Embed Size (px)
Citation preview
Herpetic Corneal InfectionsSonal S. Tuli, MD
VOLUME XXVI, NUMBER 8
SEPTEMBER 2008 (MODULE 2 OF 3)
Reviewers and Contributing Editors
George A. Stern, MD, Editor for Cornea & External Disease
Kristin M. Hammersmith, MD, Basic and Clinical Science Course Faculty, Section 8
Christie Morse, MD, Practicing Ophthalmologists Advisory Committee for Education
FocalPoints
Consultants
James Chodosh, MD, MPH
Kirk R. Wilhelmus, MD, PhD
Clinical Modules for Ophthalmologists
Claiming CME CreditAcademy members: To claim Focal Points CME cred-
its, visit the Academy web site and access CME Central
(http://www.aao.org/education/cme) to view and print
your Academy transcript and report CME credit you
have earned. You can claim up to two AMA PRA Cate-
gory 1 Credits™ per module. This will give you a maxi-
mum of 24 credits for the 2008 subscription year. CME
credit may be claimed for up to three (3) years from
date of issue. Non-Academy members: For assistance
please send an e-mail to [email protected] or a
fax to (415) 561-8575.
Focal Points (ISSN 0891-8260) is published quarterly by the American Academy of Ophthalmology at 655 Beach St., San Francisco, CA 94109-1336. Print and online 1 year subscription is $175 for Academy members (2 years, $315; 3 years, $445) and $235 for nonmembers (2 years, $425; 3 years, $600). Online only 1-year subscription is $145 for members (2 years, $260; 3 years, $370) and $195 for nonmembers (2 years, $350; 3 years, $500). Periodicals post-age paid at San Francisco, CA, and additional mailing offices. POSTMASTER: Send address changes to Focal Points, P.O. Box 7424, San Francisco, CA 94120-7424.
The American Academy of Ophthalmology is accredited by the Accredita-tion Council for Continuing Medical Education to provide continuing medical education for physicians.
The American Academy of Ophthalmology designates this educational activity for a maximum of two AMA PRA Category 1 Credits™. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Reporting your CME online is one benefit of Academy membership. Non-members may request a Focal Points CME Claim Form by contacting Focal
Points, 655 Beach St., San Francisco, CA 94109-1336.The Academy provides this material for educational purposes only. It is not
intended to represent the only or best method or procedure in every case, nor to replace a physician’s own judgment or give specific advice for case manage-ment. Including all indications, contraindications, side effects, and alternative agents for each drug or treatment is beyond the scope of this material. All information and recommendations should be verified, prior to use, with current information included in the manufacturers’ package inserts or other indepen-dent sources and considered in light of the patient’s condition and history. Ref-erence to certain drugs, instruments, and other products in this publication is made for illustrative purposes only and is not intended to constitute an endorse-ment of such. Some material may include information on applications that are not considered community standard, that reflect indications not included in approved FDA labeling, or that are approved for use only in restricted research settings. The FDA has stated that it is the responsibility of the physician to determine the FDA status of each drug or device he or she wishes to use, and to use them with appropriate informed patient consent in compliance with applicable law. The Academy specifically disclaims any and all liability for injury or other damages of any kind, from negligence or otherwise, for any and all claims that may arise out of the use of any recommendations or other information contained herein. The author(s) listed made a major contribu-tion to this module. Substantive editorial revisions may have been made based on reviewer recommendations.
Subscribers requesting replacement copies 6 months and later from the cover date of the issue being requested will be charged the current module replacement rate.
©2008 American Academy of Ophthalmology®. All rights reserved.
ii F O C A L P O I N T S : M O D U L E 8 , 2 0 0 8
Focal Points Editorial Review BoardGeorge A. Stern, MD, Missoula, MT
Editor in Chief, Cornea & External Disease
Thomas L. Beardsley, MD, Asheville, NC
Cataract
William S. Clifford, MD, Garden City, KS
Glaucoma Surgery; Liaison for Practicing Ophthalmologists Advisory
Committee for Education
Bradley S. Foster, MD, Springfield, MA
Retina & Vitreous
Anil D. Patel, MD, Oklahoma City, OK
Neuro-Ophthalmology
Eric P. Purdy, MD, Fort Wayne, IN
Oculoplastic, Lacrimal, & Orbital Surgery
Steven I. Rosenfeld, MD, FACS, Delray Beach, FL
Refractive Surgery, Optics & Refraction
C. Gail Summers, MD, Minneapolis, MN
Pediatric Ophthalmology & Strabismus
Albert T. Vitale, MD, Salt Lake City, UT
Ocular Inflammation & Tumors
Focal Points StaffSusan R. Keller, Acquisitions Editor
Kim Torgerson, Publications Editor
Clinical Education Secretaries and StaffGregory L. Skuta, MD, Senior Secretary for Clinical Education,
Oklahoma City, OK
Louis B. Cantor, MD, Secretary for Ophthalmic Knowledge,
Indianapolis, IN
Richard A. Zorab, Vice President, Ophthalmic Knowledge
Hal Straus, Director of Print Publications

F O C A L P O I N T S : M O D U L E 8 , 2 0 0 8 1
IntroductionThe word herpes is derived from the Greek word meaning “to crawl,” because of the serpiginous nature of herpetic lesions. Herpes viruses affecting humans include herpes simplex virus types 1 and 2 (HSV-1, HSV-2), varicella- zoster virus (VZV), cytomegalovirus, and Epstein- Barr virus. These double- stranded DNA viruses have a viral- derived capsid enclosed in a host cell–derived envelope with viral- derived glycoprotein projections (Figure 1).
ContentsIntroduction 1
Herpes Simplex Keratitis 2Life Cycle of Herpes Simplex Virus 2
Epithelial and Stromal Keratitis 3
Diagnosis 5
Long-Term Complications 5
Treatment 5
Herpes Zoster Ophthalmicus 7Diagnosis 8
Acute Keratitis 8
Chronic/Relapsing Keratitis 8
Long-Term Complications 9
Treatment 9
Conclusion 11
Clinicians’ Corner 13
•
•
•
•
•
•
•
•
•
•
Financial Disclosures
The authors, reviewers, and consultants disclose the following finan-
cial relationships. James Chodosh, MD, MPH: (S) National Eye
Institute. Kristin M. Hammersmith, MD: (L) Allergan. Steven I.
Rosenfeld, MD, FACS: (L) Allergan. Albert T. Vitale, MD:
(C) Bausch & Lomb.
The following contributors state that they have no significant financial
interest or other relationship with the manufacturer of any commer-
cial product discussed in their contributions to this module or with the
manufacturer of any competing commercial product:
Thomas L. Beardsley, MD; William S. Clifford, MD; Bradley S.
Foster, MD; Christie Morse, MD; Anil D. Patel, MD; Eric P. Purdy,
MD; George A. Stern, MD; C. Gail Summers, MD; Sonal S. Tuli, MD;
Kirk R. Wilhelmus, MD, PhD.
C = consultant fee, paid advisory boards, or fees for attending a
meeting
L = lecture fees (honoraria), travel fees, or reimbursements when
speaking at the invitation of a commercial entity
S = grant support
Learning ObjectivesUpon completion of this module, the reader should be able to:
Describe the different clinical presentations of herpes simplex and herpes zoster corneal infections, including unusual presentations and complications of these diseases
Discuss the Herpetic Eye Disease Study, its outcomes, and its limitations
Explain the current therapies available for herpetic eye disease, including surgery, understand the rationale for using these treatments, and outline their complications
•
•
•
Figure 1 Structure of herpes simplex virus.
2 F O C A L P O I N T S : M O D U L E 8 , 2 0 0 8
For the ophthalmologist, the three most important of these viruses are HSV-1, HSV-2, and VZV, all of which are neurotrophic. Once primary infection occurs, they enter the sensory nerve ganglia and reside there permanently. Periodic reactivations result in the morbidity seen with these viruses. In the United States, estimates note 60,000 new and recurrent cases of HSV keratitis and 50,000 to 100,000 cases of VZV keratitis, also called herpes zoster ophthalmicus (HZO), per year. Not only are these viruses a significant medical problem, but the economic implica-tions are staggering. Studies have estimated that treat-ment of each acute episode of HSV costs $200 to $300 and that systemic antiviral prophylaxis costs $8500 per event averted. In addition, there are intangible losses related to HSV infection, such as the loss of manpower.
Herpes Simplex KeratitisKeratitis caused by HSV, or herpes simplex keratitis (HSK), is the most common cause of corneal blindness in devel-oped nations. It was previously thought that HSV-1 had a predilection for the trigeminal ganglion and HSV-2, for the sacral ganglion. However, an increasing number of cases of ocular herpes are caused by HSV-2, and anec-dotal reports suggest that ocular HSV-2 infections may be more severe and cause more scarring.
