Embed Size (px)
Citation preview

Fluids , Electrolytes
Sudqi Hamadah


Children are NOT simply small adults
AgeWeight

4
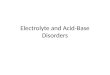
Total body water

Total body Water
Premature
Full Term
2 year old
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%

Internal Distribution of Water

Internal Distribution of Water

ECF - quantity
Age % BW
28-week fetus 55
Newborn 40
12 months 25
Adult 20
Age %BW
12-week fetus 90
Newborn 80
12 months 60
Adult 60
TBW
Internal Distribution of Water

Fluids and Electrolytes• Fluid compartments are separated by membranes
that are freely permeable to water.
• Movement of fluids due to:
– hydrostatic pressure
– osmotic pressure
• Capillary filtration (hydrostatic) pressure
• Capillary colloid osmotic pressure
• Interstitial hydrostatic pressure
• Tissue colloid osmotic pressure

10
Fluids and Electrolytes

Transport of Water and Fluids

Transport of Water and Fluids• Osmosis:
– Movement of water across a membrane from a less concentrated solution to a more concentrated solution
• Diffusion: – The random movement of particles down a concentration
gradient. (high to low)• Active transport:
– movement of solutes across membranes; requires expenditure of energy
• Filtration: – Transfer of water and solutes through a membrane from a
region of high pressure to a region of low pressure

Solutes – dissolved particles
• Electrolytes – charged particles– Cations – positively charged ions
• Na+, K+ , Ca++, H+
– Anions – negatively charged ions
• Cl-, HCO3- , PO4
3-
• Non-electrolytes - Uncharged • Proteins, urea, glucose, O2, CO2

0
100
200
300
400
Protein
Organic Phos.
Inorganic Phos.
Bicarbonate
Chloride
Magnesium
Calcium
Potassium
Sodium
Summary of Ionic composition
InterstitialH2O
PlasmaH2O
CellH2O
Solutes – dissolved particles

ICF (mEq/L) ECF (mEq/L)Sodium 20 135-145Potassium 150 3-5 Chloride --- 98-110Bicarbonate 10 20-25Phosphate 110-115 5Protein 75 10
ECF and ICF Composition
Solutes – dissolved particles

Dehydration-Case 1
• A 5 month male old infant is brought to your ER with 4 day history of vomiting, diarrhea, and reduced oral intake. UOP is markedly reduced. On exam, the infant is fussy but consolable. He pushes you away when you try to examine him.
• Pre-illness Weight is 7 kg (cwt 6.3) (5-25th %ile), BP is 90/55 (50th %ile), HR is 190 (>95th %ile).
• The fontanelle is slightly sunken and his skin turgor is diminished. The cardiopulmonary, abdominal, and neurologic exams are normal.
• He has stopped vomiting but refuses to drink.

Na K Cl HCO3Gastric juice 20-80 15 125 0Small-intestinal juice 100-140 15 155 40Diarrhea 10-90 40 40 40Sweat normal 10-30 10 25 0Sweat CF 50-130 15 75 0
Electrolytes in Body Fluids (mEq/L)
Fluid and electrolytes requirements

Clinical assesment of dehydration

Clinical Observations
Examination 3-5% (mild) 10% (moderate) >10% (severe)Skin turgor Normal Tenting NoneSkin-touch Normal Dry DryBuccal mucosa/lips Moist Dry DryEyes Normal Deep set SunkenCrying/tears Present Reduced NoneFontanelle Flat Soft SunkenCNS Consolable Irritable LethargicPulse Regular Slight increase IncreasedUrine output Normal Decreased Anuric
Clinical assessment of dehydration

Urine specific gravityUrine electrolytesFractional excretion of Na+ (UNa/PNa)/(UCr/PCr)Serum electrolytesSerum osmolality
– 2(Na) + BUN/2.8 + glucose/18 Renal function
Lab assessment of dehydration

ECF and ICF Percentage of Loss
% fluid of deficit % fluid of deficitDuration of illness from ECF from ICF<3 days 80 20>3days 60 40
Fluid and electrolytes requirements

Fluid and electrolytes requirements
Maintenance requirements(metabolism, growth, excretion)
Deficit replacement
Continuing loss
Total requirements

