Embed Size (px)
Citation preview
Improving Early Identification and Treatment of Adolescent Depression
in Primary CareFlorida Mental Health Summit
August 2015
Elise Fallucco, MDChild and Adolescent Psychiatrist, Nemours Children’s Specialty CarePhysician Scientist, Nemours Center for Health Care Delivery Science

Can adolescents get depressed?Symptoms: 2 weeks +
Irritability, loss of interestHopeless, helpless, worthlessChanges in sleep, appetite, energy, concentrationSuicidal thoughts
Over 2 million new cases of adolescent depression each year
Depression is often a chronic illness50% single episode50% multiple episodes
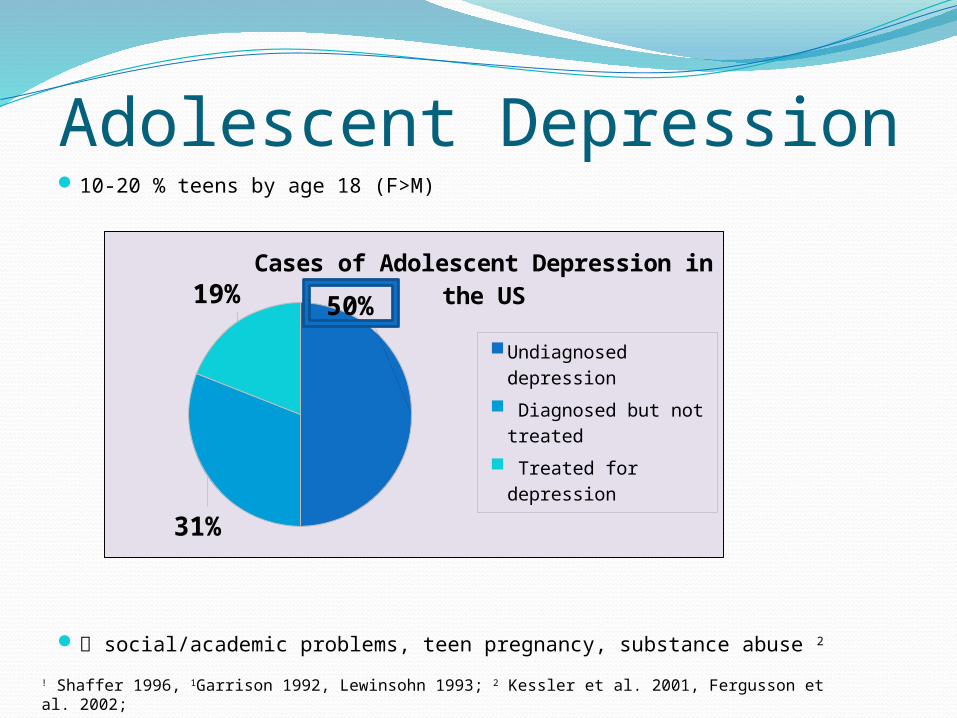
Adolescent Depression10-20 % teens by age 18 (F>M)
social/academic problems, teen pregnancy, substance abuse 2
! Shaffer 1996, 1Garrison 1992, Lewinsohn 1993; 2 Kessler et al. 2001, Fergusson et al. 2002;
50%
31%
19%
Cases of Adolescent Depression in the US
Undiagnosed depression
Diagnosed but not treated
Treated for depression
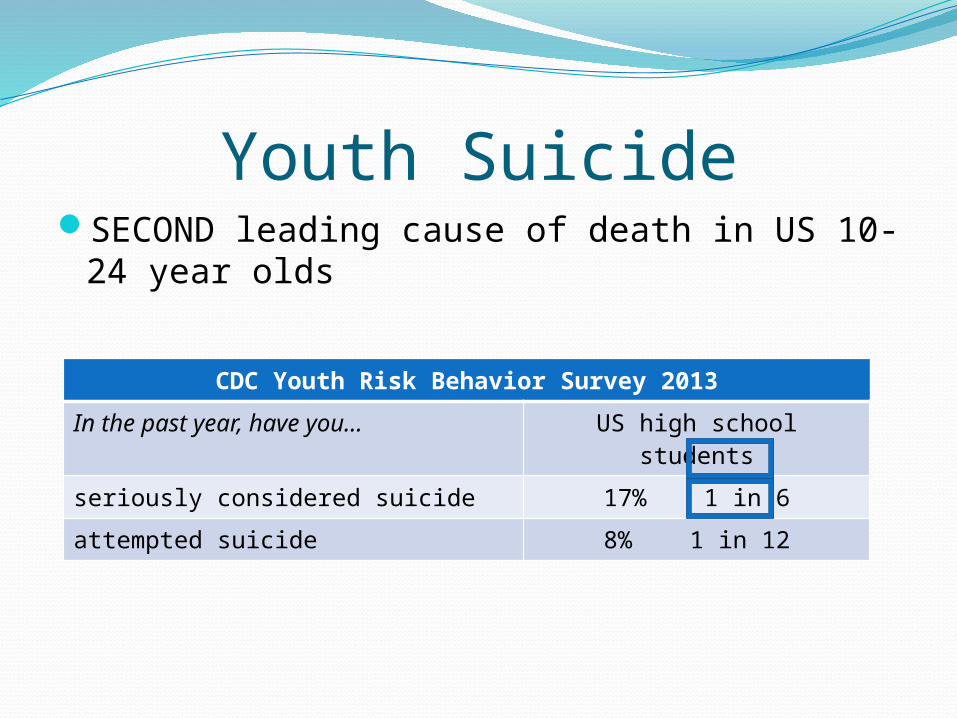
Youth SuicideSECOND leading cause of death in US 10-24
year olds
CDC Youth Risk Behavior Survey 2013
In the past year, have you… US high school students
seriously considered suicide 17% 1 in 6
attempted suicide 8% 1 in 12
Aaron, 15 years oldStraight-A student at prestigious prep schoolVarsity athleteVisit to grandfather’s house

Opportunities to identify teensPrimary care is an ideal setting
Primary care providers (PCPs) are trusted health care professionals
PCPs see > 70% US adolescents annually (Newachek et al, 1999)
Each PCP sees between 200-500 teens each yearMany suicide victims (45%) saw PCP in the month
