Embed Size (px)
Citation preview

GLAUCOMA
Five-year forecasts of the Visual Field Index (VFI) with binocularand monocular visual fields
Ryo Asaoka & Richard A. Russell & Rizwan Malik &
David F. Garway-Heath & David P. Crabb
Received: 11 July 2012 /Revised: 25 September 2012 /Accepted: 13 November 2012 /Published online: 7 December 2012# Springer-Verlag Berlin Heidelberg 2012
AbstractBackground In clinical care, visual field (VF) damage isassessed using monocular VF testing, yet patients perceivethe world binocularly. This study was conducted to compare5-year forecasts for the Visual Field Index (VFI) generatedfrom series of binocular and monocular VFs.Methods Series of ten consecutive VFs (Humphrey 24–2Full-threshold) spanning on average 3.7 (SD: ±0.8) yearsfrom 60 eyes of 30 glaucomatous patients were retrospec-tively examined. The VFs of both eyes were merged toproduce the integrated VF and its VFI score (BinocularVFI) was estimated. Forecasts of binocular and monocularVFIs were calculated for each patient by projecting the fittedlinear regression 5 years ahead from the last VF following
the method on the Humphrey Guided Progression Analysis(GPA) print-out. The precisions of the forecasts were calcu-lated as the width of the 95 % prediction limit (PL).Results The mean 5 year forecast for binocular VFIs was92 % (SD: 11 %), which was significantly higher thanforecasts from right and left eyes (79 % [SD: 19 %] and82 % [SD: 16 %] respectively; P<0.05). The width of the95 % PL for 5-year predictions with monocular VFIs (meanright eye: 29 % [SD: 19 %] and mean left eye: 27 % [SD:16 %]) were significantly larger than that of the binocularVFI (mean: 12 % [SD: 7 %]; P<0.05).Conclusions Five year forecasted VFI values using binocu-lar measures return significantly better values, and can bemade with greater confidence than those based on monocu-lar measures. In turn, forecasts of a patient’s binocular VFImight be more relevant to estimating the patient’s futurefunctional VF.
Keywords Perimetry . Glaucoma . Visual Field Index .
Progression
Introduction
Visual field (VF) damage impairs the Quality of Visual Life(QoV) of patients with glaucoma [1–8], and this has recentlybeen reviewed [9, 10]. In clinical care, VF damage isassessed using monocular VF testing, yet patients perceivethe world binocularly. Binocular measures of the VF, suchas the binocular Esterman test, currently used to assess theVF component of legal fitness to drive in the UK [3, 11–17],are better-suited to estimate a patient’s QoV [11, 18]. How-ever, in a busy glaucoma clinic, VF resources are generallydevoted to monocular measurements, and binocular VF testsare rarely performed. Previously, a method of estimating apatient’s binocular field of view from their monocular meas-urements has been proposed [19–21]. In this approach,
Some of the authors (R Malik, DF Garway-Heath) receive fundingfrom the National Institute for Health Research (UK) BiomedicalResearch Centre at Moorfields Eye Hospital and the UCL Institute ofOphthalmology. Professor Garway-Heath’s chair at UCL is supportedby funding from the International Glaucoma Association. The viewsexpressed in this publication are those of the authors and notnecessarily those of the Department of Health.
R. Asaoka :R. A. Russell :D. P. Crabb (*)Department of Optometry and Visual Science,City University London, Northampton Square,London EC1V 0HB, UKe-mail: [email protected]
R. Asaokae-mail: [email protected]
R. A. Russelle-mail: [email protected]
R. Asaoka :R. A. Russell :R. Malik :D. F. Garway-HeathNIHR Biomedical Research Centre at Moorfields Eye HospitalNHS Foundation Trust and UCL Institute of Ophthalmology,London, UK
R. Malike-mail: [email protected]
D. F. Garway-Heathe-mail: [email protected]
Graefes Arch Clin Exp Ophthalmol (2013) 251:1335–1341DOI 10.1007/s00417-012-2214-2

individual sensitivity values from left and right eye VFs aremerged to generate a central binocular visual field, termedthe integrated visual field (IVF). Removing the need forextra testing beyond monocular examinations is an advan-tage of this approach. Furthermore, it has been reported thatthe IVF provides a better estimate of some aspects of apatient’s QoV than the Esterman test [20, 22].
