Embed Size (px)
Citation preview

April 21 - 25, 2009Phoenix Convention Center, Phoenix, Arizona
Final Program
International Pediatric Endosurgery group
18th Annual Congress for Endosurgery in Children
2009 Surgical Spring Week
Held in conjunction with the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES)

Inside Front Cover
Storz Ad

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 1
General InformationIPEG’s 18th Annual Congress for Endosurgery in ChildrenApril 21 - 25, 2009
2009 Meeting Objectives: The objectives of the activity are to educate, expose and allow pediatric surgeons and urologist the opportunity to discuss the developing techniques and management principles regarding minimally invasive surgical techniques and scientific developments that will affect their patient population.
Specific Objectives include:
•Presentationofnewanddevelopingminimally invasive surgical techniques in a scientific environment.•Opportunitytointeractwithexperts
in the fields of minimally invasive pediatric surgery and urology via panel interactions and audience response systems.•Discussionofcurrentandfuture
controversial issues regarding minimally invasive surgery in infants and children.•Advancetheuseofminimallyinvasive
surgical procedures in infants and children.•Encourageinternationalinteractionsin
the management and minimally invasive surgical interventions for infants and children.
Attheconclusionofthisevent,theparticipant will be able to implement the information and techniques that were obtained during the event and by doing this the care of that population will be improved and will continue to advance.
Scientific Session Objectives:
Attheendofthissession,participantswill understand the current and emerging practices and procedures in minimal access surgery and other developing applications.Participantswillacquireinformation, which relates to indications, contraindications, diagnosis, technique, prevention and management of complications, and results of minimal access surgery, endoscopic, and general surgicalproceduresParticipantswillrecognize the scientific and physiologic basis of minimal access surgery, endoscopy and emerging surgical technology (e.g. robotics,singleportaccess,andNOTES®).
IPEG Is Going Green!Presentations will be made available on the IPEG website.
Table of Contents 1 MeetingDescription&Objectives 2 RegistrationHours,ExhibitDates&Times,PosterHours,PhoenixMap 3 MeetingLeaders,AboutIPEG 4 Accreditation&CMEWorksheet 5 SpeakerBios 4 IPEGSchedule-at-a-Glance 7 Floorplan&LearningCenterInfo. 8 IPEGAdvanceLaparoscopicSingleIncisionCourse 9 OpeningExhibitReception 9 Thursday, April 23, 2009 9 IPEG/SAGESJointBreakfastVideoSession:Hepatobiliary&SolidOrgan 10 ScientificSession:ClinicalandBasicScience ScientificSession:HowIDoIt 11 IPEGPresidentialAddress&ScientificSession:Thorax 12 KarlStorzLecture Panel:ShowdownattheAnorectalCanal PosterTours 13 Friday, April 24, 2009 13 MorningVideoSession:MyFavoriteTricks ScientificSession:Gastrointestinal&Hepatobiliary 14 KeynoteLecture:MISinChina ScientificSession:AllShortPapers 15 Robotics&EmergingTechnology 16 Panel:CuttingEdgeGenitourinaryReconstruction SAGES/IPEGJointPanel:Urgent&EmergentAcute CareProblemsinPediatricsandAdults 17 IPEG/SAGESSimulatorSession IPEG/SAGESGala 18 Saturday, April 25, 2009 18 IPEGGeneralAssembly ScientificSession:NOTES®,SingleIncisionAccessSurgery,&Urology 19 IPEGAwardsSession ScientificVideoSession:Miscellaneous 20 IPEGFaculty 23 FacultyDisclosures 24 PresenterDisclosures 26 OralAbstracts 47 VideoAbstracts 50 PosterAbstracts 66 ExhibitsFloorPlan 67 ExhibitorListing 76 Long Term Research Fund
Description: Thethemeofthe2009IPEGMeetingwillbe a case oriented approach to challenges in clinical situations with expert panels, joint sessions, and with invited faculty whowillspeakonspecifictopics.Includedare oral sessions, video presentations, and poster presentations of abstracts selected byProgramCommittee.Panelinformationand information about the abstract &videopresentationsessionswillbeavailableintheFinalProgramdistributedon-site.
What is included?IncludesentrancetotheIPEGScientificsessionsonThursday,Friday,&Saturday,entrancetotheexhibithall&welcomereception,generalsessionbreaks,ThursdayPosterTours,FridayLunchintheExhibitHall,andMainevent
Where?Phoenix Convention Center100NorthThirdStreetPhoenix,AZ85004
Who?International Pediatric Endosurgery Group (IPEG)11300W.OlympicBlvd.,Suite600 LosAngeles,CA90064 Phone:310-437-0553Fax:310-437-0585 Email:[email protected] Website:www.ipeg.org
Hotels Wyndham Phoenix (IPEG Headquarters) 50EastAdamsStreet,Phoenix,AZ85004Phone:602-333-5500or800-996-3426

2 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
IPEG Corporate SupportersThank you to all IPEG’s 2009 corporate supporters!
DIAMOND DONORS
KARL STORZ ENDOSCOPY-AMERICA
STRYKER ENDOSCOPY
PLATINUM DONORS
COVIDIEN
GOLD DONORSCHILDREN’S MERCY HOSPITALS AND CLINICS
BRONZE DONORSCHILDREN’SHOSPITALCINCINNATIETHICONENDO-SURGERy,INC.
Exhibit Dates and TimesWednesday, April 22, 2009 OpeningReception 5:00PM-7:00PM
Thursday, April 23, 2009 HallOpen 9:30AM-3:30PM
Friday, April 24, 2009 HallOpen 9:30AM-3:30PM
Saturday, April 25, 2009 HALL CLOSED Posters&Learning Centerstillopen 9:30AM-1:30PM
SAGES&IPEGexhibitswilltakeplaceatthePhoenixConventionCenterinNorthExhibitHallD-E.
SAGES & IPEG Registration HoursTuesday, April 21, 2009: 12:00PM-5:00PM
Wednesday, April 22, 2009: 6:30AM-6:00PM
Thursday, April 23, 2009: 7:00AM-6:00PM
Friday, April 24, 2009: 6:30AM-6:00PM
Saturday, April 25, 2009: 7:00AM-2:00PM
IPEG Registrants: AttendtheSAGESScientificSessionforonly$150.Askat theRegistrationDeskfordetails.
Poster HoursThursday, April 23, 2009 PosterHours: 9:30AM-3:30PMPoster Tour: 5:00 PM - 6:30 PM (with Beer & Wine service)
Friday, April 24, 2009 PosterHours: 9:30AM-3:30PM
Saturday, April 25, 2009 PosterHours: 9:30AM-1:30PM
Speaker Prep Room HoursWednesday, April 22, 2009: 6:30AM-5:00PM
Thursday, April 23, 2009: 6:30AM-6:00PM
Friday, April 24, 2009: 6:00AM-6:00PM
Saturday, April 25, 2009: 6:30AM-3:30PM
General Information
CME & Evaluation FormsIPEG Registrants, please complete the IPEG CME & Evaluation form and turn in at the IPEG Membership Booth to have your CME certificate mailed to you after the meeting.
IPEG members who have also registered for the SAGES meeting and need to claim credits, please complete the SAGES CME Worksheet included in the SAGES final program and turn in at any of the SAGES CME drop boxes.
Please allow 4-6 weeks for processing for all CME requests.

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 3
IPEG 2009 Meet ing Leaders2009 IPEG Program Chairs
Program Chair: Daniel J. Ostlie, MD
Program Co-Chair: Benno M. Ure, MD, PhD
2009 Program Committee
HosseinAllal,MD
AayedR.Alqahtani,MD
MariaMarcelaBailez,MD
Klaas(N)M.A.Bax,MD
PeterBorzi,MD
SanjeevDutta,MD
CiroEsposito,MD
KeithE.Georgeson,MD
MuntherJ.Haddad,MD
CarrollM.Harmon,MD
GeorgeW.HolcombIII,MD
ThomasH.Inge,MD,PhD
MichaelIrish,MD
MarcA.Levitt,MD
ThomE.Lobe,MD
MarceloH.MartinezFerro,MD
GirolamoMattioli,MD
PhilippeMontupet,MD
AzadNajmaldin,MD
DanielJ.Ostlie,MD
OlivierReinberg,MD
StevenS.Rothenberg,MD
JürgenSchleef,MD
ShawnSt.Peter,MD
BennoM.Ure,MD,PhD
Jean-StéphaneValla,MD
HolgerTill,MD
DavidvanderZee,MD,PhD
JohnH.T.Waldhausen,MD
MarkL.Wulkan,MD
C.K.yeung,MD
Executive Committee
President – GeorgeW.HolcombIII,MD
President Elect – MarceloH.MartinezFerro,MD1st Vice President – BehrouzBanieghbal,MD2nd Vice President – GordonA.MacKinlay,MD,FRCSSecretary – BennoUre,MD,PhDTreasurer – MarcA.Levitt,MDJournal Editor – ThomE.Lobe,MDAsia/Africa Representative – TadashiIwanaka,MD,PhDEuropean Representative – JürgenSchleef,MDAmericas Representative – Carroll“Mac”Harmon,MD,PhDImmediate Past President – Jean-StéphaneValla,MD
IPEG Past PresidentsJean-StéphaneValla,MD (2008)
Atsuyukiyamataka,MD (2007)
KeithE.Georgeson,MD (2006)
Klaas(N)M.A.Bax,MD (2005)
C.K.yeung,MD (2004)
CraigT.Albanese,MD (2003)
VicenzoJasonni,MD (2002)
PeterBorzi,MD (2001)
StevenS.Rothenberg,MD (2000)
JohnHT.Waldschmidt,MD (1999)
HockLimTan,MD (1998)
TakeshiMiyano,MD (1997)
StevenRubin,MD (1996)
Gunter-HenrichWillital,MD (1995)
Why IPEG?Now is an excellent time to become anIPEGmember.JoinIPEGnowandreceive a substantial discount on the meeting registration by being an IPEGmember!yourduesalsoincludea subscription to the Journal of Laparoendoscopic & Advanced Surgical Techniques (A$900valueisyoursforFREE).
About IPEG
International Pediatric Endosurgery Group Member Benefits:IPEGexiststosupportexcellenceinPediatricMinimalAccessSurgeryandendoscopythrough education and research; to provide a forum for the exchange of ideas in PediatricMinimalAccessSurgeryandendoscopy;andtoencourageandsupportdevelopmentofstandardsoftrainingandpracticeinPediatricMinimalAccessSurgeryandEndoscopy.Benefitsofmembershipinclude:
•Subscriptiontoourofficialjournal:Journal of Laparoendoscopic & Advanced Surgical Techniques. (A $900 savings!IPEGmembersreceivetheJournalforFREE).
•SignificantdiscountsonregistrationfeesfortheAnnualCongressforEndosurgeryinChildren.(Note:registeringfortheIPEGScientificSession,asamember,willsaveyoutheequivalentofoneyear’sdues.)
•Affordableduesforsurgeonsandsurgeons-in-traininginanycountry.
•Opportunitiestomeetanddiscusspediatricminimallyinvasivesurgerywiththeleaders and innovators of the field.
•AccesstotheIPEGoutcomessiteontheweb.
For more information and applications, please go to: http://www.ipeg.org/whyjoin.html
Who Should Attend?The 18thAnnualCongressoftheInternationalPediatricEndosurgeryGroup(IPEG)haselementsthathavebeenspecifically designed to meet the needs of practicing pediatric surgeons, urologists &otherrelatedspecialties,physicians-in-training,GIassistantsandnurseswhoareinterested in minimally invasive surgery in children&adolescents.TheIPEGProgramCommitteerecommendsthatparticipantsdesign their own attendance schedule based on their own personal educational objectives.

4 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
IPEG Accreditat ionThisactivityhasbeenplannedandimplementedinaccordancewiththeEssentialsandStandardsoftheAccreditationCouncilforContinuingMedicalEducationthroughthejointsponsorshipoftheSocietyofAmericanGastrointestinalandEndoscopicSurgeons(SAGES).SAGESisaccreditedbytheACCMEtoprovidecontinuingmedicaleducationforphysicians.SAGESdesignatesthisContinuingMedicalEducationactivityfor
5.5AMAPRACategory1Credit(s)™fortheAdvanceLaparoscopicLecture
4.0AMAPRACategory1Credit(s)™fortheAdvanceLaparoscopicHandsOnLab
7.0AMAPRACategory1Credit(s)™forThursdaySessions
8.0AMAPRACategory1Credit(s)™forFridaySessions
2.0AMAPRACategory1Credit(s)™forSaturdaySessions
for a total of 26.5 AMA PRA Category 1 Credit(s)™. Physiciansshouldonlyclaimcreditcommensuratewiththeextentoftheirparticipation in the activity.
CME WorksheetThisisnotyourCMEcreditform.PleaseusetheworksheetbelowtotrackthenumberofCMEhoursyouattendforeachactivity.yourCMEcreditformcanbefoundinsideyourregistrantbag.FillinthenumberofhoursyouattendedeachactivityinthechartbelowtotrackyourCMEcredits.
TIME ACTIVITY CREDITS AVAILABLE
HOURS ATTENDED
TUESDAY, APRIL 21, 200912:00PM–6:00PM Advanced Laparoscopic & Single Incision Course Lecture 5.5
Total Credits Available for Tuesday, April 21, 2009: 5.5
WEDNESDAY, APRIL 22, 20097:00AM–11:00AM Advanced Laparoscopic & Single Incision Course Lab 4.0
Total Credits Available for Wednesday, April 22, 2009: 4.0
THURSDAY, APRIL 23, 20097:45AM–8:45AM IPEG/SAGES Joint Breakfast Video Session: Hepatobiliary and Solid Organ 1.08:45AM–9:00AM Welcome Address 09:00AM–10:00AM Scientific Session: Clinical & Basic Science 1.010:30AM–11:30AM Scientific Session: How I Do It 1.011:30AM–12:00PM IPEG Presidential Address: Can Prospective Clinical Trials
Be Applied to MIS in Children?0.5
1:00PM–2:15PM Scientific Session: Thorax 1.252:15PM–3:00PM Karl Storz Lecture: History & Development of a
Minimally Invasive Repair for Pectus Excavatum0.75
3:30PM–5:00PM Panel: “Showdown at the Anorectal Canal” 1.55:00PM–6:30PM Poster Tours with Beer & Wine 0
Total Credits Available for Thursday, April 23, 2009: 7
FRIDAY, APRIL 24, 20097:00AM–8:00AM Morning Video Session: “My Favorite Tricks” 1.08:00AM–9:30AM Scientific Session: Gastrointestinal & Hepatobiliary 1.59:30AM–10:00AM Keynote Lecture: “What is Going on with MIS in China?” 0.510:30AM–11:30AM Scientific Session: All Short Papers 1.011:30AM–12:30PM Scientific Session: Robotics & Emerging Technology 1.01:30PM–3:00PM Panel: Cutting Edge Genitourinary Reconstruction 1.53:30PM–5:00PM SAGES/IPEG Joint Panel: Urgent & Emergent Acute Care Problems 1.55:15PM–6:15PM IPEG/SAGES Simulator Session 0
Total Credits Available for Friday, April 24, 2009: 8
SATURDAY, APRIL 25, 20098:00AM–9:00AM General Assembly 09:00AM–10:30AM Scientific Session: Single Port Access/Notes 1.011:15AM–12:15AM IPEG Awards Session 011:15AM–12:15PM Scientific Video Session: Miscellaneous 1.012:15PM–12:30PM Closing Remarks 0
Total Credits Available for Saturday, April 25, 2009: 2.0
TOTAL CREDITS 26.5
To receive your CME credit:
TurninyourCMEformattheIPEGMembershipBoothtohaveyourCMEcertificatedmailedtoyouafterthemeeting. Pleaseallow4-6weeksforprocessing.

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 5
George W. Holcomb III, MDDr.HolcombhasservedasSurgeon-In-ChiefandtheKatharineBerryRichardsonEndowedChairinPediatricSurgeryatChildren’sMercyHospitalsandClinicssince1999.HealsoisaProfessorofSurgeryattheUniversityofMissouri-KansasCitySchool
ofMedicineandservesasDirectorofthePediatricSurgeryResidencyTrainingProgramandDirectoroftheCenterforMinimallyInvasiveSurgeryatChildren’sMercy.
Dr.HolcombreceivedhismedicaldegreeandcompletedhissurgeryresidencyatVanderbiltUniversityMedicalCenter.HecompletedhisfellowshipinpediatricsurgeryatTheChildren’sHospitalofPhiladelphia.BeforejoiningthemedicalstaffatChildren’sMercy,hewasanAssociateProfessorintheDepartmentsofPediatricSurgeryandPediatricsatVanderbilt.HecompletedhisMBAattheHenryBlochSchoolofBusinessatUMKCin2002.
Dr.HolcombisthecurrentPresidentoftheInternationalPediatricEndosurgeryGroup.Inaddition,heisanewlyelectedmemberoftheExecutiveCommitteeoftheSectiononSurgeryintheAAP.Heservesontheeditorialboardoffourmajor surgical journals and is the author of more than 200 publications,abstractsandbookchapters.Heisinternationallyrecognized as one of the leading experts in pediatric minimally invasive surgery and has made more than 100 presentations around the world on pediatric surgical topics.
Donald Nuss, MB, Ch.B., FRCS©, FACS, FAAPDr.NusswasborninPietermaritzburg,RepublicofSouthAfricaandgraduatedfromtheUniversityofCapeTown,SouthAfricain1963.Dr.NusscompletedhisGeneralSurgeryResidencyattheMayo
Clinicin1971andhisFellowshipinPediatricSurgeryatRedCrossWarMemorialChildren’sHospitalinCapeTownin1973.Dr.NussservedastheDirectorofCHKD’sDivisionofPediatricSurgeryandProfessorofSurgeryandPediatricsatEasternVirginiaMedicalSchoolinNorfolk,VirginiaandcurrentlyservesasamemberoftheBoardofDirectorsofChildren’sHospitalofTheKing’sDaughtersHealthSystem,Inc.
Dr.NussservedontheMedicalExecutiveCommitteeofChildren’sHospitalofTheKing’sDaughtersfor25yearsandasSurgeon-in-ChiefandVicePresidentforSurgicalAffairsfor20years. He helped facilitate the development of the operating roomsatChildren’sHospitalofTheKing’sDaughtersandsawthe volume of surgical patients grow from 2,200 patients per annum to over 11,000 patients per annum during his tenure as Surgeon-in-Chief.
Dr.NussisthedeveloperoftheMinimallyInvasiveProcedureforPectusExcavatumandconductsanintensiveinternationalworkshopandtrainingcourseeachyearattheChildren’sHospitalofTheKing’sDaughter’sinNorfolk,Virginia.Dr.NusshasbeenaguestlecturerandvisitingProfessoratmanymajormedicalcentersinNorthAmerica,SouthAmerica,Europe,Asia,AfricaandhasbeenaninvitedguestspeakeratnumerousNationalandInternationalSurgicalCongresses.
Dr.NussandhiswifeTessahavemadeNorfolk,Virginiatheirhome since 1977. He is the father of three daughters, Kara Saperston,MD,ElizabethPrier,MD,andKristiMilburn.
IPEG Speaker BiosLong Li, MDProfessorLiiscurrentlyProfessorofPediatricSurgeryatthedepartmentofPediatricSurgeryattheCapitalInstitutionofPediatricsinBeijing,China.HegraduatedfromtheChinaMedicalUniversityin1985,completed his postgraduate pediatric
surgicaltraining,andstartedhiscareerasafull-timepediatricsurgeoninBeijingChildren’sHospital.In1997,hereceivedtrainingasVisitingResearchFellowinpediatricsurgeryatQueenMaryHospital,HongKong.In2000,hereceivedoverseastrainingasVisitingSurgicalFellowinadvancedlaparoscopicpediatricsurgeryattheJuntendoUniversitySchoolofMedicine,andinpediatriclivertransplantationattheTokyoUniversitySchoolofMedicineinTokyo,Japan.Since2001,ProfessorLiand his team have developed a large pediatric laparoscopic surgeryprograminChina.Healsoestablishedpediatriclivertransplantation program with the first successful pediatric liver transplantationinBeijinginNovember2001.Hehascontributedmorethan170articles,2books,1setoflaparoscopicvideoandseveralbookchapterstothepediatricsurgeryliterature.
ProfessorLihasspecialinterestsinPediatrichepatobiliarysurgery and pediatric minimally access surgery and his team haveundertakenmorethan4000laparoscopicoperationsforchildren.
Gary Dunnington, MD, FACSProfessor and Chairman of Surgery, Southern Illinois University
GaryDunnington,M.D.,joinedthefacultyatSouthernIllinoisUniversityinSeptemberof1997,whereheiscurrentlyProfessorandChairmanofSurgery.HereceivedhisMD
degreefromIndianaUniversityandcompletedsurgicaltrainingattheUniversityofArizona.Dr.DunningtoncomestoSIUafternearlysixyearsattheUniversityofSouthernCaliforniawherehewasAssociateProfessorofSurgeryandSeniorAssociateDeanforAcademicAffairsfortheUSCSchoolofMedicine.Dr.Dunnington’sareaofclinicalpracticeissurgicaloncologywithafocusinbreastandendocrinedisease.AftercomingtoUSCin1991,hedevelopedtheUSC/NorrisBreastCenter,amultidisciplinary breast cancer treatment team, and has served asMedicalDirectoroftheUSC/NorrisBreastCentersincethattime.HeservesasPrincipalInvestigatoronnumerouslocalandnationalbreastcancerresearchtrials.WhileatUSC,heservedasbothClerkshipDirectorfortheDepartmentofSurgery,aswellasProgramDirector.Hehasreceivedatotaloftwelveteachingawards,havingbeennamedOutstandingFacultyTeacheroftheyeareighttimesatthreeinstitutions.Hehasbeeninvolvedin surgical education research for many years and has been the directorofafellowshipprograminsurgicaleducationatUSCandatSIU.HeisPastPresidentoftheAssociationforSurgicalEducationandreceivedthe1999DistinguishedEducatorAwardfrom this organization. He is one of five faculty who, for the lastseveralyears,havetaughttheannualSurgeonsasEducatorsCoursefortheAmericanCollegeofSurgeons.HeisafrequentvisitingprofessorofeducationtoDepartmentsofSurgerythroughouttheUnitedStatesandCanada,andisinvolvedinfaculty development seminars both regionally and nationally.

6 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
IPEG Schedule-at-a-GlanceProgram Chair: Daniel J. Ostlie, MD
Tuesday, April 21, 200912:00pm-6:00pm Advanced Laparoscopic & Single Incision
Course (Lecture) Chair:StevenS.Rothenberg,MD Co-Chairs:Carroll“Mac”Harmon,MD,Phd&DanielJ.Ostlie,MD WyndhamHotelSalon3-4
Wednesday, April 22, 20097:00am-11:00am Advanced Laparoscopic & Single Incision
Course (Lab) Chair:StevenS.Rothenberg,MD Co-Chairs:Carroll“Mac”Harmon,MD,PhD&DanielJ.Ostlie,MD Conv.Ctr.NorthExhib.HallA
5:00pm-7:00pm IPEG/SAGES Evening Exhibit Opening Reception Conv.Ctr.NorthExhibitHallD-E
Thursday, April 23, 2009
Exhibits, Posters & Learning Center Open
7:45am-8:45am IPEG/SAGES Joint Breakfast Video Session: Hepatobiliary and Solid Organ Chairs:KentKercher,MD&BennoM.Ure,MD,PhD Conv.Center–West301D
8:45am-9:00am Welcome Address GeorgeW.Holcomb,III,MD Conv.Center–West301D
9:00am-10:00am Scientific Session: Clinical and Basic Science Moderators:BennoM.Ure,MD,PhD& Atsuyukiyamataka,MD Conv.Center–West301D
10:00am-10:30am Break Foyer
10:30am-11:45am Scientific Session: How I do it Moderators:GordonA.MacKinlay,MD&C.K.yeung,MD Conv.Center–West301D
11:45am-12:15pm Presidential Address & Lecture: ”Can Prospective Clinical Trials Be Applied to MIS in Children?” Speaker:GeorgeW.Holcomb,III,MD Introductionby:DanielJ.Ostlie,MD Conv.Center–West301D
12:15pm-1:15pm Lunch (On own)
1:15pm-2:15pm Scientific Session: Thorax Moderators:StevenS.Rothenberg,MD&ShawnD.St.Peter,MD Conv.Center–West301D
2:15pm-3:00pm Karl Storz Lecture: “The Nuss procedure – The First 10 Years” Speaker:DonaldNuss,M.B.,Ch.B.,FRCS(C),FACS,FAAP Introductionby:GeorgeW.Holcomb,III,MD Conv.Center–West301D
3:00pm-3:30pm Break Foyer
3:30pm-5:00pm Panel: “Showdown at the Anorectal Canal” Chair:MarcA.Levitt,MD Conv.Center–West301D
5:00pm-6:30pm Poster Tours: Moderators:MiguelA.Guelfand,MD,TimothyD.Kane,MD,OliverMuensterer,MD,ToddA.Ponsky,MD,KlausSchaarschmidt,MD,&JürgenSchleef,MD Conv.Center-NorthExhibitHallB-C
Friday, April 24, 2009Exhibits, Posters & Learning Center Open7:00m-8:00am Morning Breakfast Video Session:
My Favorite Tricks Moderators:MarceloMartinezFerro,MD&Carroll“Mac”Harmon,MD Conv.Center–West301D
8:00am-9:30am Scientific Session: Gastrointestinal & Hepatobiliary Moderators:DouglasBarnhart,MD&GirolamoMattioli,MD Conv.Ctr–West301D
9:30am-10:00am Keynote Lecture: “What is Going on with MIS in China” Speaker:LongLi,MD Introductionby:GeorgeW.Holcomb,III,MDConv.Center–West301D
10:00am-10:30am Break Foyer10:30am-11:45am Scientific Session: All short papers
Moderators:MohamedE.Hassan,MD&ThomasH.Inge,MD,PhD Conv.Ctr–West301D
11:45am-12:30pm Scientific Session: Robotics & Emerging Technology Chair:AayedAlqahtani,MD Co-Chairs&Faculty:CelesteHollands,MD,&JohnJ.Meehan,MD Conv.Ctr–West301D
12:30pm-1:30pm Lunch (Free Lunch in the Exhibit Hall) NorthExhibitHallD-E
1:30pm-2:30pm Panel: Cutting Edge Genitourinary Reconstruction Chair:MarcA.Levitt,MD Conv.Center–West301D
2:30pm-3:00pm Break Foyer3:30pm-5:00pm SAGES/IPEG Joint Panel:
Urgent and Emergent Acute Care Problems in Pediatrics and Adults Chairs:Carroll“Mac”Harmon,MD,PhD(IPEG) &JohnSweeney,MD(SAGES) Conv.Center-TBD
5:15pm-6:15pm IPEG/SAGES Simulator Session (Non-CME) Chair:DavidvanderZee,MD Co-Chair:SanjeevDutta,MD Conv.Center–West301D
7:30pm-11:00pm Main Event & International Sing-Off CoronaRanch
Saturday, April 25, 20098:00am-9:00am General Assembly Conv.Ctr–West301D
Moderators:GeorgeW.HolcombIII,MD9:00am-10:30am Scientific Session: NOTES®,
Single Incision Access Surgery, & Urology Moderators:MuntherJ.Haddad,MBBCH,FRCS,DanielJ.Ostlie,MD,ToddA.Ponsky,MD Conv.Ctr–West301D
10:30am-11:00am Break Conv.Center–West301D11:00am-11:15am Awards (Basic Science, IRCAD, My Favorite
Trick & How I Do It) DanielJ.Ostlie,MDBennoM.Ure,MD,PhDConv.Ctr–West301D
11:15am-12:00pm Scientific Video Session: Miscilleaneous Moderators:AzadS.Najmaldin,MD&DanielJ.Ostlie,MD Conv.Center–West301D
12:00pm-12:15pm Closing Remarks Speakers:GeorgeW.Holcomb,III,MD& DanielJ.Ostlie,MDConv.Center–West301D

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 7
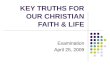
F loorplans
ENTRANCEENTRANCE
CYBERCAFE
SPEAKERREADY ROOM
SAGES + IPEGMEMBERSHIP
SAGES FOUNDATIONLOUNGE
ENTRANCE
SAGES + IPEG
HANDS ONCOURSES
ESCALATORSTO LEVEL 200
SAGESMAIN
SESSIONS(HALLS A-B)
IPEGGENERALSESSION(HALL D)
SAGES + IPEG
POSTERS ANDLEARNING CENTER
SAGES + IPEG
EXHIBITS
REGISTRATION
SKYBRIDGE
SAGESCONCURRENT
I (HALL C)
CMEKIOSKS
PHOENIX, AZPHOENIX CONVENTION CENTER - HALLS A-D
APRIL 22-25, 2009SAGES & IPEG 2009
SAGES Learning CenterAttention IPEG Attendees:visitthePediatricBasicLaparoscopicSkills(PBLS),station11.ThisstationwillvalidatethePediatricBasicLaparoscopicSkills(PBLS)Test,whichisdesignedtotestthebasictechnicalskillsnecessarytoperform pediatric minimal access surgery.
Thisskillstestisdesignedintwostages,BASIC(PBLS-1)andADVANCEDNEONATAL(PBLS-2).Whenfullyvalidated,itisourhopethattrainingcenterscanusethePBLStoestablishproficiencyinbasicskillsbeforecandidatesprogress to operations on real patients, and also as a practice platform. The IPEG Education Committee asks that all IPEG members take a moment to stop by the SAGES Learning Center and try their hands on the PBLS to help us validate this useful new tool.

8 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
12:00pm-6:00pm Location: IPEG Headquarters Hotel The Wyndham Phoenix (Salon 3-4)
IPEG Advanced Laparoscopic & Single Incision Course (Lecture)Chair: Steven S. Rothenberg, MD; Co-Chairs: Carroll “Mac” Harmon, MD, PhD & Daniel J. Ostlie, MDLab Coordinator: Todd A. Ponsky, MDDescription of Course: Thistwo-partcourseisdesignedspecificallyforpediatricsurgeonsinpracticeinterestedinmanagingmorecomplexpediatriccases,usingminimallyaccesstechniques.Pediatricsurgeonsintrainingarewelcomeaswell.Ondayone,lectureswillfocuson the management of advanced operations using the minimally invasive approach. The format will be interactive in which casepresentationsareaccompaniedbydiscussionandquestionandanswersessions.Onthenextmorning,ananimatelaboratorywillbeutilizedtodemonstratemanyofthesetechniques.Inthelaboratoryexperience,attendeeswillpracticetheskillsnecessarytoperformadvancedpediatricMISprocedures.Aftercompletingthecourse,attendeeswillbebetterprepared to recognize and manage advanced situations in pediatric thoracoscopic and laparoscopic surgery. This course will alsohelpidentifyareasinpediatricMISinwhichadditionaltrainingmaybeuseful.
Objectives:• Attendeeswillunderstandtheelements,whichcompriseadvancedpediatricMIScases• SurgeonswillbeabletopredictpotentialproblemareasduringtheperformanceofadvancedpediatricMIScases• Surgeonswillbeabletounderstandtheindications,keysteps,andpotentialproblemareasforthefollowingpediatricMISoperations:
TIME TOPIC FACULTY12:00pm-12:05pmWelcome & Introduction StevenRothenberg,MD,Carroll“Mac”Harmon,MD,PhD&DanielJ.Ostlie,MD12:05pm-12:30pmEsophageal Atresia GeorgeW.Holcomb,III,MD12:30pm-12:40pmQ & A 12:40pm-1:15pmLung Biopsy and Lobectomy StevenRothenberg,MD1:15pm-1:25pm Q & A 1:25pm-2:00pm Diaphragmatic Hernia TimothyD.Kane,MD2:00pm-2:10pm Q & A 2:10pm-2:40pm Break(Single Port Access Surgery Video) ToddA.Ponsky,MD2:40pm-3:15pm Redo Antireflux Operations Carroll“Mac”Harmon,MD,PhD3:15pm-3:25pm Q & A 3:25pm-4:00pm Duodenal Atresia, Intussusception DanielJ.Ostlie,MD4:00pm-4:10pm Q & A 4:10pm-4:45pm Spleen, Adrenal, Pancreas SanjeevDutta,MD4:45pm-4:55pm Q & A 4:55pm-5:30pm Inflammatory Bowel Disease MarcLevitt,MD5:30pm-5:40pm Q & A 5:40pm-5:55pm Hirschsprung Disease and High Imperforate Anus KeithE.Georgeson,MD5:55pm-6:00pm Q & A
Wednesday, Apr i l 22, 20097:00am-11:00am* Space is limited Location: Phoenix Convention Center – North Hall A (Section 2)
Advanced Laparoscopic & Single Incision Hands-On CourseChair: Steven S. Rothenberg, MD; Co-Chairs: Carroll “Mac” Harmon, MD, PhD & Daniel J. Ostlie, MDLab Coordinator: Todd A. Ponsky, MD *Please dress comfortably, disposable scrubs will be provided. PROCEDURES Seromuscular Colon Biopsy Gastrojejunostomy side-to-side as model of duodenoduodenostomy Nephrectomy as model of splenectomy Pulmonary Lobectomy Esophageal transaction and anastomosis Single Port Access Surgery (Cholecystectomy)FACULTYAt stations: DouglasBarnhart,MD GordonMacKinlay,MD,FRCS HolgerTill,MDSanjeevDutta,MD MarceloMartinezFerro,MD DavidvanderZee,MDThomasH.Inge,MD,PhD OliverMuensterer,MD BennoM.Ure,MD,PhdTimothyD.Kane,MD JürgenSchleef,MD,PhD Atsuyukiyamataka,MDMarcA.Levitt,MD ShawnSt.Peter,MD Floaters: MariaMarcelaBailez,MD,Carroll“Mac”Harmon,MD,PhD,KeithE.Georgeson,MD,DanielJ.Ostlie,MD, ToddA.Ponsky,MD,StevenS.Rothenberg,MD,MarkWulkan,MD
IPEG acknowledges unrestricted educational grants in support of this course and lab from Covidien, Karl Storz Endoscopy-America, Novare Surgical Systems, Olympus-Gyrus ACMI, and SurgiQuest
IPEG acknowledges contributions in-kind in support of this course from Covidien, Karl Storz Endoscopy-America, MedSurg, Novare Surgical Systems, Olympus-Gyrus ACMI, Stryker Endoscopy and SurgiQuest.
Tuesday, Apr i l 21, 2009

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 9
Thursday, Apr i l 23, 20097:45AM-8:45AM
IPEG/SAGES Joint Breakfast Video Session: Hepatobiliary and Solid OrganChairs: Kent Kercher, MD & Benno M. Ure, MD, PhDDescription:Thiscoursewillfocusonminimally-invasiveapproachestosolidorgansurgery,includingdifferencesinthemanagementofadultandpediatricdiseaseprocessesrequiringsolidorganresectionand/orablation.Thetechniquesdescribedwillincludesolidorganresectionaswellasthepotentialrolefororgan-preservingsurgery.Thecourseformatwillrevolvearoundvideosthatdescribethevarioustechniquesdiscussed.Videopresentationswillbesupplementedwithslidesintendedtoaddressboth the technical aspects of the various procedures as well as indications and outcomes.
Objectives:Attheconclusionofthiscourse,participantswillbeableto:
• Listtheindicationsandtechniquesforsplenic-preservingsurgeryinthepediatricpopulation• Describethestrategiesavailableforcombiningminimallyinvasivehepaticresectionandtumorablation• Explainthepotentialrolesforminimally-invasivesurgeryintreatingpediatricrenalandadrenaltumors• Discussthetechniquesforlivedonornephrectomyandunderstandtheimportantconsiderationsrelatedtochoosingtheappropriatekidneyfororgandonation
SCHEDULE7:45AM Introduction KentKercher,M.D.&BennoUreMD,PhD7:50AM Laparoscopic Splenectomy in Children: Total or Partial Splenectomy? JacobC.Langer,MD8:05AM Minimally Invasive Approaches to Liver Surgery: Combining Resection and Ablation Kidney and Adrenal Techniques for Laparoscopic Nephrectomy and Adrenalectomy DavidIannitti,MD8:20AM The Role for Minimally Invasive Surgery for Wilms Tumor and Neuroblastoma GordonMacKinlay,MD,FRCS8:35AM Live Donor Nephrectomy: Which Technique, Which Kidney? KentKercherMD
Panelists:Jacob C. Langer, MD -LaparoscopicSplenectomyinChildren:TotalorPartialSplenectomyDavid Iannitti, MD -MinimallyInvasiveApproachestoLiverSurgery:CombiningResectionandAblationKidneyand
Adrenal:TechniquesforLaparoscopicNephrectomyandAdrenalectomyGordon A. MacKinlay, MD, FRCS -Theroleforminimally-invasivesurgeryforWilmstumorandNeuroblastomaKent Kercher, MD - LiveDonorNephrectomy:WhichTechnique,WhichKidney
IPEG acknowledges an unrestricted educational grant in support of this session from Covidien.
8:45AM-9:00AM
Welcome Address: George W. Holcomb III, MD, 2009 IPEG President
Wednesday, Apr i l 22, 2009 5:00PM-7:00PM Exhibit Hall – Free for all IPEG & SAGES Registrants & Guests
Please join us for the…
IPEG/SAGES Welcome Exhibit Opening ReceptionIPEG and SAGES exhibits will take place at the Phoenix Convention center in North Exhibit Halls D-E. SAGES Learning center and IPEG/SAGES Posters will NOT be open until Thursday.
Date: Wednesday,April22,2009
Time: 5:00-7:00PM
Place: ExhibitHall
Fee: NoFeeforRegistrants®isteredguests
Dress: Businesscasual
Special promotions, presentations and entertainment. Great food! Open bar!
Note: Children under the age of 14 will not be permitted in the Exhibit Hall due to safety considerations.

10 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
9:00AM-10:00AM
Scientific Session: Clinical and Basic Science Moderators: Benno M. Ure, MD, PhD & Atsuyuki Yamataka, MD
9:00AM S001: Immunological Alterations After Laparoscopy In Different Age Groups In Rats, TulinOztas,MDUnalBicakci,MD,BurakTander,MD,RizaRizalar,MD,FerideDuru,MD,TuncFisgin,MD,EnderAriturk,MD,SuatHAyyildiz,MD,FeritBernay,MD,OndokuzMayisUniversity,DepartmentofPediatricSurgery
9:08AM S002: Do Gastric And Intestinal Motilities Change By Pneumoperitoneum In Young Rats?AhmetUnlu,MD,BaranTokar,MD,yaseminAydin,MDHuseyinIlhan,MDDilsadDemet,MDUmutAlici,MD,EskisehirOsmangaziUniversity,SchoolofMedicine,DepartmentofPediatricSurgeryandPhysiology,Eskisehir,Turkey
9:16AM S003: Helium Instead Of CO2 For Laparoscopic Pneumoperitoneum? - An Experimental Risk Analysis, SteffenRichter,FelixProf.Schier,ThomasHuckstadt,DevrimAksakal,DanielaKlitscher,TobiasWowra,Christoph,Prof.Kampmann,HolgerProf.Till,PediatricSurgeryUniversitalMedicalCenterLeipzig;UniversitalMedicalCenterMainz
9:21AM S004: Histological Immunohistochemical And Morphological Evaluation In Refluxing Ureters Treated With Dextranomer/Hyaluronic Acid Copolymer., SalvatoreArenaMD,CarmineFazzariMD,MariaGraziaScuderiMD,AlessandraImplatiniMD,FrancescoArenaMD,PieroAntonioNicòtinaMD,VincenzoDiBenedettoMD,UnitofPediatricSurgery-UniversityofCatania(ITALy);UnitofHistopathologicalDiagnosis-UniversityofMessina(ITALy)
9:29AM S005: Laparoscopy Induced Changes In Cardiac Parameters At Repeated IAP Elevations, ThomasHückstädt, Felix SchierPhD,DevrimAksakal,SteffenRichter,DanielaKlitscher,TobiasWowra,ChristophKampmannPhD,1DepartmentofPediatricSurgery,UniversityMedicalCenterMainz,Germany
9:37AM S006: Calorimetric Measurements During Laparoscopy In An Animal Model, DevrimAksakal,FelixSchierPhD,SteffenRichter,ThomasHückstädt,DanielaKlitscher,TobiasWowra,ChristophKampmann,1DepartmentofPediatricSurgery,UniversityMedicalCenterMainz,Germany
9:45AM S007: A Middle Fidelity Model Is Effective In Teaching And Retaining Skill Set Needed To Perform A Laparoscopic Pyloromyotomy, JosephAIoconoMD,MargaretPlymaleMS,JamesHospkinsBS,DanielDavenportPhD,UniversityofKentucky
9:50AM S008: Long-Term Outcomes Of Laparoscopic Nissen Fundoplication Versus Laparoscopic Thal Fundoplication: A Prospective Randomised Study, RainerKubiakMD,JamesAndrews,HughGrant,DepartmentofPediatricSurgery;JohnRadcliffeHospital,Oxford,U.K.
9:30AM-3:30PM
IPEG/SAGES Exhibits & Posters Open; Learning Center Open10:00AM-10:30AM
Break: Exhibits, Posters, Learning Center10:30AM-11:45AM
Scientific Session: How I Do ItModerators: Gordon A. MacKinlay, MD & C. K. Yeung, MDDescriptionThe topic is open and the objective is to have participants share their experience about how they handle cases in their MASpractice.Forexample:difficultcases,managementofcomplications,anatomicanomalies,specialmaneuvers,unusualpathologies,etc.Participantswillhave5minutestopresenttheirvideoand/orpowerpointpresentation.Theaudiencewillalsohaveanopportunitytointeractwithpresentersviaautomatedresponsesystem(ARS)
Objectives:• Topromotetheexchangeofnewideasandtechniques,thatfacilitatesthedevelopmentofminimallyaccesssurgery(MAS).
• Promotetheadvancementofminimallyaccesssurgery(MAS)inPediatrics.
• Tostimulatethedevelopmentofnewideasandtechniquesoutsidethehabitualscientificframework.
10:30AM S009: The Benefit Of Stay Sutures During Thoracoscopic Esophagoesophagostomy In Patients With Esophageal Atresia, AkihiroShimotakaharaMD,RyoSueyoshiMD,TadaharuOkazakiMD,GeoffreyJLaneMD,AtsuyukiyamatakaMD,DepartmentofPediatricGeneralandUrogenitalSurgery,JuntendoUniversitySchoolofMedicine
10:35AM S010: Laparoscopic-Assisted Repair Of Femoral Hernias In Children, ObinnaOAdibeMD,EricNHansenMD,FedericoGSeifarthMD,CathyABurnweitMD,OliverJMuenstererPhD,Children’sHospitalofAlabama,Birmingham,AlabamaandMiamiChildren’sHospital,Miami,Florida
10:40AM S011: Ureka:Umbilical Ring Easy Kannula Access - A Technique For Initial Laparoscopic Port Placement, JaredWCarlsonMD,JamesMDeCouMD,HelenDeVosChildren’sHospital,GrandRapids,Michigan,USA
10:45AM S012: Laparoscopic Pancreatic Resection In Children: How We Do It, KaushikMukherjeeMD,StephenEMorrowMD,EdmundyangMD,MonroeCarellJr.Children’sHospitalatVanderbilt
10:50AM S013: Microlaparoscopic Pyloromyotomy For Hypertrophic Pyloric Stenosis – Our Technique, SalmaiTurialMD, Ruth Freudenberger,KathrinKrause,BarbaraGoldinger,VeronikaEngel,FelixSchierMD,UniversityMedicalCentre,Departmentofpediatricsurgery,Mainz,Germany
10:55AM S014: Ligasure For The Management of Tubular Duplication Of Esophagus, HamidRezaForoutanMD,SeyedAbbasBananiMD,ShirazUniversityofMedicalSciences
Thursday, Apr i l 23, 2009

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 11
11:00AM S015: Laparoscopic Omentoplasty For Lower Extremity Lymphedema, HamidRezaForoutanBA,ShirazUniversityofMedicalSciences
11:05AM S016: Split Appendix Technique For Appendiceal Lengthening For Malone And Mitrofanoff Conduits,CurtisASheldonMD,BelindaDickieMD,ShumyleAlamMD,MarcALevittMD,CincinnatiChildren’sHospitalMedicalCenter
11:10AM S017: Preperitonescopic Bladder-Neck Suspension For The Fascia Sling Procedure In Children. GirolamoMattioliMD,PieroBuffaMD,MicheleTorreMD,VincenzoJasonniMD,DeptofSurgery,GasliniInstitute,UniversityofGenova
11:15AM S018: Laparoscopic Restorative Procto-Colectomy In Children., GirolamoMattioliMD,PaoloGandulliaMD,GiovanniRapuzziMD,VincenzoJasonniMD,GasliniInstitute-UniversityofGenova-Italy
11:20AM S019: The Endoscopic U-Sticth Technique For Primary Button Placement, NeilNixdorffBS,JenniferDilucianoRN,ToddPonskyMD,RobertParryMD,WalterChwalsMD,ScottBoulangerMD,DivisionofPediatricSurgery,DepartmentofSurgery,CaseWesternUniversitySchoolofMedicine
11:25AM S020: Laparoscopic Diagnosis And Treatment For Intestinal Malrotation In Children, SuolinLIMD,yingchaoLI,WeiliXU,DepartmentofPediatricSurgery,2ndHospitalofHebeiMedicalUniversity,Shijiazhuang,050000,China.
11:30AM S021: Mini-Invasive Treatment Of Intestinal Duplication In Newborns And Small Infants, ClaudioVellaMD, Massimo GarriboliMD,LucianoMaestriMD,GianlucaMonguzziMD,GiovannaRiccipetitoniMD,DepartmentofPediatricSurgery,Children’sHospital ;V.Buzzi.Milan,(Italy)
11:35AM S022: Fetal Endoscopic Treatment Of Congenital High Airway Obstruction (CHAOS), ShinjiroHiroseMD, Hanmin Lee MD,UniversityofCalifornia,SanFrancisco
IPEG acknowledges an unrestricted educational grant in support of this session from Stryker Endoscopy.
11:45AM-12:15PM
IPEG Presidential Address: Can Prospective Clinical Trials Be Applied to MIS in Children?
George W. Holcomb III, MDIntroduction by: Daniel J. Ostlie, MD
IPEG acknowledges our Diamond Level Donors for their support of the Presidential Address: Karl Storz Endoscopy-America and Stryker Endoscopy
12:15PM-1:15PM
Lunch Break: Exhibits, Posters, Learning Center1:15PM-2:15PM
Scientific Session: Thorax Moderators: Steven S. Rothenberg, MD & Shawn D. St. Peter, MD
1:15PM S023: Experience With Thoracoscopic Tracheal Surgery In Infants And Children, StevenSRothenbergMD,TheRockyMountainHospitalforChildren
1:20PM S024: Thoracoscopy In The Management Of Residual Disease In Patients Treated For Hodgkin lymphoma (HL) And Non-hodgkin lymphoma (NHL). A Single Centre Experience.,Eleonora1CescaMD,Paola1MidrioMD,PietroBetalliMD,AngeloRosolenMD,PiergiorgioGambaMD,DepartmentofPediatrics,PediatricSurgery,2DepartmentofPediatrics,PediatriconcologyUniversityofPadua-ITALy
1:25PM S025: New Fully Endoscopic Pectus Carinatum Repair Using Subpectoral CO2 Insufflation And Sternal Nuss Bar Compression Or Mis-Hybrid Technique, Establishing A Differential Indication. KlausSchaarschmidtBA,AndreasKolberg-SchwerdtBA,MichaelLempeBA,FrankSchlesingerMD,HeliosCenterforPediatric&AdolescentSurgery,Berlin-Buch,Germany
1:33PM S026: Noninvazive Correction Of Pectus Carinatum With Compresive Orthotic Bracing In Children: Preliminary Results Of One Instutition, GulceHakguderMD,OguzAtesMD,MustafaOlgunerMD,FezaMAkgurMD,DepartmentofPediatricSurgery,DokuzEylülUniversity,MedicalSchool,Izmir,Turkey
1:41PM S027: Thoracoscopic Repair Of Congenital Diaphragmatic Hernia in Neonates: Lessons Learned, AnneCKimMD, BenjaminSBrynerMS,BegumAkayMD,JamesGeigerMD,RonaldBHirschlMD,GeorgeBMychaliskaMD,DivisionofPediatricSurgery,UniversityofMichiganHealthSystem,AnnArbor,Michigan
1:49PM S028: Which Is The Best Vessel And Bronchial Sealing Method For PEdiatric Thoracoscopic Lobectomy? Marcelo Martinez-FerroMD,HoracioBignonMD,EnriqueBuelaMD,HospitalPrivadodeNinosFundacionHospitalaria
1:54PM S029: Thoracoscopic Lobectomy For Severe Lobar Bronchiectasis In Children, KeithAKuenzlerMD,WilliamMiddlesworthMD,StevenSRothenbergMD,MorganStanleyChildren’sHospitalofNy-Presbyterian,ColumbiaUniversityMedicalCenter,Newyork,NyandTheRockyMountainHospitalforChildren,Denver,CO
Thursday, Apr i l 23, 2009

12 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2:02PM S030: Thoracoscopic Thoracic Duct Ligation For Plastic Bronchitis, CurtSKoontzMD,S.SalmanAShawMD,ClaireSNicholasMD,MarkLWulkanMD,Children’satEgleston/EmoryUniversitySchoolofMedicine
2:07PM S031: Usage Of Simulators On Real Organic Inanimate Models For Training In Neonatal Thoracic Surgery, SoniaGuzman-MartinezMD,AlfonsoGalvan-MontañoMD,FernandoPuente-CompeanMD,SergioLanda-JuarezMD,WeimarMaldonado-ArzeMD,JoseA.AMartinez-Hernandez,FlorencioDelaConcha-BermejilloMD,GustavoJurado-BarriosMD,HospitalGeneralDr.ManuelGeaGonzalez
IPEG acknowledges an unrestricted educational grant in support of this session from Karl Storz Endoscopy-America.
2:15PM-3:00PM
Karl Storz Lecture: History & Development of a Minimally Invasive Repair for Pectus Excavatum
Speaker: Donald Nuss, MB, Ch.B., FRCS©, FACS, FAAPIntroduction by: George W. Holcomb, III, MD
3:00PM-3:30PM
Break: Exhibits, Posters, Learning Center3:30PM-5:00PM
Panel: “Showdown at the Anorectal Canal” Chair: Marc A. Levitt, MD
Panelists:Keith E. Georgeson, MD & Alberto Peña, MD
Description:This session will cover the scope of practice related to the surgical management of anorectal malformations, focusing on the technical details of the surgical approaches to its repair. The target audience is pediatric surgeons, all of whom takecareofthesetypesofpatients.Thecontentrelatestoaspecificpatientgroup–childrenbornwithcongenitalanorectal malformations. There will be discussion of controversies related to laparoscopic vs. posterior sagittal approach toanorectalmalformations,identificationofpitfalls,andhoningofknowledgeabouttechnicaldetailsrelatedtotheoperations.Theformatofthissessionwillbecase-oriented.ThesessionchairwillpresentthecasesandtheaudiencewillhaveanopportunitytoparticipateinthepaneldiscussionandexchangeofideasthroughtheQ&Asessionanduseoftheautomatedresponsesystem(ARS).
Objectives:• Understandthekeytechnicaldifferencesbetweenthelaparoscopicandposteriorsagittalapproachtoanorectal
malformations.
• Understandthekeypitfallsrelatedtoboth.
• Understandtheadvantagesanddisadvantagesofeachtechnique.
TIME TOPIC 3:30PM Introduction
3:35PM Case #1: Technical Challenges
3:45PM Panel discussion & audience participation
3:52PM Case #2: Pitfalls
4:02PM Panel discussion & audience participation
4:09PM Case #3: Potential Complications
4:16PM Panel discussion & audience participation
4:23PM Case #4: Issues of Continence
4:33PM Panel discussion & audience participation
4:40PM Case #5: Indications for Laparoscopy
4:50PM Panel discussion & audience participation
5:00PM-6:30PM
Poster Tours with Beer & Wine Moderators: Miguel A. Guelfand, MD, Timothy D. Kane, MD, Oliver Muensterer, MD, Todd A. Ponsky, MD, Klaus Schaarschmidt, MD, & Jürgen Schleef, MD
Thursday, Apr i l 23, 2009

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 13
7:00AM-8:00AM
Morning Video Session: “My Favorite Tricks”Chairs: Marcelo H. Martinez Ferro, MD & Carroll “Mac” Harmon, MD, PhDDescription: Thetopicisopenandtheobjectiveistohaveparticipantssharetheirbest“tricks”theyusewhenperformingminimalaccesssurgery(MAS).Forexample:makingknots,instrumentuse,trocarplacement,specialmaneuvers,specialpositioningofthepatientorofthesurgeon,etc.Participantswillhave3minutestopresenttheirvideoand/orpowerpointpresentation.Theaudiencewillalsohaveanopportunitytointeractwithpresentersviaautomatedresponsesystem(ARS)
Objectives • Topromotetheexchangeofnewideasandtechniques,thatfacilitatesthedevelopmentofminimallyaccesssurgery(MAS).• Promotetheadvancementofminimallyaccesssurgery(MAS)inPediatrics.• Tostimulatethedevelopmentofnewideasandtechniquesoutsidethehabitualscientificframework.
7:00AM V001: Laparoscopic Excision Of Large Hepatic Cyst ParissaTabrizianMD,AdheeshSabnisMD,PeterMidullaMD,MountSinaiSchoolofMedicine
7:05AM S032: “Lasso”-Needle For Vats-Aortosternopexy By Tracheomalacia, yuryKozlovMD,VladimirNovogilovMD,AlexeyPodkamenevMD,PavelyurkovMD,NatalyaAleynikovaMD,IrinaWeberMD,MarinaKononenko,SvetlanaKuznecova,VitalyKovalev,AndreyMachov,MunicipalPediatricHospitalIrkutsk,DepartmentofNeonatalSurgery
7:10AM S033: Laparscopic Excision Of An Endoscopically Irretrievable Colonic Polyp, PeterFitzgeraldMD,WasmiAlfadhliMD,AnaSant‘AnnaMD,McMasterChildren’sHospital,Hamilton,Ontario
7:15AM V002: Intrathoracic Kidney: MIS Approach, MarioRiquelmeMD,ArturoArandaMD,EnriqueVillarrealMD,SanJoseHospital,ITESMUniversity,Monterrey,Mexico
7:20AM S034: A Modified Nathanson Style Liver Retractor Is Able To Provide Excellent Exposure For Paediatric Laparoscopic Fundoplication. ColinLazarus,MilindChitnis,ItayiSimango,MieElsen,EasternCapePediatricSurgicalService,EastLondon,SouthAfrica.
7:25AM V003: Thoracoscopic Patent Ductus Arteriosus Ligation In Very Low Birth Weight Infants Utilizing A Novel Retractor, JeffreyRLukishMD,TheNationalNavalMedicalCenterandWalterReedArmyMedicalCenter
7:30AM S035: Cutting Balloon Dilatation Of Congenital Ureteric Strictures, BNarayanaswamyMD,LateWGManson*MD,AGWilkinsonMD,GAMacKinlayMD,RoyalHospitalforSickChildren,Edinburgh,UK
7:35AM V004: Laparoscopic Bilateral Gonadal Resection And Hernioplasty In 46 XY DSD Female Raised Patients. How We Do It. MBailezMD,ARuesmannMD,DiagnosisandTreatmentArgentineInstitute,BuenosAires,Argentina
7:40AM S036: Improvement Of Tracheal Compression After Pectus Excavatum Repair, GoMiyanoMD,RomeoCIgnacio,Jr,RobertEWoodMD,ThomasHIngePhD,CincinnatiChildren’sHospitalMedicalCenter
7:45AM S037 Minimally Invasive, Laparoscopic-Assisted, Percutaneous Liver Biopsy In Children, RichardCarterMD, Martin GrahamMD,DavidLanningMD,VirginiaCommonwealthUniversityHealthSystem
IPEG acknowledges our Diamond Level Donors for their support of this symposium: Karl Storz Endoscopy-America, Inc.
Stryker Endoscopy
8:00AM-9:30AM
Scientific Session: Gastrointestinal & Hepatobiliary Moderators: Douglas Barnhart, MD & Girolamo Mattioli, MD
8:00AM S038: Esophageal Manometry In Postoperative Achalasia Repair,MelissaLoganMD,PrithviReddyMD,RathnaAmarnathMD,JuanCampsMD,PalmettoHealthChildren’sHospital
8:08AM S039: Laparoscopic Ladd’s Procedure: Safe, With Improved Short-Term Results. RavindraKVeguntaMD, Kavitha KalvakuriMD,AmyBStanfillMD,LizabethJWallaceMS,RichardHPearlMD,UniversityofIllinoisCollegeofMedicineatPeoriaandChildren’sHospitalofIllinois,Peoria,Illinois
8:16AM S040: The Safety Of Laparoscopy In Pediatric Patients With Ventriculoperitoneal Shunts, JasonDFraserMD,PabloAguayoMD,SusanWSharpPhD,DanielJOstlieMD,GeorgeWHolcombMD,ShawnDSt.PeterMD,TheChildren’sMercyHospital
8:24AM S041: Risk Of Ventriculoperitoneal Shunt Infections After Laparoscopic Placement Of Chait Trapdoor™ Cecostomy Catheters In Children, Sanizyamout,MD,BettyJ.Huo,MD,VeetaliLiMD,MauricioAEscobarMD,MichaelGCatyMD,WomenandChildren’sHospitalofBuffalo
8:29AM S042: Laparoscopy-Assisted Stoma Closure In Children: Outcome Comparison With Conventional Open Approach, GoMiyanoMD,ManabuOkawadaMD,ToshihiroyanaiMD,TadaharuOkazakiMD,GeoffreyLaneMD,AtsuyukiyamatakaMD,JuntendoUniversitySchoolofMedicine
8:34AM S043: Laparoscopic Nissen Fundoplication In Very Small Patients, CarlosGarciaHernandezMD,LourdesCarvajalFigueroaMD,JuanCarlosDueñasRamirezMD,HospitalInfantilPrivado
8:39AM S044: Long-Term Follow-Up After Laparoscopic Gastropexy In Children With Gastric Volvulus. MarioMendoza-SagaonMD,OlivierReinbergMD,AlexandreDaraniMD,RudolfLeuthardtMD,DepartmentofPediatricSurgery,CentreHospitalierUniversitaireVaudoisandOspedaleRegionalediBellinzonaeValli.Switzerland.
Fr iday, Apr i l 24, 2009