Isonatremic dehydration:– Serum sodium: 130-150 mEq/L.
– 70-80%.
– No fluid shift between ECF and ICF.
Hypernatremic dehydration: – Serum sodium: >150.
– 10-15%.
– Fluid shifts: from ICF to ECF.
– Signs of dehydration modified.
– Irritable and fussy.
– Fever; DI; concentrated formula or ORS;
Types of Dehydration
Hyponatremic dehydration:– Serum sodium: <130.
– 10-15%.
• Fluid shift from ECF to ICF.– Exacerbates volume depletion.
– Diuretics; water without sodium


Cell in a hypertonic solution

Cell in a hypotonic solution

• Isotonic Solutions No change in ICF • Hypertonic Solutions Decrease ICF• Hypotonic Increase ICF
SOLUTIONS USED FOR VOLUME REPLACEMENT THERAPY

0.9 NaCL 154 0 308
Ringers lactate 130 0 272
0.3 NaCl 3.3% dex 53 33 269
0.18 NaCl 5% dex 35 43 321
5% dex 0 50 252
3% NaCl 513 0 1027
Solution Na glucose osmolaritymmol/L gm/L mOsml/L
Osmolality and Tonicity of IV Fluids

0.9 NaCL 154 154 308 5.5
Ringers lactate 130 109 272 6.5
0.45 NaCl 77 77 154 5.5
0.2 NaCl 5% dex 35 35 321 4
5% dex 0 0 252 4
3% NaCl 513 513 1027 5.5
Na Cl Osmolality Solution mmol/L mmol/L mOsmol/L pH
Osmolality and tonicity of IV fluids

SOLUTIONCARBOHYDRATE (G/L)
SODIUM (MMOL/L)
POTASSIUM (MMOL/L)
CHLORIDE (MMOL/L)
BASE* (MMOL/L)
OSMOLARITY (MOSM/L)
ORS
World Health Organization (WHO) [2005]
13.5 75 20 65 10 245
WHO [2002] 13.5 75 20 65 30 245
WHO (1975) 20 90 20 80 30 311
European Society of Paediatric
Gastroenterology, Hepatology and Nutrition
16 60 20 60 30 240
Enfalyte† 30 50 25 45 34 200
Pedialyte§ 25 45 20 35 30 250
Rehydralyte¶ 25 75 20 65 30 305
CeraLyte** 40 50-90 20 NA†† 30 220
COMMONLY USED BEVERAGES (NOT APPROPRIATE FOR DIARRHEA TREATMENT)
Apple juice§§ 120 0.4 44 45 N/A 730
Coca-Cola¶¶ Classic 112 1.6 N/A N/A 13.4 650
Composition of ORS fluids

• Guideline for ORS, – 50mL/kg of the (ORS) within 4hr to in mild dehydration
and – 100mL/kg over 4hr in moderate dehydration
• Supplementary ORS is given to replace ongoing losses from diarrhea or emesis. 10mL/kg of ORS is given for each stool
• ORS is given in small amounts at short intervals (1tsp every 1-2min). Emesis usually lessens over time
ORS guidelines

Overview of IV Rehydration Strategy• Phase I (immediate): If the patient is hemodynamically
unstable or in shock, “one or more” boluses of 20 cc/kg isotonic fluid (0.9%NS or LR) should be given in the first 30 minutes
• Phase II (deficit, maintenance, ongoing fluid replacement):
1. Calculate fluid deficit
2. Calculate maintenance fluid
3. Give ½ of deficit therapy + maintenance over first 8 hours and remainder of deficit + maintenance over next 16 hours
4. Adjust above based on consideration of ongoing losses likely to be encountered

Fluid Management in Children-maintenance
simplified method for calculating caloric expenditure from body weight
Body weight (kg) Caloric expenditure
Up to 10 100 kcal/kg
11 to 20 1000 kcal + 50 kcal/kg for each kg >10 kg
above 20 1500 kcal + 20 kcal/kg for each kg >20 kg
Maintenance fluids and electrolytes: 100 ml water [35ml insensible water loss, 65ml urinary water loss] and 2-4 mmol Na and K for each 100 kcal expended
Nelson Textbook of Paediatrics WB Saunders Company

Fluid Management in Children-maintenance

Body Surface Area MethodFor non-dehydrated patientsWater 1500 ml/M2/24 hrSodium 30-50 mEq/M2/24 hrPotassium 20-40 mEq/M2/24 hr
Mild dehydrationWater 2000 ml/ M2/24 hr
Moderate dehydrationWater 2500 ml/ M2/24 hr
Fluid Management in Children-maintenance

