Embed Size (px)
Citation preview

First nationwide survey of the health of schoolchildren in Chad
Michael Beasley1, Simon Brooker1, Montanan Ndinaromtan2, Ester M. Madjiouroum2, Marie Baboguel3,
Elie Djenguinabe4 and Don A. P. Bundy5
1 Department of Infectious Disease Epidemiology, Imperial College School of Medicine, London, UK2 Hopital General de Reference, N’Djamena, Chad3 School Health Commission, Ministere de la Sante, N’Djamena, Chad4 School Health Commission, Ministere de l’Education, N’Djamena, Chad5 International School Health Initiative, Human Development Division, The World Bank, Washington DC, USA
Summary Survey data are presented from a nationwide survey of the health of schoolchildren in Chad. The
country was stratified into distinct ecological zones based on satellite sensor environmental data.
Twenty schools were visited and 1024 children aged between 6 and 15 years were included in the
study. The overall prevalence of stunting, underweight, anaemia and goitre was 18.7, 16.5, 25.1 and
23.3%, respectively. Schistosoma haematobium, Schistosoma mansoni and hookworm were the only
helminth species found with prevalences of 13.2, 1 and 32.7%, respectively. A greater proportion of
boys were stunted, underweight, anaemic and infected with S. haematobium and hookworm than
girls. Older children were more stunted, underweight and infected with S. haematobium and
hookworm than younger children, but less anaemic. The prevalence of infection showed marked
geographical heterogeneity, with hookworm prevalence being highest in the Sudanian and tropical
zone, and S. haematobium being most prevalent in the Sahelian zone and the Logone and Chari basins
in the west of the country. These data show that there is a high prevalence of helminth infection in
Chad, but that treatment for S. haematobium and hookworm should be targeted to different
geographical areas.
keywords hookworm, schistosomiasis, anaemia, goitre, stunting, underweight, schoolchildren, Chad
correspondence Simon Brooker, Department of Infectious Disease Epidemiology, Imperial College
School of Medicine, Norfolk Place, London W2 1PG, UK. E-mail: [email protected]
Introduction
As part of its recent education reform, the Government of
Chad has identified health and nutrition as major con-
straints on the quality of school learning and educational
achievement of children. Before health services can be
planned efficiently, data are required concerning the
prevalence and distribution of infection and malnutrition
in the country. Previous studies of these problems among
schoolchildren in Chad have for the most part been rare,
limited and extremely dated (Buck et al. 1970; Gigase et al.
1988; Massenet et al. 1995), with the recent exception of a
national survey of iodine deficiency (Wyss et al. 1996). For
this reason, it was deemed necessary to conduct the first
nationwide survey of the nutritional status and parasitic
infections of Chad’s schoolchildren. The present paper
reports the results of this survey.
Materials and methods
Sample design and study population
A nationwide survey was undertaken in Chad in November
2000. The country was divided into separate ecological
zones based on the mean annual summaries (1982–2000
inclusive) of multitemporal remotely sensed (RS) data from
the Advanced Very High Resolution Radiometer (AVHRR)
(see Brooker et al. 2002a for details) (Figure 1). Overlay-
ing this map with available data on population density
(Deichmann 1996) helped guide the sample protocol,
focusing on the populous south-west of the country. In this
area, there are three ecological zones (Sahelian, Sudanian
and Tropical) and an urban zone (the capital, N’Djamena).
Internal travel is extremely difficult in many areas of
Chad and finance and availability of staff for the survey
Tropical Medicine and International Health
volume 7 no 7 pp 625–630 july 2002
ª 2002 Blackwell Science Ltd 625

were limited. These factors constrained the sample to a
total of 20 schools all situated not more than 30 km from
the country’s main roads. The number of schools sampled
in each zone was then proportional to the national
population in each zone. For example, 10% of Chad’s
population lives in the Tropical zone, consequently two
schools were sampled here.
