Embed Size (px)
Citation preview
American Journal of Medical Genetics 43:1006-1011 (1992)
~
Five Years Experience of Predictive Testing for Myotonic Dystrophy Using Linked DNA Markers W. Reardon, J.L. Floyd, J. Myring, L.P. Lazarou, A.L. Meredith, and P.S. Harper Institute of Medlcal Genetlcs, University Hospital of Wales, Heath Park, Cardiff, Wales
We report on a 5 year experience in providing presymptomatic and prenatal molecular di- agnostic services for myotonic dystrophy, using closely linked markers, representing 235 completed results in 161 families. Only 10 an- alyses (4.3%) proved uninformative, but a fur- ther 5 requests (1.9%) could not be reported because of uncertainty in clinical status. Seven of 81 (8.6%) patients considered to be at low risk on clinical grounds were found to be at high risk of carrying the gene. The impor- tance of interpreting molecular results in con- junction with clinical findings is emphasised by the illustrative examples provided. Careful clinical examination and appropriate investi- gation remain a cornerstone of diagnosis in myotonic dystrophy and are crucial if errors in assigning genotype status by molecular means are to be minimised. o 1992 wiley-fiss, InC.
KEY WORDS presymptomatic diagnosis, muscular dystrophy, chro- mosome 19 markers
INTRODUCTION Myotonic dystrophy is the commonest muscular dys-
trophy of adult life [Harper, 19891. Because of its autoso- ma1 dominant inheritance and variable manifestations the diagnosis of this condition in a patient frequently raises concern in other relatives as to their own status. Several biochemical, endocrine, and immunological markers have been assessed as markers of gene carrier status but none has been found satisfactory [Schubert et al., 1980; Harper, 1973; O’Brien and Harper, 1984; Walsh et al., 1970; Barbosa et al., 1974; Bundey et al., 1970; Roberts and Bradley, 19773 and the primary gene product remains unknown. It has long been recognised that absence of symptoms is not a reliable indicator of
Received for publication August 12, 1991; revision received De- cember 16, 1991.
Address reprint requests to Dr. Reardon, Institute of Medical Genetics, University Hospital of Wales, Heath Park, Cardiff CF4 4XN, Wales.
0 1992 Wiley-Liss, Inc.
genotype status but, in combination with electro- myography (EMG) and slit lamp examination of the lenses, clinical examination frequently detects asymp- tomatic affected individuals though the proportion of gene carriers detected in this manner is uncertain [Har- per, 19891. These data, combined with age-of-onset curves for myotonic dystrophy, for many years formed the basis of genetic counselling in this condition, but the wide differences in age-at-onset even within a single family have limited the accuracy of these risk estimates.
The establishment of linkage between the gene for myotonic dystrophy and chromosome 19 markers pro- vided a method of predicting genetic status of a person at risk that was independent of age and of phenotype [Eiberg et al., 19831. In particular, identification of close linkage between the ApoCII and myotonic dystrophy gene loci meant that a highly polymorphic marker was available for clinical application [Shaw et al., 19851. The value of this strategy was quickly established [Meredith et al., 19861 and in a review of 145 diagnostic requests pertaining to 99 families, some of the practical problems encountered in providing this service were emphasised [Norman et al., 19891. Since early 1986 this department has offered predictive testing for myotonic dystrophy using linked DNA markers. New, more closely linked probes have been introduced to the service during this period, thus reducing the problem of uninformativeness in families.
We now report our 5 year results of molecular testing for myotonic dystrophy and discuss some of the relevant principles which have been established, as well as the remaining problems. The total data include those given in our earlier report [Norman et al., 19891.
METHODS Family Data
Requests for molecular investigation were made on behalf of 161 kindreds, 41 of whom were within our own region, 20 from abroad and 100 from other U.K. centres. Clinical data, pedigree information, and blood or DNA samples were provided by the referring centre, in close consultation with us. Since 1989 Cardiff has formed part of the West of Britain Molecular Genetics Consortium and is responsible for molecular analysis for myotonic dystrophy families referred through the 5 health re- gions forming this group.
Predictive Testing for Myotonic Dystrophy 1007
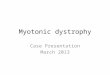
TABLE I. Distribution of Reauests Over the 5 Year Period
Presymptomatic Year requests 198611987 35 1988 31 1989 21 1990 19 1991 15
Total 121 (end June)
Informativeness for prenatal Prenatal
diagnosis requests diagnoses Total 48 5 88 33 6 70 15 4 40 17 3 39 6 2 23
119 20 260
DNA Analysis The DNA extraction, restriction endonuclease diges-
tion, size fractionation, and membrane transfer were as reviously described [Norman et al., 19891. Probes were
'P radiolabelled by the random hexanucleotide label- ling method [Feinberg and Vogelstein, 19831 and excess label removed by washing in progressively less concen- trated solutions of SSC. Autoradiographs were gener- ated on Fuji X-ray film using intensifying screens at -70°C for 1-7 days.
