa-tion of groups of nurses and physicians in the EWMA UCM training programme (see www.ewma.org/english/education/ewma-ucm.html), which runs during the EWMA conference, as well as support for specific wound care meetings and seminars in Russia and across the region. m
Russian Spoken Symposium:
Symposium at EWMA 2012 and other activities
EWMA
On November 1st 2011, Professor Finn Gottrup and Chair of EUCOMED Advanced Wound Care Sector Group (AWCS) Hans Lundgren met with Vittorio Prodi, member of the European Parliament.
MEP Prodi is very concerned with wounds and under-stands the constraints wounds have on patients and the health care system across Europe. He is dedicated to bringing this matter forward within the EU agenda and pushing for a higher understanding of the impact of wounds on patients and society in general.
In 2012, MEP Prodi will seek to influence the European Commission as well as highlighting the work of EWMA and thereby try to better the conditions for health care professionals working with wounds and thus also improving the situation for patients with wounds.
This was the fourth time that EWMA has meet with MEP Prodi and he was very pleased to host the visit. MEP Prodi is keen to maintain and develop the positive relationship which EWMA and AWCS have achieved with him.
Meeting with MEP Vittorio Prodi
Hans Lundgren, EUCOMED AWCS, MEP Vittorio Prodi and Finn Gottrup, EWMA
EWMA Journal 2012 vol 12 no 1 51

The 3rd Diabetic Foot Course, “Manage-ment of the Diabetic Foot”, was held in Pisa, Italy, 3-6 October 2011.
The course, which is endorsed by the Inter-national Diabetes Federation (IDF) and by the European Wound Management Association (EWMA) follows the experience of the national courses that in Pisa in 15 years trained more than 600 health professionals.
The key objectives of the course were - firstly, to increase the knowledge and operative skills in the management of the diabetic foot; secondly, to support the establishment of multidisciplinary diabetic foot clinics or departments based on the recommendations of the International Consensus Document, and thirdly, to facilitate international consensus on structure of treatment of the diabetic foot.
The course structure aimed to combine theory with practical training. Theoretical lectures were held in the mornings and practical sessions were held in the afternoons at the specialised diabetic foot clinic at the University Hospital of Pisa. By combining lectures from different specialists and
training in the clinic, the aim of the course par-ticipants was to gain insight in both the up-to-dated pathogenetical, diagnostic and therapeutic theoretical basis of this complex pathology and the practical methods and strategies of a team which works in a highly specialised centre with 20-year experience.
Practical training encompassed all the aspects of the modern approach to Diabetic Foot, includ-ing a live session of endovascular revascularization casted from the cath-lab of the interventional ra-diology section of the University Hospital of Pisa.
The course finished with a two hour long direct transmission from the clinic, where Alberto Pi-aggesi and his staff carried out two operations, on which three faculty members commented and discussed as they happened.
The participants in the course included clinicians from various professions such as endocrinologists, vascular and orthopaedic surgeons, specialised nurses, chiropodists, podiatrists and other health care professionals involved in the management of the Diabetic Foot.
Alberto PiaggesiMD, Professor,
EndocrinologistDirector of the
Diabetic Foot Section of the Pisa University
HospitalDept of Endocrinology
and MetabolismUniversity of Pisa
Pisa, Italy
Course organiser
Conflict of interest: none
Pisa International Diabetic Foot Course 2011
Participants and faculty members in the 2011 Course
EWMA
EWMA Journal 2012 vol 12 no 1 52

This 4 day theoretical course & practical training gives participants a thorough intro-duction to all aspects of diagnosis, manage-ment and treatment of the diabetic foot.
Lectures will be combined with practical sessions held in the afternoon at the diabetic foot clinic at the Pisa University Hospital.
Lectures will be in agreement with the International Consensus on the Diabetic Foot & Practical Guideline on the Management and Prevention on the Diabetic Foot.
·COURSE ENDORSED BY
·
EUR
OPEAN
· WOUND ·MANAGEMENT· A
SSO
CIA
TIO
N
This course is endorsed by EWMA.
Management ofthe Diabetic FootTheory & Practice4 Day Course, 8 - 11 October 2012Pisa, Italy
www.diabeticfootcourses.org
In all 34 participants from 18 different countries, 11 inter-national faculty members and 12 national faculty members took part in the 2011 course. The occasion of sharing this experience in such a close context, with many of the most recognized international experts in a most interactive way characterized the courses and is something unique in the field of DF.
An evaluation survey and general comments during the course suggest great satisfaction with the outcome of the course, especially emphasising the combination of practice and theory. The participants found the theoretical lectures very interesting. Likewise the practical hands-on sessions were very popular, giving the participants new angles to their fields. Finally the course provided an excellent forum for the exchange of knowledge, ways to handle the prob-lems in the field of diabetic foot, and discussions among the participants and with the faculty. Hopefully the par-ticipants gained a lot of knowledge which they can apply to their own fields in their own countries.
The 4th Diabetic Foot Course will be held in Pisa 8-11 October 2012. Further information is available on www.diabeticfootcourses.org or by contacting the Course Secretariat: [email protected] m
The course structure aimed to combine theory with practical training.
EWMA Journal 2012 vol 12 no 1 53

EWMA
Author: Stephen Thomas.Medetec Publications, Cardiff. 2010.708 pages.Cost unknown.
This book brings together the history, de-velopment of, information and evidence for wound dressings, providing a technical guide to dressings. The main body of the text comprehensively covers the composi-tion of and physical properties related to 13 types of dressings and wound interven-tions. The author provides a straightfor-ward classification system that he uses as the framework for effectively describing the broad range of wound treatments. In these chapters the author covers low adherent; film, foam, polysaccharide, hydrocolloid, hydrogels & xerogels, honey & sugar, silver, odour con-trolling and silicone dressings. Also included are maggot therapy – a topic for which the author is well known for developing and Topical Negative Pressure. Within each of the chapters he covers history, as well as topics such as its development, physical properties, experimental studies, modes of action and clinical experience.
The book begins however, with a succinct account of the anatomy of skin and wound healing, wound aetiologies and economics, including the key feature exudate, one of the main wound characteristics that influence practition-ers’ dressing selection.
Two distinctive chapters are the Development of Dress-ings and Laboratory Testing of Surgical Dressing. The first of these provides a fascinating insight into modern wound treatments and a unique perspective on the background of the concepts that underpin the development of dress-ings. Whereas the second deals with importance of bench testing in the laboratory and the variety of tests that need to be conducted in order to develop safe and efficacious dressings. Setting standards for dressing materials is also essential to developing dressings through adopting a con-sistent approach to assessing structure, performance and safety. Laboratory tests, including equipment and wound
models are described for fluid handling, microbial control and odour.
Maggot Therapy is beautifully illustrated with images of larvae and adult flies and guides practitioners from understanding the theory to delivering patient care. In addition, the evidence that supports mag-got therapy is clearly summarised.
This book is a must for libraries as its unique aspects are the history and technical aspects of developing wound dressings. However, it will be equally valuable to those wanting a comprehensive text on dressings. Sue Bale
SURGICAL DRESSINGS AND WOUND MANAGEMENT
Book Review
Are you interested in submitting an article or paper
for EWMA Journal?
Read our author guidelines atwww.ewma.org/english/authorguide
EWMA Journal 2012 vol 12 no 1 54