In each sampled school, a target of 25 boys and 25 girls
in Class 3 (9–10 year olds) were randomly selected. If there
were insufficient pupils in Class 3 additional pupils were
sampled from Classes 4–7. Many of the schools visited
were small, and this, compounded by low female enrol-
ment, meant that in many schools all girls were selected to
achieve the target sample size, and in some cases fewer
than 25 girls were present, and therefore examined.
Participation was voluntary and was approved by the
school committee and parents.
Investigations
The height and weight of each child was measured to the
nearest 0.1 cm and 0.1 kg, respectively, using a stadiom-
eter (‘Leicester’ Model, Child Growth Foundation, UK)
and electronic scales (Soehnle, CMS Weighing Equipment,
UK). Z-scores of height-for-age, weight-for-age and
weight-for-height were calculated using NCHS reference
values using Anthro software (CDC, Altanta, GA, USA).
Children with a Z-score of height-for-age, weight-for-age
or weight-for-height of £ 2 SD below the NCHS median
were defined as stunted, underweight or wasted, respect-
ively. Finger prick blood was used to estimate the haemo-
globin concentration using a portable photometer
(Hemocue Ltd, Sheffield, UK). Anaemia was defined as a
haemoglobin concentration < 110 g/l. Children underwent
a brief standardized clinical examination to assess presence
and size of goitre, which was graded: grade 0, no goitre;
grade 1, not visible but palpable; grade 2, thyroid visible.
No grade 2 was seen during the survey and therefore all
goitre is taken as not visible but palpable.
A faecal sample was collected from each child and
examined using the Kato–Katz method and the concen-
tration of helminth eggs was expressed as eggs per gram of
faeces (epg). Ten millilitres of a urine specimen collected
from each child was collected and filtered through a
13-mm diameter polycarbonate membrane with a 12-lm
pore size (Millipore Ltd, UK). The presence of Schistosoma
haematobium eggs was noted and the concentration
expressed as eggs/10 ml urine. Individual children found
infected with schistosomiasis were given a 40-mg/kg dose
of praziquantel and those infected with geohelminth
species were given 400 mg albendazole.
Data analysis
The aims of this study were to first describe the prevalence
and distribution of helminth infection and undernutrition
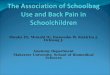
(a) (b)
Figure 1 (a) Ecological zones in Chad based on RS-derived variables; and (b) the population density of chad. Data source: Deichmann (1996).
Tropical Medicine and International Health volume 7 no 7 pp 625–630 july 2002
M. Beasley et al. Health of schoolchildren in Chad
626 ª 2002 Blackwell Science Ltd

in Chad, and secondly to examine the variations within
individuals. The relationship between undernutrition and
infection with age group and sex was assessed using logistic
regression. Models were constructed which controlled for
either age group or sex. Differences in means were
compared using either a Student’s t-test and Mann–
Whitney U-test. Analysis was undertaken using Stata
(version 6, College Station, TX, USA).
Results
Table 1 summarizes the prevalence of undernutrition and
micronutrient deficiency by ecological zone. Stunting, a
measure of chronic or long-term malnutrition was similar
throughout the Sahelian, Sudanian and Tropical zones
(approximately 20%) and was lower in N’Djamena
(10.7%). The prevalence of anaemia varied from 12 to
35.3%, being highest in the Sahelian zone and lowest in
N’Djamena. Goitre rates ranged from 7 to 18% in
the South and N’Djamena to 33–45% in the Sahel and the
Logone and Chari basins in the West of the country.
Table 2 summarizes the prevalence and intensity of
infection in Chad by ecological zone. Schistosoma
haematobium, S. mansoni and hookworm were the only
helminth species found with prevalences of 13.2, 1 and
32.7%, respectively. Mean egg counts were light for both
S. haematobium and hookworm. Few children (7.1%)
were infected with both species. The prevalence of
S. haematobium and hookworm was found to vary
considerably between zones, with S. haematobium being
most prevalent in the Sahelian and Sudanian zones and
lowest in the south near the Central African Republic and
in N’Djamena. In the Sudanian zone, S. haematobium
infection was most common in the Logone and Chari
basins. By contrast, hookworm was most prevalent in the
south of the country, in the Sudanian and Tropical zones.