14 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
8:44AM S045: Laparoscopic Endorectal Pull-Through For Hirschsprung’s Disease ? 10 Years Experience, ClareMReesMD,NiamhGeogheganRN,DianedeCaluweMD,SimonClarkeMD,MuntherHaddadMD,Chelsea&WestminsterNHSFoundationTrust,London,UK
8:49AM S046: Air Insufflation Of The Stomach Following Laparoscopic Pyloromyotomy Does Not Reliably Detect Perforation, StevenLLeeMD,RomanMSydorakMD,StanleyTLauMD,KaiserPermanente,LosAngelesMedicalCenter
8:54AM S047: Technical Challenges Of The Laparoscopic Approach For Patients With Anorectal Malformation And Rectobladderneck FIstula, AndreaBischoffMD,MarcALevittMD,BelindaDickieMD,AlbertoPenaMD,CincinnatiChildrenHospital
8:59AM S048: Wrap It, Stitich It And Patch It! ? A New Technique In Laparoscopic Fundoplication, AniruddhVDeshpandeMD,StephenFarrellMD,IreneTsang,AlbertShunMD,Children’sHospitalatWestmead,Sydney,Australia
9:07AM S049: New Techniques And Late Results Of Laparoscopic Subtotal >90% Splenectomy For Haemolytic Anaemia Or ITP In Children And Adolescents, KlausSchaarschmidtMD,AndreasKolberg-SchwerdtMD,MichaelLempeMD,FrankSchlesingerMD,IrinaHayekMD,JanPatino-Meyer,HeliosCenterforPediatric&AdolescentSurgery,Berlin-Buch,Germany
9:15AM S050: Laparoscopic Splenectomy And Pericardial Devascularization With Endoligature For Portal Hypertension In Children, SuolinLIMD,ZengwenyU,yinghcaoLI,DepartmentofPediatricSurgery,2ndHospitalofHebeiMedicalUniversity,Shijiazhuang,050000,China.
9:20AM S051: Laparoscopically Assisted Pull Through For Hirschprung’s Disease: The Edinburgh Experience, GillianDuthie, MaryamDavoodi,DerrickWilson-Storey,RoyalHospitalforSickChildren,Edinburgh
IPEG acknowledges an unrestricted educational grant in support of this session from Covidien.
9:30AM-10:00AM
Keynote Lecture: What is Going on with MIS in China?Speaker: Long Li, MDIntroduction by: George W. Holcomb, III, MD
IPEG acknowledges our Platinum Level Donor for their support of this lecture: Covidien
9:30AM-3:30PM
IPEG/SAGES Exhibits and Posters Open, Learning Center Open
10:00AM-10:30AM
Break: Exhibits, Posters, Learning Center10:30AM-11:45AM
Scientific Session: All Short Papers Moderators: Mohamed E. Hassan, MD & Thomas H. Inge, MD, PhD
10:30AM S052: Laparoscopic Assisted Anterior Gastropexy For Primary Gastric Volvulus In Children, PaulCyChangMD, Ming-LunyehMD,Beng-HuatLouMD,Chih-ChunChaoMD,ShinKongMemorialHospital,Taipei,Taiwan
10:35AM S053: Does The Use Of Peri-Operative Antibiotics During Minimal Access Gastrostomy Insertion Decrease The Incidence Of Wound Infection?, JuliaRFishmanMD,RameshMNatarajaMD,MHaywoodBS,JEkpeBS,GMallonRN,SAClarkeMD,MHHaddadMD,ChelseaandWestminsterHospitalNHSFoundationTrustandImperialCollegeLondon
10:40AM S054: Laparoscopy In The Management Of Abdominal Trauma In Children, AhmedRMarwanMD,GeniSmithRN,CarrolMHarmonPhD,KeithEGeorgesonMD,OliverJMuenstererPhD,Children’sHospitalofAlabama,Birmingham,Alabama
10:45AM S055: Laparoscopic Management Of The Impalpable Testes In Children. New Classification, Lessons Learned And Rare Anomalies. MohamedEHassanBA,ARMustafawiBA,AlWaslHospital,Dubai,UAE
10:50AM S056: Laparoscopic Contralateral Groin Exploration: Is It Cost Effective? StevenLLeeMD,RomanMSydorakMD,TalarTejirianMD,StanleyTLauMD,KaiserPermanente,LosAngelesMedicalCenter
10:55AM S057: Laparoscopic Pyeloplasty For Repair Of Ureteropelvic Junction Obstruction In Children, ManuelLopezMD, FrançoisMichelMD,EmmanuelleGuyeMD,FrançoisVarletPhD,DepartmentofPediatricSurgery,UniversityHospitalofSaintEtienne-France
11:00AM S058: Surgical Management Of Ovarian Disease In Infants, Children And Adolescents: A 15-Year Review,BradleySegura,MD,IndranilSauMD,SoniaPerez-Bertolez,TimothyDKane,Children’sHospitalofPittsburghofUPMC,Pittsburgh,Pennsylvania,USA
11:05AM S059: The Role Of Gasless Laparoscopy In Newborns With Necrotizing Enterocolitis: Preliminary Experience, GiovannaRiccipetitoniMD, ClaudioVellaMD,EnricaCaponcelliMD,ErnestoLevaMD,MassimoGarriboliMD,DepartmentofPediatricSurgery-Children’sHospital,V.Buzzi,Milan,(Italy)
Fr iday, Apr i l 24, 2009

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 15
Fr iday, Apr i l 24, 200911:13AM S060: New Trends In Reduction Of Intussusception In Children: A Minimal Invasive Vision, HSteyaertPhD,JLauron
MD,JSVallaPhD,LenvalFoundationforChildren
11:18AM S061: Computer-Aided Workflow Comparison Of Laparoscopic Versus Robot-Assisted Nissen Fundoplication In Infant Pigs, AlexandraKraussMS,ThomasNeumuthPhD,RobinWachowiakMD,BerndDonaubauerMD,WernerKorbPhD,OliverBurgertPhD,OliverJMuenstererPhD,UniversityofLeipzig,PediatricSurgery,InnovationCenterComputerAssistedSurgery,AnesthesiaandIntensiveCareMedicine,Leipzig,Germany;PediatricSurgery,Children’sHospitalofAlabama,Birmingham,Alabama
11:24AM S062: Laparoscopic Management Of Intussusception In Pediatric Patients, JasonDFraserMD,PabloAguayoMD,SusanWSharpPhD,DanielJOstlieMD,GeorgeWHolcombMD,ShawnDSt.PeterMD,TheChildren’sMercyHospital
11:29AM S063: Short Term Natural History Of The Standard Approaches For Gastrostomy Tube Placement In The Pediatric Patient, JasonDFraserMD,ToddAPonskyMD,PabloAguayoMD,ScottBoulangerMD,RobertParryMD,NeilNixdorfMD,JenniferDiLucianoRN,PattiSmithRN,SusanWSharpPhD,GeorgeWHolcombMD,DanielJOstlieMD,ShawnDSt.PeterMD,TheChildren’sMercyHospitalandRainbowBabiesandChildren’sHospital
11:34AM S064: Laparoscopic Total Colectomies In Children, MichelFrancois,MD,ManuelLopezMD,EmmanuelleGuyeMD,S.IrtanMD,ABonnardMD,PDeLagausiePhD,HStaeyertMD,J-SVallaPhD,MDemarcheMD,PErpicumMD,HLardyPhD,MRobertPhD,GpodevinPhD,yHélouryPhD,OReingbergPhD,PMontupetMD,HMartelliPhD,J-FColombaniMD,DWeilMD,CPiolatPhD,FVarletPhD,UniversityhospitalofSaintEtienneandGECI.France
11:45AM-12:30PM
Robotics & Emerging Technology Chairs: Aayed Alqahtani, MD, Celeste Hollands, MD, & John J. Meehan, MD
11:45AM S065: Robotic Thymectomy In Children, FranklinCMargaronMD,ClaudioOiticicaMD,DavidLanningMD,VirginiaCommonwealthUniversity
11:50AM S066: Robotic Surgery Facilitates Learning Curve In MIS, JuanCampsMD,TreyBradleyMD,PalmettoHealthChildren’sHospital
11:55AM S067: A New Platform For Basic And Advanced Endoscopic Skills Training, MLimaMD,CMelchiorri,GRuggeriMD,GDeNovi,TGarganoMD,PediatricSurgery?UniversityofBologna,ItalyFacultyofEngineering?UniversityofBologna,Italy
12:00PM S068: Development Of A New 2.4 MM Laparoscope For Microlaparoscopy In Children. SalmaiTurialMD, Miriam LuiseKnab,VeronikaEngelMD,FelixSchierMD,UniversityMedicalCentre,DepartmentofPediatricSurgery,Mainz
12:05PM S069: The “Endo-Paed-Trainer”: Why A Laparoscopic Training Device Is Indispensable In Pediatric Surgery, MarkusDuerschMD,BertramReingruberMD,Departmentofpediatricsurgery-Regensburg
12:10PM S070: A Novel Transoral Esophageal Anastomosis Device (EAD): Toward A NOTES Approach To Esophageal Atresia Repair, ZacharyJKastenbergBS,PabloGarciaMS,SanjeevDuttaMD,MultidisciplinaryInitiativeforSurgicalTechnologyResearch-StanfordUniversity/SRIInternational,PaloAlto,CA,USA
12:15PM S071: Comparative Performance Evaluation Of Force Triverse? ModeE vs. Starndard Electrosurgical Modes, HannahKSwayzeMD,ArlenKWard,MyronSt.LouisMD,DavidTashjianMD,KevinPMoriartyMD,DepartmentofSurgery,BaystateChildren’sHospital,PioneerValleyLifeSciencesInstitute,Springfield,Massachusetts
12:20PM S072: Serial Intestinal Lengthening Using A Re-Deployable Intraluminal Spring Device, ShantShekherdimianMD, MohanchandraPandurangaPhD,GregoryCarmanPhD,JamesDunnMD,UniversityofCalifornia,LosAngeles
12:25PM V005: Robotic Resection Of A Mediastinal Neuroblastoma, JohnJMeehanMD,SeattleChildren’sHospital
12:30PM-1:30PM
Don’t forget: Friday lunch in the Exhibit Hall, free for all IPEG & SAGES Scientific Session registrants!

16 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
Fr iday, Apr i l 24, 20091:30PM-3:00PM
Panel: Cutting Edge Genitourinary ReconstructionChair: Marc A. Levitt, MD
Description:This session will describe what the latest surgical options are in the area of complex genitourinary anomalies including ureteral,bladder,vaginal,andcloacalreconstructions.AdvancedtechniquesincludingMIS,tissueengineering,andoperativedetails will form the basis of the presenations, and the panel will then be presented with challenging cases for discussion.
Objectives:• Tounderstandthelatestadvancesinureteralreconstruction.
• Tounderstandthelatestadvancesinvaginalreplacements.
• Tounderstandthelatestadvancesinbladderaugmentation.
• Tounderstandthelatestadvancesincloacalmalformationreconstruction.
TIME TOPIC FACULTY1:30PM What’s New in Vaginal Replacement Surgery MariaMarcelaBailez,MD
Q & A /Discussion
1:50PM What’s New in Bladder Surgery StevenG.Docimo,MD
Q & A /Discussion
2:10PM What’s New in Ureteral Surgery AlbertoPeña,MD
Q & A /Discussion
2:30PM What’s New in Cloacal Reconstruction Surgery C.K.yeung,MD
Q & A /Discussion
3:00PM-3:30PM
Break: Exhibits, Posters, Learning Center3:30PM-5:00PM
SAGES/IPEG Joint Panel: Urgent and Emergent Acute Care Problems in Pediatrics and Adults Chairs: John Sweeney, MD (SAGES) & Carroll “Mac” Harmon, MD, PhD (IPEG)
There are many general and pediatric surgeons who treat pediatric and adult patients with complex surgical problems. The topicscoveredinthisjointSAGES/IPEGactivitywilloutlinethedifferencesinpresentation,diagnosisandmanagementofseveral complex surgical problems in pediatric and adult patients.
Objectives:Attheconclusionofthissession,participantswillbeableto:
• Describethedifferencesinthepresentation,diagnosis,andtreatmentofacuteappendicitis,intestinalmalrotation,andintussusception in pediatric and adult patients
• Reviewtheroleoflaparoscopyinthetreatmentofsmallbowelobstruction• Identifymethodsforimprovingtheearlydetectionofintestinalischemia• Discusscurrentrecommendationsfornon-operativeandoperativemanagementofacutediverticulitis
SCHEDULE3:30PM Introduction JohnF.Sweeney,MD&Carroll“Mac”Harmon,MD,PhDDiagnosis and Management in Pediatric and Adult Patients3:35PM Acute Appendicitis ShawnD.St.Peter,MD3:45PM Intestinal Malrotation StevenS.Rothenberg,MD3:55PM Intussusception KeithGeorgeson,MD4:05PM Discussion Other Emergent Problems4:15PM Small Bowel Obstruction: Is There a Role for Laparoscopy? VadimSherman,MD4:25PM Intestinal Ischemia: Tips for Intervening Before It’s Too Late S.ScottDavis,MD4:35PM Diverticulitis: Current Management and Recommendations for Surgical Intervention EdwardP.Dominguez,MD4:45PM Discussion 4:55PM Closing Remarks JohnF.Sweeney,MD&Carroll“Mac”Harmon,MD,PhD

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 17
Fr iday, Apr i l 24, 20095:15PM-6:15PM
IPEG/SAGES Simulator Session Location: West 301D Ballroom
Chairs: Sanjeev Dutta, MD & David van der Zee, MD
Course Description:Simulationasamodalityfortrainingistakingcenterstageinsurgicaleducation.Part-tasktrainersandvirtualrealitysimulatorsarebecomingmoreprevalentfortechnicalskillstraining.Thiscoursefamiliarizesattendeestotherangeofcommerciallyavailablesimulators,andgivesanoverviewoftheroleoftechnicalskillssimulationinthesurgicaleducationcurriculum.
Learning Objectives:• Tobecomefamiliarwithavarietyofsurgicalsimulatortechnologiescurrentlyavailablecommercially.
• Tounderstandtheroleofsimulationintrainingsurgicaltechnicalskillswithrespecttopractice,performancefeedback,and assessment.
5:15PM Introduction DavidvanderZee,MD
5:15PM Industry Presentations Haptica,Simbionix,&SurgicalScience
5:30PM State-of-the-Art Lecture: “Skills Simulation: The Practice Arena before the Performance Arena” GaryDunnington,MD,FACS
6:00PM Roundtable Discussions SanjeevDutta,MD
IPEG acknowledges unrestricted educational grants in support of this session from Hapatica, Simbionix and Surgical Science.
7:30PM-11:00PM
IPEG/SAGES Main Event & International Sing-Off Viva La SAGES! Viva La IPEG! Gala An Evening at Corona Ranch Dinner and Sing-OffDate: FridayEvening,April24,2009
Place: CoronaRanch
Time: 7:30-11:00PM
Dress: Casual(reallycasual!)
Fee: IncludedinRegistrationforSAGESSuperPass(OptionA),IPEGmeeting®isteredguests.
Ticketed Event
The evening will conclude with the SAGES International Sing-Off.
Shuttles begin departing at 7:15 PM in front of the Sheraton Phoenix Downtown, Hyatt Regency Phoenix and Wyndham hotels. Buses will circle all evening until the event ends.
CME & Evaluation FormsIPEG Registrants, please complete the IPEG CME & Evaluation form and turn in at the IPEG Membership Booth to have your CME certificate mailed to you after the meeting.
IPEG members who have also registered for the SAGES meeting and need to claim credits, please complete the SAGES CME Worksheet included in the SAGES final program and turn in at any of the SAGES CME drop boxes.
Please allow 4-6 weeks for processing for all CME requests.
COPYRIGHTThe program and talks presented at the 2009 IPEG meeting are copyrighted products of the International Pediatric Endoscopic Group. Any reproduction or rebroadcasting without the express written consent of IPEG is prohibited.

18 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
9:30AM-1:30PM
Posters and Learning Center Open (Exhibits CLOSED)8:00AM-9:00AM
IPEG General Assembly – All IPEG Members Encouraged to Attend!Moderator: George W. Holcomb, III, MD
9:00AM-10:30AM
Scientific Session: NOTES®, Single Incision Access Surgery, & UrologyModerators: Munther J. Haddad, MBBCH, FRCS, Daniel J. Ostlie, MD, & Todd A. Ponsky, MD
9:00AM S073: Treatment Of Ureteropelvic Junction Obstruction In Children With A Laparoscopic Vascular Sling Technique And Pelvic Pexy: A Case Series,KrisMilbrandtMD,SarahWongBS,AnthonyCookMD,AlbertaChildren’sHospital,Calgary,Alberta,Canada
9:05AM S074: Functional Outcome After Laparoscopic Dismembered Pyeloplasty In Children, PhilippOSzavayMD, Tobias LuithleMD,JoergFuchsMD,DepartmentofPediatricSurgeryandUrology,Children’sHospital,UniversityofTuebingen
9:10AM S075: Is Balloon Burst Pyeloplasty A Useful Alternative To Open Or Laparoscopic Pyeloplasty? BomaAdikibiMD, RachelMHallMD,A.GrahamWilkinsonMD,GordonA.MacKinlayMD,RoyalHospitalforSickChildren,Edinburgh.
9:15AM S076: Laparoscopic Maneuver For Orchidopexy In High Intra-Abdominal Testes When Cremasteric Artery Is Present: A Technical Report, ClaudioDeCarliMD,MichaelLeonardMD,MarcosBettolliMD,LuisGuerraMD,UniversityofOttawa,Children’sHospitalofEasternOntario.DeptofSurgery-DivisionsofPediatricUrologyandGeneralSurgery
9:20AM S077: Laparoscopic Extravesical Reimplantation For Vesico-Ureteral Reflux. ManuelLopezMD,EmmanuelleGuyeMD,MichelFrançoisMD,FrançoisVarletPhD,DepartmentofPediatricSurgery,UniversityHospitalofSaintEtienne-France
9:25AM S078: Our Experience Of A Single Port Laparoscopic Appendectomy In Children, TakashiNogamiBA,MakotoyagiBA,yukoUdatsuBA,HidekiyoshidaMD,yujiMorishitaMD,HitoshiShiozakiMD,HarumasaOhyanagiMD,DivisionofPediatricsurgery,DepartmentofSurgery,KinkiUniversityofMedicine
9:30AM S079: Endoscopic Treatment Of Duodenal Webs On Pediatric Patients,F.yankovicMD,F.SaituaMD,CCastilloMD,CnavarreteMD,LuisCalvoMackennahospital,ClinicaAlemanadesantiago
9:35AM S080: Rigid NOTES: The Transurethral Approach In Female Piglets, MartinLMetzelderMD,JoachimFKueblerMD,GertrudVietenPhD,JanGosemannMD,BennoMUrePhD,DepartmentofPediatricSurgery,HannoverMedicalSchool,Hannover,Germany
9:43AM S081: Scarless Abdominal Surgery: Single Incision Laparoscopic Splenectomy, Cholecystectomy, And Appendectomy SanjeevDuttaMD,DivisionofPediatricSurgery,LucilePackardChildren’sHospital,StanfordUniversity
9:48AM S082: Experience With Modified Single Port Laparoscopic Procedures (SPA) In Children, StevenSRothenbergMD, TheRockyMountainHospitalforChildren
9:53AM S083: Preliminary Experience With Single Incision Laparoscopic Surgery In Children, ToddAPonskyMD,ScottBoulangerMD,WalterChwalsMD,EdwardBarksdaleMD,RobertParryMD,RainbowBabiesandChildren’sHospital,CaseWesternReserveUniversity
10:01AM S084: Transumbilical Laparoscopic Assisted Appendectomy (TULAA) In Children - First Experience. RobertBergholzMD,ThomasKrebsMD,KatharinaWenkeMD,AltonaChildren’sHospital,UKEMedicalSchool,UniversityofHamburg,Germany
10:06AM S085: A Homemade Grasper For “Single Conventional Port” Laparoscopic Appendectomy: Swing Poylpropylene Suture Introduced Through A Single Vascular Needle,FezaMAkgurMD,MustafaOlgunerMD,GulceHakguderMD, OguzAtesMD,DepartmentofPediatricSurgery,DokuzEylulUniversity,Schoolofmedicine,Izmir,Turkey
10:11AM V006: Single Site Laparoscopic Splenectomy In A Child, ToddAPonskyMD,ScottBoulangerMD,RainbowBabiesandChildren’sHospital,CaseWesternReserveUniversity
10:16AM V007: Modified Single Port Cholecystectomy In A Child, StevenSRothenbergMD,TheRockyMountainHospitalForChildren
IPEG acknowledges an unrestricted educational grant in support of this session from Karl Storz Endoscopy-America.
10:30AM-11:00AM
Break: Posters and Learning Center Open (Exhibits CLOSED)
Saturday, Apr i l 25, 2009

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 19
Saturday, Apr i l 25, 200911:00AM-11:15AM
IPEG Awards SessionModerators: Daniel J. Ostlie, MD & Benno M. Ure, MD, PhD
11:15AM-12:00AM
Scientific Video Session: MiscellaneousModerators: Azad S. Najmaldin, MD & Daniel J. Ostlie, MD
11:15AM V008: Laparoscopic Repair Of Traumatic Abdominal Wall Hernia From Handlebar Injury, ErinERowellMD, AnthonyCChinMD,Children’sMemorialHospital
11:20AM V009: Thoracoscopic Repair Of An H-Type TEF In An Year Old Female, StevenSRothenbergBA,KristenShipmanBA,TheRockyMountainHospitalforChildren
11:25AM V010: Extraperitoneal Splenopexy For Wandering Spleen, EarlCDowneyBA,UniversityofUtahDepartmentofSurgery,DivisionofPediatricSurgery
11:30AM V011: Laparoscopic Treatment Of A Rectovaginal Fistula. Feasibility And Technical Details Of A Rare Anorectal Malformation.(ARM), MBailezMD,EPazMD,VDibenedettoMD,PediatricSurgeryGarrahanChildren’sHospital.BuenosAires.Argentina
11:35AM V012: Laparoscopic Repair Of A High Urogenital Sinus And Duplex Vagina, JoergFuchsMD,GuidoSeitzMD,MonikaSchroederMD,JuergenFSchaeferMD,StevenWWarmannMD,UniversityChildren’sHospital,DepartmentofPediatricSurgery,Tuebingen,Germany
11:40AM V013: Laparoscopic Removal Of A Gastric Trichobezoar In A Pediatric Patient, CharlesMLeysMD,JasonDFraserMD,ShawnDSt.PeterMD,TheChildren’sMercyHospital,KansasCity,MO
11:45AM V014: Laparocopic Cholecystectomy And Concomitant Splenectomy – Four Working Ports And A 5 MM Bipolar Sealer. MBailezMD,ARuesmannMD,NTamburriMD,DiagnosisandTreatmentArgentineInstitute,BuenosAires,Argentina
11:50AM V015: Laparoscopic Dismembered Pyeloplasty And Repair Of An Infundibulo-Pelvic Stenosis In A Horseshoe Kidney, FlorianObermayrMD,PhilippOSzavayMD,JoergFuchsMD,DepartmentofPediatricSurgery,Children’sHospital,UniversityofTuebingen
11:55AM V016: Laparoscopic Inguinal Hernia Inversion And Ligation In Female Children, AaronMLipskarMD,SamuelZSofferMD,RichardDGlickMD,NelsonGRosenMD,StephenEDolginMD,AndrewRHongMD,SchneiderChildren’sHospital,NorthShore-LongIslandJewishHealthSystem
12:00PM-12:15PM
Closing RemarksGeorge W. Holcomb, III, MD & Daniel J. Ostlie, MD
IRCAD AwardAsaresultofagenerousgrantprovidedbyKarlStorzEndoscopy,theBestresidentabstract
presenterwillbeselectedbytheIPEGExecutiveCommitteetoreceivethe2009IRCADaward.
TheawardrecipientwilltraveltoStrasbourg,Francetoparticipateinacourseinpediatric
minimallyinvasivesurgeryattheworldfamousEuropeanInstituteofTelesurgery.Thiscenter,
onthecampusoftheUniversityofStrasbourg,isastate-of-the-artinstituteforinstructioninall
aspects of endoscopic surgery that is now providing a series of courses in pediatric surgery.
Best Basic Science AwardTheBestBasicScienceAbstractAwardwillbeacashprizeofUS$1000tobepresentedduring
theThursdaysessionoftheAbstractPresentations.TheProgramCommitteewillselectthe
Awardrecipient.TheIPEGExecutiveCommitteeiscommittedtoeducationandfeelsthisis
a very concrete way to express that commitment.

20 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 IPEG FacultyAayad Alqahtani, MD:Riaydh,SAUDIARABIA
Maria Marcela Bailez, MD:BuenosAires,ARGENTINA
Douglas C. Barnhart, MD: SaltLakeCity,Utah,USA
Steven Docimo, MD: Pittsburgh,Pennsylvania,USA
Sanjeev Dutta, MD, FRCS: Stanford,CaliforniaUSA
Keith E. Georgeson, MD: Birmingham,Alabama,USA
Miguel A. Guelfand, MD: Santiago,CHILE
Munther J. Haddad, MBBCH, FRCS: London,England,UNITEDKINGDOM
Carroll “Mac” Harmon, MD, PhD: Birmingham,Alabama,USA
Mohamed Hassan, MD: Dubai,UnitedArabEmirates
George W. Holcomb III, MD:KansasCity,Missouri,USA
Celeste Hollands, MD: Mobile,Alabama,USA
David Iannitti, MD: Charlotte,NorthCarolina,USA
Thomas H. Inge, MD, PhD:Cincinnati,Ohio,USA
Timothy D. Kane, MD: Pittsburgh,Pennsylvania,USA
Kent Kercher, MD: Charlotte,NorthCarolina,USA

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 21
2009 IPEG FacultyJacob C. Langer, MD: Toronto,Ontario,CANADA
Marc A. Levitt, MD: Cincinnati,Ohio,USA
Gordon A. MacKinlay, MD, FRCS: Edinburgh,Scotland,UNITEDKINGDOM
Marcelo H. Martinez Ferro, MD:Olivos,BuenosAires,ARGENTINA
Girolamo Mattoli, MD: Genova,Italy
John Meehan, MD: Seattle,Washington,USA
Oliver Muensterer, MD: Birmingham,Alabama,USA
Azad S. Najmaldin, MD, FRCS: Leeds, England,UNITEDKINGDOM
Daniel J. Ostlie, MD: KansasCity,Missouri,USA
Todd A. Ponsky, MD: ClevelandHeights,Ohio,USA
Steven S. Rothenberg, MD: Denver,Colorado,USA
Klaus Schaarschmidt, MD: Berlin,GERMANy
Jürgen Schleef, MD: Trieste,ITALy
Shawn D. St. Peter, MD: KansasCity,Missouri,USA
Holger Till, MD: Leipzig,GERMANy
Benno M. Ure, MD, PhD: Hannover, GERMANy

22 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 IPEG FacultyDavid C. van der Zee, MD, PhD: Utrecht,TheNETHERLANDS
Mark L. Wulkan, MD: Atlanta,Georgia,USA
Atsuyuki Yamataka, MD: Tokyo,JAPAN
C.K. Yeung, MD: HongKong,CHINA

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 23
IPEG Faculty Disc losuresName Nothing to Disclose Company Received Role
AayedAlqahtani,MD NothingtoDisclose
MariaMarcelaBailez,MD NothingtoDisclose
DouglasBarnhart,MD NothingtoDisclose
StevenG.Docimo,MD NothingtoDisclose
GaryL.Dunnington,MD NothingtoDisclose
SanjeevDutta,MD,FRCS Novare ConsultingFee Proctoring
KeithE.Georgeson,MD NothingtoDisclose
MiguelA.Guelfand,MD NothingtoDisclose
MuntherJ.Haddad,MBBCH,FRCSNothingtoDisclose
CarrollM.Harmon,MD,PHD StrykerEndo AdvisoryCommittee
MohamedHassan,MD NothingtoDisclose
GeorgeW.HolcombIII,MD NothingtoDisclose
CelesteHollands,MD NothingtoDisclose
DavidIannitti,MD Inneroptic ConsultingFee/ResearchGrant Consulting/PI Microsulis ConsultingFee/ResearchGrant Consulting/PI Valleylab ConsultingFee/ResearchGrant Consulting/PI
ThomasHInge,MD,PhD. Ethicon Grantfee Consulting
TimothyD.Kane,MD NothingtoDisclose
KentW.Kercher,MD Ethicon Honoraria Speaking W.L.Gore Honoraria Speaking
JacobLanger,MD NothingtoDisclose
MarcA.Levitt,MD NothingtoDisclose
LongLi,MD NothingtoDisclose
GordonA.MacKinlay,MD NothingtoDisclose
MarceloH.MartinezFerro,MD NothingtoDisclose
GirolamoMattioli,MD NothingtoDisclose
JohnJ.Meehan,MD Intuitive Honoraria TestingEquipment
OliverJ.Muensterer,MD NothingtoDisclose
AzadS.Najmaldin,MD,FRCS NothingtoDisclose
DonaldNuss,MB Biomet-Microfixation Royalty Contractexpiresin2008
DanielJ.Ostlie,MD NothingtoDisclose
AlbertoPena,MD NothingtoDisclose
ToddA.Ponsky,MD Novare Honoraria Speaking
StevenRothenberg,MD KarlStorz ConsultingFee
KlausSchaarschmidt,Prof NothingtoDisclose
JürgenSchleef,MD NothingtoDisclose
ShawnD.St.Peter,MD NothingtoDisclose
HolgerTill,MD NothingtoDisclose
BennoM.Ure,MD,PhD. Aesculas Honoraria Workshop
DavidvanderZee,MD NothingtoDisclose
MarkL.Wulkan,MD NothingtoDisclose
Atsuyukiyamataka,MD NothingtoDisclose
C.K.yeung,Prof NothingtoDisclose

24 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
Name Nothing to Disclose Company Received Role
ObinnaOAdibe,MD NothingtoDisclose
BomaAdikibi,MD NothingtoDisclose
DevrimAksakal NothingtoDisclose
SalvatoreArena,MD NothingtoDisclose
MMBailez,MD NothingtoDisclose
RobertBergholz,MD NothingtoDisclose
UnalBicakci,MD NothingtoDisclose
AndreaBischoff,MD NothingtoDisclose
JuanCamps,MD NothingtoDisclose
JaredWCarlson,MD NothingtoDisclose
RichardCarter,MD NothingtoDisclose
PaulCyChang,MBChB NothingtoDisclose
AnthonyCChin,MD NothingtoDisclose
ClaudioFabianDeCarli,MD NothingtoDisclose
AniruddhVDeshpande,MS, NothingtoDiscloseDNB,MCh
BelindaDickie,MD NothingtoDisclose
EarlCDowney,MD NothingtoDisclose
GillianDuthie,MBChB,MRCS NothingtoDisclose
SanjeevDutta,MD Novare ConsultingFee Speakingand/orTeaching
JuliaRFishman,MD NothingtoDisclose
PeterFitzgerald,MD NothingtoDisclose
HamidRezaForoutan,Dr NothingtoDisclose
HamidRezaForoutan,MD NothingtoDisclose
MichelFRANCOIS,MD NothingtoDisclose
JasonDFraser,MD NothingtoDisclose
JoergFuchs,MD NothingtoDisclose
PiergiorgioGamba,MD NothingtoDisclose
CarlosGarciaHernandez,MD NothingtoDisclose
SoniaGuzman-Martinez,MD NothingtoDisclose
GulceHakguder,MD NothingtoDisclose
MohamedEHassan,MD,PhD NothingtoDisclose
ShinjiroHirose,MD NothingtoDisclose
ThomasH¸ckst‰dt NothingtoDisclose
JosephAIocono,MD NothingtoDisclose
AnneCKim,MD NothingtoDisclose
CurtSKoontz,MD NothingtoDisclose
yuryKozlov,MD NothingtoDisclose
AlexandraKrauss,MS NothingtoDisclose
RainerKubiak,MD NothingtoDisclose
KeithAKuenzler,MD NothingtoDisclose
ColinLazarus NothingtoDisclose
StevenLLee,MD NothingtoDisclose
CharlesMLeys,MD NothingtoDisclose
SuolinLI,MD NothingtoDisclose
AaronMLipskar,MD NothingtoDisclose
ManuelLopez,MD NothingtoDisclose
JeffreyRLukish,MD NothingtoDisclose
FranklinCMargaron,MD NothingtoDisclose
MarceloMartinez-Ferro,MD NothingtoDisclose
IPEG Presenter Disc losures

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 25
Name Nothing to Disclose Company Received Role
AhmedRMarwan,MD NothingtoDisclose
GirolamoMattioli,MD NothingtoDisclose
MarioMendoza-Sagaon,MD
JohnJMeehan,MD IntuitiveSurgical Honorarium Speakingand/orTeaching
MartinLMetzelder,MD NothingtoDisclose
BrettMichelotti,BS NothingtoDisclose
GoMiyano,MD NothingtoDisclose
KaushikMukherjee,MD NothingtoDisclose
BommayyaNarayanaswamy,MS,NothingtoDiscloseFRCS(Paed)
NeilNixdorff,BS NothingtoDisclose
TakashiNogami,PhD NothingtoDisclose
FlorianObermayr,MD NothingtoDisclose
ToddAPonsky,MD Novare Honorarium Sugiquest Honorarium Speakingand/orTeaching Covidien Honorarium Speakingand/orTeaching Novare Honorarium Speakingand/orTeaching
ClareMRees,MD NothingtoDisclose
GiovannaRiccipetitoni,MD NothingtoDisclose
SteffenRichter NothingtoDisclose
MarioRiquelme,MD NothingtoDisclose
StevenSRothenberg,MD Covidien ConsultingFee Consulting Storz ConsultingFee Consulting Covidien ConsultingFee Consulting Storz ConsultingFee Consulting Covidien ConsultingFee Speakingand/orTeaching Storz ConsultingFee Consulting Covidien ConsultingFee Speakingand/orTeaching Storz ConsultingFee Consulting
FranciscoSaitua,MD NothingtoDisclose
KlausSchaarschmidt,MD NothingtoDisclose
KlausSchaarschmidt,Prof.MD, NothingtoDisclosePhD
AkihiroShimotakahara,MD NothingtoDisclose
AmyBStanfill,MD NothingtoDisclose
HSteyaert,PhD NothingtoDisclose
PhilippOSzavay,MD NothingtoDisclose
ParissaTabrizian,MD NothingtoDisclose
BaranTokar,MD NothingtoDisclose
SalmaiTurial,MD NothingtoDisclose
SarahWong,BS NothingtoDisclose
SaniZyamout,MD NothingtoDisclose
IPEG Presenter Disc losures

26 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Oral AbstractsS001IMMUNOLOGIC ALTERATIONS AFTER LAPAROSCOPY IN DIFFERENT AGE GROUPS IN RATS, TulinOztasMD,UnalBicakciMD,BurakTanderMD,RizaRizalarMD,FerideDuruMD,TuncFisginMD,EnderAriturkMD,SuatHAyyildizMD,FeritBernayMD,OndokuzMayisUniversity,DepartmentofPediatricSurgeryPurpose: To compare alterations of immun responses of endoscopic and open accesses in rats of different age groups. Methods:24Wistarratsweredividedinto3groups[infant(n=8),prepubertal(n=8),adult(n=8)][subgroups:laparoscopy(n=4),laparotomy(n=4)].Lymphocytesubgroups(CD4-CD25,CD4/CD8a)were measured . Results:TheCD4/CD8aratiowasdepressedinallagegroupsofopen access; but in endoscopy group of infants and adults, this ratio was elevated, indicating that the tissue damage is obvious afterlaparatomy(p>0.05).Inadultagesubgroups,theCD4-CD25depressionwasmoreinopenaccessgroupaftersurgery(p>0.05),indicatingthattheactiveTlymphocytsweredepressed.CD8ameasurements were increased in open surgery group of all ages, theyweredecreasedafterendoscopy(p>0.05).
IPreop/Postop PPreop/Postop APreop/PostopEndoCD4-CD25 1.36/1.23 0.12/0.67 1.39/0.93EndoCD4/CD8a 2.27/2.67 2.69/2.27 1.62/1.68OpenCD4-CD25 1.40/1.47 1.36/2.33 4.00/1.99OpenCD4/CD8a 2.90/2.28 2.95/1.35 1.39/1.05
I:Infant;P:Prepubertal;A:Adult Conclusion: Althoughstatisticallynotsignificant,endoscopicsurgery seems to cause less tissue damage compared to open access especially in adult rats. Laparoscopy may have minimal immun response in all age groups.
S002DO GASTRIC AND INTESTINAL MOTILITIES CHANGE BY PNEUMOPERITONEUM IN YOUNG RATS?,AhmetUnluMD,BaranTokarMD,yaseminAydinMD,HuseyinIlhanMD,DilsadDemetMD,UmutAliciMD,EskisehirOsmangaziUniversity,SchoolofMedicine,DepartmentofPediatricSurgeryandPhysiology,Eskisehir,TurkeyPurpose:Inliterature,thedataareverylimitedanditisstillnotclear whether a pneumoperitoneum induces significant changes in gastricandintestinalmotilitiesinchildren.Inthisexperimentalstudyon rats, the aim was to determine the effect of pnuemoperitonium on gastric and intestinal motility for both pediatric and adult ages. Methods:Of4groups,group1and2werepediatricagegroups;ingroup1(n=8),pnuemoperitoniumwasapplied,ingroup2(n=7)laparotomywasperformed.Inadultagegroups,ingroup3(n=10),pnuemoperitoniumwasapplied,ingroup4(n=10)laparotomywasperformed. The duration of the procedures was one hour for all groups.Carbondioxideinsufflationwith5mmHgpressure-0.5ml/minflowwasappliedwithThermoflator(Karl-Storz,Germany).Postoperativegastricandintestinalmotilitystudieswereperformed.AcetylcholineandKCL(between10-8-10-3mMdoses)contractionresponseswererecordedbyIsometricTransducer(Biopac,USA)andanalyzedwithDataAcquisitionAnalyzingSystem(MP100Biopac,USA).Results: The lowest mean contraction responses were obtained in group 1 for both gastric and intestinal studies, but when all groups were compared statistically, the difference wasnotsignificant.Conclusion:Thisstudymaysuggestthatpnuemoperitonium does not cause a significant change in gastric and intestinal motilities in children comparing with adults and pediatriccaseshavinglaparotomy.Ournextstepistodesignnewexperimental and clinical motility studies comparing different ages including newborns, different pressures, operation and pnuemoperitonium durations, and the effect of different surgical procedures in children.
S003HELIUM INSTEAD OF CO2 FOR LAPAROSCOPIC PNEUMOPERITONEUM? - AN EXPERIMENTAL RISK ANALYSIS, SteffenRichter,FelixProf.Schier,ThomasHuckstadt,DevrimAksakal,DanielaKlitscher,TobiasWowra,ChristophProf.Kampmann,HolgerProf.Till,PediatricSurgeryUniversitalMedicalCenterLeipzig;UniversitalMedicalCenterMainzCarbondioxideisthecommonusedgasforlaparoscopy.InertgaseslikeHeliumarediscussedasalternatives,especiallytopreventlokaltissue acidosis, decreased postoperative tumor growth and less spreadoftumorstoportsites.1,2Duringlaparoscopicprocedures
gas bubbles caused by micro vessel injuries could be detected in the right ventricle by echocardiographic examination.3 AIM:Evaluationofcardiopulmonaryreactionswhileeithercarbondioxide or helium was injected into the venous system of young piglets. METHODS: Tenmalepigletsaged5to7weeks(meanbodyweight10,9kg)wereanesthesizedbyintravenousinfusionofpentobarbitalandfentanylandapressure-controlledventilationwasperformed.Three piglets received a carbon dioxide, three piglets a helium and three piglets first a carbon dioxide and then a helium gas embolism. Thegaswasinjectedrapidlyintotheinferiorcavavenewith2mL/kgBWinallcases.Onepigletreceivedalternatelycarbondioxide(3times,9mL)andhelium(2times,first3mLandthen9mL)gasembolism.Heartrate(HR),meanarterialpressure(MAP),meanpulmonarypressure(PAP)andendtidalcarbondioxide(etCO2)weremeasured continuously since embolism start until 20 minutes follow up(15minutesduringalternatebolus). (animalrightscommitteeapprovedstudy1.5177-07/051-6) RESULTS: AllanimalssurvivedInthecarbondioxidegroup.AfterinitialincreaseofHRanddecreaseofMAPandetCO2baselinelevelswerereachedwithin20minutes.Intheheliumgrouponepigletdiedattwoandoneat14minutesafterembolism.Inthemixedgroupallanimalssurvivedcarbondioxideembolismsimilarlikeinthefirstgroup. Two of these died in the first minutes of helium embolism. None of the helium embolism piglets reached baseline levels within 20minutes.DecreaseinHRandMAPoccurredjustbeforedeath.Theanimalwithalternatedembolismsurvivedallgasapplikations.Duringheliumembolismsignificantgreatercardiopulmonalreactions with prolonged readaption were monitored. CONCLUSION: Helium embolism is associated with greater cardiopulmonary reactions in comparison to carbon dioxide embolism and probably often leads to a letal outcome. The readaptation after a gas embolism with helium needs more time in comparison to carbon dioxide. 1DähnS,etal.Surg.Endosc.2005;19:65-70-2NeuhausSJ,etal.Surg.Endosc.2001;15:553-60-3SchmandraTC,etal.Br.J.Surg.2002;89:870-6
S004HISTOLOGICAL, IMMUNOHISTOCHEMICAL AND MORPHOLOGICAL EVALUATION IN REFLUXING URETERS TREATED WITH DEXTRANOMER/HYALURONIC ACID COPOLYMER., SalvatoreArenaMD,CarmineFazzariMD,MariaGraziaScuderiMD,AlessandraImplatiniMD,FrancescoArenaMD,PieroAntonioNicòtinaMD,VincenzoDiBenedettoMD,UnitofPediatricSurgery-UniversityofCatania(ITALy);UnitofHistopathologicalDiagnosis-UniversityofMessina(ITALy)IntroductionEndoscopicinjectionofabulkingagentisconsideredan alternative to conservative medical treatment and sugical ureteral reimplantationinpatientaffectedbyvesicoureteralreflux(VUR).Dextranomer/Hyaluronicacid(Dx/HA)copolymerisconsideredidealfortreatingVURbecauseitisbiocompatible,biodegradeble,nomigratoryandshowsnosignsofmutagenesis.Dx/HAtreatmentisknowntobeassociatedwithagranulomatousinflammatoryreaction,subsequentlyreplacedbyfibrosis.Aimwastoevaluatehistologicalchanges,immunolocalizeCD68positivecells,tryptasemast cells and myofibroblasts and to perform a morphological analysisinrefluxingureterstreatedwithDx/HA. Materials and methodsWeperformedanhistologcal,immunohistochemicalandmorphologicalanalysisin22Dx/HAtreatedrefluxingureteralendingsandcompareddatawith17untreatedones.ForimmunohistochemestryweusedCD68(ormonocytes/macrophagesandepithelioidcells),mastcelltryptase(formastcell)andalpha-smoothmuscleactin/vimentin(formyofibroblasts)antibodies.Areaandthicknessofuretersweremeasured in treted and untreated ureteral endings. ResultsLightmacroscopyshowedachronicinflammatoryreactionandasignificantenhancementofhistologicallesion,CD68+cellsandtryptasemastcellsinDx/HAtreatedureters.Amyofibroblasticinvasionwasdisplayedarounddextranomerparticles.AreaofDx/HAtreated ureters was significantly less as compared to untreated ones. ConclusionsOurdatadocumentedasignificantaccumulationofcollagenousstroma,andenhancementofCD68+cellsandtryptasepositive mast cells with an abnormal recruitment of myofibroblasts inDx/HAtreatedrefluxigureteralendings.Moreover,morphologicalanalysis howed a significant reduction of ureteral area in treated ureters. Myofibroblastic invasion suggests a their role in tissue contraction promoting reduction of ureteral area, modifying ureteral lengthtodiameterratio,preventingsourinereflux.

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 27
2009 Oral AbstractsS005LAPAROSCOPY INDUCED CHANGES IN CARDIAC PARAMETERS AT REPEATED IAP ELEVATIONS, ThomasHückstädt,FelixSchierPhD,DevrimAksakal,SteffenRichter,DanielaKlitscher,TobiasWowra,ChristophKampmannPhD,1DepartmentofPediatricSurgery,UniversityMedicalCenterMainz,GermanyAim Laparoscopy has become a surgical method in newborns. Insufflationoftheabdomenresultsinincreasementofintraabdominalpressure(IAP).Inpreviousstudiestherearedifferentstatementsaboutthehemodynamicconsequences.ElevatedIAPwasassociated with increased cardiac output as well as with decreased cardiacoutput.WeinvestigatedhemodynamicparametersduringrepeatedIAPelevationsinyoungpiglets. MethodsTenpiglets(medianbodyweight10,8kg)wereanesthesized by intravenous infusion of pentobarbital and fentanyl. Theinvestigationwasstartedonnormocarbia.Afterregistrationofbaselinevaluescapnoperitoneumwasinduced.Infiveanimalsintraabdominal pressure was raised in 5 mmHg steps up to 20 mmHg, followedbydesufflation.InthesecondgroupIAPwaselevatedupto8, 16 and 12 mmHg whereby after each pressure step the abdominal cavitywasdesufflated.Cardiacoutput(C.O.),meanarterialbloodpressure(pcarot),heartrate(HR)andarterialoxygenation(paO2)wereregistrated.(animalrightcommitteeapprovedstudy1.5177-07-04/G07-1-014) ResultsLowIAP-levels(5,8,10mmHg)wereassociatedwithincreasementsincardiacoutput(2,7,7%inmedianrespectively)andmeanarterialpressure(6,5,9%inmedianrespectively).NosignificantchangeswererecognizedatIAP12or15mmHg.Therewere no significant changes in oxygenation or heart rate seen at any IAP-level.AfterdesufflationcardiacoutputdecreasedineightoutoftenanimalsindependentlyofthepreviousIAPused(8,12,16and20mmHg). ConclusionsDuringlaparoscopyintraabdominalpressurecausesincreasementsincardiacoutputatlowIAP-levels,whereashigherIAP-levelscorrelatewithdecreasedcardiacparametersinyoungpiglets.Desufflationwasassociatedwithanadditionaldecreaseincardiacoutputwithinfiveminutesaftercapnoperitoneum.IfhigherIAP-levelsareusedquickdesuffaltionshouldbeavoidedaswellashypovolaemia.
S006CALORIMETRIC MEASUREMENTS DURING LAPAROSCOPY IN AN ANIMAL MODEL, DevrimAksakal,FelixSchierPhD,SteffenRichter,ThomasHückstädt,DanielaKlitscher,TobiasWowra,ChristophKampmann,1DepartmentofPediatricSurgery,UniversityMedicalCenterMainz,GermanyAim:Weinvestigatedthecarbondioxideuptakeduringlaparoscopyatdifferentintraabdominalpressure(IAP)levelsinpiglets.TheperitonealsurfaceanditsperfusiondependsontheIAPused.WesupposednolinearcorrelationbetweenIAPandcarbondioxideuptake.Theendtidalcarbondioxidepressure(etCO2)servesasagood parameter for ventilatory adaptation during any operative procedure.ThequestionariseshowreliableisetCO2measurementifcarbondioxide is used for laparoscopy. Methods: Ninepiglets(Germanlandrace,bodyweight8.9–13.3kg,median11.2kg)wereanesthesised.Theinvestigationwasstartedonnormocarbia.Afterregistrationofbaselinevaluescapnoperitoneumwas induced. The intraabdominal pressure was performed at 8, 12 and16mmHg,followedbydesufflationaftereachIAP-step.Eachpressurelevelwasmaintainedfor20minutes.Ventilationwasadjustedtonormocarbiabyelevatingtheairwaypressure.IndirectcalorimetricmeasurementswereperformedbytheDeltatrac.Carbondioxideelimination,oxygenconsumptionandarterialcarbondioxidepressure(paCO2)werecalculatedatanyIAP-levelandetCO2weremeasuredcontinuously.(animalrightcommitteeapprovedstudy1.5177-07-04/G07-1-014) Results:ThecarbondioxideeliminationincreasedatallIAPlevels.ThegreatestincreaseoccurredatthelowestIAP-level(IAP=8mmHg:+22,2%,IAP=12mmHg:+14,4%,IAP=16mmHg:+10,3%).Theoxygenconsumptionremainednearlyunchanged.ThepaCO2-etCO2differencewasincreasedwithcapnoperitoneum(IAP=8mmHg:+7mmHg,IAP=12mmHg:+3mmHg,IAP=16mmHg:+0,7mmHg).Allparametersreachedbaselinelevelsafterdesufflation. Conclusions:ResorptionofcarbondioxideduringlaparoscopydepentsontheIAPused.ThemaximumofcarbondioxideuptakeoccursatlowIAP-levels.Inthepostoperativeperiodthedifferencesbetween arterial and endtidal carbondioxide pressure is more variable than before laparoscopy. Negative differences are possible.
InventilatedpatientsventilatoryadaptationorientatedontheetCO2pressurecanleadtohyperventilation.
S007A MIDDLE FIDELITY MODEL IS EFFECTIVE IN TEACHING AND RETAINING SKILL SET NEEDED TO PERFORM A LAPAROSCOPIC PYLOROMYOTOMY, JosephAIoconoMD,MargaretPlymaleMS,JamesHospkinsBS,DanielDavenportPhD,UniversityofKentuckyBackground:Inanimatetechnicalskillstrainingforlaparoscopicpyloromyotomy(LP)hasnotbeendescribed.Wereproducedthe3consistentstepsinLPwitha“middlefidelity”model.Credibilitywas validated by a cohort of pediatric surgeons. This study tested ateachingmoduleofLPwithmedicalstudentsandearlysurgeryresidents to evaluate construct validity and retention of cognitive knowledgeandsurgicaltechnicalskillsafter8weeks.Methods: Subjectsparticipatedinthetrainingindividually.Trainingmaterialsincluded a didactic overview of pyloric stenosis and narrated videos ofaLPandtheLPmodel.TheLPmodelwasinsertedintotheProMIStrainer.Aftercompletingthetrainingmaterials,subjectsperformedthetask(pyloromyotomy)3times(Round1).ProMISautomaticallyrecordedunbiasedvaluesforeachsubject’stime,instrumentpath lengths and smoothness, and a trained observer recorded informationontaskcompletion.Subjectswerere-testedafter8weeks(Round2).Outcomemeasuresincludedsimulatoroutputfromthepost-instructionandfollow-upperformance;stepcompletionasrecordedbytheobserver;andpre-instruction,post-instructionandfollow-upknowledge-basedtestscores.Datawereanalyzedusingpairedsamplet-testsandone-wayanalysesofvariance.Results:Atotal26subjectscompletedthestudy.23subjects(88%)completedeachofthestepsofLPinRound1(post-instructionsimulatorusex3).Meantimewas156±60.9seconds,andthemeanimprovementbetweenruns1and3was85.2±75.4seconds.Basedonaone-way analysis of variance, higher level of training was associated withdecreasedmeantimes(p=.04).Ofthe16subjects(62%)thatcompleted all steps for both Rounds, mean times decreased by 35.05 secondsfromRound1toRound2(p<.001).Knowledge-basedtestpercentscoresimprovedfrompre-instructiontopost-instructionby+17.45(SEM=3.5)(p<.001),andfrompre-instructionto8weekfollow-upby+4.54(SEM=3.2)(p=.17).Conclusions: AnLPmodelprovidedaneffectivetrainingexperience.Constructvalidityofthemodelwasdemonstrated.At3months,taskcompletionratesandtaskperformancetimesshowtechnicalskillswereretainedwhereas,basedonknowledge-testscores,cognitiveknowledgewasnotaswell retained.
S008LONG-TERM OUTCOMES OF LAPAROSCOPIC NISSEN FUNDOPLICATION VERSUS LAPAROSCOPIC THAL FUNDOPLICATION: A PROSPECTIVE RANDOMISED STUDY, Rainer KubiakMD,JamesAndrews,HughGrant,DepartmentofPaediatricSurgery;JohnRadcliffeHospital,Oxford,U.K.AIM:Theaimsofthestudyweretocomparethelong-termoutcomes and control of symptoms following laparoscopic Nissen and Thal fundoplication in children. METHODS: 175 patients were recruited to this prospective, randomisedstudybetweenJuly1998andApril2007.167werefollowed-up-85hadNissenfundoplicationand82hadThalfundoplication.Demographyofthepatientswassimilarinbothgroups. The absolute outcome measure for fundoplication failure wasrecurrenceofsymptomsthatmeritedare-dofundoplicationorinsertionofatransgastricjejunostomy.Thefollow-uptimerangedfrom1to108months(median30.5).Chi-squaredandMann-WhitneyUtestswereusedforstatisticalanalysis. RESULTS:
Nissen(n=85) Thal(n=82)Re-dosurgery 4(4.7%) 10(12.2%)Jejunostomy 1(1.2%) 0Late deaths 20(23.5%) 12(14.6%)
alllatedeathswereduetootherco-morbiditiesThereasonsforrecurrenceofsymptomswere:intheNissengroup2patients had a partially undone wrap, two had a hiatus hernia, and one had an intact but ineffective wrap. The last patient underwent transgastricjejunostomy.IntheThalgroup5hadapartiallyundonewrap, 4 had a hiatus hernia and one had an intact but ineffective wrap.14outof15patientswhoneededare-doprocedurehadneurologicaldisability.There-dooperationwasperformedafteramedianof16.5months(range3-90).Dysphagiaoccurredin20patients in the Nissen group and 21 in the Thal group, however