Linked DNA Markers Used in Predictive Testing The panel of markers used has previously been sum-
marised [Norman et al., 19891 and D19S63 (DlO), which detects polymorphisms with PvuII and Hinc 11, has been added to the panel. Initially ApoCII alone was employed and combined use of the different polymorphisms which it detects gave an individual a 66% chance of being heterozygous and informative with this probe alone. The problem of uninformativeness with ApoCII was ex- acerbated by linkage disequilibrium between the Apo- CII polymorphisms [Wallis et al., 19841. This problem has been largely overcome by the introduction of CKM, BCL3, and most recently D19S63. The linkage disequi- librium observed between D19S63 and myotonic dystro- phy has not as yet been used clinically (discussed below).
RESULTS To date 260 requests have been processed from 161
families. Table I gives the distribution of requests over the 5 year period. The initial influx of requests in the first 2 years of the service related mainly to families already known, whereas more recent requests have in- volved newly ascertained patients and families. In the first year of testing the ApoCII polymorphisms formed the mainstay of predictive testing and uninformative- ness precluded a result in over 25% of requests. This problem has been resolved by the subsequent introduc- tion of further markers. Most of those initial failures to answer a request have since been overcome and in only 10 of 235 (4.3%) results has it proven impossible to offer a service due to uninformativeness with the poly- morphic markers used in the series.
There have been 121 requests for classification of gene carrier status; >2/3 of which were for females (Table 11). The main reason for failure to generate a result was the unavailability of DNA from key relatives. A satisfactory result could not be obtained in 2 instances due to failure
TABLE 11. Presymptomatic Tests
Total no. of requests
Results obtained
Males Females
High Risk Low risk Uninformative Unable to set phase due to uncertain clinical
Total
Minors Poor DNA. Repeat sample requested but not
No DNA received on key family members Request withdrawn Request processed elsewhere Ongoing Total
status in key person
Results not obtained
received
121 39 82
19 76 5 2
102
4 2
6 1 1 5
19
to establish the identity of the asymptomatic gene car- rier in a previous generation and, thus, t~ set phase.
One hundred nineteen requests for informativeness in a future prenatal diagnosis have been processed (Ta- ble 111). The female preponderance among patients re- questing this service is most readily explained by the maternal transmission of the congenital form of the disease [Harper, 19891.
Requests for prenatal diagnosis have numbered 20 (Table IV). Notwithstanding the expenditure of much laboratory effort in preparing for prenatal diagnoses prior to pregnancy (Table 1111, most prenatal diagnostic requests concern patients who have not had molecular analysis prior to pregnancy (Table IV). While disap- pointing for the families, the uninformative status of 2 pregnancies is an inherent hazard of having these tests
TABLE 111. Informativeness for Prenatal Diacrnosis
Total no. of requests
Results obtained
Females Males
High risk females High risk males Uninformative Unable to establish phase Total
119 93 26
89 24 3 3
119
1008 Reardon et al.
TABLE IV. Prenatal Diagnoses
Total no. of pregnancies Informativeness determined prior to pregnancy Pregnancy preceded receipt of samples Mother affected Father affected Samples received
cvs Amniocytes
Miscarriages prior to sampling Results
Low risk predicted High risk predicted Uninformative Amniocytes failed to grow
Total Terminated Congenitally affected child Infant of affected father; clinically normal a t birth
Total Normal infants delivered Pregnancy ongoing Lost to follow-up (abroad)
Outcome of pregnancies a t high risk
Outcome of pregnancies at low risk
~~
20 8
12 17 3
18 15 3 2
8 7 2 1
7 5 1 1
8 6 1 1
performed without prior determination of informative- ness. Both pregnancies occurred in the early stages of the program (198711988) and this outcome is much likely now due to the influence of other available poly- morphisms. No example of an incorrect prenatal predic- tion has come to our attention. However, it is apparent from our data that not all couples have prenatal diag- nosis with a view to terminating high risk pregnancies. In our series 2 such pregnancies continued to term, one resulting in a congenitally affected infant. The second couple electing to continue the pregnancy had already terminated an earlier pregnancy when the baby was predicted to be 98% likely to have inherited myotonic dystrophy from its father. A similar risk was predicted in the second pregnancy, which was continued, and signs of disease were not apparent at birth.
The identification of only 19 high risk individuals indicates that predictive tests are used by clinicians where clinical signs are absent or equivocal. Seven such patients, detailed in Table V, were entirely normal clini-
cally. Of the remaining 12, all were normal clinically. Five of the 12 had normal EMGs and 7 did not have this investigation. However, all 12 patients had ophthalmic evidence of the disease when examined by slit lamp, although this examination frequently followed molecu- lar prediction of high risk.
There have been 9 instances in which the molecular data have been at odds with the clinical findings. Most (7) have concerned clinically normal patients, in whom molecular results predict the inheritance of the disease (Table V). A further 2 cases were identified at low risk on haplotype analysis whose clinical data call this conclu- sion into question (Table V). Some of the problematic cases encountered in our series are discussed below as practical examples of the difficulties which can arise even with informative markers in favourably structured families when presymptomatic tests are undertaken.