Nowhere in the country did Ascaris lumbricoides and
Trichuris trichiura occur at detectable levels.
Stratification by age revealed considerable differences in
the prevalence of infection and undernutrition: older
children were more stunted and underweight, had higher
rates of goitre and were more infected; whilst younger
children were more anaemic (Table 3). There were also
significant differences between the sexes, with significantly
more boys than girls infected with S. haematobium and
hookworm (Table 4); and boys were more heavily infected
than girls with S. haematobium (15.6 vs. 9.4 eggs/10 ml,
P < 0.05) and hookworm (208 vs. 132 eggs/gram,
P < 0.02). Boys were also more stunted, underweight and
anaemic, while girls had more goitre (Table 4).
Table 2 Prevalence of infection and mean egg counts of helminths by ecological zone in Chadian schoolchildren
Schistosoma haematobium Hookworm Both*
Ecological zone N Per cent infected Mean epg N Per cent infected Mean epg Per cent infected
N’Djamena 152 2.6 4.9 142 9.2 72 0.7Sahelian� 258 39.1 27.5 258 3.1 4 1.6Sudan 511 23.2 10.9 506 47.8 256 12.2Tropical 99 6.1 0.3 97 67.0 408 5.3
Total 1020 22.5 13.2 1003 32.7 180 7.1
* Nine hundred and ninety-four children provided both a stool and urine sample.�Not including N’Djamena.
Table 1 Prevalence of undernutrition and anaemia by ecological zone in Chadian schoolchildren
Ecologicalzone N
Per cent anaemia(Hb < 110 g/l) Mean Hb Per cent goitre
Per cent stunted(HAZ ± 2 SD)
Per cent underweight(WAZ ± 2 SD)
Per cent wasted(WHZ ± 2 SD)*
N’Djamena 151 12.0 121 11.8 10.7 18.0 7.1Sahelian� 258 35.3 114 44.6 20.2 28.7 10.4Sudan 514 23.4 118 17.0 19.9 10.5 0.5Tropical 101 26.7 117 17.8 20.8 13.9 0.0
Total 1024 25.1 117 23.3 18.7 16.5 4.6
* Sample size ¼ 392. Only calculated for below age 10 years for girls and 11.5 years for boys.�Not including N’Djamena.
Tropical Medicine and International Health volume 7 no 7 pp 625–630 july 2002
M. Beasley et al. Health of schoolchildren in Chad
ª 2002 Blackwell Science Ltd 627

Discussion
Good health and nutrition are essential prerequisites for an
effective education. Some health conditions of the greatest
importance for education can be dealt with most cost
effectively by schools themselves. The FRESH partnership
(Focusing Resources on Effective School Health) of the
World Health Organization, UNICEF, UNESCO and the
World Bank, has identified school health and nutrition
programmes as an essential component of efforts to achieve
equitable access to Education for All in low-income
countries.
Table 3 Mean anthropometric, haemoglobin and parasitological measurements and indices in children in Chad by age group, and thepercentage of children classified as stunted, underweight and anaemic
Mean (SD)
Ten years and below >10 years Significant difference (t-test)
Body mass index 15.1 16.1 <0.001Height-for-age z-score )0.65 )1.41 <0.001Weight-for-age z-score )0.96 )1.48 <0.001Haemoglobin (g/l)* 114.3 121.1 <0.001
(%) (%) Adjusted OR� (95% CI)
Stunted 11.1 26.6 2.88 (2.02–4.00)Underweight 10.1 23.2 2.61 (1.83–3.71)Body mass index < 15 50.1 26.1 0.35 (0.27–0.46)Anaemic (Hb < 110 g/l) 31.7 18.3 0.45 (0.34–0.61)Goitre 20.7 26.0 1.39 (1.03–1.85)Hookworm 27.5 38.1 1.58 (1.21–2.07)Schistosoma haematobium 18.5 26.6 1.50 (1.11–2.03)Schistosoma haematobium and hookworm 3.8 10.6 2.82 (1.63–4.87)
* Males as referent, controlling for age group.�6–10 years as referent, controlling for sex.