28 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Oral Abstractsthe dysphagia appeared to be worse in the Nissen group as 50% underwentoesophagoscopy+/-dilatation,whereasonly10%intheThal group required intervention. No late death was related to the primary surgical procedure. CONCLUSION: There was no significant difference between the need for revisional surgery between laparoscopic Nissen and laparoscopicThalfundoplication.Theincidenceofpost-operativedysphagia was similar between the two groups, however more required intervention in the Nissen group. Late deaths were due to otherco-morbidities.
S009THE BENEFIT OF STAY SUTURES DURING THORACOSCOPIC ESOPHAGOESOPHAGOSTOMY IN PATIENTS WITH ESOPHAGEAL ATRESIA, AkihiroShimotakaharaMD,RyoSueyoshiMD,TadaharuOkazakiMD,GeoffreyJLaneMD,AtsuyukiyamatakaMD,DepartmentofPediatricGeneralandUrogenitalSurgery,JuntendoUniversitySchoolofMedicineWereporttheefficacyofusingstaysuturesduringthoracoscopicesophagoesophagostomy(TEES)inpatientswithesophagealatresia. Following excision of the tip of the proximal end of the esophagus to create an opening of adequate size for anastomosis, thetracheoesophagealfistulaisdivided4/5mediallytopreventretractionofthedistalesophagusandTEEScommenced.Firstly,a5/0sutureisplacedthroughthelateraledgeoftheproximalesophagus. This suture is exteriorized through the thoracic wall usingasastaysuturewithouttyingusingaLAPA-HER-CLOSURE®.Asecondsutureisthenplacedthroughthemedialedgesoftheproximal and distal ends of the esophagus. This suture is tied and exteriorizedthrougha5mmtrocarplacedinthemid-axillaryline.These 2 improvised stay sutures allow the luminal surfaces of the anterior and posterior walls of the proximal and distal ends of the esophagustobeexposednicely.Itiscrucialthatbothsuturesincludethe mucosa, since when tension is gently applied on the sutures, the mucosae of both the proximal and distal ends of the esophagus can be exposed much more effectively than if such sutures are not used andmucosa-to-mucosaanastomosisduringTEESisgreatlyfacilitated.These 2 stay sutures are also effective for releasing tension on the anastomosis when the gap between the proximal and distal ends of the esophagus is long. This technique has been used in 5 patients with esophageal atresia, and based on our experience, it facilitates accurateanastomosisduringTEES.
S010LAPAROSCOPIC-ASSISTED REPAIR OF FEMORAL HERNIAS IN CHILDREN, ObinnaOAdibeMD,EricNHansenMD,FedericoGSeifarthMD,CathyABurnweitMD,OliverJMuenstererPhD,Children’sHospitalofAlabama,Birmingham,AlabamaandMiamiChildren’sHospital,Miami,FloridaBackground: Femoral hernias in children are rare, difficult to diagnose, and require a different treatment approach than the standard indirect inguinal hernia repair. There has been a recent trend towards laparoscopic repair of these atypical pediatric hernias. Objective:Wehavedevelopedasimple,effectivelaparoscopic-assisted femoral hernia repair that avoids opening the inguinal canal. Methods: 1)A5mmtrocarisplacedintheumbilicusandthefemoralherniaisvisualizedintracorporeallyviaa30-degreelaparoscope.2)Thelaparoscopeisthenpassedintotheherniasacwiththevisualaxispointinganteriortowardstheskin.3)Guidedbytransillumination,a1cmskinincisionismadeovertheherniasacatthe upper thigh; the fundus of the sac is grasped extracorporeally anddissectedfreefromsurroundingtissue.4)Thesacisthengraspedwithin the abdomen, inverted, twisted, and an endoscopic tie is placedatitsneck.5)Thedefectbetweenthemedialpectinealandinguinal ligaments is closed externally with an absorbable suture. Results: The described technique was successfully used on 3 boys eachwithrightfemoralhernias(age4to11,mean=7).Onone-monthfollow-up,allpatientshadexcellentcosmeticresultswithminimal scars and no recurrence. Conclusion: Laparoscopic-assistedfemoralherniarepairisstraightforward, efficient, and avoids dissection of the inguinal canal,therebycircumventinganyriskofinjurytothevasdeferensandspermaticvessels.Althoughtheseearlyresultsareencouraging,alargerstudyandlongerfollow-upisnecessarytosubstantiateourtechnique.
S011UREKA: UMBILICAL RING EASY KANNULA ACCESS -- A TECHNIQUE FOR INITIAL LAPAROSCOPIC PORT PLACEMENT, JaredWCarlsonMD,JamesMDeCouMD,HelenDeVosChildren’sHospital,GrandRapids,Michigan,USAIntroduction:Initiallaparoscopicportplacementinthepediatricpopulation can be difficult, particularly for larger patients and those with prior abdominal surgery. Knowing that umbilical hernias afford easy access to the peritoneal cavity, we began using a technique of dissection around the umbilicus in patients without clinical hernias, andfoundapatentumbilicalringinessentiallyeverypatient.Inthisretrospectivestudy,wedescribetheumbilicalringeasykannulaaccess(UREKA)techniqueandreviewourresults,evaluatingthesafety and potential decrease in complications related to initial port placement. Methods:IntheUREKAtechnique,asupra-orinfraumbilicalincisionismadefollowedbycircumferentialdissectionoftheumbilicalstalk.Theskinisdissectedfreefromthefascia,exposingtheumbilicalring.ASTEPCannulasheathispassedthroughthering,stiffenedwithaguardedVeressneedle.Afterestablishingpneumoperitoneum,theSTEPCannulaisplacedthroughthesheath.Thefasciaislaterclosedwithafigure-of-8suture,withthesamesutureusedtosecuretheumbilicalskinbackdowntothefascia. Medical records were reviewed for all laparoscopic procedures using UREKAperformedbyonepediatricsurgeonovera14monthperiod.Dataincludedpatientage,weight,gender,diagnosis,procedure,andoperativeandpost-operativecomplications. Results:Ninety-fourpatients(48male,46female)underwentlaparoscopicsurgerywithinitialportplacementviaUREKA.Agesrangedfrom0.25to18years(mean10years),andweightsfrom5to135kg(mean44kg).Appendectomy(n=57)wasthemostcommonprocedure,followedbyfundoplication(15)andcholecystectomy(10).Elevenoftheappendectomieswereforperforatedappendicitis.There were no bowel or bladder injuries and no other intraoperative complications related to port placement. The only postoperative complicationwasasuperficialwoundinfectionina135kgpatientfollowing cholecystectomy, treated successfully with oral antibiotics alone. Conclusion: The umbilical ring persists to some degree in nearly all pediatric patients and provides a safe portal of entry for laparoscopic surgery.UREKAhasfewcomplicationsandisastraightforward,reproducible technique for gaining initial laparoscopic access.
S012LAPAROSCOPIC PANCREATIC RESECTION IN CHILDREN: HOW WE DO IT, KaushikMukherjeeMD,StephenEMorrowMD,EdmundyangMD,MonroeCarellJr.Children’sHospitalatVanderbiltINTRODUCTION: Laparoscopy has been applied successfully for children with traumatic pancreatic injuries and pancreatic masses. Wereportourtechniqueandexperiencewithfourcases. OPERATIVE TECHNIQUE: Thepatientispositionedsupine.Anumbilical trocar is used for the camera. Three or more additional 5mm trocars are positioned bilaterally in the epigastrium. The gastrocolic ligament is opened and the stomach is retracted superiorly.Avesselsealingelectrosurgicaldeviceisusedtodissectalongtheinferiormarginofthepancreas.Dissectionproceedsproximally or distally depending on the location of the pathology. The proximal injured pancreatic duct is oversewn for trauma cases, and for tumors the pancreas is divided with a 45 mm stapling device. The distal pancreas is mobilized from the splenic vessels, usually in a proximaltodistaldirection.Ifthevesselscannotbeseparatedsafely,then they are divided and a laparoscopic splenectomy is performed as well. The specimen is placed in a retrieval bag and removed throughasmallincision.Drainsareplacedpriortoclosure. CASE EXPERIENCE:Wereport4cases:twopatientswithpseudopapillary tumors and two with traumatic pancreatic injuries. Operativetimerangedfrom206to305min.Meanhospitalizationwas5.75days(range5-8).Oralintakewastolerated1.5dayspostoperatively(range1-3days).Therewerenodeaths.Onepatientwasreadmittedforaperipancreaticfluidcollectionandrequireda3weekcourseofTPNforresolution.Therewerenoothercomplications. CONCLUSIONS: Laparoscopic pancreatic resection in children is feasible, safe, and leads to rapid recovery without significant morbidity. The spleen can often be spared, minimizing future infectiousrisks.Thisinitialexperienceshouldencouragewideruseofminimally invasive techniques for pancreatic resection in children.

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 29
2009 Oral AbstractsS013MICROLAPAROSCOPIC PYLOROMYOTOMY FOR HYPERTROPHIC PYLORIC STENOSIS – OUR TECHNIQUE, SalmaiTurialMD, RuthFreudenberger,KathrinKrause,BarbaraGoldinger,VeronikaEngel,FelixSchierMD,UniversityMedicalCentre,Departmentofpediatricsurgery,Mainz,GermanyPurpose: The aim of this prospective feasibility study was to determine the value and safety of the microlaparoscopy for pyloromytomy in children. Methods and Patients: This study included 21 consecutive children (11boysand7girls,agesrangedfrom3to12(average4.8)weeks)undergoing microlaparoscopic pyloromyotomy for hypertrophic pyloricstenosis.AMini-Portewasinsertedinfraumblicalforthesmalldiameterscopes(1.9to2.4mm)insupinepositionofthepatient.AnothertwoworkingMini-portswereinsertedpararectallyatumbilical level for a 2mm grasper on the right side and in the left Hypochondriumforthepyloromyotomyknife.Theduodenumwas grasped just distal to the pylorus olive and a serosal incision was made along the pylorus olive in the avascular plane by usingmonopolarcautery.A2mmgrasperwasusedtosplitthehypertrophiedmuscleuntilmucosawasvisualized.Attheendofproceduresthetrocarswereremovedandtheskinwasapproximatedwith strips only. Results:Infirst10casesalaparoscopicpyloromyotomyspreader,inserted directly through the abdominal wall, was used to complete the pyloromyotomy. Later on, by performing a complete serosa incisionwithhigh-powermonoploarcauterythe2mmgrasperwas sufficient to spread the muscles and to use the spreader was notneeded.Allmicrolaparoscopicprocedureswereperformedsuccessfully. The operative time ranged form 9 to 18 min (average 13min).Nocomplicationsoccurredduetotheexclusiveuseof2mminstruments and small diameter scopes. There were no intraoperative or late postoperative complications (duodenal perforation, conversion, incomplete pyloromytomy, wound infection, readmission tofourweeksaftersurgery)noted. Prolongedvomitingoccurredintwoinfantsinfirstpostoperativeday. The feeding was started four hours after surgery and full feeding was reached in first postoperative day in 16 infants. Conclusion:Accordingtothesmallnumberofpatientsinthisstudy,it appears that the microlaparoscopic pylormyotomy in children is feasible, safe and effective.
S014LIGASURE FOR THE MANAGEMENT OF TUBULAR DUPLICATION OF ESOPHAGUS, HamidRezaForoutanMD,SeyedAbbasBananiMD,ShirazUniversityofMedicalSciencesTubular duplications of esophagus is very rare. To treat these patients major surgeries through thoracotomy, laparatomy, or thoracoscopy approaches have been recommended. Resection, side to side anasthomosis or interposistion procedures have been performed. Here we present a very minimally invasive surgery, without thoracotomy,thoracoscopy, laparatomy, or laparoscopy as an innovative procedure for the treatment of these anomalies with complete remission of symptoms. A15daysoldboywasadmittedinNICUduetorespiratorydistress.Hewasintubatedandwasartificiallyventilatedsincebirth.Duringintubation they noticed an orifice in oropharynx posterior to esophagus.Endoscopywasperformedwhichconfirmedatubularesophageal duplication originating posteriorly in the oropharynx and parallel to esophagus for almost its length and was distally blind ended.Themucosaofbothlumensseemednormal.Esophagographywas performed which confirmed the double esophagus. There was norefluxandperistalsiswasnormal.ChestCTscanwithdoublecontrastwasnotveryconclusive.Echocardiographywasnormalandnootherassociatedanomalywaspresent.Undergeneralanesthesia,videoendoscopewasinsertedandwithLigaSure5mm,thecommonwall was gradually sealed and cut till the end of the duplication. The patient was ventilated for a few days and gradually was tapered offwithinafewdays.Bariumswallow,twoweeksafteroperation,showedwellpatentnormalesophaguswithgoodperistalsis.Re-endoscopythreeweeksafteroperationrevealednormalmucosawithminimal redness at the lateral parts of the esophagus. The patient graduallywelltoleratedthefeedingandwasdischarged.Inthefollow-uponemonthlaterhewasdoingwellwithgoodweightgain. Conclusion: wehighlyrecommendLigaSureforpatientswithtubular duplication of esophagus.
S015LAPAROSCOPIC OMENTOPLASTY FOR LOWER EXTREMITY LYMPHEDEMA, HamidRezaForoutanBA,ShirazUniversityofMedicalSciencesOmentoplastyasapalliativetherapyhasbeenrecommendedforpatients with lower extremity lymphedema. Here we present a patient with severe lower extremity lymphedema who was treated laparoscopically. The patient was a 14 years old girl with history of longstanding left lower extremity lymphedema.The edema involved her thigh and leg. The diameter was almost two times of her right leg. the patient haddifficultyinwalking.Shehadbeentreatedconservativelywithnobenefit.Thedeepveinswerepatent.Omentumwasdissectedlaparoscopically and through a tunnel in left groin the omental patchwasperformedinthegroinforabout10x10cm.Withinafewdays after operation the edema decreased and became much softer. thepatientwasabletowalkmucheasier. Conclusion: Werecommendlaparoscopicomentoplastyforpatientswith intractable lymphedema.
S016SPLIT APPENDIX TECHNIQUE FOR APPENDICEAL LENGTHENING FOR MALONE AND MITROFANOFF CONDUITS, CurtisASheldonMD,BelindaDickieMD,ShumyleAlamMD,MarcALevittMD,CinciinatiChildren’sHospitalMedicalCenterPurpose: Management of fecal and urinary incontinence often include mitrofanoff and malone conduits, which sometimes can be performed during the same operative procedure For each of these procedures, the appendix is extremely useful and durable as a catherizablechannel.Wedescribeatechniquetosplittheappendixand elongate the base of the appendix so it can be used for both purposes. Methods: The appendix is examined for length and a suitable mesentery.Anadequatelengthofthedistalaspectoftheappendixbased on the appendicial blood supply is initially selected for the urinary reconstruction. The remaining proximal portion of the appendixisthenleftforthemaloneappendicostomy.Becausethisportion of the appendix is often not long enough to allow plication, itiselongatedwithafiringoftheendovascularTAstapleralongthe cecum on the antimesenteric side with preservation of the vascular supply. This is done over a twelve French foley catheter for calibration.Cecalplicationisthenperformedtopreventleakage. Results: Wehaveperformedthesplit-appendixapproachin29patients.Allpatientshavehadadequateconduitsforbothurinarycatheritizationandantegradecontinentenemas.Wehavealsousedthis technique in patients with cloaca extrophy who have short appendices. The appendiceal lengthening technique can avoid the needofaneoappendicostomy.UseoftheendovascularTAstaplerfacilitates this maneuver. Conclusions: Withthistechniqueofsplittingtheappendixandelongating its base, the appendix can be used to provide access for both bladder catherizations and administration of antegrade continent enemas
S017PREPERITONEOSCOPIC BLADDER-NECK SUSPENSION FOR THE FASCIA SLING PROCEDURE IN CHILDREN., GirolamoMattioliMD, PieroBuffaMD,MicheleTorreMD,VincenzoJasonniMD,DeptofSurgery,GasliniInstitute,UniversityofGenovaAimofthestudyistopresentthetechnicaldetailsofourpreliminaryexperienceontheendoscopicpneumoCO2preperitonealapproachtothebladderneckandU-typeslingsuspensionandbladderaugmentation. Patient: A13yearoldboywasadmittedtoourORinordertotreat bladder incontinence due to neurogenic lower urinary tract dysfunctionandspinabifida.Abladderaugmentationandbladdernecksuspensionwasplanned. Alefttransperitonealsubcostalfirstportwasinserted.Thepreperitoneal space was prepared under direct transperitoneal visualization.Asthespacewassufficient,atotalofthreeportswereinsertedinthepreperitonealspace:oneinthemidlineinthenaveland the other two ports laterally to the rectus muscles in order to preservetheintegrityofthefasciatoperformthebladdernecksuspension. Dissectionofthebladderwasveryeasyandrapidlythedeeppelvis,octuratoria and retropubic space were exposed. Arigidtubewasinsertedintherectumandafoleycatheterinthe

30 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Oral Abstractsbladderinordertoexactlyidentifythebladderneck,uretraandbowel. Underdirectvisualizationthebladderwaspreparedandseparatedfromtherectumsoonaftertheprostaticregion.Aloopwasinsertedand used for positioning of the rectus fascia. Durationofthisprocedurelasted2hours.Nocomplicationsoccurred. Technical details will be showed. Discussion: Thedirectvisualizationofthebladderneckandtheminimal traumatic dissection of the deep pelvis is very useful and safe.Inthisdifficultareaitisnoteasytocontrolthevesselsandviscerawhichisofutmostimportanceinordertoreducetheriskofcomplications.OurpreliminaryexperienceontheminimalinvasivepreperitonealpneumoCO2endoscopicassistedaccessis,inouropinion,tobeconsideredaninterestingminimal-invasiveandsaferalternative to the perineal or the laparotomic approach to the bladderneckinordertoperformtherectusfasciaslingsuspensioninchildren. References: ChrzanR,DikP,KlijnAJ,deJongTP.Slingsuspensionofthebladderneckforpediatricurinaryincontinence.JPediatrUrol.2008Oct29.
S018LAPAROSCOPIC RESTORATIVE PROCTO-COLECTOMY IN CHILDREN., GirolamoMattioliMD,PaoloGandulliaMD,GiovanniRapuzziMD,VincenzoJasonniMD,GasliniInstitute-UniversityofGenova-ItalyAimofthestudyistodefinetheroleandfeasibilityoflaparoscopicrestorative proctocolectomy in children with refractory ulcerative colitis(UC)ortotalcolonicaganglionosis(CA)andtodemonstratesome details of the technique. Patients: 18consecutivepatients(13UCand5CA),undergoingrestorative total proctocolectomy were prospectively included in the studyintheperiod2006-2008. Results: Endorectalpull-through(ERPT)andstraightileo-analanastomosiswasperformedin4/18andileo-rectalanastomosisin14/18. Medianageatsurgerywas8.6years(44days-17years).Minimumfollow-upafterbowelrestorationwas3months. InallcasesofUC,colectomywassupportedbyacutepancolitisandbleeding, diagnosed by clinical examinations and endoscopies. 12patientsunderwentrestorativeproctocolectomyandJ-pouchdouble-stapledrectalanastomosis(Knight-Griffen)andonecaseunderwentstraightGeorgeson-SoaveERPT. CAwasdiagnosedbyhistochemicalanalysis.AnERPTwasdonein3out5andaretrorectalpull-through(Duhamel)in2out5. Inallthecasesileostomywasdonebeforebowelrestoration. 5complicationsoccurred:2anastomoticstenosiswhichrequiredsimple dilation, 1 abdominal abscess due to rectal pouch dehiscence after colectomy which needed drainage and 2 bowel adhesions. Meanpost-operativein-hospitalstaywas7days. Discussion: Intheperiodbefore2006,restorativeproctocolectomieswereperformedthroughanopenapproach.Astheexperienceincreased, the number of laparoscopic procedures grew as well and nowtheminimally-invasiveaccesssurgery(MIAS)isourstandardasitis feasible, guarantees a shorter hospitalization, lower problems and agoodqualityoflife.Detailsofthetechniquewillbediscussed. References: GeorgesonKE,Laparoscopic-assistedtotalcolectomywithpouchreconstruction,SeminPediatrSurg.2002Nov;11(4):233-6
S019THE ENDOSCOPIC U-STICTH TECHNIQUE FOR PRIMARY BUTTON PLACEMENT, NeilNixdorffBS,JenniferDilucianoRN,ToddPonskyMD,RobertParryMD,WalterChwalsMD,ScottBoulangerMD,DivisionofPediatricSurery,DepartmentofSurgery,CaseWesternUnviersitySchoolofMedicineIntroduction: There are several techniques for the primary placementofagastrostomybutton.Abrahamianetal.recentlyreportedtheirrecordofsuccesswithalaparoscopicU-stitchtechnique(JLaparoendoscAdvSurgTechA.2006Dec;16(6):643-9.)Here,wedescribetheperformanceandsafetyprofileforanendoscopic version of that laparoscopic technique, the endoscopic U-stitch(EUS)technique,thatispracticedatourinstitution. Methods:Ahospitaldatabaseretrospectivestudyandchartreviewofprimarygastrostomyplacementsbetween2003–2008. Results: Outof277primaryproceduresforgastrostomytubeplacement,103weredoneusingtheEndoscopicU-Stitchtechnique.56(55%)EUSprocedureswereperformedinneurologicallyimpairedpatients.Themedianpatientagewas3.51years(Range0.12-23.89;Mean1.34;25/75%quartiles–0.59/3.3years).Incaseswhere
operativetimesandweightswererecorded(n=43),themedianoperativetimewas15minutes(Range5–39;Mean16;25/75%quartiles–14/22.5minutes)andthemedianweightwas11.3kg(Range3.2-70.0;Mean11.34;25/75%quartiles–5.67/12.78kg).Weidentified perioperative complications in 5 patients which included postoperativebloodyemesis(2),postoperativecellulitis(2)andgastrostomyperforation(1).Inadditiontothe103EUSprocedures,6casesthatwerestartedasEUSprocedureshadtobeconvertedintraoperatively to laproscopic or open procedures due to technical challenges. Conclusion: TheEndoscopicU-stitchgastrostomytechniqueissafeandallowsprimarybuttonplacementininfantsandchildren.Itscomplication rate compares favorably to other reported gastrostomy techniques.
S020LAPAROSCOPIC DIAGNOSIS AND TREATMENT FOR INTESTINAL MALROTATION IN CHILDREN, SuolinLIMD,yingchaoLI,WeiliXU,DepartmentofPediatricSurgery,2ndHospitalofHebeiMedicalUniversity,Shijiazhuang,050000,China.Objective The aim of this study was to evaluate the effectiveness of a laparoscopic approach for the diagnosis and surgical treatment of intestinal malrotation and to explore the optimal repairing condition for midgut volvulus. Methods FromJuly2002toMarch2008,23childrenwithsuspectedintestinal malrotation underwent a diagnostic laparoscopy. There were13malesand10females.Agerangewasfrom5daysto12years(average,1.9years).Theprocedurewasperformedusing3trocarsof3.5mmto5.5mmdiameter.Underlaparoscopicvision,themidgut volvulus was untwisted by grasping and pulling the instine, Ladd¡¯s band was divided and broadened, the duodenum and proximal jejunum were mobilized, and the concomitant abnormities were treated at the same time. Results 23 cases suffered from intestinal malrotation were certainly diagnosed and completely operated through the laparoscope. 18 cases with midgut volvulous from 270 to 960 degrees were corrected successfully.Ofthem,2caseswithparaduodenalhernia,1duodenalweb,1ectopicpancreasand1Meckle¡¯sdiverticulumalsohadaprocedure meanwhile.The average operative time was 65.2¡À15.8 min(35¡ª150min).Feedingswerestartedonpostoperative1to3days.Therewerenocomplications.Butonecasewasreoperatedforproximal jejunal adhension after 2 months. 21 patients had followed up from 1 month to 5 years resoluting their symptoms and growing well. Conclusions The intestinal malrotation is exactly diagnosed and treatedwithlaparoscopy.Itcanbeperformedinneonatessecurelyandappropriatedforasubacutemidgutvolvulus.Patientsalsobenefit from this minimally invasive approach, as manifested by anearlieroralintake,anearlierdischargefromthehospitalandabetter cosmesis.
S021MINI-INVASIVE TREATMENT OF INTESTINAL DUPLICATION IN NEWBORNS AND SMALL INFANTS, ClaudioVellaMD, Massimo GarriboliMD,LucianoMaestriMD,GianlucaMonguzziMD,GiovannaRiccipetitoniMD,DepartmentofPediatricSurgery-Children’sHospital-V.Buzzi–Milan–(Italy)INTRODUCTION The laparoscopic approach is particularly indicated in the treatment of intestinal duplications in newborns and small infants.Itpermitstodefineacorrectdiagnosisandtoidentifythe type of duplication and the eventual presence of associated intestinal anomalies. The procedure seems to be feasible, easy to perform, with faster recovery and better cosmetic results. MATERIAL AND METHODS FromJuly2007toNovember2008fourbabies, aged between 1 and 3 months, 3 males and 1 female, were referred to our institution for an antenatal suspicion of intestinal duplication.Inallcasesthediagnosiswasconfirmedpost-natallybyultrasonography(US)andmagneticresonanceimaging(MRI).Atthephysical examination, two babies presented a palpable mass in the rightabdomenwithreferredincreasingdimension.In3casesthelaparoscopicapproachwascarriedoutusingasingletrans-umbilicaloperative telescope, in the remaining case a 3 mm trocar was added. RESULTSAtsurgerywefound2casesofcysticilealduplication,in1case the duplication interested the ileocecal valve; isolated multiple cystic duplications were detected in the fourth case. The 2 ileal duplications were extracted from the umbilical trocar site and submitted to limited intestinal resection. The ileocecal duplication was exteriorized with the same procedure and resected

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 31
2009 Oral Abstractswith an extra mucosal approach preserving the ileocecal valve.The patient with isolated multiple cysts was entirely treated laparoscopically. No complications occurred, the cosmetic results were excellent. DISCUSSIONWerecommendremovinganintestinalduplicationassoon as possible, because they may lead to volvulus, intussusceptions, perforationorbleeding.Alsointhisimagingadvancednewerathediagnosisandcharacterisationisn’talwayspossible. The laparoscopic approach permits to define the diagnosis, to identify the different type of duplication and to perform a proper treatmentwithamini-invasivetechniqueandexcellentcosmeticresults. CONCLUSIONIntestinalduplicationscanbeconsideredagoodindication for video assisted surgery in newborns and small infants
S022FETAL ENDOSCOPIC TREATMENT OF CONGENITAL HIGH AIRWAY OBSTRUCTION (CHAOS), ShinjiroHiroseMD,HanminLeeMD,UniversityofCalifornia,SanFranciscoCongenitalhighairwayobstruction(CHAOS)isararedisorderconsisting of tracheal obstruction resulting in massive distention of the lungs, ascites, pleural effusions, and fetal hydrops. Left untreated,thisanomalyisalmostuniformlyfatal.Wepresentacaseofanatomic,fetoscopictreatmentofCHAOS. Maternalultrasoundat22weeksgestationrevealednormalamnioticfluid,markedfetalascites,distendedlungswitheverteddiaphragms,and a dilated distal trachea. Weperformedmaternallaparotomyandfetalbronchoscopyat23weeksgestationvisualizingthelarynx,vocalcords,andesophagus.Weplacedawireacrosstheairwayobstructionusingacombinationof direct vision and ultrasound and subsequently decompressed the distalairway.Follow-upultrasounddemonstratedresolutionoftheascites, improvement in lung distention, and normalization of the diaphragms. TheinfantwasbornviaEXITprocedureat30weeksgestation,during which we placed a tracheostomy. He subsequently has undergone repeat endoscopy, and his trachea remains patent and as been dilated to 2mm. He is at home and remains on positive pressure ventilation.
S023EXPERIENCE WITH THORAOCSCOPIC TRACHEAL SURGERY IN INFANTS AND CHILDREN, StevenSRothenbergMD,TheRockyMountainHospitalforChildrenPurpose: Complexthoracoscopicproceduresininfantsandchildren,suchasTEFrepairandlungresectionhavealreadybeenshowntobe safe and efficacious in infants and children. This study evaluates the application of thoracoscopic techniques in more complex and unusual tracheal anomalies. Methods: FromJanuary2002toOctober20089patientswithmorerare anatomic tracheal anomalies, between the thoracic inlet and the carinaweretreatedbythoracoscopy.Agesrangedfrom5monthsto 8 years and weights ranged from 5.4 to 8 years and weight from 5.9to42Kg.Pathologyincluded3HtypeTEFs,2recurrentTEFsfollowing previous open repair of an esophageal atresia with fistula, resectionofagianttrachealpouch,and3tracheo-bronchiwithassociated abnormal lung parenchyma. Results: Allprocedureswerecompletedsuccessfullythoracoscopically.Operativetimesrangedfrom60to130minutes.Proceduresincludeddivisionandclosureofthe3Htypefistulasand 2 recurrent fistulas, resection of the tracheal pouch, 2 upper lobectomies, and resection of an aberrant upper lobe segment bysegmentectomy.Therewerenooperativeorpost-operativecomplications.Chesttubeswereleftinforanaverageof1dayandhospital stay averaged 2.2 days. Conclusion: Thoracoscopy provides an excellent technique for approaching tracheal pathology from the level of the thoracic inlet tothecarina.Athoracoscopicapproachavoidsthemorbidityofamajorthoracotomy,andoramajorneckexploration,whileprovidinggreater exposure, especially in the upper thorax.
S024THORACOSCOPY IN THE MANAGEMENT OF RESIDUAL DISEASE IN PATIENTS TREATED FOR HODGKIN LYMPHOMA (HL) AND NON-HODGKIN LYMPHOMA (NHL). A SINGLE CENTRE EXPERIENCE.,Eleonora1CescaMD,Paola1MidrioMD,Pietro1BetalliMD,Angelo2RosolenMD,Piergiorgio1GambaMD, 1DepartmentofPediatrics,PediatricSurgery,2DepartmentofPediatrics,PediatriconcologyUniversityofPadua-ITALyIntroduction.Thesurgeon’sjobinthemanagementofpatientsaffected by HL and NHL with residual mediastinal or lung nodules afterthecompletionofthechemo/radiotherapicprogram,istoobtainspecimenfordiagnosisortoremoveresidualmasses.Samplesof residual masses can be obtained by thoracoscopy. Methods. Records and operative reports of patients treated for HL andNHLundergoingthoracoscopybetweenJanuary2002andJune2008inourCentrewereretrospectivelyreviewedfordemographics,diagnoses, operative management, and outcomes. Results. Sevenpatients(6M,1F),meanage13years,underwentthoracoscopy:4biopsiesofmediastinalmasses,2biopsiesoflungnodules,and1removalofaresidualmediastinalmass.In1/5patientswith persistent mediastinal tumor histopathological examination revealedthepresenceofneoplasticcells.In1/5casesathymiccystwasexcised.Necrotictissuewaspresentin3/5cases.The2patients with suspected lung lesions had non neoplastic cells in the excised tissue. Mean operative time was 50 minutes without major complications nor need to conversion. Mean hospital stay was 2 days. Atamedianfollow-upof10months,sixpatientsarealiveandfreefrom disease and one is alive and in disease progression. Conclusions.Patientswithpersistentthoraciclesionsrequirerepeated clinical and radiologic examinations to reduce surgery indications. Thoracoscopy should be the technique of choice for diagnosticandtherapeuticsecondlookprocedures.
S025NEW FULLY ENDOSCOPIC PECTUS CARINATUM REPAIR USING SUBPECTORAL CO2 INSUFFLATION AND STERNAL NUSS BAR COMPRESSION OR MIS-HYBRID TECHNIQUE, ESTABLISHING A DIFFERENTIAL INDICATION., KlausSchaarschmidtBA,AndreasKolberg-SchwerdtBA,MichaelLempeBA,FrankSchlesingerMD,HeliosCenterforPediatric&AdolescentSurgery,Berlin-Buch,GermanyObjective: No universally applicable endoscopic minimal access pectus carinatum repair has been devised, few sizeable series arereported.Severepectuscarinatumbeyondadolescenceandcombineddeformitieswithpectusexcavatumand/orcostalflaringseeminaccessibletoMIS.Thisprospectivestudyof143minimalaccesspectuscarinatumrepairsinBerlin-Buchintendstoestablishdifferentialindicationsfor2MIScarinatumtechniques. Methods: From2/2001to12/2007weminimizedaccess(2.9-4.7cm)byendoscopichybridtechnique(EH)with2transsternalHegemann-Willitalbars.136EHpatientsaged17.1±3.4y(12-41y)wererecordedprospectivelyandfollowed52.3±13.9mo(10-92mo-7redos). In2008weusedendoscopicNussbarcompression(ENBC)in7patients(age16.3±2.4yrange12-19y)withminimaloperativetrauma.WeimplantastandardNussbarintoanendoscopicallydissectedsubmuscularpresternalpocketcorrectingpectuscarinatumbysternalback-pressure.ThebarswerebenttoaconcavityoverthemaximalprominenceofthePCandputundertensionbybackwardtraction via stabilizers and 3 endoscopically placed pericostal wire sutures. Results:All143pectuscarinatumrepairsweredonebyminimalaccesswithnoconversion(Haller0.68-1,89).Therewere3seromasintheEHseries(4/136)managedconservatively.125patientsjudgedtheir result as excellent, 11 as good, in 74 patients struts were removed with no recurrence so far. Inall7ENBCpatientsfullcorrectionofthePCcouldbeachieved,in3endoscopicrepairofcostalflaringwasadded.TherewerenocomplicationsinthepurelyendoscopicENBCseries,5patientsjugedtheirresultasexcellent2asgood,noENBCbarwasremovedsofar. Conclusions:Bothmethodsaresafeandeffectivesofar. EHendoscopichybridrepairyieldsresultsatleastasgoodasconventional carinatum repair and was applicable in all 136 cases including the most severe and is our new standard technique. For younger patients up to 20y ears with more compressible protrusions fully endoscopic compression technique may become a farlessinvasivealternativetechnique-however,thisisaveryearlyENBCexperience.

32 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Oral AbstractsS026NONINVAZIVE CORRECTION OF PECTUS CARINATUM WITH COMPRESIVE ORTHOTIC BRACING IN CHILDREN: PRELIMINARY RESULTS OF ONE INSTUTITION, GulcehakguderMD,OguzAtesMD,MustafaOlgunerMD,FezaMAkgurMD,DepartmentofPediatricSurgery,DokuzEylülUniversity,MedicalSchool,Izmir,TurkeyAim: Amongthechestwalldeformities,pectuscarinatum(PC)hasnotgiventhesameattentionaspectusexcavatum.PatientswithPC,complain of cosmetic matters because it draws attention in spite of wearingclothes.AlthoughtheclasicaltreatmentofPEisoperative,recently compressive orthotic braces have been used with good cosmeticresults.Wehereinpresenttheresultsofthenoninvasivecorrection of pectus carinatum with compressive orthotic bracing in our department. Materialsandmethod:BetweenApril2006andOctober2008,18patientswithPCweretreatedwithcompressiveorthoticbracing.Patientswithpositivemanualcarinatumflexibility(compression)test were began bracing protocol. The patients were evaluated with echocardigraphyandrespiratuaryfunctiontests.Baselinethoraxcomputedtomographies(CT)wereobtainedandcustom-fittedorthoticbraceswerepreparedforeachpatient.Angleofsternalrotationofthepatientswereevaluated.Patientswerefrequentlyfollowed up. The patients started wearing the brace with a 6 hours duration and prolonged the duration time by one hour every month. Thebracewaswornfor16hoursperdayuntilthePCdeformityiscorrected.Thepatientswerefrequentlyevaluatedforskinlesions and patients compliance. The patients who completed their treatmentwerereevaluatedbyathoraxCT. Resuts: There were 15 boys and 3 girls aging between 5 to 16 years, meanageof11.4±6.TenpatientshadanasymetricalPCdeformity.Treatment of the 3 patients were completed with excelent visual results. The average duration of the bracing was 21 months in thesepatients.Inthosewhosuccessfullycompletedtreatment,animprovementintheangleofsternalrotationwasfound.Oneofthe patients abandoned bracing because of noncompliance. The remaining 14 patients are still under bracing. Conclusion: Compressiveorthoticbracingisanoninvazive,effectiveand safe alternative to surgical correction in the treatment of PCdeformityevenasymmetryispresent.Patientsandthefamilycompliance is important for reaching good results.
S027THORACOSCOPIC REPAIR OF CONGENITAL DIAPHRAGMATIC HERNIA IN NEONATES: LESSONS LEARNED, AnneCKimMD, BenjaminSBrynerMS,BegumAkayMD,JamesGeigerMD,RonaldBHirschlMD,GeorgeBMychaliskaMD,DivisionofPediatricSurgery,UniversityofMichiganHealthSystem,AnnArbor,MichiganPurpose:WesoughttocharacterizeourrecentexperiencewiththoracoscopicCDHrepairandidentifypatientselectionfactors. Methods: Wereviewedmedicalrecordsoffulltermneonatal(<1monthofage)patientswhounderwentthoracoscopicCDHrepairbetween2004-2008,n=15.Weobtaineddataonprenataldiagnosis,characteristicsoftheCDHandrepair,complicationsandoutcome. Results: Allpatientswerestabilizedpreoperativelyandunderwentrepairatanaverageof5.7±1.3days.Sixwereinbornandhadbeenprenatallydiagnosed.Thirteenofthedefectswereleft-sided;thetworight-sideddefectshadliverherniation.Allwereintubatedshortly after birth and two required extracorporeal membrane oxygenation(ECMO).Twelveof15(80%)underwentsuccessfulthoracoscopic primary repair, including one of the patients who requiredECMOpriortorepair.Conversiontoanopenprocedureoccurredin3/15(20%)becauseoftheneedforpatchclosureorintraoperativeinstability.Amongthoseconvertedtoopen,allhadleft-sidedCDHdefectsandtwohadstomachherniation(outoffoursuchpatients).Patientsspentanaverageof6.9±1.0daysontheventilatorfollowingrepair.Theaveragetimeuntilfull-enteralfeedingwas16.7±2.25days,andaveragelengthofhospitalstaywas23.8±2.73days.Allfifteenpatientssurvivedtodischarge,andaveragelengthoffollow-upwas460±101days. Conclusions: ThoracoscopicrepairofCDHisasafeandeffectivestrategy in patients who have undergone prior stabilization. Stomachherniationisassociatedwith,butdoesnotcategoricallypredict,conversiontoopenrepair.ECMOusepriortorepairshouldnot be an absolute contraindication to thoracoscopic repair.
S028WHICH IS THE BEST VESSEL AND BRONCHIAL SEALING METHOD FOR PEDIATRIC THORACOSCOPIC LOBECTOMY?, Marcelo Martinez-FerroMD,HoracioBignonMD,EnriqueBuelaMD,HospitalPrivadodeNinos.FundacionHospitalariaIntroduction: Thoracoscopic lobectomy is performed with increasingfrequencyinchildren.Severalpublishedreportssuggestthoracoscopic resection is safe, with the potential advantage of shorterhospitalstay,quickerrecovery,andcomparablelongtermresults. Limitations still remain, however, mostly because of technical restrictionsregardingvesselandbronchialsealing.Weanalizeandreport our experience in 20 consecutive pediatric cases in order to define the best method for both procedures. Methods:Meanagewas4,1years(6d-12y).Preoperativediagnosisincludedcongenitalcysticadenomatoidmalformation(n14),Bronchiectasis(n4)andIntralobarPulmonarySequestration(n2)..Threeorfour3-5&12mmportswereuseddependingonthepatientage.Singlelungventilationandcontrolledlowpressurepneumothorax were used in every case. Methods for vascular sealing includedtheuseofLigasure®,Hemo-Lock®clipsoracombinationofboth(ProximalclipplusdistalsealingandcuttingwithLigasure).MethodsforbronchialsealingincludedHemo-Lock®clips,EndoGiaII®staplersorthecombinationsofboth.WedefinedasvascularIncident(VI)whenbleedingappearedafterthefirstintentofsealingavessel.Achesttubewasleftinallcases. Results: Of20procedures,16werecompletedthoracoscopically.Operatingtimesrangedfrom60to330min(mean,150min).Therewere 4 upper, 2 middle, and 14 lower lobe resections. None of the 4 conversionswhererelatedtoaVI.Therewere5VI(25%),allofthemarteriesandcouldbesolvedbythoracoscopy.Onepatientrequiredintraoperativebloodtransfusion.NoneoftheVIoccurredduringdissection,butalwaysafteranapparently“good”sealingwiththeLigasuredevice.AlloftheVIoccurredinpatientsolderthan2years.Also,inallpatientsyoungerthan2years,bronchialsealingwasachievedusingdifferentsizesofHemo-Lok®clips,butolderpatientsrequired the use of staplers or the combination of both. Conclusions: The age of the patient, is a crucial data to consider at themomentofplanningapediatricthoracoscopiclobectomy.Inourexperience in order to obtain a reliable vessel sealing, patients older than 2 years needed a combination of a proximal clip plus distal Ligasure.Asfortheairwaysealing,acombinationofstaplerplusclips was the best choice for the same age group of patients.
S029THORACOSCOPIC LOBECTOMY FOR SEVERE LOBAR BRONCHIECTASIS IN CHILDREN, KeithAKuenzlerMD,WilliamMiddlesworthMD,StevenSRothenbergMD,MorganStanleyChildren’sHospitalofNy-Presbyterian,ColumbiaUniversityMedicalCenter,Newyork,NyandTheRockyMountainHospitalforChildren,Denver,COBACKGROUND/PURPOSE: Lung resection should be considered for severe, localized bronchiectasis causing recurrent infections inpatientswithcysticfibrosis(CF)andotherdiseases.Thisseriesrepresentstheauthors’experienceandresultswiththoracoscopiclobectomy for treatment of bronchiectasis confined to a single lobe. METHODS: 18 thoracoscopic anatomic lobectomies were performedbetweenJuly1994andAugust2008.Patientageatthetime of surgery ranged from 3 to 22. Left lower lobectomy was the mostfrequentlyperformedprocedure(n=9).EightpatientssufferedfromCF,5hadchronicpneumonia,2hadchronicaspiration,and3 had other diagnoses. RESULTS: Mean operative time was 162 minutes(range:65to300minutes),andnocasesrequiredconversionto thoracotomy. The mean duration of postoperative chest tube drainagewas3.2days(range:1to9days).Themeanpostoperativelengthofstaywas3.6days(range:1to12days).Onepatienthadaprolongedairleaklasting9days,whichresolvedwithplacementofasecondchesttube.Anothersmallhydropneumothoraxpersistedafterchest tube removal but resolved spontaneously. CONCLUSIONS: Thoracoscopic lobectomy for severe lobar bronchiectasis with recurrent infection may be technically challenging, but appears to besafeandeffective.Avoidanceofathoracotomyinthesepatientsallows for earlier mobilization, less postoperative pain with cough and chest physiotherapy, and faster recovery. There appear to be significant benefits in this group of patients with chronic respiratory illnesses.

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 33
2009 Oral AbstractsS030THORACOSCOPIC THORACIC DUCT LIGATION FOR PLASTIC BRONCHITIS, CurtSKoontzMD,S.SalmanAShawMD,ClaireSNicholasMD,MarkLWulkanMD,Children’satEgleston/EmoryUniversitySchoolofMedicineBackground: Plasticbronchitis(PB)isadiseaseinwhichthick,arborizing casts of the tracheobronchial tree develop resulting in airwayobstruction.PatientswhohavecongenitalheartdiseasethatrequireaFontanprocedureareatriskforthisunusualdisease.OnetheoryforthedevelopmentofPBisthathighintrathoraciclymphaticpressureswithlympho-bronchialfistulasarethecauseofthecasts.Thereisarecentreportof2successfulcuresofPBwithligationofthethoracicductviathoracotomy.Wearereportingour2casesofPBtreated with thoracoscopic thoracic duct ligation. Methods:Twopatientsunderwentright-sidedthoracoscopicthoracicductligationforPB.AVeressneedlewasusedtocreatea pneumothorax. Three 5mm trocars were placed. The inferior pulmonaryligamentwastakendown.Thepleurawasopenedandthe structures identified. The thoracic duct was found between the aorta&theesophagusjustabovethediaphragm.Visualizationwasfacilitatedwithcream&methylenebluedyeadministeredviaanasogastric tube. The duct was ligated and divided between clips. Chesttubes(CT)wereplacedselectively.Datawasobtainedfromretrospective chart review. Results: Patient#1wasa12yofemale&weighed35.4kg.Shehadhadapreviousthoracotomyonthesameside.Operativetimewas131min.ShewasdischargedhomeonPOD3.ShehadasingularrecurrenceofPBapproximately16monthspost-operativelyafteranupperrespiratoryinfection.Sheiscurrently19monthspost-op. Patient#2wasa11yofemale&weighed40.1kg.Operativetimewas108min.Achesttube(CT)wasnotplacedduringtheinitialsurgery.OnPOD2shedevelopedapleuraleffusionthatwasconfirmedonthoracoscopicreexplorationtobeachyleleak.AdditionalclipswereplacedaswellasaCT.TheCTwasthenremovedonPOD2.ShewasdischargedhomeonPOD7fromtheinitialsurgery.Shehashadresolutionofhersymptomsover13monthsoffollow-up. Conclusions: Thoracoscopic thoracic duct ligation is a feasible techniquefortreatingPBevenifapatienthashadapreviousthoracotomy.Complicationscanbemanagedusingminimallyinvasive techniques with minimal morbidity.
S031USAGE OF SIMULATORS ON REAL ORGANIC INANIMATE MODELS FOR TRAINING IN NEONATAL THORACIC SURGERY, SoniaGuzman-MartinezMD,AlfonsoGalvan-MontañoMD,FernandoPuente-CompeanMD,SergioLanda-JuarezMD,WeimarMaldonado-ArzeMD,JoseA.AMartinez-Hernandez,FlorencioDelaConcha-BermejilloMD,GustavoJurado-BarriosMD,HospitalGeneralDr.ManuelGeaGonzalez [email protected]: The first models used for simulation of medical procedureswereperformedinthe17thcenturyinParis,France.These models evolved to virtual reality simulators. OBJECTIVE:Establishtheeffectivenessofaninanimatemodelwithorganic components of the oviparous family to develop surgical dexterity for neonatal thoracoscopy. MATERIAL AND METHODS: Bybuildinganinanimatesiliconmodelthat simulates reality in shape, texture and size of a newborn, incorporating organic components that include thorax previously removinganteriorthoraciccage,andneckleavingesophagusandtracheaintactitisfixedtothebase.Inserting23mmportsandone5mm port for the camera, dissecting and sectioning and carrying out the anastomosis of the trachea and followed by the same procedure for the esophagus Using30°5mmlensweincideonthesiliconmodelwithscalpelandintroduce lens and two ports. Next we proceed by dissecting the tracheafirst.Itissectionedentirelyandbothendsareseparated.Itisthenapproximatedandtracheoplastyispracticedbyplacingnon-absorbiblewithintracorporealandextracorporealknots.Afterthiswetakeontheesophagus,beingthelatteralessrigidstructurethe degree of dexterity increases significantly for dissecting and for anastomosis. DISCUSSION: Traditionally laparoscopic training has been done eitheronvirtualmodelsororganiclivemodels.Beingthefirstveryeffectivetheylacktextureandresistanceofrealtissue,thereforetheinconvenience for the student when presented with a live patient. Ontheotherhandlivemodelsprovidetextureandresistance,but are extremely expensive for the apprentice to continue until
ready for operating on a real patient even more if the patient is a newborn. Withtheexistenceofcongenitalpathologylikethecaseofesophageal atresia whose incidence is low, and the scarce experience on thoracoscopic surgery, we were launched to search for an organic model based on low cost which provides surgical dexterity. Therefore we manufactured a silicon model that simulated thorax and the abdomenofanewborn.Itissimilarinsizetexture,color,thickness,permeability,resistanceandflexibility.Highlightingthesimilarityin characteristics of the oviparous with the newborn as to texture size and resistance of tissue it is considered an excellent organic model to acquire neonatal thoracoscopic dexterity. The advantage of this model consists on the low cost considering the organic parts are of easy acquisition due to the regular human consumption of the donator and specially the introduction of the apprentice with the handling of delicate tissue of the newborn . These being characteristics that are absent in the virtual simulator for a rare pathologylikeesophagealatresia. CONCLUSION: Intheendourstudyrevealedsignificantimprovementintimemeasuredpractice.Consideringtheevaluationof faculty members and surgical residents, either of them with previous thoracoscopic experience.
S032“LASSO”- NEEDLE FOR VATS-AORTOSTERNOPEXY BY TRACHEOMALACIA, yuryKozlovMD,VladimirNovogilovMD,AlexeyPodkamenevMD,PavelyurkovMD,NatalyaAleynikovaMD,IrinaWeberMD,MarinaKononenko,SvetlanaKuznecova,VitalyKovalev,AndreyMachov,MunicipalPediatricHospitalIrkutsk,DepartmentofNeonatalSurgeryBackground. The thoracoscopic aortopericardiosternopexy proposedbyK.Schaarschmidtin2002istheprocedureofchoiceinseveretraceomalacia.Wereportamodifiedtechniqueofthisoperation with using original method of transduction of the aortic suture through sternum. Methods. The patient was intubated endotracheally with no attemptforsingle-lungventilationmade.Themidlineofthesternumwasmarkedfortheorientationoffutureinsertionoftheneedles.The three cannulae were inserted in a triangular configuration in the midaxillaryregionontheleft.CO2wasinsufflatedatapressureof4mmHgandaflow1L/min.Thethymuswasmobilizedandshiftedinto the left pleural cavity and the ascending aorta with pericardial reflectionandinnominatearterywereseen.Thesteelloop(“lasso”-shaped)wasinsertedintoenteringtipoftheinjectionneedle.Theneedle should be directed perpendicular to the sternum and passed throughthesternuminthemidlineintomediastinum.The“lasso”was passed to distal tip of the needle. Three longitudinal rows of strictlyadventitialprolenesutureswitharound-bodiedneedle(4/0)were placed from the innominate artery to the pericardial sleeve on the aortic root and the cranial pericardium. The distal tips of this sutures after remove of the suture needle were inserted in the steel loop.Theintroducingneedleconsisting“lasso”withaorticsuturewas removed under direct visualization. Underbronchoscopiccontrol,theaorticsuturesweretiedinthe presternal subcutis. There is no need to pull the aorta and innominate artery completely against the sternum. The lung was reexpanded. The incision after ports insertion was closed with adhesive strips. Results. Two children 3 and 6 months old with tracheomalacia were receivedathoracoscopicaoptopericardiosternopexy.Intraoperativetracheoscopy showed the trachea to be widely open. The patients were very well tolerated to the operation and can be rapidly extubated.Operatingtimewas80and90minutes.Therewerenopostproceduralcomplications–nobleedingandrepeatoftherespiratorysymptoms.Patientsweredischargedonthe9and14postoperative day. Conclusions. There is little experience with modified technique of the aortopericardiosternopexy. This technique gives excellent transsternal transduction of the aortic sutures and preservation of the intrathoracic structures.
S033LAPAROSCOPIC EXCISION OF AN ENDOSCOPICALLY IRRETRIEVABLE COLONIC POLYP, PeterFitzgeraldMD,WasmiAlfadhliMD,AnaSant‘AnnaMD,McMasterChildren’sHospital,Hamilton,OntarioBACKGROUND:Patientswithendoscopicallyirretrievablecolonic polyps traditionally have required open or laparoscopic assistedsurgicalremoval.Wepresentatechniqueofremoval

34 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Oral Abstractsof an endoscopically irretrievable colonic polyp by a completely laparoscopic approach. METHOD: Aneighteen-month-oldfemaleofAfricandescentpresented with intermittent abdominal pain and rectal bleeding. Colonoscopyrevealedalargeendoscopicallyirretrievablecolonicpolypofthedescendingcolon.Surgicalremovalinvolvedathreetrocarlaparoscopictechnique.Weidentifiedtheareaofthepolypand stabilized the bowel to the anterior abdominal wall with a singlesuture.Enterotomyandexcisionofthepolypwascompleted,followed by intracorporeal suture closure of the bowel. The specimen was left in the bowel and passed by the patient. RESULTS: The patient had an uneventful recovery from surgery and passedthespecimenonthesecondpost-operativeday.Pathologicanalysisofthespecimenrevealedalargejuvenilepolyp.Follow-up at three months confirmed no further bowel symptoms and an excellent cosmetic appearance of the abdominal wall. CONCLUSION:Laparoscopic“assisted”proceduresforcoloniclesions have been described. However, our technique fully utilizes the advantages of laparoscopic surgery by avoiding any extension ofatrocarincision.Additionaloptionsforspecimenretrievalarediscussed.
S034A MODIFIED NATHANSON STYLE LIVER RETRACTOR IS ABLE TO PROVIDE EXCELLENT EXPOSURE FOR PAEDIATRIC LAPAROSCOPIC FUNDOPLICATION., ColinLazarus,Milind Chitnis,ItayiSimango,MieElsen,EasternCapePaediatricSurgicalService,EastLondon,SouthAfrica.Particularlyininfancy,liverretractiontoprovideadequateexposurecan be to be one of the more problematic aspects of laparoscopic fundoplication.Snake,3finger,fanretractorsorlockingAllisandBabcockretractorsappliedtothecruraareallusedforthispurpose. Wehaveovercometheproblemofexposureofthehiatusbytheuseof a Nathanson style liver retractor whose atraumatic blades have been modified in size to provide a selection of 5 blades suitable for infants, children and adolescents. The retractor blade is inserted without a cannula through a 5 mm incision immediately below and to the left of the xiphoid, is placed under the left lobe of the liver which is elevated to provide access to the hiatus. The retractor is then fixed by an adjustable clamp to an armattachedtotherailofthetableonthepatient’sright. The shape of the Nathanson style retractor blades allows an even distribution of the liver lobe on the retractor. The particular value of the smaller blades is in ensuring the elevation of the left lobe itself. Whilethestemoflargerbladestendstoslipintotheinterlobarfissureallowingthelobetoflopdownwardsandthusdiminishingexposure, placing a smaller blade under the lobe itself ensures elevation of the lobe and enhances exposure of the hiatus. Wehaveusedtheretractorin42consecutivelaparoscopicfundoplications in the 3 year period to November 2008 without difficulty in insertion, any damage to the liver and with consistent excellent exposure of the hiatus.
S035CUTTING BALLOON DILATATION OF CONGENITAL URETERIC STRICTURES, BNarayanaswamyMD,LateWGManson*MD,AGWilkinsonMD,GAMacKinlayMD,RoyalHospitalforSickChildren,Edinburgh,UKBackground & Aim - Congenitaluretericstricturesareararecauseof upper urinary tract obstruction for which surgical management hasbeenreported.Balloondilatationhasbeenperformedinadultswith ureteric strictures resulting from previous surgery or secondary totuberculosisorschistosomiasis.IthasalsobeensuccessfullyundertakenforPUJobstructioninadultsandchildren.Wedescribeour novel use of cutting balloon dilatation in the management of congenital ureteric strictures in two children. Patients - Two boys, each with a unilateral congenital ureteric stricture have been treated at our institution during the period 2007-2008.OnechildpresentedwithantenatallydiagnosedLefthydronephrosis and the other presented with recurrent episodes of abdominalpainoveraperiodof7years.Inbothchildren,imagingshowed hydronephrosis and a dilated proximal ureter as well as failure of drainage on diuretic isotope renography. The latter child had significant deterioration in function to 30% on the affected side. Procedures & Outcome - Afterconfirmatoryretrogradestudies,both children underwent attempted conventional balloon dilatation of their ureteric strictures, at 18 months and at nearly 11 years of age respectively.Althoughthisfailedtoabolishthestrictures,subsequentuseofacuttingballoonprovedsuccessful.Follow-upultrasound
andisotopescansapproximately6monthspost-procedurehaveconfirmed resolution of dilatation and significant improvement in drainage in both children as well as good recovery of function to 45%inthelatterchild.Bothchildrenremainclinicallywellat21and7months’follow-uprespectively. Conclusion -Webelievethistobethefirstdescriptionofcuttingballoon dilatation for paediatric congenital ureteric sticture, which is a feasible, effective and minimally invasive treatment option. *WGMansonpassedawayinMay2008.Thisabstractissubmittedinhis memory.
S036IMPROVEMENT OF TRACHEAL COMPRESSION AFTER PECTUS EXCAVATUM REPAIR, GoMiyanoMD,RomeoCIgnacio,Jr,RobertEWoodMD,ThomasHIngePhD,CincinnatiChildren’sHospitalMedicalCenterA4year-oldfemalepresentedwithahistoryofmultipleepisodesof respiratory infections since infancy and was diagnosed with tracheomalacia(TM).Duetothepresenceofpectusexcavatum(PE),thathadgraduallyworsenedsinceinfancy,aortopexywasnotconsideredtobeatechnicallyfeasiblenorlikelysuccessfultreatmentforherTM.However,minimallyinvasivePErepairwassuccessfullyperformed in an effort to correct her TM. Her intraoperative course was uneventful, and postoperative bronchoscopic view demonstrated themarkedimprovementoftheairwaycaliber.At2yearsfollow-upsince the bar was removed, chest wall appearance is normal and she has remained asymptomatic, even with exertion. Minimally invasive PErepairshouldbeconsideredasatreatmentoptionforTMwhenthe two conditions coexist.
S037MINIMALLY INVASIVE, LAPAROSCOPIC-ASSISTED, PERCUTANEOUS LIVER BIOPSY IN CHILDREN, RichardCarterMD, MartinGrahamMD,DavidLanningMD,VirginiaCommonwealthUniversityHealthSystemBackground:Acommonapproachforliverbiopsyinchildrenisultrasound-guidedpercutaneousneedlebiopsy.Theonlymethodof hemostasis is for the child to lay on their right side for an extendedperiodoftime.Bleedingofsomedegreeisinvariableandismonitoredbyserialhemoglobinlevels.Childrenoftenhave abdominal pain and some require abdominal imaging, a blood transfusion, or even surgical intervention. To minimize bleeding, small biopsy needles are often used, which can result inaninadequateamountoftissuefordiagnosis.Wepresentourexperienceusingaminimallyinvasive,laparoscopic-assisted,percutaneous technique for obtaining a liver biopsy. Methods: Laparoscopic-assistedliverbiopsywasperformedon13 patients. The technique involved placing a 3 or 5 mm trocar attheumbilicusandcreatingapneumoperitoneum.Astandardlaparoscopichookcauterywasplacedthroughasmallstabincisionintheepigastrium.A14gaugetru-cutbiopsyneedlewasthenplacedthroughasmallnickintheskinintherightupperquadrant.After2to4corebiopsieswereobtainedwiththeneedle,thehookcauterywasusedtoobtainhemostasisatthepuncturesites.Woundswereclosedinstandardfashionafterinjectinglocalanesthesia.Wereviewed records of children who underwent this approach for liver biopsyfrom2005-2008.Adequacyofspecimen,lengthofhospitalstay, and complications associated biopsy were examined. Results: Patients3monthsto16yearswithmildtosevereliverdiseaseunderwentbiopsy.Specimensobtainedwerealladequatefordiagnosis.Elevenpatientsweredischargedonthesamedayasthe procedure once recovering from anesthesia. Two patients had additional procedures and were admitted for reasons unrelated to the biopsy. There were no intraoperative or postoperative complications. Conclusions:Potentialforpost-biopsybleedingwithacuteorchronicliverdiseaseisasignificantconcern.Wepresentatechniqueoflaparoscopic-assisted,percutaneousliverbiopsythatoffersasafeand cost effective method for the diagnosis and staging of liver disease in children. For patients with mild to moderate disease we feel that this technique offers a safe method for obtaining adequate tissue for diagnosis in the setting of a same day procedure thus reducing medical cost. Furthermore, for patients with advanced disease, this technique allows collection of an adequate biopsy utilizing a minimally invasive approach where hemostasis is ensured.