AG
-BS-
1551
-10
/ 11
sorbion sachet borderWound Bed Preparation
www.sorbion.com
Finally sealed.sorbion sachet border – the space you need.
NEW
Quick and easy application
Hypoallergenic
Flexible and breathable
Excellent absorption and retention
AZ_EWMA_border_210x297.indd 1 28.10.11 10:37

Editor: Jayesh B. ShahCo-editors: Paul, J. Sheffield and Caroline, E. Fifein partnership with International Atmo2011, Best Publishing Company. USA
The Wound Care Certification – Study Guide is written by a multi professional group of wound care specialists in Texas, USA. According to the authors the aim of the study guide is to help professionals or students prepare for any certification exams within wound care. It is designed to provide a quick, concise review from an exam-oriented perspective. Examples of test questions are presented at the end of each chapter.
The 32 chapters include such topics as pathophysiology and aetiology of wounds, wound assessment and treatment, patient education, pain management, documentation, legal and ethical issues in wound care as well as evidence–based practice and research. The co-editors stress in foreword that “The goal of this text is to help you master the foun-dational information upon which you may develop your career as a wound expert.”
The study guide includes list of detailed issues. For exam-ple, Chapter 4: Cellular components in wound healing includes the list:Cellular Growth factors1. Complex proteins, released by cells, that stimulate: a) Chemotaxis b) Mitosis c) Angiogenesis d) Apoptosis e) Growth factor production by other cells f) Production and degradation of
extracellular matrix.
At first I found the guide somewhat confusing; a little bit like reading someone else’s lecture notes. However, as the co-editors Sheffield and Fife point out in forewords to the book “The study guide focuses on key information that various wound care certifying agencies consider important
in their examinations. It is assembled in a format that makes it easy for a candidate to review the topics and iden-tify areas of strength and areas that need further study.” This explains that the intention of the study guide is as a
supplement providing additional study material and offering self-testing of the reader’s knowledge about wound care.
The Study Guide summarises a lot of information and includes, especially in the tables, a comprehensive amount of information on various specific issues, e.g. Table 1: Signs of malnutrition (p.94). Also the pictures are informative and support the learning objective. At the end of the book, Chapter 30 highlights national treatment guidelines for venous ulcers, diabetic foot ulcers, arterial ul-cers and pressure ulcers. This enables the
reader to pick out the most important facts of the guide-lines. I found Dr Shah’s wound management guidelines in Chapter 31 especially interesting. These were presented as algorithms. Chapter 32 “Post-course practice exam” is built on case descriptions with pictures and key questions related to the presented case. The right answers are given at the end of the chapter. This format for presenting learning challenges is inspiring and also challenges the reader to think and link their knowledge to clinical practice.
The study guide is obviously produced for the educational system in the US and is test and exam oriented. To be able to benefit from this book in connection with independ-ent study, extra educational material, such as books and research articles is needed. For professors and teachers of wound care, the Study Guide provides a checklist of elements to be included in the content of a course and provides examples of tests and material for educational as-signments and independent studies, which play an increas-ing role in the learning process at all levels of the education of health professionals. For me, Study Guide was also a journey into the American certification system, which is very different from the Finnish educational system. Salla Seppänen
Book Review
WOUND CARE CERTIFICATION – STUDy GUIDE
EWMA
EWMA Journal 2012 vol 12 no 1 56

Traumatic Wounds Full/Partial Thickness Wounds EB Wounds Skin Tears Burns Fragile Skin Burn
Fragile Skin Burns Skin Tears EB Wounds Full/P
artial T
hickness Wounds Traumatic Wounds Fragile
FERRIS MFG. CORP. | 16W300 83rd St., Burr Ridge, IL 60527 USA | International: +1 630.887.9797 | WWW.POLYMEM.EU Unless otherwise indicated, all trademarks are owned by or licensed to Ferris. © 2010, Ferris Mfg. Corp., 16W300 83rd Street, Burr Ridge, IL 60527 USA MKL-383-I, REV-4, 0910
References: 1. Sessions R. Examining the Evidence for a Drug�free Dressing’s Ability to Decrease Wound Pain. Poster Presentation. Clinical Symposium on Advances in Skin & Wound Care. October 2008. Las Vegas, NV USA.
2. Stenius M. Fast Healing of Pressure Ulcers in Spinal Cord Injured (SCI) People Through the Use of PolyMem® Dressings. Poster Presentation. EWMA. May 2008. Lisbon, Portugal. 3. Tamir J, Haik J. Polymeric Membrane Dressings for Skin Graft Donor Sites: 4 Years Experience on 800 Cases. Poster Presentation. Clinical Symposium on Advances in Skin & Wound Care. October 2008. Las Vegas, NV USA.
Wounds Respond to
PolyMem’s unique formulation has the ability to reduce
patients’ total wound pain experience while actively
encouraging healing1,2,3

EWMA
The 1st EWMA Master Course was held on 13-14 October in Budapest on the theme “Is Oedema a Challenge in Wound Healing?”
The programme consisted of a mixture of the-oretical lectures and practical workshops centered on diagnosis, prevention and management of oedema in wound healing. Twelve expert lecturers shared their knowledge and experience with the participants in order to enable them to enhance their theoretical knowledge and practical skills which they use in their everyday clinical practice.
The course attracted 48 participants with very different, but highly specialised backgrounds at-tended the course, and provided some valuable feedback.
Evaluation of the 2011 Master CourseIn general, the participants were satisfied with the course: n 68% said the course met their expectations
or was better than they expectedn 100% said the course presenters were either
good or excellentn 82% would recommend the course to others
In addition, for future courses participants recom-mended that we:n Enhance the focus on and increase the
number of practical workshops n Increase the time available for discussion
and sharing of experiences amongst the participants
n Consider providing material for preparation before the course.
Future EWMA Master CoursesAt its meeting in March the EWMA Council will decide on the future structure of the EWMA Master Courses. Therefore, no Master Course is planned for 2012 due to the need for a thorough evaluation of the 1st Master Course and the con-cept.
More information about future EWMA Master Courses will follow at www.ewma.org/woundcourse m
Zena Moore
Chair of the EWMA Education Committee
· EWMA MASTER COURSE·EU
RO
PEAN· WOUND ·MANAGEMENT· A
SSO
CIA
TIO
N
Participants in workshops during EWMA Master Course 2011
The EWMA Master Course 2011
EWMA Journal 2012 vol 12 no 1 58

Say hello to SNaP.®
My partner in healing.
The SNaP® Wound Care System combines the portability of advanced wound dressings with the proven efficacy of negative pressure therapy in a discreet design that won’t get noticed.
m Small, silent, lightweight design disappears under clothes
m Demonstrated non-inferiority in wound healing outcomes
for patients completing at least 4 weeks of therapy1
m The SNaP® System interferes significantly less with overall
activity, sleep and social interactions than the V.A.C.® System1
www.spiracur.com
Spiracur Inc.1180 Bordeaux Drive Sunnyvale, CA 94089+1.408.701.5300
1. Armstrong, D. G., W. A. Marston, et al. “Comparison of Negative Pressure Wound Therapy with the SNaP® Wound Care System vs. V.A.C.® Therapy System for the Treatment of Chronic Lower Extremity Ulcers: A Multicenter Randomized Controlled Trial.” Wound Rep Reg 2011; 19; 173-180. Spiracur, SNaP and SNaP & Design are registered trademarks of Spiracur Inc. The SNaP® Wound Care System is protected by one or more U.S.patents, with other U.S. and certain foreign patents pending. ©2011 Spiracur Inc. All rights reserved.
Active healing that’s out of sight.
SNaP-SayHelloAD-A4.indd 1 11/1/11 10:48 AM