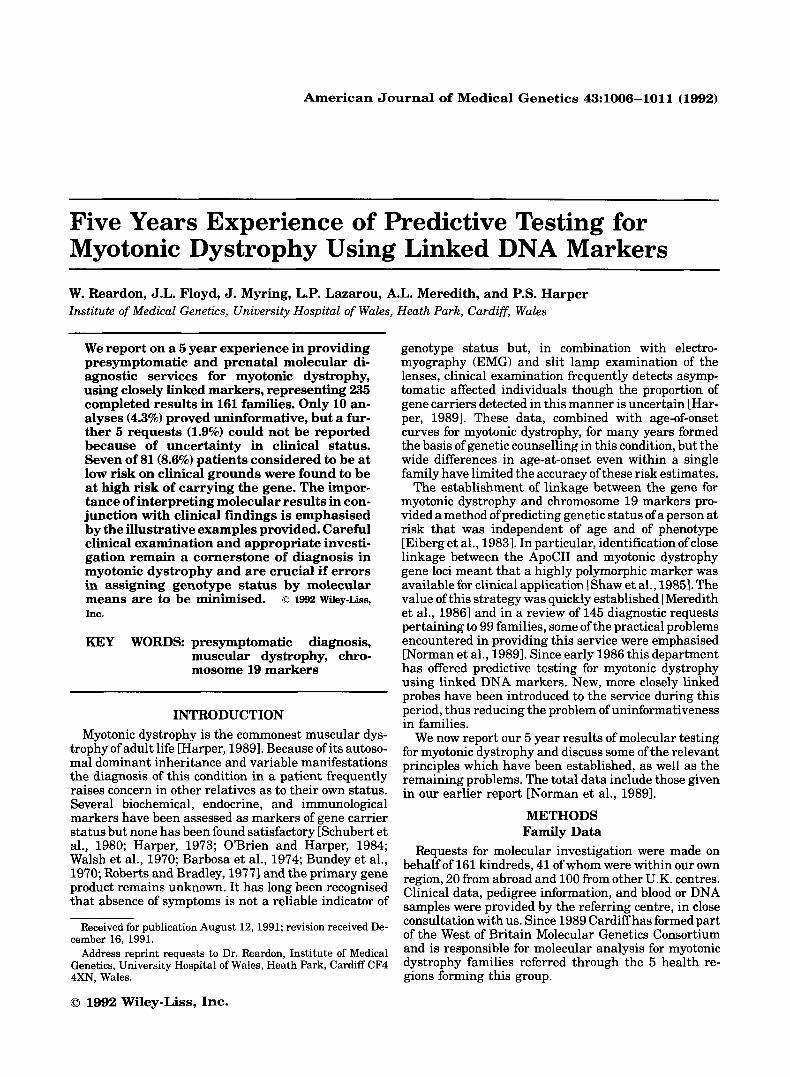
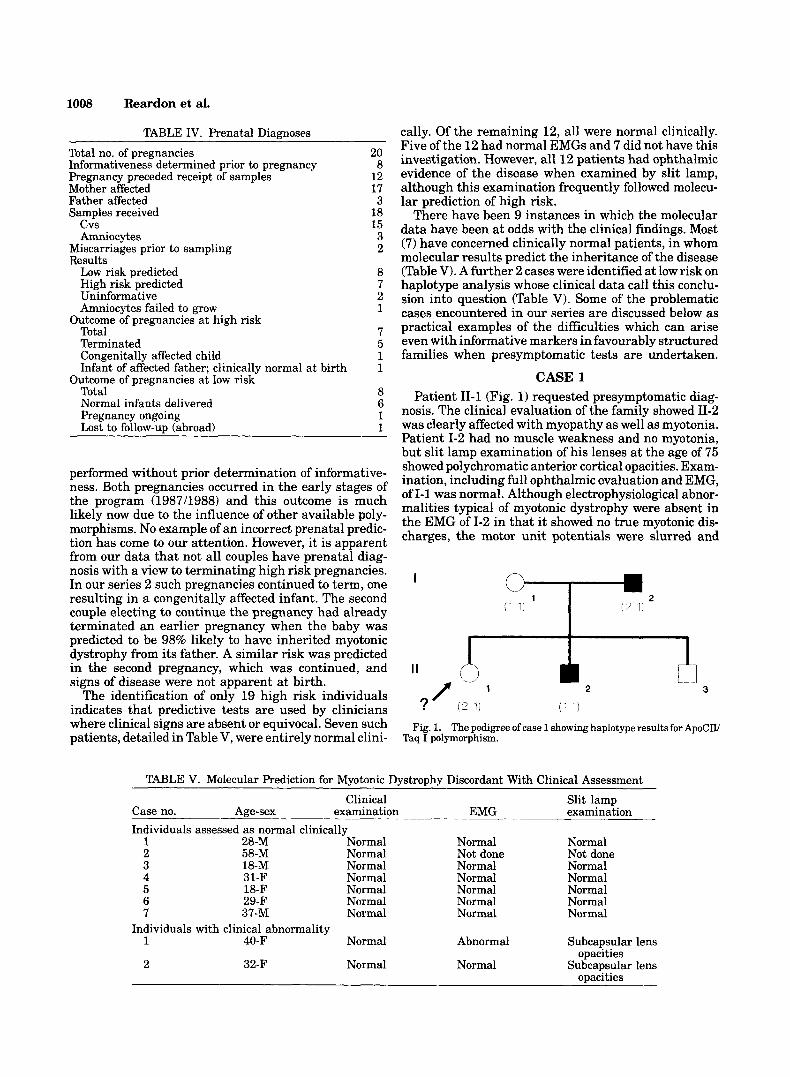
CASE 1 Patient 11-1 (Fig. 1) requested presymptomatic diag-
nosis. The clinical evaluation of the family showed 11-2 was clearly affected with myopathy as well as myotonia. Patient 1-2 had no muscle weakness and no myotonia, but slit lamp examination of his lenses at the age of 75 showed polychromatic anterior cortical opacities. Exam- ination, including full ophthalmic evaluation and EMG, of 1-1 was normal. Although electrophysiological abnor- malities typical of myotonic dystrophy were absent in the EMG of 1-2 in that it showed no true myotonic dis- charges, the motor unit potentials were slurred and
I
?' (2 1)
m 2
Fig. 1. The pedigree of case 1 showing haplotype results for ApoCIV Taq I polymorphism.
TABLE V. Molecular Prediction for Myotonic Dystrophy Discordant With Clinical Assessment
Clinical Slit lamp Case no. Age-sex examination EMG examination Individuals assessed as normal clinically
1 28-M Normal 2 58-M Normal 3 18-M Normal 4 31-F Normal 5 18-F Normal 6 29-F Normal 7 37-M Normal
1 40-F Normal
2 32-F Normal
Individuals with clinical abnormality
Normal Not done Normal Normal Normal Normal Normal
Abnormal
Normal
Normal Not done Normal Normal Normal Normal Normal
Subcapsular lens
Subcapsular lens opacities
Predictive Testing for Myotonic Dystrophy 1009
abnormal. This, combined with the abnormality of the lenses, was used to establish him as the gene carrier in generation I.