Table 4 Mean anthropometric, haemoglobin and parasitological measurements and indices in boys and girls in Chad, and the percentageof children classified as stunted, underweight and anaemic
Mean (SD)
Male Female Significance difference (t-test)
Body mass index 15.6 (1.5) 15.5 (1.7) 0.562Height-for-age z-score )1.15 (1.11) )0.84 (1.20) <0.001Weight-for-age z-score )1.31 (0.82) )1.08 (0.82) <0.001Weight-for-height z-score* )0.71 (0.77) )0.81 (0.78) 0.228Haemoglobin (g/l)� 116 (15) 120 (14) <0.001
(%) (%) Adjusted OR� (95% CI)
Stunted 20.8 15.4 2.84 (2.02–4.00)Underweight 19.0 12.6 2.61 (1.83–3.72)Wasted* 4.6 4.5 0.97 (0.34–2.79)Body mass index < 15 36.6 40.9 1.11 (0.85–1.44)Anaemic (Hb < 110 g/l) 29.0 18.9 0.52 (0.38–0.72)Goitre 21.3 26.4 0.26 (0.13–0.51)Hookworm 35.3 28.5 1.58 (1.21–2.08)Schistosoma haematobium 28.8 12.7 1.50 (1.11–2.03)Schistosoma haematobium and hookworm 10.0 2.6 2.82 (1.63–4.87)
* Only calculated for below age 10 years for girls and 11.5 years for boys.�Males as referent, controlling for age group.
Tropical Medicine and International Health volume 7 no 7 pp 625–630 july 2002
M. Beasley et al. Health of schoolchildren in Chad
628 ª 2002 Blackwell Science Ltd

Each school health programme must be tailored to its
specific national context. Before a programme can be
designed, a clear understanding is needed of the prevalence
and distribution of the problems to be addressed. But in
many low-income countries, studies of malnutrition and
infection of school-aged children are rare, limited in scope
or out of date. The data from the present study describe the
health status of schoolchildren in Chad, which were
collected according to ecological rather than geographical
areas, where the number of samples needed is much less
than required by traditional methods of surveying, and so
costs are reduced dramatically. In the absence of other data
from Chad, it is not possible to detect whether our
sampling protocol incurred any particular bias. It is
possible that patterns of transmission and malnutrition
may have differed in more remote areas of the country but
this is purely speculative. The survey was completed during
a 4-week period in November 2000 at an approximate cost
of US $34 000. This sum included purchase of necessary
equipment, transport costs and all consultant and staff
costs. It is not clear that, had more children been sampled,
unit costs would have been reduced.
The survey results show that the prevalence of undernu-
trition in Chad was comparable with other African countries
and while a cause for concern is marginally better than in
some (Stoltzfus et al. 1997a; PCD 1998; Lwambo et al.
2000). Anaemia was also less prevalent than in other African
countries (Stoltzfus et al. 1997b; Lwambo et al. 2000; PCD
2001). Intensity of helminth infection is believed to be a
major determinant of morbidity because of helminth infec-
tion, such as anaemia (Stephenson 1987; Stoltzfus et al.
1997b; Lwambo et al. 2000); thus, a possible explanation
for the relatively low prevalence of anaemia are the light
infections harboured by children in Chad.
An extensive survey of iodine deficiency in Chad was
conducted in 1993, reporting goitre prevalences of
60–70% across the country, with the exception of
N’Djamena where the prevalence was 25% (Wyss et al.