Life Cycle of Herpes Simplex Virus
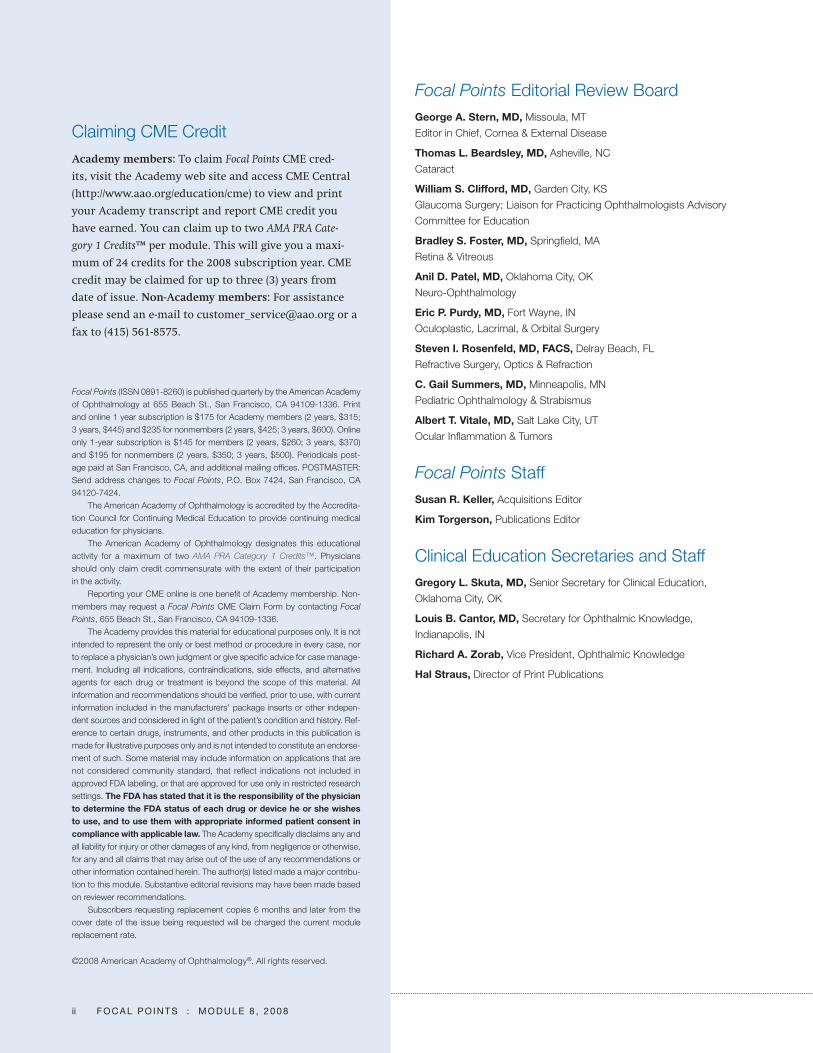
Primary HSV infection occurs by direct contact with infected secretions. On contact, the virus enters epithe-lial cells and starts replicating. Within hours, it enters the sensory nerve endings and travels to the sensory gan-glion, where it may remain in a dormant form called latency (Figure 2). Alternatively, it may replicate and travel back down the nerve to cause a primary infection that is clinically evident in 1% to 6% of infected patients. Once the primary infection resolves, the virus becomes latent and remains in this state until certain triggers, such as fever, sunlight exposure, stress, and menses, cause it to reactivate, multiply, and travel back down the nerve to cause recurrent infection. It is uncertain whether ocular recurrences are caused by virus that initially infected ocular tissues or by “back-door spread,” via the trigemi-nal ganglion, from an initial oral infection. HSV utilizes cellular enzymes for replication and the cell dies when it is released from the cell. The loss of ganglion cells with recurrent infections leads to decreased corneal sensa-tion, one of the hallmarks of HSK.
Primary HSV Infection. Primary HSV ocular infection is frequently missed and rarely affects the cornea. The most common pattern of infection is blepharoconjunc-tivitis that heals without scarring. The associated fol-licular conjunctivitis is often mistaken for adenoviral conjunctivitis. However, unilateral, nonepidemic follic-ular conjunctivitis should always make one suspect HSV, as studies have shown at least 25% of such cases to be culture- positive for HSV.
In rare instances, especially in patients with severe eczema or other immunocompromised states, this usu-ally innocuous infection can become life- threatening. Kaposi’s varicelliform eruption is characterized by exten-sive vesicular eruptions over the entire body surface and can lead to multisystem failure.
Recurrent HSV Infection. Recurrent HSV infection most frequently involves the cornea, although all other parts of the eye can be affected concurrently or independently. HSV can cause retinitis, trabeculitis, uveitis, and optic neuritis; discussion of these noncorneal infections is beyond the scope of this module.
Figure 2 Life cycle of herpes simplex virus. TG = trigeminal ganglion.
F O C A L P O I N T S : M O D U L E 8 , 2 0 0 8 3
Epithelial and Stromal Keratitis
HSK can be subdivided into epithelial and stromal kera-titis, although both are often present to some degree. Understanding the anatomic basis for this classification may give the ophthalmologist a clearer picture of the pathophysiology and treatment of the disease.
Epithelial Keratitis. These forms of keratitis are usually caused by actively replicating virus. Presentations of epi-thelial HSK include the following.
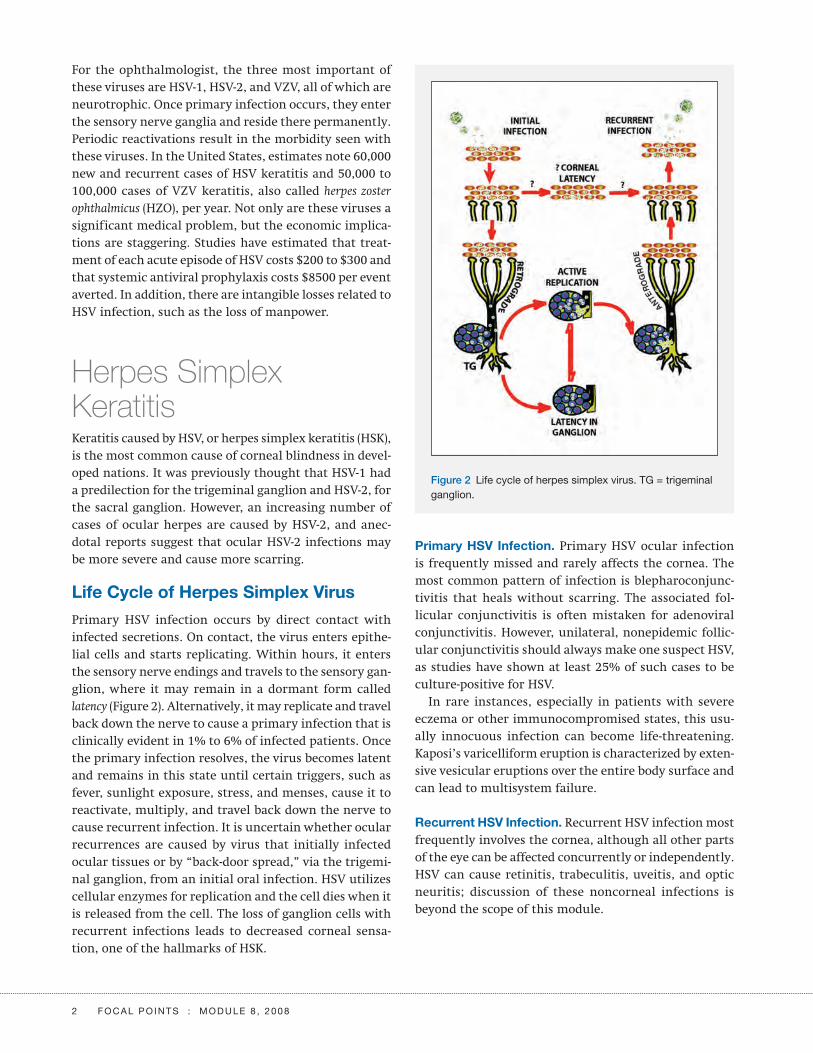
Dendritic ulcer is the classic herpetic corneal lesion, caused by replicating virus. The lesion is linear and dichotomously branching, with each branch terminat-ing with a bulb (Figure 3). The borders of the lesion are slightly raised and grayish and consist of HSV- infected cells that stain with rose bengal (RB) dye. In Figure 3, these HSV- infected cells have undergone balloon degen-eration. In contrast, the center of the lesion is devoid of cells and stains with f luorescein. The underlying stroma has minimal inf lammation. After dendritic epithelial keratitis resolves, a dendritic scar, called a ghost dendrite, may remain in the superficial stroma.
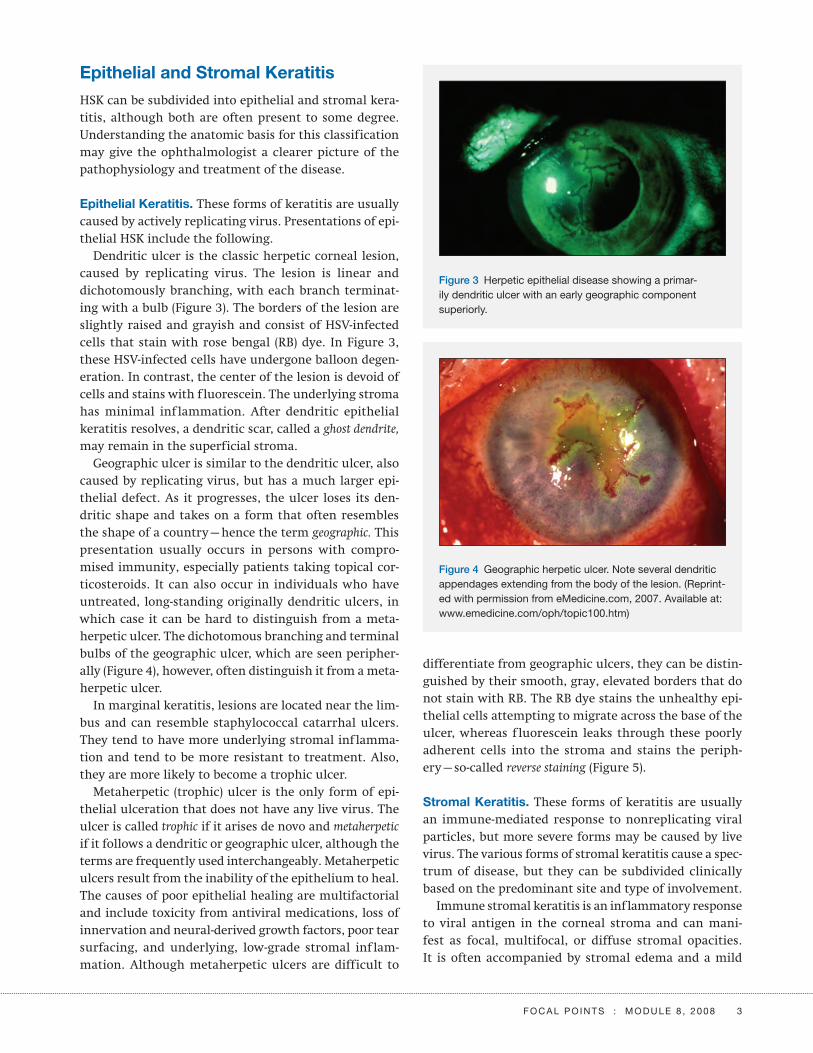
Geographic ulcer is similar to the dendritic ulcer, also caused by replicating virus, but has a much larger epi-thelial defect. As it progresses, the ulcer loses its den-dritic shape and takes on a form that often resembles the shape of a country—hence the term geographic. This presentation usually occurs in persons with compro-mised immunity, especially patients taking topical cor-ticosteroids. It can also occur in individuals who have untreated, long- standing originally dendritic ulcers, in which case it can be hard to distinguish from a meta-herpetic ulcer. The dichotomous branching and terminal bulbs of the geographic ulcer, which are seen peripher-ally (Figure 4), however, often distinguish it from a meta-herpetic ulcer.