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 35
2009 Oral AbstractsS038ESOPHAGEAL MANOMETRY IN POSTOPERATIVE ACHALASIA REPAIR,MelissaLoganMD,PrithviReddyMD,RathnaAmarnathMD,JuanCampsMD,PalmettoHealthChildren’sHospitalBackground: Achalasiaisararediseasewithanincidenceof1in100,000people,andonlyaminorityaffectingchildren.Itis,however,associatedwithsignificantmorbidity.Wedescribeamodifiedsurgical approach to the treatment of achalasia using a laparoscopic anteriorcrura-myotomyplicationandpartialanteriorfundoplication.The purpose of this study is to analyze the esophageal function in pediatric patients after surgical intervention for achalasia. Methods: Between2003and2008twelvechildrenunderwenttheproposed technique and have been followed for an average of 33.2 months.UnderIRBapproval,allpatientshavehadapostoperativemanometrytoassestheesophagealfunction.Allpatientshadesophagogram, esophageal manometry and one time endoscopic esophageal dilatation prior to surgery. Results: Allcaseswereperformedsuccessfullybylaparoscopywithnoimmediatepostoperativecomplications.Onepatientrequired an additional pyloroplasty at the initial surgery because of a poor gastric emptying. Two patients developed postoperative symptomsofdysphagiawithinthefirst6monthsfromsurgery.Atight anterior gastric fundoplication was the cause of dysphagia and corrected after laparoscopic surgical release of the stomach wrap.AveragepreoperativeLESPwas48.25mmHgandwasreducedtonormalinallpatientswithanaverageofLESPof11.69mmHg.AveragepreoperativerestingLESPwas26.51mmHgcomparedtopostoperativeaveragerestingLESPof4.07mmHg.Thereisnoimprovement in the underlying esophageal motility dysfunction despiteimprovementonthepatient’ssymptoms.Therewasanaverage of only 15% of postoperative esophageal coordinated contractions and an average of 60% of retrograde contractions ornonpropulsiveesophagealcontractions.Despiteofsymptomsimprovement, manometry esophageal peristalsis has shown no differencesfrompreoperativeandpostoperativevalues.Allpatientsareeatingregularsoftdiet.Somepatientshavehadvaguesymptomsofchestpainorheartburnmostlikelyrelatedtoesophagealpoormotilityorgastro-esophagealreflux. Conclusions: Despitethedramaticclinicalimprovementofthese12patients tolerating regular diet, esophageal manometry study has shown poor real functional improvement of the esophageal motility. However, decreasing significantly the lower esophageal resting pressure seems to be the only factor that surgery can do to help this patients with achalasia.
S039LAPAROSCOPIC LADD’S PROCEDURE: SAFE, WITH IMPROVED SHORT-TERM RESULTS., RavindraKVeguntaMD,KavithaKalvakuriMD,AmyBStanfillMD,LizabethJWallaceMS,RichardHPearlMD,UniversityofIllinoisCollegeofMedicineatPeoriaandChildren’sHospitalofIllinois,Peoria,IllinoisIntroduction:LaparoscopicLadd’s(LL)procedureiscurrentlynotwidely accepted for management of malrotation of the midgut in children.SinceMay2004LLhasbeenthestandardapproachinourinstitution. Method:IRBapprovedretrospectiveanalysisofallLadd’sproceduresinourinstitutionbetweenSeptember1998andJune2008comparingopen(OL)andLL.Patientswithdiaphragmaticherniaandgastroschisis are not included. Results: Atotalof156childrenunderwentLadd’sprocedureduringthestudyperiod.Therewere120inOLand36inLL.Seetable:
Allnumbersexcept‘woundinfection’aremediansOL LL p-value
DOS 76 75 0.22Sartfeeds-days 4 1 0.001Fullfeeds-days 6 2 0.001LOS-days 7 3 0.001Woundinfection 14(11.7%) 0 0.041
DOS:durationofsurgery;LOS:post-opstayConversionrateinLLwas8.3%.RecurrentvolvulusfollowingLadd’sprocedurewasseenonceinOLandtwiceinLL.Bowelobstructionledtore-admissioninOLin13.3%ofthegroupandnoneinLL. Conclusion:Inelectiveandsemi-electivesituations,Ladd’sprocedurecanbeperformedsafelybylaparoscopicmeans.Short-termresultsaresuperiorinLLcomparedtoOL.
S040THE SAFETY OF LAPAROSCOPY IN PEDIATRIC PATIENTS WITH VENTRICULOPERITONEAL SHUNTS, JasonDFraserMD,PabloAguayoMD,SusanWSharpPhD,DanielJOstlieMD,GeorgeWHolcombMD,ShawnDSt.PeterMD,TheChildren’sMercyHospitalIntroduction:Inthepediatricpatientsrequiringabdominaloperations,ventriculoperitoneal(VP)shuntsforhydrocephalusareafrequentlyencounteredco-morbidity.Laparoscopyhasnotbeenextensively evaluated in this population and there is concern about thesafetyofinsufflationunderpressurewiththeshuntinplace.There is a paucity of data in the literature to address this issue. Therefore,wereviewedofourexperienceinpatientswithVPshuntswho underwent either open or laparoscopic abdominal procedures to determine the safety of laparoscopy in these patients. Methods:WeconductedaretrospectivereviewofallpediatricpatientswithVPshuntswhounderwentlaparoscopicand/oropenabdominaloperationsatasingleinstitutionfrom1998-2008.Complicationsweredefinedasashuntorsurgery-relatedevent(includinganyshuntrevisions)withinsixmonthsofabdominalsurgery.Continuousvariableswerecomparedusinganindependentsample,2-tailedStudent’sttest.DiscretevariableswereanalyzedwithFisher’sexacttestwithyatescorrectionwhereappropriate.SignificancewasdefinedasPvalue<of0.05. Results: Atotalof91intraabdominaloperationswereperformedonpatientswithVPshunts,47laparoscopicand44open.Meanagewas3.17versus2.93yearsrespectively(p=0.37).Thedistributionofoperations is listed in Table 1.There were no episodes of air embolism into the shunt. There was one shunt infection in the laparoscopic groupandthreeintheopengroup(p=0.57). Table1.Distributionsofproceduresperformed
Conclusions: Ourdatasuggestthatlaparoscopyissafeinpatientswith ventriculoperitoneal shunts.
S041RISK OF VENTRICULOPERITONEAL SHUNT INFECTIONS AFTER LAPAROSCOPIC PLACEMENT OF CHAIT TRAPDOOR™ CECOSTOMY CATHETERS IN CHILDREN, SANIZyAMOUTMD, BETTyJHUOMD,VEETAILIMD,MAURICIOAESCOBARMD,MICHAELGCATyMD,WomenandChildren’sHospitalofBuffaloINTRODUCTION: LaparoscopicplacementofChaitTrapdoor™cecosotomy catheters has been practiced in our institution since 1999.Chaitcecostomycathetersallowantegradeirrigationofthecolon without the complications associated with appendicostomies. The use of laparoscopy allows precise placement of these catheters intothececum.AlthoughplacementofChaitcathetersunderdirectvisionmaymakethisproceduresafer,thepresenceofaconcomitantventriculoperitoneal(VP)shuntinpatientswhoundergocatheterplacement raises concerns for the potential for shunt infection.MATERIALS AND METHODS: This is a retrospective review of all patientswithVPshuntswhounderwentlaparoscopicplacementofaChaitcecostomycatheterfrom1999to2008.Werecordedpatientdemographics, duration of operation, hospital stay, follow up duration, and incidence of shunt infection.RESULTS:SixteenpatientswithspinabifidaandVPshuntswhounderwentlaparoscopicplacementofVPshuntinfectionswereidentified.Thereweretwelvemales.Meanfollowupwas46±27months(range,3to87months).Meanoperativetimewas90±55minutes(range,45to235minutes).Meanhospitalstaywas3±2days(range,1to6days).Twopatients(12.5%)hadaVPshuntinfectionsrelatedtotheplacementoftheircecostomycatheter.Oneshunt infection occurred five days postoperatively and the other occurred several years later, when the shunt and cecostomy catheter tractsmergedinthesubcutaneoustissue.Bothpatientsunderwentshunt externalization, and subsequently did well.CONCLUSION: CecostomycatheterplacementinpatientswithpreexistingVPshuntsmayincreasetheriskofshuntinfections.OurseriesillustratestwodifferentmechanismsbywhichaVPshuntcangetinfectedaftercecosotomycatheterplacement.Inthefirstcase,leakageofentericcontentfromapoorlysealedtractprobably

36 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Oral Abstractsresulted in the shunt infection. More secure fixation of the cecum to the abdominal wall, using intracorporial sutures rather that T-fasteners,mayavoidthiscomplication.Thesecondcomplicationmight have been avoided if the cecostomy catheter had been placed furtherawayfromtheVPshunt.
S042LAPAROSCOPY-ASSISTED STOMA CLOSURE IN CHILDREN: OUTCOME COMPARISON WITH CONVENTIONAL OPEN APPROACH, GoMiyanoMD,ManabuOkawadaMD,ToshihiroyanaiMD,TadaharuOkazakiMD,GeoffreyLaneMD,AtsuyukiyamatakaMD,JuntendoUniversitySchoolofMedicinePurpose: This study was conducted to compare outcome of stoma closure(SC)withorwithoutlaparoscopicassistance(LA). Methods: Datafrom44consecutivepatientswhounderwentSCbetween 2005 and 2008 were collected prospectively and analyzed according to incidence of postoperative wound infection and adhesivebowelobstruction.AllSCwithLA(LASC)wereperformedbythesame2pediatricsurgicaltrainees,andconventionalSCwithoutLA(CSC)wereperformedbyboardcertifiedpediatricsurgeons.Woundinfectionswereclassifiedas:Grade-1:superficialrednessnotrequiringantibioticsordrainage,Grade-2:requiringantibioticsonly,andGrade-3:requiringdrainage.Thesameantibioticswereusedinbothgroups.Bowelobstructionswereclassifiedas:Grade-1:requiringnasogastrictubedecompressiononly,Grade-2:requiringnasojejunaltubedecompression,andGrade-3:requiring laparotomy. Results: Ofthe44patients,22hadLASCand22hadCSC.Ageatstomaclosure(LASC1.5yr;CSC2.3yr),durationoffollow-uplength(LASC1.7yr;CSC1.9yr),indications(anorectalmalformation,Hirschsprung’sdisease,intestinalatresia,meconiumplugsyndrome,etc),andlocation/typeofstomaweresimilarforbothgroups.Meanoperativetimewas136minutesforLASCand114minutesforCSC(p=NS).Therewerenointraoperativecomplications.Postoperatively,woundinfectionsweresignificantlymilderinLASC(p<.05).Specifically,inLASC,only2Grade-1infectionsoccurred,butinCSC,1casehadGrade-1,2hadGrade-2,and3hadGrade-3.Noincisionalherniaswereidentifiedineithergroup.Incidenceofbowelobstructionwasnotsignificantlydifferent(p=NS:LASC:1caseinGrade-1,2casesinGrede-2,nocasesinGrade-3;CSC:1caseinGrade-1,3casesinGrade-2,nocasesinGrade-3). Conclusions: This is the first report to compare outcome between LASCandCSCinchildren.LASCappearstobeassociatedwithlowerincidenceofwoundinfectioninchildreneventhoughSCwasperformed by more junior staff.
S043LAPAROSCOPIC NISSEN FUNDOPLICATION IN VERY SMALL PATIENTS, CarlosGarciaHernandezMD,LourdesCarvajalFigueroaMD,JuanCarlosDueñasRamirezMD,HospitalInfantilPrivadoBackground: The difficulty to perform minimal invasion procedures in small patients has limited its use despite of the benefitsofthistechniqueprovedbyRothenbergandIwanaka.Thegastroesophagealrefluxdiseasethataffectssmallpatientsthreattheir lives, because of this it is necessary to carry on a surgical treatment in complicated patients that will indeed benefit if the procedure was performed by laparoscopic means. Methods:BetweenMarch1999andOctober2008,wehavecarriedon a surgical procedure of Nissen Funduplication in 1312 patients using laparoscopy. The patients of this group whose weights were below 3000 grams were selected. Results: 22 patients with weights between 1480 and 2900 grams (X=2.27kg)weresubmittedtosurgery,ofthistotal9hadcyanosis,7 had apnea and 6 had pneumonia. Most of the subjects were premature and they had as certain anomalies; one had a cloacal malformation, two of them esophageal atresia, one duodenal atresia , , three anorectal malformation, one Hirschprung, one withpolycystickidneysaswellasonewithhydrocephalyandonewithaorticcoarctation.Ofthesesubjects5ofthemhadcolostomy,2 with renal insufficiency with peritoneal dialysis and 1 with aventricleperitonealvalve.In21patientstheprocedurewasperformed without complications, one conversion due to ventilatory difficulties.In6withperformedgastrostomy.Averagesurgicaltime of 59 minutes, oral feeding after 25.2 hours. 5 of the patients sufferedpostsurgicalpneumonia.Allofthemhadcontroloftherefluxsymptomatology3ofthesepatientsdied,2ofthemofrenalinsufficiencyandoneasacauseofanon-relatedsepsisaftertheprocedure. Conclusion: Theverysmallpatientwithweightslowerthan3kgis
benefited when a minimal invasion procedure is carried on. However aslimitswehave:-1)Workinginsmallerspacesthatarealsosharedwithcolostomiesandcatheters,2)Theventilatorproblemsduetothepneumoperitoneum,sowehavetoinsuflatedthemwithlowerpressuressmallerthan8mmHg.And3)ThepatientstendtohavehypothermiawhichaggravatesiftheCO2isprovidedfortoolong.Ifthesecomplicationsaren’tpresentedthentheprocedureisfeasibleto perform by laparoscopic approach
S044LONG-TERM FOLLOW-UP AFTER LAPAROSCOPIC GASTROPEXY IN CHILDREN WITH GASTRIC VOLVULUS., MarioMendoza-SagaonMD,OlivierReinbergMD,AlexandreDaraniMD,RudolfLeuthardtMD,DepartmentofPediatricSurgery,CentreHospitalierUniversitaireVaudoisandOspedaleRegionalediBellinzonaeValli.Switzerland.The aim of this study was to evaluate the long term results of our technique of laparoscopic gastropexy in children with gastric volvulus.Methods:Thefilesofallchildrenwithgastricvolvulusoperatedwithalaparoscopicgastropexyin2Swissmedicalinstitutionswereanalyzed.Results:Fifteenchildrenwereincludedinour study. Range of age was between 1 and 11 months at the time of surgery. Main symptoms included sudden postprandial crying, probablyrelatedtoabdominalpain,vomitingandirritability.In3 patients, apneic episodes associated with cyanosis, pallor and hypotoniawererecorded.InallcasesthediagnosiswasestablishedwithupperGIseries.Organo-axialgastricvolvuluswasfoundinallcases.Thelaparoscopicgastropexywasperformedwithan8-mmHgCO2-pneumoperitoneumusing3-mminstrumentsanda5mmtelescope.Ourtechniqueincludes3steps:1)esophagofundopexy,2)phrenofundopexyand3)anteriorgastropexy.Averagetimeofsurgerywas60minutes.Oneconversionwasperformed.Follow-uprangedfrom1yearto8years.Onepatientneededalaparoscopichemifundoplicationforapersistentgastro-esophagealrefluxoneyear after the gastropexy. To date, all patients are free of symptoms .Conclusion:Ourtechniqueoflaparoscopicgastropexyisagoodoption and offers excellent results in children with gastric volvulus.
S045LAPAROSCOPIC ENDORECTAL PULL-THROUGH FOR HIRSCHSPRUNG’S DISEASE – 10 YEARS EXPERIENCE, ClareMReesMD,NiamhGeogheganRN,DianedeCaluweMD,SimonClarkeMD,MuntherHaddadMD,Chelsea&WestminsterNHSFoundationTrust,London,UKAims: Todescribeourexperienceoflaparoscopicendorectalpull-through and investigate long term outcomes of this procedure. Methods:AllchildrendiagnosedwithHirschsprung’sDisease(HD)from1999-2008wereidentified.Casenotes,radiologyandpathologyreportswerereviewed.Patientswhohadendorectalpull-throughforHDhaddetaileddataextractedandanalysed.Dataarepresentedas%andmedian(range).MannWhitneytestwasusedforcomparisonsand p<0.05 considered significant. Results: Of74patientsidentified,68hadaconfirmeddiagnosisofHD.45(66%)hadendorectalpull-throughastheirdefinitiveprocedure,11hadotheroperations;79%weremale.Diagnosiswasmadeonsuctionrectalbiopsyin27/50(54%)patients,16%had>1biopsy.Diagnosiswasmadeatamedianageof32days(range1dayto9years),ageatopenbiopsywas470days,comparedto12daysforsuctionbiopsy(p=0.001).Patientsweremanagedwithrectalwashouts(62%)orlaxatives(29%)untildefinitivesurgery.Plannedlaparoscopicendorectalpull-throughwasperformed4monthsafterdiagnosis(range0.5-52)atamedianageof7months(1.8months-13yrs).3patientsunderwentlaparoscopicassistedDuhamelforlongsegmentdisease(2converted).Medianpost-operativestaywas4days(range2-11).Patientswerefollowedupfor20months(range1-118).27%hadepisodesofenterocolitis(EC);patientshadamedianof4hospitaladmissions(range1-29),significantlyhigherinpatientswhohadEC(6vs.3,p=0.03).Atfollowup13%wereconstipatedand33% had some degree of faecal incontinence. 18% required anal dilatationand4%hadanACEprocedure.6patientshadsignificantcomplications, requiring multiple operations and stoma formation. Overall36%werefelttohavegoodpost-opsatisfaction,42%fairand 21% poor outcome. Conclusions:Endorectalpull-throughisthemanagementofchoiceinourinstitutionforpatientswithrectosigmoidHD.Patientscanbe managed safely at home with rectal washouts and operation performedsomemonthslater.Continenceoutcomesappearpoorerthan published data but constipation and enterocolitis are reduced, and families are generally satisfied with the results.

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 37
2009 Oral AbstractsS046AIR INSUFFLATION OF THE STOMACH FOLLOWING LAPAROSCOPIC PYLOROMYOTOMY DOES NOT RELIABLY DETECT PERFORATION, StevenLLeeMD,RomanMSydorakMD,StanleyTLauMD,KaiserPermanente,LosAngelesMedicalCenterPurpose: Undetectedperforationduringlaparoscopicpyloromyotomycanbefatal.Detectingaperforationatthetimeoflaparoscopic pyloromyotomy is difficult. The purpose of this study is todeterminewhetherairinsufflationofthestomachreliablydetectsperforation during laparoscopic pyloromyotomy. Methods: Aretrospectivereviewofallpatientswhounderwentlaparoscopicpyloromyotomyfrom2007-2008wasperformed. Results: 61 patients underwent laparoscopic pyloromyotomy and 2patients(3.3%)hadperforation.Oneperforationoccurredatthegastric end of the pylorus and the other occurred in the middle of thepyloromyotomyattheinferioredge.Insufflatingthestomachwithairdidnotdemonstratetheperforationinbothcases.Bothperforations were detected by careful inspection of the myotomy; asmallamountofmucuswasseenattheperforationsite.Bothpatientsunderwentopensuturerepairwithanomentalpatch.Bothhadunremarkablepostoperativecourses. Conclusions: Airinsufflationofthestomachduringlaparoscopicpyloromyotomydoesnotreliablyrule-outperforation.Ahighindexof suspicion and careful inspection of the entire myotomy may help detect perforation.
S047TECHNICAL CHALLENGES OF THE LAPAROSCOPIC APPROACH FOR PATIENTS WITH ANORECTAL MALFORMATION AND RECTOBLADDERNECK FISTULA, AndreaBischoffMD,MarcALevittMD,BelindaDickieMD,AlbertoPenaMD,CincinnatiChildrenHospitalIntroduction: Laparoscopy is ideally indicated to replace laparotomy, when the rectum can not be reached posterior sagitally because it is locatedveryhighinthepelvis(rectobladderneckfistula).Inmales,thisonlyoccursin10%ofcases.Wereportthetechnicalchallengesthat we found during the laparoscopic approach for patients with anorectalmalformationandrectobladderneckfistula. Methods: Aretrospectivereviewofourlastsixcaseswithrectobladderneckfistulawasconducted,withspecialemphasisonthetechnical challenges encountered during the laparoscopic approach. Results:Inallsixcasesthefistulacouldbeligatedlaparoscopically.Following fistula ligation, all rectums required dissection and ligation ofseveralinferiormesentericarterybranchestogainlength.Onecase was repaired entirely laparoscopically. The other five were considered laparoscopically assisted, since an abdominal incision was requiredto:takedownamucousfistulawhenthecolostomywasplacedtoodistalinthesigmoid(2),mobilizeahighrectumwithadifficultmesentericarcadedissection(2),andtotaperabulbousdistalrectum(1). Conclusion: Laparoscopy provides excellent exposure of the peritonealfloor,whichallowsanaccurateandsafedissectionandligationofarectobladderneckfistula.Anincorrectplacementofthecolostomyinthesigmoidmaylimitthepull-throughandthelaparoscopic approach. Limitations also might be found in identifying and safely cauterizing branches of the mesenteric vessels to gain length on a very high rectum, and in order to taper a dilated rectum.
S048WRAP IT, STITCH IT AND PATCH IT! – A NEW TECHNIQUE IN LAPAROSCOPIC FUNDOPLICATION, AniruddhVDeshpandeMD, StephenFarrellMD,IreneTsang,AlbertShunMD,Children’sHospitalatWestmead,Sydney,Australia.Background-Thecommonestcauseoffailureofsurgicaltreatmentofgastroesophagealrefluxinchildrenisthefailureofthehiatalrepair.Recently, we have adopted the technique of reinforcing the hiatal repair with a bioprosthetic patch. Aim: The aim of this study is to report the novel use of a bioprostheticpatch(Surgisis,CookSurgical,Inc.)inlaparoscopicfundoplication in children, and to report the initial results of its safety and efficacy. Methods:Thisstudyincludedallpatientswhohadundergonelaparoscopicfundoplicationbyasinglesurgeonbetween2001-7andwasapprovedbytheHumanResearchEthicsCommittee.Alleligiblepatients were recruited to the study by a letter. Surgical technique-Allpatientsinthisstudyunderwenta360degreelooselaparoscopicNissen’sfundoplication.Thehiatuswas
repairedwithinterruptedstitchesof2(0)Ticron–(Group1,n=59).Insome, the hiatal repair was additionally reinforced with a patch of Surgisiswhichwasstitchedtothehiatusandtheposterioraspectofthefundalwrap(Group2,n=16).<@> Follow-up -The patients were prospectively assessed as outpatients by a blinded independent surgical trainee using a validated questionnaire and barium studies were performed in the symptomaticpatients.Informationwasobtainedonsymptomsintheimmediate postoperative period as well as at the time of assessment forthestudy.Datawasanalysedfortheincidenceofsymptomsandrecurrent hiatal hernia in the 2 groups as well as any side effects of the procedure. Results: Intotal,75(16withSurgisis)eligiblepatientswereidentifiedandtodate,25(5fromGroup2)patientshavebeenassessed.Themedianageforthegroupis75months(range18-196months).Themeanfollow-upforthegroupis90months,whilethatfor the group 2 is 26 months.There was a trend towards an increased incidence of dysphagia and gagging after feeds in the immediate postoperativeperiodinGroup2whichresolvedovertime.Threepatients(15%)inthegroup1hadradiologicallyconfirmedhiatalhernia recurrence, no patient in group 2 had evidence of recurrence. There were no side effects or complications associated with the use ofSurgisispatch. Discussion: This is the first report of use of a bioprosthetic patch in fundoplicationinchildren.Althoughthestudyisinitsinitialstages,the early comparative trend from the available data suggests that its use is safe and may provide a clinical benefit as has been shown in adults.
S049NEW TECHNIQUES AND LATE RESULTS OF LAPAROSCOPIC SUBTOTAL >90% SPLENECTOMY FOR HAEMOLYTIC ANAEMIA OR ITP IN CHILDREN AND ADOLESCENTS, KlausSchaarschmidtMD,AndreasKolberg-SchwerdtMD,MichaelLempeMD,FrankSchlesingerMD,IrinaHayekMD,JanPatino-Meyer,HeliosCenterforPediatric&AdolescentSurgery,Berlin-Buch,GermanyIntroduction: Splenectomyshouldbeavoidedinyoungchildrenbut also adolescents with symptomatic haemolytic disease becauseaperfusedsplenicrestmostlikelyeliminatestheriskofpostsplenectomy sepsis. Moreover laparoscopic subtotal splenectomy affordssymptomaticreliefinrarerhematolgicdiseaseslikePyruvatkinasedeficiency,Thalassaemia,Hypersplenism,Feltysyndrome,severelytransfusiondependentITP,andrecurrentspleniccystsorhemangiomas. Methods and Procedures: Inthe15-yearperiod7/1993–6/2008,out of 197 total laparoscopic splenic procedures 128 children and adolescentsaged7.2±3.7years(range1.1-28.2years)receivedsubtotallaparoscopicsplenectomywithfollowupof3.6±1.9years(range10.4-0.6y).Mostpatientsrequiredbloodtransfusions,mean3.4±4.1(range0-189)orupto342Thrombocyteand/orimmunoglobulin transfusions. Spleensizesrangedfrom8,9-41cm,overlargespleensweredeliveredinseveralbagstransumbilically.From3-55mm-portspolarvesselswere preserved and the spleen divided by ultrasonic scalpel retaining 10.5±4%ofsplenicvolume.2subtotalsplenectomiesweresuccessful redos of insufficient partial splenectomies elsewhere. Results: There were 2 conversions and 3 relaparoscopies due to haemorrhageresultinginresectionof2splenicrests.Afterinitialviability of all splenic rests late viability could not be proven in 4 patients.Inallotherslateviabilityofthesplenicrestswasprovenbydopplersonography and scintigraphy, Hemoglobins rose permanently andsignificantly(p<0.0001)from6.9±1.3g/dl(lowestpreop)to13.1±1.1g/dl(lowestpostop). There was moderate regrowth of all spleens by up to 50% predominantly during the first year, but only 4 required late laparoscopicremovalofthesplenicrestafter3.1±1.6y(range0.8-4.1)3forrecurrenthemolysis,1duetohyperbiliruinaemia. Conclusions:Meanfollow-upof3.6±1.9yearsisstillshort,butaccording to the present data laparoscopic subtotal splenectomy reduces transfusion requirements effectively for years. New and rare indications and new techniques are presented.
S050LAPAROSCOPIC SPLENECTOMY AND PERICARDIAL DEVASCULARIZATION WITH ENDOLIGATURE FOR PORTAL HYPERTENSION IN CHILDREN, SuolinLIMD,ZengwenyU,yinghcaoLI,DepartmentofPediatricSurgery,2ndHospitalofHebeiMedicalUniversity,Shijiazhuang,050000,China.Objective The aim of this study was To explore the clinical effects

38 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Oral Abstractsof laparoscopic splenectomy and pericardial devascularization with endoligature for portal hypertension complicated hemorrhagic varices in children. Methods From 2003 to 2007, 6 children with portal hypertension complicated hemorrhagic varices. There were 5 males and 2 females.Agerangewasfrom8to17years.Byusingsilkligatureandhamonicscapel or Ligasure, six patients underwent laparoscopic massive splenectomy and selective pericardial devascularization. Results Alltheoperationswerecompletedsuccessfullyundertotal laparoscope. The intraoperative average blood loss was 150 ml(80¡ª200ml).Noneofthepatientsrequiredbloodtransfusionorconversion to an open procedure. The operatinn time was 180¡ª270 minutes(mean,210minutes).Therewerenosurgicalcomplications,and all patients had returned to usual activity by 5 days. There weren¡¯t recurrent variceal hemorrhages by following up of 8 to 40 months. Conclusions Laparoscopic massive splenectomy with selective pericardial devascularization with endoligature is a feasible, effective, safe, little blood loss and minimally invasive procedure for portal hypertension with esophagogastric varices.
S051LAPAROSCOPICALLY ASSISTED PULLTHROUGH FOR HIRSCHPRUNG’S DISEASE: THE EDINBURGH EXPERIENCE, GillianDuthie,MaryamDavoodi,DerrickWilson-Storey,RoyalHospitalforSickChildren,EdinburghIntroduction: SurgicalmanagementofHirschprungsdiseasehas evolved over the past two decades with minimally invasive techniquesnowattheforefront.Wereviewourunit’s10yearexperienceoflaparoscopicallyassistedpullthroughforHirschprung’sDisease. Methods: PatientswereidentifiedfromtheLothianSurgicalAuditSystem.Atenyearperiodwasanalysed.Thecasenotes,pathologyand radiology were also reviewed. Results: 33 patients underwent a laparoscopically assisted pullthrough. 73% were male. The age at presentation ranged from 1dayoldto2yearsofage.97%werebornatterm.Sevenpatientspresentedoutwiththeneonatalperiod.Ageatdiagnosisrangedfrom 3 to 732 days of age with age at operation ranging from 34 to762days.Onlyfivepresentedwithfailuretopassmeconium,biliousvomitingandabdominaldistension.Onepatientpresentedwithenterocolitis.Averagelengthofstaywasoneweek.Contrastenemas were performed in 30 patients of which 4 failed to identify a transition level. Radiology matched pathology in terms of the transition zone in 56%. 6.5cm of ganglionic bowel was removed on average with 11.4cm of aganglionic bowel excised. 40% of patients had a complication. These included 33% with enterocolitis. Two patients required colostomies for recurrent enterocolitis whilst one patient had a post operative perforation requiring a colostomy. 20 patients required admission following their pullthrough with a total of 82 admissions. 7 were admitted for dilatation and four for manual evacuations.At3/12postpullthrough70%werestooling1-3timesdaily.At6/12followup50%werestooling1-3timesdailywith4patientsonlaxativesandtwoundergoingwashouts.At1year60%hadregularstooling.At2yearspostsurgery63%werestoolingregularly with two patients on laxatives and one undergoing regularwashouts.At4yearsfollowupthemajoritywerestoolingsatisfactorily but with 75% on laxatives. Conclusion:MinimallyinvasivesurgeryforHirschprung’sDiseasehasbeendescribedasthegoldstandard.SurgeryforHirschprung’sisnotwithoutitscomplicationsregardlessofthetechniqueemployed.Ourseries reports a high frequency of enterocolitis and constipation in comparisontopreviousstudies.Itdoeshoweverreportgoodoveralloutcomes.Asaresultofthisreviewwearenowroutinelycalibratingall patients.
S052LAPAROSCOPIC ASSISTED ANTERIOR GASTROPEXY FOR PRIMARY GASTRIC VOLVULUS IN CHILDREN, PaulCyChangMD, Ming-LunyehMD,Beng-HuatLouMD,Chih-ChunChaoMD,ShinKong Memorial Hospital, Taipei, TaiwanBACKGROUND/PURPOSE:Non-acuteorchronicgastricvolvulusisrareandusuallymoredifficulttodiagnose.Inpatientswithprimarygastric volvulus, there are no associated etiologies such as previous surgery, diaphragmatic hernias, or hiatal hernias. The authors report 3patientswithprimary,non-acute,intermittentgastricvolvuluswhowere treated successfully by laparoscopy. MATERIALS/METHOD: Thefirstpatientwasahealthy,7-day-oldneonate,whopresentedwithintermittentnon-biliousvomiting
andmilddehydration.Pyloricstenosiswasexcludedbyabdominalultrasound.BariumupperGIserieswasdiagnostic.Laparoscopicanterior gastropexy was performed with a single 5.5 mm trocar via the umbilicus. The greater curvature of the stomach was sutured to the anterior abdominal wall via three sutures which were inserted percutaneouslyandtiedsubcutaneously.Webelievethiswastheyoungest patient in the literature with primary gastric volvulus who had undergone laparoscopic gastropexy. Thesecondpatientwasan18-months-oldgirlwithfetalalcoholsyndrome, developmental delay and cleft palate who lives in a nursinghome.Sehasbeenreceivingsuboptimalnasogastrictubefeedingduetointermittentnon-biliousvomitingandfailuretothrive. Metabolic and infectious causes were excluded and there was noevidenceofgastro-esophagealrefluxdisease. Thethirdpatientwasa7-year-oldboy,whowasrelativelywellexceptforrecurrentpost-prandialabdominalfullnessandbloating.Therewasnohistoryofacuteabdominalpain.Inbothofthesepatients,bariumupperGIserieswerealsodiagnosticofgastric volvulus. Laparoscopic anterior gastropexy was performed successfully by using two 5 mm trocars. Four to six fixation sutures wereusedfortheseolderchildren.Allpatientsrecoveredwellpost-operativelyandstartedtogainweight,andweresymptom-freeat3years,2years,and7monthsfollow-uprespectively. CONCLUSION: Gastricvolvulus,althoughrareinchildren,shouldbe considered in the differential diagnosis of pediatric patients with ahistoryofvomitingandpost-prandialbloating.BariumupperGIseries are usually diagnostic, even in cases with intermittent volvulus. Laparoscopic anterior gastropexy is simple, safe and effective in both children and neonates.
S053DOES THE USE OF PERI-OPERATIVE ANTIBIOTICS DURING MINIMAL ACCESS GASTROSTOMY INSERTION DECREASE THE INCIDENCE OF WOUND INFECTION?, JuliaRFishmanMD, Ramesh MNatarajaMD,MHaywoodBS,JEkpeBS,GMallonRN,SAClarkeMD,MHHaddadMD,ChelseaandWestminsterHospitalNHSFoundationTrustandImperialCollegeLondonBackground / Purpose: Minimal access gastrostomy formation inchildrenisarelativelycommonprocedure.Woundinfectionremainsasignificantsourceofearlypostoperativemorbidity.Useofantibioticsinpreventionisunclear.Acomparisonofwoundinfectionrates was performed at our centre. Methods: WeperformedaretrospectivecasenotereviewbetweenJanuary2001andAugust2008inclusive.Allpatientswhounderwenta gastrostomy insertion either with laparoscopic or endoscopic techniques(withorwithoutanotherprocedure)wereidentifiedfromtheelectronicpatientrecords&theatrelogbooks.Ethicalapprovalwasobtained.Gender,ageatoperation(months),indicationforprocedureanduseofperioperativeantibioticswerenoted.Primaryoutcomewasearlypost-operativewoundinfectiondefinedasinflammation,pusandapositivewoundculture.Secondaryoutcomemeasuresincludedtimetofullfeeds(days),%weightgainandtechnique. Results:Weidentified89patientswhohadaminimalaccessgastrostomyinsertion(18laparoscopicand71endoscopically).Postoperative infection rate was 13.5% for all gastrostomies. 49 received peri-operativeantibiotics.Patientswhoreceivedantibioticshadaninfection rate of 12.4% compared to 15% in patients who did not receiveantibiotics.Thiswasnotstatisticallysignificant(p=0.76). Conclusion:Peri-operativeantibioticsdonotinfluencetheincidenceof wound infection with minimally invasive gastrostomy placement. Weareinitiatingarandomisedcontrolledtrialtofullyestablishourfindings.
S054LAPAROSCOPY IN THE MANAGEMENT OF ABDOMINAL TRAUMA IN CHILDREN, AhmedRMarwanMD,GeniSmithRN,CarrolMHarmonPhD,KeithEGeorgesonMD,OliverJMuenstererPhD,Children’sHospitalofAlabama,Birmingham,AlabamaBackground: Laparoscopic surgery has been used for both diagnosis and therapy of abdominal trauma in children, however only few small series have been reported. Objective: To systematically analyze our experience concerning indications, procedures, and outcome using laparoscopy in pediatric trauma patients over the last 11 years. Methods:Ourtraumadatabasewassearchedforpatientswhounderwent laparoscopy after being admitted for abdominal trauma. The cases were grouped into diagnostic and therapeutic procedures.Successwasdefinedasattainingthecorrectdiagnosis,or

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 39
2009 Oral Abstractsas the ability to repair the traumatic injury by laparoscopic surgery, respectively.Successratesfordiagnosticandtherapeuticlaparoscopywere calculated. Results: There were 4836 pediatric trauma admissions over a period of 11 years, of which 92 had open or laparoscopic abdominal explorationsforblunt(n=47)andpenetrating(n=35)injuries.Twenty-onediagnosticand5therapeuticlaparoscopicprocedureswereperformed.Overall,19ofthe21diagnosticlaparoscopiesweresuccessful(90.5%),and5ofthe5therapeuticlaparoscopicproceduresweresuccessful(100%).Therewasasignificantdifferencein success rate of diagnostic laparoscopy between acute and delayedcases(p<0.001),aslaparoscopyfailedtoidentifytheinjuryin2patientswithlatepresentation(2and3weeksaftertrauma).Retrospectively, laparotomy was avoided in 13 out of 21 patients (62%)overall,andin10outof10patientswithpenetratingtrauma(100%)(p=0.02). Conclusions: Laparoscopy is useful in the early management of the hemodynamically stable pediatric patient with abdominal trauma. Itislessvaluableincaseswithdelayedpresentation.Mostinjuriesare amenable to laparoscopic repair. Laparoscopy can decrease the need for exploratory laparotomy, especially in patients who sustained penetrating abdominal trauma. Laparoscopy is currently underutilized in the management of pediatric abdominal trauma.
S055LAPAROSCOPIC MANAGEMENT OF THE IMPALPABLE TESTES IN CHILDREN. NEW CLASSIFICATION, LESSONS LEARNED AND RARE ANOMALIES., MOHAMEDEHASSANBA,ARMUSTAFAWIBA,ALWASLHOSPITAL,Dubai,UAEIntroduction:Cryptorchidismisthemostcommongenitourinaryanomalyinmalechildren.About20%ofcryptorchidtesticlesare impalpable. Laparoscopy has become one of the important diagnostic modalities for management of impalpable testes. The aim of present study is highlighting the lessons and rare anomalies encountered during the management of impalpable testes in children over a period of 10 years in a single pediatric surgery centre and to establish a new classification that better describe the anomalies. Patients and methods: Aretrospectivereviewof93laparoscopicexplorations for nonpalpable testes between 1998 and 2008 wasconducted.Demographicdata,intraoperativefindingsandmanagement, associated anomalies and postoperative follow up was collectedandanalyzed.Anewlaparoscopicclassificationisdescribed. Results:agerangewas7months-8years.20bilateralversus73 unilateral impalpable testes were operated. 4 groups were establishedwithsubgroupsineachgroup.Group1(vanishingsyndrome)30cases;Group2(peepingtestes)18cases,Group3 (Intraabdominaltestes)37casesandgroup4(disordersofsexdevelopment)8cases.Associatedanomaliesincluded4casesofDownsyndrome,7casesneurologicalimpairment,3renalanomalies,3 cardiac anomalies and 1 case of eye anomalies. Follow up range was3-6years. Conclusion: Anewlaparoscopicclassificationisdescribedthatbetter describe the anomalies and help planning the treatment of impalpabletestes.ImpalpabletesteswithDownsyndromesometimesassociatedwithbizarreanatomy.Parentsshouldbewellexplainedallthe possible findings especially in bilateral cases.
S056LAPAROSCOPIC CONTRALATERAL GROIN EXPLORATION: IS IT COST EFFECTIVE?, StevenLLeeMD,RomanMSydorakMD,TalarTejirianMD,StanleyTLauMD,KaiserPermanente,LosAngelesMedicalCenterPurpose: Transinguinal laparoscopy offers a safe and effective method for evaluating the contralateral groin during unilateral inguinalherniarepair(UIHR).Thepurposeofthisstudyistodetermine whether laparoscopic contralateral groin exploration (LCGE)iscosteffective. Methods: AretrospectivereviewofallchildrenwhounderwentUIHRandLCGEfrom2006-07byasinglesurgeonwasperformed.CostanalysiscomparingthetimetoperformtheLCGEandtimetorepairthecontralateralpatentprocessusvaginalis(CPPV)tothecostsaved by preventing future operation for a contralateral inguinal hernia repair was calculated based on Medicare reimbursement. Results: 81patientsunderwentUIHRwithplannedLCGE.78(96.3%)hadsuccessfulLCGE.8patients(10.3%)hadaCPPVandunderwentcontralateralopenrepair.Costanalysisshownbelow. CostforLCGE: TimeforUIHR+LCGE(n=78):37minutes
TimeforUIHRalone(n=105):31minutes TimeforLCGE:6minutes CostforLCGE($20/min):$120 TotalcostforLCGE(78x$120):$9360 TimetorepairCPPV:11minutes CosttorepairCPPV($20/min):$220 SurgeonfeetorepairCPPV:$245 TotalcosttorepairCPPV(8x$465):$3720 TOTAL($9360+$3720):$13080 CostforreturntriptoORforherniarepair: Hospital/ORreimbursement:$1954 Surgeonfee:$491 Anesthesiafee:$220 TOTAL8x($1954+$491+$220):$20440 Conclusion: Lapraocsopic contralateral groin exploration at the time of unilateral inguinal hernia repair is cost effective.
S057LAPAROSCOPIC PYELOPLASTY FOR REPAIR OF URETEROPELVIC JUNCTION OBSTRUCTION IN CHILDREN, ManuelLopezMD, FrançoisMichelMD,EmmanuelleGuyeMD,FrançoisVarletPhD,DepartmentofPediatricSurgery,UniversityHospitalofSaintEtienne-FrancePURPOSE: To report our initial experience with laparoscopic pyeloplasty(LP)inchildrenwithpelvi-uretericjunction(PUJ)obstruction, to describe the evolution and to evaluate the results for theses patients. MATERIALS AND METHODS: BetweenMay2005andSeptember2008, we retrospectively reviewed the records of 30 consecutive infantsandchildrenwithunilateralPUJobstruction,whounderwentLP.Thepatientwasplacedina¾lateralpositionwiththreeports.ThePUJwasresectedandtheanastomosismadeusingabsorbablesutures.AJJstentwasinsertedbylaparoscopyinamajorityofpatients.Follow-upincludedclinicalandultrasoundassessment,andisotope renography at 6 months. RESULTS: LPwasfeasiblein28of30patients(93%).Theprocedurecould not be completed by laparoscopy in two patients, the main reasonbeingdifficultyincompletingtheanastomosis.Stentinsertionwassuccessfulin27casesofthem.Anaberrantcrossingvesselwasfound in four patients. For two of them we held up the aberrant crossingvesselandPUJbytwotothreenot-absorbablesutureswithout tension without the needed pyeloplasty. For the others two casesweperformedaLPenabledureterictransposition. There were 3 postoperative complications; pyelonephritis in two patientsandonepatientrequiredoperativeinterventionforPUJleakage,andunderwentnephrostomywithafurtheruneventfulcourse. The mean operative time was 130 minutes (range 70 to 270 min),inthelastthirteencasesafterweusethestaysuturesthemeanoperative time was reduce about 90 min, without convertions. The averagehospitalstaywas4days(1-8)days. Meanfollow-upwas18months(range6to40months).Atotalof28patientsthatunderwentUPJwereasymptomaticafterremovalofthedoubleJJstent,showingreductionofthedegreeofhydronephrosisinallpatients,andhadalsoimprovedPUJdrainageon isotope renography or sonography. CONCLUSIONS:LPiseffectiveandsafeinchildrenwithminimalmorbidityandgivesexcellentshort-termresults.Thefeasibilityisalsoexcellentinpatientsyoungerthan1year.Thetrans-abdominalapproach revealed good exposition without a disadvantage for the patient.
S058SURGICAL MANAGEMENT OF OVARIAN DISEASE IN INFANTS, CHILDREN AND ADOLESCENTS: A 15-YEAR REVIEW, BrettMichelottiBS,IndranilSauMD,SoniaPerez-Bertolez,TimothyDKane,Children’sHospitalofPittsburghofUPMC,Pittsburgh,Pennsylvania,USABackground:Wereviewedourexperiencewiththemanagementof ovarian disease in children to evaluate the surgical indications, results, and outcomes for pediatric age groups. Methods: ThisIRB-approved(#7060026)retrospectivereviewincluded all patients who underwent surgical management of ovariandiseasefromJanuary1,1992-July10,2007.Patientswithectopicpregnancy,orknownpelvicinflammatorydiseasewereexcluded.Demographics,clinicalsignsandsymptoms,diagnosis,surgicaloutcomeswereobtained.Statisticalanalysisincludedcomparisonofmeans,pairedt-test,chi-squaredtest,andmultivariateanalysis where indicated. Results: There were a total of 221 patients with a mean age of 12.8

40 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Oral Abstractsyears(range3weeks-20years).Therewere211(95.5%)benigndiagnosesand10(4.5%)malignant.Therewere156simpleorhemorrhagiccysts(70.5%),and46matureteratomas(20.8%).Threemorbidities(1.3%)wereassociatedwithsurgeryandnomortalities.OperativeoutcomesforbenigndiseasewerecomparedbetweenMISand open cases over the entire time period as well as within three consecutive5-yeartimeintervals. TimePeriodTotalCases#BloodLoss(cc)LOS(days)OperativeTime(min) MISvOpen 1992-2007148v73*10.4v71.4*1.9v4.5*84v127* 1992-199615v36*21.0v81.4*2.1v5.1*103.5v123.2 1997–200145v16*10.0v52.5*1.9v4.1*100.7v147.6* 2002-200781v16*9.5v81.3*1.8v4.0*73.1v123.1* *P<0.05consideredsignificant-#for12cases,intervaltimeofsurgery could not be determined Conclusions: There was a notable a shift toward the management ofbenignovariandiseaseviaminimallyinvasivesurgery(MIS)overthecourseofthreedifferent5-yearintervals.Thisapproachwasassociated with shorter hospital stay, less operative blood loss, and shorteroperativetimeswhencomparedtoanopenapproach.Whenindicated, laparoscopic surgery should be performed for presumed benign ovarian disease in children.
S059THE ROLE OF GASLESS LAPAROSCOPY IN NEWBORNS WITH NECROTIZING ENTEROCOLITIS: PRELIMINARY EXPERIENCE, GiovannaRiccipetitoniMD, ClaudioVellaMD,EnricaCaponcelliMD,ErnestoLevaMD,MassimoGarriboliMD,DepartmentofPediatricSurgery–Children’sHospital–V.Buzzi–Milan–(Italy)INTRODUCTION Alimitednumberofnewbornsaffectedbynecrotizingenterocolitis(NEC)andprogressiveclinicaldeteriorationmay have not specific surgical indications. Laparoscopy can give useful informations on intestinal viability avoiding unnecessary laparotomy or deciding for an early surgical operation.Wereportourpreliminaryexperiencein4casestreatedduring the last year. MATERIAL AND METHODS The study includes 4 newborns, 3 males and 1 female with abdominal distension and clinical sepsis not responding to aggressive medical treatment; none had radiological evidence of perforation. The gestational age ranged from 28 to34weeks,weightfrom990grto1550gr;themedianageatlaparoscopywas13days(range7–20days). AgaslesslaparoscopywithgentleliftupoftheabdominalwallwascarriedoutintheIntensiveCareUnit,usinga3mmumbilicaltelescope. RESULTS Arightcolonperforationwasdetectedin3cases,localizedleft colon pneumatosis in 1 case. Inthelastpatientweinsertedadrainunderlaparoscopicdirectvision, the remaining 3 cases underwent to laparotomy. Two cases with colonic perforation were treated performing resection and primaryanastomosis,onecasehadadivertingstoma.Allthenewborns well tolerated the procedure and they were discharged preserving a normal intestinal function. CONCLUSIONDiagnosticlaparoscopyisasafeandusefulprocedureinthemanagementofcriticalNECcaseswithouttypicalradiologicalfindings. Itgivesgoodinformationforacorrecttimingoflaparotomyavoiding unnecessary surgical procedures.
S060NEW TRENDS IN REDUCTION OF INTUSSUSCEPTION IN CHILDREN : A MINIMAL INVASIVE VISION, HSteyaertPhD,JLauronMD,JSVallaPhD,LenvalFoundationforChildrenBackground: The use of barium or air enema affords both confirmationandcompletereductionofintussusception(ISS)inaround80%ofthepatients.Incaseoffailurealaparotomyismostlyconductedonanemergencybasis.Inordertoassessthefeasabilityand the potential advantages of a laparoscopic approach in case of surgery authors conducted a prospective survey of all patients seen forISSattheLenvalInstitutionduringaheightyearperiod. Material and Methods:AllchildrenmanagedatourinstitutionforISSbetween06/06/2000and06/06/2008wereintroducedinasurveyconcentratingonanamnesis(durationofsymptoms),radiologicalreduction(numberofattempts)andoperativeresults.Incaseofoperation all children were first approached by laparoscopy. Results: duringthatperiod241patientswereincluded;197(82%)wereradiologicallyreduced.7(16%)oftheoperatedpatientswere reduced just at laparoscopic examination (after induction of
generalanesthesia).5patients(11%)neededaconversionforseveralreasons:doubtaboutperfectreduction(1),tripleISSnotseenduringthefirstlaparoscopy(1),technicalproblem(1),bowelnecrosis(2). Discussion: managementofISSisevolving.Successrateofradiological treatment may be increased with the help of anesthesiological sedation and level of X rays decreased by the use ofanultrasoundcontrolduringairreduction.SurgicalmanagementisalsoevolvingincountrieswereISSiswellknownbypaediatriciansan seen quite soon. Laparocopy has to become the second level treatment:becauseseveralcasesarejustreducedduringinductionofanesthesia;becausethe“pushing”methodisnotmoreadogmalookingtotheresultsoflaparoscopicreductionandbecauseof, even in case of complicated cases, laparoscopy may solve the problem or decrease the length of the incision. Conclusion: authors propose a new algorythm for the management ofISSthathastobeadaptedtolocalconditionsandrecommandstrongly a laparoscopic approach in case of operation.
S061COMPUTER-AIDED WORKFLOW COMPARISON OF LAPAROSCOPIC VERSUS ROBOT-ASSISTED NISSEN FUNDOPLICATION IN INFANT PIGS, AlexandraKraussMS, Thomas NeumuthPhD,RobinWachowiakMD,BerndDonaubauerMD,WernerKorbPhD,OliverBurgertPhD,OliverJMuenstererPhD,UniversityofLeipzig,PediatricSurgery,InnovationCenterComputerAssistedSurgery,AnesthesiaandIntensiveCareMedicine,Leipzig,Germany;PediatricSurgery,Children’sHospitalofAlabama,Birmingham,AlabamaBackground: Adecadeago,theDaVincirobotwasintroducedasatoolthatfacilitatesdissectionandknot-tyingduetoits3-dimensionalendoscopicvisionandadditionaldegreesoffreedomwhen moving the instruments. To date, however, no objective data exists on whether robotic surgery is indeed superior to conventional laparoscopy. Objective: This study compares conventional laparoscopic Nissen fundoplication(CLNF)versusrobot-assistedNissenfundoplication(RANF)intermsofspeed,safety,accuracyandefficiencyusingcomputer-basedworkflowanalysisinaninfantpigmodel. Methods:CLNFwasperformedin12,RANFin13pigs(weight7-10,8kg).Basedonsynchronizedintraoperativemovierecordings,thesurgicalworkflowwassegmentedintotemporalphases(preparation,dissection,reconstruction,conclusion).Allactionswererecordedina virtual timeline and the time necessary to perform these actions wascomparedbyt-test.Qualityofknot-tyingwasevaluatedbyanobjectiveskillscoringsystem(compositeindex,Changetal.2003).TotesttheefficacyofCLNFandRANF,CardiayieldPressures(CyP)were determined pre and post fundoplication. The incidence of complications was compared using the fisher exact test. Results: No difference in the average time required to complete the preparation, dissection, and conclusion phases of the operation was found.ThereconstructionphasetooklongerinRANFcomparedtoCLNF(2836+/-642vs.2005+/-608seconds,respectively,p=0.004).The composite index as a measure of suturing quality was more favorableforCLNFcomparedtoRANF(117+/-13.4vs.109+/-23,respectively,p=0.02).TheaveragepostoperativeriseinCyPwassimilarinbothgroups.Theincidenceofworkflow-interruptinghemorrhage was comparable, but pneumothorax occurred more frequentlyduringCLNFcomparedtoRANF(p=0.04).Moresuturebrokeduringrobot-assistedoperations(p=0.002). Conclusions: The robot provides no clear advantage in operating speed compared to conventional laparoscopy for Nissen fundoplicationinthismodel.Infact,thereconstructionphasetooklongerintherobot-assistedcomparedtothelaparoscopicoperations.Conversly,lesspneumothoracesoccurredduringRANF,possiblyduetotheimproved,3-dimensionalvisualizationofthehiatusduringdissection.RANFandCLNFwereequallyefficient.For robotic surgery to manifest its full potential, more complex operations may have to be evaluated.
S062LAPAROSCOPIC MANAGEMENT OF INTUSSUSCEPTION IN PEDIATRIC PATIENTS, JasonDFraserMD,PabloAguayoMD,SusanWSharpPhD,DanielJOstlieMD,GeorgeWHolcombMD,ShawnDSt.PeterMD,TheChildren’sMercyHospitalIntroduction:Minimallyinvasiveapproachesarebeginningto be employed in the management of pediatric patients with intussusceptionwhofailradiographicreduction.Successfullaparoscopic reduction has been documented, but the utility of laparoscopy for more complex cases is less well documented.