Finn GottrupChair of Leg Ulcer and Compressions
Seminars 2011,EWMA
Hugo Partsch
Chair of Leg Ulcer and Compressions
Seminars 2011,ICC
The Leg Ulcer & Compression Seminars, or-ganised by the International Compression Club (ICC) and the European Wound Management Association (EWMA) in collaboration with lo-cal wound management associations, were held on October 10th in Bratislava, October 11th in Vienna and on October 13th in Budapest.
The seminars attracted many local participants – doctors, nurses and healthcare professionals. In addition, several local companies decided to send participants and exhibit their products at the semi-nars. In total, 295 participants attended and 15 companies exhibited at the Leg Ulcer & Compres-sion Seminars.
With a lunchtime satellite symposium about compression treatment and the latest products de-veloped for this, 3M was the main sponsor of the three seminars. Hartmann supported the seminars with a general sponsorship.
ProgrammeThe scientific programme consisted of two scien-tific sessions before the lunch break – one on Leg Ulcers and one on Compression, each consisting of three lectures held by local experts in the field.In the afternoon there was a workshop on clini-cal and instrumental diagnosis and two rotat-ing company workshops, where the companies demonstrated their products. The Seminar ended with a round table discussion that summed up the
topics of the day and discussed future prospects for the improvement of leg ulcer prevention and treatment in the respective countries.
For more information about the programme, please visit the seminar web site www.ewma.org/icc-ewma-seminar
Political session – future leg ulcer & compression projectsThe local wound management associations invited a number of decision-makers and representatives from health authorities in order to move forward the agenda for leg ulcers and compression treat-ment in their countries.
The invitees participated in a closed political debate and in the following round table discus-sion, which was open to all participants. As a re-sult, a more informed debate concerning the issues of prevention and treatment of leg ulcers has been started in all three countries. In the longer per-spective it is intended that local working groups will be formed in each country with the main objective to move forward the political agenda.
Future Leg Ulcer & Compression SeminarsEWMA and the ICC are currently planning more Leg Ulcer & Compression Seminars in other European countries. More information will fol-low at www.ewma.org m
EWMA
The seminars were organised in coorporation
with the local EWMA Cooperating
Organisations.
Conference Report
Leg Ulcer & Compression Seminars 10, 11 and 13 October 2011, Bratislava, Vienna and Budapest
Round table discussions and Hugo Partsch at Leg Ulcer & Compression Seminars in Slovakia
EWMA Journal 2012 vol 12 no 1 60

2-K041
See the complete details online including continuing education statements,learning objectives, session descriptions, faculty credentials, informationfor submitting oral and poster abstracts, and registration information.
2-K041 FP WC12 ad_Layout 1 11/18/11 3:06 PM Page 1

Wound ManagementSmith & Nephew Medical Ltdwww.smith-nephew.com/wound
Sorbion AGwww.sorbion.com
Systagenix Wound Managementwww.systagenix.com
ArjoHuntleighwww.ArjoHuntleigh.com
B. Braun Medical www.bbraun.com
BSN medical GmbHwww.bsnmedical.comwww.cutimed.com
Chemvironwww.chemvironcarbon.com
Curea Medical GmbHwww.curea-medical.de
Corporate A
ConvaTec Europewww.convatec.com
Covidien (UK) Commercial Ltd.
Paul Hartmann AGwww.hartmann.info
3M Health Carewww.mmm.com
Abbott Nutritionwww.abbottnutrition.com
Absorbestwww.absorbest.se
Advanced BioHealing, Inc.www.AdvancedBioHealing.com
AOTI Ltd.www.aotinc.net
KCI Europe Holding B.V.www.kci-medical.com
Lohmann & Rauscherwww.lohmann-rauscher.com
Mölnlycke Health Care Abwww.molnlycke.com
Ferris Mfg. Corp.www.PolyMem.eu
Corporate Sponsor Contact Data
Corporate B
www.drawtex.com
Flen pharma NVwww.flenpharma.com
Life Wavewww.life-wave.com
Nutricia Advanced Medical Nutritionwww.nutricia.com
Organogenesis Switzerland GmbHwww.organogenesis.com
Phytoceuticalswww.1wound.info
Argentum Medical LLCwww.silverlon.com
Söringwww.soering.com
Laboratoires Urgowww.urgo.com
Welcare Industries SPAwww.welcaremedical.com
EWMA
EWMA Journal 2012 vol 12 no 1 62

EWMA is proud to present the following new b-sponsors:
www.absorbest.se
www.chemvironcarbon.com
www.soering.com
EFORT
EWMA and the European Federation of National Associa-tions of Orthopaedics and Traumatology (EFORT) continue the collaboration in 2012.
EWMA session at EFORTThis year EWMA will have a guest session at EFORT’s annual conference, which takes place 23-25 May 2012 in Berlin, Germany.
EWMA will have a session Thursday 24 May 2012, 09:15-10:45. The EWMA session is entitled Orthopaedics in Wounds – a multidisciplinary approachChair: Sue Bale
Orthopaedics in Wounds – a multidisciplinary approachSpeaker: Sue Bale, United Kingdom
Foot Surgery in treating the diabetic footSpeaker: To be confirmed
Amputations as a consequence of wounds and infectionSpeaker: Klaus Kirketerp-Møller, Denmark
Nurse DayEWMA will also be represented at the EFORT Nurse Day on Wednesday 23 May 2012, 09:00-18:15. The EFORT Nurse Day is a full day course for orthopedic and trauma nurses as well as other allied health care providers. EWMA will be represented by:17:00 -18:00. EWMA: Pressure ulcer Sue Bale, United Kingdom
More information about the EFORT programme, the EWMA session and the Nurse Day is available on www.efort.org/berlin2012
The EWMA Patient Outcome Group– Developing study protocol templates
The EWMA Patient Outcome Group is currently working on a set of study protocol templates, including the relevant research questions related to the primary types of chronic wounds: leg ulcers, diabetic foot ulcers and pressure ulcers.
The development of these templates is a successor to the previous work of the EWMA Patient Out-come Group; the recommendations on use of outcome measures in wound studies published JWC in June 2010.
The templates will serve as a checklist for produc-ing RCTs, cohort studies and non-interventional studies that meet the EWMA recommendations. The final objective is still to increase the amount of high level evidence in wound care.
·PAT
IENT OUTCOME GROUP·EUR
OPEAN
· WOUND ·MANAGEMENT· A
SSO
CIA
TIO
N
Enhanced collaboration between EPUAP and EWMADuring the EPUAP conference in Porto, it was agreed between EPUAP and EWMA to strengthen the mutual exchange of knowledge and lessons learned. This will be achieved by means of a future EPUAP guest session at the annual EWMA conference as well as a EWMA guest session at the annual EPUAP conference.
The first step will be an EPUAP guest session at the EWMA Vienna 2012 Conference which will take place on Thursday 24 May 8:00-9:30.
www.drawtex.com
EWMA Journal 2012 vol 12 no 1 63