Information relating to the amount of VF loss can besummarized by global indices such as mean deviation(MD). Recently, there has been a renewed interest in summa-ry measures of the VF, with the development of the VisualField Index (VFI) [23]. The VFI is expressed as percentagefrom 100 % (normal VF) to 0 % (perimetrically blind). The
VFI disregards reductions in sensitivity unless they are asso-ciated with pattern deviation probability outside normal limits(if the pattern values are within the 95th percentile of healthyobservers, the location is treated as normal and is given avalue of 100 %), and as a result, the VFI is potentially lessinfluenced by cataract. In addition, numerical values fromlocations in the centre of the VF, assumed to be more func-tionally important, are more heavily weighted, and thereforemake a greater contribution to the VFI than those in theperiphery. The rate, or speed, of progression of VFI from aseries of VFs (% loss per year) is displayed on the HumphreyGuided Progression Analysis™ (GPA) software, now avail-able on Humphrey Visual Field Analyser (HFA, Humphrey
Fig. 1 A sample of theHumphrey Guided ProgressionAnalysis™ (GPA) summary re-port. VFI (%) is shown as a ploton time. The rate, or speed, ofprogression of VFI from a se-ries of VFs and its 95 % pre-diction limit (PL) is displayed,as well as magnitude in 5 yearstime
1336 Graefes Arch Clin Exp Ophthalmol (2013) 251:1335–1341

Field Analyzer Zeiss–Humphrey Systems, Dublin, CA,USA). In the GPA output, the index is plotted against thepatient’s age to make future forecasts of VFI to furtherencourage clinical interpretation of the rate, or speed, of VFloss in the patient’s lifetime.
It is assumed that a patient’s VF in their better eye (theeye with the least VF damage) is more reflective of theirfunctional VF. However, it has been demonstrated previous-ly that monocular measures, such as better-eye MD, cangive the impression that a patient’s VF loss is more degradedthan it might be under binocular viewing [24]. These differ-ences are more pronounced in patients with advanced VFdefects, and where there is asymmetry in the defects be-tween eyes. The aim of this report is to investigate the VFIin series of VFs as presented in the GPA, to see if binocularmeasures, derived from the IVF, confer advantages overconsidering monocular measures in isolation, as monocularVFs are the current diagnostic standard used in practice.
Material and methods
This retrospective study included 60 eyes from 30 patientswith a definitive diagnosis of primary open-angle glaucomaor normal tension glaucoma from the general glaucomaclinic at Moorfields Eye Hospital, London between June1994 and January 2002. All patients had a minimum often VF tests over a follow-up period of at least 2 years.
Criteria for inclusion were visual acuity better than 6/12,refraction less than 5 dioptre ametropia, no previous ocularsurgery (except for cataract extraction and intraocular lensimplantation), open anterior chamber angle, and no otherposterior segment eye disease. All VFs were recorded usingthe 24–2 test pattern and the full-threshold strategy with aGoldmann size III target. Reliability criteria applied werefixation losses less than 25 % and false-positive responsesless than 15 % [25]. All patients had a glaucomatous VFdefect in at least one eye, defined as three or more contiguouspoints at p<0.05, or two or more contiguous points at p<0.01in the total deviation plot, or a 10 dB difference across thenasal horizontal midline at two or more adjacent points, or aMD worse than −5 dB [26]. Cases who experienced intraoc-ular surgical treatments during the observed period were ex-cluded from the analysis. This study conformed to the tenetsof the Declaration of Helsinki. The study was approved by
research governance committees of the participating institu-tions, and all data were transferred to a secure computerdatabase at the University.
