Embed Size (px)
Citation preview

www.ineedce.com 1
FluorideGuide
$59.00
Earn
4 CE creditsThis course was
written for dentists, dental hygienists,
and assistants.
Written by Fiona M. Collins, BDS, MBA, MA and Michael Florman, DDS

ForewordOptimizing a fluoride protocol for individuals at dental caries risk is the most important measure that can be done to prevent future and arrest current disease. However, fluoride therapy remains complex and controversial. Since the introduction of water fluoridation, fluoride supplements, and topical fluoride therapies in the late 1940s, the mechanisms of action, dosages and delivery systems have been debated and have evolved.
Originally, the mechanisms of fluoride action were ascribed solely to reducing enamel solubility. Now, other mechanisms such as fluoride’s effect on remineralization and its effect on bacterial metabolism also are recognized. Similarly, the initial dosage of fluoride supplements was empirical, based on simulating fluoride exposure from optimally fluoridated water. As a result of epidemiologic studies showing mild fluorosis in some children with the original dosage and the fact that fluoride is now a ubiquitous part of a child’s diet, the fluoride supplement dosage has been altered several times over the past 30 years. These issues of dosage are further compounded by epidemiologic studies showing changing prevalence of caries and fluorosis.
Topical fluoride use in preschool children, as well, has evolved. New modalities, such as fluoride varnishes, have become more prevalent for office treatment for children because of the safety of premeasured doses, ease of application and better patient acceptance.
Overlaying both the issues of topical fluoride therapy and fluoride supplement use is the current focus on individualized therapy for patients based on caries risk. One should no longer prescribe fluoride supplements or perform a professionally applied topical fluoride treatment without considering an individual’s caries risk. Recent recommendations suggest limited use of fluoride for those at low caries risk, but significantly more frequency and intensity for those at high risk.
This Fluoride Guide addresses the current concepts of fluoride mechanism, systemic and topical therapy based on the best evidence in the literature. Not only does the Guide provide scientific rationale, it also offers the dental provider options, based on efficacy for systemic fluoride, office treatments and home-use fluoride products.
Dr. Norman TinanoffChairman of the Department of Health Promotion and Policy, University of Maryland

Educational ObjectivesThe overall goal of this article is to provide the reader with information on the use of systemic and topical fluorides for caries prevention.
Upon completion of this course, the dental professional will be able to do the following:1. List intentional and unintentional sources of systemic fluoride.2. List and describe caries risk factors and the ADA recommendations for in-office topical
fluorides corresponding to different risk levels.3. List and describe the considerations involved in selecting in-office and home-use topi-
cal fluorides.4. List and describe the various home-use topical fluorides available and the clinical
efficacy of each.
AbstractWater fluoridation heralded the use of fluoride as an anti-caries agent. Since that time, both systemic and topical fluorides have become available and the use of fluorides has contributed greatly to reducing the level of caries seen in the population. Systemic fluoride supplements are available as tablets and drops, for use in accordance with the recommendations on fluoride supplement dosing. Vehicles for topical fluorides include in-office fluoride varnishes, gels, and foams, and home-use fluoride dentifrices, rinses and prescription products. The primary mechanisms of action involved with the use of topical fluorides are the prevention of demineralization and promotion of remineralization, by ensuring the ready availability of intra-oral fluoride.
Considerations in selecting an appropriate in-office and home-use topical fluoride proto-col for individual patients include the patient’s age, caries risk level, exposure to fluoride from all sources, and the current recommendations on professionally-applied topical fluorides. Other important considerations include product efficacy and safety, the patient’s dental status as well as compliance with brushing and age-appropriate use of fluoride toothpaste, and clinician and patient preferences.

2 www.ineedce.com
IntroductionFluoride has been used in the United States as an anti-caries agent since the 1940s, when water fluoridation was first introduced. Since then, numerous agents have become available for both the systemic and topical applications of fluoride.
Currently available fluorides include sodium fluoride, sodium monofluorophosphate, acidulated phosphate fluoride and stannous fluoride. In addition to its use as a caries preventive to help prevent demineralization and aid remineralization, fluoride is used for the treatment of dentinal hypersensitivity.
The focus of this guide is on the anti-caries benefits of fluoride. Systemic and topical fluorides will be addressed, including the mechanisms of action, categories of fluoride products and evidence for their use, as well as current recommendations on systemic and topical fluorides.
Systemic fluorideIntentional sources of systemic fluoride for the prevention of caries include fluoridated water and fluoride supplements. Inadvertent (unintentional) sources include naturally oc-curring fluoride in well water, fluoride toothpaste, brewed tea, bottled water, drinks and goods processed using fluoridated water, and foods such as fish. In addition, certain medications contain fluoride. (Table 1)
Table 1. Sources of systemic fluoride
Intentional UnintentionalFluoridated water High fluoride level well waterFluoride supplements Foods containing fluorideFluoridated salt Home-use topical fluoride products,
including fluoride toothpasteFluoridated milk Medications containing fluorideFluoridated foods High fluoride level bottled water
Water fluoridationWater fluoridation was first introduced in the 1940s,1 and its use has resulted in substan-tial declines in caries rates. Water fluoridation, as a public health measure, is achieved through the addition of fluoride at water plants, typically to obtain a level of 1 ppm fluoride in drinking water. In other areas where the level of fluoride is substantially higher than the recommended level, excess fluoride can be removed during processing.

www.ineedce.com 3
Fluoride-enriched saltFluoridated salt has been used in several areas of the world, including parts of Europe and Latin America. A recent review of the literature led to the determination that there are no randomized, controlled clinical trials on the use of fluoridated salt to enable conclu-sions to be drawn as to its efficacy. The same reviewer located two studies on fluori-dated milk, one of which showed, at the conclusion of the study, a significant reduction in caries in children age 8 after three years of use.2
Fluoride supplementsFluoride supplements can be given to at-risk children as drops, lozenges or tablets, with the dose varying with the level of fluoride contained in the domestic water supply and age of the child. The use of fluoride supplements by pregnant women does not result in any benefit for the baby.
• Current recommendations from the American Academy of Pediatric Dentistry, Ameri-can Dental Association and American Academy of Pediatrics are to start fluoride supplements, if required, at 6 months3,4 (Table 2)
• The Centers for Disease Control and Prevention (CDC) suggests that fluoride supple-ments be given to children living in areas with suboptimal water fluoridation who are at high risk of caries5
• Chewing or sucking fluoride tablets and lozenges prior to swallowing will maximize the effect of these supplements by providing an additional topical effect.
Table 2. Recommended fluoride supplement dosing (mg/day)
Fluoride in domestic water supply Age of Child < 0.3 ppm 0.3-0.6 ppm > 0.6 ppm
Up to 6 months None None None
6 months to 3 years 0.25 mg/day None None
3-6 years 0.5 mg/day 0.25 mg/day None
6-16 years 1.0 mg/day 0.5 mg/day None
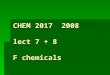
Systemic fluoride and mechanisms of actionDuring tooth development, the cumulative ingestion of fluoride prior to pre-eruptive enamel maturation results in fluoride ions replacing hydroxyl ions and the formation of fluorapatite crystals instead of hydroxyapatite crystals.6 (Figure 1) The fluorapatite crystals are smaller and stronger than hydroxyapatite crystals and are more resistant to demineral-ization associated with the dental caries process. Recent reviews have suggested that the effect of fluoride, including that contained in supplements, foods and drinks, is mainly the result of its topical effect.7,8,9

4 www.ineedce.com
Figure 1. Crystal formation and fluoride substitution
Ca++
O–
POHCa++
O––O
O
Ca++
O–
PFCa++
O––O
O
Hydroxyapatite Fluorapatite
Substitution
of �uoride
Ingested fluoride works through a number of mechanisms:• Systemic fluoride use results in a concentration of fluoride of 1,000 – 2,000 ppm in
the outer layer of the enamel• The remainder of the enamel contains about 20 –100 ppm• Pre-eruptively, formed enamel is bathed in plasma that contains fluoride and contrib-
utes to the outer fluoride-rich layer• Post-eruptively, the enamel is bathed in fluoride contained in saliva and crevicular
fluid, that was derived from systemically absorbed (ingested) fluoride• Both the fluoride-rich layer and the inner layers of the enamel containing 20 – 100
ppm fluoride are still susceptible to acid attacks10 • Ongoing caries prevention from fluoridated water and other fluoride-containing drinks
and/or foods also occurs as a result of their direct topical effect with some retention of fluoride intra-orally on the teeth and in dental biofilm (plaque). Inadvertent ingestion of excessive amounts of fluoride during enamel development,
from all sources combined, can result in fluorosis and is dependent on the dose, age of the child and duration of excessive fluoride ingestion. A risk of fluorosis with regular use of fluoride supplements and toothpaste has been found, underscoring the importance of total fluoride ingestion when prescribing supplements.11
Fluorosis Fluoride sources that may contribute to a high total level of fluoride ingested, and therefore fluorosis, include high-fluoride-level well water, foods and drinks containing high levels of fluoride, the repeated ingestion of fluoride intended for topical use only and certain medications. • Mild fluorosis results in white mottled areas of enamel as a result of hypomineraliza-
tion, which can be a cosmetic concern in the anterior dentition Severe fluorosis can result in pitted and malformed areas of enamel, brittle enamel, breakdown of areas of enamel and teeth with abnormal morphology
• Fluorosis seen in the United States is generally very mild or mild12 • Severe fluorosis is more common in areas with high-fluoride-level well water• For fluorosis to occur, excess fluoride must be ingested prior to pre-eruptive enamel
maturation; ingestion after this developmental phase cannot result in fluorosis• Fluorosis as a result of excess ingestion of fluoride from age 6 onward is not a con-
cern as pre-eruptive enamel maturation of the anterior (and majority) of the dentition has been completed by then and for all of the dentition by age 8
• Topical fluorides are relevant for fluorosis only if inadvertently swallowed.