before death (Luoma et al, 2002)
Case for Primary Care ScreeningOnly 2 strategies proven to reduce suicide rates
(JAMA 2005)Educating physicians in depression recognition and
managementLimiting access to lethal means
Screening for depression recommended in primary careUnited States Preventive Services Task Force (2009)American Academy of Pediatrics (AAP; 2007, 2009,
2010)
Missed opportunitiesLimited primary care screening occurs
Only 22% PCPs routinely screen for depression (Fallucco, 2010)
PCPs screen few teens at well-visits (34%; Ozer, 2009)
Barriers to screening Inadequate PCP training, knowledge regarding
depression assessment and treatment (Olson, 2001)Limited access to child psychiatrists (Thomas,2006)
8 child psychiatrists (CAPs) : 100,000 children <18 yoFlorida: 7.0 CAPs per 100,000Delaware: 7.2 CAPs per 100,000
Addressing barriersScreening, assessment and treatment of adolescent
depression (SATD) workshop for PCPs2+1/2 hour training developed by a team of child and
adolescent psychiatrists, therapists, and pediatriciansInvolves skill-building seminar and hands-on practice
Over 200+ pediatricians and pediatric ARNPs trained 12 STL pediatric residents (Fallucco, 2010) and 15 pediatric
gastroenterologists 46 STL PCPs (Fallucco, 2012) 90 Jax PCPs (Fallucco et al, 2015) 70 Nemours PCPs in Delaware and Central Florida
Part One: Skill-Building Seminar
•How to screen for depression•3-step algorithm for evaluating positive screens•How to assess patient for suicide risk•When/where to refer•Treatment strategies
• Antidepressants• referral for therapy
•Billing and coding for screening