Details for formulating the “better sensitivity” IVF aredescribed in previous reports [19, 21, 24]. In short, eachlocation in a monocular VF has a corresponding point in theVF of the fellow eye in binocular viewing. The maximumtotal deviation (most sensitive) value was used from each ofthe two overlapping locations in order to give an estimate ofthe binocular sensitivity at each point.
VFI scores were obtained following the method reportedby Bengtsson & Heijl (2008) [23]. First, test points havingthreshold sensitivities within normal limits in the patterndeviation map (if MD≥−20 dB) or the total deviation map(if MD<−20 dB) were considered normal and scored100 %. Otherwise, the percentage of normal sensitivity ateach point was calculated using our normative database andthe formula: 100 − [(|total deviation| ⁄ age-corrected normalthreshold) × 100]. Next, a weighting system (from 3.29 to0.57, according to eccentricity) was applied such that centrallocations are weighted more than peripheral locations; thisweighting is based on published estimates of the spatialmagnification present in the occipital cortex [23, 27]. Final-ly, the weighted mean VFI score of all points was calculated.Note that test points at coordinates (x, y degrees): (27, 3),(−27, 3), (27, −3), (−27, −3) were not included in thecalculation of the IVF VFI (referred to here as the binocular
Table 1 Characteristics of thestudy participants
MD: mean deviation values atthe first visit
Age (mean±standard deviation, range) (years old) 64 ± 8 (43 to 76)
Male: female 8: 22
Observation period (mean±standard deviation, range) (years) 3.7 ± 0.8 (2.5 to 6.2)
MD of right eye (mean±standard deviation, range) (dB) −3.6 ± 4.2 (−12.2 to 2.0)
MD of left eye (mean±standard deviation, range) (dB) −4.1 ± 5.6 (−24.7 to 1.0)
Calculated VFI (%)
Prin
ted
VF
I (%
)
Fig. 2 An agreement plot (with line of unity) of the calculatedmonocular VFI scores and the VFI recorded on the GPA (each pointwas jittered). The mean (± SD) of the differences between the calcu-lated VFI and VFI on the GPA printout was 1.0±1.9 %
Graefes Arch Clin Exp Ophthalmol (2013) 251:1335–1341 1337

VFI), and so the mean was adjusted accordingly. The sen-sitivity at locations (15, 3) and (15, −3) were automaticallytaken from left eyes and conversely, those at (−15, 3) and(−15, −3) were taken from right eyes, because these pointscorrespond to the location of the blind spot of right and lefteyes respectively. This method closely followed a report byArtes et al. [28]. Our estimates of the monocular VFI (usedin subsequent analyses) were compared with the VFIrecorded on the GPA in order to analyse the agreementbetween the two. Then the binocular VFI score was com-pared to the VFIs of right and left eyes.
Analysis closely following the Humphrey Guided Pro-gression Analysis™ (GPA) summary report, as illustrated inFig. 1, was then carried out. Linear regression of VFI ontime for the whole series was used to estimate the speed ofloss in each eye and the IVF. Forecasts were then generated5 years after the date of the tenth examination, by extrapo-lating the regression lines for each of the binocular andmonocular VFI scores. The forecasts and the width of the95 % PL for this prediction in each patient were comparedamong the three VFI scores. The width of this 95 % PL wascalculated for each patient. This represents an estimate ofthe precision of the forecast, with narrower limits suggestingbetter forecasts. The average values of the prediction valueand the average width of the 95 % PL were comparedamong the binocular and monocular VFIs. All statisticalanalyses were carried out using the statistical programminglanguage R (ver. 2.11.1, the R Foundation for StatisticalComputing, Vienna, Austria); 95 % PLs were calculatedusing the ‘predict.lm’ function in the R package ‘stats’,which assumes that future observations have the same errorvariance as those used for fitting the regression line.
Results
Characteristics of the study sample are summarized inTable 1.
