Embed Size (px)
Citation preview
Fluids in ICUJMO teaching 5th July 2016
Objectives• Physiology of fluid infusion
• History of fluid resuscitation
• Physiology of fluid resuscitation
• Types of resuscitation fluid
• The ideal resuscitation fluid
• Fluid overload and how to avoid it
Physiology of fluid infusion
• What are the effects of rapid infusion of a litre of 5% dextrose into a patient?
Physiology of fluid infusion
• What are the effects of rapid infusion of a litre of 0.9% saline (Normal saline) into a patient?
Physiology of fluid infusion
• What are the effects of rapid infusion of a litre of 5% normal serum albumin solution into a patient?
Physiology of fluid infusion
• Which of the 3 infusions would be excreted the quickest and why?
History of fluid resuscitation
• 1832 = Robert Lewis administered “Saline injections into the vines” vs cholera pandemic
“… the quantity necessary to be infected will probably be found to depend upon the quantity of serum lost; the object being to place the patient in nearly his ordinary state as to the quantity of blood circulating in the vessels”
History of fluid resuscitation
• Sidney Ringer (1834-1910) developed solution 1884
• Alexis Hartmann (1989-1964) modified solution by addition of lactate
• 1941 => blood fractionation => development of Albumin … used at Pearl Harbour same year
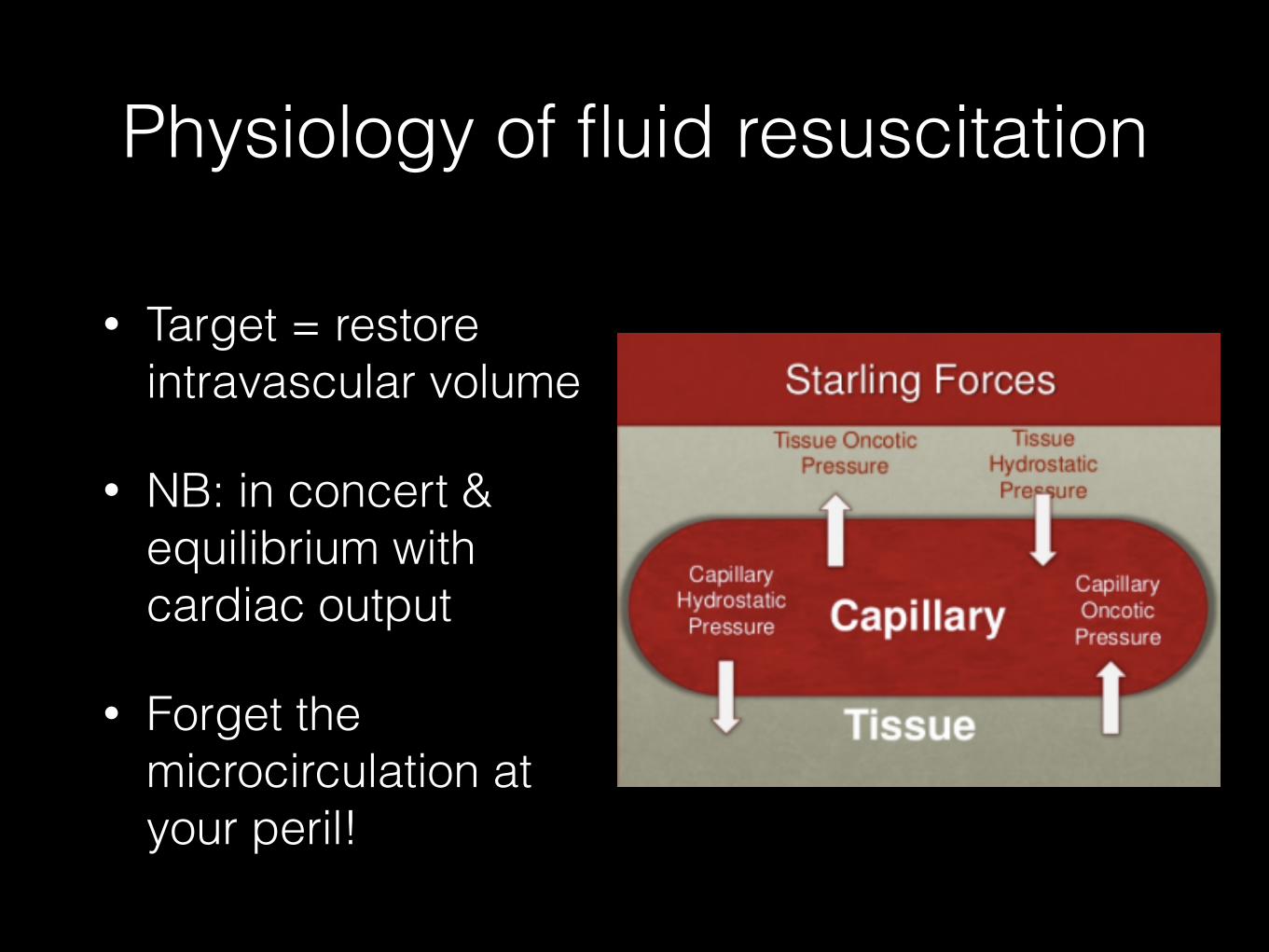
Physiology of fluid resuscitation
• Target = restore intravascular volume
• NB: in concert & equilibrium with cardiac output
• Forget the microcirculation at your peril!