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 41
2009 Oral AbstractsTherefore, we reviewed our experience with laparoscopy in patients with radiographically irreducible intussusception to document the safety and effectiveness of this approach. Methods:Weconductedaretrospectivereviewofallofthepatientswho had a radiographically irreducible intussusception treated via thelaparoscopicapproachatasingleinstitutionfrom1998-2008. Results:Atotalof22patientswereidentifiedwithanaverageagewas2.8years.Averagelengthofstaywas2.67dayswithamedianof2days.Meanfollow-upwas80days.Twentyofthesewereableto be managed entirely laparoscopically or via extension of the umbilical incision, while two necessitated conversion using a right lowerquadrantincision.Tenpatients(46%)hadabowelresectionofwhich 5 were an ileocecectomy and 5 were segmental small bowel resection.TherewerefourMeckel’sdiverticularesected.Onepatientreturned with obstructive symptoms and underwent an adhesiolysis forpost-operativesmallbowelobstruction.Therewerenoothercomplications noted. Conclusions: Ourdatasuggestthatlaparoscopyisasafeandeffective means to manage pediatric intussusception, even in the event when bowel resection is necessary.
S063SHORT TERM NATURAL HISTORY OF THE STANDARD APPROACHES FOR GASTROSTOMY TUBE PLACEMENT IN THE PEDIATRIC PATIENT, JasonDFraserMD,ToddAPonskyMD,PabloAguayoMD,ScottBoulangerMD,RobertParryMD,NeilNixdorfMD,JenniferDiLucianoRN,PattiSmithRN,SusanWSharpPhD,GeorgeWHolcombMD,DanielJOstlieMD,ShawnDSt.PeterMD,TheChildren’sMercyHospitalandRainbowBabiesandChildren’sHospitalIntroduction: Gastrostomyplacementisacommonprocedureinthepediatricpopulation.Standardapproachesoftubeplacementinclude open, laparoscopic and percutaneous endoscopic methods. Placementofthegastrostomyinrelationtothefundusandtheanterior abdominal wall is crucial to ensure adequate comfort and functionality. Misplacement may require repositioning of the gastrostomy,therateofwhichhasnotbeenwelldocumented.Wetherefore have reviewed our experience with gastrostomy tube placementtodeterminetheshort-termnaturalhistoryofplacementbasedonapproachandtoestablishacohorttodeterminethelong-term natural history. Methods: Weconductedaretrospectivereviewofallpediatricpatients who underwent percutaneous endoscopic, laparoscopic, or opengastrostomyplacementattwoinstitutionsfrom2000-2008. Results:Therewereatotalof1544patientswhounderwentgastrostomy tube placement during this time period. The distribution ofproceduresperformedislistedinTable1.Therewere3(0.2%)gastrostomy tubes that required repositioning to a new site due to encroachmentupontheribmargin.TwowereopenandonewasPEG(p=0.55).Eighteenof35patientswhohadanopenfundoplicationfollowinggastrostomy(10openand8PEGs)hadthegastrostomytakendownduringtheoperationcomparedto4of24patients(P=0.01)whounderwentlaparoscopicfundoplicationfollowinggastrostomy(3lapand1PEG). Table1.Distributionofproceduresperformed.
Conclusions: This data demonstrates that the need for gastrostomy tube repositioning is rare in the short term regardless of approach, althoughatakedownofthegastrostomyismorelikelywhenanopen fundoplication is performed placement.
S064LAPAROSCOPIC TOTAL COLECTOMIES IN CHILDREN, Michel FRANCOISMD,ManuelLOPEZMD,EmmanuelleGuyeMD,S.IrtanMD,ABonnardMD,PDeLagausiePhD,HStaeyertMD,J-SVallaPhD,MDemarcheMD,PErpicumMD,HLardyPhD,MRobertPhD,GpodevinPhD,yHélouryPhD,OReingbergPhD,PMontupetMD,HMartelliPhD,J-FColombaniMD,DWeilMD,CPiolatPhD,FVarletPhD,UniversityhospitalofSaintEtienneandGECI.FrancePurpose: To report our experience with laparoscopic total colectomie(LTC)inchildren,todescribetheevolutionandtoevaluate the results for theses patients.
Material and methods: Between1995and2008,11centersofpaediatric surgery in French languages countries retrospectively reviewedtherecordsof44casesofLTCandweredividedintwogroups.GroupA:10caseswithtotalcolonichirschsprungdisease,themeanagewas13monthsold,andgroupB:34caseswithinflammatorycolitis(IC)andfamilyadenomatouspolyposis(FAP),themean age was 13 years old. Results:InthegroupA:LTCwasfeasiblein10/10cases.ThetechniqueusedinallcaseswasDuhamel’sprocedures,withoutprotectiveileostomy,exceptonewhohadananastomoticleakageduringtheperitoneallavage.Inthisgroupthemeanoperativetimewas 3.8hs. There were 6 postoperative complication; 1 functional bowel obstruction in immediate postoperative period, 1 small bowel obstruction, 3 partial obstructions, and 1 persistent diarrhea. The averagehospitalstaywas12days.Meanfollow-upwas3.8years,5 children had 2 or 3 stools by day, 1 had 4, 1 between 6 to 8 and 1 between 8 and 10 by day, with soiling for the 2 last cases. InthegroupB:LTCwasfeasiblein33/34.In22casesasmalllaparotomywasassociated.Anileorectalanastomosiswasperformedin16patientsandanileoanalanastomosisin18patients,withaJpouchin12andaprotectiveileostomyin5.Inthisgroupthemeanoperative time was 7 hours. 5per-operativecomplicationsoccurred(15%):1anastomotictwist necessitating an immediate redo, 1 impossible pull through (ileostomy),1ureteralperforationwithEndoGIA*,1duodenalperforation and 1 colonic perforation. Therewere11immediatepostoperativecomplications(32%):anastomoticleakages(2),smallbowelobstructions(3);functionalobstruction(1),anastomotictwist(1),1urinoma(1),anastomoticstenosis(AS)(2)andparietalinfection(1). Twelvepatients(37.5%)haddelayedcomplications:AS(4),smallbowelobstruction(1),pouchitis(2)andpersistentrectalinflammatorydiseases(5).Theaveragehospitalstaywas14days.Meanfollow-upwasinthisgroupwas4.3years:13patientswhohad5stoolsormoreby day and soiling in 4. Conclusion:LTCisfeasibleinchildren;themorbidityisfrequentespeciallyincasesofICandFAP.
S065ROBOTIC THYMECTOMY IN CHILDREN, FranklinCMargaronMD, ClaudioOiticicaMD,DavidLanningMD,VirginiaCommonwealthUniversityMinimally invasive techniques for thymectomy in children with juvenile myasthenia gravis are desired due to the morbidity associatedwithmediansternotomy.Acervicalopenapproach,aleftthorascopicapproach,andothershavebeenadvocated.Completeradical thymectomy is required to achieve maximal improvement. Anatomically,thethymusisrelativelylargeinthesmallmediastinalspace in children and the improved maneuverability of the robotic technique presents definite advantage over standard thorascoscopy. Robotic extended thymectomy has been shown to be feasible and safeinadults,withgoodoutcomes.Wepresentfourchildrenwhounderwent 3 port robotic thymectomy from the left chest using thedaVincisurgicalrobot.Agesofthechildrenwere2,3,6,and14years.Onlyonepatienthadplacementofanintervalchesttubewhich was removed without complication on post operative day one. Allfourchildrenwereabletobedischargedhomeonpostoperativedayone.Operativetimesrangedfrom2hours46minutesto3hours10minutes(avg2h59minutes).Therewerenointraoperativeorpostoperative complications and all had improvements in their symptomsatlastfollowup.ThedaVinciroboticsurgicalsystemwithits3Dimagingandarticulatinginstrumentscanbeusedtosafelyperform a complete thymectomy in children with minimal morbidity.
S066ROBOTIC SURGERY FACILITATES LEARNING CURVE IN MIS, JuanCampsMD,TreyBradleyMD,PalmettoHealthChildren’sHospitalBackground: Minimal invasive surgery has become a routine and accepted tool to perform surgery in pediatric patients. The use of robotics in pediatric surgery has been recently added to the surgical armamentarium. The aim of the study is to show the learning curve of using robotics compared to laparoscopic technique in a common pediatric surgical procedure. Methods:Allsurgicalcaseshavebeenperformedbythesamepediatricsurgeon.SinceNissenfundoplicationandgastrictubeplacement are very common surgical procedures in pediatrics, both procedures are compared in a chronological consecutive manner toevaluatethelearningcurveintheRoboticsurgicalgroup.Inthe

42 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Oral AbstractsNissenFundoplicationgroup,laparoscopic(A)=8casesandRobotic(B)=8cases.IntheNissenFundoplicationwithaGastrictubeplacementgroup,Laparoscopic(C)=7casesandRobotic(D)=7. Agerangeinyearsissimilarinthegroups,laparoscopicGroupA=3.38andGroupB=4.75,RoboticGroupC=0.86andGroupD=0.71.Tominimizethelaparoscopiclearningcurve,GroupsAandCarechosenafter 100 consecutives cases in laparoscopic Nissen Fundoplication have been performed. Results: Allcaseswereperformedandcompletedwithoutanyimmediateorlatesurgicalcomplications.Despiteofdiversecomplexity of the laparoscopic group, there is no significant statistical variation in surgical average time of cases performed with laparoscope.GroupA=1.37hrsorR2=0.029,GroupC=2.18hrsorR2=0.187.IntheRoboticcases,thereisasignificantstatisticalimprovement in the learning curve decreasing the surgical time just afterafewcasesaredone.GroupB=2.22hrsorR2=0.502,GroupD=3.06hrsorR2=0.724. Conclusion: The use of Robotic in pediatric patients facilitates the learning curve even after only few robotic surgical cases have been performed. Robotic equipment provides better space perception andopticswithahighdefinition3Dvision.Intuitiveandincreasedmaneuverability of instruments is another important factor to improve the learning curve.
S067A NEW PLATFORM FOR BASIC AND AVANCED ENDOSCOPIC SKILLS TRAINING, MLimaMD,CMelchiorri,GRuggeriMD,GDeNovi,TGarganoMD,PediatricSurgery–UniversityofBologna,ItalyFacultyofEngineering–UniversityofBologna,ItalyIntroduction.TheapplicationsofMinimallyInvasiveSurgery(MIS)arerapidlyexpanding.Surgicaleducationisquicklychanging,severalfactorsincludingbudgetconstraintsandmedico-legalconcernslimitopportunitiesforpediatrictrainees.Newmethodsofskillstrainingsuch as low fidelity bench trainers and virtual reality simulators offernewavenuesforsurgicaleducation.Whilemanysurgeonsfeel that the use of minimally invasive techniques eliminates force feedbackandtactilesensation,theimportanceofhapticsinMIShasnot been fully evaluated. Moreover, there is considerable interest inthedevelopmentofhapticsimulatorsforMISeventhoughtheimportanceofforcefeedbackremainspoorlyunderstood. Methods.Wepresentanewinnovativelaparoscopictrainingsolution.TheLaplabisanhapticsimulatorsforMISdesignedtoexerciseandtesttheskillsofsurgeons.ItallowstotestnewinstrumentsandusemodernGraphicProcessingUnitandthehapticdeviceslowcost(SensiblePhantom).Moreoverthissoftwareisusablebymid-lowcostpersonalcomputer. ThroughtheuseofforcefeedbackimpulsedevicesinVRsimulators,one should be able to create a more realistic theatre in which the novicesurgeoncanlearnoperativeskills. Conclusion.Surgicalsimulationisanexcitingareaofsurgicaleducation. The future is bright as advancements in computing and graphical capabilities offer new innovations in simulator technology. Simulatorsmustcontinuetoundergorigorousvalidationstudiestoensure that time spent by trainees on virtual reality simulators will translateintoimprovedsurgicalskillsintheoperatingroom.
S068DEVELOPMENT OF A NEW 2.4 MM LAPAROSCOPE FOR MICROLAPAROSCOPY IN CHILDREN., SalmaiTurialMD, Miriam LuiseKnab,VeronikaEngelMD,FelixSchierMD,UniversityMedicalCentre,DepartmentofPediatricSurgery,MainzPurposes: Recently, a prototype laproscope of 2.4 mm in diameter wasdevelopedincooperationwithKarlStorzTuttlingen,Germany.Ourexperienceswiththisnewprototypescopearereportedandthepreliminary results of prospectively collected data are presented. Description: BetweenNovember2007andMarch2008anewprototypescope0°,2.4mmindiameterand18cmoflengthwasdevelopedincooperationwithKarlStorzTuttlingen,Germanyspecifically for this microlaparoscopy study group at our department. Alldataconcerningtheintraabdominalillumination,depthperception,parallaxes,shadowingandlightreflexesontissue,aswelltheinfluenceofdifferentlightcableswerecollectedperioperatively in the theater. Results: The prototype scope was used since March 2008 in a variety ofmicrolaparoscopicapproachesin113children(agedfrom3weeksto17years,Median:2.8years,andinone31-year-oldwoman).Amongtheproceduresperformedwere76(67%)inguinalherniarepairs,12(10%)diagnosticmicrolaparoscopiesforacuteorchronicabdominalpain,5(4%)ovariancysteunroofingsordetorsions
ofovaries,threecaseseachofmicrolaparoscopically-assistedpull-throughsforHirschsprung’sdisease,microlaparoscopically-assistedgastrostomiesandVP-shuntdisfunctions,twocaseseachofpyloromyotomies, varicocele ligations, intussusceptions, treatments of urachal remnant, Nissen fundoplication and a transperitoneal pyeloplasty.Allprocedureswerecompletedsuccessfully.Therewas no need to exchange the 2.4 mm scope for a 5 mm scope. No complications occurred due to the use of 2.4 mm scope. The new 2.4 mm scope provides very good results in all technical parameters, and theimagequalityisclosetothe5mmscopes.Although,thisscopepassesthroughtheminiports,however,insufflationcannolongerbeprovided though the same trocar due to the tight fit of the scope in the miniport trocar. Conclusion: Basedonourpreliminaryresults,itseemsthattheuseof the 2.4 mm prototype scope is safe and feasible. Technologically, it provides nearly identical qualities to the 5 mm scopes, and it still fits through the miniports. Intheverynearfuture,thisnew2.4mmscopewillbeseries-produced and be available beginning from Febuary 2009 commercially.
S069THE “ENDO-PAED-TRAINER”: WHY A LAPAROSCOPIC TRAINING DEVICE IS INDISPENSABLE IN PEDIATRIC SURGERY, MarkusDuerschMD,BertramReingruberMD,Departmentofpediatricsurgery-RegensburgOff-patientlaparoscopictrainingforoperatorsatalllevelsofexperiencehasbecomewellestablishedtoenhanceskillsandtestnewtechniquesandinstruments.Whatweespeciallyneedinpediatricsurgeryistopreparefortheindividualcase.Variationsindisease,thepatient’sage,sizeandcomorbiditymaketherequirementsdifferentthanforadultlaparoscopictraining.Theskillsto be taught are of a more general nature and emphasis needs to be placedonworkingwithamultidisciplinarysurgicalteamratherthanonlearningskillsspecifictoaparticularorgan. OurEndo-Paed-Trainerconsistsofahumantorsothesizeofa4-year-oldchild.Thereareflexiblelidscoveringtheabdominalandthoraciccavities which maintain tension in convexity and can be perforated bytrocars.Porcineorgansaremountedinside.Specialfeaturesinclude the possibility of intubation and ventilation of an airtight trachea-lungspecimen,anabdominalspecimenincludingesophagus,stomach, small and large intestines as well as liver, pancreas and its excretory ducts with the possibility of attaching a blood circulation. Ascorecardsystemhasbeendevelopedandvalidatedforvariousskillsandlevelsofexperiencetoassesstheaptitudeoftheindividualcandidate and monitor progress. Regularperiodicstandardizedin-housetrainingroundshavebeenestablishedatthreelevelsofskillsandexperience(inlinewiththeproposedqualityassurancecertificateoftheGermanSocietyofPediatricSurgery).Specialsituationsarerehearsedaswell.Theseinclude: -thespecialcase,preoperativeon-sitebriefingoftheteam:surgeon,assistant,scrubnurse,anesthetist,anestheticnurse.Issuestobediscussed include placement of the patient, placement of trocars and positioning of surgeon, assistant, scrub nurse. -interdisciplinaryworkingwithpediatricgastroenterologists -newinstruments Examplesofscorecardsforindividualsandgroupsarepresented. Thelaparoscopictrainingdeviceoffersfarmorethanjustorgan-specifictrainingasisusuallydoneinworkshops.Preparationfortheindividual case is good for the patient and saves time; the scorecard is a strong motivator of young surgeons and is a source of additional experience for advanced operators. Inourdepartmentofpediatricsurgery,theEndo-Paed-Trainerhasbecome an essential device not only for laparoscopic surgery but for the whole range of endoscopic and minimally invasive procedures in children of all ages.
S070A NOVEL TRANSORAL ESOPHAGEAL ANASTOMOSIS DEVICE (EAD): TOWARD A NOTES APPROACH TO ESOPHAGEAL ATRESIA REPAIR, ZacharyJKastenbergBS,PabloGarciaMS,SanjeevDuttaMD,MultidisciplinaryInitiativeforSurgicalTechnologyResearch–StanfordUniversity/SRIInternational,PaloAlto,CA,USABACKGROUND: Amajortechnicalimpedimenttominimalaccessrepairofesophagealatresia(EA)iscreationoftheanastomosis,whichpreventsmanysurgeonsfromutilizingthisapproach.Wearedeveloping a device that greatly facilitates thoracoscopic esophageal anastomosis, and in the future may comprise one component of a

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 43
2009 Oral Abstractsnaturalorificetransluminalendoscopicsurgery(NOTES)approachtoEA. METHODS:TheEADisacomprehensivecatheter-within-a-catheterinstrument that is distally equipped with a novel mechanism for achievingend-to-endanastomosis.Afterthesurgeonfreestheesophageal segments from their plural encasement using traditional thoracoscopicinstruments,theEADispositionedtransorallyacrossthe proximal esophageal pouch into the distal esophageal segment under thoracoscopic guidance. The surgeon then manipulates the EADusingcontrolsatthepatient’smouthtoapproximatetheesophageal segments prior to actuating the anastomotic mechanism. This presentation will describe the device and demonstrate its function in a tissue model. FUTURE DIRECTIONS: TheEADisundergoingfeasibilitytestinginapigletmodel.Outcomemeasuresinclude:(1)anastomoticburststrengthand(2)anastomoticleakratesinnecroscopyandsurvivalprotocols.Toachievethelong-termgoalofdevelopingacompletelytransoralrepairofEAwithtracheoesophagealfistula(TEF),additionalproceduralstepswillneedtobeaddressedincluding:(1)accessingthethoraciccavitytransorally,(2)dividingtheTEF,and(3)exposing the esophageal limbs from their pleural encasings.
S071COMPARATIVE PERFORMANCE EVALUATION OF FORCE TRIVERSE– MODE VS. STANDARD ELECTROSURGICAL MODES, HannahKSwayzeMD,ArlenKWard,MyronSt.LouisMD,DavidTashjianMD,KevinPMoriartyMD,DepartmentofSurgery,BaystateChildren’sHospital,PioneerValleyLifeSciencesInstitute,Springfield,MassachusettsPurpose: Standardelectrosurgicaldevisesofferthreeoptionsforsurgicaldivisionoftissue;1)cut,2)fulgurate,3)blend.Thefullcut mode utilizes a continuous duty cycle that offers swift tissue division with little or no hemostasis. The fulgurate mode utilizes an intermittent duty cycle providing higher levels of hemostasis with resultant increased levels of thermal spread and reduced cutting speed.AnewelectrosurgicaldeviceForceTriVerse–(Valleylab/Covidien,Boulder,CO)utilizesaclosedloopcontrolsystemwithaRFoutput that is continuously monitored and adjusted due to changing tissue impedance. The objective of this study was to evaluate the performanceoftheForceTriVerse–modecomparedtothestandardcut and fulgurate modes. Methods: AfterobtainingIACUCapproval11(30–60kilograms)femaleporcinewereanesthetized.Atotalof174sequential,15cmincisionswereperformedwithanEDGEcoated,spatulatippedelectrosurgicalblade(Valleylab/Covidien,Boulder,CO).Aroboticdevisewasemployedtoprovideaconstantforce(0.12lbs)andaconstanttissuedepthadvancement(3/16inch)foreachincision.AForceTriadGenerator(Covidien/Valleylab,Boulder,CO)wasusedforthecut,fulgurateandTriVerse–modes.Allthreemodesweretestedat30,45and60Watts.Dragontheelectrosurgicalbladewasmeasuredwhilemaintainingaconstantvelocityof10m/sec.Instantaneousvelocitymeasurementsweretakenevery0.01seconds.Statisticalanalysiswasperformedusingthestudent’st-test. Results: TheTriVerseTMmodedoesnotdemonstrateastatisticallydifference in drag when compared to cut or fulgurate modes at 30, 45or60Watts.Thecutmodedemonstratedastatisticallysignificantdifferenceindragcomparedtofulgurateat30watts.(p=0.039). Conclusions:TheTriVerseTMmodedidnotofferadecreaseindragwhen incising skinversusfulguration.Standardcutmodehadstatisticallysignificantly less drag than the fulgurate mode at 30 watts.
S072SERIAL INTESTINAL LENGTHENING USING A RE-DEPLOYABLE INTRALUMINAL SPRING DEVICE, ShantShekherdimianMD, MohanchandraPandurangaPhD,GregoryCarmanPhD,JamesDunnMD,UniversityofCalifornia,LosAngelesBackground: Shortbowelsyndromeresultsininadequatenutritionandhydration.Currenttreatmentsarefraughtwithsignificantmorbidity and mortality, while experimental techniques are limited bytheirrelianceonextra-abdominaldevices,spaceconstraintswithinthe abdominal cavity, and the need to isolate segments of bowel. Description: Acompressedspringmadefrombiocompatiblematerialandcapableofbeingre-compressedendoluminallyisimplantedintoade-functionalized(butnotisolated)segmentofsmallintestineandthebowelisallowedtolengthen.Subsequently,the spring is serially recompressed and deployed, lengthening adjacentintestinalsegments.Onceadequatelengthhasbeenachieved,thespringisremovedandde-functionalizedintestinal
segmentreattachedtothein-continuitybowel. Preliminary Results: Usingtheproposedspringdevice,wehavesuccessfullybeenabletolengthenintestinalsegments4-fold.Furthermore, we have demonstrated increased intestinal enzymatic activity in lengthened segments. Conclusion: Thefeasibilityofserialre-deploymentsandre-implantationoflengthenedintestineremaintobedetermined.Ifsuccessful, the proposed device will have the capability to lengthen intestinal segments without the need to isolate them and without any exterior components. Furthermore, serial lengthenings may be performed eliminating limitations due to the unidirectional lengthening capability of prior devices. Finally, it may be possible to implant,re-deployandultimatelyremovethisdeviceendoscopically,eliminating the need for surgical intervention.
S073TREATMENT OF URETEROPELVIC JUNCTION OBSTRUCTION IN CHILDREN WITH A LAPAROSCOPIC VASCULAR SLING TECHNIQUE AND PELVIC PEXY: A CASE SERIES, KrisMilbrandtMD,SarahWongBS,AnthonyCookMD,AlbertaChildren’sHospital,Calgary,Alberta,CanadaBackground:TheoptimaltreatmentforUPJobstructioninchildrenhasnotbeensettled.Ofparticulardiscussionistherolethatanteriorcrossing vessels have in either causing an external mechanical type obstructionattheUPJregionorareinnocentbystanders.Treatmentsin the past have included endopyleotomy, open or laparoscopic dismembered pyleoplasty, and recently a vascular slinging technique tomovethesevesselsoutoftheway.Wedescribeourcaseseriesofpatients utilizing a vascular sling technique in combination with a renal pelvis pexy with excellent results to date. Results: Three patients have been treated with a laparoscopic vascular sling procedure where we mobilize the crossing lower pole vessels,anchorthemtothelateralGerota’sfasciaoverthekidney,and pexy the renal pelvis down to the psoas muscle to splay open thisregionandrelievetheobstruction.Intraoperativevideoandpicturesareincludedinthetechniquesection.Averageoperatingtime was 122 mins including time for cystoscopy, pyelogram, and stentplacement.Intraoperativebloodlosswasminimalandnocomplicationsoccuredpostoperatively.Patientsweredischargedfromhospital,onaverage,within2.2days.Follow-upimagingafterstent removal has demonstrated excellent relief of the mechanical obstruction and relief of symptoms at one year. Conclusion: Thelaparoscopicvascularslingprocedure(LVS)withrenal pelvis pexy appears to be an attractive solution to those patients with evidence of an external compression from crossing vessels.Shorttermfollowuphasbeenencouragingbutlongertermoutcomes will need to be verified. INDEX WORDS: UPJobstruction,crossingvessels,vascularsling,pediatric
S074FUNCTIONAL OUTCOME AFTER LAPAROSCOPIC DISMEMBERED PYELOPLASTY IN CHILDREN, PhilippOSzavayMD, Tobias Luithle MD,JoergFuchsMD,DepartmentofPediatricSurgeryandUrology,Children’sHospital,UniversityofTuebingenIntroduction: Laparoscopic or retroperitoneoscopic pyeloplasty for uretero-pelvic-junction(UPJ)obstructioninchildrenhavebecomeroutineprocedures.Purposeofthisstudywastoevaluatefunctionaloutcome, i.e. differential renal function of patients who had undergone laparoscopic dismembered pyeloplasty. Patients and Methods: BetweenMarch2004andOctober200870children underwent laparoscopic dismembered pyeloplasty. Median follow-upwas24months(1-48).Werevieweddifferentialrenalfunction with diuretic renography before as well as 3 and 12 months afteroperation.Datawerecomparedto30patientsundergoingopenpyeloplastybetweenFebruary2003andJune2006. Result:Inthelaparoscopicgroupmedianageatoperationwas20months(1-178).Medianoperatingtimewas140minutes(95-220).Intra-orperioperativecomplicationsoccurredin4patients.Inone patient a minor perforation of the colon lead to severe septic peritonitis.Meandifferentialrenalfunctionoftheoperatedkidneywas 46% preoperatively, as well as 3 months and one year after operation.Nosignificantdifferencecouldbenoticed(p>0.05).Intheopenpyeloplastygroupmedianageatoperationwas7.5months(2-180).Medianoperatingtimewas115minutes(50-280).Inthisgroupnointra-orperioperativecomplicationsoccurredanddifferentialrenal function was preserved in all patients. Conclusion: Intermsofpreservationofdifferentialrenalfunctionthe laparoscopic approach is as effective as standard open surgery.

44 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Oral AbstractsOperatingtimesforlaparoscopicpyeloplastyarecompetitive.Asdescribedinliterature,complicationssuchasperforationofthe bowel may occur. Therefore we conclude that laparoscopic pyeloplasty requests large experience in laparoscopic pediatric urology.
S075IS BALLOON BURST PYELOPLASTY A USEFUL ALTERNATIVE TO OPEN OR LAPAROSCOPIC PYELOPLASTY?, BomaAdikibiMD, RachelMHallMD,A.GrahamWilkinsonMD,GordonA.MacKinlayMD,RoyalHospitalforSickChildren,Edinburgh.Introduction: Wereviewourexperienceofendoluminalballoondilatationforpelvi-uretericjunctionobstructionover13years. Methods: Aretrospectivereviewwasperformedonallpatientsthatunderwentballoondilatationinourinstitution.WeutilisedadrainagescorederivedfromtheMAG3diureticrenographyconverting the time to half counts to a numerical value ranging from 1-aT1/2<15minsto6-arisingcurveat55minutes.Ultrasonographywas used to measure the anterior posterior diameter of the renal pelvis(APD)beforeandafterintervention. Results: There were 50 endoluminal balloon dilatations performed in 44 patients since 1995. 31 patients were male.The age range was 5 months to 18 years and 6 months with a median of 5 years and 8 months.There were 29 primary procedures performed on 28 patients. Thepre-balloonmedianAPDwas30mm(range6.7-75mm).ThemedianMAG3scorepriortointerventionwas4(range1-6).Pre-operative imaging is incomplete for 5 patients. WehavecompletepostoperativeimagingforhalfthepatientsandthisdemonstratesareductioninthemedianpostprocedureMAG3scoreto2(range1-4)andthemedianAPDto21mm(range9-43). 20% required further surgical intervention.There were 21 balloon dilatationsperformedon16patientswhohadrecurrentPUJOaftertreatment. The previous treatment entailed 12 open pyeloplasties, 8 endoluminal balloon dilatations, 4 nephrostomies and 1 retroperitoneoscopic pyeloplasty. Thepre-proceduremedianAPDandMAG3scorewas38mmand5respectivelywithrangesof18-70and4-6.ThemedianMAG3scorefellto3(range1-3)afterintervention.TheAPDalsodecreasedtoamedianof19mm(range8-32).57%requiredsubsequentintervention.Halfofthepatients(6)hadrepeatballoondilatation.Oftheremainingsixpatients2requiredanopenpyeloplastyand2subsequently had nephrectomies performed. Conclusion: OurresultsdemonstratethatballoondilationforPUJOiseffectivewithadecreaseintheMAG3drainagescoreandtheAPD. Overall36%ofpatientsrequiredfurtherintervention.Themajorityofthesepatients(66%)hadrecurrentPUJOafterprevioustreatment,most commonly with open pyeloplasty . 50% of the patients who required further intervention in the primary group had significant reduction in function at the time of intervention.
S076LAPAROSCOPIC MANEUVER FOR ORCHIDOPEXY IN HIGH INTRA-ABDOMINAL TESTES WHEN CREMASTERIC ARTERY IS PRESENT: A TECHNICAL REPORT, ClaudioDeCarliMD,MichaelLeonardMD,MarcosBettolliMD,LuisGuerraMD,UniversityofOttawa,Children’sHospitalofEasternOntario.DeptofSurgery-DivisionsofPaediatricUrologyandGeneralSurgeryIntroduction: Preservationofthetesticularbloodsupplyiscrucialforthemanagementofintra-abdominaltestesduringlaparoscopicorchidopexy.Independentofthepreferredtechnique(Fowler-Stephensorprimarydescent),thecomplementarybloodsupplyis essential for testicular survival. The deferential and cremasteric arteries are both responsible for the testicular collateral circulation. However,cremastericartery(CA)isunderestimatedbythemajorityofsurgeons.AnatomystudyinfetusdemonstratedthepresenceofCAin72%ofthecases.Dissectionsinpediatriccadaversrevealedtheexistenceoflarge-caliberanastomosisbetweentheCAandvasal-testicularsystemin50%ofthespecimensexamined.Wereportacaseofahighintra-abdominaltestis(HIT)associatedwithpresenceofCA.OurprimaryaimistodescribethemostadequatesurgicalapproachforlaparoscopicorchidopexyandpreservationoftheCA. Methods and patient:Usinga3-porttechnique,5mminstrumentsand a 0 degree scope, abdominal exploration was carried out in a 2 year-oldboywithleftnon-palpabletesticle.Thetesticlewasfoundin a high intra abdominal position next to the left iliac vessels and theinternalinguinalringwasnotopen.Dissectionofthetesticularand deferential arteries was performed to achieve primary testicular descent.TheCAwasidentifiedrunningparallelandanteriorto
the deferential vas, arising from the inferior epigastric artery and ending at the lower pole of the testicle. The deferential artery was seen between the umbilical ligament and the bladder and joining thedeferentialvas.Primarytension-freeorchidopexywasachievedperformingthePrentissmaneuverwhilepreservingtheCA. Conclusion: InthepresenceofHIT,surgeonsshouldbeawareoftheCAaspartofthetesticularcollateralcirculation.Acarefuldissectionof the spermatic cord allows for the identification and preservation oftheCA,whichmayimprovetesticularsurvivalinHIT.ThePrentissmaneuver was used to avoid compression and strangulation of the CAaroundtheepigastricvesselswhiledescendingthetesticle.
S077LAPAROSCOPIC EXTRAVESICAL REIMPLANTATION FOR VESICO-URETERAL REFLUX., ManuelLopezMD,EmmanuelleGuyeMD,MichelFrançoisMD,FrançoisVarletPhD,DepartmentofPediatricSurgery,UniversityHospitalofSaintEtienne-FranceINTRODUCTION: Laparoscopy may have a place in the treatment ofvesico-ureteralreflux(V.U.R).WereportourinitialexperienceinthetreatmentofV.U.Rbylaparoscopicextravesicaltransperitonealapproach(L.E.T.A)todescribetheevolutionandtoevaluatetheresults and benefits of this technique for theses patients. MATERIALS AND METHODS: BetweenAugust2007andOctober2008,14children(20ureters)withV.U.Randdeteriorationofrenalfunctiononisotoperenography(8unilateraland6bilateral)weretreatedwithL.E.T.A(Lich-Gregoirtechnique).Themeanagewas48.2months(range12-62),andtherewere11femalesand3male.Twopatientshadadoubletotalcollectorsystemassociatedwithrefluxinalowersystem.Oneofthemwithalittleureteroceleandanotherwith complete deterioration of upper polar rein function. RESULTS: The mean surgical time was 70 minutes in unilateral and 120inbilateralV.U.R.Allproceduresweresuccessfullycompletedlaparoscopicallyandtherefluxwascorrectedinallpatients,atthesame time, 1 heminephrectomy and 1 ureterocele were removed bylaparoscopyandendoscopy.Wehad1ureterperforationwithleakagefifteendaysafterpostoperativeandunderwentaredo-procedure.Themeanhospitalisationwas24hours.Thefollow-upwasranging6-20months,withoutrecurrenceofRVU. CONCLUSION:L.E.T.AforR.V.Uisasafeandeffectiveapproachevenin unilateral, bilateral simultaneous and duplex ureters, with success rates similar to the open technique, and a dramatic reduction in postoperative stay.
S078OUR EXPERIENCE OF A SINGLE PORT LAPAROSCOPIC APPENDECTOMY IN CHILDREN, TakashiNogamiBA,MakotoyagiBA,yukoUdatsuBA,HidekiyoshidaMD,yujiMorishitaMD,HitoshiShiozakiMD,HarumasaOhyanagiMD,DivisionofPediatricsurgery,DepartmentofSugery,KinkiUniversityofMedicine[Background and purposes]Laparoscopicappendectomy(LA)hasbecomepopularforthetreatmentofacuteappendicitis.SinceLAwas first described, its modification has been reported many times. Also,asingle-portLAhasannouncedfromseveralinstitutions.Weintroduceoursimpletechniqueofasingle-portLA. [Materials and Methods] AsingleportLAwasattemptedfor22patients(8boysand13girls).Theirageranged4yearsto15years.Undergeneralanesthesia,a12-mmtrocarwasinsertedthroughumbilicus. The finger part of latex surgical gloves covered the orifice ofthetrocartopreventairleak,whena5-mmcameraanda5-mmforceps were inserted into the trocar at the same time. The appendix was grasped and dissected from the surrounded tissues with a single grasper or a dissector. The grasped appendix was withdrawn into the trocar and extracted from the abdominal wall with the trocar. The appendix was removed using a conventional procedure outside of the abdominal cavity. [Results] Laparoscopic appendectomy was completed in 13 casesthroughasingleport.Additionaltrocarwasrequiredin8complicated cases. [Conclusions] This unique method further improves minimal invasivenessofLAbecauseofusingasingleport.Thistechniqueis a safe and highly minimally invasive procedure with excellent cosmetics and cost effectiveness.
S079ENDOSCOPIC TREATMENT OF DUODENAL WEBS ON PEDIATRIC PATIENTS,F.yankovicMD,F.saituaMD,CcastilloMD,CnavarreteMD,LuisCalvoMackennahospital,ClinicaAlemanadesantiagoIntroduction:Partialduodenalobstructionduetoduodenalwebs

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 45
2009 Oral Abstractsisaninfrequentcondition,seenmostlyonnewbornpatients.Opensurgeryisthestandardmanagement.Wereportfourpediatriccases of duodenal webs treated by endoscopic surgery. Patients and methods:FromMarch2007toJune2008,twonewbornandone 14 years old child, with diagnose of duodenal webs, received endoscopictreatment.Undergeneralanesthesia,endoscopywasperformed.Afterfenestratedmembranevisualization,a12,15or 20 mm. hydrostatic balloon was used for web dilatation. Then, usinganeedleknifesphincterotome,weperformed2or3cutsintherestofthemembrane,oppositetotheVaterampulla.Results: Allthreepatientsweresuccessfullytreated.Meansurgicaltimewas50minutes.Oralfluidsstartedonthesameday.Allpatientsweredischarged without complications and all of them are asymptomatic (meanfollowupof5month).ConclusionEndoscopictreatmentof duodenal webs seems to be a valid minimal invasive therapeutic option. The procedure is a safe and effective, reduces surgical time, postoperative fasting time and length of hospitalization.
S080RIGID NOTES: THE TRANSURETHRAL APPROACH IN FEMALE PIGLETS, Martin L Metzelder MD, Joachim F Kuebler MD, Gertrud VietenPhD,JanGosemannMD,BennoMUrePhD,DepartmentofPediatricSurgery,HannoverMedicalSchool,Hannover,GermanyBackground:NaturalOrificeTransluminalEndoscopicSurgery(NOTES)hasbeenintroducedtoreducescarsandthesurgicaltrauma.Thefeasibilityofthistechniqueinchildrenisnotknown.Theaimof our animal study was to determine the feasibility of various procedures via a transurethral assisted approach. Materials and Methods: SpeciallydesignedAesculap-Braun©instrumentsandEndoligasure©wereusedin12anesthetizedandmechanicallyventilatedfemalepiglets(meanweight15.2kg;range:14-17).Amodified12mmtrocarincludinga30degreeopticandaworkingchannelwasusedfortheumbilicalapproachandforCO2insufflation(8mmHg,Flow5L/min.)Subsequently,a3mmtrocarincluding a 2mm optic was introduced via the urethra and the dome of the urinary bladder into the abdominal cavity. The endpoint of the studywasthefeasibilityofnephroureterectomy(n=8)andbilateraltuboovarectomy(n=4). Results:Allnephroureterectomiesandbilateraltuboovariectomieswereperformedsuccessfully.AttheendoftheprocedurestheurinarybladderwassafelyclosedwithEndoloops©viatheumbilical“Twoinonesystem”.Intracorporalsuturing,knottingandplacementofEndoclips©duringnephrectomyweretimeconsumingduetorestrictedmotionofthe“Twoinonesystem”.Theuseofavesselsealing device allowed a safe, fast and easy nephroureterectomy. Conclusions: Modifications of instruments and approaches aremandatoryforNOTES,andtheyhavetobetestedinanimalmodelsbeforebeingusedininfantsandchildren.Weshowedthatnephrectomy and tuboovarectomy can be performed safely via a transurethral and umbilical approach in female piglets. The use ofvesselsealingdevicesisessentialin“Twoinonesystems”withlimited view and range of motion.
S081SCARLESS ABDOMINAL SURGERY: SINGLE INCISION LAPAROSCOPIC SPLENECTOMY, CHOLECYSTECOMY, AND APPENDECTOMY, SanjeevDuttaMD,DivisionofPediatricSurgery,LucilePackardChildren’sHospital,StanfordUniversityIntroduction:SingleIncisionLaparoscopicSurgery(SILS;akaSinglePortAccess(SPA))involvesperformingabdominaloperationsby placing multiple wristed laparoscopic instruments through a single small incision hidden in the umbilicus. The primary goal is toavoidanyvisiblescarring.ExperiencewithSILSappendectomy,cholecystectomy, and splenectomy is described. Methods: Aretrospectivereviewwasconductedof18consecutiveinpatientSILSprocedures(12M:6F;agerange2to17yrs.)fromMaytoSeptemberof2008.Outcomemeasuresincludedneedforconversion, operative time, cosmetic outcome, and complications. Results: There were 4 total splenectomies, 2 combined splenectomy/cholecystectomies,2isolatedcholecystectomies,and10appendectomiesperformed.Allprocedureswerecompletedsuccessfully without need for conversion to standard laparoscopy or opensurgery.Apatientwitha28cmspleenhadcompleteresectionusingSILS,butspecimenremovalwasthroughaPfannenstielincisionduetolackofanadequatelysizedendobag.Meanoperativetimewas 90 min for splenectomy, 67 minutes for cholecystectomy, 165 minutesforcombinedsplenectomy/cholecystectomy,and35minforappendectomy. Mean hospital stay was 1 day for appendectomy,
1dayforcholecystectomy,and2.5daysforsplenectomy.Onesplenectomypatientreceived1unitPRBCtransfusion.Allfamilieswere very pleased with the cosmetic outcome. Conclusions: SILSisfeasibleforavarietyofpediatricgeneralsurgical conditions, allowing for scarless abdominal operations. This early experience suggests that outcomes are comparable to standardlaparoscopicsurgerybutwithimprovedcosmesis.SurgeonsperformingSILSshouldhaveafirmfoundationinadvancedminimalaccesssurgicalskills,andacautious,gradatedapproachtoattempting the various procedures. Technological refinements will furtherenableSILS.Furtherstudieswillconfirmthesefindingsanddetermine if there are any benefits in terms of pain or recovery.
S082EXPERIENCE WITH MODIFIED SINGLE PORT LAPAROSCOPIC PROCEDURES (SPA) IN CHILDREN, StevenSRothenbergMD, The RockyMountainHospoitalforChildrenPurpose: To determine the safety and efficacy of limited access laparoscopic procedures in children using a modified single port access(SPA)technique. Methods:Anumberofdifferentbasiclaparoscopicprocedureswere attempted using a modified 8mm operating endoscope with a 4mm 6 degree lens and an incorporated 3mm operating channel. Most cases also involved a single 3mm stab wound or port for an additionaloperatinginstrument.ProceduresperformedincludedAppendectomy-5,Cholecystectomy-3,Enterolysis-1,Ovariancystectomy-1,andingunalheriarepair-10.Patientsagesrangedfrom10monthsto16yearsandweightfrom7to60kg. Results: Allprocedureswerecompletedsuccessfully.Therewerenooperativeorpost-operativecomplications.Allpatientsweredoneasdaysurgeryor23hourobservation.Operativetimeswerelongerthen standard laparoscopic procedures for the author, but no direct comparrison was made. Conclusion:AmodifiedSPAtechniqueappearstobeasafeandviablealternativetostandardlaparoscopicapproach.Visualizationand safe tissue manipulation is more difficult. The addition of a single 3 mm instrument allows for easier dissection, triangulation, and almost invisible scar and may be more beneficial then creating a 20mm incision in the umbilicus to allow for the insertion of multiple instruments
S084PRELIMINARY EXPERIENCE WITH SINGLE INCISION LAPAROSCOPIC SURGERY IN CHILDREN, ToddAPonskyMD,ScottBoulangerMD,WalterChwalsMD,EdwardBarksdaleMD,RobertParryMD,RainbowBabiesandChildren’sHospital,CaseWesternReserveUniversityIntroduction: Singleincisionlaparoscopicsurgery(SILS)hasrecentlybeen described in adults. Here we report our preliminary experience ofSILSinchildren. Methods: AretrospectivereviewwasperformedoftheoperativedatabaseatRainbowBabiesandChildren’sHospitalinCleveland,Ohiofrom3/2008to11/2008lookingforallcasesthatwereperformed through a single laparoscopic incision. Results: Atotalof38SILScaseswereperformed.Theseincluded:cholecystectomy,splenectomy,intussusceptionreduction, gastrostomy tube placement, and appendectomy. Two appendectomieswereconvertedtotraditional3-portlaparoscopyformesoappendix bleeding and a long appendiceal stump. There was one umbilical wound infection after an appendectomy (erythema thatrespondedtoantibiotics).Therewerenoothercomplications. Conclusion: Preliminaryexperiencewithsingleincisionlaparoscopicsurgeryinchildrenappearstobesafeandeffective.Greaternumbersand a prospective trial will be necessary to assess the true benefit of this approach.
SingleIncisionLaparoscopicProceduresProcedure N Age(yr)/Wt(kg) ORTimeChole. 5 13.3y/59kg 1:48Splenectomy 1 16y/53kg 3:53Intussusception 1 1.67y/12kg 0:35Gastrostomy 7 1.51y/7kg 0:35Appendectomy 22 10.6y/45.8kg 0:43

46 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Oral AbstractsS086A HOMEMADE GRASPER FOR “SINGLE CONVENTIONAL PORT” LAPAROSCOPIC APPENDECTOMY: SWING POYLPROPYLENE SUTURE INTRODUCED THROUGH A SINGLE VASCULAR NEEDLE, FezaMAkgurMD,MustafaOlgunerMD,GulceHakguderMD,OguzAtesMD,DepartmentofPediatricSurgery,DokuzEylulUniversity,Schoolofmedicine,Izmir,TurkeyPurpose: In“singleconventionalport”intracorporeallaparoscopicappendectomy(SCP-ILA),theappendixishungwiththeaidofatransabdominalSLINGsuturepassedusingneedleholderandsurgicalneedle.SLINGsuturereplacesthesecondportanddoesnotcauseanyscar.TofacilitatethetransabdominalSLINGsutureplacementwehaddevelopedanewtechnique:transabdominalSWINGsutureintroduced through a single vascular needle. Materials and methods: DuringJanuary2008-November2008,67patients(38boys,29girls)underwentSCP-ILA.An11mm“conventionalumbilicalport”throughwhicha10mmscope(0o)withaparalleleyepieceand6mmworkingchannelwasinserted.The appendix was grasped and dissected from the surrounding tissues.A16Gvascularneedlewasinsertedpercutaneouslyfromrightlowerquadrantintotheperitonealcavity,afoldedUSP0or1polypropylene suture was passed through the vascular needle and theneedlewaswithdrawn.ThusaSLINGwasformed,whichwecallitaSWINGregardingitsswingingcapabilities.GraspedappendixwasplacedwithinthisSWINGsutureandtractionwasappliedonthesuturetohangtheappendix.AppendixhangingpositionwaschangedbyreleasingtheSWINGsutureandrepositioningtheappendixasrequired.Afterdissectionofthemesoappendixwithhookcautery,thebaseoftheappendixwasligated.Theappendixwas extracted together with the trocar. Results: Thepatientsaged5-17years(mean8.2±3.2).SCP-ILAwas performed successfully in all the patients and no complications observed.TransabdominalSWINGsuturefacilitatestheintroductionoftheSLINGsutureespeciallyinobesepatients.Italso,withitsswinging capability, enables the repositioning the appendix. Previouslyweuseda“non-conventionaldoublelumen11mmport”through which 5 mm scope and a 5 mm instrument were passed separately.Usageofa“singleconventionalport”throughwhichasingle10mmsidewievingscopewitha6mmworkingchannelisinserted provides easier control ofthe camera movements. Keeping thetargetinthemiddleoftheviewandadjustingzoomin-zoomoutpositionsareeasierasthecameramovesparallelwiththeworkinginstrument, surgeon only controls zoom. Conclusion:InSCP-ILA,LAcanbeperformedwithoutthenecessityof a cameraman as surgeon can control the camera movements byhim/herself(singlesurgeontherapeuticlaparoscopythroughsingleconventionalport).NewhomemadetransabdominalSWINGsuturefacilitatestheintroductionoftheSLINGsutureespeciallyinobesepatients.Italso,withitsswingingcapability,enablestherepositioning the appendix as required
S085TRANSUMBILICAL LAPAROSCOPIC ASSISTED APPENDECTOMY (TULAA) IN CHILDREN – FIRST EXPERIENCES., RobertBergholzMD,ThomasKrebsMD,KatharinaWenkeMD,AltonaChildren’sHospital,UKEMedicalSchool,UniversityofHamburg,GermanyBACKGROUND: Aimofourstudywastoevaluate,whethertransumbilicallaparoscopicassistedappendectomy(TULAA)issuccessful and safe in children with appendicitis. MATERIAL AND METHODS:FromSeptembertoOctober2008,children with appendicitis were selected for laparoscopy via umbilicalincision(10mmport,0°-videsocope,integratedinstrumentchannel).ItwasintraoperativelydecidedwhethertoproceedwithTULAAorchangetoathree-portapproach.InTULAA,afterfreedfrom adhesions, the appendix was grasped and pulled through theumbilicalincision.Disinflationofthecapnoperitoneumallowed exteriorization and ligation of the appendix as in open appendectomy.Afterrepositionofthecoecumintotheabdominalcavity,thelaparoscopewasre-introducedtocheckforanydamage.TheabdomenwasirrigatedwithRinger’s-solution,drainswereputinwhennecessaryandtheileumwasinspectedforMeckel’sdiverticulum.Cephalosporinesandmetronidazoleweregivenforantibiotic prophylaxis. Patientswereevaluatedprospectivelyforage,sex,timetofirstandfulloralintake,operativetime,durationofhospitalstayandcomplications. RESULTS: 44childrenwithappendicitiswereoperatedon:acohortof6patients(4female,2male)withTULAA.Medianoperativetimewas72minutes(range53-93minutes).Therewerenointraoperativeor postoperative complications and no conversions. Time to first oralintakewasoneday,andallpatientswereonfulloralfeedsonpostoperative day 3. Median duration of hospital stay was 5 days (range4-6days).Thelearningcurveshowedadecreaseinoperativetime.Adaptationtothe0°-videoscopeandthepartialblockingofthevisualfieldwhenoperatinganinstrumentintheworkingchannel was the most demanding and time consuming part of the procedure.Becauseonlyoneinstrumentcanbeused,inspectingthesmallintestinetoexcludeMeckel’sdiverticulumwasnearlyimpossible, even in extreme Trendelenburg position. DISCUSSION: TULAAisasafeandsuccessfulalternativetothree-portlaparoscopicappendectomyinchildren.Itwieldstheadvantageofreducingthecostsforsurgery,becausenostaplingorendo-loop devices are needed. The postoperative course is similar as expectedintraditionalthree-portorconventionalappendectomy.Anyadditionalprocedureishardertoperformwithonlyoneinstrumentathand.Performinglargerscalecontrolledtrialsshouldbe encouraged.

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 47
2009 Video AbstractsV001LAPAROSCOPIC EXCISION OF LARGE HEPATIC CYST, ParissaTabrizianMD,AdheeshSabnisMD,PeterMidullaMD,MountSinaiSchoolofMedicineWedescribeacaseofa2monthold,3kgfulltermfemalewhowasfoundtohavealargeintra-abdominalcysticlesionofunknownorigin on prenatal ultrasound. The cyst was found to originate from the inferior left lateral segment of the liver and was successfully resectedlaparoscopicallywiththeuseoftheHarmonicScalpel.Hepatic cysts are rare in the pediatric population and their optimum treatmentunclear.Inalargeseriesof400cases,only12werereported in children under 2 years of age. They account for 10 % of benignhepaticlesionsinchildren.Congenitallivercystsarebenignand result from isolated aberrant biliary ducts. Failure of complete excision of the cyst has been associated with high recurrence rate. This has been attributed to failure in ablating the secreting lining of the cyst wall. Laparoscopic hepatic cyst excision was first described in1991byPaterson-BrownandGardenusingaNd-yAGlaser.Thistechnique has been well described in the adult population. However, there is a paucity of literature in the treatment of neonatal liver cysts.Ourapproachconsistedofalaparoscopicenblocresectionofthehepaticcyst.Werecommendthistechniqueassafeandfeasible.
V002INTRATHORACIC KIDNEY: MIS APPROACH, MarioRiquelmeMD, ArturoArandaMD,EnriqueVillarrealMD,SanJoseHospital,ITESMUniversity,Monterrey,MexicoIntroduction: This case is of a 3 year old female, with the past medical history of having recurrent respiratory infections and two hospitaladmissionsforpneumonia.SheisevaluatedwithChestXraysandanelevationoftherightdiaphragmisnoted.OnCTAngio,therightkidneyisseeninaveryupwardposition,abovetheleftlobeoftheliver,withaverythindisplasticdiaphragm.Thekidneyhilumis oriented down and inward. The renal artery is long, and travels diagonally after arising from the abdominal aorta. Materials and Methods: The patient is selectively intubated. Then,sheispositionedinrightlateralposition.Withtherightlungdown,threetrocars,5mmeach,areplaced.Gentleinsufflationupto 5mmHg is achieved. The diaphragmatic defect is observed, with thekidneyoccupyingthelowerandposteriorareaofthethoraciccavity.Weassessedthediaphragmandencounteredaverythin,flexible,softtissue.Then,weproceededtoperformadiaphragmaticplacationusingPolyestersuture2-0.Theneedleisstraightenedinordertofacilitateitsentrancethruthetrocar.So,theplicationisstartedwiththisstitchanddoingintra-corporealknottying.Sequentialstitchesareplacedandintermittentlywestoppedinordertoassesstheoperationandtoseehowfardownthekidneywasbeingpusheddowntowardsanabdominalposition.Atotalofeleven stitches were placed in order to achieve the desired degree of plication.Attheendoftheoperation,clipsareplacedinsomesutureknotsinordertohaveaneasyfollow-upoftherepairareaonchestX rays. Results:Patientrecoveredwellandwasdischargedhomeinpostoperativedaythree.Onfollowupshehasremainedasymptomatic.And,onXrays,therepairedarealooksintact. Conclusion: TheuseofMISprovidesaverygoodapproachtoperform diaphragmatic plication, without any downsides.
V003THORACOSCOPIC PATENT DUCTUS ARTERIOSUS LIGATION IN VERY LOW BIRTH WEIGHT INFANTS UTILIZING A NOVEL RETRACTOR, JeffreyRLukishMD, The National Naval Medical CenterandWalterReedArmyMedicalCenterINTRODUCTION:Patentductusarteriosus(PDA)ligationisapotentially life saving procedure that is often required in very low birthweightinfants(VLBW).Thoracoscopyisanidealapproach.However,thoracoscopicPDAligationhasonlybeenreportedininfants greater than 1500 grams, there is no data documenting atechniquethatcouldbeutilizedinVLBWinfants.WepresentatechniqueutilizinganovelretractorthatallowssafePDAligationinthese neonates. METHODS: This infant is a 740 gram neonate who developed perforated necrotizing enterocolitis 4 days prior to this operation. He was treated with drain placement and is stable. He was not a candidate for medical therapy. He underwent a left thoracoscopic PDAligation.Athoracostomytubewasnotutilized. RESULTS: This infant recovered uneventfully and post operative echo
confirmedligationofthePDAwithnoductalflow.Postoperativechest xray did not show a pneumothorax. The operative time of this procedure was 25 minutes. CONCLUSIONS:Ourtechniqueisminimallyinvasiveandprovidessuperior visualization of the patent ductus arteriosus and surroundinganatomiclandmarks.Utilizingthisnovelretractor,thoracoscopicPDAligationissafeandfeasibleineventhesmallestinfants. The ease and practicality of thoracoscopy utilizing this retractor may facilitate the performance of more advanced thoracoscopic procedures in very low birth weight infants.
V004LAPAROSCOPIC BILATERAL GONADAL RESECTION AND HERNIOPLASTY IN 46 XY DSD FEMALE RAISED PATIENTS . HOW WE DO IT., MBailezMD,ARuesmannMD,DiagnosisandTreatmentArgentineInstitute.BuenosAires.ArgentinaDiagnosisandTreatmentArgentineInstitute.BuenosAires.Argentina MostofDSD46xypatientsraisedasfemalesrequireearlygonadal(usuallytesticles)resection.Quiteanumberofthesepatientshaveaconcomitant inguinal hernia. Aim : The aim of this video is to show different technical details of a simultaneous laparoscopic treatment. SurgicalTechnique:Twopatientsundergoingthisprocedureareshown to illustrate our preferred surgical strategies.Their ages were 3and6monthsold.OnehadatesticulardysgenesisandtheotheraCAIS(completeandrogeninsensitivitysyndrome). A4mm30degreelensintheumbilicuswasusedinboth.A3mmportforaMarylanddissectorwasusedforthesurgeon’slefthandandashort 5mm for the left. .Differentinstrumentswereusedfordevascularization:a5mmbipolar sealer in one and a bipolar Robi( a variant that lets you grabthetissueanddissectwithaKellyliketip)Weavoidchanginginstrumentsoptimizingitsuseineverymaneuver:forexamplewhenwe introduce the Robi we dissect grab and fulgurate all the gonadal vascular supplies in both sides and then change to scissors. Openprocessusvaginaliswereclosedwithalaparoscopicsuturein2differentways:acompletedissectionoftheperitoneumsurroundingthe inguinal ring before placing the suture was done in one and a closure stich at the time of gonadal resection in the other . Bothgonadswereremovedgentlythroughthe5mmport.
V005ROBOTIC RESECTION OF A MEDIASTINAL NEUROBLASTOMA, JohnJMeehanMD,SeattleChildren’sHospitalThis video is an example of using robotic surgery to resect a solid chesttumorandalsoanintroductionofanew8.5mm3-Dcamera.A5 month old boy presented with new onset lower extremity paralysis. Workuprevealedalargemassintherightchestthatwastraversinginto the spinal column through a nerve foramina creating spinal cord impingement. The initial size of the tumor was 7.4 x 4.2 x 7.4 cm. Biopsyconfirmedaneuroblastomaandheunderwentchemotherapywith a reasonable reduction in tumor size. His paralysis also resolved duringchemotherapy.Thetumorshrunktoasizeof6.2x1.8x4.9cm and surgery was planned using robotic technology. The child was now8monthsoldand7.3kginweight.Anew8.5mm3-Dcamerawas used in this procedure along with two 5 mm robotic ports. Additionally,one5mmhandheldaccessoryportwasneededforsuctioning and assisting in retraction. The video will demonstrate the highlights of the case including positioning of the robot and trocar placement.Nodifficultieswerenotedwiththisnew3-Dcameraandthe visualization was excellent. The tumor was resected en bloc and achesttubewasleftinplace.Asmallchylousleakwasnotedduringfeeding which delayed his discharge but this resolved after about 48 hours.Hewenthomeonpost-opdaynumber4. Summary: Robotic technology affords excellent mobility for resecting solid mediastinal tumors even in small children. The additionofthe8.5mm3-Dcameraimprovesvisualizationandisareasonable sized camera for thoracic procedures even in the small chest of an infant.