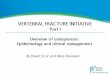
The comparison between estimates (calculated) of mon-ocular VFI scores and those actually recorded on the GPA(printed) is shown in Fig. 2. The mean (± SD) of the differ-ences between the calculated VFI and VFI on the GPAprintout for all of the 600 VFs was 1.0±1.9 %. The pro-gression of monocular VFIs and the binocular VFI is illus-trated for a single patient in Fig. 3a, b and c. In this patient,VFI forecasts 5 years after the final visit were 16 % and59 % for the right and left eyes respectively, and 67 % forthe binocular VFI. The width of the 95 % PL was muchnarrower with the binocular VFI (PL: 61 to 71 %) than withthe monocular VFIs (PL: −5 to 37 % for the right eye and 39to 79 % for the left eye).
Summary measures of the VFIs at baseline and last visit,forecasted VFI, and the 95 % PL of the predicted VFI are
VF
I of r
ight
eye
(%
)
Years
Years
VF
I of l
eft e
ye (
%)
Years
Bin
ocul
ar V
FI (
%)
a
b
c
Fig. 3 Comparison of the trends of the binocular VFI and the monocularVFI, with grayscale images of each VF, in an sample patient. a and bShow the trends of the VFI scores of the monocular VFIs of right and lefteyes (R200.71, p<0.05 and R200.27, p00.13 respectively). c Shows thetrend of the VFI score of the binocular VFI (R200.83, p<0.05). Thepredicted VFI scores 5 years after the final visit were 16.1 % (PL: −4.8 to37.2 %) for monocular VFI of right eye and 58.9 % (PL: 38.7 to 79.1 %)for monocular VFI of left eye. The predicted VFI score for the binocularVFI was 66.8 % (PL: 60.8 to 70.9 %). VFI: Visual Field Index, binocularVFI: VFI of the integrated visual field (better sensitivity method), PL:95 % prediction limit
1338 Graefes Arch Clin Exp Ophthalmol (2013) 251:1335–1341

shown in Table 2. Average binocular VFIs were significant-ly greater than those of right and left eyes at both baselineand last visit (p<0.001, Friedman test). The average pre-dicted VFI (5 year forecast) was significantly better with thebinocular VFI than with monocular VFIs (p<0.001, Fried-man test). There was an average two-fold reduction in thewidth of the prediction limit for the binocular VFI whencompared to the monocular VFIs (p<0.001, Friedman test).
Discussion
In a clinical setting, VF measurements are generally carriedout on each eye separately and the binocular VF is rarelymeasured; however, in real life it is mainly binocular visualfunction that matters to the patient. Thus, it is sensible topresume that the impact of VF impairment on a patient’sQoV is better measured using a binocular measure [18].Indeed, previous studies support this view [3, 11–14, 16,17]. In the current study, VFI scores were calculated for 30patients with glaucoma, and VFI progression was forecastedbinocularly and monocularly, using linear regression. Aver-age 5-year forecasts of the VFI were significantly largerwith a binocular measure, suggesting a better visual prog-nosis than might be implied by considering monocularmeasures alone. Moreover, the precision of these VFI fore-casts was better with the binocular measure than with themonocular measures, suggesting that the predictions can bemade with greater confidence.
In the current study, progression of VFI is assumed tooccur linearly, and thus the prediction of future progressionwas made based on this hypothesis (just as the GPA soft-ware of the HFA assumes). The validity of the linear modelhas already been reported by Bengtsson et al. (2009); theauthors used linear regression to predict the 10th or laterVFI from an initial five VFs, and showed that in 70 % ofpatients the predicted VFI was within ±10 % of the estimat-ed value [29]. In addition, a recent report evaluated thevalidity of this approach by examining the transition of VFIsof ocular hypertensive (OH) patients and patients with glau-coma (followed for 6 years), and reported a good agreement
between predicted and actual VFI scores [30]. Others haveassumed VFI progression to occur in a linear manner, but thismay be dependent on the stage of glaucoma [31]. On the otherhand, other reports have suggested no association between thespeed of progression and visual field status [32–35].