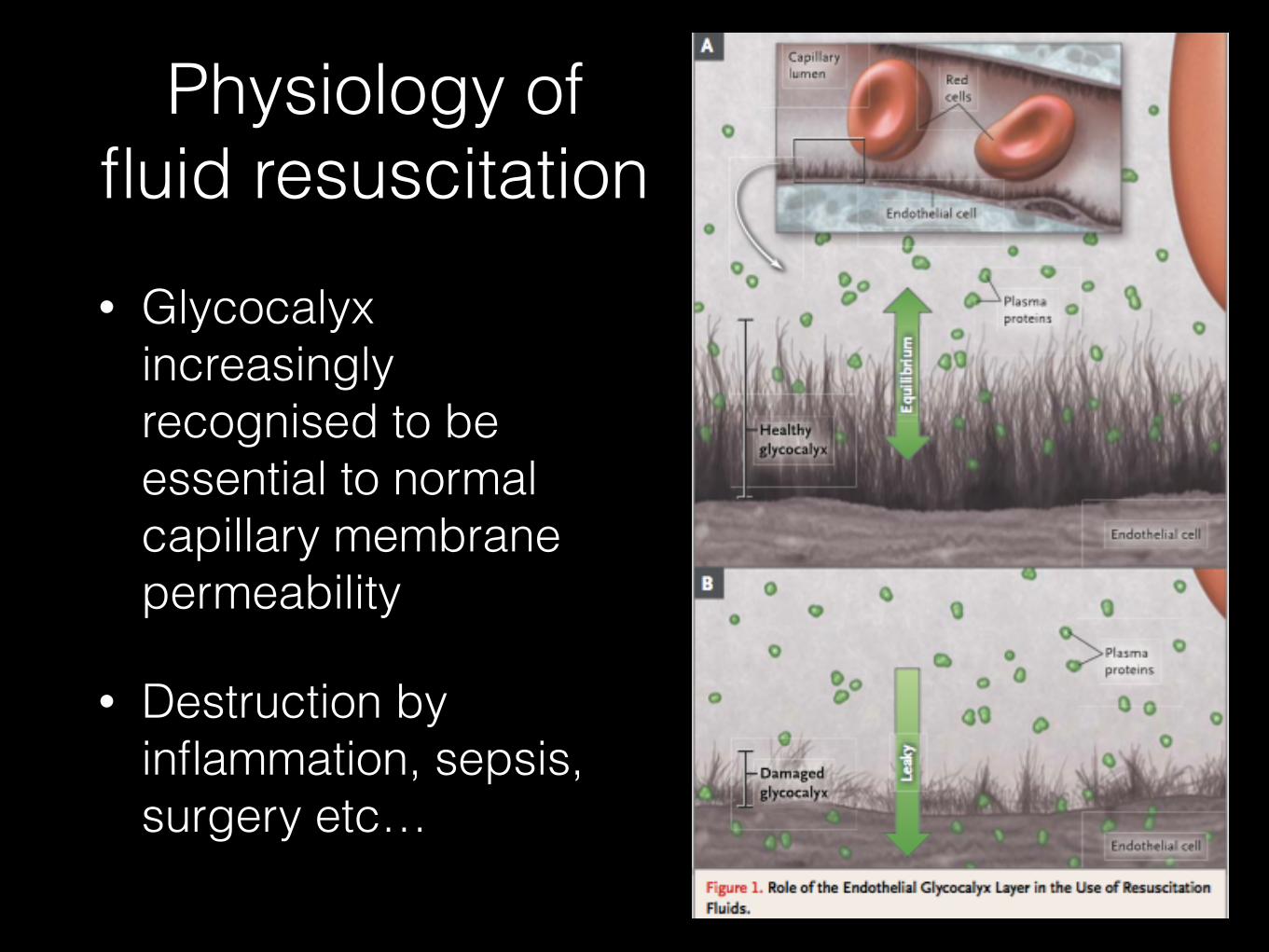
• Glycocalyx increasingly recognised to be essential to normal capillary membrane permeability
• Destruction by inflammation, sepsis, surgery etc…
Physiology of fluid resuscitation
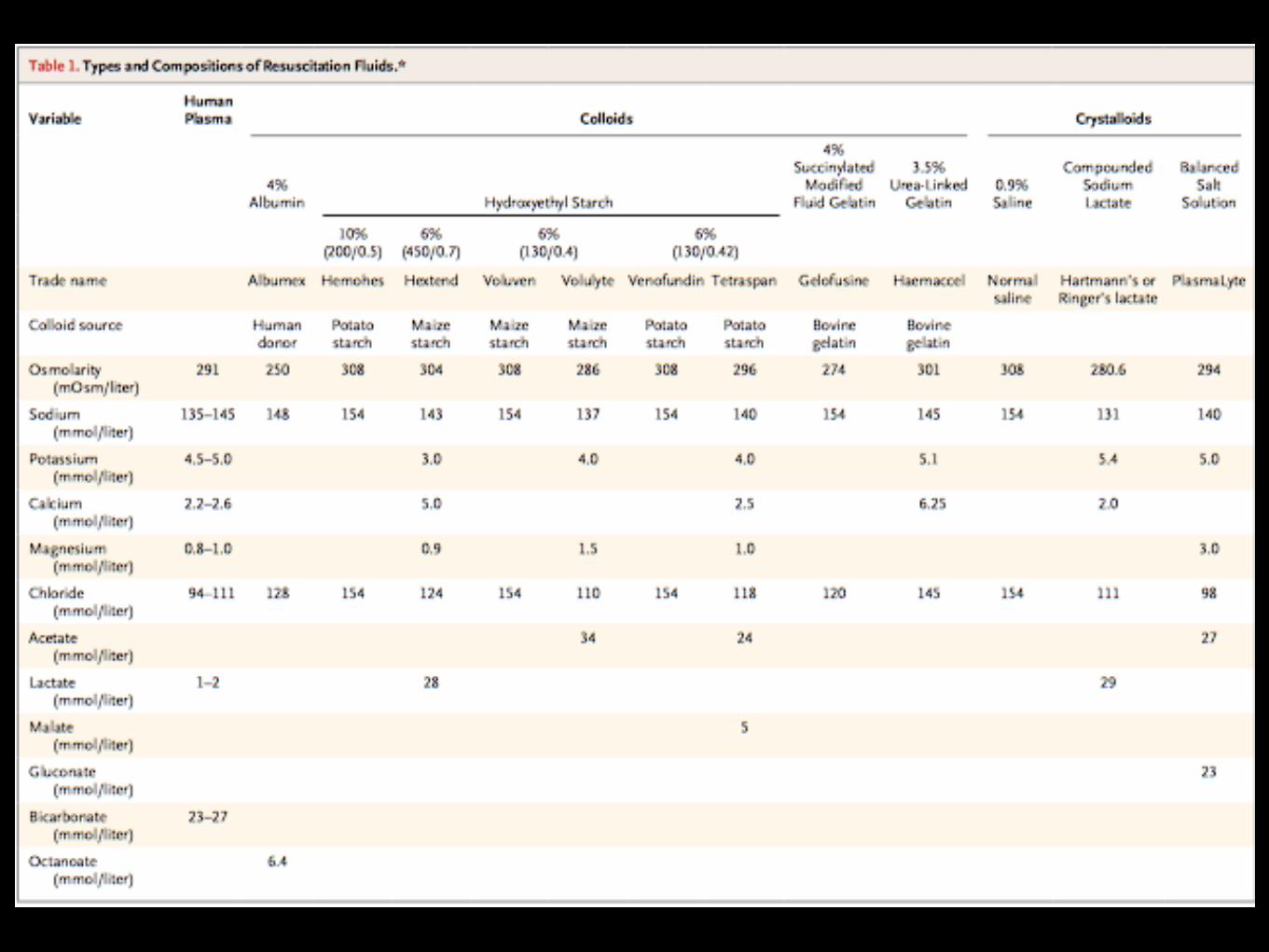
Types of resuscitation fluid
Colloids
• Albumin
• HES (10%, 6%)
• Synthetic starch
Crystalloids
• 0.9% saline
• Hartman’s / CSL
• Plasmalyte
NB: huge variation in global use of these solutions
Ideal resuscitation fluid• Predictable response
• Sustained increase in intravascular volume
• Truely balanced vs ECF
• Metabolised and exerted without accumulation
• No adverse metabolic or systemic effects
• Cheap
• NB: this does not exists currently
Albumin• Reference colloid solution
• Fractionation blood => heat treated
Advantages:
• Safe
• Not as much coagulopathy / renal failure as other colloids
Disadvantages:
• Expensive (not so much in Australia)
• Limited availability in low/middle income countries
• Short shelf life (~1yr)
Albumin• 1998 Cochrane meta-analysis, 24 trials,1419 patients, albumin vs
N/S in hypovolaemia, burns and hypovolaemia => increased mortality (6% increase in absolute risk of death)
• SAFE trial (NEJM, 2004): MRCT, n = 6997, vs 28 day mortality, powered for 3% absolute reduction in mortality
• 4% albumin ‘safe’ compared to normal saline
• Post hoc analysis = TBI and major trauma had worse outcomes with albumin and patients with septic shock tended to better with albumin.