In marginal keratitis, lesions are located near the lim-bus and can resemble staphylococcal catarrhal ulcers. They tend to have more underlying stromal inflamma-tion and tend to be more resistant to treatment. Also, they are more likely to become a trophic ulcer.
Metaherpetic (trophic) ulcer is the only form of epi-thelial ulceration that does not have any live virus. The ulcer is called trophic if it arises de novo and metaherpetic if it follows a dendritic or geographic ulcer, although the terms are frequently used interchangeably. Metaherpetic ulcers result from the inability of the epithelium to heal. The causes of poor epithelial healing are multifactorial and include toxicity from antiviral medications, loss of innervation and neural- derived growth factors, poor tear surfacing, and underlying, low- grade stromal inf lam-mation. Although metaherpetic ulcers are difficult to
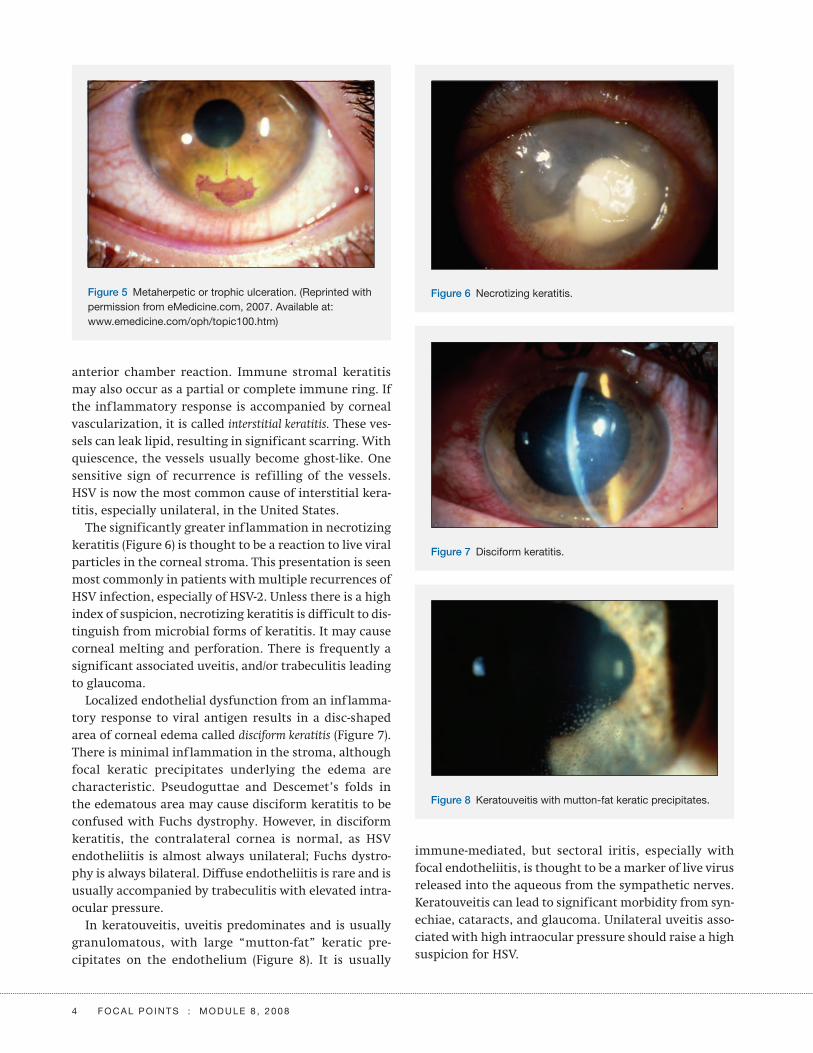
differentiate from geographic ulcers, they can be distin-guished by their smooth, gray, elevated borders that do not stain with RB. The RB dye stains the unhealthy epi-thelial cells attempting to migrate across the base of the ulcer, whereas f luorescein leaks through these poorly adherent cells into the stroma and stains the periph-ery—so-called reverse staining (Figure 5).
Stromal Keratitis. These forms of keratitis are usually an immune- mediated response to nonreplicating viral particles, but more severe forms may be caused by live virus. The various forms of stromal keratitis cause a spec-trum of disease, but they can be subdivided clinically based on the predominant site and type of involvement.
Immune stromal keratitis is an inflammatory response to viral antigen in the corneal stroma and can mani-fest as focal, multifocal, or diffuse stromal opacities. It is often accompanied by stromal edema and a mild
Figure 3 Herpetic epithelial disease showing a primar-ily dendritic ulcer with an early geographic component superiorly.
Figure 4 Geographic herpetic ulcer. Note several dendritic appendages extending from the body of the lesion. (Reprint-ed with permission from eMedicine.com, 2007. Available at: www.emedicine.com/oph/topic100.htm)
4 F O C A L P O I N T S : M O D U L E 8 , 2 0 0 8
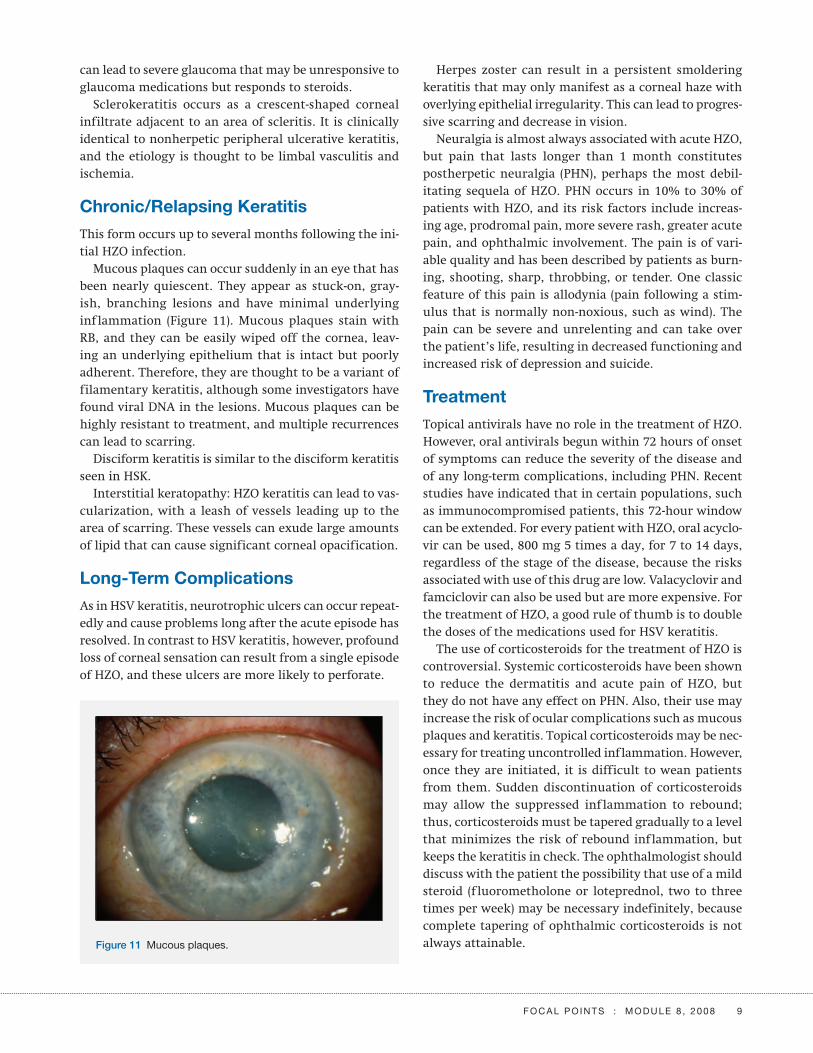
immune- mediated, but sectoral iritis, especially with focal endotheliitis, is thought to be a marker of live virus released into the aqueous from the sympathetic nerves. Keratouveitis can lead to significant morbidity from syn-echiae, cataracts, and glaucoma. Unilateral uveitis asso-ciated with high intraocular pressure should raise a high suspicion for HSV.
anterior chamber reaction. Immune stromal keratitis may also occur as a partial or complete immune ring. If the inflammatory response is accompanied by corneal vascularization, it is called interstitial keratitis. These ves-sels can leak lipid, resulting in significant scarring. With quiescence, the vessels usually become ghost-like. One sensitive sign of recurrence is refilling of the vessels. HSV is now the most common cause of interstitial kera-titis, especially unilateral, in the United States.