DNA analysis showed that 11-1 had inherited the op- posite paternal allele from her affected brother 11-2 and so appeared, with the ApoCII polymorphism, to be at low risk (Fig. 1). Clinical evaluation was performed in paral- lel with the molecular analysis and she was found to have bilateral posterior subcapsular lens opacities and an abnormal EMG. In light of these findings it was thought that a recombination had taken place between ApoCII and the myotonic dystrophy gene and her risk was revised accordingly. Subsequent reanalysis of the pedigree using the closely linked probe, D10, continues to show the recombination.
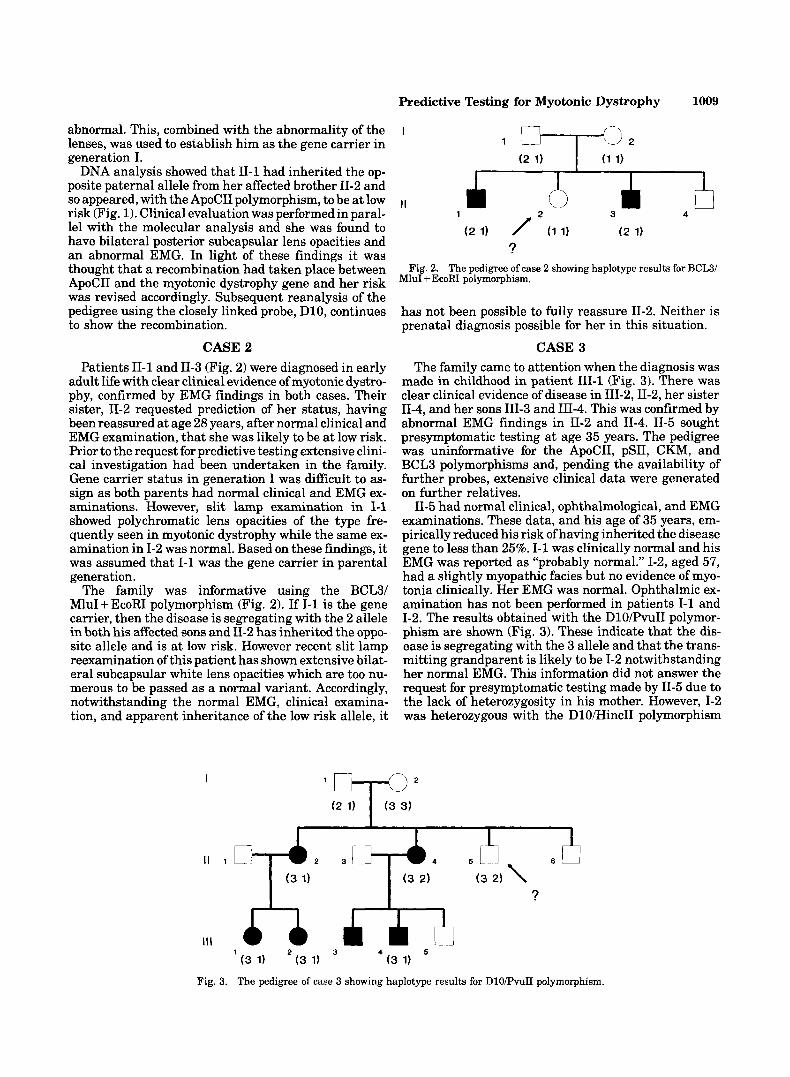
CASE 2 Patients 11-1 and 11-3 (Fig. 2) were diagnosed in early
adult life with clear clinical evidence of myotonic dystro- phy, confirmed by EMG findings in both cases. Their sister, 11-2 requested prediction of her status, having been reassured at age 28 years, after normal clinical and EMG examination, that she was likely to be at low risk. Prior to the request for predictive testing extensive clini- cal investigation had been undertaken in the family. Gene carrier status in generation I was difficult to as- sign as both parents had normal clinical and EMG ex- aminations. However, slit lamp examination in 1-1 showed polychromatic lens opacities of the type fre- quently seen in myotonic dystrophy while the same ex- amination in 1-2 was normal. Based on these findings, it was assumed that 1-1 was the gene carrier in parental generation.