• Martin (CCM, 2005) = pts hypoproteinaemic with ARDS given albumin + frusemide vs frusemide alone => improved oxygenation & CVS stability
AlbuminAn approach …
• Use in
• Spontaneous bacterial peritonitis
• Early resuscitation of ICU patients esp sepsis (further studies pending)
• ARDS in patients with low albumin with frusemide
• NOT to be used in TBI
• ???
• To correct hypoalbuminaemia (<20)
0.9% NaCl• Isotonic
• Not that ‘normal’
• Adverse effects
• Hyperchloraemic metabolic acidosis (strong ion difference = 0)
• Immune and renal dysfunction
0.9% NaCl
• vs HES
• CHEST (NEJM 2012): MRCT, 7000 pts, no significant difference in mortality at 90 days
• HES => pruritus and 21% relative increase in RRT
Plasmalyte solution• Not truely ‘balanced’
• Recommended first line in surgery, DKA, burns, ? trauma
• Single centre trials indicate significant decrease in rate of major complications, infections, CRRT, transfusions
• Adverse effects
• Metabolic alkalosis
• Hyperlactaemia
• Hypotonic (low Na+)
• Micro thrombi (Ca2+ with citrate containing blood transfusions)
• Large RCT about to start …
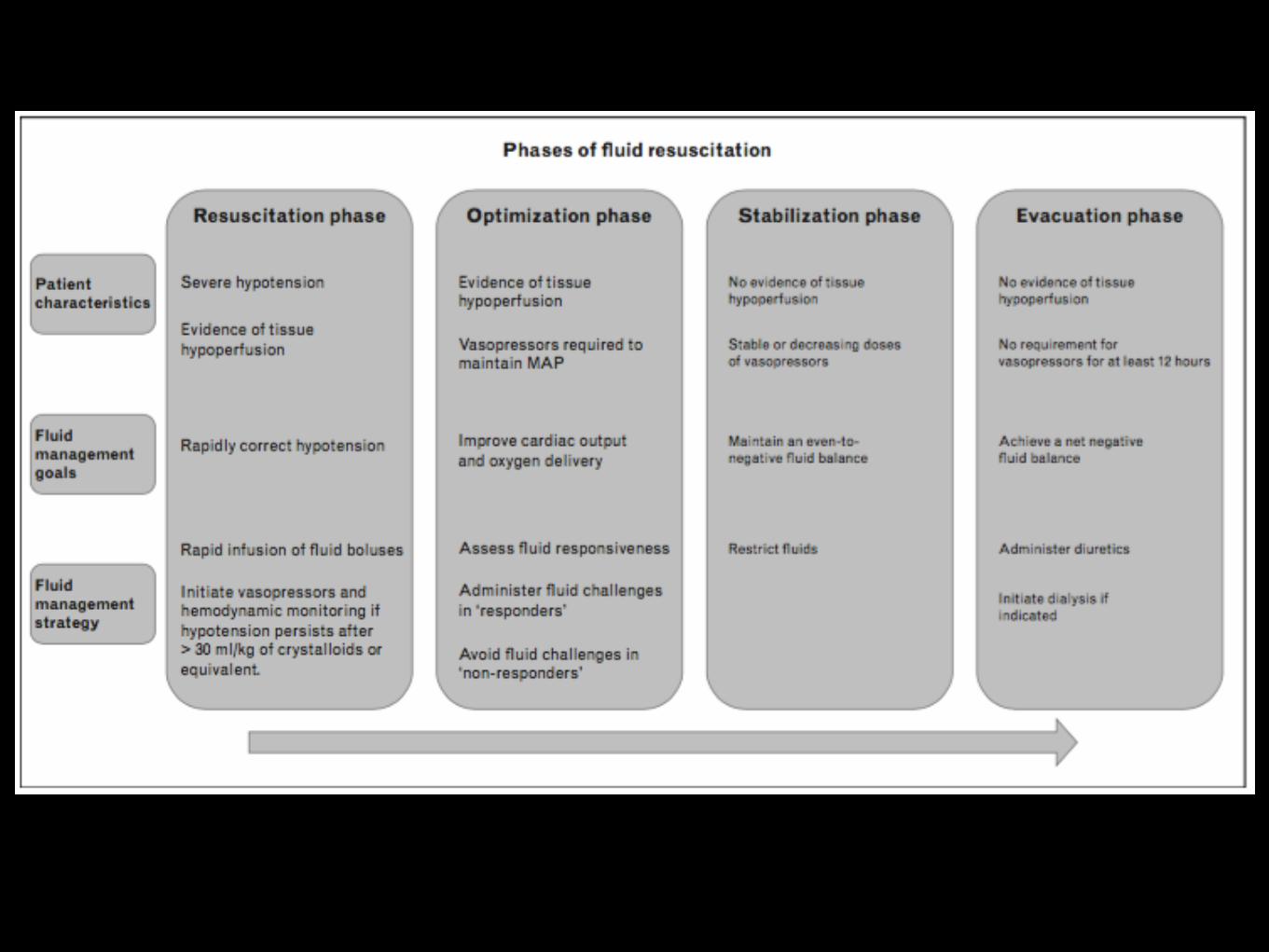
Fluid administration
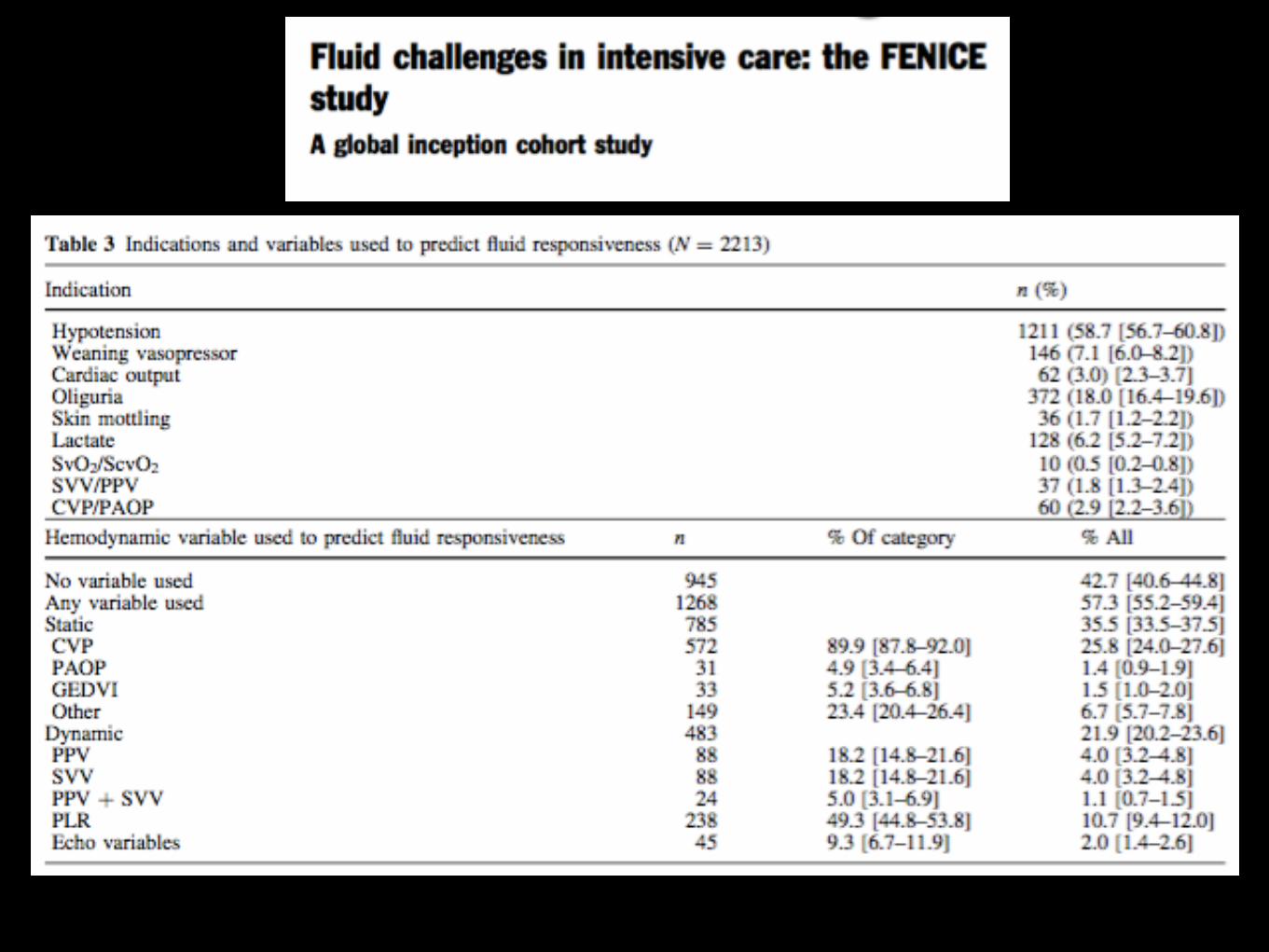
• How do you decide to administer a fluid bolus?