The scatterplot of the rate of progression of MD in thereport of Rao et al. (2011) suggests that the progression rateof MD is slower in the early stages of glaucoma [31]. Inaddition, it has been reported that the fluctuation of visualfield sensitivity becomes larger as glaucoma advances [36,37]; as a result, the precision of MD becomes worse inadvanced glaucoma. This suggests that the VFI will alsohave smaller precision at this stage of disease. It is widelyknown that VF measurements are particularly noisy andtest–retest variability is high in patients [38–43]. The lowreproducibility of VF results is particularly problematic forclinical interpretation of VF damage, as it interferes with theassessment of VF progression. As the IVF integrates twosets of measurements from monocular VFs, it is inherentlymore precise, which allows a more accurate interpretation ofVF damage. This is seen in Fig. 3a compared to Fig. 3b andc, and is confirmed by the average two-fold improvement inthe surrogate for precision used in this study.
The results from this study also highlight the limitationsof 5-year forecasts as shown on the GPA output. The 95 %prediction intervals on 5-year forecasts for VFI in the pereye analysis have a width of about 27–30 %, representingmore than a quarter of the entire range of the VFI score. Inshort, this questions the utility of predictions that are farfrom precise, albeit improved when using the binocularmeasure. Furthermore, these calculations were performedusing ten VFs, a frequency of testing not afforded in mostroutine follow-up. Other studies have concluded that a suf-ficient number of VFs must be done, or sufficiently longobservation time allowed, to ensure a reliable estimate ofrate of loss [44, 45]. Indeed, it has even been proposed thatestimates of speed of loss, and predictions based on thatspeed of loss, should not be made until the patient has beenmonitored for more than 5 years [46, 47].
A limitation of the current study was that the data wereanalysed retrospectively. VF progression could have been
Table 2 VFI at baseline and last visit, the predicted VFI, and the width of 95 % PL of the predicted VFI
Binocular VFI Right VFI Left VFI
Initial VFI: mean±SD (min–max) 96.1±5.7 (77.5–100.0) 85.9±12.8 * (55.4–98.0) 85.3±15.9 * (22.2–98.6)
Last VFI: mean±SD (min–max) 94.1±7.4 (70.4–100.0) 82.0±15.2 * (50.5–98.5) 84.0±15.4 * (25.8–97.4)
Predicted VFI: mean±SD (min–max) 92.0±11.3 (49.1–103.0) 79.1±19.4 * (15.3–104.2) 81.9±15.6 * (21.5–99.8)
Width of 95 % PL of predicted VFI: mean±SD (min–max) 12.4±7.2 (3.8–35.6) 29.4±19.1 * (0.1–91.5) 27.3±15.7 * (8.2–68.2)
VFI: Visual Field Index, SD: standard deviation, min: minimum, max: maximum, Binocular VFI: VFI of the integrated visual field, Right VFI: VFIof right eye, Left VFI: VFI of left eye. Initial VFI: VFI at the baseline, Last VFI: VFI at the end of the observation, Predicted VFI: forecast VFI for5 years after the last visit (*: p<0.001 against binocular better VFI, Friedman test), PL: 95 % prediction limit
Graefes Arch Clin Exp Ophthalmol (2013) 251:1335–1341 1339

influenced by the change of the treatments over the obser-vation period. Also, we have only looked at one way ofderiving IVF; others have been suggested. In a previousstudy [48], various binocular sensitivity prediction models,including averaging eyes, binocular summation, and IVFmethod, were evaluated. The result was that the IVF ap-proach provides a prediction very close to the real binocularsensitivity. Another limitation is that GPA forecast analysisis only instigated when the follow-up period is more than3 years, and forecasts are made 5 years in the future whenthe follow-up period is greater than or equal to 5 years,otherwise forecasts are made at a period in the future equalto the follow-up period. A potential bias in our study sampleis that the frequency of VF testing in this sample of patientsis high (ten in a follow-up period between 2.5 and 6.2 years).This high frequency may represent a suspicion of VF pro-gression in these patients. Therefore, the rates of progressionin the current study may be faster than the ‘real world’population. However, we do not expect this to influenceour overall conclusions, as the aim of our study was todetermine the precision of the binocular VFI relative to themonocular VFI. Finally, it is worth highlighting that theVFIs analysed in this report were computed following themethods described in the original reporting of the index[23]. These computed values were slightly different to theones that we found on the GPA print-out, probably due tousing our own normative database (as we did not haveaccess to the HFA values), but the differences were negligi-ble (Fig. 2) and are unlikely to impact on the results andconclusion of this report.