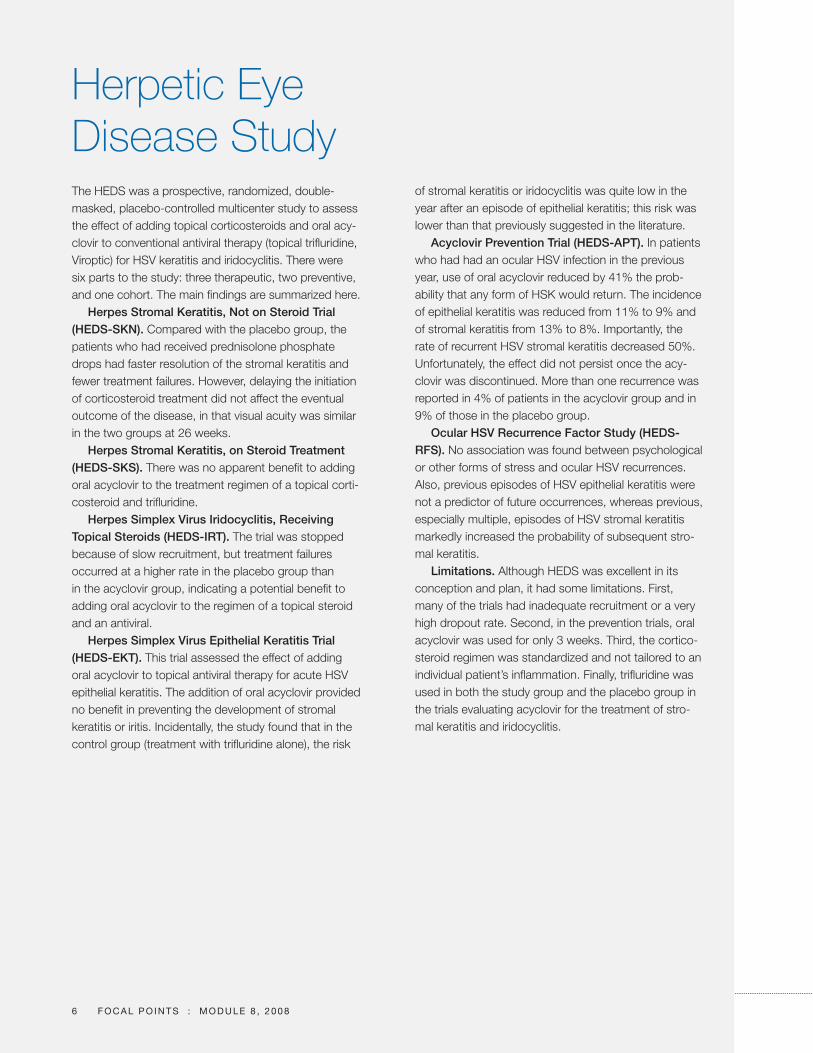
The significantly greater inflammation in necrotizing keratitis (Figure 6) is thought to be a reaction to live viral particles in the corneal stroma. This presentation is seen most commonly in patients with multiple recurrences of HSV infection, especially of HSV-2. Unless there is a high index of suspicion, necrotizing keratitis is difficult to dis-tinguish from microbial forms of keratitis. It may cause corneal melting and perforation. There is frequently a significant associated uveitis, and/or trabeculitis leading to glaucoma.
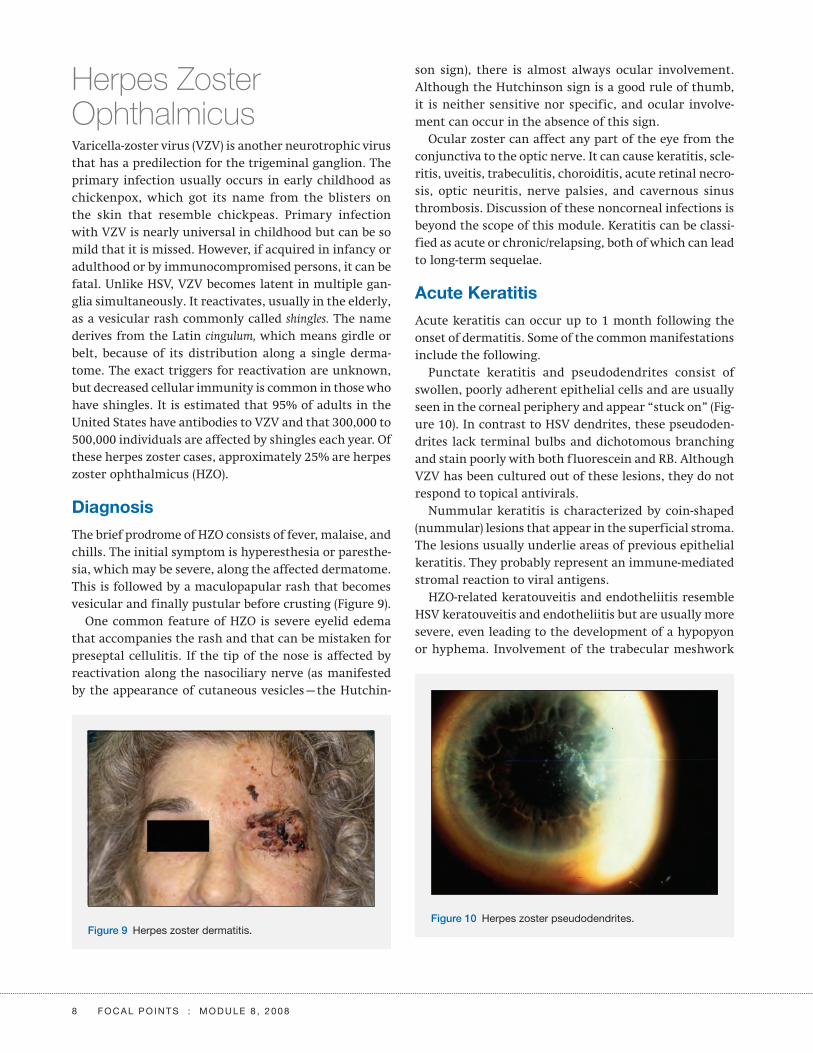
Localized endothelial dysfunction from an inflamma-tory response to viral antigen results in a disc- shaped area of corneal edema called disciform keratitis (Figure 7). There is minimal inflammation in the stroma, although focal keratic precipitates underlying the edema are characteristic. Pseudoguttae and Descemet’s folds in the edematous area may cause disciform keratitis to be confused with Fuchs dystrophy. However, in disciform keratitis, the contralateral cornea is normal, as HSV endotheliitis is almost always unilateral; Fuchs dystro-phy is always bilateral. Diffuse endotheliitis is rare and is usually accompanied by trabeculitis with elevated intra-ocular pressure.
In keratouveitis, uveitis predominates and is usually granulomatous, with large “mutton-fat” keratic pre-cipitates on the endothelium (Figure 8). It is usually
Figure 5 Metaherpetic or trophic ulceration. (Reprinted with permission from eMedicine.com, 2007. Available at: www.emedicine.com/oph/topic100.htm)
Figure 6 Necrotizing keratitis.
Figure 7 Disciform keratitis.
Figure 8 Keratouveitis with mutton- fat keratic precipitates.

F O C A L P O I N T S : M O D U L E 8 , 2 0 0 8 5
Diagnosis
Diagnosis of HSV epithelial keratitis is usually made based on clinical findings, and laboratory tests are sel-dom needed. Laboratory tests are of no use in stromal keratitis. The following tests can be useful in challenging cases of epithelial keratitis.
Herpes Culture. Various viral transport media (eg, Rich-ards viral transport, HH medium) can be used. The virus, once grown, can be typed to HSV-1 or HSV-2. A practical point is that RB is virucidal, and cultures done following RB corneal staining may be falsely negative for HSV.
Fluorescent Antibody (FAB) Testing. The corneal swab can be smeared on a slide, or impression cytology using a nitrocellulose membrane can be performed. Use of f luo-rescein staining before FAB testing interferes with test results.
DNA Amplification. This test does not require a high number of viral particles, but it is more expensive than the other tests mentioned here.
Tzanck Smear. Papanicolaou or Giemsa stains of corneal smears are examined for the presence of multinucleated giant cells and intranuclear eosinophilic inclusion bodies (Cowdry type A).
Serum Antibody Testing. This is of limited use. The pres-ence of anti-HSV IgM in a child may indicate active infec-tion. However, false negatives are common and positive titers in adults merely indicate past infection, which is nearly universal.
Long-Term Complications
Unfortunately, resolution of HSK does not protect the eye from future complications.
Recurrent disease is the major cause of the morbid-ity associated with HSK. Each recurrent episode causes increased inf lammation and scarring and further decreased corneal sensation. In addition, the risk of stro-mal disease increases with multiple recurrences of HSV epithelial keratitis.
Even when HSK is treated promptly, scarring is com-mon and can cause significant morbidity. A recurrent episode usually occurs adjacent to the site of a previ-ous episode—thus the visual axis is invariably involved eventually.
Corneal hypesthesia is a sensitive sign of previous HSK. The lack of innervation causes poor tear production and
decreased release of growth factors in response to injury, leading to persistent epithelial defects and neurotrophic ulcers that may melt and perforate.
Treatment
Treatment of HSV epithelial keratitis differs dramati-cally from that of HSV stromal keratitis, ref lecting the differing pathogeneses of these diseases. (See “Herpetic Eye Disease Study” for additional information.)
Infectious Epithelial Keratitis. Epithelial keratitis often resolves spontaneously; however, the aim of treatment is to minimize scarring and stromal inflammation. The infected cells are poorly adherent, and gentle wiping debridement with a cotton- tipped applicator removes nearly all infected cells without damaging normal epi-thelium. Debridement results in much faster resolution and consequently less scarring. Debridement should be performed prior to initiating drug therapy.
The mainstay of treatment in the United States is topi-cal trif luridine, which is very effective and should result in complete resolution. Topical acyclovir ointment, how-ever, is the drug of choice in most other parts of the world because of low toxicity. It is not commercially available in the United States but can be formulated at compounding pharmacies. Topical acyclovir ointment may be used in children, in whom frequent drops would be impractical, and in patients with trif luridine allergy. Oral acyclovir may be another option for both pediat-ric and allergic patients. A good rule of thumb is that epithelial disease that is adequately treated but persists beyond 2 or 3 weeks is either metaherpetic (noninfec-tious), caused by virus that is resistant to the antiviral agent, or due to drug toxicity. If culture of persistent epithelial disease is negative, it should be treated as a metaherpetic ulcer.
