Embed Size (px)
Citation preview
Fitting professionalism into
medical curricula
Charlotte Rees PhD, FRCP (Edin)
Faculty of Medicine, Nursing & Health Sciences
2
Talk overview
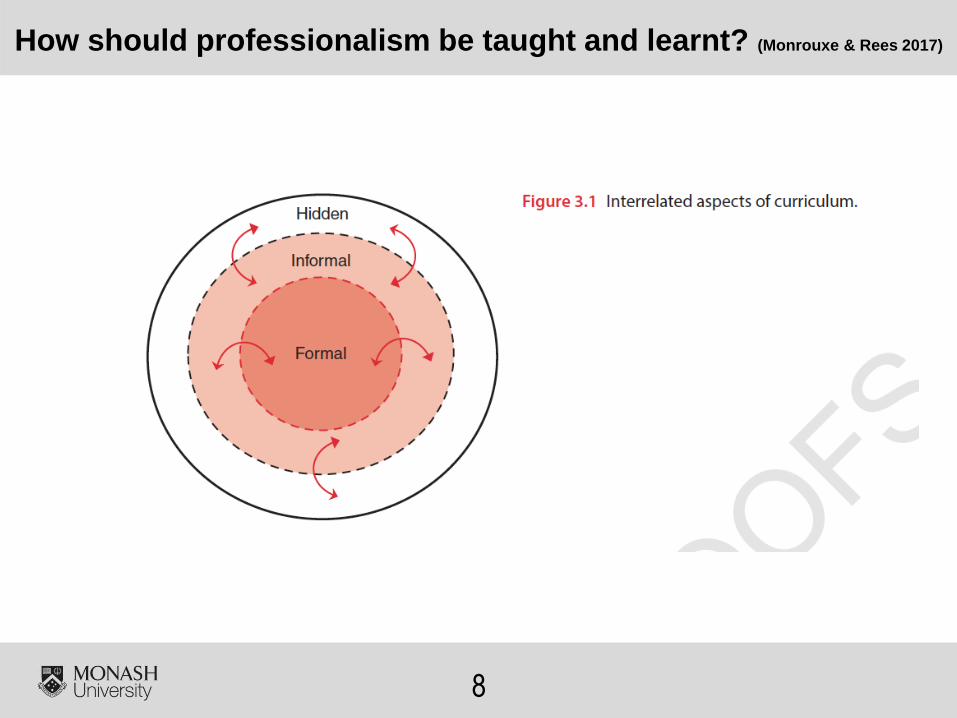
Medical students learn
professionalism though inter-related
aspects of curricula
How should educators best fit
professionalism into the medical
curriculum?
– What is professionalism?
– How should it be taught, learnt and
assessed?
– What are the tensions?
3
What is professionalism?
No consensus definition of
professionalism
Understandings vary by
person, context and time
Definitions should be context-
specific (Monrouxe & Rees 2017)
4
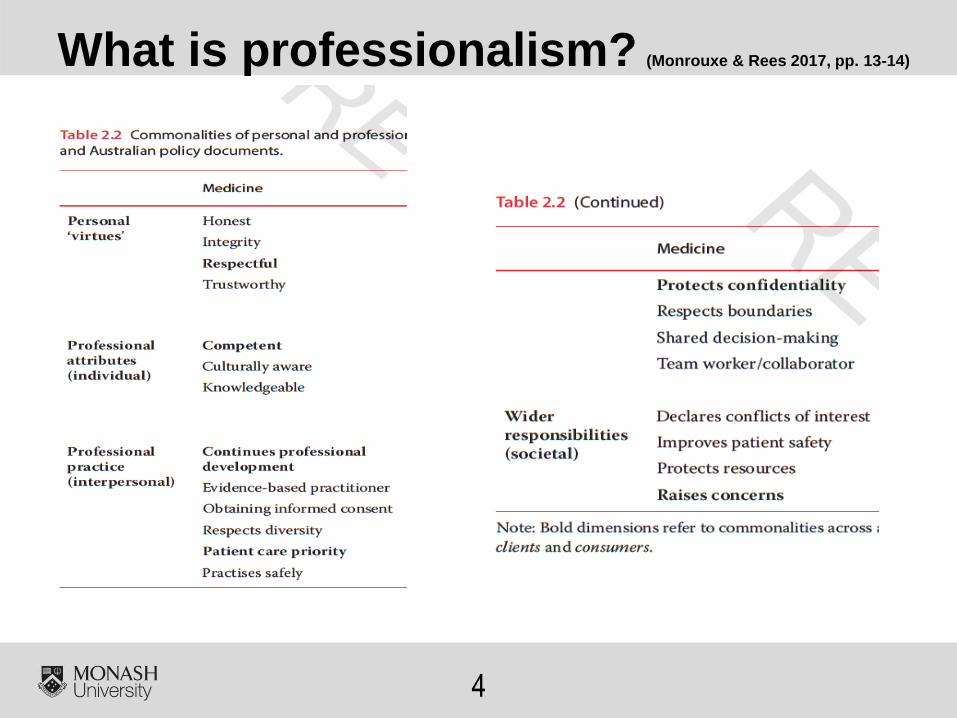
What is professionalism? (Monrouxe & Rees 2017, pp. 13-14)
5
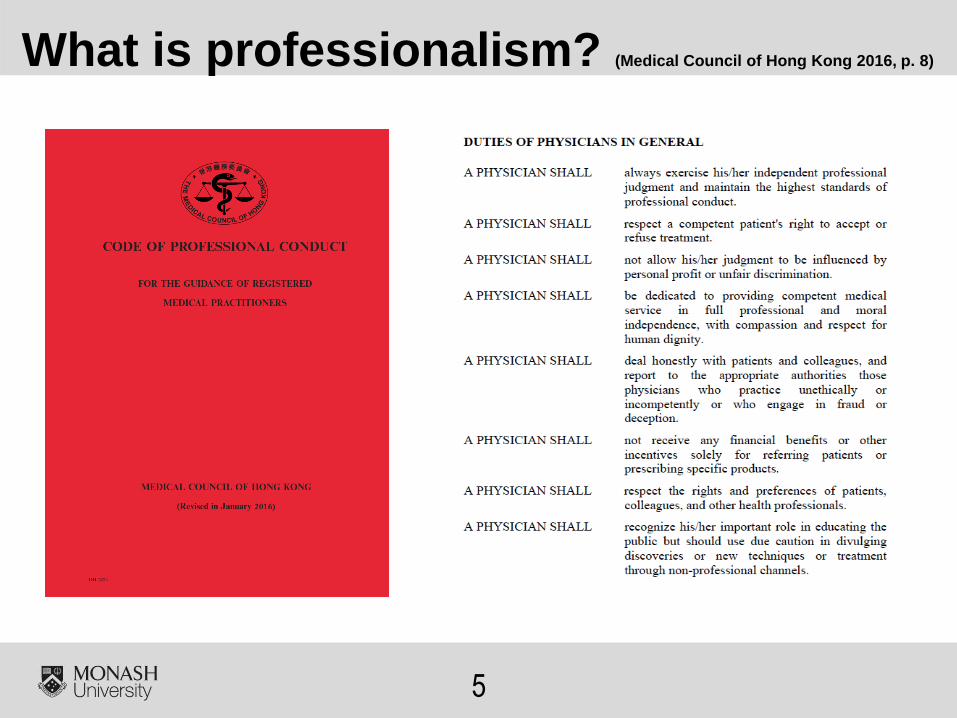
What is professionalism? (Medical Council of Hong Kong 2016, p. 8)
6
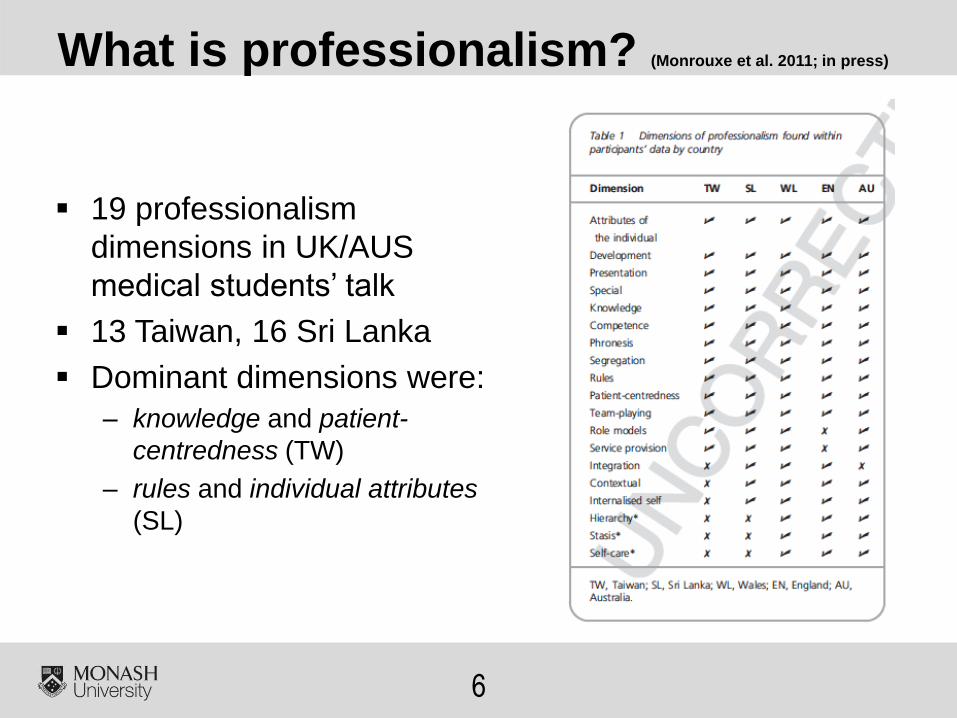
What is professionalism? (Monrouxe et al. 2011; in press)
19 professionalism
dimensions in UK/AUS
medical students’ talk
13 Taiwan, 16 Sri Lanka
Dominant dimensions were:
– knowledge and patient-
centredness (TW)
– rules and individual attributes
(SL)
7
What is professionalism? (Monrouxe et al. in press)
Knowledge: “we should have the medical
knowledge that we need… before we go to see
patients, that’s a basic” (TWY5F1)