Monocular measures, like better-eye MD, can give theimpression that a patient’s VF loss is more degraded than itmight be under binocular viewing. This effect is morepronounced in patients with advanced VF defects [24]. Untilnow, no study has made a comparison between the progres-sion of the binocular VFI and that of the monocular VFI.However, such a study is important, because binocularmeasures of VF relate more closely with QoV, whereasmonocular function is used in clinical practice to gaugedisease status. The VFI was devised to reflect a patient’sfunctional vision, and the calculation applies a weightingprocedure to reflect the spatial magnification present in theoccipital cortex [23]. Therefore, the binocular VFI is prob-ably better-suited to assess a patient’s QoV, and be moremeaningful when attempting to predict future progression ina patient’s QoV. In turn, many patients may not reachdisabling visual impairment in their expected lifetime ifthe binocular VF is considered. However, it is important tonote that for the purposes of detecting VF progression, pereye analyses will be more sensitive than any analysis basedon the IVF. Furthermore, the VFI discards spatial informa-tion with regard to VF damage, so integrating monocularVFs into the IVF further exacerbates the ability to detect VF
progression. In conclusion, we have shown that binocularVFI returns higher values than monocular VFIs, with ‘bet-ter’ forecasted values compared to monocular VFIs; fore-casts on binocular VFIs are also more precise than onmonocular VFIs. The VFI represents a commendable at-tempt at making indices from perimetry more reflective ofpatient’s visual function, but it seems sensible to take thestep of providing binocular measures where possible.
References
1. Gutierrez P, Wilson MR, Johnson C, Gordon M, Cioffi GA, RitchR, Sherwood M, Meng K, Mangione CM (1997) Influence ofglaucomatous visual field loss on health-related quality of life.Arch Ophthalmol 115:777–784
2. Janz NK, Wren PA, Lichter PR, Musch DC, Gillespie BW, GuireKE (2001) Quality of life in newly diagnosed glaucoma patients:the Collaborative Initial Glaucoma Treatment Study. Ophthalmology108:887–897, discussion 898
3. Parrish RK 2nd, Gedde SJ, Scott IU, Feuer WJ, Schiffman JC,Mangione CM, Montenegro-Piniella A (1997) Visual function andquality of life among patients with glaucoma. Arch Ophthalmol115:1447–1455
4. Ringsdorf L, McGwin G Jr, Owsley C (2006) Visual field defectsand vision-specific health-related quality of life in African-Americans and whites with glaucoma. J Glaucoma 15:414–418
5. Spaeth G, Walt J, Keener J (2006) Evaluation of quality of life forpatients with glaucoma. Am J Ophthalmol 141:S3–S14
6. Varma R, Wu J, Chong K, Azen SP, Hays RD (2006) Impact ofseverity and bilaterality of visual impairment on health-relatedquality of life. Ophthalmology 113:1846–1853
7. Wang JJ, Mitchell P, Smith W (2000) Vision and low self-ratedhealth: the Blue Mountains Eye Study. Invest Ophthalmol Vis Sci41:49–54
8. Wilson MR, Coleman AL, Yu F, Bing EG, Sasaki IF, Berlin K,Winters J, Lai A (1998) Functional status and well-being inpatients with glaucoma as measured by the medical outcomesstudy short form-36 questionnaire. Ophthalmology 105:2112–2116
9. Glen FC, Crabb DP, Garway-Heath DF (2011) The direction ofresearch into visual disability and quality of life in glaucoma.BMC Ophthalmol 11:19