www.ineedce.com 5
Topical fluoridesTopical fluorides are available as in-office fluorides and home-use fluorides. Topical fluorides act intra-orally by:• Providing periodic high doses of fluoride (in-office) • Providing low regular doses of fluoride (home-use).
Topical fluorides available in the United States include:• Sodium fluoride • Sodium monofluorophosphate • Acidulated phosphate fluoride (or acidulated sodium fluoride) • Stannous fluoride • Fluoride from glass ionomer cements • Other fluoride-releasing dental materials.
Acidulated formulations were first investigated with the goal of increasing fluoride uptake and ion exchange through the use of a low pH. These included phosphate to prevent dissolution of dental hard tissues.13,14 Other investigators focused on formula-tions that had the potential to bind the fluoride to the tooth surface or to prolong the application for greater fluoride release and availability.
Caries and the mechanism of action of topical fluorideDental caries is a multifactorial infectious disease that always requires the presence of cariogenic bacteria – primarily mutans streptococci (Streptococcus mutans and S. sobrinus) as well as lactobacilli. These bacteria metabolize fermentable carbohydrates, producing acid that is capable of demineralizing dental hard tissues at below pH 5.5, under conditions favoring this. During acid attacks, subsurface dissolution occurs at pH 3.8 – 4.8, with the loss of calcium and phosphate ions from the crystals. The intra-oral pH rebounds approximately 30 minutes after an acid attack, during which time reminer-alization with calcium phosphate and fluoride ions occurs at the site of demineralization.
DURING ACID ATTACkS, SUBSURFACE DISSOLUTION OCCURS AT pH 3.8 – 4.8, WITH DEMINERALIzATION AND THE LOSS OF CALCIUM AND PHOSPHATE IONS
FROM THE CRySTALS. IN DENTIN, UNHINDERED DISEASE PROGRESSION IS MORE RAPID DUE TO COLLAGEN FIBRIL DEGRADATION.
As a result of repeated episodes of demineralization (and in the absence of reminer-alization), white spots may appear due to subsurface demineralization. In orthodontic pa-tients, these white spots can be found adjacent to brackets in particular and are referred to as orthodontic decalcifications.15 Unhindered, once sufficient subsurface structure has been lost, the surface collapses and cavitation occurs. Disease progression is more rapid in dentin as demineralization of the dentin is followed by enzymatic degradation of the exposed collagen fibrils.16,17 (Figure 2, 3)

6 www.ineedce.com
Figure 2. Caries process: demineralization and remineralization
Demineralization RemineralizationpH pH
Acid Attack
Ca++
Ca++
PO4
PO4
Ca++
PO4
Ca++
PO4
Drop in pH as a result of an acid attack results in loss of ions and demineralization of the tooth structure; under favorable conditions, this is followed by the migration of ions to the site of the
lesion and remineralization.
Figure 3. Destructive phase of the caries process in dentin
Demineralization Degradation of collagen �brils
+Ca++
Ca++
PO4
PO4
Drop in pH as a result of an acid attack results in loss of ions and demineralization of the tooth structure; if the lesion is not remineralized, this is followed by degradation of the exposed collagen
fibrils resulting in more rapid progression of caries in dentin than in enamel.
Anti-caries benefit of fluorideThe anti-caries benefit derived from topical fluorides can be attributed primarily to the prevention of demineralization and the promotion of remineralization. Ensuring the ready availability of intra-oral fluoride helps prevent demineralization from occurring and, should it occur, aids remineralization. The application of high concentrations of topical fluoride results in the formation of alkali-soluble calcium fluoride-like globules at the tooth surface, the amount being influenced by the length of application and the con-centration of fluoride used. These globules act as a fluoride reservoir and have been observed with scanning electron microscopy.18,19,20 It is believed that the phosphate associated with these globules is responsible for their stability at a normal pH. When

www.ineedce.com 7
acid attacks occur, the globules start to break down and release calcium, phosphate and fluoride, resulting in a higher concentration of these ions at the tooth surface than internally. These then migrate to demineralized sites and remineralize these defects, also forming fluoridated hydroxyapatite. (Figure 4)
At lower concentrations of topical fluoride (as used in dentifrices and rinses), fluo-ride is retained in solution in saliva as well as being retained as alkali-soluble calcium fluoride. Thus, topical fluorides result in the retention of fluoride on the tooth surface; in saliva and dental plaque; and on intra-oral soft tissues, especially the tongue and lower posterior vestibule of the mouth.18,19,21
Figure 4. Fluoride adsorption and caries control
Ca++
Ca++
PO4
PO4
F-
F-
F-
F-
F-
Acid Attack
Acid Attack
F-
F-
High concentrations of topical fluorides result in the formation of calcium fluoride-like globules. These are stable until exposed to acid, when they release calcium, phosphate and fluoride. Low concentrations
of topical fluorides also result in the presence of bioavailable fluoride in plaque, saliva and oral mucosa. Together, these mechanisms provide for reservoirs of fluoride available during acid attacks.
Topical fluoride is also believed to inhibit caries activity through bacterial inhibition.16 (Figure 5)
Figure 5. Bacterial inhibition
Hydrogen fluoride molecules enter the bacterial cell
Fluoride and hydrogen dissociate, enabling fluoride activity inside the cell
Fluoride-induced inhibition of enzymes responsible for carbohydrate metabolism
Fluoride combines with hydrogen and then enters the bacterial cell. Following entry into the cell, the fluoride and hydrogen dissociate and the fluoride inhibits enyzmes involved in bacterial metabolic processes; this includes inhibition of
enolase that metabolizes fermentable carbohydrates, thereby reducing the production of acid involved in the caries process.

8 www.ineedce.com
Most of the topical effect of fluoride is due to the presence of available fluoride rath-er than the influence of fluoride uptake during fluoride therapy (in-office or home-use). As previously mentioned, ingested fluoride also contributes to the topical effect of fluorides. Omitting plaque removal with a professional prophylaxis prior to the use of in-office topi-cal fluorides has been found to still result in the formation of calcium fluoride-like globules at the tooth surface and, in fact, to increase fluoride retention and the efficacy of fluoride therapy. Regular rinsing with fluoride in the presence of plaque has been shown to result in the deposition of alkali-soluble (available) fluoride.22,23,24
MOST OF THE TOPICAL EFFECT OF FLUORIDE IS DUE TO THE PRESENCE OF AVAILABLE FLUORIDE.
In-office fluorides In-office fluorides are available as varnishes, gels, foams and rinses. These differ by type of fluoride, concentration, and method and length of application. (Table 3)
Table 3. Fluoride concentration in ppm fluoride
5% sodium fluoride varnish 22,600 ppmAPF gels and foams 12,300 ppmSodium fluoride gels and foams 9,050 ppmDual rinses 3,300 ppm
The selection, use and frequency of use of in-office fluorides for an individual patient should be based on his or her risk level, and should consider ADA recommendations;25 pa-tient age; product efficacy, clinical support and safety; ease of use and patient preference.
VarnishesIn the United States, fluoride varnish is available as 5% sodium fluoride, equivalent to 22,600 ppm fluoride. While the FDA has cleared varnish as a device for the relief of hypersensitivity and as a cavity liner, the vast majority of clinical trials, evidence-based studies and the major use worldwide is as an in-office topical fluoride for the preven-tion of dental caries. In addition, the American Dental Association recommends the use of 5% sodium fluoride varnish for caries prevention for children of all ages (including children under 6 years of age) and for adults. Both tinted and white/clear versions are available in tubes and/or unit doses. Studies have demonstrated patient preference for white/clear varnish due to the improved esthetics while the varnish remains on the teeth, while clinicians have found the use of unit doses simplifies application, results in the use of a defined amount of varnish and reduces any risk of cross-contamination. Applica-tion frequencies of twice or four times per year have been advocated, as well as more frequently than four times per year in some cases of early childhood caries.26,27