Conferences Theme 2012 Days City Country
FWCS Annual Meeting Feb 2-3 Helsinki Finland
NIFS Annual Meeting The Diabetic Foot Feb 2-3 Haugesund Norway
CNC Annual Meeting Feb 16-17 Kortrijk Belgium
5. Freiburg Wundsymposium Mar 10 Freiburg Germany
The Global Conference on Amputation Prevention, Diabetes Management, and Diabetic Foot and Diabetic Wound Care
Global Perspectives, Local Care
Mar 15-17 Los Angeles USA
10th National Australian Wound Management Association Conference
Mar 18-22 Sydney Australia
Congress of Association Francophone d’Infirmiers en Stomathérapie, Cicatrisation et Plaies Belgique
Mar 27 Charleroi Belgium
First Annual Focus Meeting of the EPUAP Apr 16-17 Tel-Aviv Isreal
Tissue Viability Society 2012 Annual Conference Apr 18-19 Kettering United Kingdom
The Annual Spring Symposium on Advanced Wound care (SAWC/WHS)
Apr 19-23 Atlanta Georgia USA
ICW Annual Congress May 9-10 Bremen Germany
Congress of the Swiss Association for Wound Care May 19 Morges Switzerland
22nd Conference of the European Wound Management Association
Wound healing – different perspectives, one goal
May 23-25 Vienna Austria
13th EFORT Congress 2012 May 23-25 Berlin Germany
DGfW Annual Meeting Jun 14-16 Kassel Germany
4th Congress of the World Union of Wound Healing Societies Better care – Better Life Sep 2-6 Yokohama Japan
10th Scientific Meeting of Diabetic Foot Study Group (DFSG) Sep 28-30 Berlin-Potsdam Germany
National Congress of the Belgian Federation of Wound Care Oct Uccle Belgium
4th Scientific Congress of the Polish Wound Management Association
Oct 3-6 Bydgoszcz Poland
Pisa International Diabetic Foot Courses Oct 8-11 Pisa Italy
2013
The French and Francophone Society of Wounds and Wound Healing annual conference
Jan 20-22 Paris France
Conference Calendar
Organisations
For web addresses please visit www.ewma.org
EWMA 201315 -17 May 2013
Danish WoundHealing SocietyDanish WoundHealing Society
COPENHAGENDenmark
WWW.EWMA.ORG / EWMA2013
EWMA Journal 2012 vol 12 no 1 64

Impact-Faktor = 0,733
2010
Submit your next paper to Phlebologie
iris.weiche@schattauer.
de

Michael ClarkEPUAP President
www.epuap.org
The 14th EPUAP Annual Meeting in Porto PortugalOver 400 attendees participated in the 14th Euro-pean Pressure Ulcer Advisory Panel (EPUAP) 2011 meeting which was held in the beautiful city of Porto, Portugal on August 31st to September 2nd. The meeting, with a theme of “Pressure Ulcer Research Achievements Translated to Clinical Guidelines” – to reflect the increasingly growing implementation of the EPUAP/NPUAP International Guidelines for Prevention of Treatment of Pressure Ulcers which were launched last year – was rich in scientific content as well as in clinical perspectives.
The opening session addressed interactions between the clinical and financial problems in pre-venting and treating pressure ulcers, and demon-strated interestingly similar situations in different European countries, where financial decisions need to be taken with respect to practical allocation of equipment and manpower for prevention. This was followed by presenting the Experienced Investigator Award to Prof. Dan Bader (University of Southamp-ton, UK) and the Novice Investigator Award to Dr. Dimitri Beeckman (Ghent University, Belgium) for their contributions to pressure ulcer research. Towards the end of the day the EPUAP pre-sented its first Honorary Life Member award to Dr George Cherry without whom the EPUAP would not have grown into the organisation it is today.
On the next day, basic science developments were addressed, particularly as related to cell migration and wound contraction during healing, and use of MRI to quantify changes in tissue stiffness as a potential damage indicator. Pressure ulcers in the paediatric population was another topic which attracted much attention, where in a dedicated session the development of the skin was reviewed and the prevalence of pressure ulcers in the paedi-atric population was addressed. There was a session on repositioning, where the work of the late Prof. Tom Defloor was high-lighted by his ex PhD student Dr. Katrien Vander-wee; a session on debridement addressing both guidelines and technologies for optimal cleansing of wounds; and a session dedicated to implementa-tion of the international guidelines across different countries in Europe.
The meeting closed with a session on innovations in pressure ulcer prevention and treatment, with focus on electrical stimulation, microclimate, new technologies to promote wound healing, and new clothing solutions for people who use a wheelchair. Other than that, there were industry sessions, a high-quality student paper competition, poster presentations, workshops on the design of clinical trials and classification of pressure ulcers, and an impressive commercial exhibition.
All this action was accompanied by wonderful Portuguese food, wine and hospitality (thanks to the local organizer Paulo Alves), which attendees enjoyed throughout the conference but mostly at the dinner which took place in a fish restaurant just by the beach overlooking the Atlantic.
In 2012, the EPUAP will run two international meetings. The first, which will take place in Tel Aviv University, Tel Aviv Israel on April 16-17 will focus on Technological Innovations in Pressure Ulcer Pre-vention, Diagnosis and Treatment, with an interna-tional panel of invited speakers who are leaders in the science and technology of pressure ulcer care.
The second meeting, on 19-21 September, will be the 15th Annual Conference, which will be in Cardiff UK, on the theme of “Identifying research gaps and clinical needs in pressure ulcer prevention and management”. Detailed information regarding both meetings will be posted online at www.epuap.org m
The 14th EPUAP Annual Meeting in Porto PortugalEPUAP
European Pressure Ulcer Advisory Panel
Organisations
The photo shows Dr Cherry receiving his certificatefrom Professor Cees Oomens, EPUAP President.
EWMA Journal 2012 vol 12 no 1 66

For further details contact: EWMA Secretariat, Nordre fasanvej 113,2000 Frederiksberg,Denmark
Tel: +45 7020 0305Fax: +45 7020 [email protected]
In May 2010 the following EWMA Document was published:
Outcomes in controlled and comparative studies on non healing wounds – Recommendations to improve quality of evidence in wound management
The document is written by members of the EWMA Patient Outcome Group, based on common discussions in the group.
The large POG Evidence document was summarized in a pixi version explaining the key messages.Furthermore the Patient Outcome Group has published another pixi which describes the work and objectives of the group.
Other EWMA documents e.g. Position Documents can be downloaded from www.ewma.org
EWMA DOCUMENTS
Outcomes in controlled and comparative studies on non-healing woundsRecommendations to improve the quality of evidence in wound management
A EWMA Patient Outcome Group Document
EWMA front cover.indd 5
20/5/10 13:14:26
EWMA will produce two new documents in 2012:The EWMA Document on Antimicrobials aims to meet the on-going discussion across Europe concerning the consequences of a biological mutation of infections and the subsequent potential resistance to current wound treatment. The document will describe the related aspects of antiseptic, antibiotic treatment and other relevant treatment methods.
The EWMA document on Debridement aim to provide an updated overview of the various debridement options. It will offer a clarification of the principal role of debridement and define the possibilities and limitations for standard and new debridement options.
EWMA Documents on Debridement and Antimicrobials