Patient-centeredness: “You are doctors and
they believe in you so, what you can do is… just
[be with them]…” (TWY6F40)
Rules: “Maybe it’s not solely defined by our
profession, what our profession is, it’s rather on
the society... so their expectations should be the
standard of our professionalism” (TWY7M40)
Attributes of individual: “the way they [doctors]
behave… the way they move, [the] way they talk,
how they deal with people… all are included in…
professionalism” (SLY2M4)
8
How should professionalism be taught and learnt? (Monrouxe & Rees 2017)
9
How is professionalism taught through the formal curriculum? (Monrouxe & Rees 2017)
• Difficult to integrate professionalism into FC
as it crosses ‘departments’ (O’Sullivan et al. 2012)
• Different levels of integration across
schools
• Professionalism should take place in most
‘authentic’ context (O’Sullivan et al. 2012)
• Huge variation in methods with no
consensus about best practice (Birden et al. 2013)
• Personal reflections facilitated by faculty,
mentoring and role-modeling are most
effective (Birden et al. 2013)
10
How is professionalism learnt through the informal curriculum? (Monrouxe & Rees 2017)
Students learn professionalism through role modeling
Role models are defined as: “people we can identify with,
who have the qualities we would like to have, and are in
positions we would like to reach” (Paice et al. 2002)
Role models are thought to possess clinical competence,
teaching skills and personal qualities
Learning from role models can occur through:
– Unconscious incorporation of observed behavior into practice
– Conscious reflection and attunement of emotion/values and then
adoption or resistance of observed behaviors (Cruess et al. 2008)
11
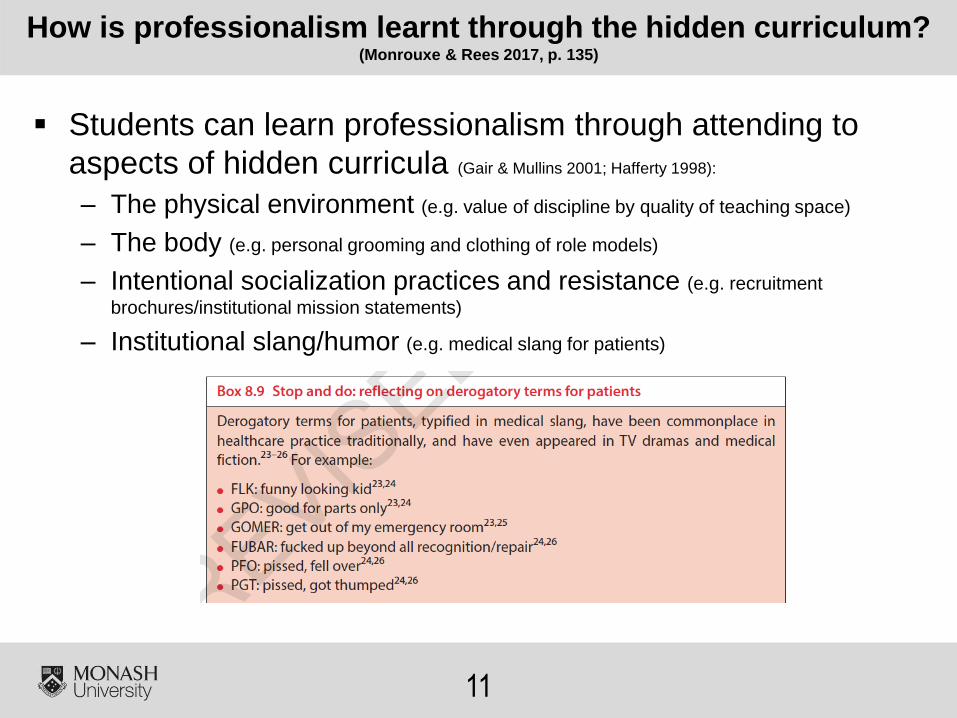
How is professionalism learnt through the hidden curriculum? (Monrouxe & Rees 2017, p. 135)
Students can learn professionalism through attending to
aspects of hidden curricula (Gair & Mullins 2001; Hafferty 1998):
– The physical environment (e.g. value of discipline by quality of teaching space)
– The body (e.g. personal grooming and clothing of role models)
– Intentional socialization practices and resistance (e.g. recruitment
brochures/institutional mission statements)
– Institutional slang/humor (e.g. medical slang for patients)
12
How should professionalism be assessed? (Monrouxe & Rees 2017)
Many argue for programmatic approach to assessment (Van Mook et al. 2009)
Assessment methods should depend on purpose and
characteristics (Sullivan & Arnold 209)
Some argue for professionalism assessment at
individual, interpersonal and institutional levels (Hodges et al.
2011)