• What measures do you use to predict fluid responsiveness?
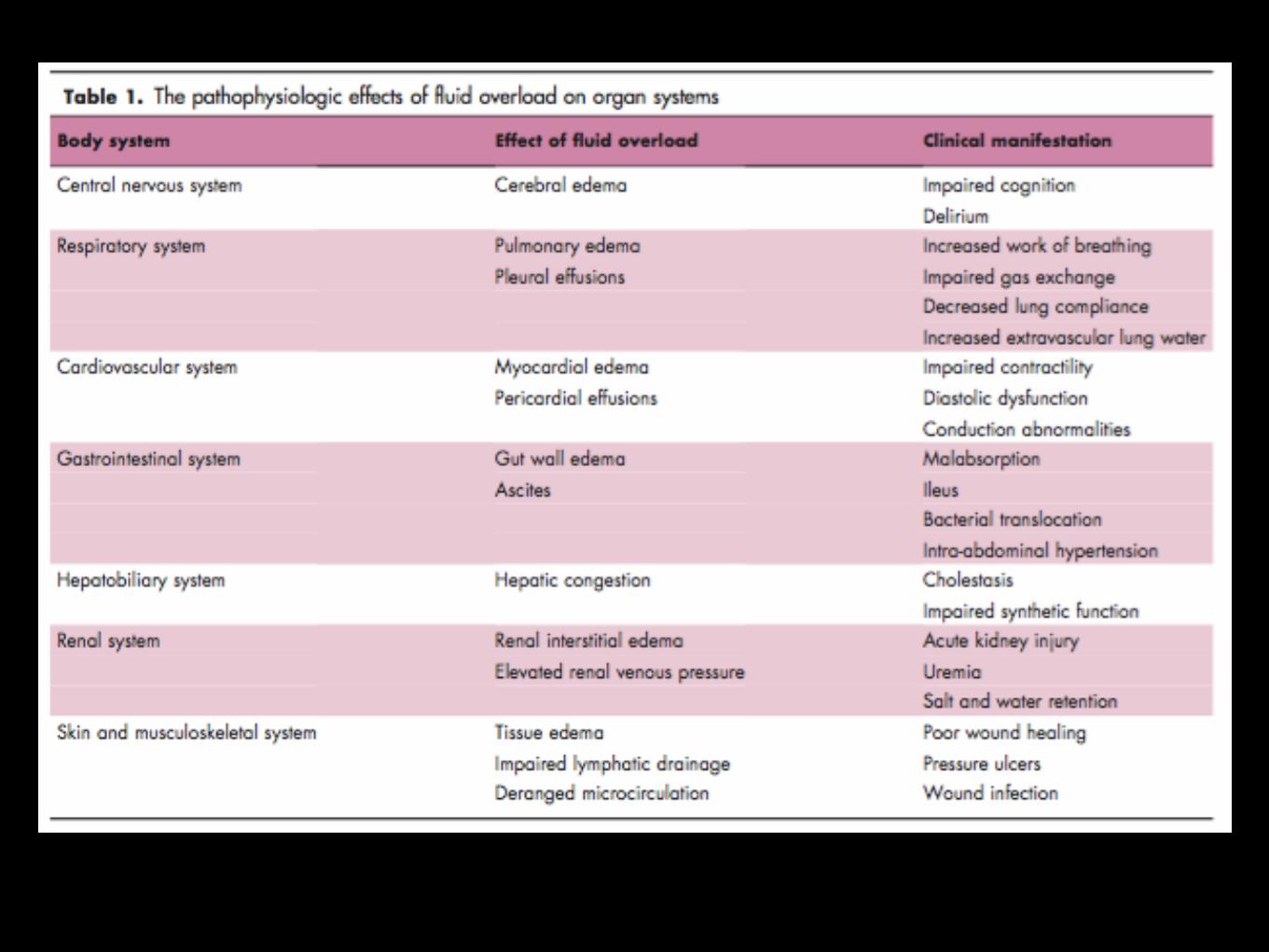
Fluid administration
• What are the adverse effects of excessive fluid administration?