www.ineedce.com 9
THE AMERICAN DENTAL ASSOCIATION RECOMMENDS THE USE OF 5% SODIUM FLUORIDE VARNISH FOR CARIES PREVENTION FOR CHILDREN OF ALL AGES AND FOR ADULTS.
Clinical effectivenessFive percent sodium fluoride varnish has been found to be effective in reducing caries in the primary dentition – including early childhood caries – and the permanent dentition.28,29,30,31 Trials and studies have demonstrated reductions in coronal and root caries as well as recurrent caries. One meta-analysis by Marinho et al. pooled data from clinical studies of at least one year’s duration in patients under age 17 who were blinded or double-blinded and met all criteria. They found an overall caries reduction in the primary dentition (dmfs) of 33%, with a range of 19 – 48%, and in the permanent dentition (DMFS) of 46%, with a range of 30 – 63%.32 An earlier, smaller meta-analysis with fewer studies had yielded a caries reduction of 38% in children (Helfenstein and Steiner).33 In an open study, Weinstein et al. found a significant increase in the reversal of enamel decalcifications in children with early childhood caries.34 Studies using 5% sodium fluoride varnish have also reported on its effectiveness in reducing orthodontic decalcification.35
Table 4. Overview of sodium fluoride varnish clinical efficacy
Study Caries reductionMarinho et al. Meta-analysis 33% dmfs reduction (19% to 48%)
46% DMFS reduction ( 30% to 63%)Helfenstein, Steiner Meta-analysis 38% reduction
Holm et al. 36 Pre-school children 44% dmft reduction
Weinstein et al. Early childhood caries 51% reversal of enamel decalcification(open study)
The high level of fluoride and prolonged fluoride release compared to other in-office topical fluorides are factors considered to result in the high caries reductions that have been found with this vehicle.
Gels and foamsGels and foams are available as acidulated phosphate fluoride and as sodium fluoride.
Acidulated phosphate fluoride (APF) gels and foams contain 12,300 ppm fluoride, and neutral sodium fluoride gels contain approximately 9,000 ppm fluoride. These are available as either a four-minute or a one-minute application:• There is clinical support and evidence for the efficacy of four minute gel applications• There is insufficient evidence of caries efficacy for a one-minute application of gel or
foam• Foam has the advantage of resulting in a lower dose of applied fluoride compared
to gel, reducing the risk of ingestion.

10 www.ineedce.com
The American Dental Association recommends the use of 4-minute fluoride gel in children age 6 and older and in adults. The use of in-office fluoride gels and foams is not recommended for children under age 6, who are at greater risk of fluoride ingestion during application and have less ability to spit out excess afterward.
Clinical efficacyIn a meta-analysis of fluoride gels, a caries reduction average of 21% was found (range of 14 – 28%) across 14 placebo-controlled studies.37 A separate systematic review of 23 trials (some of which did not have placebo controls) found a caries reduction (DMFS) average of 28% (range of 19 – 37%).38 It was also concluded in these studies that there was insufficient evidence of any effect in the primary dentition. A systematic review by van Rijkom et al. of clinical trials using acidulated phosphate gels found an average reduction of 22%, with greater reductions for higher caries incidence patients than for lower caries incidence patients.39 An in vitro study by Garcia-Godoy et al. resulted in the conclusion that APF gel treatment with a one-minute or a four-minute application resulted in equivalent reductions in enamel lesion depths.40 A recent study conducted on 3 – 4-year-olds on the twice-annual use of in-office APF foam found a primary caries reduc-tion (dmfs) of 24%, attributable to its effect on approximal surfaces and no effect on oc-clusal surfaces.41 A second study by Jiang et al. assessed the efficacy of APF foam and gel in 6-7 year-old children in a 24-month clinical trial, and found these were equivalent with a 41% caries reduction on smooth surfaces for each. 42 (Table 5) The ADA does not recommend or endorse the use of one-minute gels and does not recommend the use of fluoride foams, due to the paucity of clinical evidence.25
Table 5. Clinical efficacy of fluoride gels and foams
Study Caries reductionMarinho et al. Meta-analysis (gel) 21% DMFS reduction
(14% to 28%)Marinho et al. Systematic review (gel) 28% DMFS reduction
(19% to 37%)v Rijkom et al. Systematic review (gel) 22% average reduction
Jiang et al. APF gel and foam comparison 41% caries reduction for each
Jiang et al. Pre-school children (foam) 24% dmfs reduction
In-office fluoride rinsesIn-office topical rinses are available as 2% sodium fluoride rinses and dual rinses con-taining stannous fluoride and acidulated phosphate fluoride. These should not be used in young children, due to the risk of ingestion. • There is limited in vitro data suggesting an effect for dual rinses • There is no clinical evidence for efficacy of these rinses• The American Dental Association does not recommend the use of in-office fluoride
rinses.25

www.ineedce.com 11
Risk levels and ADArecommendations for in-office fluorides
Patients can be classified as being at low, moderate or high risk for caries at a given time. Low-risk patients are those who have no factors that may increase their risk of car-ies and who have had no incipient, cavitated or secondary carious lesions in the prior three years, according to the guidelines in the ADA recommendations on professionally applied fluorides. All other patients are either moderate or high risk. (Table 6)
Table 6. Moderate- and high-risk levels
Moderate risk High risk
< 6 years of age No incipient/cavitated carious lesions during the last 3 years At least one risk factor
Any incipient/cavitated lesions in last 3 years and/or multiple risk factors
6+ years of age one/two incipient/cavitated lesions in last 3 yearsand/or at least one risk factor
3 or more incipient/cavitated carious lesions in the last 3 yearsand/or multiple risk factors
Adapted from: Evidence-based Clinical Recommendations: Professionally Applied Topical Fluoride
For moderate- and high-risk patients, the American Dental Association recommen-dations are for the use of fluoride varnish in children under age 6 and either fluoride varnish or a four-minute gel in patients age 6 and over. The recommended frequency of application for these patients is two to four times per year, depending on risk level.25 The ADA recommendations do not include the use of foam specifically because there are few clinical trials conducted on foam to demonstrate its efficacy. However, those that were conducted, together with laboratory data, suggest that it may be equivalent to fluoride gel. For low-risk patients, in-office topical fluorides are not recommended, and the use of fluoride dentifrice may suffice. Professional judgment is required for individual patients.25 (Table 7)
Risk factors are destructive factors in the caries process, while the use of fluoride and other preventives are protective factors. (Table 8)

12 www.ineedce.com
Table 7. American Dental Association recommendations
Low-risk patients* Moderate-risk pa-tients**
High-risk patients
< 6 years of age
Professional fluoride may be of no benefit
Fluoride varnish 2 times per year
Fluoride varnish 2 - 4 times per year
6 - 18 years of age
Professional fluoride may be of no benefit
Fluoride varnish or gel 2 times per year
Fluoride varnish or gel 2 - 4 times per year
18+ years of age
Professional fluoride may be of no benefit
Fluoride varnish or gel 2 times per year
Fluoride varnish or gel 2 - 4 times per year
* Use professional judgment. Fluoride dentifrice may be sufficient. **Moderate-risk may benefit from up to 4 times per year. Adapted from: Evidence-based Clinical Recommendations: Professionally Applied Topical Fluoride.
Table 8. Destructive (risk) and protective factors
Risk factors
Suboptimal fluoride exposure Xerostomia
Poor oral hygiene High bacterial load
Familial high caries rate High frequency sugar and other carbohydrate
consumption
Enamel defects Defective restorations
Tobacco use Drug or alcohol abuse
Exposed roots Orthodontic appliances
Low SES Inability to perform adequate oral hygiene
Protective factors
Optimal fluoride exposure High salivary flow
Use of xylitol Use of antimicrobials
Home use of Recaldent-containing products
Clinical examplesClinical examples of at-risk and high-risk patients can be found below. a. Patient with early childhood caries b. Orthodontic patient c. Patient with exposed roots
Courtesy of Dr. N. Sue Seale Courtesy of Dr. Michael Florman Courtesy of Dr. Scott Froum