SAfWSwiss Association
for Wound Care
Severin Läuchli
President of the Swiss Association
for Wound Care (German Section)
This year’s annual meeting of the Swiss Associa-tion of Wound care (SAfW) took place in Zürich. The congress title was “Standards and Innovation in Wound Therapy”. Needless to say, this attracted a lot of interest and we were able to welcome over 400 wound experts and the support from over 40 industry members.
The focus of the morning session was to set the scene for the definition of standards and some upcoming great ideas. Standards in wound therapy are not as trivial they might seem. Every patient is different and so is every wound. There are numer-ous manufacturers of all kinds of dressings and ointments with minimal differences or advantages one over the other. Very often clear clinical evi-dence is lacking for these treatments and therefore experience-based medicine prevails and helps in the decision-making process. In all these treatment decisions the holistic approach is very important. A multi-disciplinary team, including the patient and the caregiver with the medical professionals, should try to work in concert to achieve the best outcome.
The opening presentation by Dr. Severin Läuchli focused on “Evidence Based Medicine” (EBM) in wound therapy and its challenges. Medical devices (CE marked) don’t need to produce large clinical studies to get to the markets, yet a lot of the differ-ent dressings ‘claim’ to have advantages over others. This has not been proven for any particular dressing and experience-based practise is necessary to choose a treatment that serves best to improve patient related concerns. In EBM, a clear hierarchy and definition of evidence (see the ‘evidence pyra-mid’) exists. During this presentation the different therapies and their levels of evidence were high-lighted with the conclusion that treating the cause of the ulcer, for example with compression therapy, is most important, but recognising that there are methodological challenges in conducting evidence-based clinical trials. Recent publications of the EWMA Patient Outcome Group discuss these chal-lenges and make sensible recommendations for study endpoints.
The second presentation by Mr. Carsten Hampel-Kalthoff about supportive measures that should be part of a standard treatment followed. This presen-tation echoed some of the ideas of the first presen-tation, namely, that wound healing is complex
requiring an holistic approach that involves both patient and caregiver, and also the importance of establishing a treatment goal and verifying achieve-ments against that objective. Statistics in Germany have shown that without a proper follow-up, even after the wound is healed, 60% to 90% of the patients will re-ulcer within 12 months.
Mrs. Patricia Grocott (UK) explained in her presen-tation why a unified approach with a clear defini-tion on expected outcome should be standard. Patients with chronic, hard-to-heal wounds not only suffer from pain, social isolation and a reduced quality of life; it very often impacts the entire family too. We should not forget that this also comes at a high cost to society in general.
The second part of the morning had parallel ses-sions on patient-oriented wound management, wound therapy of the future and currently available advanced wound therapies.
The third group of presentations focused on the current advanced therapies available today. Dr. Silvia Gretener presented some surgical and interventional advances in vascular medicine with the introduction of micro catheters and small stents that allow work on finer arteries or veins. Several studies showed a clear advantage for healing of arterial ulcers where re-vascularisation has been achieved, but very often older patients with co-morbidities are less fit for longer surgical interventions and therefore a less invasive, hopefully ambulatory therapy, is more appropriate in their case.
The next two presentations by Prof. J. Hafner and Dr. D. Mayer concentrated on advanced treatments such as skin equivalents, either from living human cells or cellular, animal-derived matrices, available in the Swiss market. One of the conclusions from the presentations was that at least 20 to 30% of all wounds are considered to be very difficult to heal and that this group of patients would benefit from such advanced methods. It is clear that an ambula-tory application of a skin equivalent can help reduce overall cost, since no hospitalisation is necessary. A successful hospitalisation, including surgical intervention might require 10 to 20 days with average cost of more than CHF 15,000.
Jürg HafnerProf.Dr.med.
General DermatologyDermatologic Surgery
(Skin Cancer)
www.safw.chwww.safw-romande.ch
13th Symposium on Modern Wound Therapy
Interprofessional collaboration to provide good standard treatment and use innovations appropriately
EWMA Journal 2012 vol 12 no 1 68

Lunch time was dedicated to two company-sponsored symposia.
In the afternoon, parallel workshops (hands-on sessions) covered documentation, nutrition, debridement, dressings, news in reimbursement and skin equivalents and how they relate with the roles of doctors and wound experts.
The latter workshop met with particular interest, as Switzer-land has a pioneering role in Europe. Switzerland is the only country in Europe that has two living tissue engineered prod-ucts available for patients with chronic wounds. An agree-ment could be reached between the health authorities and the insurance companies that the application of skin equiva-lents will be reimbursed by the insurance companies if they are used by certified wound care centres and under condi-tions which have been set down by the Swiss Association for Wound Care in collaboration with the Swiss Association for Dermatology and Venerology. This workshop looked at the different roles of doctors and wound experts in the treatment of a patient with a skin equivalent. The workshop followed the ‘debate’ scheme, where both parties, doctors and wound experts, explained in a heated debate their different roles and their responsibilities. Skin equivalents, like Apligraf (a bi-layered living cellular construct), are considered as prescription medication on the Swiss market and, therefore, require a prescription by a med-ical doctor.
The wound experts are trained to manage much of the daily business in a professional manner. Once the team has set a treatment goal for a particular patient it is important that the wound experts follow that plan. Should treatment progress stop they need to ensure a new assessment and a treatment path is initiated with the doctor. For this reason it is also important that the wound experts play a central role in the correct pre-selection of patients potentially profiting from an advanced method. Once a patient has received a skin equivalent, follow-up is important and needs to be done in collaboration with the wound clinic. After initial application of a skin equivalent, the wound should be inspected and the dressing changed at least once a week. During these weekly follow-ups and with a careful re-assessment of the wound and its progress, a reapplication might be necessary to complete healing. Interestingly, the conclusion of the debate was that both doctors and wound experts are necessary to run a successful wound clinic. Wound experts very often have a closer rela-tionship with the patient and the caregivers and therefore learn more about the external factors. The doctor can clearly benefit from the additional information and use it to establish the indications and prescribe the appropriate therapy. m
Organisations
We were able to welcome over 400 wound experts and the support from over 40 industry members.
EWMA Journal 2012 vol 12 no 1 69