48 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Video AbstractsV006SINGLE SITE LAPAROSCOPIC SPLENECTOMY IN A CHILD, Todd APonskyMD,ScottBoulangerMD,RainbowBabiesandChildren’sHospital,CaseWesternReserveUniversityBackground: Laparoscopic splenectomy was described in 1993 by Tulman et al. This has become the preferred technique for spleen removal as it leads to less pain, better cosmetic outcome, and shorter hospitalstaythantheopenapproach.Herewedescribeasingle-sitelaparoscopic splenectomy in a child. Case: This patient is a 12 year old male with idiopathic thrombocytopenicpupura(ITP)thathasbeenrefractoryto6monthsof aggressive medical therapy. The decision was made to perform a laparoscopic splenectomy through a single incision in the umbilicus. Oneumbilicalskinincisionwascreatedthroughwhichtwo5mmand1 12mm ports were placed through the fascia. The splenectomy was performedusingflexible,reticulatinginstruments.Atthecompletionof the case the three incisions were connected to create one 15mm fascialincision.Therewasminimalbloodlossandnointra-operativeorpost-operativecomplications.Thepatientisdoingwellwithnovisiblescar1monthspost-operatively. Conclusion: SingleSiteSplenectomyisfeasible.Alargerserieswillbenecessarytoassesssafety,painreduction,andcost-efficiency.
V007MODIFIED SINGLE PORT CHOLECYSTECTOMY IN A CHILD, StevenSRothenbergMD,TheRockyMountainHospitalForChildrenPurpose:ThereisagreatdealofinterestinNOTESandSinglePortAccesssurgeryinadultMIS,howevertheapplicationsinthepediatricpopulation are still unclear. This video represents one of our initial attemptsatamodifiedSPAprocedureinachild. Methods:A9yearoldmalewitha4monthhistoryofRUQabdominalpainandawork-upconsistantwithbiliarydyskenesiaunderwent laparoscopic cholecystectomy. The patient weighed 34 Kg. The procedure was performed using a special modified 8mm operating laparoscope with a built in 4mm 6 degree telescope and a4mmoperatingchannel.Asecond3mmportwasplacedintheepigastrium for a second operating 3mm instrument. Results: The procedure was completed successfully laparoscopically withoutcomplication.Operativetimewas38minutes.ThepatientswasdischargedthefollowingmorningonIbuprofenforpain,onaregular diet, and with no activity restrictions. Conclusion: This procedure demonstrates that a more limited access laparoscopiccholecystectomyissafeandviableinchildren.Whilethisis not a true single port procedure we feel it may be more acceptable and beneficial then creating a 15 or 20mm umbilical incision which in a child can result in significant pain and perhaps more cosmetic abnormality then a single 3mm epigastric port.
V008LAPAROSCOPIC REPAIR OF TRAUMATIC ABDOMINAL WALL HERNIA FROM HANDLEBAR INJURY, ErinERowellMD, AnthonyCChinMD,Children’sMemorialHospitalINTRODUCTION:A14yearoldboypresentsafterflippingandfalling over the handle bar of his bicycle. He was seen at an outside hospital and discharged home. He was subsequently seen in our emergencyroomwithpersistentcomplaintsofpain.ACTscanrevealed disruption of the muscles of the upper right abdominal wallcontainingthehepaticflexurewithasmallamountofintraperitonealfreefluid.Thepatientwaspreparedforadiagnosticlaparoscopy for repair of a traumatic abdominal wall hernia and possible hollow viscus injury. METHODS: The procedure was approached with a laparoscopic techniqueusing3ports(2-5mmand1-12mm)and2separatestabincisions. The traumatic hernia was repaired utilizing interrupted suturesplacedwithanENDOCLOSE-(Covidien,Mansfield,MA)trocar site closure device. The mesenteric defect in the colon was repaired with intracorporeal sutures. RESULTS: The patient recovered well and was discharged home. He hadcompleteresolutionofhissymptoms.Follow-uprevealednoabdominal wall defect and resolution of his symptoms. CONCLUSION(S): Laparoscopic repair of a traumatic abdominal wall defect and exploratory laparoscopy following trauma is feasible and safeinthepediatricpatient.Itshouldbeconsideredasanalternativeapproach to an exploratory laparotomy for trauma injuries in a stable patient with potentially less morbidity.
V009THORACOSCOPIC REPAIR OF AN H-TYPE TEF IN AN YEAR OLD FEMALE, StevenSRothenbergBA,KristenShipmanBA,TheRockyMountainHospitalforChildrenPurpose: To show and describe the technique of thoracoscopic repairofanH-typefistula. Methods: An8yearoldfemalewithalonghistoryofrecurrentrespiratory infections and reactiove airway disease was found to haveanH-typefistlaonBariumswallow,andwasconfirmedbybronchoscopy. The patient then underwent thoracoscopic ligation anddivisionoftheH-typeTEF.Theprocedurewasperformedthrough3-5mmports., Results:Theproceduretook85minutes.Therewerenointraorpost-operativecomplications.Nochesttubewasleftin.Acontrastswallowonpost-opday1showedtoleakandoralfeedswereresumed.Thepatientwasdischargedonpost-opdaynumber2. Conclusion: This video demonstrates thet thoracoscopic repair of an H_type fistula is a safe and effective technique. The thoracoscopic approach offers excellent visualization, allows for precise dissection, andavoidsthemorbidityofalargeneckincision.
V010EXTRAPERITONEAL SPLENOPEXY FOR WANDERING SPLEEN, EarlCDowneyBA,UniversityofUtahDepartmentofSurgery,DivisionofPediatricSurgeryWanderingspleenprediposestotorsionandischemiaandcanbesymptomatic.Splenopexypreventstorsion.Atechniqueutilizinglaparoscopy is presented that illustrates a simple and effective method for splenopexy using placement of the spleen in an extraperitoneal position.
V011LAPAROSCOPIC TREATMENT OF A RECTOVAGINAL FISTULA. FEASIBILITY ANDTECHNICAL DETAILS OF A RARE ANORECTAL MALFORMATION.(ARM), MBailezMD,EPazMD,VDibenedettoMD,PediatricSurgeryGarrahanChildren’sHospital.BuenosAires.ArgentinaIntroduction: WehavepreviouslypresentedourexperiencewiththelaparoscopictreatmentofselectedARMlikebladderneckandprostatic fistulas in males and high rectocloacal fistulas in females.Encouragedbyitsexcellentvisualizationofpelvicstructuresandmagnification and our functional results we decided to use it in the reconstructionof2femaleswithaveryunusualARM(arectovaginalfistula) The aim of this video is show the feasibility and technical details of this procedure. Surgical Technique: Patientswere.A4mm30degrees20cnlenswas inserted in the umbilicus using the transumbilical approach . Twoworkingportswereused:1left3mmoneinsertedatthemedialedge of the colostomy and 1 5 mm one at the right lower quadrant .Atransparietalstichwasusedtosuspendtheuterustotheanteriorabdominal wall.The fistula was dissected and visualized clearly , suturedwith5/0absorvablesutureanddividedinitsvaginalending. Anexternalandlaparoscopicmusclestimulatorswereusedtolocalizetheanalsiteandthepelvicfloormuscles.A1cmverticalincision was made and proximal dissection under laparoscopic vission achieved.AlowprofileStepVerresneedlewithradiallyexpandingsheat was placed into the perineal wound and passed through under laparoscopic vission and a blunt trocar replaced the needle into the sheat. The rectum was grasped and gently guided down while distendingitsdescentchannell.Itwassuturedtothesurroundingmuscles as in the open procedure and anoplasty done in the usual wayusing5/0sutures.
V012LAPAROSCOPIC REPAIR OF A HIGH UROGENITAL SINUS AND DUPLEX VAGINA, JoergFuchsMD,GuidoSeitzMD,MonikaSchroederMD,JuergenFSchaeferMD,StevenWWarmannMD,UniversityChildrensHospital,DptofPediatricSurgery,Tuebingen,GermanyIntroduction The association of high urogenital sinus and duplex vaginaisarareandcomplexvariantofurogenitalmalformations.BynowthetotalurogenitalmobilisationandthePenaprocedurehavebeen proposed as approach for surgical correction. Here we present the minimally invasive vaginal pullthrough for correction of this condition.

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 49
2009 Video AbstractsPatient and Methods: The girl suffered from hydrometrocolpos immediatelyafterbirth.Diagnosticworkuprevealedaduplexvaginaopening with a single orifice into the proximal dorsal urethra at the levelofthebladderneck.Thedilatedvaginacausedbilateralureteralcompression. The initial management consisted of vaginal drainage. Atthreemonthsofagethesurgicalcorrectionwasperformed.The presented video highlights the initial cystoscopy as well as the definite operative procedure. Results: Weperformedalaparoscopyinwhichtheuterusandvagina were separated from the posterior bladder and bladder neck.Thefistulatotheurethrawastranssectedandtheurethrawassuturedwithinterruptedstiches.Anexpandabletrocarwasintroduced from the vestibulum into the pelvis and the vagina was pulled through. The vaginal septum was resected externally before the anastomosis between vagina and vestibulum was realised. The postoperative course was uneventful, a urethral stenosis was excluded by voiding urethrography. Conclusions: Laparoscopic vaginal pullthrough, for high urogenital sinusmayserveasanalternativeapproachinselectedcases.Inthe presented patient the combination with vaginal duplication did not cause further complications in the course of the patient. The presented approach has never been described before in this malformation.
V013LAPAROSCOPIC REMOVAL OF A GASTRIC TRICHOBEZOAR IN A PEDIATRIC PATIENT, CharlesMLeysMD,JasonDFraserMD,ShawnDSt.PeterMD,TheChildren’sMercyHospital,KansasCity,MOTrichobezoars from the ingestion of hair typically develop into alargesphericalforeignbodywithinthestomach.Duetothefrequently large size, endoscopic removal is usually not feasible beyonddiagnosis.Likewise,thesizeoftenhasforcedsurgeonstoremove these trichobezoars via laparotomy. Laparoscopic removal of gastric trichobezoars has been reported, but the concern with this technique is complete removal of the large bezoar without spillage ofhairsintheperitonealcavitymaybedifficult.Assuch,mostofthereportsarelaparoscopic-assistedbutstillutilizeanextendedincisiontofacilitatedirectremovalfromtheperitonealcavity.Inthisvideo, we demonstrate complete laparoscopic removal of a giant trichobezoar in a 10 year old child without spillage, using piecemeal removal through the umbilical incision without extending the incisions.
V014LAPAROSCOPIC CHOLECYSTECTOMY AND CONCOMITANT SPLENECTOMY - FOUR WORKING PORTS AND A 5 MM BIPOLAR SEALER., MBailezMD,ARuesmannMD,NTamburriMD,DiagnosisandTreatmentArgentineInstitute.BuenosAires.ArgentinaAim: To show how to enhance the use of ports to acomplish 2 different procedures in a single patient.To describe the technical details of the splenectomy completely done with a 5 mm bipolar sealer. Case:9 years old girl refered for an elective splenectomy and cholecystectomy due to hereditary spherocytosis and gallbladder stones. Surgical technique:Weusethestandardsettingforalaparoscopicsplenectomy adding only 1 on the rigth side for the gallbladder fundus:a10mmumbilicalportforthelens,25mmonesinthesupraumbilical mid line and 1 in each side, lateral to the umbilicus. Gallbladderhiliumisexposedbyholdingthefundustowardsthediafragmneedingsomeworkupwiththe30degreeslenstoadaptthedifferentworkangleofthesurgeon´slefthand.Thesurgeon´srigthandlefthandsareplacedinthesupraumbilicalports.Cysticarteryisdissectedandsealedwiththebipolardevice.ARoederknotis placed in the proximal end of the cystic duct while a transient seal is applied to the distal one . CholecystectomyiscompletedwithmonopolarhookusingtheValleylabmodeoftheenergyplatform.Thesurgeonusesthesupraumbilical lower port for his left hand and the left lateral port for his rigth hand to complete the splenectomy .The assistant uses the top supraumbilical one to place the suction probe to elevate thespleen.Disectionandsealingofvesselsusingbothhandsstarts
in the lower pole and continues with the gastric vessels, leaving the splenichiliumforthefinalpart.Surgeonusesonly2instruments,a Maryland type one and the bipolar sealer, in either hand during alltheprocedure.Anaccesoryspleenisresected.Principalsplenicarteries and veins are carfully dissected and separately sealed.The final posterior attachments are freed and the spleen is placed in an endo bag and exteriorized through the umbilicus .
V015LAPAROSCOPIC DISMEMBERED PYELOPLASTY AND REPAIR OF AN INFUNDIBULO-PELVIC STENOSIS IN A HORSESHOE KIDNEY, FlorianObermayrMD,PhilippOSzavayMD,JoergFuchsMD,DepartmentofPediatricSurgery,Children’sHospital,UniversityofTuebingenIntroduction: Laparoscopic dismembered pyeloplasty for ureteropelvicjunction(UPJ)obstructionisconsideredtobearoutineprocedureinmanypediatriccenters.UPJobstructionisknowntobeassociatedwithhorseshoe-kidneyandseveralreportsonsuccessfullaparoscopic repair in such cases exist. Case description: Thecaseofa9montholdgirlwithTurner´ssyndromeisreported.AhorseshoekidneywithgradeIVhydronephrosis on the left side was diagnosed by ultrasound, in theneonatalperiod.MAG3-diureticrenographyanddynamicMRI-nephrography showed a differential renal function of 31% and 69% on the left and right side respectively. No drainage from the left renal pelvis could be demonstrated. Result: LaparoscopyshowedacombinedUPJobstructionandaninfundubulo-pelvicstenosiswithmassivedilatationoftheupperpolecalicesontheleftsideofthehorseshoe-kidney.Laparoscopicdismemberedpyeloplastyandadditionalinfundibulo-pelvicanastomosis was performed. No intraoperative complications occurred. The immediate postoperative course was uneventful. Unobstructeddrainageandanimproveddifferentialrenalfunctionontheleftside(38%)couldbedemonstratedonMAG3diureticrenography6weekspostoperatively. Conclusion:Inconclusion,laparoscopicrepairofcomplexmalformationsoftheupperurinarytractsuchasacombinedUPJobstructionandaninfundubulo-pelvicstenosisinahorseshoe-kidneyis feasible and leads to good functional outcome in selected cases.
V016LAPAROSCOPIC INGUINAL HERNIA INVERSION AND LIGATION IN FEMALE CHILDREN, AaronMLipskarMD,SamuelZSofferMD,RichardDGlickMD,NelsonGRosenMD,StephenEDolginMD,AndrewRHongMD,SchneiderChildren’sHospital,NorthShore-LongIslandJewishHealthSystemInguinalherniorrhaphyisthemostcommonlyperformedoperationin the pediatric population. Traditionally, these operations are performed via a groin incision and a high ligation of the hernia sac. Alaparoscopicapproachtopediatricfemaleinguinalherniashasbeendescribedinvolvingherniainversionandligation.Wepresenta video describing the instrument placement and the detailed steps of this relatively straightforward procedure. The operation is performed with only one trocar, placed at the umbilicus in order to allowfora5mm,30-degreetelescope.Twoadditional3mmincisionsaremadeintheflanksattheleveloftheumbilicus.Thepelvisisfirstinspected carefully in order to delineate the anatomy and define thepathology.Using3mmgraspers,theherniasacisinvertedandthe round ligament is bluntly freed from its attachments to the labia.Theherniasacisthenligatedusing0-PDSpre-tiedloopsandresected.Wehaveperformed135laparoscopicinguinalherniainversion and ligations in female children ranging from 1 month to 18yearsofageinthepast5years.Wehavehadnoperi-operativecomplicationsorconversionstoopen.Wehavehad1recurrenceinour series that occurred in our first case when we did not resect the herniasac.Wesubsequentlyroutinelyresectthesacandconsiderthistobecriticalinpreventingrecurrence.Anadditionalbenefitofthelaparoscopic approach is the ability to diagnose and treat bilateral disease.Webelievethatalaparoscopictechniqueinvolvinginversionand ligation of the hernia sac is safe and effective in the pediatric female population.

50 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Poster AbstractsP001THORACOCSOPIC AND LAPAROSCOPIC PLACEMENT OF A PLEURO-PERITONEAL SHUNT IN A PATIENT WITH CONGENITAL LYMPHEDEMA AND A SYMPTOMATIC PLEURAL EFFUSION, JoanneEBaergMD,HarryOuMD,LomaLindaUniversityChildren’sHospitalINTRODUCTION:Wepresentacaseofendoscopy-guidedplacementofapleuro-peritonealshuntinapatientwithcongenitallymphedema, multiple abdominal lymphoceles, an episode of spontaneous bacterial peritonitis and recurring symptomatic pleural effusions. CASE: Afifteenyearoldboywithcongenitallympedema,hadundergone multiple thoracenteses and chest tubes for a left pleural effusion.Anincisionwasmadeintheposterioraxillarylineatthesixth intercostal space. The pleural portion of the shunt was placed ingoodpositionguidedbythefivemillimeter,thirty-degreecamera.Theshuntandpumpchamberweretunneledundertheskin.A5mmincision was made in the left upper quadrant, a purse string suture was placed in the posterior rectus sheath and the 5mm port was inserted into the abdomen under direct vision. Pneumoperitoneumwasobtainedtoapressureof13mmHgandthecamerawasinserted.Afrozenabdomen,withsignificantadhesions,wasidentified.Withlaparoscopicguidance,anareawasdissectedinwhichtoplacetheshunt.Immediategoodshuntfunction was observed. DISCUSSION: This previously unreported use of endoscopy to successfullyplaceapleuro-peritonealshunt,allowedapatienttobe discharged from hospital free of oxygen and external tubes. Informationwasobtainedaboutthepatient’sabdomenwhichwillguide future therapy.
P002NEPHRECTOMY IN CHILDREN: WHAT’S THE ROLE?, G.Mattioli,S.Costanzo,P.Buffa,G.M.Ghiggeri,V.Jasonni,DeptofSurgery,UrologyandNephrology-G.GasliniInstitute-UniversityofGenova,Italy.Background and aim of the study.Indicationsfornephrectomyin children are not well established and a lot has changed. The aim of our study is to critically analyze the indications and the surgical strategies for children who underwent nephrectomy and to discuss about the role of endoscopic approach. Patients and methods. Dataaboutdemographics,diagnosis,technical details and hystopathological analysis of patients who underwentnephrectomyintheperiod2003-2008werereviewed. Results. Atotalof76patients,42malesand34females,underwenta nephrectomy or heminephrectomy in the period of study. The meanagewas4.12years(11days-23years).70nephrectomiesand6heminephrectomieswereperformed.Endoscopicapproachwascontraindicatedincaseofcancer.Postoperativesurgicalspecimensshowed:23renalhypodisplasias(hydronephrotic/pyelonephritis),22Wilms’tumours,10multicisticdisplastickidneys(nocaseswithneoplasticdegeneration),8neuroblastictumours,7duplexsystems,2 cystic nephromas, 1 high grade malignant lymphoma, 1 congenital mesoblasticnephroma,1renalcarcinoma,1post-traumatickidney.Nomajorsurgical-relatedcomplicationsoccurred. Discussion. The main indication for nephrectomy in children is cancer. Renal hypodisplasia, particularly when symptomatic (abdominalpain,hypertension,UTI),isanotherindication,buttherearenoclearguidelinesinliteratureaboutit.MCDKisnotrecognizedas a real indication for nephrectomy, according to recent studies. More studies are advocated to better define this topic. References. CambioAJ,EvansCP,KurzrockEA.Non-surgicalmanagementofmulticysticdysplastickidney.BJUInt.2008Apr;101(7):804-8
P003THE RESPIRATORY ADVANTAGES OF LAPAROSCOPIC FUNDOPLICATION WITH NEUROLOGICALLY IMPAIRED CHILDREN AND NORMAL CHILDREN, MakotoKomuraMD,TadashiIwanakaMD,yoshihiroKitanoMD,HirooUchidaMD,HiroshiKawashimaMD,TetuyaIshimaru,yujirouTanakaMD,TeturouKodakaMD,MasahikoSugiyamaMD,yutakaKanamoriMD,KaoriSatouMD,MarikoyoshidaMD,DepartmentofPediatricSurgery,GraduateSchoolofMedicine,UniversityofTokyoLaparoscopicfundoplication(LF)isreplacingtheopenapproachinthetreatmentofchildrenwithgastroesphagealreflux.LFhasbecome the standard of care for the management of symptomatic gastroesophagealrefluxdisease(GERD).Thepostoperative
respiratoryadvantagesseemobviousbutunclear.Wehypothesizedthat LF provides postoperative respiratory advantages in neurologically impaired children and normal children. One-hundredtwenty-sevenLFswereperformedbetweenJune1997andOctober2008atSaitamaChildren’sMedicalCenter,Saitama,andUniversityofTokyoHospital,Tokyo,inJapan.ThechartsofallLFsfrom 1997 were reviewed. Median age of the patients was 13 years old.?@Therewere103(81%)neurologicallyimpairedchildrenand24(19%)neurologicallynormalwithGERD.Thesepatientsweretreatedby a LF and followed up for a median of 8.6 years postoperatively. Conversiontoopensurgerywasnecessaryintwopatients,andthesecaseswereexcludedfromthisstudy.Clinicaldataregardingageatsurgery, presence of neurological handicap, period of neurologically impaired condition, swallowing disturbance, feeding style, scoliosis, preoperativetracheostomyand/orlaryngotrachealdiversion,symptomsrelatedtoreflux(digestiveorrespiratory,includingrecurrentlunginfectionsandreactiveairwaydiseases),concomitantsurgical procedures, complications, and results were retrospectively collected.Alsonecessityofpostoperativetracheostomyand/orlaryngotracheal diversion was discussed. LF was safe procedure with acceptable complication indices. Ultimatelycontroloftypicalgastroesophagealrefluxsymptomswasachieved.Overalltherespiratorysymptomswereimprovedinthemajority of patients without swallowing disturbance. LF combined with tracheostomy or laryngotracheal diversion was beneficial for neurologically impaired children with swallowing disturbance.
P004LAPAROSCOPIC APPROACH OF THE INGUINAL HERNIA IN CHILDREN: RESECTION WITHOUT LIGATION, CarlosGarciaHernandezMD,LourdesCarvajalFigueroaMD,JuanCarlosDueñasRamirez,HospitalInfantilPrivadoBackground: The laparoscopic treatment of the inguinal hernias in children has many advantages; however its use has been limited dueahighrecurrencerate.Untilnowalltheproceduresincludethe ligature of the hernia sac, however the physiopathology of the inguinal hernia in children it is just the persistence of the peritoneum vaginal processes and it is not an aponeurotic defect; therefore it can be treated just with the resection of the hernia sac. Material and methods: Byperformingatransperitonealapproachof three ports with 3mm instrumental, the peritoneum vaginal process can be localized. The process on male subjects differs from the process in female subjects, as the process in males consists in a dissection of the spermatic way and it afterwards a total resection isperformed.Inthecaseofthefemalesubjectstheonlyresectionoccurs in the hernia sac, creating a denudated area of peritoneum that unites together after removing the neumoperitoneum. Results: IntheperiodthatgoesfromJanuary2006toSeptember2008, a number of 115 patients were treated, with ages that varied from1monthto14years.Inthisperiodanumberof152resectionsoftheherniasacwereperformed.Afteraperiodof2yearsofobservation just one case of recurrence has occurred. No elements of the spermatic cord were damaged. Conclusion: TheresectionofthesacItisadifferentwaytoresolvethe inguinal hernia in children, without the use of sutures according to the physiopathology of this disease in children. The resection of theherniasacisaneasytechniquethatallowstakingadvantageof the minimal invasion in the treatment of the inguinal hernia on children, with very low rate of recurrence
P005LAPAROSCOPIC INTUSSUSCEPTION REDUCTION: A MULTI CENTRE STUDY, NCFeatherstoneMD,HDixon,JDearden,NRahmanMD,KWChanMD,KHLeeMD,PTamMD,JICurryMD,MHaddadMD,SAClarkeMD,PaediatricSurgery,Chelsea&WestminsterHospital,London;PaediatricSurgery,PrinceofWalesHospital,HongKong;GreatOrmondStreet,LondonBackground: Intussusceptionisacommonpaediatricsurgeryemergency.Severalcentreshavereportedsuccesswiththelaparoscopicapproach.Wepresentthefindingsfromamulticentrestudy. Methods: Aretrospectivecasenotereviewofallintussuceptionspresented to three surgical centres was carried out over a 10 year period. The method of reduction, success rates, recurrence and length of stay were analysed. Results:Of532intussusceptionstherewere112operativereductions.23/31(74%).underwentasuccessfullaparoscopicreduction. Failure was directly related to need for resection. Length ofstaywassignificantlyshorter(P=0.02)forthoseundergoing

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 51
2009 Poster Abstractslaparoscopy(median5days:range3-10)comparedtoopensurgery(median7daysrange5-28). Conclusion: Laparoscopic reduction can be successfully used as the first line treatment for patients who require operative intervention. Itissafeandresultsinasignificantlyshorterhospitalstay.
P006MICROLAPAROSCOPIC INGUINAL HERNIA REPAIR IN CHILDREN AND INFANTS – OUR EXPERIENCES IN 180 CASES, SalmaiTurialMD,RuthFreudenberger,KathrinKrause,BarbaraGoldinger,VeronikaEngel,FelixSchierMD,MedicalUniversityCentre,departmentofpediatricsurgery,Mainz,GermanyPurpose: The aim of this prospective feasibility study was to determine the value and safety of the microlaparoscopy for inguinal herniarepairinchildren.Wealsoreportthepreliminaryresultsofarecently developed 2.4 mm prototype scope, specifically developed for the present study. Methods and Patients: This study included 180 consecutive children (129 boys and 51 girls, ages ranged from one day to 15 (average2.8)years)undergoingmicrolaparoscopy(theexclusiveuse of 2 mm instrument sets and small diameter scopes (1.7 mm to 1.9mmindiameter))foringuinalherniarepair.Alldatarelatedtopatients and procedures were prospectively collected. The technical observations concerning the scopes and light lines were noted in the operating theatre and all procedures were documented by video recording. Results: Atotalof256inguinalherniasacswereclosed(104unilateral, 76 bilateral, 5 recurrences from previous open herniotomy orconventionallaparoscopicherniorrhaphy).Theoperativetimerangedform7to15min.(average11min.)fortheunilateralherniasandfrom12to20min.(average15min)forthebilateralhernias respectively. No complications occurred due to the exclusiveuseof2mminstrumentsandsmalldiameterscopes.Allmicrolaparoscopy procedures were performed successfully. There were no intraoperative or late postoperative complications noted (followup32to3(median13.5)months).Inthefinal44cases,weused a recently developed 2.4 mm prototype scope. The 1.7 to 1.9 mm scopes provide less indirect depth perception. The new 2.4 mm scope provides very good results in all technical parameters, and the image quality is nearly identical to the 5 mm scopes. The reason for the poor light quality of small diameter scopes was not the scope itselfin60%ofthecases,butaninsufficientlightline.Itsseemsthatdefects of old and overused light lines are hardly noticeable with 5 mmscopes,butthattheymakeabigdifferencewhenusingsmalldiameter scopes. Conclusion:Basedonourpreliminaryresults,themicrolaparoscopichernia repair in children is feasible, safe and effective.
P007LAPAROSCOPIC REMOVAL OF INTRAPERITONEAL FOREIGN BODIES, BurakTanderMD,UnalBicakciMD,RizaRizalarMD,EnderAriturkMD,FeritBernayMD,OndokuzMayisUniversity,DepartmentofPediatricSurgery,Samsun,55139TurkeyAim: Wereporttwochildrenwithintraabdominalforeignbodiestreated laparoscopically. Case1: 7 year old boy was admitted with a history of foreign body ingestion.TherepeatedabdominalX-raysshowedtheingestedmetalic jewel persisting at the right lower quadrant. The abdominal CTindicatedtheforeignbodywithintheappendiceallumen.Thepatient underwent a laparoscopic appendicectomy using 5 mm telescope and instruments. The foreign body was found within the appendiceal lumen. Case 2: 2 ½ years old girl was admitted with a history of bilateral pelvic osteotomy by Kirschner wire due to the developmental dysplasiaofthehip.AbdominalX-rayindicatedtherightKirschnerwire was migrated into the peritoneum. The patient underwent a laparoscopic exploration of the peritoneum using 5 mm telescope and instruments. The Kirschner wire was found within the abdomen ontherightsidecoveredbytheomentum.Ithasbeenremovedlaparoscopically and no injury to the abdominal organs was noted. Conclusion: Laparoscopy is an effective and safe method for the diagnosis and treatment of the intraabdominal foreign bodies both ingested and migrated.
P008LAPAROSCOPIC RETRIEVAL OF INTESTINAL FOREIGN BODIES, SuzanneMyoderMD,SaundraMKayMD,StevenSRothenbergMD,RockyMountainHospitalforChildrenBackground/Purpose:Ingestedforeignbodiesareacommonproblem in the pediatric population. Though most pass uneventfully, occasionally a complication, such as obstruction or enteric fistula, may result due to properties of the ingested object. Laparoscopy, oftenincombinationwithfluoroscopy,canbeusedtotreatthose foreign bodies that have failed to pass and their resultant complications. Methods: Aretrospectivereviewwasconductedofallpatientstreated for retained foreign body from February 2007 to February 2008.Patientdata,preoperativeevaluation,operativetechniquesandpost-operativecoursewereanalyzed. Results: There were 4 patients with a mean age of 5.56 years (range9m-17y)andmeanweightof20.7kg.Theretainedintestinalforeign bodies included an endoscopy capsule, magnets, batteries, andascrew.OnepatienthadknownCrohn’sdisease.Twopatientshad witnessed ingestions of foreign bodies. Three of the patients presented with signs and symptoms of at partial bowel obstruction. Allpatientshadpreoperativeimagingthatrevealedtheforeignbody. Flouroscopy was used to help localize the foreign body in 3 out of 4 patients.Onepatientunderwentattemptedcolonoscopicremovaloftheforeignbodypriortoproceedingtolaparoscopy.Onepatientrequired only a simple appendectomy to treat the retained foreign body. Two patients underwent laparoscopic bowel resection and re-anastomosis.Twopatientshadentericfistulasrelatedtomagnetingestion. Mean operative time was 72.5 minutes. There were no conversions in this series. Averagetimetofullfeedswas3.5dayswithonepatientbeingdischarged 6 hours after their procedure. Conclusion: Alaparoscopicapproachtoretainedintestinalforeignbodies is a safe and effective way treat obstructions and fistulas caused by these foreign bodies. Flouroscopy is a helpful adjunct to this approach and though never a substitute for running the bowel, allowsforquickconfirmationandlocalizationoftheproblem.
P009NOVEL TECHNIQUE FOR MANAGEMENT OF ESOPHAGEAL STRICTURES: USE OF UROLOGIC DILATORS, DOUBLE-J STENTS AND A SAFE ANTEROGRADE MITOMYCIN-C DELIVERY SYSTEM, GustavoAVillalonaMD,MohammadSarhanMD,RajinderPGandhiMD,DepartmentofPediatricSurgery,HarlemHospitalCenter,CollegeofPhysiciansandSurgeons,ColumbiaUniversity,NewyorkBackground: Currentmanagementofesophagealstricturesusingmultiple dilations is the standard of care for symptomatic relief and cure.Diversearraysoftechniqueshavebeendevelopedwithsimilarsuccessrates.Inthisstudywesuggesttheuseofurologicdilatorsasa safe, alternative method for management of esophageal strictures. WealsopresentanoveltechniqueforsafeanterogradeMitomycin-Cdelivery. Case Report: Patientwithahistoryofasevere,recurrentesophagealstricturesecondarytotracheo-esophagealfistularepair,treatedusingAmplatzurologicdilatorsanddouble-Jstentasamechanicaltemporizerforanesophagealstrictureatriskforcompletere-stenosis.AnanterogradeMytomicin-Cdeliverysystemwas also employed successfully. Technique description: Undergeneralanesthesiaaflexibleendoscope was passed into the proximal esophagus to visualize thestricture.Aglidewirewaspassedthroughthestrictureanditsplacementwasconfirmedbyfluoroscopy.Theendoscopewasthen removed and a series of urologic dilators sizing from 12Fr to 32Fr,werepassedthroughthestrictureunderfluoroscopicvision.Followingthis,Mitomycin-Csoakedneuro-spongeswerepassedthroughanendo-esophagealtubeutilizinganendoscopicsnareintothe upper esophagus under direct visualization. This tube was then retractedexposingthestricturetoMitomycin-C.Finallyadouble-Jstent was left in place for further dilation sessions and to prevent complete stenosis. Discussion:Urologicdilatorsareanovelandsimpletechniqueforthe treatment of esophageal strictures. This patient has had over 75 dilation procedures using this technique with no complications. Initially,steroidinjectionswereused,howeverMitomycin-Cwasrecentlyintroducedduetoitsknownanti-fibroticproperties.

52 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Poster AbstractsP010THE LAPAROSCOPIC TREATMENT OF HYDATID CYSTS IN CHILDREN, MartinLvanNiekerkMD,HeinevanderWaltMD,UniversityofPretoria,SouthAfricaIntroduction: Hydatid cyst is a parasitic disease caused by the tapewormEchinococcusgranulosisandEchinococcusalveolaris.Inpediatric patients hydatid cysts are mainly found in the lungs and intheliver.Althoughmedicaltherapiesandpercutaneousdrainagehave been suggested for the treatment of these cysts, surgery is still the best therapy. Laparoscopic treatment of hydatid cysts in children remainscontroversial,mainlybecauseofthelackoflargeseriesintheliterature.Wereportonfivepatientswithhydatidcystoftheliver, which we treated laparoscopically. Patients and method: Five children between the ages of 4 and 17 years presented each with a hydatid liver cyst. The size of the cysts rangedfrom4cmto8cm.AllpatientshadchestX-rays,abdominalsonographyandhydatidserologybeforeoperation.Athree-porttechniquewasused.TheareaaroundthecystwaspackedwithH2O2swabs.Thecystwaspuncturedwithathickendoscopicovariancystneedle,andasmuchaspossibleofthecontentwasaspirated.H2O2was injected into the cyst. The dome of the cyst was removed and suction debridement of the cyst was done. The cavity was rinsed with H2O2.Nocomplicationswereobservedduringoraftertheoperationofanyofthepatients.Averageoperationtimewas55minutesandaverage hospital stay two days. Conclusion: Laparoscopy provides an excellent approach in the treatment of hydatid cysts of the liver, and results in excellent cosmesis, short operative time and rapid recovery.
P011THE LAPAROSCOPIC INSERTION OF A BUTTON COLOSTOMY AS A VENTING STOMA ENHANCES THE NUTRITIONAL STATUS OF CHILDREN WITH AFRICAN DEGENERATIVE LEIOMYOPATHY., ColinLazarus,TrollipLeigh,MilindChitnis,MieElsen,ItayiSimango,EasternCapePaediatricSurgicalService,EastLondon,SouthAfrica.BACKGROUND:AfricanDegenerativeLeiomyopathy,anuncommoncondition primarily affecting the colon and rectum of children of Southern,EasternandCentralAfrica,manifestsasgrossgaseousabdominaldistension,aninabilitytoevacuateflatusandfaeces,anorexia and malnutrition with death in adolescence or early adult life.Surgicalinterventionhaspreviouslybeenrecommendedonlyinthe management of complications such as colonic volvulus. PATIENTS AND METHODS:WehaveplacedaMIC-KEyskinleveldevice(button)laparoscopicallyasacolostomyinsixchildrenwiththisdisease.Asize8feedingtubepassedthroughthebuttonisusedmanytimeseachdaytodeflatethecolonortoinstillantegradeenemas to evacuate stool. Qualitativenutritionalscores(appetite,foodintake,pain,nausea,vomitingordiarrhoea)andquantitativemeasurements(tricepsandsubscapularskinfoldthicknessesandmidarmcircumferencemeasurement)determinedatthetimeofthesurgeryhasbeencomparedtothestatus4-18months(mean13.3months)aftertheinsertion of the button. RESULTS: Allpatientshavedemonstratedanimprovementinbothquantitative and qualitative scores. Qualitative scores improved fromameanof12/25toameanof18/25.Increasesinthemidarmcircumferenceandtricepsandsubscapularskinfoldmeasurementswere demonstrated in all patients. CONCLUSION:ThenutritionalstatusofchildrenwithAfricanDegenerativeLeiomyopathyhasbeenimprovedfollowingthelaparoscopic insertion of a button colostomy as a venting stoma. The quality of life of the six patients has enhanced with this intervention.
P012LAPAROSCOPIC CORRECTION FOR HIGH ANORECTAL MALFORMATIONS., MiguelGuelfandMD,Pedro-JoseLopezMD,MarcelaSantosMD,AndreaPobleteMD,HospitalExequielG.Cortes-Santiago-CHILEHighAnorectalmalformationsareknownforthedifficultythathavetoachivethesiteoftherectalfistula(Bladder,Prostaticurethra).Sometimesrequiringasagitalandanabdominalapproachatthesame time. Laparoscopic correction of this type of malformation allows less dissection, mobilization and a fantastic view and control of the fistula. Wepresent3casesofmaleswithhighanorectalmalformations(Rectal-prostaticurethrafistula)thatwerecorrectedwitha3trocarlaparoscopictechnique.Allofthemweremanagedatnewbornwith
a colostomy and correction of the malformation in the first 3 months of life. Two patients were fully corrected laparoscopiclly and one hadasagitalapproachduetotheanatomyofthemalformation.Inthis case the laparoscopic mobilization and dissection of the fistula helpedinthegoodoutcome.Allofthepatientswerecorrectedwithno further problems. Laparoscopic correction of high anorectal malformations is a safe an effective technique, even in patients that needs sagital approach.
P013MODIFIED LAPAROSCOPIC HILL GASTROPEXY A PHYSIOLOGIC ALTERNATIVE TO NISSEN PROCEDURE IN PEDIATRIC AGE, SalvatoreFabioChiarenzaMD,MariaGraziaScarpaMD,LorenzoCostaMD,BarbaraRomanatoMD,LucianoMusiMD,DEPTPEDIATRICSURGERyS.BORTOLOHOSPITALVICENZAITALyINTRODUCTION:theopenHillrepairforgastroesophagealrefluxdisease(GERD)isanestablishedandeffectiveantirefluxproceduresince‘60(Hill,AnnSurg;1967)ingeneralsurgery.ThistechniquewasmodifiedandperformedlaparoscopicallybySnowin1990.Inthis paper we report on our preliminary experience on 24 pediatric patientswhounderwentlaparoscopicHill-Snowrepair. AIMS:theaimsare:1)torestorenormalanatomicalandphysiologicalantirefluxmechanismatthegastro-esophagealjunction;2)nottoalterthenormalcardialanatomy;3)toevaluatethefeasibilityoflaparoscopicHilltechniqueinpediatricage;4)tominimize, especially in neurologically normal patients, sympthoms related to other traditional procedures such as fundoplicatio (Nissen, Toupet,etc). METHODS: we performed modified laparoscopic Hill repair in 24 pediatric patients (5 months to 10 years, average and median 3yrs)requiringantirefluxsurgeryforseveregastroesophagealreflux,associatedwithhiatalhernia.Allpatientsunderwentlaparoscopicprocedurewith:1)freeingoftheabdominalesophagus;2)retroesophagealcruroplasty;3)posterioresophagocardiopexydowntotheoriginofthecrura;4)re-creationoftheangleofHis.Operativetimerangedfrom95to195min.Nomortalityorseriousintraoperative or postoperative complications have occurred. Dischargewasusuallyatthe4thp.o.day.Patientsre-startertoeatsolidsafter2weeks,onlytwopatientscomplainedofamilddysphagia that lasted 15 and 25 days respectively. RESULTS: durationoffollowuprangesfrom1to26months.Allpatients had an gastroesophageal contrast study 6 months after operation, while 4 patients underwent esophagogastroscopy 1 years aftertheprocedure.Onehadrecurrenceofreflux(cerebralpalsy).Atthe moment 2 patients have gastrointestinal symptoms, 3 patients have dysphagia, none of them have gas bloat syndrome or other related symptoms. CONCLUSIONS AND DISCUSSION: authors conclude from these preliminary results that laparoscopic Hill repair, already used in generalsurgeryforgastroesophagealreflux,canbeperformedsafely with excellent functional results in children, since it restores thenormalanatomicalandphysiologicalantirefluxmechanismandespeciallybecauseitminimizestherisksofdysphagiaand/orgasairbloat syndrome or others sympthoms related to other procedures suchasfundoplicatio(Nissen,Toupet,Thaletc).Thetechniqueisstillyoung and the number of operated patients is limited, so its final evaluationisnotpossibleuntillong-termresultsareavailable.
P014AN UNUSUAL CAUSE OF RECURRENT ABDOMINAL PAIN IN A 17 YEAR-OLD GIRL: EXTRALUMINAL LYMPHANGIECTASIA OF THE CECUM MANAGED BY LAPAROSCOPY, ClaudioFDeCarliMD,MarcosBettolliMD,UniversityofOttawa,Children’sHospitalofEasternOntario.DivisionofPaediatricGeneralSurgery,Ottawa.ON.CanadaIntroduction: Recurrentabdominalpain(RAP)isacommonproblemin children. The prevalence in the pediatric population has been reported as high as 34%, with an organic pathology responsible for 45%ofcases.WereportararecauseofRAPina17year-oldgirl. Methods and patient: A17year-oldfemale,withahistoryofRAPduring the last 2 years and acute right lower quadrant abdominal pain during the last 2 days, presented to the emergency department. The patient was stable and had a normal white cell count. Abdominalultrasoundshowedaround,heterogeneousstructurewith hyperechoic and hypoechoic components, increased hyperemia, andasmallamountoffreefluid.Thiswassuggestiveofanearlyperforatedappendicitis.Theovarieswerenormal.Diagnosticlaparoscopywasundertaken.Acystic-likestructurewasfoundsubserosallyontheantimesentericfaceofthececum.Subsequent

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 53
2009 Poster Abstractslaparoscopic dissection revealed a firm, extraluminal cystic lesion. Removalofthecystwasachievedwithoutenteringthececum.Amacroscopically normal appendix was not removed. Histopathology confirmed an encystic extraluminal lymphangiectasia with internal hemorrhage. There were no intraoperative complications and recovery was uneventful. The patient remains free of symptoms at 1-yearfollowup. Conclusion:Toourknowledge,thisisthefirstreportofanextraluminallymphangiectasiaofthececumasacauseofRAP.Laparoscopywasavaluabletoolfordiagnosisandtreatment.Giventhe unusual nature of this finding, the authors felt it reportworthy.
P015HIV AND RECTOVAGINAL FISTULAE IN CHILDREN: AN OMINOUS MARRIAGE, BeelkeD’hondtMD,MartinLVanNiekerkMD,ErnstMullerMD,MarizaDeVilliersMD,DepartmentofPediatricSurgery,UniversityofPretoria,SouthAfricaIntroduction:TheincidenceofHIV/AIDSrelatedsurgicalconditionsinsub-SaharanAfricanchildrenhasbeenrisingoverthelastdecade.The instauration of a successful treatment however has proven to be achallengingtask. Methods and procedures: This retrospective study involves twenty girls aged five months to five years who attended our hospital over a period of four years with a rectovaginal fistula and associated immunedeficiency.NineteengirlswereHIVpositivebyenzyme-linkedimmunosorbentassayandorpolymerasechainreactionandonegirlwasHIVnegativebutsufferedfromanonspecifiedimmunodeficiency disorder. The surgical treatment was modified over time because of primarily poorresults.Initiallyacolostomywasperformedwithoutattendingtothefistula.LateraprimaryresectionoftheRV(rectovaginal)fistula without defunctional colostomy was tried, but with poor outcome.Currentlyadefunctionalcolostomyisperformed.Anti-retroviraltreatment(ART)isthenstartedforaminimumoffourweekspriortoresectionoftheRVfistula.Closureofthecolostomyfollows three to six months later. Results: Twenty immunocompromised girls who presented with associatedRVfistulaweretreatedbytwodifferentsurgeons.Noimmediate mortality was related to the fistula per se but twelve children developed some degree of morbidity, mainly local perineal sepsis due to the existing fistula or fistula recurrence. Recurrence of the fistula occurred in ten girls, with a decreasing incidence when ARTwasstartedbeforeattemptinganyclosureoftheRVfistula.Stomalprolapsewasencounteredintwocases. Conclusion: HIV/AIDSrelatedrectovaginalfistulaeinchildrenaredifficulttotreat.Ourcurrenttreatmentwithdefunctioningcolostomy,followedbyARTforaminimumoffourweeksandsubsequentresectionoftheRVfistulahasproventobesuccessful,although the morbidity related to the underlying condition can be major.Differenttreatmentoptionsshouldbeconsidered,withthemain focus set on improving the recurrence rate after fistula excision.
P015INTRA-ABDOMINAL ABSCESS FORMATION AFTER LAPAROSCOPIC APPENDECTOMY FOR PERFORATED APPENDICITIS., JuanCampsMD,TamsinDurandMD,CayceCohenMD,MyostPhD,PalmettoHealthChildren’sHospital/USC-SOMBackground: Intra-abdominalabscess(IAA)formationisapostoperative occurrence after appendectomy for perforated appendicitis.Itnecessitatesasecondprocedurefordrainplacement.Inpediatrics,thisrequiressedationandincreaseslengthofstay,makingitasignificantlymorbidevent.Thepurposeofthestudyis to identify preoperative predictive values in those patients with postoperativeIAA.PostoperativeIAAformationseemstooccurin
perforated appendicitis regardless of surgical technique; open versus laparoscopic,drainornodrain.TheincidenceofIAAformationinopenappendectomywithintra-operativedrainplacementis12,5%versusnodrainplacementof21,7.Intheopentechnique,IAAratesrangefrom10%to38%,averaging16%.Ourexperiencewiththelaparoscopic technique is consistent with these numbers 16.1%. Methods:Ourstudygroupincluded35childrenundertheageof18years who were treated for perforated appendicitis at our institution betweenMay2003andJune2008.Allchildreninthestudygrouphad their operations performed by the same surgeon using the laparoscopictechniquewithoutadrainplacement.Allwereinitiallytreatedwiththesame2antibiotics;clindamycin(10mg/kg/8hrs)andgentamicin(5mg/kg/24hrs).Aretrospectivechartreviewwasdonetodeterminehowmanypatientsdevelopedintra-abdominalabscess.Anumberofotherpredictivevariableswerereviewedintheinitialassessment:WBC,Bands,daysofsymptoms,CTscanfindings,temperature, diffuse or localize pain, age, and sex. Results: RepeatCTscanrevealedintra-abdominalabscessformationinnineofthechildren(9/35,25.7%).Sixpatients(6/35,17.1%)hada percutaneous drainage tube placed by interventional radiology. No abdominal reoperations were required. The average length of stay was 11.00 days in the group requiring drain placement and 6.90 days in the group without drain placement, which was a statistically significantdifference(p=0.002). Conclusion:IAAformationafterappendectomyforperforatedappendicitisisacommonoccurrence.Afterevaluationofthedata,there were not predictive values that suggested which patient would needadrain.IAAformationisarguablyanaturalprogressionofthisdisease process which cannot be avoided in certain patients.
P016LAPAROSCOPIC RESECTION OF A RECTAL SARCOMA, Lardy M HubertPhD,BenchellalMZine,DommangeMFlorenceMD,BoscqMMoniqueBA,ChapetMSophieMD,MachetMMarieChristineMD,RobertMMichelMD,ChruToursOutcomeofsofttissuesarcomasdependoninitiallocalisationandsurgical resectability. Rectal localisation is very rare and the difficulty lies in proper diagnosis. The treatment demands a multidisciplinary approach. Wereportthecaseofaneuroectodermalsarcomaoftherectumtreated by neoadjuvant chemotherapy then by coloproctectomy followed by adjuvant radiotherapy and chemotherapy. Clinicalhistorybeginsbyredbloodrectalbleedingandconstipation.Examinationandrectaltouchrevealedanendoluminalmassinfiltrating the right lateral wall of the rectum. The coloscopy showed a polypoid, crumbly, bleeding mass and the biopsy a neuroectodermal sarcoma of the rectum confirmed by molecular biology.Extensionbilanwasnegative.ThepatientwastreatedaccordingtotheEUROEWING99protocol.MRIpostchemotherapyassessment showed an important tumor decline of the endoluminal partofthetumorbutnoeffectonthewalloftherectum.After6 courses of chemotherapy, the patient had a laparoscopic coloprotectomy with coloanal anastomosis and a protective temporary ileostomy. Pathologyoftheresectionshowedan11%remainderoftheinitialtumour with healthy safety therapeutic margins. However, the patient received a neoadjuvant chemotherapy and radiotherapy after bilateral laparoscopic ovariopexy. Restoration of the continuity of the gastrointestinal tract followed a surgical intervention 8 months after the first operation. Tumours of the rectum in children are rare and difficult to diagnose. Inourcase,therectaltouchenabledadiagnosiswithcertainty.Treatment of these tumors demands a multidisciplinary approach and the collaboration of adult surgeons who are used to these typeoftumors.Protectiveileostomyisrequiredandenablessimplerestoration of gastrointestinal tract continuity and a better tolerance ofradiotherapy.Withmorethan2yearssincethelastchemotherapy,this patient seems to have a favourable outcome although more than 10 % of the tumour remained after neoadjuvant chemotherapy.
P017HEM-O-LOCK’S USE FOR LAPAROSCOPIC CHOLECYSTECTOMY... BE CAREFUL! A CASE OF BILE LEAKEAGE RESULTING FROM CLIP’S EROSION, HSteyaertMD,FObadiaMD,JSvallaPhD,LenvalFoundationforChildrenbackground :bileleakage(BL)isthemostcommoncomplicationafterlaparoscopiccholecystectomy(LC)(1.4%to4%).Inadultsmortalityrateiaftersuchacomplicationturnsaround3to12%.BLmay be due to several causes.