www.ineedce.com 13
Considerations for in-office and home-use fluoridesIn addition to the ADA recommendations for professional fluorides, professional judgment, efficacy and safety, and other considerations contribute to the selection of in-office and home-use fluorides. These include pH, alcohol content, propensity for stain, and preferences.
pH of topical fluoridesThe pH range of topical fluorides is approximately pH 3 – 7 (neutral). Acidulated phosphate fluoride (acidulated sodium fluoride) topicals are formulated for rapid uptake of fluoride; however, their use over time has the potential to etch and alter the surface of ceramics, resin-based composites and glass ionomers.43,44 In addition, acidulated phosphate alters the surface of titanium alloys, therefore caution is advised with re-spect to use of these formulations in implant patients.45 In patients for whom these are considerations, the use of neutral sodium fluoride products would be indicated.
Alcohol contentWhile not a consideration for in-office topical fluorides or systemic fluoride, home-use fluoride rinses are available with an alcohol content range of 0 – 21.6%. Alcohol-con-taining rinses can result in irritation in some patients, and a drying sensation in patients with xerostomia, and should not be used by alcoholics or patients sensitive to alcohol.46 Rinses containing alcohol are generally not advised for use in children. The alcohol content of rinses can be found on the label, under the inactive ingredients.
Extrinsic stainingThe potential for extrinsic staining of teeth is greater in patients with poor oral hygiene, smokers, red wine, tea and coffee drinkers, and with the use of stannous fluoride prod-ucts. The staining propensity of products varies with formulation and can generally be controlled provided the patient performs excellent oral hygiene.
Patient preferences and conveniencePatient preference and convenience play important roles in the selection of home-use products, especially where patient compliance plays a key role. The fluoride selected must be acceptable to the patient, with pleasant taste, texture, smell and vehicle. Patient compliance must be consid-ered with respect to frequency and regularity of use, ease of use, and length of application.
Table 9. pH of fluoride productsProduct pH1.23% APF gel, foam 3-4Sodium fluoride varnish, gel, foam NeutralNaF and MFP dentifrices Neutral0.4% stannous dentifrice 2.8-4Sodium fluoride pastes, gels, rinses NeutralAPF (Rx) paste/gel 5.1-5.6Acidulated phosphate fluoride rinses 4

14 www.ineedce.com
Home-use fluoridesHome-use fluorides include fluoride dentifrices as well as over-the-counter and prescription gels, pastes, and rinses.
Fluoride dentifrices The majority of over-the-counter dentifrices available in the United States and Canada contain 1,000 – 1,100 ppm fluoride, available as sodium fluoride, sodium monofluo-rophosphate and stannous fluoride, and have been found to be effective with these formulations. (Table 10)
Table 10. 1,000 – 1,100 ppm fluoride dentifrices
0.23 – 0.24% sodium fluoride
0.76% sodium monofluorophosphate
0.4% stannous fluoride
Use of fluoride dentifrice twice daily provides a regular supply of fluoride that results in the presence of low levels of fluoride intra-orally on the teeth and soft tissues. It is recommended to commence use of a fluoride dentifrice in children at age 2, using only a pea-sized amount twice daily from the age of 2 and until reaching 6 years of age (due to the risk of fluorosis with excess ingestion). Children under the age of 6 should always be supervised while brushing (and may require supervision until 10 - 11 years of age), and they should expectorate and rinse after brushing with fluoride dentifrices. Extensive numbers of clinical trials on fluoride dentifrices have been conducted, documenting their anti-caries efficacy. There is strong evidence supporting their use, based on reviews by Twetman and by Topping and Assaf.47,48
USE OF FLUORIDE DENTIFRICE TWICE DAILy PROVIDES A REGULAR SUPPLy OF FLUORIDE THAT RESULTS IN THE PRESENCE OF LOW LEVELS OF
FLUORIDE INTRA-ORALLy ON THE TEETH AND SOFT TISSUES.
Clinical efficacyThe number of clinical trials conducted using fluoride dentifrices is extensive, with clinical trials conducted throughout the world. These have demonstrated a substantial anti-caries benefit with the use of fluoride dentifrices. Early studies were conducted in urban and rural communities, in both cases demonstrating a substantial decline in caries with the use of fluoride dentifrices.49 In one meta-analysis of 70 such trials that were conducted in children age 16 and under, in controlled, blinded conditions, an average reduction of 24% in DMFS was found (21% – 28%) across the studies, and varying with caries risk levels. This caries reduction benefit was found in subjects in

www.ineedce.com 15
fluoridated and non-fluoridated areas, with a greater caries reduction in higher risk individuals.50 Caries efficacy with use of fluoride dentifrices has been demonstrated for children, adults, coronal and root caries. A root caries reduction (DFS) of 67% was found in a one-year study with fluoride dentifrice.51 A recent study also found the addition of calcium and phosphate to a fluoride dentifrice resulted in an incremental reduction in root caries compared to the control fluoride dentifrice.52 A dose-response has also been found, with higher fluoride level dentifrices conferring greater anti-caries benefits than lower fluoride level dentifrices.53, 54 Supervised daily brushing with fluo-ride dentifrice in school programs has also been found to be a successful methodology for the control of caries in school-age populations, including in high-risk children.55,56,57
ExTENSIVE NUMBERS OF CLINICAL TRIALS ON FLUORIDE DENTIFRICES HAVE BEEN CONDUCTED, DOCUMENTING THEIR ExCELLENT ANTI-CARIES EFFICACy.
Prescription pastes/gels Prescription home-use 1.1% sodium fluoride, equivalent to 5,000 ppm fluoride, is avail-able as pastes containing a mild abrasive and as gels/liquids containing no abrasive. These can also be used in mouth trays for extended at-home application. Use of 1.1% sodium fluoride gel in trays has been found to be effective as a caries preventive in head and neck radiation (high-risk) patients suffering from xerostomia.58 Patients using 5,000 ppm fluoride gels and paste should expectorate after using them, without rinsing with water. Prescription pastes and gels are:• Formulations containing 5,000 ppm fluoride• Typically applied as brush-on pastes and gels• Typically used in place of regular dentifrice• Also available in an acidulated version (APF) targeting orthodontic patients.
In a small study on available fluoride in proximal saliva and plaque following use of 5,000 ppm paste, it was found that rinsing after brushing with the paste reduced the available fluoride 2.4-fold compared to expectorating only, underscoring the importance of following the instructions to expectorate only when using these prescrip-tion products.59
Clinical efficacy Use of 5,000 ppm fluoride has been found to be effective in reducing root caries. An early study by De Paola et al. demonstrated a 91% rate of arrestment for root caries le-sions following one year of use of 1.1% sodium fluoride gel in trays.60 A second study by Baysan et al. demonstrated 57% remineralization of root caries lesions over a six-month period of use of 5,000 ppm fluoride dentifrice.61

16 www.ineedce.com
Fluoride rinsesPrescription and OTC fluoride rinses are available, variously utilizing sodium fluoride, acidulated phosphate fluoride and stannous fluoride. A dose-response relationship has been observed, with higher ppm fluoride rinses incrementally increasing the plaque and salivary fluoride levels.62 A separate 24-hour study by zero et al. found that night-time fluoride use resulted in extended fluoride retention in whole saliva.63
Prescription rinse: 0.2% sodium fluoride rinsePrescription fluoride rinses are available as 0.2% sodium fluoride, equivalent to 920 ppm fluoride. These are intended for weekly use and have been used in children over the age of six and in adults as caries preventives. Due to risk of ingestion, 0.2% sodium fluoride rinse is not intended for use in children under the age of six. The anti-caries efficacy of weekly rinsing with 0.2% sodium fluoride has been demonstrated in numerous studies.
Clinical supportHeifetz et al. found significant reductions in caries in children using 0.2% sodium fluo-ride rinse.64 In a study by Driscoll et al., caries reduction of up to 55% was demonstrat-ed in schoolchildren rinsing once weekly at school during a 30-month period.65 Seven years of rinsing weekly with 0.2% sodium fluoride rinse resulted in a 57.8% reduction in caries in the permanent dentition in another study. It was also concluded, however, that other factors contributed to the reductions, since reduced caries in the primary dentition was found that pre-dated rinsing.66
THE ANTI-CARIES EFFICACy OF WEEkLy RINSING WITH 0.2% SODIUM FLUORIDE HAS BEEN DEMONSTRATED IN NUMEROUS STUDIES.
Over-the-counter rinses0.05% sodium fluoride rinseSimilar to the daily use of toothpaste, daily sodium fluoride rinsing has been shown in vivo to elevate salivary fluoride levels and plaque fluoride levels, an effect that disap-pears after ceasing to rinse daily. Children age 6 and over can use 0.05% sodium fluoride rinse daily; it is not recommended for use in children under age 6 due to the risk of ingestion.
Clinical supportSignificant caries reductions have been observed with daily rinsing with 0.05% sodium fluoride in subjects living in areas with up to 0.3 ppm fluoride in the water.64 In his assessment, Ripa cited a 31% reduction in caries in non-fluoridated communities.67 A 48-month study in an urban geriatric population compared the use of placebo rinse,