Dr. David Keast,President of
WAWLC
The annual meeting of the World Alliance on Wound and Lymphoedema Care (WAWLC) took place in Geneva on the 17-18 Nov 2011. Amongst other activities during the meeting, the following report on WAWLC activities during 2011 was presented by Dr. Terry Treadwell, Chair of the WAWLC Programme Development Commit-tee.
n Cameroun: A Buruli day took place at the University of Yaoundé in early Nov 2011 with the participation of the Healthcare Secretary. On this occasion it was decided to create two modular courses on A) Buruli Ulcers and B) General Wound Care.
Cameroun: A partnership has been established between the Yaoundé University and the medical faculty of the University of Geneva. Faculty people from Cameroun will be invited by MSF to participate in the EWMA 2012 confer-
ence and learn more about wounds and also network with European participants.
Cameroun: The Buruli treatment facility in Akonolinga will start to offer general wound care. Home-based care will be introduced as the hospital does not have space for more than 60 in-patients and patients prefer to stay at home to attend school and working activities.
n Ethiopia: A working programme on Eradication of Podoconiosis in Ethiopia was initiated by Robyn Björk, who carried out an initial field visit in July 2011, in conjunction with the “Mossy Foot Project”.
WAWLC has been invited to provide a speaker for the annual Medical Meeting in Addis Ababa, Ethiopia, in February, 2012. Dr. Tom Serena will present one or two wound care talks on behalf of WAWLC at the meeting.
Overview on WAWLC activities during 2011WAWLC
World Alliance on Wound and
Lymphoedema Care
On request of the Ministry of Health of Kuwait, WAWLC and EWMA representatives visited wound care representatives from Kuwait.
Organisations
EWMA Journal 2012 vol 12 no 1 70

It is hoped that a follow-up visit will result in a wound centre being opened at the Black Lion Hospital. Training of the physicians and staff will be done by WAWLC with all costs expected to be paid by the Black Lion Hospital/Ethiopian Ministry of Health.
The WAWLC activities on Podoconiosis were during the EWMA 2011 Brussels conference supported by a fundrais-ing campaign.
n Ghana: An additional visit to Accra, the site of two previous training programmes, has been made by John Macdonald and Terry Treadwell, who visited the Amasa-man Health Centre in Ghana to initiate a clinical research project regarding the treatment of Buruli Ulcer. The project is progressing slowly and another visit to the site is planned for December, 2011.
n Haiti: Terry Treadwell was invited to teach a two day wound care seminar at the Hôpital de L’Université d’État d’Haiti in June, 2011. Over 60 physicians and nurses attended the course. Two additional one day courses were taught at medical schools in Port-au-Prince covering the basics of wound care.
Agreements were reached with the hospital administration to help them open a wound centre at that hospital. The wound care programme is now up and running after hiring Dr. Francius Adler, a Haitian general surgeon who received wound care training at the Institute for Advanced Wound Care in Montgomery, Alabama with Terry Tread-well in May and June, 2011. Approximately 40 wound patients per day are seen at the facility.
Finally, John Macdonald has been appointed Medical Director of the Wound Care Programme at the Mevs Hospital in Port-au-Prince, Haiti and will, in the future, work one week per month in Port-au-Prince.
n South Africa: Collaboration on outreach to one region is being discussed with Liezl Naude.
n The Kuwait programme was initiated by John Macdonald, Henrik J. Nielsen and David Keast in September 2011 with a site visit and presentation of a proposal for an education programme and establishment of connection to Red Crescent.
A training visit of Dr. Salma from Kuwait to Georgetown, USA is being planned for early 2012.
The expected conditions of the WAWLC collaboration with Kuwait are that all cost related to the training to be arranged in Kuwait will be paid and that WAWLC will receive a grant for its activities in resource-poor settings.
n Other countries: Requests from institutions of wound care programmes and training have been received from Nigeria and Swaziland in Africa, sites in the South Pacific, and South America. m
Please remember the early registration deadline before 15 March 2012.
For more information about the programme, registration etc.please visit the web-site.
ienna · Austria · Österreich
Organised by the European Wound Management Association in cooperation with Die Österreichische Gesellschaft für Wundbehandlung AWA (Austrian Wound Association)
Organisiert von: der Europäischen Wound Management Organisation in Zusammenarbeit mit der Österreichische Gesellschaft für Wundbehandlung, AWA
WWW.EWMA.ORG / EWMA2012
EWMA 201223-25 May / Mai · 2012
WOUND HEALING – DIFFERENT PERSPECTIVES, ONE GOAL
WUNDHEILUNG – UNTERSCHIEDLICHE PERSPEKTIVEN, EIN ZIEL
EWMA Journal 2012 vol 12 no 1

Dr. Georgina Gethin
Chairperson Scientific Organising
Committee and immediate past-president
www.wmai.ie
In October 2011, the WMAI held its 15th anniver-sary conference in the beautiful but windy city of Galway on the West coast of Ireland. Despite the challenges faced by many in the current economic climate this conference was the biggest and one of the most successful to date. Over 300 delegates from nine countries attended over the two days.The theme was, Building the Future of Wound Care, and the key note address on day one, delivered by Prof. Keith Harding, certainly focused minds on what has been achieved to date but also on the challenges ahead. Prof. Harding made particular reference to the importance of the multi-disciplinary team as it is only through such sharing of ideas, knowledge and experience can we really build the future and advance our understanding of wound healing. Further presentations by Prof. David Gray discussed the management of complex wounds and the development of remote monitoring of wounds through the process of tele-medicine.
Pain is a major issue in wound healing, whether it is an acute traumatic wound or the chronic leg ulcer. Dr. Brian McGuire of NUI Galway discussed the physiology of pain and the mechanisms which clini-cians can use to assess pain and help the patient to cope with pain.
Conferences such as the WMAI actively promote the engagement of the novice practitioner and this conference encouraged the participation of a range of disciplines across a range of workshops. Dele-gates attended workshops on wound assessment, documentation, repositioning, gait assessment, assessment of the diabetic foot, vascular assess-ment, debridement, bandaging and compression. These were delivered by a range of experts in the field including; Sinead Murphy, Marion Cahill-Col-lins, David Watterson, Kate Arkley, Mary Burke, Zena Moore, Julie Jordan-O’Brien, Adelene Greene and Caroline McIntosh. The only criticism of the workshops was that there was not enough time and delegates have requested more workshops in the future.
An interesting feature of the WMAI conference is the panel discussion. This year the topic was: Technology versus dressings in wound management – is there a difference in outcomes? The session was chaired by Dr. Georgina Gethin and panel mem-bers included Mr. Henry James, Dr. Zena Moore, Prof. Raj Mani and Ms. Susan Mendez-Eastman.
While the role of technology in wound manage-ment was discussed, the panel and delegates reiter-ated the need for appropriate assessment of the patient and their wound and emphasised that in the absence of a comprehensive assessment appropri-ate management cannot advance.
On day two, the conference held the first of the concurrent sessions. Palliative wound care was presented by two experts in the area, Dr. Patricia Grocott and Dr. Sebastian Probst. Both the concept of the ‘unbounded body’ and the need to develop dressings to fit the complex needs of patients with palliative wounds were well articulated by both presenters. There is a need to build a core body of knowledge in palliative wound care which can support the individual and the clinician. Four presenters, Prof. Sean Tierney, Prof. Raj Mani, Prof. Robert Strohal and Dr. Georgina Geth-in, discussed the current advancements in wound diagnostics and the micro environment of the wound. Delegates heard presentations on the WAR assessment tool for assessment of wound infection risk and the role of pH in wound bed assessment. Later that morning Dr. Breda Cullen introduced the concept of using modern technology in wound diagnostics and spoke about the role of protease in wound healing and tissue repair.
Prof. Finn Gottrup provided the keynote address for day two. Prof. Gottrup discussed the challenges in evidence and outcomes in wound healing and the challenges faced in designing randomised control-led trials in patients with chronic wounds. This session provided the platform for some interesting audience participation in the debate on wound healing outcomes and reinforced the need for further dialogue on this topic.
Economics would seem to be at the forefront of all conversations related to resources at this time. Prof. Charles Normand provided some useful means through which one can consider economics and wound care and provided some valuable tools and resources which clinicians can use in making the case for additional resources. Ms. Susan Men-dez-Eastman gave a comprehensive overview of the effect of topical negative therapy on wound tissues and healing outcomes. Dr. Caroline Dowsett explored the evidence in support of topical negative therapy currently and in the future of wound healing.
Building the Future of Wound Care15th Anniversary Conference of Wound Management Association of Ireland
WMAIWound
Management Association
of Ireland
EWMA Journal 2012 vol 12 no 1 72