Modifications
Increase DecreaseFever (12% for each oC Renal failure
above 37 oC ) Heart failureHigh ambient temperature Inappropriate secretionDiabetes mellitus of ADHDiabetes insipidus High-humidity respiratoryVigorous exercise therapy
Fluid Management in Children-maintenance

Renal failure: Oligo-anuric patients should receive fluid intake equal to their total output; output must include insensible losses
Neonates:Insensible losses in neonates vary with gestational age and
birth weight and may be dramatically increased by phototherapy or radiant warmers
Newborns cannot concentrate urine as well and GFR is lower so they are more prone to fluid overload
Fluid Management in Children-maintenance

Deficit: Fluid• Definition: Amount of fluid lost before treatment is
begun
• Methods:– Weight loss due to acute illness
• Fluid deficit (L) = Preillness weight (kg) – current weight (kg)
– Estimation of % dehydration• Fluid deficit (L) = [% dehydration x Preillness
weight (kg)] / 100

Deficit: Electrolytes
• Sodium: usually in pediatrics, losses are gastrointestinal or due to a relatively short period of decreased oral intake– approximated by 0.45 NS
• Potassium: deficit replacement is based on rate of safe replacement and not amount since danger of hyperkalemia is greater than hypokalemia– Add 20 mEq potassium/L after UOP is established– Potassium infusion rate should not exceed 1
mEq/kg/hour unless in monitored setting

Case 1: Solution Combined Deficit/Maintenance
• Bolus: 140 cc (20 cc/kg) of NS given for hemodynamic instability
• Deficit Fluid:• Oliguria, tachycardia, no shock 10% dehydrated• Deficit = 10% x 7kg wt loss / 100*= 0.7L or 700cc
– (alternatively 10cc/kg weight loss x 7 kg = 700 cc)
• Maintenance Fluid:– Holliday-Segar: 4 cc/kg for first 10 kg = 7 kg x 4 cc/kg = 28
cc/hr
*Note: Should use preillness weight to calculate deficit = (6.3 kg x 100)/(100-10%) = 7 kg

Case 1: Solution Combined Deficit/Maintenance
• First 8 hours: – Maintenance:
• 28 cc/hr x 8 hours = 224 cc
• In theory: D5 0.2 NS + 20 mEq KCl/L
• In practice: D5 0.45 NS + 20 mEq KCl/L
– Half Deficit = 700/2 = 350 cc of 0.45 NS– Total Fluid = 574 cc/ 8 hour = 71.8 cc/hr
– IVF: 75 cc/hr of D5 0.3 NS + 20 mEq KCl/L• In practice, we would give D5 ½ NS + 20 K
– ADH is increased
– We usually choose between ¼ NS and ½ NS

Case 1: Solution Combined Deficit/Maintenance
• Next 16 hours: – Maintenance:
• 28 cc/hr x 16 hours = 448 cc
• In theory: D5 0.2 NS + 20 mEq KCl/L
• In practice: D5 0.45 NS + 20 mEq KCl/L
– Half Deficit = 700/2 = 350 cc of 0.45 NS– Total Fluid = 798 cc/ 16 hour = 49.9 cc/hr
– IVF: 50 cc/hr of D5 0.45 NS + 20 mEq KCl/L

Dehydration- Case 2
• A 12 year old male is found unresponsive at the bottom of a swimming pool. He is resuscitated in the field and on arrival to the ER is intubated and ventilated but has a spontaneous pulse. In the trauma room, he develops generalized tonic-clonic seizures. He is loaded with phenytoin.
• His weight is 45 kg, BP is 100/70 (normal), HR is 100 (normal). On exam, he is unresponsive and his right pupil is sluggish.

• His stat sodium then returns at 110 mmol/L.
Dehydration- Case 2

Hyponatremic Dehydration
Frequently seen in children with vomiting and diarrhea who have received tap water as an oral replacement
Shock is an early symptom
Physical exam findings usually exaggerate amount of dehydration
Correcting Na+ to quickly in adults can lead to central pontine myelinosis; ???children

Hyponatraemia - Na <130 mmol/L
Equals an expanded ICF
Is it water gain or salt loss?
Salt lossHypernatraemic urineGI tractSweat
Water gainIV fluidsoral fluidscardiac and renal failure
Hyponatremic Dehydration

Acute or Chronic?
SymptomaticSymptomatic oror asymptomatic?asymptomatic?
Hyponatremic Dehydration