www.ineedce.com 17
0.05% sodium fluoride mouth rinse and APF gel twice per year plus placebo rinse. It was found that reductions in new lesions were statistically similar for the combination of APF gel plus placebo rinse and for 0.05% sodium fluoride rinse alone, while the reversal of lesions was greatest using the fluoride rinse.68 A more recent study assessed arrestment of smooth-surface carious lesions in 11 – 15-year olds with use of 0.05% sodium fluoride rinse once daily, finding an arrestment rate of 84.4%.69 Geiger et al. found reductions in white spot lesions (orthodontic decalcifications) following use of 0.05% sodium fluoride rinse during orthodontic treatment. While compliance issues in this study resulted in only 13% rinsing daily with the mouth rinse, a significant reduction in white spot lesions was found and correlated to the frequency of rinsing (daily as recommended versus less frequently).70 In reviewing the Cochrane Database clinical trials that addressed reductions in white spot lesions during fixed orthodontic appliance therapy, Benson et al. concluded that rinsing daily with 0.05% sodium fluoride rinse reduced the severity of enamel lesions adjacent to fixed appliances.71
THE ANTI-CARIES EFFICACy OF DAILy RINSING WITH 0.05% SODIUM FLUORIDE HAS BEEN DEMONSTRATED IN NUMEROUS STUDIES.
0.02% sodium fluoride rinseSodium fluoride rinses are available at 0.02% concentrations in the United States and Canada. These rinses should be used twice daily, given the lower concentration of fluo-ride, and are recommended for use in children age 6 and over. In vitro fluoride uptake studies using 0.02% sodium fluoride rinse have shown superior fluoride uptake. No clini-cal trials have been published using this rinse.
Acidulated phosphate fluoride/sodium fluoride rinsesAcidulated phosphate (sodium) fluoride rinses are available in 0.044% and 0.021% con-centrations, both available over-the-counter. These are also intended for use in children age 6 and older and in adults. 0.044% acidulated phosphate fluoride has been recommended mainly for orthodontic patients, and its daily use is clinically supported. 0.021% acidulated sodium fluoride is available for twice daily rinsing.
Clinical efficacyOne early study (1978) showed that 0.044% acidulated phosphate fluoride rinse reduced the development of white spots in orthodontic patients by up to 58%.72
Stannous fluoride rinsesStannous fluoride rinses at a concentration of 0.63% are available as prescription rinses, and they are then diluted to provide a 0.1% rinse. This was shown in an early study to be effective in reducing caries and inhibiting bacterial metabolism.73

18 www.ineedce.com
Table 11. Clinical support for fluoride rinses and for 5,000 ppm fluoride gel/paste
Study Caries reduction
5,000 ppm (Rx) sodium fluoride
de Paola et al. Root caries, 1-year study
91% arrestment of root caries lesions
Baysan et al. Root caries, 6-month study
57% remineralization of root caries lesions
0.2% (Rx) sodium fluoride rinse
Driscoll et al. Schoolchildren, weekly rinsing, 30-month
Up to 55% reduction
Leverett et al. Weekly rinsing, 7 years
57.8% reduction permanent dentition
0.05% sodium fluoride rinse
Ripa Coronal caries 31% caries reduction
Wallace et al. Root caries Up to 71% reduction
Heifetz et al. Coronal caries children Up to 40% reduction (permanent dentition)
Duarte et al. Smooth surface, 11-15 year olds
84.4% arrestment of carious lesions
0.044% APF rinse
Hirschfield et al. Orthodontic patients Up to 58% reduced development of white spots
Biofilm, rinsing and intra-oral fluoride Fluoride dentifrice use has greatly contributed to caries reductions for several decades and continues to provide anti-caries benefits. The presence of moderate amounts of biofilm does not deter fluoride from reaching the tooth surface, and fluoride has been shown to penetrate through and concentrate in light biofilm layers, increasing the retention of intra-oral fluoride. 74
FLUORIDE DENTIFRICE USE HAS GREATLy CONTRIBUTED TO CARIES REDUCTIONS FOR SEVERAL DECADES.
Considerations include the assessed compliance of the individual patient with ap-propriate brushing and use of a fluoride dentifrice, as well as his or her risk level. Non-compliant patients may brush inadequately or brush for an inadequate length of time,75 reducing the effectiveness of brushing and exposure to fluoride toothpaste. Post-brushing rinsing, which is standard practice for most patients, also removes fluoride that was

www.ineedce.com 19
just delivered by the dentifrice and reduces the amount of intra-oral available fluoride. Although no controlled clinical trials are available on its impact, post-brushing rinsing has been shown to reduce the level of intra-oral bioavailable fluoride.76
POST-BRUSHING RINSING HAS BEEN SHOWN TO REDUCE THE LEVEL OF INTRA-ORAL BIOAVAILABLE FLUORIDE.
zamataro et al. found a 250% reduction in intra-oral bioavailable fluoride as a result of rinsing with 15 ml of water after use of a standard dentifrice containing 1,100 ppm fluoride.76 Adjunctive use of fluoride rinses has been advocated for moderate- and high-risk patients, together with routine oral hygiene procedures, to increase the amount of available fluoride and increase protection against caries.77,78 Increasing the flow rate of fluoride rinse has also been suggested as a possible mechanism to increase the amount of fluoride penetrating biofilm.79
ADJUNCTIVE USE OF FLUORIDE RINSES HAS BEEN ADVOCATED FOR MODERATE- AND HIGH-RISk PATIENTS.
SummarySuccessful fluoride preventive interventions began with the use of fluoridated water and fluoride dentifrices, and now include the use of professional topical fluorides as well as prescription pastes, gels and rinse and over-the-counter rinses. The individual patient’s risk level and age, and the product’s efficacy, clinical support and safety must be considered when determining the appropriate combination of preventives. Other factors to consider include clinician and patient preferences and the specifics of a given formulation. The use of fluorides has contributed greatly to reducing the level of caries seen in the population and continues to do so.
Author ProfilesFiona M. Collins, BDS, MBA, MADr. Collins earned her dental degree from Glasgow University and holds an MBA and MA from Boston University. She is a member of the American Dental Association and the Organization for Asepsis and Safety Procedures.
Michael Florman, DDSDr. Florman received his dental degree from Ohio State University and completed his orthodontic post graduate training at New york University. He is a member of the American Dental Association, California Dental Association, and the American Association of Orthodontists.
DisclaimerThe authors of this course have no commercial ties with the sponsors or the providers of the unre-stricted educational grant for this course.
Reader FeedbackWe encourage your comments on this or any PennWell course. For your convenience, an online feedback form is available at www.ineedce.com.