10. Ramulu P (2009) Glaucoma and disability: which tasks are affected,and at what stage of disease? Curr Opin Ophthalmol 20:92–98
11. Jampel HD, Friedman DS, Quigley H, Miller R (2002) Correlationof the binocular visual field with patient assessment of vision.Invest Ophthalmol Vis Sci 43:1059–1067
12. Jampel HD, Schwartz A, Pollack I, Abrams D, Weiss H, Miller R(2002) Glaucoma patients’ assessment of their visual function andquality of life. J Glaucoma 11:154–163
13. Nelson P, Aspinall P, Papasouliotis O, Worton B, O’Brien C (2003)Quality of life in glaucoma and its relationship with visual func-tion. J Glaucoma 12:139–150
14. Noe G, Ferraro J, Lamoureux E, Rait J, Keeffe JE (2003) Associ-ations between glaucomatous visual field loss and participation inactivities of daily living. Clin Exp Ophthalmol 31:482–486
15. Scott IU, Feuer WJ, Jacko JA (2002) Impact of graphical userinterface screen features on computer task accuracy and speed in acohort of patients with age-related macular degeneration. Am JOphthalmol 134:857–862
16. Turano KA, Rubin GS, Quigley HA (1999) Mobility performancein glaucoma. Invest Ophthalmol Vis Sci 40:2803–2809
1340 Graefes Arch Clin Exp Ophthalmol (2013) 251:1335–1341

17. Viswanathan AC, McNaught AI, Poinoosawmy D, Fontana L,Crabb DP, Fitzke FW, Hitchings RA (1999) Severity and stabilityof glaucoma: patient perception compared with objective measure-ment. Arch Ophthalmol 117:450–454
18. Esterman B (1982) Functional scoring of the binocular field.Ophthalmology 89:1226–1234
19. Crabb DP, Fitzke FW, Hitchings RA, Viswanathan AC (2004) Apractical approach to measuring the visual field component offitness to drive. Br J Ophthalmol 88:1191–1196
20. Crabb DP, Viswanathan AC (2005) Integrated visual fields: a newapproach to measuring the binocular field of view and visualdisability. Graefes Arch Clin Exp Ophthalmol 243:210–216
21. Crabb DP, Viswanathan AC, McNaught AI, Poinoosawmy D,Fitzke FW, Hitchings RA (1998) Simulating binocular visual fieldstatus in glaucoma. Br J Ophthalmol 82:1236–1241
22. Owen VM, Crabb DP, White ET, Viswanathan AC, Garway-HeathDF, Hitchings RA (2008) Glaucoma and fitness to drive: usingbinocular visual fields to predict a milestone to blindness. InvestOphthalmol Vis Sci 49:2449–2455
23. Bengtsson B, Heijl A (2008) A visual field index for calculation ofglaucoma rate of progression. Am J Ophthalmol 145:343–353
24. Asaoka R, Crabb DP, Yamashita T, Russell RA, Wang YX,Garway-Heath DF (2011) Patients have two eyes!: binocular versusbetter eye visual field indices. Invest Ophthalmol Vis Sci 52:7007–7011
25. Bengtsson B, Heijl A (2000) False-negative responses in glaucomaperimetry: indicators of patient performance or test reliability?Invest Ophthalmol Vis Sci 41:2201–2204
26. Caprioli J, Park HJ, Ugurlu S, Hoffman D (1998) Slope of theperipapillary nerve fiber layer surface in glaucoma. Invest Oph-thalmol Vis Sci 39:2321–2328
27. Levi DM,Klein SA, AitsebaomoAP (1985) Vernier acuity, crowdingand cortical magnification. Vis Res 25:963–977
28. Artes PH, O’Leary N, Hutchison DM, Heckler L, Sharpe GP,Nicolela MT, Chauhan BC (2011) Properties of the statpac visualfield index. Invest Ophthalmol Vis Sci 52:4030–4038
29. Bengtsson B, Patella VM, Heijl A (2009) Prediction of glaucomatousvisual field loss by extrapolation of linear trends. Arch Ophthalmol127:1610–1615