Stromal Keratitis. The mainstay of treatment is topical corticosteroids. Although HEDS did not show any statis-tically significant difference in visual outcome with the use of corticosteroids, they do accelerate resolution of HSV ocular infection. Simultaneous oral antiviral pro-phylaxis decreases the risk of HSV reactivation at the ganglion level. Some authors advocate matching topi-cal antivirals drop for drop with topical corticosteroids. Because doing so does not prevent reactivation at the ganglion level and may increase toxicity, this author does not advise this, except in the treatment of necrotizing keratitis. In that case, aggressive antivirals—both topical and systemic—and corticosteroid use are indicated.
Herpetic Eye Disease StudyThe HEDS was a prospective, randomized, double- masked, placebo- controlled multicenter study to assess the effect of adding topical corticosteroids and oral acy-clovir to conventional antiviral therapy (topical trifluridine, Viroptic) for HSV keratitis and iridocyclitis. There were six parts to the study: three therapeutic, two preventive, and one cohort. The main findings are summarized here.
Herpes Stromal Keratitis, Not on Steroid Trial (HEDS-SKN). Compared with the placebo group, the patients who had received prednisolone phosphate drops had faster resolution of the stromal keratitis and fewer treatment failures. However, delaying the initiation of corticosteroid treatment did not affect the eventual outcome of the disease, in that visual acuity was similar in the two groups at 26 weeks.
Herpes Stromal Keratitis, on Steroid Treatment (HEDS-SKS). There was no apparent benefit to adding oral acyclovir to the treatment regimen of a topical corti-costeroid and trifluridine.
Herpes Simplex Virus Iridocyclitis, Receiving Topical Steroids (HEDS-IRT). The trial was stopped because of slow recruitment, but treatment failures occurred at a higher rate in the placebo group than in the acyclovir group, indicating a potential benefit to adding oral acyclovir to the regimen of a topical steroid and an antiviral.
Herpes Simplex Virus Epithelial Keratitis Trial (HEDS-EKT). This trial assessed the effect of adding oral acyclovir to topical antiviral therapy for acute HSV epithelial keratitis. The addition of oral acyclovir provided no benefit in preventing the development of stromal keratitis or iritis. Incidentally, the study found that in the control group (treatment with trifluridine alone), the risk
of stromal keratitis or iridocyclitis was quite low in the year after an episode of epithelial keratitis; this risk was lower than that previously suggested in the literature.
Acyclovir Prevention Trial (HEDS-APT). In patients who had had an ocular HSV infection in the previous year, use of oral acyclovir reduced by 41% the prob-ability that any form of HSK would return. The incidence of epithelial keratitis was reduced from 11% to 9% and of stromal keratitis from 13% to 8%. Importantly, the rate of recurrent HSV stromal keratitis decreased 50%. Unfortunately, the effect did not persist once the acy-clovir was discontinued. More than one recurrence was reported in 4% of patients in the acyclovir group and in 9% of those in the placebo group.
Ocular HSV Recurrence Factor Study (HEDS-RFS). No association was found between psychological or other forms of stress and ocular HSV recurrences. Also, previous episodes of HSV epithelial keratitis were not a predictor of future occurrences, whereas previous, especially multiple, episodes of HSV stromal keratitis markedly increased the probability of subsequent stro-mal keratitis.
Limitations. Although HEDS was excellent in its conception and plan, it had some limitations. First, many of the trials had inadequate recruitment or a very high dropout rate. Second, in the prevention trials, oral acyclovir was used for only 3 weeks. Third, the cortico-steroid regimen was standardized and not tailored to an individual patient’s inflammation. Finally, trifluridine was used in both the study group and the placebo group in the trials evaluating acyclovir for the treatment of stro-mal keratitis and iridocyclitis.
6 F O C A L P O I N T S : M O D U L E 8 , 2 0 0 8

F O C A L P O I N T S : M O D U L E 8 , 2 0 0 8 7
Metaherpetic Keratitis. The basic principle of therapy for this disease is to rapidly heal the epithelial defect. Methods to accomplish this include stopping use of toxic medications, performing punctal occlusion, instilling tear film supplements, fitting a bandage contact lens, amniotic membrane grafting, tarsorrhaphy, and, if there is significant underlying inflammation, cautiously using topical corticosteroids while watching carefully for cor-neal melts.
Prophylaxis and Medications. Oral antivirals are typi-cally used as systemic prophylaxis against reactivation of HSV at the ganglion level. Topical medications are toxic with prolonged usage and are usually reserved for acute epithelial disease. Prophylaxis is useful in patients who have multiple recurrences (two or more in one year); those who have scarring close to the visual axis; those who are using topical corticosteroids for stromal disease; and those who are systemically immunocompromised. For prophylaxis of HSV infection, acyclovir is most com-monly used at a dosage of 400 mg twice daily.
All the current antivirals used in the treatment of ocular HSV (see Table 1) are nucleoside analogues that inhibit viral replication by competitively inhibiting viral DNA polymerase. As they may also interfere with host DNA synthesis, they can cause significant toxicity. Acy-
clovir is the most specific for viral polymerase and thy-midine kinase and therefore causes the least cellular toxicity of these antivirals; however, it is the most likely to induce viral resistance.
Topical antivirals are the drugs of choice for acute epithelial disease. Trif luridine is effective in the treat-ment of epithelial keratitis but can cause significant epithelial toxicity as mentioned above. It also contains thimerosal as a preservative and has a highly acidic pH that adds to its toxicity. Trif luridine has a short half- life and must be used every 2 hours. Systemic antivirals are used primarily for prophylaxis of recurrent disease or as an antiviral cover during corticosteroid therapy for stro-mal keratitis. The three main systemic antivirals for the treatment of HSK are acyclovir, valacyclovir, and fam-ciclovir. They have a high therapeutic index but resis-tance is an issue, especially in immunocompromised patients. Unfortunately there is cross- resistance among these three agents.
Topical corticosteroids used for the treatment of HSV stromal keratitis and uveitis are always given under anti-viral cover. Typically, 1% prednisolone acetate or 0.1% dexamethasone is used. The dosing frequency should be based on the severity of the inf lammation. On resolu-tion of the inflammation, the steroids need to be tapered gradually to prevent rebound inflammation.
Table 1. Antiviral Medications Used for the Treatment of Ocular Herpes Simplex Virus
D R U G ( T R A D E N A M E )
R O U T E / D O S A G E
F O R M D O S E F R E Q U E N C Y C O M M E N T S
Trifluridine (Viroptic) Topical drops 1% Every 2 hours Adverse effects include follicular conjunctivitis, redness, delayed epithelial healing.
Vidarabine (Ara-A) Topical ointment 3% 5 times a day Adverse effects same as for trifluridine. Can be obtained from compounding pharmacy.
Acyclovir (Zovirax) Topical ointment 3% 5 times a day Minimal adverse effects. Not commercially available in the US. Can be obtained from compounding pharmacy.
Oral 400 mg 5 times a day for treatment and twice a day for prophylaxis
Adverse effects include headache, nausea, nephrotoxicity, neurotoxicity.
Valacyclovir (Valtrex) Oral 500 mg 3 times a day for treatment and twice a day for prophylaxis
Adverse effects same as for acyclovir; thrombotic thrombocytopenic purpura and hemolytic uremic syndrome in immunosuppressed persons.
Famciclovir (Famvir) Oral 250 mg 3 times a day for treatment and twice a day for prophylaxis
Adverse effects same as for acyclovir.
8 F O C A L P O I N T S : M O D U L E 8 , 2 0 0 8
Herpes Zoster OphthalmicusVaricella-zoster virus (VZV) is another neurotrophic virus that has a predilection for the trigeminal ganglion. The primary infection usually occurs in early childhood as chickenpox, which got its name from the blisters on the skin that resemble chickpeas. Primary infection with VZV is nearly universal in childhood but can be so mild that it is missed. However, if acquired in infancy or adulthood or by immunocompromised persons, it can be fatal. Unlike HSV, VZV becomes latent in multiple gan-glia simultaneously. It reactivates, usually in the elderly, as a vesicular rash commonly called shingles. The name derives from the Latin cingulum, which means girdle or belt, because of its distribution along a single derma-tome. The exact triggers for reactivation are unknown, but decreased cellular immunity is common in those who have shingles. It is estimated that 95% of adults in the United States have antibodies to VZV and that 300,000 to 500,000 individuals are affected by shingles each year. Of these herpes zoster cases, approximately 25% are herpes zoster ophthalmicus (HZO).
Diagnosis
The brief prodrome of HZO consists of fever, malaise, and chills. The initial symptom is hyperesthesia or paresthe-sia, which may be severe, along the affected dermatome. This is followed by a maculopapular rash that becomes vesicular and finally pustular before crusting (Figure 9).
One common feature of HZO is severe eyelid edema that accompanies the rash and that can be mistaken for preseptal cellulitis. If the tip of the nose is affected by reactivation along the nasociliary nerve (as manifested by the appearance of cutaneous vesicles—the Hutchin-
son sign), there is almost always ocular involvement. Although the Hutchinson sign is a good rule of thumb, it is neither sensitive nor specific, and ocular involve-ment can occur in the absence of this sign.
Ocular zoster can affect any part of the eye from the conjunctiva to the optic nerve. It can cause keratitis, scle-ritis, uveitis, trabeculitis, choroiditis, acute retinal necro-sis, optic neuritis, nerve palsies, and cavernous sinus thrombosis. Discussion of these noncorneal infections is beyond the scope of this module. Keratitis can be classi-fied as acute or chronic/relapsing, both of which can lead to long- term sequelae.