1996). Although our sample and that of the 1993 survey
differed (7–12 vs. 10–20 year olds; school based vs.
community based), the results do indicate that the
situation has marginally improved, but that more regional
variation now exists than formerly. While goitre rates
have fallen considerably in the South and N’Djamena
(7–18%), rates remain elevated in the Sahel (45%) and
also in the Logone and Chari basins (33%). The results
underline the need for continuing public health education
concerning the consumption of iodized salt. In 1993, few
households were found to use iodized salt – only 30% in
the Sudan zone, 27% in the Sahel and 50% in
N’Djamena. Consistent with previous studies (Wolde-
Gebriel et al. 1993; Wyss et al. 1996), our study showed
girls to have more goitre than boys, partly because of
increased iodine needs during puberty and gender-related
disparities in iodine supply.
In accordance with previous surveys (Buck et al. 1970),
no cases of infection with A. lumbricoides or T. trichiura
were found in Chad, presumably because of thermal
exclusion (see Brooker et al. 2001a, b). The extreme
temperatures experienced in Chad are unfavourable to the
ova of A. lumbricoides or T. trichiura, but they are not
detrimental to hookworm larvae in certain parts of the
country. Our results suggest that hookworm infection
occurs only in the south of Chad, with little or no infection
occurring in areas where mean land surface temperature
(LST) exceeds 48 �C (Brooker et al. 2001a). This distri-
bution pattern probably defines the upper thermal limit of
hookworm infection, which is apparently greater than the
37 �C for A. lumbricoides and T. trichiura. The high
prevalence of S. haematobium in the Sahelian zone is
corroborated by previous studies in Chad (Buck et al.
1970; Gigase et al. 1988; Massenet et al. 1995) showing
that areas of significant transmission are the Sahelian zone
and the Logone and Chari river basins.
The national survey aimed to understand the distribution
of undernutrition and infection within the country in order
to enable targeting of control programmes. The results of
the nutrition survey showed that children living in the
Sahelian zone were comparatively disadvantaged with
respect to protein energy malnutrition, anaemia and iodine
deficiency. Iodine deficiency was also a problem in the
Logone and Chari basins. School-based nutrition education
to combat protein energy malnutrition and iodine defici-
ency is needed in all areas of the country. Weekly school-
based iron supplementation should also be introduced
countrywide. Especially, priority should be given to the
promotion of all these interventions in the Sahelian zone.
According to WHO guidelines, all children living in the
Tropical and Sudanian zones should received mass treat-
ment with albendazole for hookworm infection. A pro-
gramme for schistosomiasis control, which would require
targeting schools by a questionnaire (Red Urine Study
Group 1995; PCD 1999) and a calculation to determine
the praziquantel dose based on the height of the child (Hall
et al. 1999) is required in the Sahelian zone and in the
Logone and Chari basins. Treatment is not required
elsewhere in the Sudanian zone or in the Tropical zone. In
Chad as a whole, a combined albendazole/praziquantel
treatment strategy is required only in the Logone and Chari
basins.
This survey provides comprehensive data on the preval-
ence and distribution of undernutrition and helminth
infections among schoolchildren across Chad. The results
suggest that efforts to provide nutritional interventions and
Tropical Medicine and International Health volume 7 no 7 pp 625–630 july 2002
M. Beasley et al. Health of schoolchildren in Chad
ª 2002 Blackwell Science Ltd 629

deworming to children may benefit children and improve
their learning in school.
Acknowledgements
The fieldwork was supported by the World Bank, the
Partnership for Child Development and the Wellcome
Trust. The survey was conducted at the request of the
School Health Commission of Chad, and forms part of the
preparation of the School Health Component of the Chad
Quality Education for All project, supported by the World
Bank. We thank Mourad Ezzine, Alan Dock, Lesley Drake,
Simon Hay, Kaidanoum Lea, Seung-hee Lee, N’Gooyo
Madeleine, Celia Maier, Jean-Pierre Moulia-Pelat, David J.