30. Giraud JM, Fenolland JR, May F, Hammam O, Sadat AM, Bou-mezrag AB, Renard JP (2010) Analysis of a new visual field index,the VFI, in ocular hypertension and glaucoma. J Fr Ophtalmol33:2–9
31. Rao HL, Kumar AU, Babu JG, Senthil S, Garudadri CS (2011)Relationship between severity of visual field loss at presentationand rate of visual field progression in glaucoma. Ophthalmology118:249–253
32. Kwon YH, Kim CS, Zimmerman MB, Alward WL, Hayreh SS(2001) Rate of visual field loss and long-term visual outcome inprimary open-angle glaucoma. Am J Ophthalmol 132:47–56
33. Rasker MT, van den Enden A, Bakker D, Hoyng PF (2000) Rate ofvisual field loss in progressive glaucoma. Arch Ophthalmol118:481–488
34. Stewart WC, Kolker AE, Sharpe ED, Day DG, Holmes KT, LeechJN, Johnson M, Cantrell JB (2000) Factors associated with long-term progression or stability in primary open-angle glaucoma. AmJ Ophthalmol 130:274–279
35. Drance S, Anderson DR, Schulzer M (2001) Risk factors forprogression of visual field abnormalities in normal-tension glau-coma. Am J Ophthalmol 131:699–708
36. Fogagnolo P, Sangermani C, Oddone F, Frezzotti P, Iester M, FigusM, Ferreras A, Romano S, Gandolfi S, Centofanti M, Rossetti L,Orzalesi N (2011) Long-term perimetric fluctuation in patientswith different stages of glaucoma. Br J Ophthalmol 95:189–193
37. Tattersall CL, Vernon SA, Menon GJ (2007) Mean deviationfluctuation in eyes with stable Humphrey 24–2 visual fields. Eye(Lond) 21:362–366
38. Artes PH, Iwase A, Ohno Y, Kitazawa Y, Chauhan BC (2002)Properties of perimetric threshold estimates from full threshold,SITA standard, and SITA fast strategies. Invest Ophthalmol Vis Sci43:2654–2659
39. Wall M, Woodward KR, Doyle CK, Artes PH (2009) Repeatabilityof automated perimetry: a comparison between standard automatedperimetry with stimulus size III and V, matrix, and motion peri-metry. Invest Ophthalmol Vis Sci 50:974–979
40. Heijl A, Lindgren A, Lindgren G (1989) Test-retest variability inglaucomatous visual fields. Am J Ophthalmol 108:130–135
41. Blumenthal EZ, Sample PA, Zangwill L, Lee AC, Kono Y, WeinrebRN (2000) Comparison of long-term variability for standard andshort-wavelength automated perimetry in stable glaucoma patients.Am J Ophthalmol 129:309–313
42. Kwon YH, Park HJ, Jap A, Ugurlu S, Caprioli J (1998) Test-retestvariability of blue-on-yellow perimetry is greater than white-on-white perimetry in normal subjects. Am J Ophthalmol 126:29–36
43. Piltz JR, Starita RJ (1990) Test-retest variability in glaucomatousvisual fields. Am J Ophthalmol 109:109–111
44. Chauhan BC, Garway-Heath DF, Goni FJ, Rossetti L, BengtssonB, Viswanathan AC, Heijl A (2008) Practical recommendations formeasuring rates of visual field change in glaucoma. Br J Ophthalmol92:569–573
45. Crabb DP, Garway-Heath DF (2012) Intervals between visual fieldtests when monitoring the glaucomatous patient: wait-and-Seeapproach. Invest Ophthalmol Vis Sci 53:2770–2776
46. Jansonius NM (2010) On the accuracy of measuring rates of visualfield change in glaucoma. Br J Ophthalmol 94:1404–1405
47. Wesselink C, Stoutenbeek R, Jansonius NM (2011) Incorporatinglife expectancy in glaucoma care. Eye (Lond) 25:1575–1580
48. Nelson-Quigg JM, Cello K, Johnson CA (2000) Predicting binocularvisual field sensitivity from monocular visual field results. InvestOphthalmol Vis Sci 41:2212–2221
Graefes Arch Clin Exp Ophthalmol (2013) 251:1335–1341 1341