Acute Keratitis
Acute keratitis can occur up to 1 month following the onset of dermatitis. Some of the common manifestations include the following.
Punctate keratitis and pseudodendrites consist of swollen, poorly adherent epithelial cells and are usually seen in the corneal periphery and appear “stuck on” (Fig-ure 10). In contrast to HSV dendrites, these pseudoden-drites lack terminal bulbs and dichotomous branching and stain poorly with both f luorescein and RB. Although VZV has been cultured out of these lesions, they do not respond to topical antivirals.
Nummular keratitis is characterized by coin- shaped (nummular) lesions that appear in the superficial stroma. The lesions usually underlie areas of previous epithelial keratitis. They probably represent an immune- mediated stromal reaction to viral antigens.
HZO-related keratouveitis and endotheliitis resemble HSV keratouveitis and endotheliitis but are usually more severe, even leading to the development of a hypopyon or hyphema. Involvement of the trabecular meshwork
Figure 9 Herpes zoster dermatitis.Figure 10 Herpes zoster pseudodendrites.
F O C A L P O I N T S : M O D U L E 8 , 2 0 0 8 9
can lead to severe glaucoma that may be unresponsive to glaucoma medications but responds to steroids.
Sclerokeratitis occurs as a crescent- shaped corneal infiltrate adjacent to an area of scleritis. It is clinically identical to nonherpetic peripheral ulcerative keratitis, and the etiology is thought to be limbal vasculitis and ischemia.
Chronic/Relapsing Keratitis
This form occurs up to several months following the ini-tial HZO infection.
Mucous plaques can occur suddenly in an eye that has been nearly quiescent. They appear as stuck- on, gray-ish, branching lesions and have minimal underlying inf lammation (Figure 11). Mucous plaques stain with RB, and they can be easily wiped off the cornea, leav-ing an underlying epithelium that is intact but poorly adherent. Therefore, they are thought to be a variant of filamentary keratitis, although some investigators have found viral DNA in the lesions. Mucous plaques can be highly resistant to treatment, and multiple recurrences can lead to scarring.
Disciform keratitis is similar to the disciform keratitis seen in HSK.
Interstitial keratopathy: HZO keratitis can lead to vas-cularization, with a leash of vessels leading up to the area of scarring. These vessels can exude large amounts of lipid that can cause significant corneal opacification.
Long-Term Complications
As in HSV keratitis, neurotrophic ulcers can occur repeat-edly and cause problems long after the acute episode has resolved. In contrast to HSV keratitis, however, profound loss of corneal sensation can result from a single episode of HZO, and these ulcers are more likely to perforate.
Herpes zoster can result in a persistent smoldering keratitis that may only manifest as a corneal haze with overlying epithelial irregularity. This can lead to progres-sive scarring and decrease in vision.
Neuralgia is almost always associated with acute HZO, but pain that lasts longer than 1 month constitutes postherpetic neuralgia (PHN), perhaps the most debil-itating sequela of HZO. PHN occurs in 10% to 30% of patients with HZO, and its risk factors include increas-ing age, prodromal pain, more severe rash, greater acute pain, and ophthalmic involvement. The pain is of vari-able quality and has been described by patients as burn-ing, shooting, sharp, throbbing, or tender. One classic feature of this pain is allodynia (pain following a stim-ulus that is normally non- noxious, such as wind). The pain can be severe and unrelenting and can take over the patient’s life, resulting in decreased functioning and increased risk of depression and suicide.
Treatment
Topical antivirals have no role in the treatment of HZO. However, oral antivirals begun within 72 hours of onset of symptoms can reduce the severity of the disease and of any long- term complications, including PHN. Recent studies have indicated that in certain populations, such as immunocompromised patients, this 72-hour window can be extended. For every patient with HZO, oral acyclo-vir can be used, 800 mg 5 times a day, for 7 to 14 days, regardless of the stage of the disease, because the risks associated with use of this drug are low. Valacyclovir and famciclovir can also be used but are more expensive. For the treatment of HZO, a good rule of thumb is to double the doses of the medications used for HSV keratitis.
The use of corticosteroids for the treatment of HZO is controversial. Systemic corticosteroids have been shown to reduce the dermatitis and acute pain of HZO, but they do not have any effect on PHN. Also, their use may increase the risk of ocular complications such as mucous plaques and keratitis. Topical corticosteroids may be nec-essary for treating uncontrolled inflammation. However, once they are initiated, it is difficult to wean patients from them. Sudden discontinuation of corticosteroids may allow the suppressed inf lammation to rebound; thus, corticosteroids must be tapered gradually to a level that minimizes the risk of rebound inflammation, but keeps the keratitis in check. The ophthalmologist should discuss with the patient the possibility that use of a mild steroid (f luorometholone or loteprednol, two to three times per week) may be necessary indefinitely, because complete tapering of ophthalmic corticosteroids is not always attainable.Figure 11 Mucous plaques.
10 F O C A L P O I N T S : M O D U L E 8 , 2 0 0 8
As most long- term complications of HZO are related to the neurotrophic status and relative dryness of the affected eye, ocular surface support can decrease the risk of a poor outcome. Punctal occlusion, artificial tears, bandage contact lenses, tarsorrhaphy, eyelid reconstruc-tive surgery, and conjunctival f laps all have a role to play in the treatment of the various HZO complications. Tarsorrhaphy is especially useful in recalcitrant cases of neurotrophic keratitis.
As the treatment of PHN is challenging and often frus-trating for both the clinician and the patient, it is impor-tant to give the patient the following information: (1) in most cases, the pain associated with PHN resolves sponta-neously (70% of those with pain at 1 month will be pain free at 1 year); and (2) treatment is able to “take the edge off” the pain, but unable to eliminate pain completely.
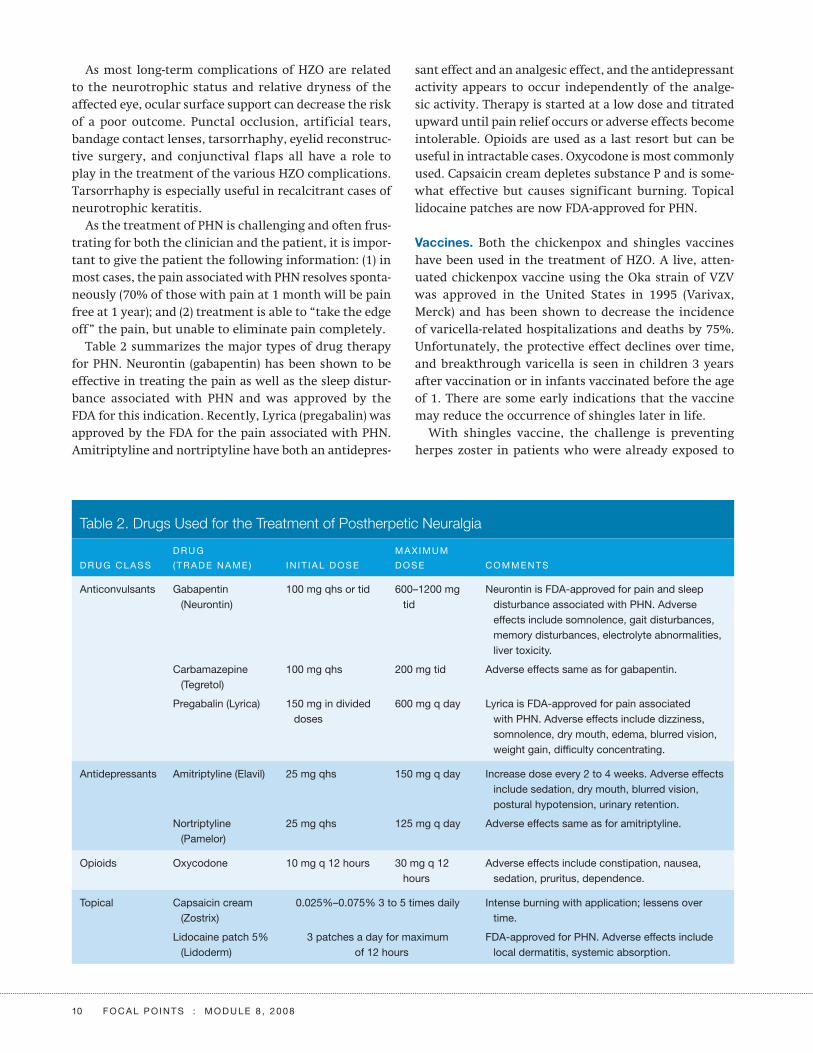
Table 2 summarizes the major types of drug therapy for PHN. Neurontin (gabapentin) has been shown to be effective in treating the pain as well as the sleep distur-bance associated with PHN and was approved by the FDA for this indication. Recently, Lyrica (pregabalin) was approved by the FDA for the pain associated with PHN. Amitriptyline and nortriptyline have both an antidepres-
sant effect and an analgesic effect, and the antidepressant activity appears to occur independently of the analge-sic activity. Therapy is started at a low dose and titrated upward until pain relief occurs or adverse effects become intolerable. Opioids are used as a last resort but can be useful in intractable cases. Oxycodone is most commonly used. Capsaicin cream depletes substance P and is some-what effective but causes significant burning. Topical lidocaine patches are now FDA- approved for PHN.
Vaccines. Both the chickenpox and shingles vaccines have been used in the treatment of HZO. A live, atten-uated chickenpox vaccine using the Oka strain of VZV was approved in the United States in 1995 (Varivax, Merck) and has been shown to decrease the incidence of varicella- related hospitalizations and deaths by 75%. Unfortunately, the protective effect declines over time, and breakthrough varicella is seen in children 3 years after vaccination or in infants vaccinated before the age of 1. There are some early indications that the vaccine may reduce the occurrence of shingles later in life.