20 www.ineedce.com
Sources
1 Dean HT, Arnold FA, Jay P, knutson JW. Studies on mass control of dental caries through fluoridation of the public water supply. Public Health Rep. 1950;65:1403 – 38.
2 Espelid I. Caries preventive effect of fluoride in milk, salt and tablets: a literature review. Eur Arch Paediatr Dent. 2009 Sep;10(3):149 – 56.
3 American Dental Association. ADA guide to dental therapeutics. 1st ed. Chicago: American Dental Association, 1998.4 American Academy of Pediatric Dentistry. Guideline on Fluoride Therapy. 20085 Centers for Disease Control and Prevention. Community water fluoridation: other fluoride products. Available at: http://
www.cdc.gov/fluoridation/other.htm6 Aoba T. The effect of fluoride on apatite structure and growth. Crit Rev Oral Biol Med. 1997;8(2):136 – 53.7 Featherstone JD, Glena R, Shariati M, Shields CP. Dependence of in vitro demineralization of apatite and remineralization
of dental enamel on fluoride concentration. J Dent Res. 1990;69:620 – 25.8 Hellwig E, Lennon AM. Systemic versus topical fluoride. Caries Res. 2004 May-June;38(3):258 – 62.9 Featherstone JD. Prevention and reversal of dental caries: role of low level fluoride. Community Dent Oral Epidemiol. 1999
Feb;27(1):31 – 40.10 Featherstone JDB. The science and practice of caries prevention. J Am Dent Assoc. 2000;131:887-99. 11 Pendrys DG, katz RV, Morse DE. Risk factors for enamel fluorosis in a nonfluoridated population. Am J Epidemiol.
1996;143(8): 12 Beltrán-Aguilar ED, Barker Lk, Canto MT, Dye BA, Gooch BF, et al. Surveillance for Dental Caries, Dental Sealants, Tooth
Retention, Edentulism, and Enamel Fluorosis --- United States, 1988--1994 and 1999--2002. MMWR. 2005;54(03):1-44. 13 Brudevold F, Savory A, Gardner DE, Spinelli M, Speirs R. A study of acidulated fluoride solutions. I. In vitro effects on
enamel. Arch Oral Biol. 1963;8:167 – 77.14 Pameijer JHN, Brudevold F, Hunt EE. A study of acidulated fluoride solutions: the cariostatic effect of repeated topical
sodium fluoride application with and without phosphate. Arch Oral Biol. 1963;8:183-185.
15 Gorelick L, et al. Incidence of white spot formation after bonding and banding. Am J Orthod. 1982; 81(2):93 – 98.16 Featherstone JD. The science and practice of caries prevention. J Am Dent Assoc. 2000;131:887 – 99.17 kawasaki k, Featherstone JDB. Effects of Collagenase on Root Demineralization. J Dent Res. 1997;76(1):588-95.18 Hellwig E, klimek J, Albert G. In vivo retention of kOH soluble and firmly bound fluoride in demineralized dental enamel.
Dtsch zahnarztl z. 1989;44(3):173 – 76.19 Ogaard B, The cariostatic mechanism of fluoride. Compend Contin Educ Dent. 1999;20(1 Suppl):10 – 17.20 Arends J, Christoffersen J. Nature and role of loosely bound fluoride in dental caries. J Dent Res. 1990 Feb;69 Spec
No:601-5; discussion 634 – 36.21 zero DT, Raubertas RF, Pedersen AM, Fu J, Hayes AL, Featherstone JD. Studies of fluoride retention by oral soft tissues after
the application of home-use topical fluorides. J Dent Res. 1992 Sep;71(9):1546 – 52.22 Hellwig E, klimek J, Schmidt HF, Egerer R. Fluoride uptake in plaque-covered enamel after treatment with the fluoride lacquer
Duraphat. J Dent Res. 1985;64(8):1080 – 83.23 Borro Bijella MFT, Bijella VT, Lopes ES, de Magalhase Bastos E. Comparison of dental prophylaxis and toothbrushing prior
to topical APF applications. Comm Dent Oral Epidemiol. 2006;13(4):208 – 11. Available at http://www3.interscience.wiley.com/journal/120033407/abstract.
24 Hellwig E, klimek J, Wagner H. The influence of plaque on reaction mechanism of MFP and NaF in vivo. J Dent Res. 1987 Jan;66(1):46 – 49.
25 American Dental Association Council on Scientific Affairs. Professionally applied topical fluoride: evidence-based clinical recommendations. J Am Dent Assoc. 2006;137:1151 – 59. Available at http://jada.ada.org.
26 Petersson LG, Arthursson L, Östberg C, Jönsson P, Gleerup A. Caries-inhibiting effects of different modes of Duraphat varnish reapplication: a 3-year radiographic study. Caries Res. 1991;25:70 – 73.
27 Sköld L, Sundquist B, Eriksson B, Edeland C. Four-year study of caries inhibition of intensive Duraphat application in 11 – 15-year-old children. Community Dent Oral Epidemiol. 1994;22:8 –12.
28 Clark DC, Stamm JW, Tessier C, Robert G. The final results of the Sherbrooke-Lac Mégantic fluoride varnish study. J Can Dent Assoc. 1987;53:919 – 22.
29 Peyron M, Matsson L, Birkhed D. Progression of approximal caries in primary molars and the effect of Duraphat treatment. Scand J Dent Res. 1992;100:314 – 18.
30 Weintraub JA, Ramos-Gomez F, Jue B, et al. Fluoride varnish efficacy in preventing early childhood caries. J Dent Res. 2006;85(2):172 – 76.
31 Petersson LG, Arthursson L, Östberg C, Jönsson P, Gleerup A. Caries-inhibiting effects of different modes of Duraphat varnish reapplication: a 3-year radiographic study. Caries Res 1991;25:70 – 73.
32 Marinho VC, Higgins JP, Logan S, Sheiham A. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2002;(3):CD002279.
33 Helfenstein U, Steiner M. Fluoride varnishes (Duraphat): a meta-analysis. Community Dent Oral Epidemiol. 1994;22:1 – 5.34 Weinstein P, Domoto P, koday M, Leroux B. Results of a promising open trial to prevent baby bottle tooth decay: a fluoride
varnish study. ASDC J Dent Child. 1994;61(5-6):338-41.35 Vivaldi-Rodrigues G, Demito CF, Bowman SJ, Ramos AL. The effectiveness of a fluoride varnish in preventing the develop-
ment of white spot lesions. World J Orthod. 2006 Summer;7(2):138 – 44.36 Holm Ak. Effect of fluoride varnish (Duraphat) in preschool children. Community Dent Oral Epidemiol. 1979;7(5):241-5.37 Marinho VC, Higgins JP, Logan S, Sheiham A. Fluoride gels for preventing dental caries in children and adolescents.
Cochrane Database Syst Rev. 2002;(2):CD002280.38 Marinho VC, Higgins JP, Logan S, Sheiham A. Systematic review of controlled trials on the effectiveness of fluoride gels for
the prevention of dental caries in children. J Dent Educ. 2003 Apr;67(4): 448 – 58.39 van Rijkom HM, Truin GJ, van’t Hof MA. A meta-analysis of clinical studies on the caries-inhibiting effect of fluoride gel treat-
ment. Caries Res. 1998;32:83 – 92.40 Garcia-Godoy F, Hicks MJ, Flaitz CM, Berg JH. Acidulated phosphate fluoride treatment and formation of caries-like lesions
in enamel: effect of application time. J Clin Pediatr Dent. 1995 Winter;19(2):105 – 10.41 Jiang H, Bian z, Tai BJ, Du MQ, Peng B. The effect of a bi-annual professional application of APF foam on dental caries