As a member of EWMA, you need access to thelatest international developments in wound management and prevention. Journal of Wound Care is a leading international MEDLINE-listed wound care journal, with a loyal global audience and contributors from every continent. Every month, JWC provides a truly global perspective on wound care, from the latest in evidence-based practice to cutting-edge researchfrom the US, Europe and elsewhere. JWC is read by a wide audience, including doctors, nurses, podiatrists, physiotherapists and occupational therapists involved in wound care.
SUBSCRIBE TODAY and receive special rates online by visiting www.journalofwoundcare.com/EWMA
j o u rnal of w o u nd ca r e
? ? C W
C
? ? ? v o l u m e 2 0 . n u m b e r 9 . s e p t e m b e r 2 0 1 1
Evaluation of the skin stripping of wound dressing adhesives
Wound healing through synergy of hyaluronan and an iodine complex
Innovation in tissue viability documentation for acute services
Necrosis in breast cancer patients with skin metastases receiving bevacizumab
Extended leg infection of diabetic foot ulcers: risk factors and outcome
Wound dressings and other topical treatment modalities in bioburden control
cover.indd 1 31/08/2011 13:49
W v o l u m e 2 0 . n u m b e r 9 . s e p t e m b e r 2 0 1 1
Evaluation of the skin stripping of wound
Wound healing through synergy of hyaluronan and an iodine complex
Innovation in tissue viability documentation for acute services
Necrosis in breast cancer patients with skin metastases receiving bevacizumab
j o u rnal of w o u nd ca r e
? ? C W
C
? ? ? v o l u m e 2 0 . n u m b e r 1 0 . o c t o b e r 2 0 1 1
Quantitative estimation of exudate volume for full-thickness pressure ulcers
A proposed method of evaluating orbital exenteration wounds
Modelling the cost-effectiveness of bioelectric stimulation therapy in chronic VLUs
The effect of temperature and humidity on the permeability of film dressings
Complex lower extremity wounds treated with skin grafts and NPWT
The effect of simulated leg-length discrepancy on plantar pressure distribution
JWC_20_10_cover.indd 1 04/10/2011 15:22
j o u ru ru nal l l of f f w o w o w u nd d d ca r e W
C
v o l u m e 2 0 . n u m b e r 1 0 . o c t o b e r 2 0 1 1
Quantitative estimation of exudate volume for full-thickness pressure ulcers
A proposed method of evaluating orbital exenteration wounds
Modelling the cost-effectiveness of bioelectric stimulation therapy in chronic VLUs
j o u rnal of w o u nd ca r e
? ? C W
C
? ? ? v o l u m e 2 0 . n u m b e r 1 1 . n o v e m b e r 2 0 1 1
The patient experience of complex wounds treated with NPWT
Ultrasound assessment of necrotic tissue in pressure ulcers with undermining
Chronic plantar ulcer secondary to congenital indifference to pain
Manuka honey as an effective treatment for chronic pilonidal sinus wounds
Silver and nanoparticles of silver in wound dressings
Efficacy of a PHMB-containing biocellulose dressing in the treatment of biofilms
JWC_20_11_cover.indd 1 03/11/2011 14:44
VISIT NOW:
www.journalofwoundcare.com/EWMA
JWC_EWMA_Offer_HP.indd 1 08/11/2011 15:04
In a very interesting session, Ms. Dympna Pearson gave delegates a thought provoking presentation on health behavioural change with particular reference to nutrition and wound healing.
The final presentation of the conference by Dr. Marlese Dempsey was to remind us all of how fortunate we are to live in a country where we have access to health care and mod-ern therapies. Dr. Dempsey recounted her role and that of her colleagues in the aftermath of the Haiti disaster in 2011.
During the conference four free papers were presented:Mr. Wael Tawfick and Mr. Sherif Sultan presented Technical and Clinical Outcomes of Topical Wound Oxygen in compari-son to conventional compression dressing in the management of refractory non-healing venous ulcers.Derk F. Frye and Liam Farrell presented The use of human fibroblast derived dermal substitute with topical oxygen in vascular compromised wounds.Paul Breen, Dr. C. McIntosh, Prof. J. Serrador, C. O’Tuathail, Dr. S. Dinneen, and Prof. G. Ó Laighin: presented Sensory neuromodulation; a new paradigm to restore peripheral sensitivity.Bryony Treston, Dr. G. Gethin, Prof. S. Tierney, M. Prender-gast, H. Strapp, and Prof. S. Cowman presented Prevalence of lower limb lymphoedema and quality of life among persons with diabetic foot disease.
Two prize winners were announced:Lilian Bradley memorial prize: Madden, J. & Cundell, J – Can podiatrists identify the level of heel pressure damage as defined by the EPUAP classification, to ensure inter-rater reliability in assessing heel pressure damage?
WMAI prize: Hamada, N., Soylu, E., Fahy, A., Tawfick, W. and Sultan, S. – The results of the sequential compression biomechanical device in patients with critical limb ischemia and non-reconstructable peripheral vascular disease.
The association is most grateful to the massive industry sup-port for this conference. Twenty-seven companies met with delegates over the two days and the Journal of Wound Care supported the organisation through the development of a conference book.
We would like to thank the work and commitment of the conference organising committee and the national executive of the association. The next conference will be held in Cork in 2013 and we look forward to building on the work of 2011 and an even bigger and better conference. We would also like to thank the many speakers who gave up not just their time to attend and present, but also the many hours which went into devel-oping their presentations. Finally, we want to thank the many delegates who attended and hope that this conference goes in some way towards Building the Future of Wound Care. Organising committee: Georgina Gethin, Adelene Greene, Caroline McIntosh, Kate Arkley, Marie Mellett, Marion Cahill Collins. m
Organisations