With shingles vaccine, the challenge is preventing herpes zoster in patients who were already exposed to
Table 2. Drugs Used for the Treatment of Postherpetic Neuralgia
D R U G C L A S S
D R U G
( T R A D E N A M E ) I N I T I A L D O S E
M A X I M U M
D O S E C O M M E N T S
Anticonvulsants Gabapentin (Neurontin)
100 mg qhs or tid 600–1200 mg tid
Neurontin is FDA- approved for pain and sleep disturbance associated with PHN. Adverse effects include somnolence, gait disturbances, memory disturbances, electrolyte abnormalities, liver toxicity.
Carbamazepine (Tegretol)
100 mg qhs 200 mg tid Adverse effects same as for gabapentin.
Pregabalin (Lyrica) 150 mg in divided doses
600 mg q day Lyrica is FDA- approved for pain associated with PHN. Adverse effects include dizziness, somnolence, dry mouth, edema, blurred vision, weight gain, difficulty concentrating.
Antidepressants Amitriptyline (Elavil) 25 mg qhs 150 mg q day Increase dose every 2 to 4 weeks. Adverse effects include sedation, dry mouth, blurred vision, postural hypotension, urinary retention.
Nortriptyline (Pamelor)
25 mg qhs 125 mg q day Adverse effects same as for amitriptyline.
Opioids Oxycodone 10 mg q 12 hours 30 mg q 12 hours
Adverse effects include constipation, nausea, sedation, pruritus, dependence.
Topical Capsaicin cream (Zostrix)
0.025%–0.075% 3 to 5 times daily Intense burning with application; lessens over time.
Lidocaine patch 5% (Lidoderm)
3 patches a day for maximum of 12 hours
FDA-approved for PHN. Adverse effects include local dermatitis, systemic absorption.

F O C A L P O I N T S : M O D U L E 8 , 2 0 0 8 11
and have latent VZV. A large clinical trial conducted by Merck and the Department of Veterans Affairs in col-laboration with the National Institute of Allergy and Infectious Diseases at the National Institutes of Health found that a higher dose of the same attenuated virus (Zostavax, Merck) reduced the incidence of herpes zoster by 51.3% and of PHN by 66.5% over 3 years. It is now rec-ommended for all individuals over the age of 60. It does not treat zoster or PHN, and there is no information on whether this vaccine should be administered to patients who have already had zoster.
ConclusionPrimary HSV infection is usually unrecognized; clinical disease is usually the result of reactivation of latent her-pes simplex virus. Lack of corneal sensation is a sensi-tive sign of prior HSV corneal infection. Dendritic and geographic epithelial ulcers are caused by live virus and are best treated with topical antiviral medications, such as trif luridine. Stromal keratitis is an immune- mediated process and is best treated with topical corticosteroids, with oral antiviral prophylaxis. Neurotrophic (metaher-petic) ulcers are neither infectious nor immune- mediated
and are treated with measures to promote epithelial healing.
The most important findings of HEDS were that use of topical corticosteroids shortened the course of HSV stro-mal keratitis, but did not alter the final outcome, and prophylactic treatment with oral acyclovir decreased the risk of recurrent HSV ocular infection by 41%.
VZV keratitis is usually a self- limited disease but can persist for years. Topical antivirals are not useful for this condition. The use of systemic antiviral medications at a high dose within 72 hours of the onset of symptoms reduces the incidence of ocular morbidity, including PHN. PHN is a significant source of debilitating symp-toms from VZV. The use of oral corticosteroids to reduce the risk of PHN is controversial. Vaccines are available for chickenpox and shingles.
Sonal S. Tuli, MD, is the director of Cornea and External Diseases Service and assistant professor at the University of Florida College of Medicine, Gainesville, Florida.

12 F O C A L P O I N T S : M O D U L E 8 , 2 0 0 8
Clinicians’Corner
Clinicians’ Corner provides additional viewpoints on
the subject covered in this issue of Focal Points. Con-
sultants have been invited by the Editorial Review
Board to respond to questions posed by the Acade-
my’s Practicing Ophthalmologists Advisory Committee
for Education. While the advisory committee reviews
the modules, consultants respond without reading the
module or one another’s responses. – Ed.
1. Are viral cultures ever necessary in the diagnosis of herpes simplex virus (HSV) keratitis? Is there any value to typing the virus (HSV-1 versus HSV-2)?
Dr. Chodosh: Viral cultures are typically negative for, and therefore not usually helpful in, herpetic stromal keratitis. Viral cultures can occasionally be useful in atypical epithelial keratitis, if the diagnosis is uncertain. At the present time, available antiviral medications work equally well for HSV-1 and HSV-2, so outside of academic interest, there is little value to differentiating the two.
Dr. Wilhelmus: For laboratory confirmation I prefer an immunoassay, but I may submit a specimen for HSV isolation when faced with deciding between HSV and another diagnosis. Some examples of this dilemma are (1) atypical dendriform epitheliopathy associated with the use of a glaucoma medication, (2) persistent epithe-lial keratitis in an immunosuppressed person, (3) severe vesicular dermatoblepharitis, and (4) recurrent blepha-roconjunctivitis or follicular conjunctivitis. Neonatal HSV-2 is a concern for pediatric ophthalmologists, and viral typing might infer the route of transmission. Not normally establishing latency in the trigeminal ganglion, HSV-2 rarely causes corneal disease in adults. Oculogen-ital spread is feasible, but I seldom find patients with both ocular and genital herpes.
2. Does debridement of the cornea have a role in the management of HSV keratitis? Are medications necessary after debridement?
Dr. Chodosh: In immune- competent individuals, herpetic epithelial keratitis is a self- limited infection and resolves without treatment. Corneal epithelial debridement in herpetic epithelial keratitis has been shown to shorten the course of infection and may be more effective when antiviral medications are used concomitantly.
Dr. Wilhelmus: Minimal wiping debridement with a dry, sterile swab can speed healing of a dendrite and is part of

F O C A L P O I N T S : M O D U L E 8 , 2 0 0 8 13
my usual treatment plan. Since a dendrite reappears in about half of debrided eyes, I almost always use adjunc-tive treatment with an antiviral agent over the week fol-lowing debridement.
3. Are stress and/or fever activators of HSV keratitis?
Dr. Chodosh: The Herpetic Eye Disease Study (HEDS), funded by the National Eye Institute, could not confirm the widely held belief that physical or emotional stress triggers reactivation of HSV and causes recurrent her-petic eye disease. Detailed analysis of the HEDS data sug-gests that the purported association between stress and HSV reactivation may be due to recall bias.
Dr. Wilhelmus: Stress rarely triggers ocular herpes, but excess sunlight and corneal injury can lead to viral shed-ding. For this reason, I may prescribe a brief course of twice- daily oral acyclovir, or its equivalent, for my HSV patients when they go snow skiing, enter a golf tour-nament, undergo LASIK or cataract surgery, or have a loose corneal suture. Because prostaglandins might be involved in HSV reactivation, aspirin or a nonsteroidal anti- inf lammatory drug might help prevent recurrent herpes in a feverish patient.
4. Is there a role for combining topical and oral antivi-rals in the management of HSV keratitis? Can den-dritic HSV keratitis be treated with oral medications alone?
Dr. Chodosh: There is no Level 1 evidence to support the use of concomitant oral and topical antiviral therapy, and HSV epithelial keratitis can be treated with oral anti-virals alone. Many corneal specialists prefer to use oral antivirals because the potential ocular surface toxicity of topical antivirals can complicate later clinical decisions.
Dr. Wilhelmus: Evidence- based ophthalmology is a goal of the Cochrane Eyes and Vision Group (www.cochraneeyes.org). The Cochrane systematic review on herpetic kerati-tis found two trials that looked at whether oral acyclovir adds any benefit over topical treatment alone: a small trial found an additive effect, but a larger trial showed little added benefit. Thus, I rarely use both topical and oral antivirals together, except for chronic viral keratitis in people with AIDS and for severe keratouveitis. Also, based on a trial in Ireland 20 years ago, I believe oral and topical antivirals are nearly equivalent for HSV epithe-
lial keratitis. I almost always prefer a topical antiviral but will change to an oral agent for severe blepharocon-junctivitis, epithelial keratitis in an immunosuppressed or thimerosal- sensitive patient, or progressive stromal keratitis or uveitis.
5. Is there a role for prophylaxis of HSV keratitis with oral antivirals?
Dr. Chodosh: The HEDS treatment trials demonstrated a reduction in the probability of recurrent HSV kerati-tis by approximately one- half when patients took oral acyclovir as compared to placebo, but did not examine who should receive antiviral prophylaxis. Subsequent cost- effectiveness studies have suggested that not every patient with HSV ocular disease should be offered antivi-ral prophylaxis. I recommend oral acyclovir prophylaxis in any patient with multiple recurrences of HSV stromal keratitis necessitating repeated or prolonged use of topi-cal corticosteroids; recurrent stromal keratitis with scar-ring and/or vascularization approaching the visual axis; or more than one episode of necrotizing HSV keratitis. I also use long- term oral antiviral prophylaxis in every patient who is undergoing corneal transplant and has a history of herpetic ocular disease.
Dr. Wilhelmus: The HEDS trials showed that long- term suppression with an oral antiviral, such as acyclovir 400 mg twice daily, reduces the recurrence rate of HSV keratitis. I advise prolonged oral antiviral prophylaxis for patients who have two or more recurrences annu-ally or whose last episode was stromal keratitis or led to a complication. As shown by recent studies from the Cornea Service at Wills Eye Hospital, atopic patients are at increased risk for HSV infections that can be sup-pressed with oral antiviral prophylaxis. A small, 1-year trial in Italy concluded that oral valacyclovir once daily is equivalent to acyclovir twice daily, but this convenience is more expensive.