The family was informative using the BCL3/ MluI + EcoRI polymorphism (Fig. 2). If 1-1 is the gene carrier, then the disease is segregating with the 2 allele in both his affected sons and 11-2 has inherited the oppo- site allele and is at low risk. However recent slit lamp reexamination of this patient has shown extensive bilat- eral subcapsular white lens opacities which are too nu- merous to be passed as a normal variant. Accordingly, notwithstanding the normal EMG, clinical examina- tion, and apparent inheritance of the low risk allele, it
I
I1 1
Ill
Fig. 3.
--
I
I
3 4 I 1
1
Fig. 2. The pedigree of case 2 showing haplotype results for BCL3/ MluI + EcoRI polymorphism.
has not been possible to fully reassure 11-2. Neither is prenatal diagnosis possible for her in this situation.
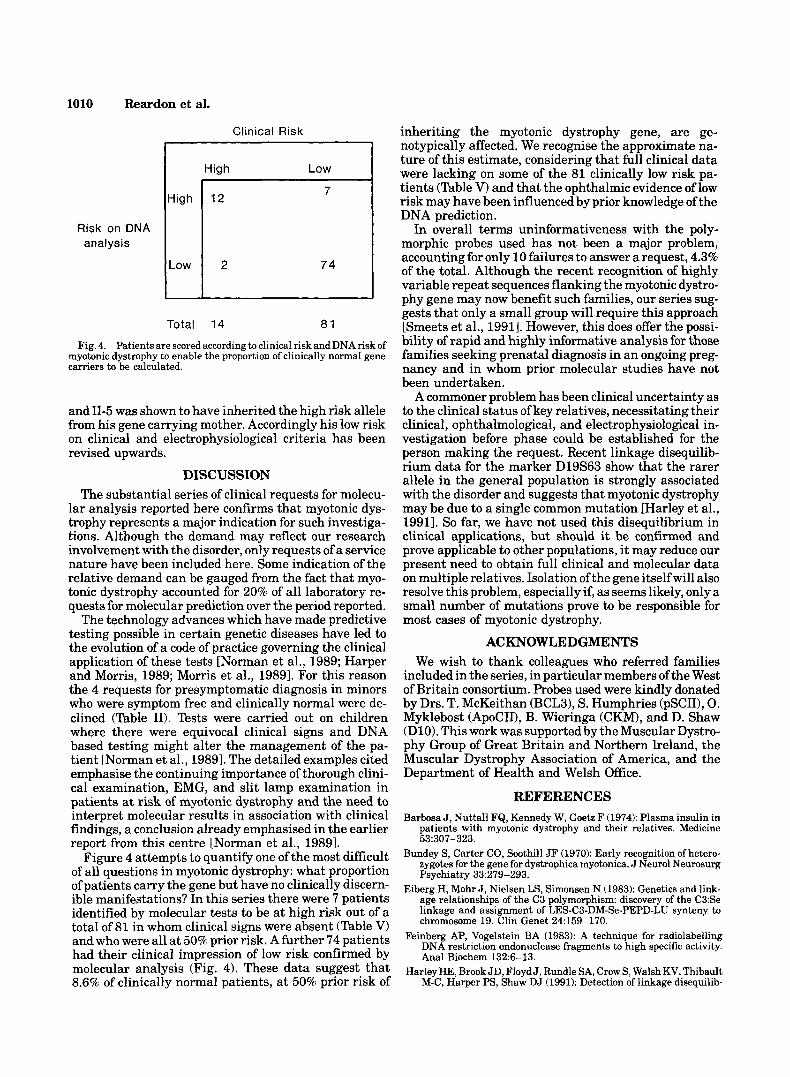
CASE 3 The family came to attention when the diagnosis was
made in childhood in patient 111-1 (Fig. 3). There was clear clinical evidence of disease in III-2,11-2, her sister 11-4, and her sons 111-3 and 111-4. This was confirmed by abnormal EMG findings in 11-2 and 11-4. 11-5 sought presymptomatic testing at age 35 years. The pedigree was uninformative for the ApoCII, pSII, CKM, and BCL3 polymorphisms and, pending the availability of further probes, extensive clinical data were generated on further relatives.