Acute Hyponatraemia
Symptoms & signs
•Headache
•Nausea and vomiting
•Somnulence
•Convulsions
•Respiratory arrest
•Brain stem coning
Hyponatremic Dehydration

Hyponatremia and the CNS
H2O
Acute (rapid) onset
Hyponatremic Dehydration

Hyponatremia – Differential Dx
• Hypovolemic– Renal loss
– GI loss
– Sweat
– Third space
• Euvolemic– SIADH
– Glucocorticoid deficiency
– Hypothyroidism
– Water intoxication
• Hypervolemic– Edema forming states
– Renal failure
Hypotonic
Hyponatremic Dehydration

Hyponatremia – Differential Diagnosis
• Isotonic Pseudohyponatremia (Osm 275-295)– Protein
– Lipids
• Hypertonic Hyponatremia (Osm > 295)– Glucose
– Mannitol
Hyponatremic Dehydration

Hyponatremic Dehydration

Correcting Na+ too quickly in can lead to central pontine myelinosis
Follow same steps as for isonatremic dehydrationAdditional Na+ neede = (D Na – S Na) X 0.6 x wt
Symptomatic: Hypertonic saline therapy (1 ml/k NaCL 3% increase serum Na by 1 mEq/L) so give 4-6 ml/k of 3% NaCLCorrect 1-2 mmol/L/hour x several hours if severly symptomaticTarget for increase in serum sodium of no more than 12 mmol/d to prevent osmotic demyelination
Hyponatremic Dehydration

Case 2: Solution• Initial management is to prevent cerebral edema and
herniation; 45 kg
• Use NaCL 3%: 4-6* 45
• The goal of therapy is to increase the serum sodium by 4-6 mmol/L in 3 hours.

Dehydration- Case 3
• A 1 week old female neonate is admitted to the PICU after increasing lethargy and difficulty with breastfeeding. Her birthweight was 3.8 kg. Her admission weight is 3.3 kg.
• On exam, the infant is difficult to arouse. BP is 72/62 (75th %ile), HR is 120 (50th %ile), RR is increased at 60. The PE is unrevealing except for hypotonia and decreased level of consciousness.

• The nurse informs you the sodium is 165 mmol/liter.
Dehydration- Case 3

Serum Na > 150 mEq/L
Mortality can be high
Often iatrogenic
The circulating volume is preserved at the expense of the intracellular volume and circulatory disturbance is delayed
The patient looks better than you would expect based on fluid loss
Hypernatremic Dehydration

Hypernatremia: Clinical Manifestations
• Related to CNS dysfunction; sequelae are prominent when the increase in serum sodium is rapid or large
• Infants: hyperpnea, muscle weakness, restlessness, high-pitched cry, insomnia, lethargy, or coma. Seizures are uncommon.
Hypernatremic Dehydration

Hypernatremic Dehydration

• Slow Correction– Patients with hypernatremia of longer or unknown
duration– Correct sodium by 0.5 mmol/L/hr or 10 mmol/d with goal
of 145 mmol/L
• Rapid Correction– Improves prognosis in patients in whom hypernatremia
developed acutely (sodium loading)– Correct serum sodium by up to 1 mmol/L/hr
Hypernatremic Dehydration-management

• Always assume total fluid deficit of at least 10%• Aim of correction: 145-157 (24hrs), 158-170 (48hrs), 171-
183 (72hrs)
• You only want to correct half of the free water deficit in first 24 hours if Na+ < 175 mEq/L
• For Na+ > 175 mEq/L you do not want to correct faster than 1 mEq/L/hr because of risk of cerebral edema
• Use hypotonic fluids unless frank circulatory collapse exists
Hypernatremic Dehydration-management

Case 3: Solution A• Bolus?: no• Deficit Fluid:
– Deficit = 3.8 kg – 3.3 kg = 0.5 kg or 500 cc
• Maintenance Fluid:– Holliday-Segar: 4 cc/kg for first 10 kg: 3.8 kg x 4 cc/kg =
15.2 cc/hr
• 48 hours needs: – Deficit = 500 cc of 0.45 NS– Maintenance = 15 cc/hr x 48 hr = 720 cc of D5 0.2 NS + 20
mEq KCl/L– Total Fluid = 500 cc + 720 CC = 1200 cc/ 48 hour = 25 cc/h– IVF: 25 cc/hr of D5 0.3 NS + 20 mEq KCl/L