6. Discuss your management of necrotizing keratitis caused by HSV.
Dr. Chodosh: Necrotizing HSV keratitis is relatively uncommon and did not occur in sufficient numbers to be studied as a separate entity in the HEDS treatment trials. HSV necrotizing keratitis can be difficult to diag-nose, as it can mimic bacterial or fungal keratitis and

14 F O C A L P O I N T S : M O D U L E 8 , 2 0 0 8
Clinicians’Corner
may have been treated with antibiotics and/or topical cor-ticosteroids prior to presentation in the clinic. There is some evidence from the laboratory that viral replication within the corneal stroma may play a role in the intense immune and neovascular response characteristic of HSV necrotizing keratitis. I treat the keratitis with 7 to 10 days of oral antiviral therapy at therapeutic doses, followed by a combination of prophylactic doses of oral antivirals and cautious treatment with topical corticosteroids (bid or less). When treated in this fashion, patients typically heal within several days of starting topical corticosteroids.
Dr. Wilhelmus: Management of herpetic necrotizing ker-atitis begins with making the correct diagnosis. Many patients with fungal keratitis or Acanthamoeba keratitis are initially treated as if they have herpetic keratitis. I would consider the possibility of microbial keratitis, syphilis, or another disease before embarking on anti-viral and corticosteroid therapy. Another caveat: severe geographic epithelial keratitis may coexist with stromal inflammation, and antiviral therapy is needed for these eyes before corticosteroids. For HSV necrotizing stromal keratitis, I begin topical prednisolone phosphate 1% or prednisolone acetate 1%, at a dosing frequency of four to eight times per day, according to disease severity. I use a topical antiviral as prophylaxis against recurrent epithelial keratitis. I may switch to an oral antiviral if there is an allergic or toxic reaction to trif luridine or if stromal keratouveitis responds slowly to corticosteroids. The topical corticosteroid is tapered over the next several weeks as corneal inflammation diminishes.
7. What are your “pearls” for managing penetrating keratoplasty in patients with HSV?
Dr. Chodosh: First and foremost, I begin an oral antiviral at therapeutic doses several days prior to surgery. I taper the antiviral over the first year after keratoplasty, until I reach prophylactic dose levels, and then maintain the medication indefinitely. Patients are instructed that they will need to take the oral antiviral for life. Otherwise, my use of topical corticosteroids is the same as with other keratoplasty patients. I use interrupted corneal sutures so that individual sutures can be removed as necessary. Patients with significant postherpetic corneal hypesthe-
sia prior to keratoplasty surgery may require permanent punctal occlusion and occasionally tarsorrhaphy to pre-vent postoperative complications.
Dr. Wilhelmus: I worry about undertaking corneal graft-ing in patients with herpetic keratitis because recur-rent herpes, allograft rejection, and other complications increase the risk of graft failure. Therefore, unless per-foration is about to happen, I consider surgery only after the eye has been noninflamed for several months and the patient has tapered corticosteroid treatment to the desired level. Shortly before grafting, I may restart the topical corticosteroid and oral antiviral, in hopes that graft inf lammation, corneal neovascularization, and viral reactivation will be less after surgery. I prefer interrupted sutures for these grafts and will use a topical corticosteroid and oral antiviral for many months post-operatively, often a year or more.
8. Is there a role for topical cyclosporine (Restasis) in the management of HSV keratitis? Should Resta-sis be avoided in dry eye patients with a history of HSV?
Dr. Chodosh: Evidence exists to support both detriment and benefit to cyclosporine in HSV infections. Systemic cyclosporine has been associated with severe recalci-trant HSV infections, and ocular topical cyclosporine may delay resolution of HSV epithelial keratitis. Anec-dotal evidence also suggests a possible beneficial effect of topical cyclosporine in HSV stromal keratitis. I see no specific role for topical cyclosporine in the management of HSV keratitis, except possibly in stromal disease in the setting of corticosteroid- induced ocular hypertension. I do not avoid topical cyclosporine in patients with dry eye and a history of HSV, but I would discontinue its use in any patient with HSV epithelial keratitis.
Dr. Wilhelmus: While others have different experience, I do not use cyclosporine for treating herpetic keratitis. A history of herpetic keratitis is not a contraindication for using Restasis, although I would stop it if a dendrite occurred.

F O C A L P O I N T S : M O D U L E 8 , 2 0 0 8 15
9. What is your pharmacologic approach to the man-agement of postherpetic neuralgia in herpes zoster ophthalmicus (HZO)?
Dr. Chodosh: Historically speaking, postherpetic neural-gia was treated with topical capsaicin or low doses of oral amitriptyline or carbamazepine. However, the field of pain management has exploded with new treatment modalities, including the new drug pregabalin, reported to be a very effective medication for postherpetic pain. Furthermore, I find that patients with specific posther-petic neuralgia are very individual and do not all respond to the same treatment. Therefore, today I typically refer such patients to a qualified pain specialist familiar with the entire spectrum of available treatments.
Dr. Wilhelmus: I use oral valacyclovir or famciclovir, three times daily for 1 week, to reduce the duration of acute zoster- associated pain during shingles. The control of postzoster neuralgia is more challenging. Tricyclic antidepressants, opioids, and capsaicin cream can give some relief, but I often consult with a neurologist for neuropathic pain management. We have used oral gaba-pentin (Neurontin), beginning at a low dose and titrating upward, or more recently pregabalin (Lyrica).
10. Discuss your management of chronic keratitis fol-lowing HZO.
Dr. Chodosh: It is important to distinguish the sequelae of postherpetic corneal neuropathy from actual keratitis. In the former, punctal occlusion and tarsorrhaphy may be necessary to prevent corneal ulceration. In the latter,
recent evidence suggests that chronic epithelial keratitis after HZO may reflect ongoing and persistent varicella- zoster virus replication in the corneal epithelium, and may respond to antiviral therapy and reduction of topi-cal steroids. The stromal keratitis of HZO is treated with topical corticosteroids.
Dr. Wilhelmus: Zoster corneal disease can be difficult to control. Besides neurotrophic keratopathy, a par-ticular problem is distinguishing smoldering chronic zoster stromal keratitis from residual corneal opacifi-cation. Drs. Seitzman, Strauss, and Margolis coined the term “steel wool keratopathy” to describe a degenerative effect of chronic corneal inflammation. The stumbling block is when to use corticosteroids. Dr. Dan Jones uses the term “steroid neglect” to describe slowly progressive corneal disease that begs to be dampened by the timely use of a topical corticosteroid. Another challenge is how to taper. I reduce a steroid’s concentration and frequency gradually for herpes zoster stromal keratitis and often continue a low dose for a very long time. No antiviral prophylaxis is needed.
James Chodosh, MD, MPH, is a professor of ophthal-mology at the Dean A. McGee Eye Institute, Univer-sity of Oklahoma College of Medicine, Oklahoma City, Oklahoma.
Kirk R. Wilhelmus, MD, PhD, is a professor of ophthal-mology, Cullen Eye Institute, Baylor College of Medicine, Houston, Texas.

16 F O C A L P O I N T S : M O D U L E 8 , 2 0 0 8
Suggested Reading
Barron BA, Gee L, Hauck WW, et al. Herpetic Eye Disease
Study. A controlled trial of oral acyclovir for herpes simplex
stromal keratitis. Ophthalmology. 1994;101:1871–1882.
Herpetic Eye Disease Study Group. Acyclovir for the preven-
tion of recurrent herpes simplex virus eye disease. N Engl
J Med. 1998;339:300–306.
Herpetic Eye Disease Study Group. A controlled trial of oral
acyclovir for iridocyclitis caused by herpes simplex virus. Arch
Ophthalmol. 1996;114:1065–1072.
Herpetic Eye Disease Study Group. A controlled trial of oral
acyclovir for the prevention of stromal keratitis or iritis in
patients with herpes simplex virus epithelial keratitis. The
Epithelial Keratitis Trial. Arch Ophthalmol. 1997;115:703–712.
Erratum in: Arch Ophthalmol. 1997;115:1196. Comment in: Arch
Ophthalmol. 1998;116:259.
Herpetic Eye Disease Study Group. Psychological stress and
other potential triggers for recurrences of herpes simplex
virus eye infections. Arch Ophthalmol. 2000;118:1617–1625.
Kertes PJ, Conway MD, eds. Clinical Trials in Ophthalmology: A
Summary and Practice Guide. Philadelphia: Lippincott Williams
& Wilkins; 1998.
Khan BF, Pavan- Langston D. Clinical manifestations and treat-
ment modalities in herpes simplex virus of the ocular anterior
segment. Int Ophthalmol Clin. 2004;44:103–133.
Liesegang TJ. Herpes simplex virus epidemiology and ocular
importance. Cornea. 2001;20:1–13.
Liesegang TJ. Varicella- zoster virus eye disease. Cornea.
1999;18:511–531.
Liesegang TJ, Melton LJ III, Daly PJ, Ilstrup DM. Epidemiology
of ocular herpes simplex. Incidence in Rochester, Minn, 1950
through 1982. Arch Ophthalmol. 1989;107:1155–1159.
Pavan-Langston D. Viral disease of the ocular anterior seg-
ment: basic science and clinical disease. In: Foster CS, Azar
DT, Dohlman CH, eds. Smolin and Thoft’s The Cornea: Scientific
Foundations and Clinical Practice. 4th ed. Philadelphia: Lippincott
Williams & Wilkins; 2005:297–397.
Wilhelmus KR, Dawson CR, Barron BA, et al. Risk factors for
herpes simplex virus epithelial keratitis recurring during
treatment of stromal keratitis or iridocyclitis. Herpetic Eye
Disease Study Group. Br J Ophthalmol. 1996;80:969–972.
Wilhelmus KR, Gee L, Hauck WW, et al. Herpetic Eye Disease
Study. A controlled trial of topical corticosteroids for herpes
simplex stromal keratitis. Ophthalmology. 1994;101:1883–1895;
discussion 1895–1896.
Related Academy Materials
External Disease and Cornea. Basic and Clinical Science Course,
Section 8, 2007–2008.


029030C





