Some argue for assessment at all levels of Miller’s
pyramid (Miller 1990; Hawkins et al. 2009)
Most professionalism assessment occurs at does/shows
how rather than knows how/knows levels
13
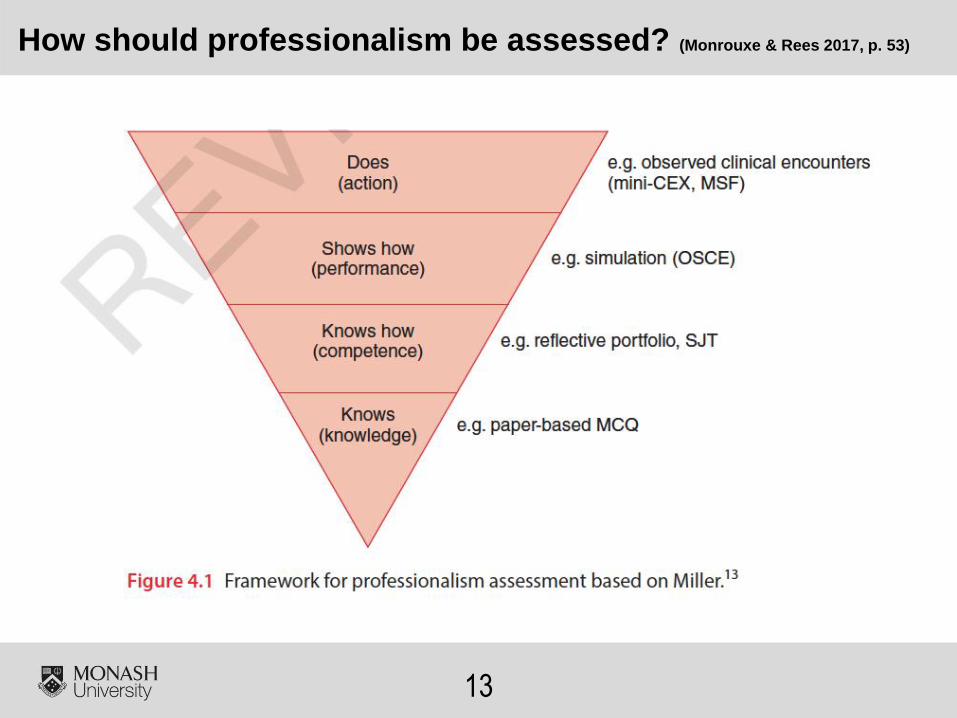
How should professionalism be assessed? (Monrouxe & Rees 2017, p. 53)
14
Tensions exist between what is
taught and what is learnt
Mixed messages create
professionalism dilemmas for
students (e.g. Monrouxe & Rees 2012)
Students commonly go along
with informal and hidden
curricula (e.g. Rees et al. 2013)
This can create moral distress
for learners (Monrouxe et al. 2015)
Curriculum tensions and professionalism dilemmas
15
16
Pay more attention to informal
and hidden curricula, plus
enhance formal curriculum
Provide students with
opportunities to de-brief
Create open/safe fora for
students to share their
experiences in small groups (Christakis
& Feudtner 1993; Monrouxe et al. 2012)
Model sharing by discussing our
own professionalism dilemmas
As educators we need to:
17
Professionalism needs to be
understood within its local context
Faculty need to think about the
impact of the IC/HC on
professionalism learning
Students experience
professionalism dilemmas within
workplace learning
We need to help them make
sense of these experiences as
part of FC
Key take home messages
18
Research collaborators (e.g.