AFIScep.beFrench Nurses’ Association in Stoma Therapy, Wound Healing and Woundswww.afiscep.be
AISLeC Italian Nurses’ Cutaneous Wounds Associationwww.aislec.it
AIUCItalian Association for the study of Cutaneous Ulcerswww.aiuc.it
APTFeridasPortuguese Association for the Treatment of Woundswww.aptferidas.com
AWAAustrian Wound Associationwww.a-w-a.at
BEFEWOBelgian Federation of Woundcarewww.befewo.org
BWABulgarian Wound Associationwww.woundbulgaria.org
CNCClinical Nursing Consulting – Wondzorgwww.wondzorg.be
CSLRCzech Wound Management Societywww.cslr.cz
CWACroatian Wound Associationwww.huzr.hr
DGfWGerman Wound Healing Societywww.dgfw.de
Danish WoundHealing Society
DSFSDanish Wound Healing Societywww.saar.dk
FWCSFinnish Wound Care Societywww.suomenhaavanhoitoyhdistys.fi
GAIF Associated Group of Research in Woundswww.gaif.net
Cooperating Organisations
GNEAUPPNational Advisory Group for the Study of Pressure Ulcers and Chronic Woundswww.gneaupp.org
ICWChronic Wounds Initiativewww.ic-wunden.de
LBAALatvian Wound Treating Organisation
LUFThe Leg Ulcer Forumwww.legulcerforum.org
LWMALithuanian Wound Management Associationwww.lzga.lt
MASCMaltese Association of Skin and Wound Carewww.mwcf.madv.org.mt/
MSKTHungarian Wound Care Societywww.euuzlet.hu/mskt/
MWMAMacedonian Wound Management Association
NATVNSNational Association of Tissue Viability Nurses, Scotland
NIFSNorwegian Wound Healing Associationwww.nifs-saar.no
NOVWDutch Organisation of Wound Care Nurseswww.novw.org
PWMAPolish Wound Management Associationwww.ptlr.pl
SAfWSwiss Association for Wound Care(German section)www.safw.ch
EWMA Journal 2012 vol 12 no 1 74

SAfWSwiss Association for Wound Care(French section)www.safw-romande.ch
SAWMASerbian Advanced Wound Management Associationwww.lecenjerana.com
SEBINKOHungarian Association for the Improvement in Care of Chronic Wounds and Incontinentiawww.sebinko.hu
SFFPCThe French and Francophone Society of Wounds and Wound Healingwww.sffpc.org
SSiSSwedish Wound Care Nurses Associationwww.sarsjukskoterskor.se
SSOORSlovak Wound Care Associationwww.ssoor.sk
STW BelarusSociety for the Treatment of Wounds (Gomel, Belarus)www.burnplast.gomel.by
SUMSIcelandic Wound Healing Societywww.sums-is.org
SWHS Serbian Wound Healing Societywww.lecenjerana.com
SWHSSwedish Wound Healing Societywww.sarlakning.se
TVSTissue Viability Societywww.tvs.org.uk
URuBiHAssociation for Wound Management of Bosnia and Herzegovinawww.urubih.ba
UWTOUkrainian Wound Treatment Organisationwww.uwto.org.ua
V&VNDecubitus and Wound Consultants, Netherlandswww.venvn.nl
WMAIWound Management Association of Irelandwww.wmai.ie
WMAKWound Management Association of Kosova
WMASWound Management Association Slovenia www.dors.si
WMATWound Management Association Turkeywww.yaradernegi.net
For more information about EWMA’s Cooperating Organisations
please visit www.ewma.org
Associated Organisations
Leg ClubLindsay Leg Club Foundationwww.legclub.org
LSNThe Lymphoedema Support Networkwww.lymphoedema.org/lsn
International Partner Organisations
AWMA Australian Wound Management Associationwww.awma.com.au
ILFInternational Lymphoedema Frameworkwww.lympho.org
AAWCAssociation for the Advancement of Wound Carewww.aawconline.org
NZWCSNew Zealand Wound Care Societywww.nzwcs.org.nz
Debra InternationalDystrophic Epidermolysis Bullosa Research Associationwww.debra.org.uk
SOBENFeEBrazilian Wound Management Association www.sobenfee.org.br
EFORT European Federation of National Associations of Orthopaedics and Trauma-tologywww.efort.org
Organisations
EWMA Journal 2012 vol 12 no 1 75

Science, Practice and Education
EBWM
EWMA
5 EditorialJan Apelqvist
7 How to rate the wound debridement trauma? Jan Stryja
14 Ensuring equitable wound management education within the Australian contextJan Rice
18 Low wound prevalence and cost burden: The impact of a multidisciplinary wound specialist teamAlison Hopkins, Fran Worboys, John Posnett
18 The results of a comprehensive wound audit in a UK primary care trustAlison Hopkins, Fran Worboys
21 Pressure ulcer programme of research – PURPOSE Nixon J, Wilson L.M, Coleman S, Gorecki C, Muir D, Pinkney L, Keen J, Briggs M, McGinnis E, Stubbs N, Dealey C, Nelson A
27 The skin’s own bacteria may aggravate inflammatory and occlusive changes in atherosclerotic arteries of lower limbsWaldemar L. Olszewski, Piotr Andziak, M. Moscicka-Wesolowska,Bozenna Interewicz, Ewa Swoboda, Ewa Stelmach
33 Problem with the post burn wound pain: Chronic profilesLaima Juozapaviciene, Rytis Rimdeika, Aurika Karbonskiene
40 Abstracts of recent Cochrane reviewsSally Bell-Syer
42 EWMA Journal Previous Issues and other Journals
44 The Austrian Wound Association AWAArja Riegler, Franz Trautinger
46 The Amputation Register Project by the Austrian Society of Surgery and the Austrian Wound AssociationGerald Zöch
48 Diabetic Foot Activities in AustriaJan Apelqvist, Thomas Pieber, Gerald Zöch
50 Wound care in Russia and Neighbouring Countries: Symposium at EWMA 2012 and other activitiesRytis Rimdeika, Robert Strohal
51 Meeting with MEP Vittorio Prodi
52 Pisa International Diabetic Foot Course 2011Alberto Piaggesi
54-56 Book ReviewSue Bale, Salla Seppänen
58 The EWMA Master Course 2011Zena Moore
60 Conference Report: Leg Ulcer & Compression SeminarsFinn Gottrup, Hugo Partsch
62 EWMA Corporate Sponsors
63 EWMA Activities Update
64 Conference Calendar
66 The 14th EPUAP Annual Meeting in Porto PortugalMichael Clark
68 SAfW – 13th Symposium on Modern Wound TherapySeverin Läuchli, Jürg Hafner
70 Overview on WAWLC activities during 2011David Keast
72 WMAI – Building the Future of Wound Care 15th Anniversary ConferenceGeorgina Gethin
74 Cooperating Organisations
75 International Partner Organisations
75 Associated Organisations
Organisations
![[XLS]gaetcy.jops-dev.comgaetcy.jops-dev.com/images/photos_news/Prenoms.xls · Web viewjoye jozafat joze jozef slovak, slovene, polish, dutch jozefa hungarian, polish jozefo jozo józsef](https://img.pdfslide.us/doc/110x75/5aab93867f8b9a2b4c8c34ba/xls-viewjoye-jozafat-joze-jozef-slovak-slovene-polish-dutch-jozefa-hungarian.jpg)












![Demencie [Re im kompatibility]) - Univerzita Pavla Jozefa ... Demencie.pdf · 30.03.2016 1 Demencie Demencie Závažný medicínsky, ekonomický, celospoločenský problém Obrovské](https://img.pdfslide.us/doc/110x75/5c06e0f509d3f268128c8d94/demencie-re-im-kompatibility-univerzita-pavla-jozefa-30032016-1.jpg)






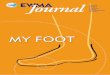


![[a. Rubanov, A. Kutepov] Problems in Geometry(BookFi.org)](https://img.pdfslide.us/doc/110x75/55cf98a0550346d03398bb8f/a-rubanov-a-kutepov-problems-in-geometrybookfiorg.jpg)