54 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Poster AbstractsCase report : we describe the case of a 5 years old girl who presentedwithBL9daysafteranuneventfullLCforasymptomaticlithiasis(hypercholesterolemy).Atre-operationwefoundanerosionof the choledocus due to a clip used closing the cystic artery. Running suture of the choledocus and wrapping of the clip in an haemostatic tissue was conducted with success true the same laparoscopic way. Discussion: in adult litterature case reports descirbing complications ofclipsafterLCarenumerous.Maincomplicationisthemigrationof the clip in the choledocus causing a lithiasis; however, acute bileleackageisalsorarelydescribed.MostlyaRoux-yoperationisproposed dealing with such a complication. Conclusion: in children, were fat is mostly not a problem, the use of simple absorbable suturing material will be the best method in order to avoid this potentially serious complication. Roux-yoperationmayprobablybeavoidedifclosureoftheleackisdonemicroscopically(orlaparoscopically).Indeed,stenosismaybeaconcern in such small choledocus
P018LAPAROSCOPIC DUODENODUODENOSTOMY FOR DUODENAL OBSTRUCTION IN NEWBORNS, SuolinLIMD,MengLI,yingchaoLI,DepartmentofPediatricSurgery,2ndHospitalofHebeiMedicalUniversity,Shijiazhuang,050000,China.Objective The aim of this study was to evaluate the feasibility and indication of laparoscopically assisted duodenoduodenostomy for neonates with congenital duodenal obstruction. Methods From May 2004 to Feburary 2008, 6 newborns with duodenalobstructionunderwentexploratorylaparoscopy.Withalower-pressurepneumoperitoneumof5-8mmHgandasuspendingsuture for right liver elevator, the procedure was performed using 3cannulasof3.3mmto5.5mmdiameter.Underthelaparoscopicvision, the cause of duodenal obstruction was diagnosed and a sutured anastomosis was performed after the duodenum mobilized. Results Findings at laparoscopy included duodenal diaphragm in 3 cases, annular pancreas in 2 cases, and preduodenal portal vein in 1 case. Three cases with duodenal diaphragmatic stenosis were encountered a partial excision of the diaphragm after vertical incision of the anterior part of duodenum followed laparoscopicallybyatransversesuture.Adiamond-shapedside-to-side duodenoduodenal anastomosis was successfully carried out in 2 cases of annular pancreas through a laparoscopic approach, but aduodenojejunostomywasconvertedtomini-laparotomyduringthe laparoscopic course of a preduodenal portal vein. The average operativetimewas102¡À16.5min(85¡ª135min).Visualizationwasexcellent, and there were no intraoperative complications. Feedings werestartedonpostoperativeday3to5.Allcaseswereonfullfeedingsafter8to10days.Follow-upuppergastrointestinaltestsshowed no evidence of stricture or obstruction. Conclusions The duodenoduodenostomy with laparoscopy can be performedinneonatessecurelyandappropriatedforafull-termnewbornwithtoleranceCO2pneumoperitoneum.Itprovidesanexcellentandmicro-invasivewaytoevaluateandtreatcongenitalduodenal obstruction.
P019PYLORIC STENOSIS WITH NARROW RING LIKE ORIFICE: DIAGNOSTIC GASTROSCOPY AND LAPAROSCOPIC PYLOROPLASTY, BaranTokarMD,HuseyinIlhanMD,AhmetUnluMD,UmutAliciMD,DilsadDemetMD,EskisehirOsmangaziUniversitySchoolofMedicine,DepartmentofPediatricSurgery,EskisehirTurkeyHypertrophicpyloricstenosisisawellknownentityininfants.Pyloricstenosis without hypertrophic pylorus is an unusual pathology and maycausechronicpartialgastricobstructionfindings.Wepresenta5-year-oldfemalepatientadmittedwithchronicabdominaldistension, halitosis and vomiting with a heavy offensive smell. Radiological investigations and gastroscopy were performed for diagnosis. AbdominalX-rayanduppergastrointestinalsystem(GIS)contraststudy showed a grossly dilated stomach resulting abdominal distension. No contrast passage was observed from stomach toduodenum.Pyloruswasnothypertrophiconultrasoundexamination.Gastroscopywasperformed,andapyloricstenosiswithnarrowringlikeorificeandretainedsolidfoodparticlesinadilatedstomachwereobserved.Gastricantralbiopsiesweretakenandpyloruswascatheterizedtovisualizeradiologicallythedistalcontinuityofthestenoticorifice.Contraststudyshowednopathologyinthedistalpart.Endoscopicdilatationhadbeentriedtwiceinanotherhospitalandwasnotsuccessful.Duringgastroscopic
evaluation,wefoundveryrigidringlikeorifice,anddidnottrydilatation.Sincetherewerechronicpartialobstructionsymptomsformore than 3 years and our findings were significant, we performed laparoscopicHeinecke-Mikuliczpyloroplasty.Thepatientdidwellpostoperatively and she is now 14 months of the follow up. Pyloricstenosiswithouthypertrophycausespartialobstructionsymptomsandsigns.Subtlesymptomsmaynotalertthefamilyintheearlyphase.RadiologicalinvestigationsforupperGISandgastroscopy are crucial for the diagnosis. Laparoscopic pyloroplasty prevents a morbid upper abdominal incision, and provides a better postoperative pain management and early postoperative discharge.
P020LEARNING CURVES IN PEDIATRIC LAPAROSCOPY, HOW MANY IS ENOUGH? THE AMSTERDAM EXPERIENCE IN LAPAROSCOPIC PYLOROMYOTOMY, M.W.N.OomenMD,L.T.HoekstraMD,R.BakxMD,H.A.HeijMD,DepartmentofPaediatricSurgery,EmmaChildren´shospital,AcademicMedicalCentre,Amsterdam,TheNetherlandsObjective: Few(large)studieshavebeenpublishedregardingthesurgical outcomes of open versus laparoscopic pyloromyotomy in the treatment of hypertrophic pyloric stenosis. The question arises which technique is better in terms of postoperative complications. The aim of this study was to compare the postoperative complications ratefollowingopenpyloromyotomy(OP)viaumbilicalincisionwithlaparoscopicpyloromyotomy(LP)forinfantilehypertrophicpyloricstenosis.ThelearningcurveafterintroductionofLPwasanalysedbycomparingthenumberofcomplicationsinthefirsthalfoftheLPprocedureswiththesecondhalfoftheLPprocedures. Method: Aretrospectiveanalysiswasperformedin209patientswithaninfantilehypertrophicpyloricstenosis.Between2002and2008,138infantsunderwentOPcomparedwith71infantswereanLPwasperformed. Results: There was a significant difference in median operating time betweentheOP(33min)andLP(40min)group.MedianhospitalstayaftersurgeryinOPpatientswas3daysandinLPpatients2days(p=0.002).ThepostoperativecomplicationratewasnotsignificantlydifferentbetweentheOPgroup(27.5%)andtheLPgroup(22.5%,p=.434).Inthefirst35LP-procedures,complicationswereseenin31.4% of the patients, while this rate decreased to 14.3% in the second35LP-procedures(p=0.088).AmongthesecomplicationsthereweretwoperforationsandthreeconversionsinthefirstLPgroup,whileinthesecondLPgrouponeperforationwasobserved. Conclusion: There was a decrease in number of complications betweenthefirstgroupoftheLPpatientsandthesecondgroupofLPpatientsindicatingalearningcurveeffect.NotonlythecomplicationratewaslowerinthesecondLPgroup,buttherewas also a decrease in severe complications. This indicates that the learning curve for the laparoscopic pyloromyotomy involves at least 35 procedures. Next to that a significant difference in median operatingtimeandhospitalstaywasseenbetweentheOPandLPpatients. Further research by means of a randomized clinical trial is neededtojustifyLPasthestandardofcare.
P021EARLY EXPERIENCE WITH LAPAROSCOPIC-ASSISTED PULL-THROUGH FOR HIRSCHSPRUNG’S DISEASE, TimJBradnockMD, RaniaKronfliMD,EmmaStormerMD,GregorWalkerMD,GrahamHaddockMD,AtulSabharwalMD,TheRoyalHospitalforSickChildren,GlasgowIntroduction/ AimIn2001ourunitbeganusinglaparoscopyinthemanagementofHirschsprung’sdisease.Theaimofthisstudywastoreviewourexperienceusingthisapproach.MethodsPatientswereidentifiedfromaprospectivetheatredatabaseandcase-notesreviewedretrospectively.Collecteddataincludeddemographics,investigations, operative management and complications. Results 25patients(20male)wereidentifiedwithamedianfollowupof39months(range1-81months).23werebornattermwithamedianbirthweightof3.7kg.Medianageatpresentationwas10days(range1-751days).Most(18/25)presentedintheneonatalperiod.Allpatientsunderwentsuctionrectalbiopsypriortodefinitivesurgeryandmost(23/25)hadacontrastenema.Mediantimefromhistologicaldiagnosistosurgerywas22days(range5-65days).Duringthistime,allpatientsweremanagedasinpatientswithrectalwashouts, avoiding the need for stoma formation. Median weight atsurgerywas4.2kg(range3.1-13Kg)andmedianagewas39days(range12-828days).AllpatientshadaprimarySoave-Boleypull-throughafterlaparoscopicbiopsiesandfrozensectionanalysis.Intheearlypartofthisseries(6patients),laparoscopywasusedfor

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 55
2009 Poster Abstractsintra-operativebiopsiesonlywithpurelyendorectalmobilisation.Subsequently,acombinationoflaparoscopicandendorectalmobilisation was employed. There were 3 conversions to an open procedure-2fordifficultiesinmobilisation,1fordensepelvicadhesions due to recurrent enterocolitis. The intention at surgery was to pull though >5cm of bowel above a ganglionic biopsy but on histologic review the median length of normal bowel excised was3.6cm(range0-10.5cm)and6patientshadabnormalproximalresectionmargins.4patientshadatransitionzonepull-through;3remainwell,1requiredredopull-through.1hadanaganglionicresectionmarginfollowinganerrorinintra-operativefrozensectionanalysis and required further biopsies and ileostomy formation. Thefinalpatienthadfeaturesofintestinal-neuronaldysplasiabutremainswellwithnoconstipation.Therewerenoanastomoticleaks.3patientshadmajorperi-operativecomplications(2urethralinjuriesduring endorectal dissection, 1 colonic trauma during laparoscopic mobilisation).6patientshadstrictures-4anastomotic,2musclecuff.Allweremanagedwithelectivedilatationsonly.Mediantimetodischargewas7days(range3-33days).Medianageatfollowupwas3.1years(range0.1-6.8years).16patientshadastoolfrequencyof<3perday.10patientshavebeenadmittedwithpost-operativeenterocolitis(recurrentin4). Conclusion This retrospective review represents the early part of our experiencewithlaparoscopic-assistedpull-throughforHirschsprung’sdisease.Futureworkwillinvolveaprospectivecohortstudytoassesslong term bowel function in these patients.
P022PERCUTANEOUS ENDOSCOPIC VERSUS OPEN GASTROSTOMY IN CHILDREN: COMPLICATIONS AND OUTCOME, HannuLintulaMD, InkaHämynen,HannuKokkiMD,MattiEskelinenMD,DepartmentofPaediatricSurgery,KuopioUniversityHospital,Kuopio,Finland Background: Percutaneousendoscopicgastrostomy(PEG)isthepreferredrouteforlong-termenteralfeeding.Opengastrostomy(OG)isrecommendedinchildrenwithpreviousintra-abdominalsurgeries.TheaimofourstudywastocompareoutcomesofPEGversusOGinchildren. Methods: The medical records of all children who had either PEGorOGovera18-yearperiod(1990-2008)werereviewed.PEGwasperformedonlyinchildrenwithoutpreviousintra-abdominalsurgeries.AllchildrenintheOGgrouphadpreviouslyundergoneatleastoneintra-abdominaloperation. Results: Fifty-sixchildrenunderwentPEGand13childrenunderwentOG.OnePEGwasconvertedtoOG.ThePEGandOGgroupswerecomparable in terms of age, height, weight, indications for tube placement, and hospital stay. The median procedure time was 20 minutes(range,4to65minutes)inthePEGgroupand35minutes(range,10to50minutes)minutesintheOGgroup(P=0.003).Therewerenoprocedure-relateddeaths.TherewasonemajorperoperativecomplicationinthePEGgrouprelatedtotheblindpuncture of the left liver lobe. The puncture of the liver resulted in asmallhaematomawhichresolvedspontaneously.Twenty-sevenof56children(48%)inthePEGgroupand5of13children(39%)intheOGgroupexperiencedstoma-relatedlateminorcomplications(localizedinfection,peri-gastrostomyleak,granulationtissue)(P=NS).Severegastro-oesophagealrefluxnecessitatingfundoplicationwasdetectedin14children(25%)inthePEGgroupandin7children(54%)intheOGgroup(N=0.042).Fourchildren(8%)inthePEGgroupandonechild(8%)intheOGgrouprequiredlatersurgicalinterventionsrelatedtothegastrostomy(P=NS).Onepatient(2%)inthePEGgroupunderwentgastrostomyrevisionduetomigrationofthegastrostomysitetothecostalmargin.Onepatient(2%)inthePEGgroupdevelopedgastricmucosalprolapserequiringsurgical debridement at the time of conversion to a button. Two patients(4%)inthePEGgrouprequiredsurgeryforclosureofapersistent gastrocutaneous fistulae after discontinuation of their buttongastrostomies.Onechild(8%)intheOGgroupdevelopedagastrostomy site abscess which was treated by surgical drainage. Conclusion:PEGisasafeandeffectivetechniqueforestablishingenteralfeedinginchildrenwithoutpreviousintra-abdominalsurgeries,withoutcomescomparabletothatofOG.
P023LAPAROSCOPIC SPLENECTOMY: THE COMBINED SCOTTISH EXPERIENCE, CharlesKeysMD,BomaAdikibiMD,GordonAMacKinlayMD,FraserDMunroMD,GregorWalkerMD,AtulSabharwalMD,RHSCEdinburgh,RHSCGlasgowLaparoscopicSplenectomy:TheCombinedScottishExperience Introduction: Laparoscopic splenectomy was first carried out in
Edinburghin1998.In2005surgeonsfromthiscentrecollaboratedwithsurgeonsinGlasgowtoestablishlaparoscopyasthetechniqueofchoiceforsplenectomythere.WepresentthecombinedScottishdata. Methods: Retrospective casenote review of all patients including demographics, indications for splenectomy, whether cholecystectomy was also performed, major complications and outcome. Results: Atotalof40patientshaveundergonelaparoscopicsplenectomyinthetwocentres.ThefirstfivecasesinGlasgowwerecarriedoutincollaborationwithsurgeonsfromEdinburgh.Inthefirst4ofthesetheEdinburghsurgeonswerepresentinGlasgowandforthefifththeprocedurewasobservedbyatelemedicinelink-up.Themedianageatsurgerywas12years(range3-18),female:maleratio3:2.Themostcommonindicationwashereditaryspherocytosis(31/40).Laparoscopiccholecystectomywascarriedoutsimultaneouslyin19patients.Conversiontoanopenprocedureoccurredin2cases,bothforbleeding.Complicationsoccurredin2patients;onebileleakwhich required a drain and subsequent stent, and one episode of post operative pancreatitis which was managed conservatively. Conclusion: Laparoscopy is now the standard technique for splenectomyinchildreninScotland.Itisasafeandeffectiveprocedure with acceptable complication rates. Through collaboration of surgeons it is now carried out independently in two centres.
P024THE IDEAL GASTROSTOMY: A PERSONAL ODYSSEY, StevenZRubinBA,LarissaBertokBA,Children’sHospitalofEasternOntarioGastrostomy(G)maybeessentialinmaintainingnutrition.HistoricallyG-tubeinsertionincludedlaparotomy,percutaneousendoscopicgastrostomy(PEG),radiologicallyguidedpigtailinsertion.The incidence of major complication including misplacement into the peritoneal cavity, intestine fistula formation, peristomal infection, has progressively decreased to 5%. The advent of laparoscopy may further reduce complications. This paper reports an experience over the past 28 years with gastrostomies in childhood and the evolution to laparoscopic assisted gastrostomy. Methods: Two hundred children referred for gastrostomy insertion attheAlbertaChildren’sHospitalandtheChildren’sHospitalofEasternOntariowereincluded.Onlymajorcomplicationsarediscussed.G-tubeinsertionaspartofanotherabdominalprocedureis excluded Techniques: OpenG-tubeinvolvedaStammGastrostomy.PEGutilizedaflexiblegastroscopeandaretrogradepercutaneoustechnique.(InsertionofapigtailG-tubewasdonebyradiology.)Inthepast3yearslaparoscopicassistedPEGistheroutine.Laparoscopicpigtailinsertionisanalternative.Atwoporttechniqueisused.Theumbilicalport(Hasson)isplacedforthecamera.Asecondportintheright midabdomen accommodates an atraumatic grasper. Results: Gastrostomy1980-2008 OpenPEGlaparoscopyLaparoscopicassisted Patients601201030 Complications3colonicfistulas4displacementintotract.10Peristomalcellulitis.4openconversions Conclusions: Laparoscopy precise anatomical gastric placement oftheG-tubeavoidsthegastrocolicomentumandthetransversecolon. Technically related placement complications can thus be avoided.Peritonealcontaminationisminimized.InthelargerchildthesurgeoncanchoosebetweenlaparoscopicassistedPEGorpigtailcatheterinsertionInnewbornsandinfantswheregastroscopymayprejudicetheairway,laparoscopic-guidedpigtailgastrostomyisanattractive option..
P025OBLIGATION TO OPEN SURGICAL EXPERIENCE FOR LAPAROSCOPIC SURGERY: AN URBAN LEGEND,HulyaOzkan-UluMD,MineFedakar-SenyucelMD,BilalAlperMD,GulnurGolluMD,BerktugBahadirMD,AydinyagmurluMD,DepartmentofPediatricSurgery,AnkaraUniversitySchoolofMedicineMany, who are in over against laparoscopic surgery, utter the need of open surgical experience is mandatory for laparoscopic surgery. ItwasaimedtoconfutethisargumentatleastforlaparoscopicappendectomywiththedataobtainedfromaUniversityHospital. Allofacuteappendicitiswasmanagedbylaparoscopicappendectomy since 2002. There was no conversion to open during this period, and all of the residents start performing appendectomy via laparoscopy and never performed open appendectomy. Four of the residents completed their training and after having board certification of pediatric surgery, went to different parts of the country for compulsory employment. Laparoscopic surgery facilities,

56 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Poster Abstractsthenumberofappendectomiestheyperformed(lapvsopen),need for assistance, technical difficulties and complication rate was interrogated. The median time spent in compulsory employment was 18 months (6-30months).Justoneofthesurgeonshaslaparoscopicsystemand equipment in her hospital and still performing all of the appendectomies via laparoscopic surgery. Rest of the surgeons, where none of them have had experience in open appendectomy, had no laparoscopic system. The median number of appendectomies performed by these surgeons was 78. Hence, all of these surgeons were the only pediatric surgeons in their hospital; they were performing all of their operations with the scrub nurse, so they had no possibility to obtain surgical assistance and never needed, at least for appendectomies. There were only two minor wound infections observed, during this time period. They announced no technical difficulties for the operation. To conclude, there is no need for open surgical experience to perform laparoscopic surgery in laparoscopic appendectomy r vice versa.Surgicalprinciplesdonotdifferwhetherinlaparoscopicoropen surgery.
P026LAPAROSCOPIC EVALUATION OF CHILAIDITI’S SIGN IN A SEVEN MONTH OLD, HalukBGuvencMD,KemalRasaMD,OktayKaradenizMD,AnadoluMedicalCenter,DepartmentofPediatricSurgery,Kocaeli,TurkeyChilaiditi’ssignisanincidentalradiographicfinding,associatedwithintestinal disposition located between liver and right diaphragm. The prevalence ranges from 0.025% to 0.28%. The differential diagnoses include pneumoperitoneum, subphrenic abscesses, and diaphragmatichernias.Wepresenttheyoungestpatientanddiscussthe aspects of this rare entity. A7-month-oldmalewasadmittedwithanincidentaldiagnosisofrightdiaphragmatichernia.ReevaluationofhisthoraxCT,obtainedat the age of 4 months due to respiratory tract infection revealed Chilaiditi’ssign,whichwasconfirmedbyrepeatroentgenstudy.Onexamination he was free of any signs and symptoms of intestinal obstruction.Parentalconsentwasobtainedtoperformadiagnosticlaparoscopy in order to evaluate the anatomical details and possible treatment.Underlaparoscopicexaminationone-halfthelengthof the transverse colon was found lying anteriorly in the space between the hemidiaphragm and the right lobe of liver without anyanomalousfixation.Themostprominentfindingwasthelackof muscle fibers and almost transparent appearance of the medial aspectoftherighthemidiaphragm.Anysurgicalcorrectionwasregardedasunnecessary.Thepatientisdoingwellandunderfollow-up. Chilaiditi’ssignisconsideredasanacquiredratherthanacongenitalconditionaccordingtothepublishedseries.Ananteriorabdominalwall colopexy is advocated due to the reported rare possibility of colonic volvulus. The presentation of our case may bring new insight into the etiology and treatment of this rare entity.
P027LAPAROSCOPIC SPLENECTOMY. GOLD STANDARD IN THE TREATMENT OF CHILDREN WITH HEMATOLOGICAL DISEASES., RocioBarrazaMD,GilbertoUngsonMD,JuanManuelNoriegaMD,AlejandroRuizMD,MariaDelCarmenGonzalezMD,Children’sHospitalofSonoraStateandInstituteofHealthofSonoraStateBACKGROUND: The objective of this study is to confirm that the laparoscopic splenectomy is the surgical technique gold standard in children with hematological diseases. METHODS: Weretrospectivelyreviewedtheclinicalfilesof8patientsthatweretakentolaparoscopicsplenectomyfromSeptember2005toOctober2008withsurgeryindicationsbyhematological diseases. RESULTS:Weoperated8patientswithagesbetween5to15years.6 women, 2 men. 5 with diagnosis of spherocytosis and three with idiopathic thrombocytopenic purple. Inanypatientwasnecessaryconversionstoopensurgery. The mean operating time was 150 minutes. The weight of spleen was 70 to 550 grams The mean time to resume normal diet were 2 days. To this date all patients are asymptomatic and free of transfusions. Onepatienthasplateletcountof800,000,isundermedicaltreatment with aspirin protect. CONCLUSIONS:Thelaparoscopicsplenectomyisthesurgicaltechnique gold standard in the treatment of children with haematological diseases, because is a surgery with low incidence of
complications, including in patients with to big spleen. Inourstudythehelpfromageneralsurgeon,withgreatexperiencein laparoscopic surgery was fundamental for excellent results in all the patients.
P028LAPAROSCOPIC TREATMENT TO INCARCERATED INGUINAL HERNIA IN CHILDREN., QiuyunMS,LiGuiBinMD,LiLongMD,The5thCentralHospitalofTianJinChinaObjective: To evaluate the value of laparoscopic approach in treating with children suffered from incarcerated inguinal hernia. Method: The patients with incarcerated inguinal hernia received laparoscopicsurgerywereanalyzedretrospectivelybetweenJanuary2004andAugust2008.Theoperationwasgivenafterunsuccessfulmanual reduction or suspected visceral ischemic damage. The hernial content was reduced by external manual pressure and internal pulling by forceps. Hernia was repaired and intestine was observed in laparoscopy to confirm that whether it has necrosis or ischemia. Results:Inall10patientsreductionandrepairweresuccessfulbylaparoscopic treatment. No complication occurred. Conclusions: Laparoscopic treatment for inguinal incarcerated hernia in children has more graces of less trauma, discovering delitescent hernia of opposite side,observing for intestine tube by using laparoscope and few complication.
P029LAPAROSCOPIC-ASSISTED DUODENOJEJUNOSTOMY FOR SMA SYNDROME: REPORT OF TWO CASES, MakotoyagiPhD,HaruhikoImamotoPhD,HidekiyoshidaMD,yukoUdatsuPhD,TakashiNogamiPhD,DivisionofPediatricSurgery,DepartmentofSurgery,KinkiUniversitySchoolofMedicine,Osaka-Sayama,Japan[Background and purposes] Superiormesentericartery(SMA)syndrome is a rare acquired disorder, recognized as weight loss, vomiting, nausea, and postprandial pain, due to compression and partialobstructionofthethirdpartoftheduodenumbytheSMA.Whenconservativetherapyfails,thenlaparotomywithduodeno-jejunostomyorlysisoftheligamentofTreitzisindicated.Inthispaper,wereporttwocaseswhounderwentlaparoscopic-assistedduodenojejunostomy. [Patients and methods] Firstcasewasa20-yearoldadolescent,weighing19kg,withseverelyneurologicalimpairment,complicatedbygastroesophagealrefluxandgastricvolvulus.Secondcasewasanineyearoldboy.A5-cmduodenojejunostomywasperformedbyusinganEndo-GIAthroughasmallincisionattherightupperquadrant in the both cases, after preparing duodenum and jejunum laparoscopically.Inthefirstcase,aNissenfundoplicationandagastropexy were added laparoscopically. [Results] There was no intraoperative complication in both cases..Agastrograffinstudyrevealednoleakwithpatencyoftheduodenojejunal anastomosis. They showed the improvements of the symptoms, postoperatively. [Conclusions] Alaparoscopic-assistedduodenojejunostomyisafeasibleandanalternativeoptionfortreatingSMAsyndromeinthepatients who have a small abdominal cavity.
P030SUBMUCOSAL FIBRIN GLUE INJECTION FOR CLOSURE OF RECURRENT TRACHEOESOPHAGEAL FISTULA,HNevilleMD,yZhugeMD,JFarraBS,WThompsonMD,JSolaMD,UniversityofMiamiPurpose: To report a case of successful endoscopic closure of a recurrenttracheoesophagealfistula(RTEF)utilizingsubmucosalinjection of fibrin glue. Case Report:Tracheoesophagealfistula(TEF)isacommoncongenitalanomaly.OneofthemostseriouscomplicationsaftersurgicalrepairisRTEF,theincidenceofwhichhasbeenreportedfrom5-20%ofpatients.OpensurgicalrepairofRTEFistechnicallychallenging and associated with high levels of morbidity, mortality andrecurrence.Inthiscase,a37weekEGAfemalepresentedatbirthwith respiratory distress and excessive secretions. The patient was diagnosedwithTEFandunderwentprimarysurgicalrepair.OnPOD7, the patient clinically deteriorated, required intubation, and was foundtohaveaRTEFonbariumswallow.WereportthesuccessfulclosureofRTEFinthisinfantutilizinganendoscopicapproachinwhich fibrin glue was injected into the submucosa of the lateral walls of the fistula until the lumen was occluded. The technique offers anewandinnovativeapproachtotheendoscopicclosureofRTEF.Submucosalinjectioneliminatesthepossiblecomplicationofthe

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 57
2009 Poster Abstractsfibringlueplugbecomingdislodgedandaspirated.Ourtechniqueis simpler and safer in that it does not require diathermy or laser coagulationtode-epithelializethetract,andtherebyeliminatesthepotential injury to the esophagus and trachea. The patient has been followed 9 months and is without recurrence. Conclusion: RTEFisaseriouscomplicationafterrepairofTEF.Whenrecognized early, endoscopic closure utilizing submucosal injection of fibrin glue provides a safe alternative to traditional approaches.
P031LAPAROSCOPIC APPENDECTOMY (LA) VERSUS OPEN APPENDECTOMY (OA): A RETROSPECTIVE STUDY IN CHILDREN., AndreaFranchellaMD,PatrizioMondiniMD,CiroAndolfiMD,OperativeUnitofPediatricSurgery,ArcispedaleS.Anna,Ferrara,ItalyOBJECTIVE: tocompareopenappendectomy(OA)withlaparoscopicappendectomy(three-trocarandTULAA)forlengthof hospitalization, length of operation, length of canalization, complications,intra-operativediagnosisofotherpathologies,LAtoOAconversionrate. MATERIALS AND METHODS: the authors retrospectively reviewed aseriesof501appendectomies(124OAand377LA)performedonchildrenandadolescents(medianage11years).Forthepatientsoperatedusinglaparoscopy,athree-trocarprocedurewasemployedin107(21.4%),atwo-trocarprocedurein19(3.8%)andaTULAAprocedurein251(50.1%).Intheopensurgery,aMcBurneyincisionwasemployedin124patients(24.8%).The19“two-trocarprocedure”patientswereexcludedfromthestudy.26patients(6three-trocarand20TULAA)wereconvertedfromLAtoOA.Thestatisticsinclude:onewayanalysisofvariance;Kruskal-Wallisanalysis;Box&Wiskeranalysis;chi-squaretest;linearregressionanalysis. RESULTS: Medianhospitalstaywas2.4daysforTULAA,3daysforthree-trocarLAand3.9daysforOA(p<0.05).Mediandurationofsurgerywas52minutesforTULAA,85minutesforthree-trocarlaparoscopyand72minutesforOA(p<0.05).Medianlengthofcanalizationwas1.1daysforTULAA,1.3daysforthree-trocarLAand1.7daysforOA(p<0.05).Complicationswererecordedin3LAcaseswiththree-trocar(3%),5OAcases(4%)andonly1TULAA(0.4%)(p<0.05).Intra-operativediagnosisofconcomitantpathologies(ovariancysts,endometriosis,patencyofperitoneal-vaginalduct,fallopiantubetorsion)occurredin4OAcases(3.2%),in32TULAAcases(13.9%)andin10three-trocarLAcases(10%)(p<0.05).Theconversionratewas5.6%(6cases)forthree-trocarLAand8%(20cases)forTULAA;theauthorsobservedaconsiderabledecreasein the conversion rate, which declined to 0% overall for 2007. The surgicalskillimprovementispositiverelatedwithreductionoflengthofoperation(p<0.05). CONCLUSIONS: Weconcludethatinclinicalsettingswherelaparoscopic surgical expertise and equipment are available and affordable,LAseemstobeaneffectiveandsafealternativetoOA;moreover,laparoscopictransumbelicalappendectomyinourseriesseemstobeasimpleoption,evenforless-skilledlaparoscopicsurgeons.
P032THORACOSCOPIC REPAIR OF ESOPHAGEAL DUPLICATION – CASE REPORT, PiotrCzaudernaMD,MaciejiMurawskiMD,FromDepartmentofSurgeryandUrologyforChildrenandAdolescents,MedicalUniversityofGdansk,PolandIntroduction: Esophagealduplicationcyst(EDC)isanunusualcongenitalanomaly.Itcomprisesabout0.5to2.5%ofallesophageallesions.Itisusuallydiagnosedininfancyorearlychildhood.EDCisoftenasymptomaticandposesdiagnosticchallenge.Surgicalexcisionis recommended at the time of diagnosis whether or not symptoms arepresent.Wereportacaseof17-year-oldboywithEDCtreatedthoracoscopically. Case report: 17-year-oldboywasadmittedtothepediatricsurgeryunitwithdiagnosisofsolidtumorofposteriormediastinum.Initiallyhepresentedwithdysphagia.Atgastroscopyextrinsiccompressionoftheesophaguswasnoted.PatientunderwentsuccessfulthoracoscopicexcisionofEDC.Thepostoperativecoursewasuneventful and he was discharged after 3 days. Conclusions:Duplicationcystshouldbecompletelyexcisedwheneverpossible,becauseoftheriskofpotentialcomplicationssuch as respiratory distress, bleeding, or infection. Thoracoscopic surgeryiscurrentlytheprocedureofchoice.Itissafeandeffective,although it may be difficult to perform.
P033LAPAROSCOPIC RESECTION OF GIANT OVARIAN CYSTS IN ADOLESCENT GIRLS.,AndrzejGolebiewskiMD,LeszekKomasaraMD,MaciejMurawskiMD,MarekKrolakMD,MariuszSrokaMD,PiotrCzaudernaMD,FromDepartmentofSurgeryandUrologyforChildrenandAdolescents,MedicalUniversityofGdansk,PolandLaparoscopic resection of giant ovarian cysts reaching above the levelofumbilicusisdifficultduetolimitedworkingspaceandriskofcystrupture.In2006-2007threegirls12-yrsofageweretreatedbecauseofgiantovariancysts.InallcasescystshadbenignfeaturesinabdominalCTandhormonalprofile.Mediancystsizewas22cm(+/-5).Attheonsetofoperativeprocedurethecystwaspuncturedpercutaneouslyunderultrasonographic(US)control:3-5litersofserousfluidwasevacuated.Laparoscopiccystresectionfollowedwith its evacuation in a bad through enlarged umbilical incision. Abdominalcavitywasirrigatedwithsaline.Noconversionwasrequired.Nointra-andpostoperativecomplicationsoccurred.Meanoperativetimewas73minutes(+/-15).Hospitalstaywas3days.Microscopic examination showed mature teratoma in 2 cases and mucouscystin1.Follow-upUSexaminationandtumormarkerswere normal. Laparoscopic excision of giant ovarian cysts preceded bytheirpercutaneouspunctureunderUScontrolissafeandeffective providing malignant condition is ruled out by preoperative investigations and cyst spillage is prevented by adequate surgical technique.
P034LAPAROSCOPIC VERSUS OPEN APPENDECTOMY IN CHILDREN WITH PERFORATED APPENDICITIS, TobiasLuithleMD,PhilippSzavayMD,JoergFuchsMD,DepartmentofPediatricSurgery,Children`sHospital,UniversityofTuebingen,GermanyPurpose: Laparoscopic appendectomy in children is well accepted forthetreatmentofnon-complicatedappendicitis.Thetreatmentof complicated appendicitis especially in the case of perforation remains controversial. The aim of the study was to evaluate the role of laparoscopic treatment of perforated appendicitis in comparison with open surgery. Methods: Wereviewedthemedicalrecordsofallchildrenadmittedto our hospital with the diagnosis of perforated appendicitis betweenJuly2002andOctober2008.Demographicdata,whitebloodcell(WBC)count,levelofserumC-reactiveprotein(CRP),length of stay, operative time and complications were analyzed. Results: Among548patientswithappendicitis,82(15%)patientswereoperatedonforperforatedappendicitis.Forty-eightappendectomieswereperformedlaparoscopically(LA),in6patientstheoperationwasconvertedtoopensurgery.Thirty-fourpatientsunderwentopenappendectomy(OA).Therewerenosignificantdifferencesinage,sexratio,WBC,CRP,lengthofhospitalstayoroperativetimebetweenbothgroups(p>0.05).Altogether9complicationsoccurredintheLAgroup(18.8%)and6intheOAgroup(17.6%)withnosignificantdifferencebetweenthesegroups(p>0.05).Intra-abdominalabscesswasthemostcommoncomplication in both groups. Conclusions: Laparoscopic appendectomy is a safe option for the treatmentofperforatedappendicitisinchildren.Inourpatientsnoincreasedriskofpostoperativecomplicationsassuggestedinpreviousstudiescouldbeseen.Wethereforerecommendthelaparoscopic approach to all patients presenting with perforated appendicitis.
P035LAPAROSCOPIC RESECTION OF NEONATAL INTRAABDOMINAL PULMONARY SEQUESTRATION. A TWO CENTER EXPERIENCE, MiguelGuelfandMD,StevenRothenbergMD,PatricioVarela,MabelOrtegaMD,ClinicaLasCondes-SantiagoCHILEPulmonarysequestration(PS)isararelungmalformation(0.15–6.4%ofalllungmalformations).PSsituatedbelowthediaphragmareevenlessfrequent.Wepresent5casesoflaparoscopicresectionofanintraabdominalPSin4neonatesand1infant,allwithpre-natal diagnosis. DirectbloodsupplyfromtheAortaandabnormalvascularizationwere identified in all cases. The patients weight ranged from 3.5 to5kilogramsandoperationtimewas45to75minutes.Inallcasesalaparoscopic3-trocar(3and5mm)techniquewasusedforuncomplicated,completeresectionofthemasses.Patientswereuneventfully discharged within days of minimally invasive surgery. LaparoscopicresectionofPSwassafeandeffective,withunsurpassedexposure of the anatomy of the lesion and vascular supply.

58 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Poster AbstractsP036AN APPROACH TO THE ACQUISITION OF MINIMALLY INVASIVE SURGICAL (MIS) SKILLS FOR PAEDIATRIC PATIENTS IN A THIRD WORLD SETTING., ColinLazarus,MilindChitnis,ItayiSimango,MieElsen,EasternCapePaediatricSurgicalService,EastLondon,SouthAfrica.BACKGROUND.TheEasternCapePaediatricsurgicalservicebasedattheEastLondonHospitalComplexserves3.5millionpeopleofapredominantlyruralandunderresourcedprovinceofSouthAfrica.InestablishingapaediatricMISservice,obstaclestothetrainingofjuniorstaffincluded: 1.Lackofsimple“boxtrainers”ormoresophisticatedvirtualrealitytraining(VRT)devices. 2.LackofacommonlyperformedpaediatricMISproceduresuchasacuteappendicitisinwhichtoacquireinitialMISoperativeexperience (complicated appendicitis being the norm at the time of presentationinthiscommunity). APPROACH. 1.FundingwasobtainedfromtheDepartmentofHealthoftheEasternCapeforthedevelopmentofasurgicalskillslaboratoryattheEastLondonHealthResourceCentre.Componentsofthelaboratoryinclude: a.Alaparoscopicboxtrainerwithamountedjoystick(3-Dmed)usedforthetrainingofintracorporealsuturingandknottying. b.AVRTwithabasicskillsmodule(LapSimSurgicalScience)whichhasthecapacitytomonitortraininginhand-eyeco-ordination,suturing,knottying,clipapplyingandothertasks. c.DevelopmentofapaediatricMIStextbook,journalandDVDlibrary. d.InternetaccesstoWebsurg. 2. The use of laparoscopic inguinal herniotomy, laparoscopic hydrocele repair and the laparoscopic management of impalpable undescendedtestesasinitialproceduresforpaediatricsurgicalMISskillsacquisition. IMPLICATIONS. 1. Trainees are required to have obtained a defined standardontheVRTbeforebeingallowedtooperateonchildren. 2.Skillsacquisitionbytraineestoanacceptablestandardrequiresamajor investment in mentoring time. INITIAL EXPERIENCE. 1.8 students have completed their laboratory training;theiraveragetimetakentoachievetheexamstandardwas11 hours. 2.12 students are currently undergoing training. 3.SkillslearnedappeartobetransferabletotheORwithanimproved learning curve and fewer complications. 4.Studentsenjoytheexperienceofsimulatedtraining.
P037MINIMALLY INVASIVE SURGERY IN PEDIATRIC IMMATURE OVARIAN TERATOMAS, AmosLohMD,yeeLowMD,Chan-HonChuiMD,AnetteSJacobsenMD,KKWomen’sandChildren’sHospitalINTRODUCTION: Theuseofminimallyinvasivesurgery(MIS)for pediatric immature ovarian teratomas can offer benefits in diagnosticapproach,staging,andresection.Whileexcisionaloneis effective treatment, there may be potential for tumor spill and port-siterecurrence.WepresentourexperiencewithuseofMISinthesetumors.WealsousethesecasestoillustrateMIS-relatedconsiderations in the management of immature ovarian teratomas, and highlight treatment options for unexpected malignancies.METHODS: Oftwelvecasesofimmatureovarianteratomasbetween1998and2005,fourhadMISapproachesadoptedintheirmanagement.Onehadgrade3diseasewithperitonealgliomatosis,andtherestweregrade1.Cystectomywasattemptedwhenpreoperativeimagingandtumormarkersshowedlowsuspicionofmalignancy.RESULTS:Priortumorruptureinoneandspillageduringattemptedlaparoscopic cystectomy in two others necessitated conversion. Inthefourthcase,laparoscopiccystectomywasperformedforsuspected contralateral recurrence subsequently. Tumor size ranged from9-15cmindiameter.Atfollow-upofmedian4.8years(range:2.4-8.1),allpatientsarealiveanddiseasefree.Nosignificantcomplications were encountered perioperatively.CONCLUSION:UseofMIS,particularlylaparoscopiccystectomyinimmatureovarianteratomasiscontroversial.ThesecasestakenfromourearlyexperiencewithMISreflectthevalueofpreoperativecaseselection, the technical challenges of laparoscopic cystectomy, and the satisfactory outcome of these lesions despite spillage.
P038LAPAROSCOPIC TREATMENT OF A CASE OF COMPLEX DOUBLE CONGENITAL DIAPHRAGMATIC HERNIA,GiovannaRiccipetitoniMD,ClaudioVellaMD,MassimoGarriboliMD,EnricaCaponcelliMD,GiorgioFavaMD,DepartmentofPediatricSurgery–Children’sHospital–V.Buzzi–Milan–(Italy)Althoughcongenitaldiaphragmaticherniaiswelldetectedintheantenatalperiodsometimesthediagnosisoccurlate.Infact,thereare diaphragmatic defects which remain asymptomatic for years. Wepresentararecaseofcomplexdiaphragmaticdefectsina2yearold boy treated laparoscopically. Case report A2yearsoldchildwasadmittedtoourinstitutionforanemia,failuretothrive,gastro-intestinaldisturbance,abdominalpainandpectus carinatum. The first diagnostic step included a chest X ray thatshowedagastricandboweldisplacementinsidethethorax.AnMRIshowedtwodiaphragmaticdefects:alargeLarreyMorgagniHernia(LMH),whichcontainedthetransversecolon,cecumandpartof the ileum and a posterior paraesophageal defect occupied by the stomach. No respiratory symptoms were observed. Weperformedthesurgerywithalaparoscopicapproach. A10mmtelescopeportwasinsertedbyopenumbilicalapproach.Fouroperatingportswereplaced:twointherightandleftsubcostalposition(3mmand5mmtrocars)andtwointheleftandrightlowerabdomen. The stomach and the part of the herniated bowel were reduced in the abdominal cavity; anteriorly we found a very large defect (LMH)whichwasclosedusingaGore-Texdualmeshprostheticpatch(PP)measuring70mmx80mm.TheGore-Texpatchwasfixedonthe border of the diaphragmatic wall using 5 mm titanium helical fastner. The posterior diaphragmatic defect was treated by direct sutureandanoesophagealnewhiatuswascreated.AconcomitantThal Fundoplicatio was performed to prevent gastroesophageal reflux. 24 hours after surgery a right pneumotorax due to abdominal air migration in the chest required a drain with no sequels; no other surgical complications occurred. Conclusion: Intheliteraturethereareseveralreportsoflaparoscopic treatment of LMH and few experience of mininvasive approach to posterior diaphragmatic hernia. The case of associated defectslikeourpatientseemsexceptionalandwedidn’tfoundany reports of laparoscopic one stage correction. The experience in this case allows us to affirm that also these complex diaphragmatic anomalies may be successfully treated laparoscopically.
P039PARAOVARIAN CYSTS IN CHILDREN, BaranTokarMD,UmutAliciMD,DilsadDemetMD,EskisehirOsmangaziUniversitySchoolofMedicine,DepartmentofPediatricSurgeryEskisehirTurkeyPurpose: Paraovariancyst(POC)developsfromperitonealinclusions,tubeepitheliumorWolfianremnant.POCshouldbeconsideredif,on ultrasound, the ovary could be shown separately, tuba settling on the cyst and a fine thin wall of the cyst with mesenchymal vessels are observed.POCsarerarelyfoundinchildren.Torsionofthecystmayoccur,anditisknownthatlargecystshavetendencytohavetorsion. Methods: WeretrospectivelyreviewedourvideorecordofpatientswhohadbeenoperatedforPOC,ovariancystortorsion(n=24). Results: WefoundacasewithasolitaryPOCandthreecaseswithPOCassociatedwithanovariancyst(n=4).Ofthese4cases,twohadtorsionofPOC,onewithparaovarianmicrocysttorsionandtheotheronewithtorsionoflargePOCjustnearthefallopiantube.Thepatient having microcyst torsion also had an ovarian cyst with 4 cm diameter.Inbothcases,POCswereexcisedlaparoscopically.Inothertwopatients,POCsweremicrocystic,multipleandsilent. Conclusion: Sinceparaovariancystsdonothaveapedicle,andexpand into the broad ligament, torsion is usually not expected. The incidence of torsion was reported between 2.1% to 16%. PreoperativediagnosisisverydifficultforsilentandmicrocysticPOCandalsoPOCthatneedssurgicalinterventionisrareinchildren.Inthisstudy,wewouldliketostatethataphysicianwhooperateschildrenforovarianpathologiesshouldrecognizePOCandhaveahighindexofsuspicionfortorsionofPOC.

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 59
2009 Poster AbstractsP040ASPIRATED OR INGESTED FOREIGN BODIES: CLUES ON X-RAY JUST BEFORE THE ENDOSCOPIC EVALUATION, BaranTokarMD, HuseyinIlhanMD,DilsadDemetMD,UmutAliciMD,TamerKayaMD,EskisehirOsmangaziUniversity,SchoolofMedicine,DepartmentofPediatricSurgeryandRadiology,EskisehirTurkeyBackground:Thereisasignificantriskforforeignbody(FB)aspirationorgastrointestinal(GI)tractingestioninchildrenunder3yearsofage.ComplicationscausedbylodgmentofaspiratedoringestedFBareassociatedwithsignificantmorbidityandmortality.Methods: The medical records 501 children who underwent bronchoscopyforsuspectedFBaspiration(n=292),orendoscopicorsurgicalexplorationofingestedGItractFB(n=209)between1994and2008werereviewed.Results:Themajorityofthepatientswerebetween1and3yearsofage.Plainchestx-raysrevealedradiopaqueFBin15,7%ofallpatientswithFBaspiration.Emphysema,pneumonia and atelectasis were the other significant findings determinedonchestx-ray.PlainX-raysrevealedradiopaqueFBsin87%ofallpatientswithFBingestioninGItract.CoinwasthemostcommonFBdeterminedasanobjectingestedandentrappedinGItract(61,2%).Fluoroscopicexaminationperformedforthedifferentialdiagnosisofnon-radiopaqueFBingestionorinpatients with an underlying disease or esophageal stricture as a complication.Complicationsweredeterminedindelayedcases.Conclusion: Aplainx-rayprovidesanearlydiagnosisandguidancefor the forthcoming investigations and exploration. Regardless ofradiologicalfindings,whenFBaspirationoringestionisthesuspected diagnosis in a patient with a strong history and significant clinical findings, an early endoscopic examination or exploration should be considered. Morbidity and mortality increase with a delayed intervention.
P041FOUR PORT TECHNIQUE FOR BILATERAL TRANSPERITONEAL LAPAROSCOPIC ADRENALECTOMY, TimJBradnockMD,AtulSabharwalMD,GordonMacKinlayMD,TheRoyalHospitalsforSickChildren,GlasgowandEdinburghIntroduction To minimise scarring without compromising exposure and ergonomics, we have modified our approach to bilateral adrenalectomyandreportafourporttechnique.CaseReportA6-yearoldgirlwithCushing’ssyndromewasreferredforbilateraladrenalectomy.Shewaspositionedsupinewithsupportsunderherleftflanktoelevatetheoperativefieldby40degrees.A12mminfraumbilical port with a 5mm downsizer was established using theHassantechnique.Fortheleftadrenalectomy,5mmworkingportswereestablishedinsub-xiphisternalandleftupperquadrant(LUQ)asshown.Afurther5mmportwassitedintherightupperquadrant(RUQ)toenabletheuseofanendopledgettoaidomentalretraction.
Following excision, the adrenal was removed directly via the 12mm portwiththecameraattheRUQport.Paddingundertheleftflankwasthenmovedtotherightsideandthepatientpositioned40 degrees right side up. No further ports or repositioning of the patientwererequiredforrightadrenalectomy.ANathansonliverretractor(N)wasused.Anendopledget,thistimepassedviatheLUQport site, was again used to optimise operative field exposure. The rightadrenalwasremovedasbefore.Operativetimewas4hours.Post-operativelyshemadeagoodrecoveryandwasfitforsurgicaldischarge at 48 hours. Conclusion:Wepresentasimplifiedfourport technique for bilateral adrenalectomy which minimises anterior abdominal wall scarring without compromising operative field exposure.
P042SIMPLE TECHNIQUE FOR UMBILICAL FASCIAL CLOSURE USING A GROOVED DIRECTOR, RichardCarterMD,DavidLanningMD,VirginiaCommonwealthUniversityHealthSystemClosureoftheumbilicalfascialdefectafterlaparoscopicsurgerycan be challenging particularly with an obese child and a when a 10mmtrocarisused.Asimpleandreliabletechniqueisimportanttominimizehernias,bowelinjury,orexcessivetissuedamage.Ouraimistodescribeaquick,simple,anddurabletechniquetoclosethefascia at the umbilical port site. Underdirectvisionastandardgrooveddirectorisplacedthroughthe fascial defect and used to lift and stabilize the fascial edges whileafigureofeightsutureisplacedusing2-0or0absorbable,braidedsuture.Priortotyingthesuture,aneffortismadetoensurethattheunderlyingomentumisclearofthefascialedges.Afterthis technique had been used in over 100 patients without any complication, many of which had small umbilical hernias, it then becameourmethodofchoiceforsmall(<1cm)umbilicalherniarepairs. For this, a vertical incision is made in the middle of the umbilicalskinandtheadherentherniasacisentered.Thefascialdefect is closed with the grooved director as described and the herniasacisleftinplace.Theskinincisionsarereapproximatedwithinterrupted,absorbablemonofilamentsutureswiththeknotsburiedpriortocoveringwithskinglue.Atleast100umbilicalfascialclosuresand 2 dozen small umbilical hernias have been repaired with this technique without any disruptions or recurrences. Wehavefoundtheuseofthegrooveddirectortoaidinumbilicalfascial closure after port placement or small umbilical hernias as a simple, safe, and effective technique particularly in the obese patient.Useofthisinstrumentallowsforclosureoffascialdefectsunder direct vision, without injury to underlying viscera, with accurate and durable apposition of fascial edges.
P043TECHNIQUE FOR LAPAROSCOPIC APPENDECTOMY SPECIMEN RETRIEVAL, RichardCarterMD,DavidLanningMD,VirginiaCommonwealthUniversityHealthSystemBackground:Laparoscopicappendectomyhasbecomeawellaccepted technique and is routinely used for children with early appendicitis.Childrenhavelittlediscomfort,tolerateoralintakequickly,andcanbedischargedhomewithminimaltimeinthehospital. Further refinements of the laparoscopic technique can lead to decreased operative times and tissue defects as well as improved patientoutcomes.Oneoftheadvantagesofusingalaparoscopicapproach is being able to place a gangrenous or perforated appendix into an endocatch bag prior to its removal. However, there are very few recommendations in the literature for removing the appendix from the peritoneal cavity. Most surgeons try to pull the endocatch bag through the umbilical defect, which traps the appendix at the bottom of the bag. Retrieval often requires opening orstretchingthefasciaandtheskin.Thereisriskofrupturingthebag and appendix which may contaminate the wound or peritoneal cavity.Wedescribeourtechniqueforretrievaloftheappendixfollowing laparoscopic appendectomy that allows for a relatively uncomplicated specimen extraction. Methods: OncethemesoappendixhasbeencauterizedwiththeMaryland forceps and divided, 2 endoloops are placed at the base oftheappendix.Athirdendoloopisplaceddistaltothefirst2endoloops with enough space to allow for the appendix to be transected with endoshears. The third endoloop is then cut at least 6cmawayfromtheknotthusleavingalongtail.Anendocatchbagis inserted into the peritoneal cavity through a 10mm dilating trocar and opened completely with an instrument. The appendix is placed in the bag with the cut end just inside the bag and the long tail of thethirdendoloopexitingthebag.Oncethebagisclosed,theendisbrought into the tip of the trocar and the trocar removed to expose the top of the bag through the fascial defect. The endoloop tail is grasped and pulled along with the bag, allowing the appendix to be deliveredthroughthefascialdefectinalinearfashion.Ifnecessary,the appendix and bag can be grasped together with a large clamp and delivered. Conclusions: Webelievethatthistechniqueallowsfordeliveryofthe appendix through the fascial defect in a linear fashion instead ofbeingbunchedupatthebottomofanendocatchbag.Evenwhen using a 10mm trocar that dilates instead of cuts the fascia, largeappendices(13to14mmindiameter)canbesafelyandquicklyextractedwithouthavingtofurtheropentheskinorfascia.