Prof Lynn Monrouxe, Dr
Madawa Chandratilake & Prof
Ming-Jung Ho)
Our research participants
Funders (e.g. British Academy,
ASME, AMEE, HEA, NES)
CUMEC colleagues for inviting
me to talk today
Acknowledgements
19
Key reference for talk (http://au.wiley.com/WileyCDA/WileyTitle/productCd-1119044448.html)
20
Birden H et al. (2013) Teaching professionalism in medical education: A best evidence medical
education (BEME) systematic review. BEME guide no. 25. Medical Teacher 35, e1252-e1266.
Christakis DA & Feudtner MA (1993) Ethics in a short white coat: the ethical dilemmas that medical
students confront. Academic Medicine 68, 249-254.
Cruess et al. (2008) Role modeling – making the most of a powerful teaching strategy. BMJ 336,
718-721.
Gair M & Mullins G (2001) Hiding in Plain Sight. In E. Margolis (ed.) The Hidden Curriculum in
Higher Education. New York: Routledge; pp. 21-41.
Hafferty FW (1998) Beyond curriculum reform: confronting medicine’s hidden curriculum.
Academic Medicine 73(4), 403-407.
Hawkins et al. (2009) Assessment of medical professionalism: who, what, when, where, how and
why? Medical Teacher 31, 348-361.
Hodges B et al. (2011) Assessment of professionalism: Recommendations from the Ottawa 2010
Conference. Medical Teacher 33, 354-363.
Medical Council of Hong Kong (2016) Code of Professional Conduct. For the Guidance of
Registered Medical Practitioners. Hong Kong: Medical Council of Hong Kong.
Miller GE (1990) The assessment of clinical skills/competence/performance. Academic Medicine
65(9), S63-67.
Monrouxe LV et al. (2011) Differences in medical students’ explicit discourses of professionalism:
acting, representing, becoming. Medical Education 45, 585-602.
References I
21
Monrouxe LV & Rees (2012) “It’s just a clash of cultures”: emotional talk within medical students’
narratives of professionalism dilemmas. Advances in Health Sciences Education 17(5), 671-701.
Monrouxe LV et al. (in press) Taiwanese and Sri Lankan students’ dimensions and discourses of
professionalism. Medical Education.
Monrouxe LV et al. (2015) Professionalism dilemmas, moral distress and the healthcare student:
insights from two online UK-wide questionnaire studies. BMJ Open 5:e007518.
doi:10.1136/bmjopen-2014-007518.
Monrouxe LV & Rees CE (2017) Healthcare Professionalism: Improving practice through
reflections on workplace dilemmas. Oxford: Wiley-Blackwell.
O’Sullivan H et al. (2012) Integrating professionalism into the curriculum: AMEE Guide No. 61.
Medical Teacher 34, e64-e77.
Paice E et al. (2002) How important are role models in making good doctors? BMJ 325, 707-710.
Rees CE et al. (2013) Narrative, emotion, and action: Analysing ‘most memorable’ professionalism
dilemmas. Medical Education 47(1), 80-96.
Sullivan C & Arnold A (2009) Assessment and remediation in programs of teaching
professionalism. In: RL Cruess, SR Cruess & Y Steinert (Eds.) Teaching Medical Professionalism.
New York: Cambridge University Press; pp. 124-149.
Van Mook et al. (2009) Approaches to professional behavior assessment: Tools in the
professionalism toolbox. European Journal of Internal Medicine 20, e153-e157.
References II

Questions?