Rogers and William Wint for their support on various steps
of this work. S.B. is supported by a Wellcome Trust Prize
Fellowship (#062692).
References
Brooker S, Beasley NMR, Ndinaromtan M et al. (2002a) Appli-
cation of Remote Sensing and Geographical Information
Systems: The Design of a Sampling Strategy for a National
Helminth Survey in Chad. Bulletin of the World Health
Organization (in press).
Brooker S, Hay SI, Tchuem Tchuente LA & Ratard R (2002b)
Using NOAA-AVHRR data to model helminth distributions for
planning disease control in Cameroon, West Africa. Photog-
rammetric Engineering and Remote Sensing 68, 175–179.
Buck AA, Anderson RI, Sasaki TT & Kawata K (1970) Health and
Disease in Chad: Epidemiology, Culture and Environment in
Five Villages. Johns Hopkins Press, Baltimore.
Deichmann U (1996) African Population Database Documentation.
UNEP/GRID (http://grid2.cr.usgs.gov/globalpop/index/html).
Gigase PL, Mangelschots E, Bockaert R, Autier P & Kestens L
(1988) Indicateurs simples de la prevalence et de l’intensite de la
bilharziose urinaire au Tchad. Annales de la Societe Belge
Medicine Tropicale 68, 123–132.
Hall A, Nokes C, Wen ST et al. (1999) Alternatives to bodyweight
for estimating the dose of praziquantel needed to treat schisto-
somiasis. Transactions of the Royal Society of Tropical
Medicine and Hygiene 93, 653–658.
Lwambo NJS, Brooker S, Siza JE, Bundy DAP & Guyatt H
(2000) Stunting and anaemia in schoolchildren: a cross-sectional
study in Tanzania. European Journal of Clinical Nutrition 54,
36–40.
Massenet D, Abakar D & Karifene R (1995) Prevalence de la
bilharziose urinaire en millieu scolaire a N’Djamena (Tchad).
Bulletin de la Societe Pathologie Exotique 88, 34–37.
PCD (1998) The anthropometric status of school children in five
countries in the Partnership for Child Development. Proceedings
of the Nutrition Society 57, 149–158.
PCD (1999) Self-diagnosis as a possible basis for treating urinary
schistosomiasis: a study of schoolchildren in a rural area of the
United Republic of Tanzania. Bulletin of the World Health
Organization 77, 477–483.
PCD (2001) Anaemia in schoolchildren in eight countries in Africa
and Asia. Public Health Nutrition 4, 749–756.
Red Urine Study Group (1995) Identification of High Risk
Communities for Schistosomiasis in Africa: a Multi-Country
Study. Social and Economic Research Project Reports No: 15.
World Health Organization, Geneva.
Stephenson LS (1987) Impact of Helminth Infection in Human
Nutrition. Taylor & Francis, New York.
Stoltzfus RJ, Albonico M, Tielsch JM, Chwaya HM & Savioli L
(1997a) Linear growth retardation in Zanzibari school children.
Journal of Nutrition 127, 1099–1105.
Stoltzfus RJ, Chwaya HM, Tielsch JM, Schulze KJ, Albonico M &
Savioli L (1997b) Epidemiology of iron deficiency anemia in
Zanzibari schoolchildren: the importance of hookworms.
American Journal of Clinical Nutrition 65, 153–159.
Wolde-Gebriel Z, Demeke T, West CE et al. (1993) Goitre in
Ethiopia. British Journal of Nutrition 69, 257–268.
Wyss K, Guirai C, Ndikuyeze A, Malonga G & Tanner M
(1996) Prevalence of iodine deficiency disorders and goitre
in Chad. Tropical Medicine and International Health 1,
723–729.
Tropical Medicine and International Health volume 7 no 7 pp 625–630 july 2002
M. Beasley et al. Health of schoolchildren in Chad
630 ª 2002 Blackwell Science Ltd