11-5 had normal clinical, ophthalmological, and EMG examinations. These data, and his age of 35 years, em- pirically reduced his risk of having inherited the disease gene to less than 25%. 1-1 was clinically normal and his EMG was reported as “probably normal.” 1-2, aged 57, had a slightly myopathic facies but no evidence of myo- tonia clinically. Her EMG was normal. Ophthalmic ex- amination has not been performed in patients 1-1 and 1-2. The results obtained with the DlO/PvuII polymor- phism are shown (Fig. 3). These indicate that the dis- ease is segregating with the 3 allele and that the trans- mitting grandparent is likely to be 1-2 notwithstanding her normal EMG. This information did not answer the request for presymptomatic testing made by 11-5 due to the lack of heterozygosity in his mother. However, 1-2 was heterozygous with the DlO/HincII polymorphism
I
I I 2 3 4
I ?
The pedigree of case 3 showing haplotype results for DlO/PvuII polymorphism.
1010 Reardon et al.
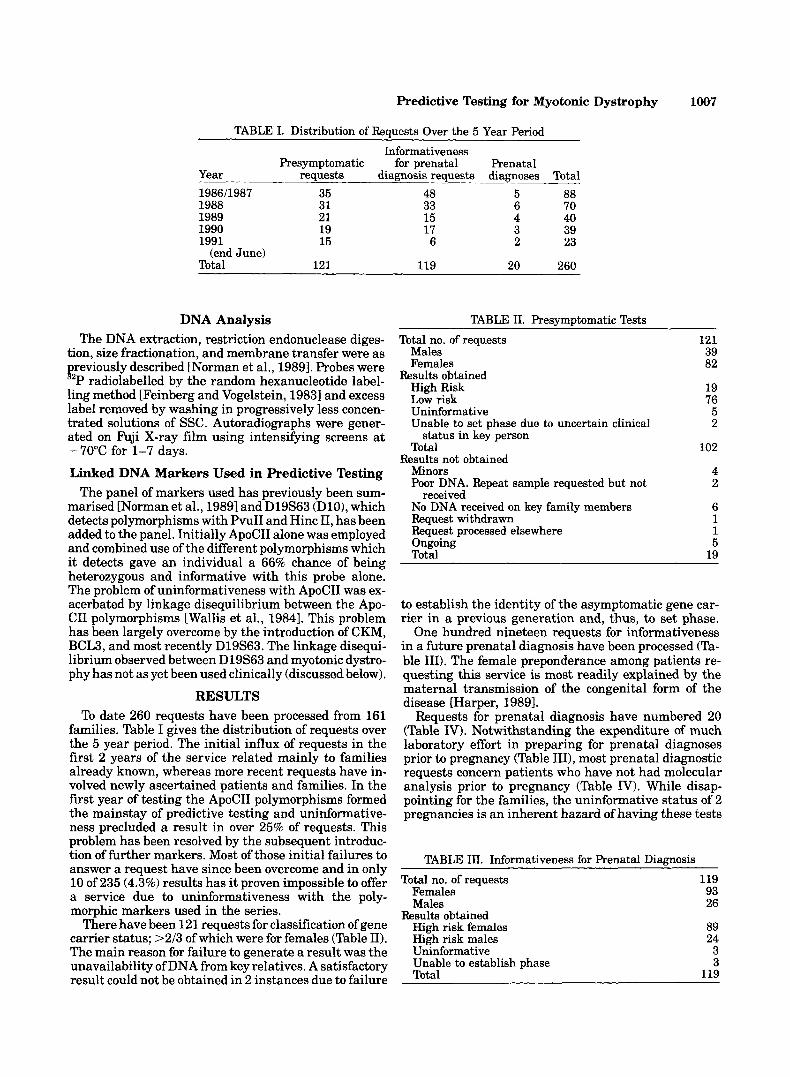
Risk on DNA analysis
Clinical Risk
High Low I
Total 14 81
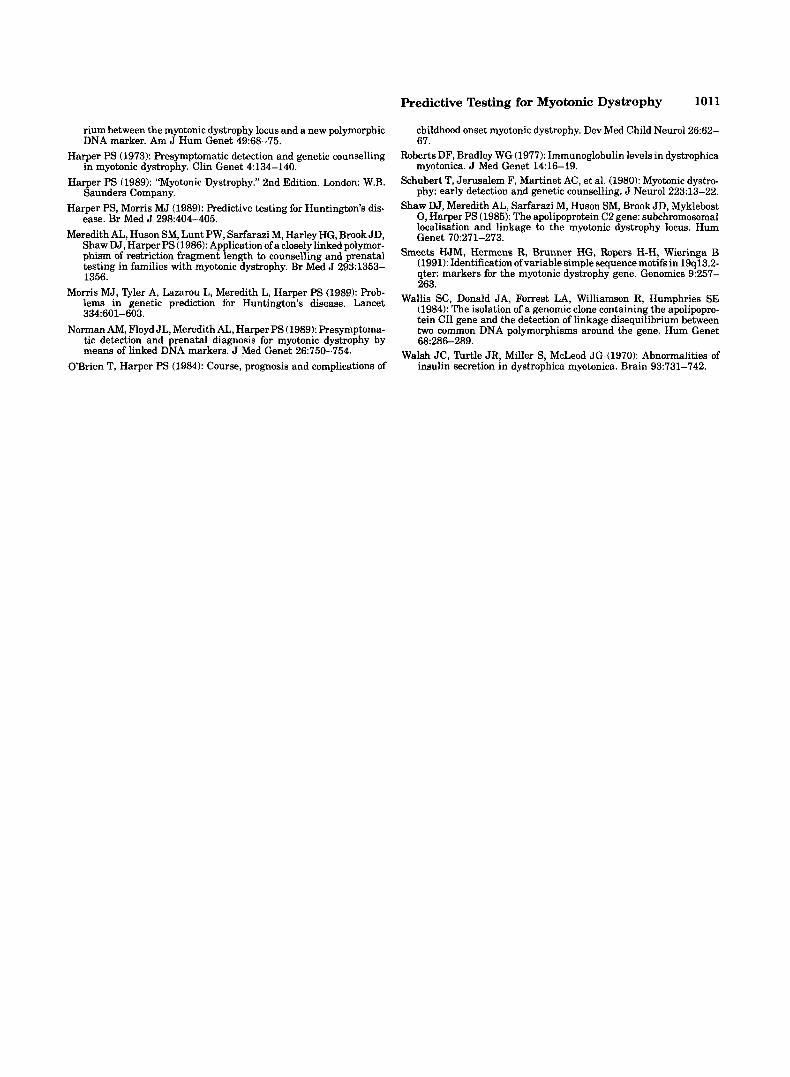
Fig. 4. Patients are scored according to clinical risk and DNA risk of myotonic dystrophy to enable the proportion of clinically normal gene carriers to be calculated.
and 11-5 was shown to have inherited the high risk allele from his gene carrying mother. Accordingly his low risk on clinical and electrophysiological criteria has been revised upwards.
DISCUSSION The substantial series of clinical requests for molecu-
lar analysis reported here confirms that myotonic dys- trophy represents a major indication for such investiga- tions. Although the demand may reflect our research involvement with the disorder, only requests of a service nature have been included here. Some indication of the relative demand can be gauged from the fact that myo- tonic dystrophy accounted for 20% of all laboratory re- quests for molecular prediction over the period reported.