63
Regulation of fluid and electrolytesWater:
• ADH
• Aldosterone
• Thirst
K• Aldosterone• Insulin
Na• Aldosterone• Renin/angiotensin• Atrial Natriuretic Peptide (ANP)

Serum Osmolality• Calculated: (2 x (Na + K)) + (BUN / 2.8) + (glucose / 18) • Measured• Osmolar gap = Osmmeas – Osmcalc
• Methanol/Ethanol/Isopropanol• Mannitol• Ethylene glycol
• Normal: 275 – 295 mOsm/L Isotonic• < 275 mOsm/L = Hypotonic• > 295 mOsm/L = Hypertonic
Regulation of fluids

Normal water homeostasis
• Serum osmolality maintained at 275-295 mOsm/L
• AVP corrects for large variations in water intake
• Osmoreceptor location uncertain, probably anterolateral hypothalamus
• Primary stimulus: increase in plasma osmolality
– Hypoosmolality: ADH secretion suppressed
– Hyperosmolality: ADH level rises

AVP receptors• V1a receptors: vascular smooth muscle, affect vascular tone
• V2 receptors: Kidneys renal collecting duct cells when AVP binds it stimulates adenyl cyclase → cAMPAquaporin-2 (AQP-2) water channels are shuttled to apical plasma membraneIncreased water reabsorption
• V3 receptors: Anterior pituitary, regulate corticotropin release
• V1a receptors: vascular smooth muscle, affect vascular tone
• V2 receptors: Kidneys renal collecting duct cells when AVP binds it stimulates adenyl cyclase → cAMPAquaporin-2 (AQP-2) water channels are shuttled to apical plasma membraneIncreased water reabsorption
• V3 receptors: Anterior pituitary, regulate corticotropin release
Normal water homeostasis

• Osmotic threshold for thirst = 5-10 mOsm/L above that for AVP release
• Kidney regulates body water in response to early, small changes
• Thirst is activated by larger, more threatening disturbances
• Capacity of AVP to limit water loss is limited
– Obligatory minimum urine output (based on solute load) is 6-10 mL/kg/d
Normal water homeostasis

Osmolality : ADH level and Thirst
From:Berl T, Robertson GL. Pathophysiology of Water Metabolism. In: Brenner AM, ed. Brenner and Rector's The Kidney. 6th ed. Philadelphia: W.B. Saunders; 2000:873.
Normal water homeostasis

Non-osmotic stimulators of AVPHypotension, hypovolemia
•Exponential relationship to vasopressin level•Mediated by baroreceptors (atria, aorta, carotid sinus)Am J Physiol Regul Integr Comp Physiol 2000;278(2):R469-75.
Angiotensin II stimulates AVP releaseKeil LC. Endocrinology 1975;96(4):1063-5.
•CHF, Cirrhosis, Nephrotic syndrome
Normal water homeostasis

ADH response in humans
to changes in osmolality,
pressure and volume
Berl T, Robertson GL. Pathophysiology of Water Metabolism. In: Brenner AM, ed. Brenner and Rector's The Kidney. 6th ed. Philadelphia: W.B. Saunders; 2000:875.
Normal water homeostasis

Normal water homeostasis

Factors affecting ADH release

Pathway of RAAS

• Atrial natriuretic peptide

ABG INTERPRETATION
Sudqi Hamadah

What’s normal PH?• The definition of metabolic acidosis in preterm
infants has not been clearly established.
• A normal arterial blood pH in the term infant: pH 7.27- 7.43 at up to 24 hours post birth and 7.32 - 7.42 at seven days of age (Koch 1968).
• Normal BE in the first 28 days of life has been defined as - 5 to + 5 mmol/litre in the preterm infant (Rennie 1999).

• The Joint Working Group of the British Association of Perinatal Medicine recommended maintaining an arterial pH >7.25 [below this pH various physiological and cellular functions are compromised] (BAPM 1992).
• Compensation The lung: CO2 excretion, for Metabolic alkalosis –only
partial compensation (no hypoventilation) The kidney Never overcompensation
What’s normal PH?