www.ineedce.com 21
increment in primary teeth: 24-month clinical trial. J Dent Res. 2005 Mar;84(3):265 – 68. 42 Jiang H, Tai B, Du M, Peng B. Effect of professional application of APF foam on caries reduction in permanent first molars in
6-7-year-old children: 24-month clinical trial. J Dent. 2005;33(6):469-73.43 El-Badrawy WA, McComb D. Effect of home-use fluoride gels on resin-modified glass-ionomer cements. Oper Dent.
1998;23(1):2-9.44 El-Badrawy WA, McComb D, Wood RE. Effect of home-use fluoride gels on glass ionomer and composite restorations. Dent
Mater. 1993;9(1):63-7.45 Matono y, Nakagawa M, Matsuya S, Ishikawa k, Terada y. Corrosion behavior of pure titanium and titanium alloys in
various concentrations of Acidulated Phosphate Fluoride (APF) solutions. Dent Mater J. 2006 Mar;25(1):104–112.46 Eldridge k, Finnie S, Stephens J, Mauad A, Munoz C, kettering J. Efficacy of an alcohol-free chlorhexidine mouthrinse as an
antimicrobial agent. J Pros Dent. 1998;80(6):685-690.47 Twetman S. Caries prevention with fluoride toothpaste in children: an update. Eur Arch Paediatr Dent. 2009 Sep;10(3):162 – 67.48 Topping G, Assaf A. Strong evidence that daily use of fluoride toothpaste prevents caries. Evid Based Dent. 2005;6(2):32.49 Hargreaves JA, Cleaton-Jones PE. Dental caries changes in the Scottish Isle of Lewis. Caries Res. 1990;24(2):137-41.50 Marinho VC, Higgins JP, Sheiham A, Logan S. Fluoride toothpastes for preventing dental caries in children and adolescents.
Cochrane Database Syst Rev. 2003;(1):CD002278.51 Jensen ME, kohout F. The effect of a fluoridated dentifrice on root and coronal caries in an older adult population. J Am
Dent Assoc. 1988 Dec;117(7):829 – 32.52 Papas A, Russell D, 5D” Singh M, kent R, Triol C, Winston A. Caries clinical trial of a remineralising toothpaste in radia-
tion patients. Gerodontol. 2008;25(2):76-88.53. ten Cate JM, Exterkate RA, Buijs MJ. The relative efficacy of fluoride toothpastes assessed with pH cycling. Caries Res.
2006;40(2):136-41.54. Steiner M, Helfenstein U, Menghini G. Effect of 1,000 ppmrelative to 250 ppm fluoride toothpaste: a meta-analysis. Am J
Dent. 2004 Apr; 17(2):85-8.55. Al-Jundi SH, Hammad M, Alwaeli H. The efficacy of a school-based caries preventive program: a 4-year study. Int J Dent
Hyg. 2006 Feb;4(1):30-4.56. Jackson RJ, Newman HN, Smart GJ, et al. The effects of a supervised toothbrushing programme on the caries increment of
primary school children, initially aged 5-6 years. Caries Res. 2005 Mar-Apr; 39(2):108-15.57. Curnow MM, Pine CM, Burnside G, Nicholson JA, Chesters Rk, Huntington E. A randomised controlled trial of the efficacy
of supervised toothbrushing in high-caries-risk children. Caries Res. 2002 Jul-Aug;36(4):294-300.58 Joyston-Bechal S, Hayes k, Davenport ES, Hardie JM. Caries incidence, mutans streptococci and lactobacilli in irradiated
patients during a 12-month preventive programme using chlorhexidine and fluoride. Caries Res. 1992;26(5):384 – 90.59 Nordström A, Birkhed D. Fluoride retention in proximal plaque and saliva using two NaF dentifrices containing 5,000 and
1,450 ppm F with and without water rinsing. Caries Res. 2009;43(1):64 – 69. Epub 2009 Feb 10.60 DePaola P., ed. Cariology for the nineties. Caries in our aging population: What are we learning?, Ed. W.H. Bowen and
L.W. Tabak. 1993; 26-35.61 Baysan A, et al. Reversal of primary root caries using dentifrices containing 1,000 and 5,000 ppm fluoride. Caries Res.
2001;35:41 – 46.62 Duckworth RM, Morgan, SN, Murray AM. Fluoride in saliva and plaque following use of fluoride-containing mouthwashes.
J Dent Res. 1987;66:1730 – 34.63 zero DT, Raubertas RF, Fu J, Pedersen AM, Hayes AL, Featherstone JDB. Fluoride concentrations in plaque, whole saliva,
and ductal saliva after application of home-use topical fluorides. J Dent Res. 1992;71:1768 – 75.64 Heifetz SB, et al. A comparison of the anticaries effectiveness of daily and weekly rinsing with sodium fluoride solutions:
final results after three years. Pediat Dent. 1982;4(4):300 – 303.65 Driscoll, WS, et al. Caries-preventive effects on schoolchildren of daily and weekly fluoride mouthrinsing in a fluoridated
community: final results after 30 months. JADA. 1982:105, 1010 – 13.66 Leverett DH, Sveen OB, Jensen OE. Weekly rinsing with a fluoride mouthrinse in an unfluoridated community: results after
seven years. J Public Health Dent. 1985 Spring;45(2):95 – 100.67 Ripa LW. A critique of topical fluoride methods (dentifrices, mouthrinses, operator-, and self-applied gels) in an era of
decreased caries and increased fluorosis prevalence. J Public Health Dent. 1991;51:23 – 41.68 Wallace MC, Retief DH, Bradley EL. The 48-month increment of root caries in an urban population of older adults partici-
pating in a preventive dental program. J Public Health Dent. 1993 Summer;53(3):133 – 37.69 Duarte AR, Peres MA, Vieira RS, Ramos-Jorge ML, Modesto A. Effectiveness of two mouth rinses solutions in arresting caries
lesions: a short-term clinical trial. Oral Health Prev Dent. 2008;6(3):231 – 38.70 Geiger AM, Gorelick L, Gwinnett AJ, Benson BJ. Reducing white spot lesions in orthodontic populations with fluoride rinsing.
Am J Orthod Dentofacial Orthop. 1992 May;101(5):403 – 407.71 Benson PE, Parkin N, Millett DT, Dyer FE, Vine S, Shah A. Fluorides for the prevention of white spots on teeth during fixed
brace treatment. Cochrane Database Syst Rev. 2004;(3):CD003809.72 Hirschfield, HE, et al. Control of decalcification by use of fluoride mouthrinse. J Dent Child. 1978;45:458 – 460. 73 Radike AW, Gish CW, Peterson Jk, king JD, Segreto VA. Clinical evaluation of stannous fluoride as an anticaries mouth-
rinse. JADA. 1973;86:404 – 408. 74 Nordström A, Birkhed D. Fluoride retention in proximal plaque and saliva using two NaF dentifrices containing 5,000 and
1,450 ppm F with and without water rinsing. Caries Res. 2009;43(1):64 – 69. Epub 2009 Feb 10.75 McCracken G, Janssen J, Heasman L, Stacey F, Steen N, et al. Assessing adherence with toothbrushing instructions using a
data logger toothbrush. Br Dent J. 2005;198(1):29–32.76 zamataro CB, Tenuta LM, Cury JA. Low-fluoride dentifrice and the effect of postbrushing rinsing on fluoride availability in
saliva. Eur Arch Paediatr Dent. 2008 Jun;9(2):90 – 93.77 O’Reilly MM, Featherstone JDB. De- and reminer alization around orthodontic appliances: an in vivo study. Am J Orthod
1987;92:33 – 40.78 FDI Commission. Mouthrinses and dental caries. Int Dent J. 2002 Oct;52(5):337 – 45.79 Stoodley P, Wefel J, Gieseke A, Debeer D, von Ohle C. Biofilm plaque and hydrodynamic effects on mass transfer, fluoride
delivery and caries. J Am Dent Assoc. 2008 Sep;139(9):1182 – 90.

22 www.ineedce.com
Questions
Online CompletionUsethispagetoreviewthequestionsandanswers.Returnto www.ineedce.com andsignin.Ifyouhavenotpreviouslypurchasedtheprogramselectitfromthe“OnlineCourses”listingandcompletetheonlinepurchase.OncepurchasedtheexamwillbeaddedtoyourArchivespagewhereaTakeExamlinkwillbeprovided.Clickonthe“TakeExam”link,completealltheprogramquestionsandsubmityouranswers.Animmediategradereportwillbeprovidedanduponreceivingapassinggradeyour“VerificationForm”willbeprovidedimmediatelyforviewingand/orprinting.VerificationFormscanbeviewedand/orprintedanytimeinthefuturebyreturningtothesite,signinandreturntoyourArchivesPage.
1.FluoridehasbeenusedintheUnitedStatesasananti-cariesagentsincethe________.a. 1930sb. 1940sc. 1950sd. noneoftheabove
2._________anintentionalsourceofsystemicfluoride.a. Fluoridatedwaterisb. Fluoridesupplementsarec. Fluoridatedsaltisd. alloftheabove
3.Theuseoffluoridesupplementsbypregnantwomendoesnotresultinanybenefitforthebaby.a. Trueb. False
4.TheCentersforDiseaseControlandPrevention(CDC)suggeststhatfluoridesupplementsbegiventochildrenlivinginareaswithsuboptimalwaterfluoridationwhoareathighriskofcaries.a. Trueb. False
5.Duringtoothdevelopment,thecumulativeingestionoffluoridepriortopre-eruptiveenamelmaturationresultsin________.a. fluorideionsreplacinghydroxylionsb. iodideionsreplacinghydroxylionsc. theformationoffluorapatitecrystalsd. aandc
6.Pre-eruptively,formedenamelisbathedinplasmathatcontainsfluorideandcontrib-utestotheouterfluoride-richlayer.a. Trueb. False
7.Inadvertentingestionofexcessiveamountsoffluorideduringenameldevelopment,fromallsourcescombined,canresultinfluorosisandisdependenton________.a. thedoseoffluorideb. theageofthechildwhenexcessivefluoride
ingestionoccurredc. thedurationofexcessivefluorideingestiond. alloftheabove
8.Topicalfluoridesavailableinclude________.a. sodiumfluorideandsodiummonofluorophosphateb. acidulatedphosphatefluoridec. stannousfluorided. alloftheabove
9.Duringacidattacks,subsurfacedissolu-tionoccursatpH3.8–4.8.a. Trueb. False
10.Diseaseprogressionismorerapidindentinthaninenamel.a. Trueb. False
11.Theanti-cariesbenefitderivedfromtopicalfluoridescanbeattributedprimar-ilytothepreventionofdemineralizationandthepromotionofremineralization.a. Trueb. False
12.Theapplicationofhighconcentrationsoftopicalfluorideresultsin_________.a. theformationofalkali-insolublecalciumfluoride-
likeglobulesatthetoothsurfaceb. theformationofalkali-solublecalciumfluoride-like
globulesatthetoothsurfacec. theformationofacid-insolublecalciumfluoride-
likeglobulesatthetoothsurfaced. noneoftheabove
13.Topicalfluoridesresultintheretentionoffluoride_________.a. onthetoothsurfaceb. insalivaanddentalplaquec. onintra-oralsofttissuesd. alloftheabove
14.Topicalfluorideisbelievedtoinhibitcar-iesactivitythroughbacterialinhibition,inadditiontoinhibitingdemineralizationandaidingremineralization.a. Trueb. False
15.Mostofthetopicaleffectoffluorideisduetothepresenceofavailablefluorideratherthantheinfluenceoffluorideuptakeduringfluoridetherapy(in-officeorhome-use).a. Trueb. False
16.Omittingplaqueremovalwithaprofes-sionalprophylaxispriortotheuseofin-officetopicalfluorideshasbeenfoundto_________.a. resultinnocalciumfluoride-likeglobulesbeing
formedatthetoothsurfaceb. increasefluorideretentionandtheefficacyof
fluoridetherapyc. decreasetheefficacyoffluoridetherapyd. aandc
17.Thevastmajorityofclinicaltrials,evidence-basedstudiesandthemajoruseworldwideoffluoridevarnishisasanin-officetopicalfluoridefor_________.a. thepreventionofdentalcariesb. thereliefofhypersensitivityc. cavityliningsd. noneoftheabove
18.Fivepercentsodiumfluoridevarnishhasbeenfoundtobeeffectiveinreducingcariesin_________.a. theprimarydentitionb. thepermanentdentitionc. patientswithrootcariesd. alloftheabove
19.Inameta-analysisoffluoridegels,acariesreductionaverageof21%wasfound(rangeof14–28%)across14placebo-controlledstudies.a. Trueb. False
20.TheADAdoesnotrecommendorendorsetheuseofone-minutegels,doesnotrecommendtheuseoffluoridefoamsduetothepaucityofclinicalevidence,anddoesnotrecommendtheuseofin-officefluoriderinses.a. Trueb. False
21.InadditiontotheADArecommenda-tionsforprofessionalfluorides,profes-sionaljudgment,efficacyandsafety,andotherconsiderationscontributetotheselectionofin-officeandhome-usefluorides.a. Trueb. False
22.Thenumberofclinicaltrialsconductedworldwideusingfluoridedentifricesisextensive,andthesehavedemonstratedasubstantialanti-cariesbenefitwiththeuseoffluoridedentifrices.a. Trueb. False
23.Useof5,000ppmfluorideprescriptionpaste/gelhasbeenfoundtobeeffectiveinreducingrootcaries.a. Trueb. False
24.Theanticariesefficacyofweeklyrinsingwith0.2%sodiumfluoridehasbeendemonstratedinnumerousstudies.a. Trueb. False
25.Theanticariesefficacyofdailyrinsingwith0.05%sodiumfluoridehasbeendemonstratedinnumerousstudies.a. Trueb. False
26.Sodiumfluoriderinsesareavailableat0.02%concentrationsintheUnitedStatesandCanada,andtheserinses_________.a. shouldbeusedtwicedailygiventhelower
concentrationoffluorideb. havepublishedclinicaltrialsc. aswith0.05%fluoriderinse,arerecommendedfor
useinchildrenage6andoverd. aandc
27.Patientpreferenceandconvenienceplayimportantrolesintheselectionofhome-useproducts,especiallywherepatientcomplianceplaysakeyrole.a. Trueb. False
28.Post-brushingrinsinghasbeenshowntoreducethelevelofintra-oralbioavailablefluoride.a. Trueb. False
29.Adjunctiveuseoffluoriderinseshasbeenadvocatedfor_________patients,togetherwithroutineoralhygieneprocedures,toincreasetheamountofavailablefluorideandincreaseprotectionagainstcaries.a. lowriskb. moderateriskc. highriskd. bandc
30.Theindividualpatient’srisklevelandage,andtheproduct’sefficacy,clinicalsupportandsafetymustbeconsideredwhendeterminingtheappropriatecombinationofpreventives.a. Trueb. False