The technology advances which have made predictive testing possible in certain genetic diseases have led to the evolution of a code of practice governing the clinical application of these tests [Norman et al., 1989; Harper and Morris, 1989; Morris et al., 19891. For this reason the 4 requests for presymptomatic diagnosis in minors who were symptom free and clinically normal were de- clined (Table 11). Tests were carried out on children where there were equivocal clinical signs and DNA based testing might alter the management of the pa- tient [Norman et al., 19891. The detailed examples cited emphasise the continuing importance of thorough clini- cal examination, EMG, and slit lamp examination in patients a t risk of myotonic dystrophy and the need to interpret molecular results in association with clinical findings, a conclusion already emphasised in the earlier report from this centre [Norman et al., 19891.
Figure 4 attempts to quantify one of the most difficult of all questions in myotonic dystrophy: what proportion of patients carry the gene but have no clinically discern- ible manifestations? In this series there were 7 patients identified by molecular tests to be at high risk out of a total of 81 in whom clinical signs were absent (Table V) and who were all a t 50% prior risk. A further 74 patients had their clinical impression of low risk confirmed by molecular analysis (Fig. 4). These data suggest that
inheriting the myotonic dystrophy gene, are ge- notypically affected. We recognise the approximate na- ture of this estimate, considering that full clinical data were lacking on some of the 81 clinically low risk pa- tients (Table V) and that the ophthalmic evidence of low risk may have been influenced by prior knowledge of the DNA prediction.
In overall terms uninformativeness with the poly- morphic probes used has not been a major problem, accounting for only 10 failures to answer a request, 4.3% of the total. Although the recent recognition of highly variable repeat sequences flanking the myotonic dystro- phy gene may now benefit such families, our series sug- gests that only a small group will require this approach [Smeets et al., 19911. However, this does offer the possi- bility of rapid and highly informative analysis for those families seeking prenatal diagnosis in an ongoing preg- nancy and in whom prior molecular studies have not been undertaken.