ABG Interpretation
• Does the patient have an acidosis or an alkalosis• The primary problem – metabolic or respiratory• Is there any compensation by the patient –
respiratory compensation is immediate while renal compensation takes time
• Normal values– pH 7.35 to 7.45– paCO2 36 to 44 mm Hg– HCO3 22 to 26 meq/L

• For a primary respiratory problem, pH and paCO2 move in the opposite direction– For each deviation in paCO2 of 10 mm Hg in either
direction, 0. 08 pH units change in the opposite direction
• For a primary metabolic problem, pH and HCO3 are in the same direction, and paCO2 is also in the same direction
ABG Interpretation

Case 1
Hasan ingests many tablets of his dad’s barbiturates. He suffers a significant depression of mental status and respiration. You see him in the ER 3 hours after ingestion with a respiratory rate of 4.
A blood gas is obtained (after doing the ABC’s). It shows pH = 7.16, pCO2 = 70, HCO3 = 22

Case 1
What is the acid/base abnormality?
1. Uncompensated metabolic acidosis
2. Compensated respiratory acidosis
3. Uncompensated respiratory acidosis
4. Compensated metabolic alkalosis

Case 2
Suzie had vomiting and diarrhea for 3 days. In her mom’s words, “She can’t keep anything down and she’s runnin’ out.” She has had 1 wet diaper in the last 24 hours. She appears lethargic and cool to touch with a prolonged capillary refill time. After addressing her ABC’s, her blood gas reveals: pH=7.34, pCO2=26, HCO3=12

Case 2
What is the acid/base abnormality?
1. Uncompensated metabolic acidosis
2. Compensated respiratory alkalosis
3. Uncompensated respiratory acidosis
4. Compensated metabolic acidosis

Case 3
You are evaluating a 15 year old female in the ER who was brought in by EMS from school because of abdominal pain and vomiting. Review of system is negative except for a 10 lb. weight loss over the past 2 months and polyuria for the past 2 weeks.
On exam, she is alert and oriented, afebrile, HR 115, RR 26 and regular, BP 114/75, pulse ox 95% on RA. Exam is unremarkable except for mild abdominal tenderness on palpation ,capillary refill time of 3 seconds.
blood gas. pH = 7.21 pCO2= 24 pO2 = 45 HCO3 = 10
BE = -10 saturation = 72%

Case 3
What is the blood gas interpretation?• Uncompensated respiratory acidosis with severe hypoxia• Uncompensated metabolic alkalosis• Combined metabolic acidosis and respiratory acidosis
with severe hypoxia• Metabolic acidosis with respiratory compensation

Expected Compensation
Respiratory acidosis
• Acute –pH ↓0.008 for 1 mm Hg ↑ in paCO2
– HCO3 0.1-1 mEq/liter per 10 mm Hg paCO2
• Chronic –pH ↓ 0.003 for 1 mm Hg ↑ in paCO2;
– HCO3 1.1-3.5 mEq/liter per 10 mm Hg paCO2

Expected Compensation
Respiratory alkalosis
• Acute – the pH increases 0.008 units for every 1 mm Hg decrease in paCO2; HCO3 0-2 mEq/liter per 10 mm Hg paCO2
• Chronic - the pH increases 0.017 units for every 1 mm Hg decrease in paCO2; HCO3 2.1-5 mEq/liter per 10 mm Hg paCO2

Expected Compensation
Metabolic acidosis
• paCO2 = 1.5(HCO3) + 8 (2)
• paCO2 1-1.5 per 1 mEq/liter HCO3
Metabolic alkalosis
• paCO2 = 0.7(HCO3) + 20 (1.5)
• paCO2 0.5-1.0 per 1 mEq/liter HCO3

Elevated AG Metabolic Acidosis
• Causes– Ketoacidosis - diabetic, alcoholic, starvation– Lactic acidosis - hypoxia, shock, sepsis, seizures– Toxic ingestion - methanol, ethylene glycol, ethanol,
isopropyl alcohol, paraldehyde, toluene– Renal failure - uremia

Normal AG Metabolic Acidosis
• Causes– Renal tubular acidosis
– Post respiratory alkalosis
– Hypoaldosteronism
– Potassium sparing diuretics
– Pancreatic loss of bicarbonate
– Diarrhea
– Carbonic anhydrase inhibitors
– Acid administration (HCl, NH4Cl, arginine HCl)
– Sulfamylon
– Cholestyramine
– Ureteral diversions

Effectiveness of Oxygenation
• Further evaluation of the arterial blood gas requires assessment of the effectiveness of oxygenation of the blood
• Hypoxemia – decreased oxygen content of blood - paO2 less than 60 mm Hg and the saturation is less than 90%
• Hypoxia – inadequate amount of oxygen available to or used by tissues for metabolic needs