PLEASE PHOTOCOPY ANSWER SHEET FOR ADDITIONAL PARTICIPANTS.
For immediate results, go to www.ineedce.com to take tests online.
answer sheets can be faxed with credit card payment to (440) 845-3447, (216) 398-7922, or (216) 255-6619.
�Payment of $59.00 is enclosed. (Checks and credit cards are accepted.)
If paying by credit card, please complete the following: MC Visa AmEx Discover
Acct. Number: _______________________________
Exp. Date: _____________________
Charges on your statement will show up as PennWell
If not taking online, mail completed answer sheet to
Academy of Dental Therapeutics and Stomatology,A Division of PennWell Corp.
P.O. Box 116, Chesterland, OH 44026 or fax to: (440) 845-3447
Educational Objectives1. Listintentionalandunintentionalsourcesofsystemicfluoride.
2. ListanddescribecariesriskfactorsandtheADArecommendationsforin-officetopicalfluoridescorrespondingto
differentrisklevels.
3. Listanddescribetheconsiderationsinvolvedinselectingin-officeandhomeusetopicalfluorides.
4 Listanddescribethevarioushomeusetopicalfluoridesavailableandtheclinicalefficacyofeach.
Course EvaluationPleaseevaluatethiscoursebyrespondingtothefollowingstatements,usingascaleofExcellent=5toPoor=0.
1.Weretheindividualcourseobjectivesmet? Objective#1:YesNo Objective#3:YesNo
Objective#2:YesNo Objective#4:YesNo
2.Towhatextentwerethecourseobjectivesaccomplishedoverall? 5 4 3 2 1 0
3.Pleaserateyourpersonalmasteryofthecourseobjectives. 5 4 3 2 1 0
4.Howwouldyouratetheobjectivesandeducationalmethods? 5 4 3 2 1 0
5.Howdoyouratetheauthor’sgraspofthetopic? 5 4 3 2 1 0
6.Pleaseratetheinstructor’seffectiveness. 5 4 3 2 1 0
7.Wastheoveralladministrationofthecourseeffective? 5 4 3 2 1 0
8.Doyoufeelthatthereferenceswereadequate? Yes No
9.Wouldyouparticipateinasimilarprogramonadifferenttopic? Yes No
10.Ifanyofthecontinuingeducationquestionswereunclearorambiguous,pleaselistthem.
___________________________________________________________________
11.Wasthereanysubjectmatteryoufoundconfusing?Pleasedescribe.
___________________________________________________________________
___________________________________________________________________
12.Whatadditionalcontinuingdentaleducationtopicswouldyouliketosee?
___________________________________________________________________
___________________________________________________________________ AGD Code 258
ANSWERSHEET
FluorideGuide
Name: Title: Specialty:
Address: E-mail:
City: State: ZIP: Country:
Telephone: Home ( ) Office ( ) Lic. Renewal Date:
Requirements for successful completion of the course and to obtain dental continuing education credits: 1) Read the entire course. 2) Complete all information above. 3) Complete answer sheets in either pen or pencil. 4) Mark only one answer for each question. 5) A score of 70% on this test will earn you 4 CE credits. 6) Complete the Course Evaluation below. 7) Make check payable to PennWell Corp. For Questions Call 216.398.7822
AUTHOR DISCLAIMERThe author(s) of this course has/have no commercial ties with the sponsors or the providers of the unrestricted educational grant for this course.
SPONSOR/PROVIDERThis course was made possible through an unrestricted educational grant. No manufacturer or third party has had any input into the development of course content. All content has been derived from references listed, and or the opinions of clinicians. Please direct all questions pertaining to PennWell or the administration of this course to Machele Galloway, 1421 S. Sheridan Rd., Tulsa, OK 74112 or [email protected].
COURSE EVALUATION and PARTICIPANT FEEDBACKWe encourage participant feedback pertaining to all courses. Please be sure to complete the survey included with the course. Please e-mail all questions to: [email protected].
INSTRUCTIONSAll questions should have only one answer. Grading of this examination is done manually. Participants will receive confirmation of passing by receipt of a verification form. Verification forms will be mailed within two weeks after taking an examination.
EDUCATIONAL DISCLAIMERThe opinions of efficacy or perceived value of any products or companies mentioned in this course and expressed herein are those of the author(s) of the course and do not necessarily reflect those of PennWell.
Completing a single continuing education course does not provide enough information to give the participant the feeling that s/he is an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise.
COURSE CREDITS/COSTAll participants scoring at least 70% (answering 21 or more questions correctly) on the examination will receive a verification form verifying 4 CE credits. The formal continuing education program of this sponsor is accepted by the AGD for Fellowship/Mastership credit. Please contact PennWell for current term of acceptance. Participants are urged to contact their state dental boards for continuing education requirements. PennWell is a California Provider. The California Provider number is 4527. The cost for courses ranges from $49.00 to $110.00.
Many PennWell self-study courses have been approved by the Dental Assisting National Board, Inc. (DANB) and can be used by dental assistants who are DANB Certified to meet DANB’s annual continuing education requirements. To find out if this course or any other PennWell course has been approved by DANB, please contact DANB’s Recertification Department at 1-800-FOR-DANB, ext. 445.
RECORD KEEPINGPennWell maintains records of your successful completion of any exam. Please contact our offices for a copy of your continuing education credits report. This report, which will list all credits earned to date, will be generated and mailed to you within five business days of receipt.
CANCELLATION/REFUND POLICYAny participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing.
© 2010 by the Academy of Dental Therapeutics and Stomatology, a division of PennWell
www.ineedce.com Customer Service 216.398.7822 23