A commoner problem has been clinical uncertainty as to the clinical status of key relatives, necessitating their clinical, ophthalmological, and electrophysiological in- vestigation before phase could be established for the person making the request. Recent linkage disequilib- rium data for the marker D19S63 show that the rarer allele in the general population is strongly associated with the disorder and suggests that myotonic dystrophy may be due to a single common mutation [Harley et al., 19911. So far, we have not used this disequilibrium in clinical applications, but should it be confirmed and prove applicable to other populations, it may reduce our present need to obtain full clinical and molecular data on multiple relatives. Isolation of the gene itself will also resolve this problem, especially if, as seems likely, only a small number of mutations prove to be responsible for most cases of myotonic dystrophy.
ACKNOWLEDGMENTS We wish to thank colleagues who referred families
included in the series, in particular members of the West of Britain consortium. Probes used were kindly donated by Drs. T. McKeithan (BCL31, S. Humphries (pSCII), 0. Myklebost (ApoCII), B. Wieringa (CKM), and D. Shaw (D10). This work was supported by the Muscular Dystro- phy Group of Great Britain and Northern Ireland, the Muscular Dystrophy Association of America, and the Department of Health and Welsh Office.
REFERENCES Barbosa J, Nuttall FQ, Kennedy W, Goetz F (1974): Plasma insulin in
patients with myotonic dystrophy and their relatives. Medicine 53:307-323.
Bundey S, Carter CO, Soothill JF (1970): Early recognition of hetero- zygotes for the gene for dystrophica myotonica. J Neurol Neurosurg Psychiatry 33:279-293.
Eiberg H, Mohr J , Nielsen LS, Simonsen N (1983): Genetics and link- age relationships of the C3 polymorphism: discovery of the C3:Se linkage and assignment of LESJ23-DM-Se-PEPD-LU synteny to chromosome 19. Clin Genet 24:159-170.
Feinberg AP, Vogelstein BA (1983): A technique for radiolabelling DNA restriction endonuclease fragments to high specific activity. Anal Biochem 132:6-13.
Harley HE, Brook JD, Floyd J , Rundle SA, Crow S, Walsh KV, Thibault M-C, Harper PS, Shaw DJ (1991): Detection of linkage disequilib- 8.6% of clinicaliy normal patients, at 50% prior risk Of
rium between the myotonic dystrophy locus and a new polymorphic DNA marker. Am J Hum Genet 49:68-75.
Harper PS (1973): Presymptomatic detection and genetic counselling in myotonic dystrophy. Clin Genet 4:134-140.
Harper PS (1989): “Myotonic Dystrophy.” 2nd Edition. London: W.B. Saunders Company.
Harper PS, Morris MJ (1989): Predictive testing for Huntington’s dis- ease. Br Med J 298:404-405.
Meredith AL, Huson SM, Lunt PW, Sarfarazi M, Harley HG, Brook JD, Shaw DJ, Harper PS (1986): Application of a closely linked polymor- phism of restriction fragment length to counselling and prenatal testing in families with myotonic dystrophy. Br Med J 2931353- 1356.
Morris MJ, 51er A, Lazarou L, Meredith L, Harper PS (1989): Prob- lems in genetic prediction for Huntington’s disease. Lancet 334:601-603.
Norman AM, Floyd JL, Meredith AL, Harper PS (1989): Presymptoma- tic detection and prenatal diagnosis for myotonic dystrophy by means of linked DNA markers. J Med Genet 26:750-754.
O’Brien T, Harper PS (1984): Course, prognosis and complications of
Predictive Testing for Myotonic Dystrophy 1011
childhood onset myotonic dystrophy. Dev Med Child Neurol26:62- 67.
Roberts DF, Bradley WG (1977): Immunoglobulin levels in dystrophica myotonica. J Med Genet 14:16-19.
Schubert T, Jerusalem F, Martinet AC, et al. (1980): Myotonic dystro- phy: early detection and genetic counselling. J Neurol 223:13-22.
Shaw DJ, Meredith AL, Sarfarazi M, Huson SM, Brook JD, Myklebost 0, Harper PS (1985): The apolipoprotein C2 gene: subchromosomal localisation and linkage to the myotonic dystrophy locus. Hum Genet 70:271-273.
Smeets HJM, Hermens R, Brunner HG, Ropers H-H, Wieringa B (1991): Identification ofvariable simple sequence motifs in 19q13.2- qter: markers for the myotonic dystrophy gene. Genomics 9:257- 263.
Wallis SC, Donald JA, Forrest LA, Williamson R, Humphries SE (1984): The isolation of a genomic clone containing the apolipopro- tein CII gene and the detection of linkage disequilibrium between two common DNA polymorphisms around the gene. Hum Genet
Walsh JC, Turtle JR, Miller S, McLeod JG (1970): Abnormalities of insulin secretion in dystrophica myotonica. Brain 93:731-742.
68:286-289.