Page 1 of 2
Flow Cytometry Report
PHYSICIANPATIENTPatient: SAMPLE PATIENTDOB/Sex:MR/Chart #:
Specimen: BONE MARROWCollected: 3/27/2012Received: 3/28/2012
SAMPLE DOCTORCopies:REPORT DATE: 3/28/2012
SPECIMEN
Accession #: All Specimens: 2 BM NA HEP, 1 BM EDTA
1. Increased Myeloid Cells2. Mild Increase in Myeloblasts with
an Abnormal Immunophenotype
INTERPRETATION:
Comment:These abnormalities can be seen in a variety of myeloid
neoplasms, including
myeloproliferative,myeloproliferative/myelodysplastic and
myelodysplastic disorders. Correlation with the CBC/Diff data
andexamination of a stained bone marrow aspirate smear suggest that
a myeloproliferative neoplasm is most likely inthis case.
CD34 positive blasts account for 2% of total white blood cells
and have an aberrant myeloid immunophenotype.Blasts espress CD34,
CD38, dim CD33, bright HLA-DR, dim CD11b, dim CD117, dim CD45,
without expression ofCD13, CD56, CD7, CD2, CD16, CD14, CD41, CD64
and CD61. The viability of the specimen is 82%. Thegranulocytes
(88% of the total white blood cells) and monocytes (1% of the total
white blood cells) reveal nosignificant immunophenotypic
abnormalities. B-cells comprise 8% of the lymphocytes and have a
kappa:lambdaratio of 1.03. Approximately 78% of lymphocytes are
T-cells with a CD4:CD8 ratio of 1.14 (Normal 1-4). NK cellsaccount
for 1% of the total white blood cells (14% of lymphocytes). Plasma
cells are not detected.
FLOW CYTOMETRY DIFFERENTIAL(% of total cells)
LYMPHOCYTES 4 B CELLS 4Kappa:Lambda Ratio 1.03 T CELLS 38CD4:CD8
Ratio 1.14 Large Granular Lymphs 5 NK CELLS 7MONOCYTES
1GRANULOCYTES 88BLASTS 2PLASMA CELLS NegativeVIABILITY 82
ANTIBODIES ANALYZED:Antibodies used for evaluation include:
CD2,3,4,5,7,8,10,11b,13,16,19,20,33,34,38,45,56,57,7AAD, HLADR,
kappa,lambda,14,41,61,64,117
Leukocytosis, thrombocytosis.CLINICAL HISTORY:
The immunohistochemical assays were developed and their
performance characteristics determined by OncoMetrix. They have not
been cleared or approved by the U.S. Food and DrugAdministration.
The FDA has determined that such clearance or approval is not
necessary. This testing is used for clinical purposes. It should
not be regarded as investigational or forresearch. This laboratory
is certified under the Clinical Laboratory Improvement Amendments
of 1988 (CLIA) as qualified to perform high complexity clinical
testing.
IDC9 Codes: 288.60, 238.71 CPT Codes: 88184; 88185x27;
88189(877) 670-HEME (4363)
Dr. Douglas W. Kingma, Laboratory Director
OncoMetrix
CLIA #: 44D0915029, TN License #: 0000003284
150 Collins Street, Memphis, TN 38812Poplar Healthcare, PLLC
Howard L. Martin, III, M.D., Medical Director
BONE MARROW ASPIRATE:
Page 2 of 2
Flow Cytometry Report
PHYSICIANPATIENTPatient: SAMPLE PATIENTDOB/Sex:MR/Chart #:
Specimen: BONE MARROWCollected: 3/27/2012Received: 3/28/2012
SAMPLE DOCTORCopies:REPORT DATE: 3/28/2012
SPECIMEN
Accession #: All Specimens: 2 BM NA HEP, 1 BM EDTA
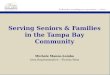
IMAGES:
Increased myeloid cells; smallpopulation of blasts present.
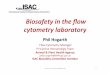
Normal myeloid immunophenotype inmaturing myeloid cells.
Normal myeloid immunophenotype inmaturing myeloid cells.
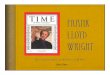
Blasts show aberrant co-expressionof CD34 and CD11b.
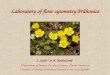
Polyclonal B-cells. Normal CD4:CD8 ratio.
Mihaela Onciu, M.D.Hematopathologist
Electronically signed3/28/2012 4:43 PM by
The immunohistochemical assays were developed and their
performance characteristics determined by OncoMetrix. They have not
been cleared or approved by the U.S. Food and DrugAdministration.
The FDA has determined that such clearance or approval is not
necessary. This testing is used for clinical purposes. It should
not be regarded as investigational or forresearch. This laboratory
is certified under the Clinical Laboratory Improvement Amendments
of 1988 (CLIA) as qualified to perform high complexity clinical
testing.
IDC9 Codes: 288.60, 238.71 CPT Codes: 88184; 88185x27;
88189(877) 670-HEME (4363)
Dr. Douglas W. Kingma, Laboratory Director
OncoMetrix
CLIA #: 44D0915029, TN License #: 0000003284
150 Collins Street, Memphis, TN 38812Poplar Healthcare, PLLC
Howard L. Martin, III, M.D., Medical Director














![FLW-AD[1] - Copy](https://img.pdfslide.us/doc/110x75/58ecbb891a28ab12068b45b3/flw-ad1-copy.jpg)