Part Two: Practice Skills with TeensPCP practices two x 10-minute mock interviews• Case 1: 16 yo with low mood, poor grades
• Case 2: 17 yo with irritability, drug use
PCP receives verbal feedback from teens about communication skillsDebriefing with CAP
Training among Jax PCPs32 PCPs (25 pediatricians, 7 ARNPs)
Years in pediatric practice: mean 16 yrs (range 1-37 yrs)
Weeks of mental health training: Mean 2.9 weeks
Adolescent patients (total n= 1315) surveyed at well-visits, “Did your doctor ask you if you have been feeling down?”n=582 baselinen=525 at 2-8 months post-trainingn=208 at 18-24 months later

Adolescent patients (n=1315)Mean age = 14.3 yo, SD 1.8 (range 12-18 yo)Gender
Male (45%) Female (55%)
Race/Ethnicity: Caucasian (78%) African American (12%) Hispanic/Latino (8%)

PCP screening for depressionGeneral trends in depression screening
Girls more likely to be screened (OR 1.65, 95% CI 1.25-2.16, p<.0003)
Older teens more likely to be screened (18 vs. 12 yo OR 2.0, 95% CI 1.3-3.8)
Screening did not differ by adolescent race, ethnicity; provider gender or degree
Generalized linear mixed effects logistic regression
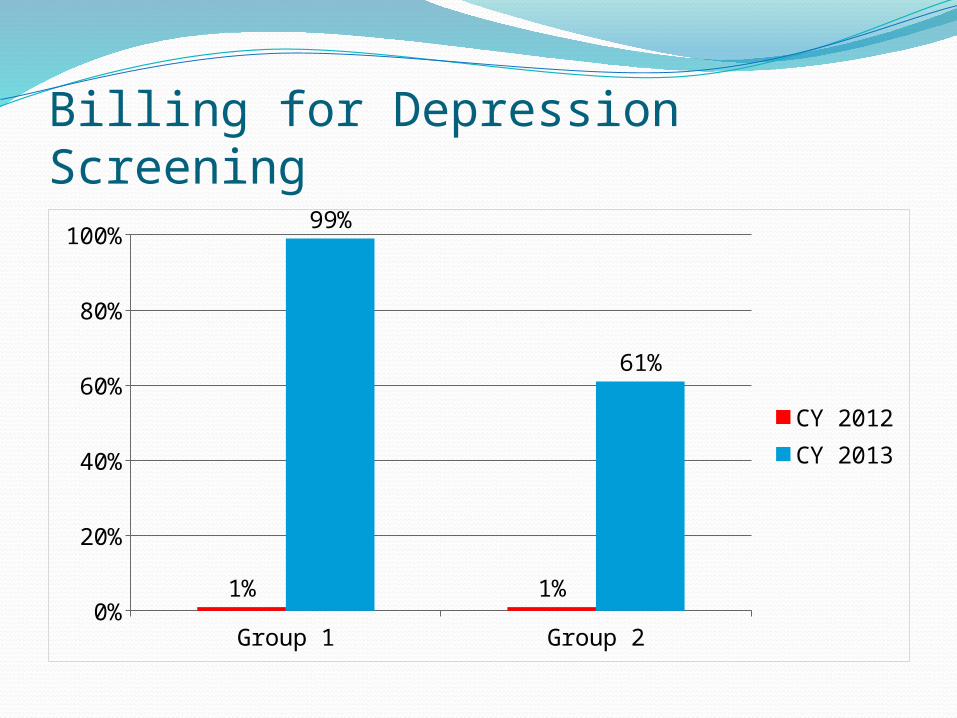
Billing for Depression Screening
Group 1 Group 20%
20%
40%
60%
80%
100%
1% 1%
99%
61%
CY 2012CY 2013
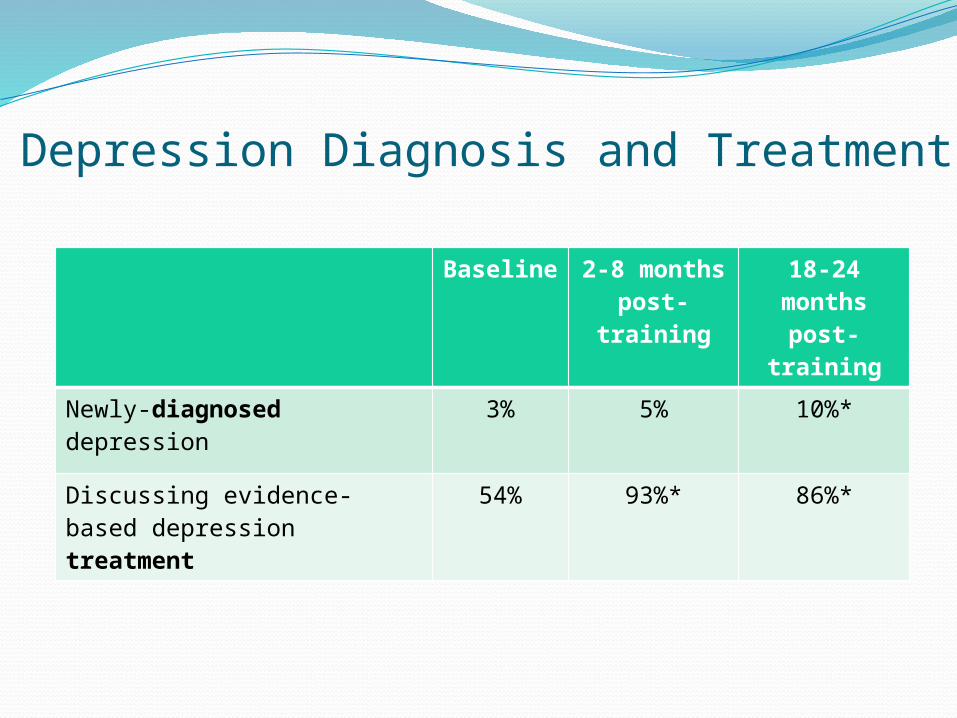
Depression Diagnosis and Treatment
Baseline 2-8 months post-training
18-24 months
post-training
Newly-diagnosed depression 3% 5% 10%*
Discussing evidence-based depression treatment
54% 93%* 86%*
Impact of TrainingFor every pediatrician trained, 200-500 teens
screened each yearJacksonville: Over 90 PCPs trained to date
12,000 – 30,000 teens screened each year