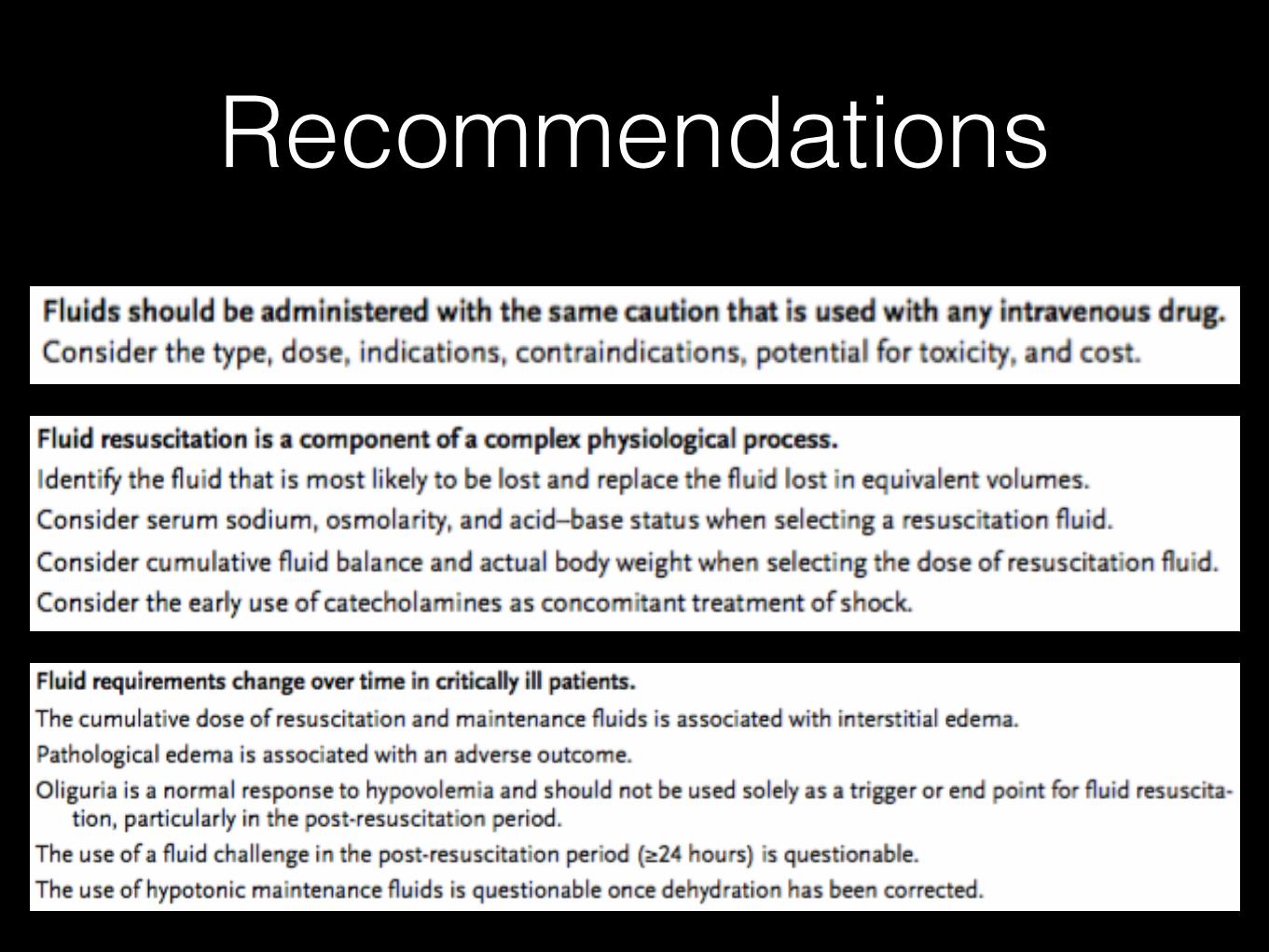
Recommendations
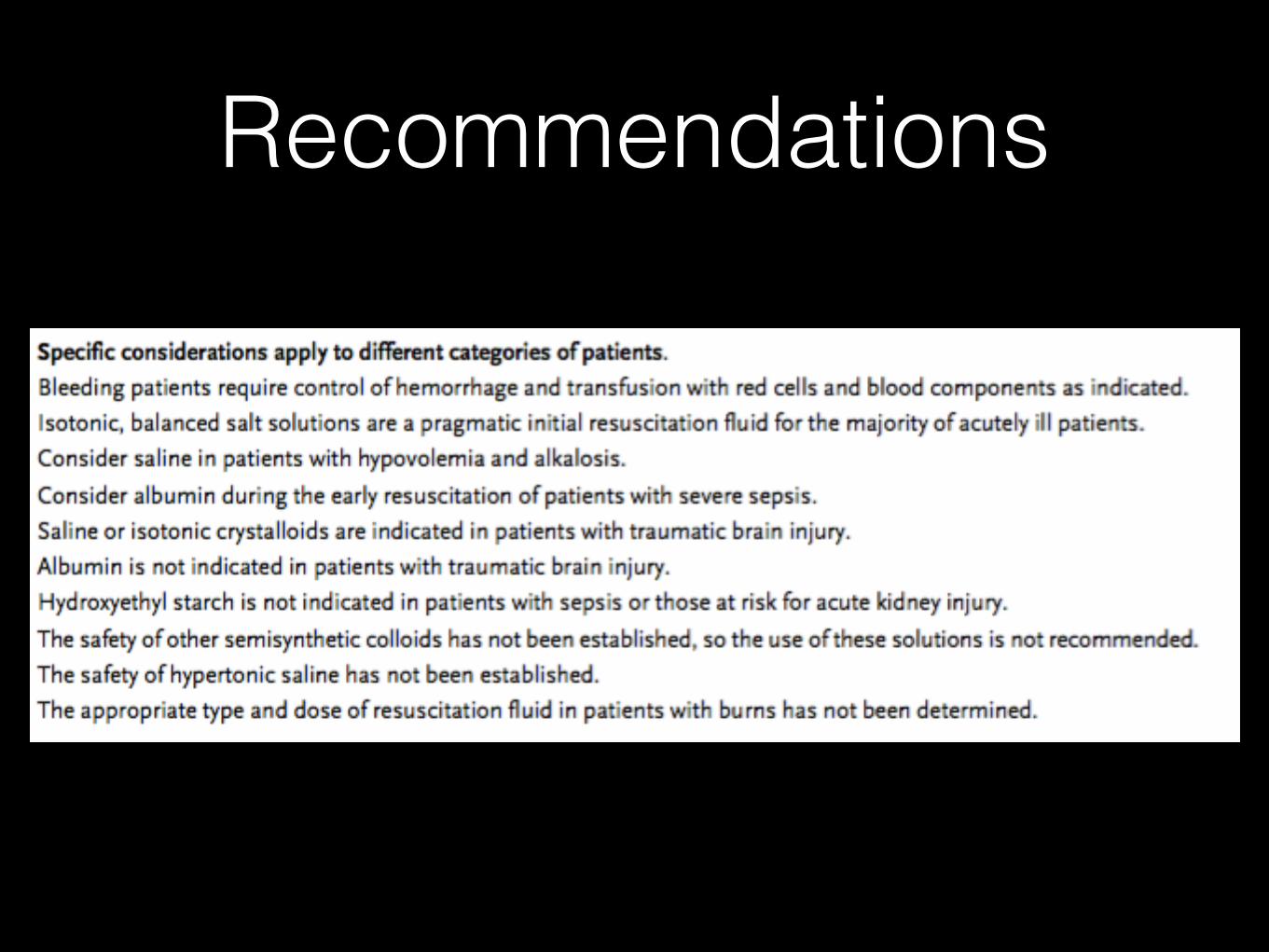
Recommendations
Thank you …• Myburgh JA, Mythen MG. Resuscitation Fluids.
N Engl J Med. 2013 Sep 26;369(13):1243–51.
• Ogbu OC, Murphy DJ, Martin GS. How to avoid fluid overload. Curr Opin Crit Care. 2015 Aug;21(4):315–21.
• CICM part II exams
• “The physiology viva” Kerry Brandis (2003)





