60 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Poster AbstractsP044CASE REPORT: SUBCUTANEOUS ENDOSCOPICALLY ASSISTED LIGATION (SEAL) OF RECURRENT SLIDING INGUINAL HERNIA IN A PEDIATRIC PATIENT WITH MARFAN’s SYNDROME., JustinDManleyMD,RupaSeetharamaiahMD,ChristopherJBlewettMD,DavidESawayaMD,UniversityofMississippiMedicalCenterObjectives:AliteraturereviewofsubcutaneousendoscopicallyassistedligationherniorrhaphyandcasereportofitsuseinMarfan’spatient with recurrent inguinal hernia. Case Presentation: 21 month old male had open bilateral inguinal herniarepairbyhighligationat6weeksofage.Subsequently,thepatientwasdiagnosedwithMarfan’sandsufferedarecurrenceoftherightinguinalhernia.Onphysicalexaminationtheherniawaseasily reducible. The technique of subcutaneous endoscopically assistedligationoftheinternalringwaschosenforrepair.Wefeltthat this technique would be the most technically feasible given previousrepair.Diagnosticlaparoscopywasperformedwitha5mmcameraintheumbilicalport.Aslidingherniawithappendixinthecanal was noted. This was reduced with a grasper placed in a 3mm portintheLLQ.Theinternalringwasencircledwithnon-absorbablesuture avoiding the vas and vessels. No complications occurred duringsurgery.Follow-upshowednorecurrence. Conclusions: SubcutaneousEndoscopicallyAssistedLigation(SEAL)closure of recurrent sliding inguinal hernia in children appears to be safe and effective. Laparoscopic inguinal hernia repair has several advantages over open inguinal herniorrhaphy. These advantages includeevaluationofthecontralateralinguinalcanal,decreasedriskof injury to the cord structures, identification of rare hernia types, diagnosticandtherapeuticforrecurrentherniasanddecreasedORtime.
P045SURGERY THROUGH NATURAL ORIFICES, PASTORESCARCEGA-FUJIGAKIMD,GUILLERMOHERNANDEZ-PEREDO-REZKMD,ULISESLEAL-QUIROGAMD,SANTIAGOHERNANDEZ-GOMEZMD,ROCIOBARRAZA-LEONMD,ABIMAELBAÑUELOS-MONTANOMD,ALEJANDRODELANGEL-AGUILARMD,CEMEV,“DR.RAFAELLUCIO”XALAPA,VER.MEXICO.INTRODUCTION: The fenestrated duodenal membrane has a prevalenceof1:10,000to1:40,000births;symptomscouldbepresent or not since birth. The surgery technique mostly used is theduodenoctomy,resectionofthemembranethroughMickulicsclosure. The purpose for this presentation is to show three cases of patientswithduodenalmembraneresolvedbyendoscopy:twoofthem with previous surgeries. CASE 1. Male patient 47 years old started with persistent vomits since birth .The first surgery procedure reported duodenal bridle whichwasresected,havingatorpidevolution.Asecondsurgeryisdone in which intraluminal occlusion is found in the third portion of the duodenum and a laterolateral duodenoyeyunanastomosis isdone.Thepatientcontinuedwithvomits.TheUpperGIseriesshowedocclusionatduodenallevel.TheupperGIendoscopyshowed obstruction of 80% of the anastomoses and a prevaterian fenestrated duodenal membrane. The membrane was resected and fulgurated.Surgerytimewas90minutes.Oralingestionwasstartednext day with a satisfactory evolution; the follow up at two year with UPPERGIendoscopyshowedapropercontrastbariumpassage. CASE 2. Male patient 5 days old with vomits, was diagnosed as having duodenal atresia, and a Kimura duodenumduodenum anastomoseswasdone.Thepatientcontinuedvomiting,anUpperGIseries and endoscopy were done finding an obstruction in the second portion of the duodenum as a result of a non fenestrated duodenal membrane.Asecondlaparotomywascarriedoutandalongitudinalincision in the membrane was done. thirty day after surgery started vomiting.Endoscopywaspracticedfindingaduodenalmembranewith a central orifice and electro fulguration was done .The next day oral ingestion was initiated without problems. Follow up upper endoscopy at two year and ten months was normal. CASE 3. Male patient 2 years and 2 months old vomiting since birth.UpperGIseriesdone;thefindingsweregastromegalyandanimportant dilation of the first and second portion of the duodenum. AnupperGIendoscopywascarriedoutfindingaduodenalfenestrated membrane which could be incised and was fulgurated with a papilotome; the surgery time was of 100 minutes. Follow up atoneyearwithupperGIcontrastbariumshowedasatisfactorypassing.
CONCLUSION. WehavetheconsiderationthatwhenfenestratedduodenalmembraneissuspectedupperGIendoscopymustbedone for being less invasive helping in the diagnosis and treatment ; besides being a secure and effective procedure , reducing surgery time and days of hospitalization
P046ROBOTIC NISSEN FUNDOPLICATION WITH GASTROSTOMY PRESERVATION IN NEUROLOGICALLY IMPAIRED CHILDREN, FranklinCMargaronMD,ClaudioOiticicaMD,JuanVillalonaMD,DavidLanningMD,VirginiaCommonwealthUniversityRobotic fundoplication has equivalent safety profiles, hospital stay, and time to alimentation compared to laparoscopic fundoplication but is not indicated for routine repair due to higher cost, decreased availability, and longer procedure time. Robotic surgery does offer keyadvantagesoverstandardlaparoscopybyemployinginternallyarticulatingarms,astablecameraplatform,and3Dimaging.Childrenpresentingforinitialorredofundoplicationafterfeedinggastrostomy are a subset of patients that may benefit from the robotic approach. Minimal dissection of the phrenoesophageal ligament in combination with four anchoring sutures from the esophagus to the crura has been shown to lead to less wrap herniation in children. This technique is particularly difficult in standard laparoscopy without dislodgement of the gastrostomy, particularly if there are abundant adhesions or an accessory left hepaticarterytopreserve.Wepresent15childrenwithneurologicimpairment and previous gastrostomy who underwent Nissen fundoplicationusingthedaVincisurgicalrobot.Agesrangedfrom1to16yearsold(avg8years)andoperativetimesrangedfrom2hours39minutesto7hours50minutes(avg4hours23minutes).AllpatientsunderwentafloppyNissenfundoplicationaftercruralclosureandplacementof4anchoringstitchestothecrura.Sixpatients(40%)hadredoNissensand5(33.3%)hadreplacedlefthepaticarteries.Sixpatientsunderwentrepairofahiatalherniaandtwo had biologic mesh placed. Four children underwent extensive lysisofadhesions(>1hr).Therewerenoconversionstoopenorintraoperativecomplications.OnechildhadlaparoscopicrevisionofthegastrostomysitebecausethepriorPEGhadbeenplacedthroughthetransversemesocolon.Post-operativecomplicationsincluded one child with a small pneumothorax, which resolved onoxygen,onechildwithpost-opileusrequiringTPN,onechildwith respiratory compromise requiring oxygen support overnight, and one child with post op bleeding requiring transfusion but no reoperation.Allchildrenweredoingwellatlatestfollowup.ThedaVincisurgicalrobotcanbeusedtosafelyperformfundoplicationsinpatients with gastrostomy tubes. The articulating instruments allow fortheplacementof4cruraltackingsutureswhilepreservingthegastrostomy even in the presence of a replaced left hepatic artery.
P047TOTAL COLECTOMY WITH J POUCH USING LIGASURE ADVANCE.(VIDEO), MariaMBailezMD,CarlosMD,GarrahanChildren´sHospital.BuenosAires.ArgentinaLaparoscopictotalcolectomyandconcomitantJpouchisatimeconsuming procedure even after the learning curve period. Strategiestoshortenoperativetimeincludetheuseofhemostaticdevices to divide the mesentery and incise peritoneal attachments . Ligasureadvanceisa5mminstrumentthatincludesatotallyhand-activated monopolar cautery tip in a bipolar sealer with dissection andcuttingcapabilities.ItcanonlybeusedwiththenewgeneratorplatformthatprovidestheValleylabmodeformonopolarcauteryandafasterbipolarsealing(Forcetriad) The aim of this video is to show the advantage of its use for this procedure . A9yearsoldpatientwithanadenomatouspoliposisunderwentatotalproctocolectomyandaJpouch.Fourportswereusedavoidingavoiding changing instruments as much as possible . The surgeon started mobilization of the sigmoid , standing on the right side using a Maryland dissector in her left hand and the hemostatic device in her right one . The assistant standing on the left side ,used a grasper for traction of the colon. They shifted position while the dissection wascarriedfromdistaltoproximalcolon.Alinearstaplerwasusedattherectosigmoidjunctiontofacilitateproximalcolectomy.Afterexteriorization of the complete devascularized colon through the rightlowerquadrantportandcreationoftheextracorporealJpouch , proctectomy was completed everting the rectum through theanus.Ileoanalanastomosiswasperformedbymeansofacircular

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 61
2009 Poster Abstractsendostapplerunderlaparoscopicvision.Anileostomywasleft.Theadvantagesobservedwiththeinstrumentsshowninthevideowere:thepossibilityofincisingtheperitonealreflectionsharply(bymeansofthemonopolarcauterytip),bluntdissection,safesealingandcutting with the same instrument completely hand activated with lessfog–smokeeffect.
P048HEAD-MOTION-CONTROLLED VIDEO GOGGLES: PRELIMINARY CONCEPT FOR AN INTERACTIVE LAPAROSCOPIC IMAGE DISPLAY (I-LID),SaraGlick,KennethSilverman,HarveyFSilvermanPhD,JermeyTAidlenMD, FrancoisILuksMD,BrownUniversityandAlpertMedicalSchoolofBrownUniversityBACKGROUND:Light-weight,low-profileandhigh-resolutionhead-mounteddisplays(HMD)nowallowpersonalizedviewingofalaparoscopic image. The advantages include unobstructed viewing regardless of position at the operating table and the possibility to customizetheimage(enhancedreality,picture-in-picture,etc.).Thebright image display allows use in daylight surroundings and the low profileoftheHMDprovidesadequateperipheralvision.Theoreticaldisadvantages include reliance for all on the same image capture andanti-cues(realitydisconnect)whentheprojectedimageremainsstatic despite changes in head position. This can lead to discomfort and even nausea. METHODS: Wehavedevelopedaprototypeofinteractivelaparoscopicimagedisplay(i-LID)thatallowshands-freecontrolof the displayed image by changes in spatial orientation of the operator’shead.TheprototypeconsistsofaHMD,aspatialorientationdeviceandcomputersoftwaretoenablehands-freepanningandzoomingofavideo-endoscopicimagedisplay.The spatial orientation device uses magnetic fields created by a transmitter and receiver, each containing 3 orthogonal coils. The transmittercoilsareefficientlydriven,usingUSBpoweronly,byanewly-developedcircuit,eachatauniquefrequency.TheHMD-mountedreceiversystemlinkstoacommerciallyavailablePC-interfacePCI-bussoundcard(M-AudiocardDelta44).Analogsignalsat the receiver are filtered, amplified and converted to digital signals, which are processed to control image display. RESULTS:Theprototypeusesaproprietarystaticfish-eyelensandsoftwarefordistortion-freereconstitutionofanyportionofthecapturedimage.Left-rightandup-downmotionsofthehead(andHMD)producereal-timepanningofthedisplayedimage.Motionoftheheadtoward,orawayfrom,thetransmittercausesreal-timezoominginor-out,respectively,ofthedisplayedimage. CONCLUSION: Thisprototypeofinteractivehead-mounteddisplayallowshands-free,intuitivecontrolofthelaparoscopicfield,independent of the captured image.
P049SINGLE PORT THORACOSCOPIC APICAL WEDGE RESECTION FOR SPONTANEOUS PNEUMOTHORAX: A PROMISING NEW TECHNIQUE IN THE PEDIATRIC POPULATION, TimothyJFairbanksMD,KeithAThatchMD,MatthewLMorontMD,L.GrierArthurMD,ShaheenJTimmapuriMD,RajeevPrasadMD,St.Christopher’sHospitalforChildren,DrexelUniversityCollegeofMedicineOBJECTIVE: Primaryspontaneouspneumothoraxisaconditionthat often presents in otherwise healthy children and adolescents. Patientswhohavearecurrence,persistentpneumothoraxorairleak,bilateraldisease,and/orlargebullaecanbeconsideredfora minimally invasive thoracoscopic intervention. The advantages of thoracoscopy over open thoracotomy include decreased postoperative pain, improved respiratory function, and better cosmesis.Disadvantagesincludeportsitecomplicationssuchaschestwall paresthesias and chronic pain. Three port thoracoscopy with apical wedge resection is the most commonly utilized technique. Recently, single port surgery for other conditions has gained popularity because of the potential for less postoperative pain, a decreasedriskofportsitecomplications,andevenbettercosmesis.Wepresentacaseofasingleportthoracoscopicapicalwedgeresection with mechanical pleurodesis and partial pleurectomy for the treatment of a spontaneous pneumothorax in a pediatric patient. METHODS:A17yearoldmaledevelopedaright-sidedspontaneouspneumothorax, which was initially treated with a chest tube. Subsequently,anairleakpersistedandthepneumothoraxrecurredduringthesamehospitalization.ACTscanrevealednumerousapicalblebs.Thepatientwastakentotheoperatingroomwherethe chest tube insertion site alone was utilized to pass a 5mm 30º thoracoscope, a 3mm grasper, and an articulating endoscopic stapler. The apical wedge resection, partial pleurectomy, and pleural abrasion
were performed without difficulty. Two chest tubes were left in place through the 3.5cm incision. RESULTS: The procedure was uncomplicated and technically easy becauseofthein-linepositionofthethoracoscope,grasper,andstapler.Postoperatively,thepatient’sminimalairleakresolvedandthechesttubeswerethenpromptlyremoved.Attwomonthfollow-up, there has been no recurrence, and the patient has no persistent pain or paresthesia. CONCLUSIONS/FUTURE DIRECTIONS: Webelievethatsingleportthoracoscopy is safe and ergonomically efficient for the surgical management of primary spontaneous pneumothorax in the pediatric population. Further experience and prospective randomized trials are necessary to evaluate this technique.
P050MULTIPLE USES OF NATHANSON RETRACTOR, ANajmaldin,EAmeh,LeedsTeachingHospitals,Leeds,UKAims: To highlight multiple uses of Nathanson liver retractor initially introduced for liver retraction during laparoscopic fundoplication. Methods and Results: Nathanson liver retractor is a useful tool in laparoscopicpaediatricsurgery.Itsmainusehasbeentoretracttheliver during laparoscopic fundoplication. Inourinstitution,wehaveusedthisinstrumentsafelyforanumberofotherprocedureswithverygoodeffect.Wehavefounditto be useful in laparoscopic cholecystectomy, choledochal cyst, retroperitonealandtransperitonealrenalandadrenalsurgery.Wehave also used it to retract the lung during thoracoscopic procedures andintestineandpelvicorgansduringotherintra-abdominalprocedures. To date we have had no specific complications. Conclusions: Nathanson retractor has multiple uses in paediatric endoscopicsurgery.Itissafe,easytouseandcosteffective.
P051ROBOTIC HELLER’s CARDIOMYOTOMY AND THE USE OF A BIPOLAR DEVICE, ANajmaldin,NAlizai,LeedsTeachingsHospitals,Leeds,UKAims: AgrowingnumberofpaediatricsurgeonsrecogniselaparoscopyastheidealmethodforHeller’scardiomyotomy.However,thetechniqueisnotwithoutlimitationswhichinclude:difficult instrumentation within the posterior mediastinum and the riskofmucosalperforationwhichcanbeashighas10%.WereporttheadvantagesoftheDaVinciroboticsystemtotreatachalasiausing a bipolar forceps. Methods: Two consecutive children who suffered classical features ofachalasiaweretreatedsurgicallyusingtheDaVinciroboticsystemand a bipolar device. The patients were 11 and 13 years old and were both males. Three robotic and one conventional laparoscopic ports and a retractor were used in each case. Results: Bothprocedureswerecompletedsuccessfully.The3dimensional steady operative view and articulated instruments were a clear advantage high up in the mediastinum. The robotic bipolar forceps allowed for easy and safe manipulation and myotomy. The totaloperatingtimeincludingthesetupandanti-refluxprocedureswas205minutes.Therewerenointra-operativeorearlypost-operativecomplications.Thepatientswereallowedtodrinkat24hours,fedat72hoursanddischargedon3rdand4thpost-operativedays. Conclusions: The articulated instruments allow for easy and simultaneous retraction and dissection within the confined mediastinal space. The bipolar diathermy forceps allows for easy, precise and safe myotomy
P052PREOPERATIVE SPLEEN EMBOLISATION MAKES LAPAROSCOPIC SPLENECTOMY A SAFER PROCEDURE IN CHILDREN, E.VanDerVekenMD,M.LaureysMD,L.DivanoMD,C.LerminiauxMD,A.FersterMD,C.DevalckMD,M.DassonvilleMD,HôpitaldesEnfantsReineFabiola,ULB-VUB,Brussels,Belgium;HôpitalBrugmann,ULB-VUB,Brussels,Belgium1/Objective : some series mention up to 68% intraoperative transfusions and important conversion rates due to hemorrhagic complicationsduringlaparoscopicsplenectomy.Wethereforeeleborated a well defined protocol, associating interventional radiology and laparoscopic surgery. 2/Descriptionofprotocol: First step : under general anesthesia an experienced radiolgist performsaspleenembolisation:byaSeldingertechniquea2.7French microcatheter is brought into the splenic artery. Through this

62 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Poster Abstractscatheter and after dilution in iodinated contrast medium 150 to 250 micronscalibratedpoly-vinyl-alcoholmicroparticlesareinjectedinthe distal portions of the two major division branches of the splenic artery, until visual stagnation is obtained. Then several platinum coils (3to6mmdiameter)areimplantedintheproximalsplenicarteryuntill a complete stop of the injected contrast is observed at the level of the proximal splenic artery. Second step : with the child still under general anesthesia immediate laparoscopic splenectomy is performed using 3 or 4 single ports.Aftercompletedissectionthespleenisplacedinanendobag,fractionned and removed through a slightly enlarged umbilcal incision. 3/Preliminary Results : Betweenjanuariandoctober2008weperformedlaparoscopicsplenectomyin3childrenwithhypersplenismduetosicklecellanemia(1)orspherocytosis(2).Agevariedfrom3to6years,weightsfrom13to19kg.Indicationforsplenectomywasmadeaccordingto clinical and biological data and after multidisciplinary consensus. Oneofthechildrensufferingfromspherocytosisalsopresentedgallstones and the gallbladder was removed during the same operation. Weappliedtheprotocolasdescribedinthe3patients.Inallcasesthe spleen was completely necrosed at laparoscopy and dissection and manipulation of the spleen were faster and safer, causing no bleedingatall.Operatingtimeswere: 95 minutes, 125 minutes and 180 minutes for the combined procedure(splenectomyandcholecyctectomy).Bloodlosseswerebetween5and20ml.Onepatientshowedaslightelevationofpancreatic enzymes with normalisation within 5 days.There were no other postoperative complications. 4/ Conclusion : preoperative spleen embolisation followed by immediate laparoscopic splenectomy seems to be a safe procedure and facilitated laparoscopic splenectomy in these 3 patients. Further dataonalargerseriesareneededtomakesingificantconclusions.
P053LAPAROSCOPIC PYLOROMYOTOMY TRAINING USING HAPTIC FEEDBACK IN A VIRTUAL SIMULATION MODEL, ShabnamParkarMD,DeanMohamedallyPhD,MuntherHaddadMD,Chelsea&WestminsterHospital,London,UKIntroduction: Existingsolutionsfortraininginlaparoscopyarelimited due to the capabilities and accuracy of current training tools,themaindisadvantagebeingthelackoftangiblefeedback.Currently,traininginlaparoscopyforsurgicaltraineesoccursinvitro using rigid instruments. These cannot accurately simulate the detailedsurgicaltechniquesneededinactualoperations.Secondly,current laparoscopic training does not incorporate measured improvements in technique. Objective: Topresentapracticalapplicationofthetrainee’sresponse time, accuracy and technique to the benefit of peer review using a haptic laparoscopic pyloromyotomy model. Facilitating the advancement of haptic simulacra training in this field, we present a solution that combines experienced surgical recordings augmented with clinically relevant temporal haptic data. Method:Ourempiricaldesigninvolves45participantsseparatedinto novices, junior trainees and experienced surgeons via a questionnaireassessment.Usingthelaparoscopicpyloromyotomymodel, they will use two specially designed haptic instruments andviewtheirapplicationin3Dformat.Theinitialphaseinvolvesteaching the technical aspects of the operation via a simulated demonstration conducted by a consultant. This serves as the benchmarkforthetrainee’sapproach.Theywillthenundergoaseries of simulations themselves that serve to advance their technical prowess.Afterassessingtheresultsof15simulatedrunsweshallprovideanempiricalanalysisofthetrainee’scapabilitiesovertime. Conclusion: This prototype provides a unique and innovative basis for teaching laparoscopy to surgical trainees in an anatomically realistic model with the advantage of tangible haptic control and feedback.
P05414 GAUGE ANGIOCATHETER: THE ASSIST PORT, JimMHotalingMD,StephanyaShearMD,ThomasSLendvayMD,SeattleChildren’sHospital,SeattleWAIntroduction: Minimally invasive techniques have emerged as standardofcareforsomepediatricreconstructiveurology.InanefforttominimizerequiredportsforRobotic-AssistedLaparoscopic(RAL)surgeriesinchildren,wedescribeanoveltechniqueforRAL
pyeloplastiesandorchiopexiesusinga14gauge(G)angiocatheterasanassistportinconcertwithvariousreadily-availablecystoscopicequipment. Methods:Afterinsertionof3roboticportsanddockingthedaVinci®SurgicalSystem(IntuitiveSurgical,Sunnyvale,CA,USA)a14Gangiocatheterwasplacedthroughtheabdominalwallunderdirectvision.The14Gangiocatheterwasthanusedtofacilitatestentplacement,provideaportforsemi-flexiblecystoscopicgraspersandtoevacuatecauterysmoke.Closureoftherenalpelvisduringpyeloplastieswasfacilitatedbyusinga14GangiocatheterforantegradeJJureteralstentplacementbySeldingertechnique.A14GangiocatheterwasalsousedforsmokeevacuationbyperiodicallyventingaLuer-lockcappedangiocatheterplacedthroughtheanteriorabdominalwall.Inaddition,wehaveusedstandard3Frsemi-flexiblecystoscopicgrapsersplacedthroughtheangiocatheterfor tissue and suture tail retraction as well as used the graspers forpointingoutanatomiclandmarksduringresidenttraining.Attheendofeachcase,the14Gangiocatheterwasremovedunderdirectvisionpriortoundockingtherobot.Avideocomprisingintra-operativefootagefromRALoutlinesthistechnique. Results:A14Gangiocatheterwasusedasanassistportin17RALurologicprocedures,16RALdismemberedpyeloplastiesand1roboticorchiopexy.The14Gangiocatheterwasusedtofacilitatestent placement, provide an assistant port for cystoscopic graspers andtoevacuatesmoke.Nocomplicationsoccurredasaresultof14Gangiocatheterplacementsuchassitebleedingorecchymosispost-operatively. Conclusions: The14Gangiocathtechniqueusesexistingequipment,requires no closure and can be placed anywhere on the abdominal wall.ItallowsRALdismemberedpyeloplastytobeperformedwithonly 3 ports instead of traditional 4 and is very versatile and easily adaptable to nearly any robotic surgery. This is the first described methodintheurologicliteratureofusinga14Gangiocathetertomaximize bedside assistance while minimizing port placement in pediatricRALsurgery.
P055THORACOSCOPIC REPAIR OF CONGENITAL DIAPHRAGMATIC EVENTRATION AND EXTRALOBAR LUNG SEQUESTRATION., MelaniecClarkMD,BomaBAdikibiMD,GordonAMacKinlayMD,FraserDMunro,RoyalHospitalForSickChildren,EdinburghTheassociationbetweencongenitaldiaphragmatichernia(CDH)andextralobarlungsequestration(ELS)isarecognisedbutrarephenomenon. The literature has scattered cases reports of this condition, but none having been performed through the minimal invasive route. Amaleinfantwasantenatallydiagnosedwithcongenitalcysticadenomatoid malformation. He was born vaginally at term, he requirednoresuscitation.ACXRondayoneofliferevealedcysticchangesatthebaseoftheleftlung.SixmonthsofagehehadaCTscanandUSSofhischest,whichreportedaprojectionfromthelefthemidiaphragminkeepingwithadiaphragmaticeventrationcontainingkidneyandspleen.Heremainedclinicallyasymptomatic.At19monthsoldhewasadmittedforthoracoscopicrepairofeventration.AtthetimeofsurgerytheleftlungwasdeflatedtorevealaposterolateraldiaphragmaticdefectpluggedbyanELSwithalargefeedingvesselcomingformtheaorta.TheELSwasdissected from the diaphragm using monopolar diathermy and the large feeding vessel was occluded using plasma Kinetic forceps. The diaphragmaticdefectwasclosedusingsixinterrupted2/0ethibondsutures.TheELSwasremovedfromthechestthroughanextendedportsite.Three5mmportswereused.Thelungwasinflated,nochest drain was inserted. The operation time was 1 hour 20 minutes. The patient made a rapid recovery and was discharged home 2 days later.ThepathologyconfirmedthefindingsofanELS.Thepatienthas been seen regularly in the 16 months post surgery. He has remained well, asymptomatic, with barely visible scars and complete symmetry of his chest. The thoracoscopic approach was beneficial over the open approach for this child, enabling him to benefit from reduced post operative pain, reduced hospital stay, early mobilisation and minimal scarring, without an increased operative time, despite the unexpected operative findings. This case reveals the versatility of thoracoscopic surgery in complex, rare and unexpected thoracic pathology.

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 63
2009 Poster AbstractsP056THE THORACOSCOPIC APPROACH TO AN H-TYPE TRACHEOESOPHAGEAL FISTULA, MartinLvanNiekerkMD, UniversityofPretoria,SouthAfricaIntroduction: H-typeTracheoesophagealfistulae(TEF)makeup4%-5%ofesophagealcongenitalabnormalities.H-typeTEFcanoccur anywhere from the cricoid to the carina. Thirty percent of casesarebelowT2.Previouslytheapproachforthissubgroupwasviaathoracotomy.Duringthepastdecademinimalinvasivesurgeryhas become very useful for the treatment of many pediatric thoracic conditions. This poster presents our experience with the thoracoscopic repairofanH-typeTEFatthelevelofT3ina5-day-oldbaby. Patient and method: A2,8kgmalebabypresentedatourinstitutionwithcoughing,chokingandcyanosisduringfeeds.AnH-typeTEFwithoutassociatedanomalieswasdiagnosedbyesophagography. Athree-porttechniquewasused.Carbondioxideinsufflationatapressureof5mmHgandaflowof0,1L/minwasusedtocollapsetheR lung. The posterior pleura was opened and the fistula identified. The fistula was tied off at the trachea and was resected. The opening intheesophaguswassuturedwithinterruptedVicrylstitches.Oralfeedingwasgiven3dayspostop,withnoclinicalsignsofleaking. Discussion: The thoracoscopic approach allows for excellent access and easy identification and resection of a fistula. Conclusion:Thismethodisfeasibleandeasytoachieve.Itoffersimportant advantages over the classic open technique.
P057VIDEO-ASSISTED PARAVERTEBRAL BLOCK IN PEDIATRIC THORACOSCOPIC SURGERY,Nicola1ZadraMD,Paola2MidrioMD,Franca1GiustiMD,Piergiorgio2GambaMD,1AnesthesiaandIntensiveCareUnit,PaduaHospital-2DepartmentofPediatrics,PediatricSurgery,UniversityofPaduaITALy.Video-assistedthoracicsurgery(VATS)isimproperlyconsideredminimally invasive and it can be associated with severe postoperative pain.Acontinuousparavertebralblock(PVB)providesgoodpainreliefafterthoracotomyinchildren(1).Recentlyavideo-assistedapproachtoPVBhasbeenproposedinadults(3)andweusedthistechniqueintwochildren(4and10yrsold)undergoneVATSforlungresection. Surgicalproceduresweremanagedundergeneralanesthesiawithonelungventilation.Attheendofsurgery,withthenondependentlung still collapsed, a scrubbed anaesthesiologist performed a percutaneousparavertebralblockatT6-T7level.Underdirectthoracoscopicviewthecorrectpositionoftheneedle’stip,theinjection of the local anesthetic solution, and the passage of the catheterbeneaththepleurawereeasilycontrolled.Childrenwere rapidly extubated in the operatory room. For postoperative pain control they received oral paracetamol and a continuous paravertebralinfusionofL-Bupivacaine(0.25-0.3mg/kg/h)for24and48hrsrespectively.Postoperativepainwasassessedevery4hrswithCHEOPSandpatientsremainedpainfreewithoutrescueanalgesicsuntil discharge. ContinuousPVBiseffectivetoprovidepostoperativeanalgesiaafterVATSinchildren.Thevideo-assistedapproachiseasierandsaferasitallowsthedirectviewoftheblock,otherwiseblindlyperformed. REFERENCES 1.EngJ,SabanathanS.Continuousparavertebralblockforpost-thoracotomyanalgesiainchildren.JPediatrSurg1992,5:556-557. 2.FeltraccoP,OriC.Anewlookattheparavertebralblock:apercutaneousvideoassistedtechnique.RAPM2007,32:538-539.
P058PERIOPERATIVE OUTCOME OF SURGERY FOR ESOPHAGEAL ATRESIA (EA) WITH TRACHEO-ESOPHAGEAL FISTULA (TEF): IS THE THORACOSCOPIC APPROACH JUSTIFIED?, PhilippOSzavayMD,SabineZundelMD,TobiasLuithleMD,MonikaGirischMD,JoergFuchsMD,DepartmentofPediatricSurgery,DepartmentofPediatricCardiologyandCriticalCare,Children’sHospital,Universityof TuebingenIntroduction: ThoracoscopicapproachforrepairofEAwithTEFhas become a standard procedure in many pediatric surgical centers. Still,therearecriticalconsiderationsofdisciplinesalsoinchargefor these infants, such as neonatologists and pediatric intensive carephysicians.Aimofourinvestigationwastoclearlydefinetheperioperative outcome and complication rate in children undergoing thoracoscopic versus open surgery.
Patient and Methods: Wereviewedpatientrecordsof60newbornsundergoingsurgeryforEAandTEFbetweenMarch2002andSeptember2008.Meangestationalagewas35weeks,meanweight was 2380 g. There were 28 girls and 32 boys. 32 children had associated anomalies. Results: There were 20 children undergoing a thoracoscopic procedure.Inthefirst8casestheoperationwasconvertedtoopenthoracotomy. Reasons for conversion were increasing hypoxia, bad sightandlacerationofthelunginonecase.Another30childrenwere operated through a thoracotomy and in 10 newborns a cervical esophagostomywasperformedduetolong-gapEA.Allchildrenbutthose with the cervical esophagostomy were provided with a chest draindisregardingthetypeofapproach.Meanoperationtime/minutes was 136 in the thoracoscopic and 113 in the thoracotomy group,withnosignificantdifference(p>0.05).Meanventilationtimepostoperatively/hourswas87inthethoracoscopicand94intheopengrouprespectivelywithnosignificantdifference(p>0.05).Complicationssuchaspneumothoraxdespitedrainage,mediastinitis,insufficiency of the anastomosis and dislocation of a clip for the tracheo-esophagealfistulawerenoticedin4childrenundergoingthoracoscopyandin6patientsofthethoracotomygroup.Again,therewasnosignificantdifference(p>0.05). Conclusion:DespiteskepticalconsiderationsthoracoscopicrepairofEAwithTEFisjustifiedduetoacomparableoutcometoopensurgery, competitive operating times, decreased trauma to the thoraciccavityandimprovedcosmesis.Complicationratesarenot higher than in children operated on through a thoracotomy. Howeveralearningcurvehastobetakenintoaccountandlargeexperience in minimal invasive surgery is mandatory for this procedure.
P059AN UNUSUAL COMPLICATION OF 3MM NEEDLE HOLDER IN THORACOSCOPIC DIAPHRAGMATIC HERNIA REPAIR, ABandiMD, MHaddad,SAClarkeMD,Chelsea&WestminsterFoundationNHSTrust,ImperialCollegeLondonA2dayoldmaleinfantunderwentanuneventfulprimarythoracoscopic repair of a left sided diaphragmatic hernia. The case wascompletedusing3mminstruments(KarlStorz).Atthefirstpost operative review an opacification was noted in the central abdominalfieldonroutinechestx-ray.OnCT(imageprovided)thelesion was confirmed as being in the left costophrenic angle and possibly metallic. Atracewasmadeoftheinstrumentwhichhadbeensentbackforhandle problems and subsequently destroyed. No mention had been made of the missing fragment. The fragment is presumed to bethe0.2mmtungstencarbidealloyplateontheanterior2/3rdsofthe jaw of the 3mm needle holder, the absence of which is difficult toseewiththenakedeye.(imagesupplied).TheMedicinesandHealthRegulatoryAgencyhaveconfirmedthesubstancetobebiocompatibleandoflowrisktothepatient. The family were fully informed and the patient remains well with no complications. No plans have been made to remove the fragment .
P060INTRATHORACIC COMPRESSION PROCEDURE ( ITCP) FOR PECTUS CARINATUM., PVarelaMD,FyankovicMD,SMontedonicoMD,HHericeMD,HospitalLuisCalvoMackenna.UniversidaddeChileIntroduction: Pectuscarinatum(PC),isthesecondmostcommonchestwalldeformity.Opensurgicalcartilagesresectiontechniqueshave been the standard procedures. Objective: To report our early experience using a minimally invasive surgerypreviouslyreportedbyAbramson. Methods:fromSeptember2007toSeptember2008,5pediatricmalepatients(averageage:14y.o.)withseverePC,weretreatedinourinstitution with this technique. The procedure uses a intrathoracic steel compression bar and two stabilizers. The bar is placed at the levelofthemaximumsternalprotrusionthrougha2.5cmskinincision at the mid axillary line and passed trough a tunnel under thepectoralmusclesabovethesternum.Afterhavingachievedthecorrection of the deformity, the bar is fixed to the ribs using two stabilizers. Results: Allprocedureswerecompletedsuccessfully.Operativemeantimewas90min.Allpatientsweredischargedfourdaysaftersurgery.Onepatientneededaredointerventionforstabilizerreplacement.Postoperativeresultsweresatisfactoryforsurgeonandpatients in all cases. Conclusions: This is an initial report for a new minimal invasive techniqueforPCtreatment.WesupporttheITCPasavalid

64 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
2009 Poster Abstractstherapeuticoption,forpatientswithPCdeformities.Long-termfollow-upisnecessarytoevaluatetheeffectivenessofthisminimallyinvasive procedure.
P061FLEXIBLE CYSTOURETHROSCOPY IN THE PEDIATRIC POPULATION, JeffreySPalmerMD,GlickmanUrologicalandKidneyInstitute,ClevelandClinicChildren’sHospitalObjectives: Theflexiblecystoscopeisthestandardendoscopeusedfor adult cystourethroscopy. However, the technology has lagged for thepediatricpopulation.Aflexiblecystoscopedesignedspecificallyfor the pediatric population that is short in length and small in diameter would enable this procedure to be performed in children. Weevaluatedaprototypeflexiblepediatriccystoscopetodeterminethefeasibilityofflexiblecystourethroscopy(CUS)inthepediatricpopulation. Methods: Weevaluatedallchildrenlessthan13yearsofageundergoingattemptedflexibleCUS.Theendoscopewasaprototype5-Frenchpediatriccystoscope(Olympus)withupwardanddownwardactivedeflectioncapability.PatientsfirstunderwentflexibleCUSandthenunderwentsemirigidCUSwitha7.5or10-FrenchpediatriccystoscopeinordertovalidatetheflexibleCUSfindings.AsuccessfulflexibleCUSrequiredaccuratelydiagnosingalllesionsnotedonsemirigidCUSandclearvisualizationofspecificendoscopiclandmarks(includingvisualizationofalloftheureteralorificesandthedomeofthebladder).Also,easyofuseoftheflexiblecystoscopeand quality of image were also noted. Results:Sixteenchildren(9girlsand7boys)between7monthsand11.9yearsofageunderwentflexibleCUS.AllpatientssuccessfullyunderwentflexibleCUSwith100%accuracyconfirmedbysemirigidCUS.Thequalityoftheimagewasclearinallcases.Theflexiblecystoscopy was considerably easier to use in the females than in the males due to anatomic reasons. No postoperative complications occurredincludingacuteurinarytractinfectionorurethral/bladdertrauma. Conclusions: This feasibility study demonstrates that the prototype flexiblepediatriccystoscopecanbeperformedwithclearimagingand with similar accuracy.
P062LAPAROSCOPIC VARICOCELECTOMY TO TREAT VARICOCELE RECURRENCE, JeffreySPalmerMD,GlickmanUrologicalandKidneyInstitute,ClevelandClinicChildren’sHospitalObjectives:Oneofthecomplicationsassociatedwithopensurgicaltechniquestotreatvaricocelesisrecurrence.Weevaluatedtheefficacyandsafetyoflymphatic-sparinglaparoscopicvaricocelectomyto correct varicocele recurrence after open varicocelectomy in the pediatric population. Methods: Weevaluatedallchildrenlessthan18yearsofageundergoing laparoscopic varicocelectomy after either an open subinguinaloringuinalvaricocelectomy.Athree-porttechniqueisused with one infraumbilical port and one port in the midclavicular linebilaterallyattheleveloftheumbilicus.Anincisionismadein the posterior peritoneum over the spermatic cord vessels. The vessels are dissected away from the lymphatics with minimal manipulation,andthentheartery/veinsaredoubleligatedwithclipsandtransected.Patientsaremonitoredpostoperativelyforvaricocelerecurrenceandhydroceleformation.Asuccessfulvaricocelectomyis defined as no varicoceles palpable in the standing position with Valsalva. Results: Eightboys10.0and16.7yearsofageunderwentlaparoscopicvaricocelectomy.Allpatientsunderwentsuccessfulvaricocelectomy. No postoperative complications occurred including hydrocele formation, infection, or testicular atrophy after at least 6 monthsoffollow-up. Conclusions:Lymphatic-sparinglaparoscopicvaricocelectomyisan effective and safe technique to treat varicocele recurrence after opensurgery.Postoperativevaricocelerecurrenceandhydroceleformation were not noted.
P063LYMPHATIC-SPARING LAPAROSCOPIC VARICOCELECTOMY IS EFFECTIVE AND SAFE, JeffreySPalmerMD,GlickmanUrologicalandKidneyInstitute,ClevelandClinicChildren’sHospitalObjectives: Complicationsassociatedwithopenvaricocelectomytechniques include varicocele recurrence and hydrocele formation. These complications have also been noted with laparoscopic
varicocelectomy.Wedeterminedtheeffectivenessandsafetyoflymphatic-sparinglaparoscopicvaricocelectomyinthepediatricpopulation. Methods:Weevaluatedallchildrenlessthan18yearsofageundergoinglaparoscopicvaricocelectomyforgrade3varicoceles.Athree-porttechniqueisusedwithoneinfraumbilicalportandoneport in the midclavicular line bilaterally at the level of the umbilicus. Anincisionismadeintheposteriorperitoneumoverthespermaticcord vessels. The vessels are dissected away from the lymphatics with minimalmanipulation,andthentheartery/veinsaredoubleligatedwithclipsandtransected.Patientsaremonitoredpostoperativelyforvaricocelerecurrenceandhydroceleformation.Asuccessfulvaricocelectomy is defined as no varicoceles palpable in the standing positionwithValsalva. Results:Forty-eightboysbetween10.0and17.6yearsofageunderwent laparoscopic varicocelectomy. No patient needed to beconvertedtoanopenvaricocelectomy.Allpatientsunderwentsuccessful varicocelectomy. No postoperative complications occurred including hydrocele formation, infection, or testicular atrophy after atleast6monthsoffollow-up. Conclusions:Lymphatic-sparinglaparoscopicvaricocelectomyisaneffectiveandsafetechniquetotreatvaricoceles.Postoperativevaricocele recurrence and hydrocele formation were not noted.
P064TYPE IV POLYORCHIDISM WITH AN UNUSUAL PRESENTATION, BaranTokarMD,UmutAliciMD,DilsadDemetMD,EskisehirOsmangaziUniversitySchoolofMedicine,DeptofPediatricSurgery,EskisehirTurkeyPolyorchidismisararepathologywithlessthan100casesreporteduptodate.Thereare4typesandtypeIVistherarestonewhichisacompleteduplicationofthetestis,epididymisandvas.Inreported locations, only 5% of the supernumerary testis is located retroperitoneally.WepresentacasehavingtypeIVunilateralpolyorchidismwithaproximaltestislocatedinabdomen.A5-year-oldboywhohadlaparoscopyandtheninguinalexplorationfora left nonpalpable testis is presented. The right testis was in the scrotum. Laparoscopic intraabdominal exploration followed by inguinalexplorationwasperformedfortheleftside.Inlaparoscopicexploration, an intraabdominal testis with its vas and vessels was determined on the left side. The testis was very mobile, and couldbeeasilytransferreddownintothescrotum.Pullingtheleft testis toward the right inguinal canal orifice was performed totestfeasibilityofthetestisfororchidopexy.Asasecondstep,inguinalincisionwasdonetoexploretheinguinalareaandtomakeorchidopexy.Inguinalexplorationshowedanothertestiswithitsownepididymis, vas and vessel. This testis was atrophic. The diagnosis was typeIVpolyorchidismontheleftside.Orchiectomywasdoneforthedistalinguinalatrophictestis.Orchidopexywasperformedfortheproximal abdominal testis. The primitive gonadal ridge is an elongated structure in fetus, polyorchidism may occur with transverse fragmentation of the gonodalridge.Acompleteseparationofthetestesanddrainagesystem is very unusual presentation in polyorchidism, and it needs duplication of both the genital ridge and the mesonephric duct. Ifthetesticularqualityispoor,orchiectomyshouldbedoneinthesupernumerary testis.
P065EARLY ENDOSCOPIC INCISION OF URETEROCELE DETECTED BY PRENATAL ULTRASOUNDS: TEN YEARS EXPERIENCE, LuciaVirardiMD,MariaGraziaScuderiMD,ElenaCamardaMD,SalvatoreArenaMD,VincenzoDiBenedettoPhD,PediatricSurgery-UniversityofCatania-ItalyAim: Prenatalultrasonographyhasresultedinadrammaticincreasein the number of infants detected with asymptomatic urophatology, allowing treatment before the potencial consequences of urinary sepsys. The aim of this study is to show our experience after ten years ofendoscopicincisionofureterocels(EIU). Methods: From 1998 to 2008, 27 children with ureterocele have been observed in our department. 18 cases were detected by prenatalultrasoundsandconfirmedinthefirstfewdaysoflife.Inallcasestheureterocelehavebeenincisedinthefirsttwoweekafterthe diagnosis as treatment of choise andin one day surgery. Results:EIUhasresultedinadrammaticdecompressionoftheureterocelesin100%ofcases(1bilateral).Refluxintheupperpolewas created in 60% of cases while upper pole preservation was achieved in 100%.

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 65
2009 Poster AbstractsSurgicalrecostructionofbladderneckandexcisionofureterocelewasdonein60%ofcases,while40%ofcaseshadonlyEIUprocedure. Conclusions: webelievethatEIUproceduremustbeconsideredthe treatment of choise for asymptomatic patients with ureteroceles detected by prenatal ultrasounds. Moreover endoscopic procedure has permitted a totally recovery of the upper pole in our series though 60% of patients undergone secondary surgical procedure.
P066OPEN VS MINIMALLY INVASIVE PYELOPLASTY IN CHILDREN: A COMPARATIVE ANALYSIS, SarahMariettiMD, ChristinaKimMD, ConnecticutChildren’sMedicalCenterThe use of minimally invasive surgery in pediatrics is constantly expanding.Inthepast,pyeloplastyhadbeenperformedexclusivelywithanopenapproach.Bothstandardlaparoscopyandroboticsurgery are options to perform the same surgery with a minimally invasiveapproach(MIS).WeshareourexperiencewithbothopenandMISpyeloplastyinchildren. BetweenJanuary2004andApril2008,ourpracticeperformed18openand28MISpyeloplasties.Welookedatlengthofoperation,postoperative pain management, rate of complications, length of hospital stay, and postoperative results. OperativetimewasclearlylongerintheMISgroupwithtotalORtime of 543 min versus 241 min respectively. 67% of open patients hadanepiduralversus0%oftheMISpatients.Therewasnostatistically significant difference in complications between the two groups There were no intraoperative complications in either group.. There were no postoperative complications in the open groupand1intheMISgroup(urineleak).ThehospitalstaywasshorterintheMISgroup.97%ptsintheMISgroupweredischargedby postoperative day 2 versus only 39% of the open group. Postoperativeimagingwasimprovedin89%oftheopengroupand83%oftheMISgroup. OurexperienceshowslowcomplicationsandgoodresultswithMISpyeloplasties.AlthoughouroperativetimeforMISishigher,itdoesnot factor in the additional step of cystoscopy and stent placement thatdidnotoccurintheopenpopulation.Whenweassessedoperative time with experience, we saw shorter operative times with moreexperience.Ourresultsreinforcethebeliefthatbothstandardlaparoscopyandroboticapproachestopyeloplastyprovidesquickerrecovery with comparable surgical results.
P067HYDROCELE IN THE PEDIATRIC PATIENTS: INGUINAL OR SCROTAL APPROACH OR LAPAROSCOPIC CORRECTION?, Hiroo TakeharaMD,HisakoKuyamaMD,DepartmentofPediatricSurgeryandPediatricEndosurgery,TokushimaUniversityHospital,Indirectinguinalherniaorcommunicatinghydroceleisthemostfrequent operation performed on children by pediatric surgeons and urologists. Hydrocele is generally treated with the traditional inguinalapproachorthescrotalapproach.WedescribeourexperiencewithLPEC(laparoscopicpercutaneousextraperitonealclosuremethod)forhydrocelecausedbythepatentprocessusvaginalis. Wehaveperformed850LPECsin670childrenwithinguinallesions (575 cases with inguinal hernia, 95 cases with hydrocele ofthecordorscrotum).TherewerenooccurrencesofhydroceleafterLPECsfor755hernias.Ofthese95patients,50(2-15yearsofage)hadcommunicatinghydrocele,45(1-9yearsofage)hadnoncommunicating hydrocele including 6 with abdominoscrotal hydrocele. Thelaparoscopiccorrectionofhydroceleinvolveshigh-circuitsuturingoftheprocessusvaginalis,asinLPECforinguinalhernia.The distal part of the noncommunicating hydrocele is left open laparoscopically via the internal inguinal ring, or a percutaneous puncture, or a small incision in the scrotum. No recurrence was observedin50communicatinghydrocelestreatedwithLPEC.Of45noncommunicatinghydrocelestreatedwithLPECandadditionaldrainage,oneabdominoscrotaltypecomplicatedwiththickenedwall of hydrocele developed to recurrence because of insufficient celotomy for concealed hydrocele. These results suggest it is unnecessary to dissect the processus vaginalis and hydrocele from the spermatic cord and vessels with inguinal approach or the scrotal approach. The advantages of this strategybyLPECarenotonlysimpleandminimallyinvasiveclosure,butalsoalowerriskofinjurytothespermaticductorvesselsandcomplete closure of the communication between the peritoneal cavity and the hydrocele to a greater or lesser degree.

66 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
IPEG 2009 Exhibits F loor P lan
ENTRANCE
SAGES / IPEGLEARNING CENTER TO POSTERS
&LEARNINGCENTER
FOOD SEATING AREA FOOD SEATING AREA
920
401
20'
30'
408
410 411
20'
30'412
414
416
418 419
420 421
422 423
424 425
426
428 429
30'
30'430
432
435
441
20'
20'
501
40'
40'
511
60'
60'
512
20'
516
20'521
20'
20'
527
20'
20'
532 533
535
601
20'
605
607
625
20'
20'
631
20'
20'
636 637
20'
20'638
642 643
644 645
700
20'
701
20'
704 705
20'706
711
50'
40'
727
40'
40'
737
739
742
743
20'
20'
744
800 801
802 803
804 805
20'806
836 837
838 839
845
901
20'902
904 905
906 907
915
917
927
20'
20'
931
20'
20'
936 937
20'938 939
940 943
944
945
1000
1002
20'
1006 1007
20'
20'
1010
1012 1013
20'
1017
1020 1021
1022 1023
1025
20'
1031
20'
20'
1037
1039
1040
1042 1043
1044 1045
1101
1103
1105
1107
1109
1111
922
1100
1102
1001
20'
ENTRANCE
SIGN-IN
CMEKIOSKSCYBER
CAFE
EXHIBITOFFICE
721
30'
30'
437
20'
539
20'
841
20'
911
20'
1014
20'
SPEAKERREADYROOM
ENTRANCE
20'
20'
20'VIEWING
AREA
FREEMANSERVICE
DESK
IPEG POSTERS
SAGES POSTERS
EXHIBITORLOUNGE
SAGES / IPEG HANDSON COURSES
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
16
SAGES / IPEGREGISTRATION
SAGES / IPEGREGISTRATION
COPYRIGHT 2000, FREEMAN DECORATING CO., ALL RIGHTS RESERVED.
EVERY EFFORT HAS BEEN MADE TO ENSURE THE ACCURACY OF ALL INFORMATION CONTAINED ON THIS FLOORPLAN. HOWEVER, NO WARRANTIES, EITHER EXPRESSED OF IMPLIED, ARE MADE WITH RESPECT TO THIS FLOORPLAN. IF THE LOCATION OF BUILDING COLUMNS, UTILITIESOR OTHER ARCHITECTURAL COMPONENTS OF THE FACILITY IS A CONSIDERATION IN THE CONSTRUCTION OR USAGE OF AN EXHIBIT, IT IS THE SOLE RESPONSIBILITY OF THE EXHIBITOR TO PHYSICALLY INSPECT THE FACILITY TO VERIFY ALL DIMENSION AND LOCATIONS.
C
9900 Business ParkwayLanham, Md 20706PHOENIX, AZ
PHOENIX CONVENTION CENTER - HALLS A-DAPRIL 22-25, 2009
SAGES 200903.24.2009

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 67
IPEG 2009 Exhibitors3-DMED SURGICAL TRAINING AIDS #704255IndustrialDriveFranklin,OH45005Tel:937-746-2901 Fax:937-746-5071Website:www.3-Dmed.com
3-DmedSurgicalTrainingAidsistheinnovatorandmanufacturerofthe“MinimallyInvasiveTrainingSystem”.The3-Dmedsystemisusedworldwideasamulti-specialtylearningenvironmentandinstrumentdemonstrationtool.3-Dmedalsooffersothermedical and surgical simulation training aids including custom solutions.
ACS BSCN #904BariatricSurgeryCenterNetwork(ACSBSCN) AccreditationProgram633N.St.ClairStreet,22ndFloorSEChicago,IL60611Fax:312-202-5063Website:www.acsbscn.org
TheACSBariatricSurgeryCenterNetwork(ACSBSCN)AccreditationProgramaccreditsbariatricsurgeryfacilitiesthatmaintain certain physical and human resources, standards of practice,andthedocumentationofoutcomes.VisitSAGESbooth#904orwww.acsbscn.org for more information.
ADOLOR CORPORATION/ GLAXOSMITHKLINE #901700PennsylvaniaAvenueExton,PA19341Tel:484-595-1500 Fax:484-595-1520Website:www.entereg.com
AdolorCorporationisabiopharmaceuticalcompanyspecializingin the discovery, development and commercialization of novel prescription pain management products. For more information, visit www.adolor.com.
GlaxoSmithKlineoffersanumberofprogramstosupporteffective health management strategies and improve patient care.Visitourexhibitforinformationaboutourproductsandprograms.
AESCULAP, INC. #7013773CorporateParkwayCenterValley,PA18034Tel:610-797-9300 Fax:610-791-6888Website:www.aesculap.com
Aesculapoffersafullrangeofmonoplarandbipolarlaparoscopic instrumention in both standard and longer bariatric lengths.Aesculap’s“SuturingMadeSimple”needleholdersare top choice for the laparoscopy surgeons instrument armamentarium.Stopbyourboothandseewhysurgeons“ThinkAesculap”forlaparoscopy.
AGENCY FOR MEDICAL INNOVATIONS, INC. #64220MainStreet,Suite205Natick,MA01760Tel:508-655-1200 Fax:508-655-0012Websitehttp://www.amisurgical.com
The(DG)HAL/RARRDopplerguidedHemorrhoidArterialLigation/RectalAnalRepairSystemisthefirstsystemtoutilizeminimally invasive surgical techniques to treat the source of hemorrhoidal disease without surgical excision, stapling or banding.AdditionalproductsincludeFaciacutterandgastricband cutter.
ALLERGAN #4112525DupontDriveIrvine,CA92612Tel:714-246-4500 Fax:714-246-4971Website:www.allergan.com
AllerganhasjoinedtheefforttofightthegrowingobesityepidemicwiththeLAP-BAND®AdjustableGastricBandingSystem,thefirstminimallyinvasivesurgicalapproachapprovedintheUnitedStatesbytheFDA,tohelppatientsachievesustained weight loss, realize theirgoals for healthy living, and reduceobesity-relatedrisks.
ALOKA ULTRASOUND #51210FairfieldBoulevardWallingford,CT06942Phone:203-269-5088TollFree:800-872-5652Fax:203-269-6075Website:www.aloka.com
AlokaUltrasoundfeaturessurgicalultrasoundsystemsthatofferexceptionalimagequalityandunmatchedclinicalversatility.Ourextensive array of transducers allows for imaging during both open and laparoscopic surgical procedures.
ALVEOLUS, INC. #7399013PerimeterWoodsDrive,SuiteACharlotte,NC28216Tel:704-926-4896 Fax:704-926-4838Website:www.alveolus.com
Alveolusisaleadingdeveloperofinnovativetechnologyintheemergingfieldofnon-vascularinterventionalstenting.Alveolushasdesignedstenttechnologyanddeliverydeviceapplicationsforuseintheesophagus(ALIMAXX-E™),biliarytract(ALIMAXX-B™)andlungs(AERO™).
ANESTHESIA HEALTHCARE PARTNERS #4163079PeachtreeIndustrialBlvd.Duluth,GA30097Tel:1-800-945-6133 Fax:678-546-3606Website:www.ahphealthcare.com
AnesthesiaHealthcarePartners®,Inc.(AHP)providesturnkeyanesthesia services to hospitals and surgery centers across the country. This includes managing daily operations, billing and recruiting permanent and locum nurse anesthetists.
ANGIOTECH #1039100DennisDriveReading,PA19606Tel:610-404-1000 Fax:610-404-2061Website:www.angiotech.com
Quill™SRSisabidirectionalbarbedsuturesystemthatcloseswoundswithoutknottying.TheresultsareimprovedefficiencyintheORwithenhancedwoundclosure.
ATRIUM MEDICAL CORPORATION #5395WentworthDriveHudson, NH 03051Tel:603-880-1433 Fax:603-386-6159Website:www.atriummed.com
Atrium’snewC-QUR™Meshproducttechnologycombineourindustry-leadingProLite™polypropylenesurgicalmeshwithaproprietary,highlypurifiedOmega3fattyacidbio-absorbablecoating.Pre-clinicalstudiesdemonstrateaminimizationofperitoneal tissue attachment, including a significant reduction inforeignbodyreactionandinflammation,resultinginawellhealed, reinforced repair.

68 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
IPEG 2009 ExhibitorsAUTOMATED MEDICAL PRODUCTS CORP #1000P.O.Box2508Edison,NJ08818Tel:732-602-7717 Fax:732-602-7706Website:www.ironintern.com
AutomatedMedicalProductsCorpofferstheIronIntern®Availableforuseinlaparoscopicandopensurgery.TheIronIntern®StieberRibGripKitprovidessuperiorexposureintheabdomen and serves liver transplants. Find out more about these products at www.ironintern.com.
B-LINE MEDICAL #644130019thStreet,Suite100NWWashington,DC20036Tel:301-768-4461 Fax:202-330-5267Website: www.blinemedical.com
B-LineMedicalisadigitalsolutionsfirmfocusedonthecapture,debriefingandassessmentofsimulation-basedmedicaltraining.B-LineMedicalspecializesinthedeliveryofrobust,yeteasytouseweb-basedsolutionsthathavehelpedoverninetytophospitals,medicalschoolsandnursingprogramsintheU.S.,Canada,Europe,andMiddleEastoperateandmanagetheirclinicalskillsandsimulationscentersmoreeffectively.
BARIATRIC TIMES #1105MatrixMedicalCommunications,LLC1595PaoliPike,Suite103WestChester,PA19380Tel:484-266-0702 Fax:484-266-0726FaxWebsite:www.bariatrictimes.com
PleasestopbyBooth1105topickuptherecentissueofBariatricTimes and information regarding discounts on our educational textbooks,includingtherecentlypublishedWeightLossSurgery:AMultidisciplinaryApproach,editedbyDrs.RaulRosenthalandDanJones.OtherMatrixMedicalpublications:Psychiatry2009/BariatricTimes/BMI:BodyMind&Inspiration/JournalofClinical&AestheticDermatology
BÂRRX MEDICAL, INC. #516540OakmeadParkwaySunnyvale,CA94085 Tel:408-328-7300 Fax:408-328-7395 Website:www.barrx.com
BÂRRXMedical,Inc.developssolutionsfortreatingBarrett’sesophagus.TheFDAapprovedHALO360andHALO90Systemsare based on patented technology that carefully control the amount of ablative energy delivered to effectively remove the diseasedtissueandfacilitatethere-growthofnewhealthytissue.
B-K MEDICAL SYSTEMS, INC. #435250AndoverStreetWilmington,MA01887Tel:800-876-7226 Fax:978-988-1478Website:www.bkmed.com
B-KMedicalhasbeenamarketleaderinSurgicalultrasoundforover30years.Weprovidecuttingedgetechnology,superiorimage quality, the highest standard in sterilization options, HIPPAcompliant,ease-of-use,aswellasadedicatedandhighlytrained staff.
BOSTON SCIENTIFIC #705100BostonScientificWayMarlboro,MA01752Tel:5086834000Website:www.bostonscientific.com
BSCiscommittedtothedevelopmentofdevicesandsystemsthatsupportourcustomers’goalsformoreefficientproceduresthatcontributetobetterpatientoutcomes.Collaborationandclinical support are at the core of how we deliver exciting new technologies.
CALMOSEPTINE, INC. #90216602BurkeLaneHuntingtonBeach,CA92647-4536Tel:714-840-3405 Fax:714-840-9810Website:www.calmoseptineointment.com
CalmoseptineOintmentisamulti-purposemoisturebarrierthatprotectsandhelpshealskinirritationsfrommoisture,suchasurinaryandfecalincontinence.CalmoseptineOintmenttemporarily relieves discomfort and itching. Free samples at our booth!
CAMBRIDGE ENDOSCOPIC DEVICES, INC. #1010119HerbertStreetFramingham,MA01802Tel:508-405-0790Website: www.cambridgeendo.com
Autonomy™Laparo-Angle™technologyenablessurgeonstohave unprecedented vision, access and control in even the most challenging single site and traditional laparoscopic procedures. Autonomyprovidessevendegreesoffreedom,fullarticulationandrotation,andtheabilitytolockinanyposition.
CINE-MED, INC. #601127MainStreetNorthWoodbury,CT06798Tel:203-263-0006 Fax:203-263-4839Website:www.cine-med.com
Ciné-MedpartnerswithSAGEStoproduceanddistributetheSAGESvideolibrary,includingSAGESGrandRounds,PostgraduateCoursesandtheSAGESPearlsseries.Stopbybooth#601formoreinformationandtoviewsamplesofthesevideosand more.
CONMED CORPORATION #521525 French Road Utica,Ny13502Tel:315-797-8375 Fax:315-797-0321Website:www.conmed.com
ConMedCorporationoffersitscustomersoneofthemedicalindustry’smostdiverseselectionofinnovative,state-of-the-artdevices and systems for the orthopedic, endoscopic, laparoscopic, gastroenterology, integrated operating room, and general surgerymarkets.
COOK MEDICAL #700750DanielsWayBloomington,IN47404Tel:800-457-4500 Fax:800-554-8335Website:www.cookmedical.com
CookMedicalwasoneofthefirstcompaniestohelppopularizeinterventional medicine, pioneering many of the devices now commonly used worldwide to perform minimally invasive medical procedures.

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 69
IPEG 2009 ExhibitorsCOVIDIEN #511150GloverAveNorwalk,CT06850Tel:800-722-8772 Fax:888-636-1002Website:www.covidien.com
Covidienisaleadingglobalhealthcarecompanythatcreatesinnovative solutions for better patient outcomes and delivers valuethroughclinicalleadershipandexcellence.Covidienmanufacturesarangeofindustry-leadingproductsinfivesegmentsincludingSurgicalandEnergy-basedDevices.
CROSPON INC. #839701PalomarAirportRoad,3rdFloorCarlsbad,CA92011Tel:760-931-4801 Fax:760-931-4804Website:www.endoflip.com
Crospon’sfirstproduct,EndoFLIP®(EndolumenalFunctionalLumenImagingProbe)isanimagingtoolwhichmeasuresthedimensions and distensibility of hollow organs in the alimentary tract.EndoFLIP®maybeusedtoassistinthediagnosisofGastroesophagealRefluxDisease(GERD),forGERDsurgeryassessment,andformeasurementinBariatricsurgery.
DAVOL INC. #625100CrossingsBlvd.Warwick,RI02886Tel:800-556-6275 Fax:401-825-8759Website:www.davol.com
BardDavol,themarketleaderinherniarepair,offersabroadrange of unique synthetic and biologic implants for laparoscopic andopenapproaches.Additionally,theNEWSorbaFix™FixationSystemprovidesstrong,consistent,andreliablefixationwithfully absorbable fasteners.
DELLTA TECH - SIMENDO #605Weena873013CHRotterdamThe Netherlands Tel:+31(0)104128014Fax:+31(0)847301117Website:www.simendo.eu
SIMENDO®isalaparoscopytrainingsimulatorforthesimpleandadvancedbasicskills.TheSIMENDOisaninnovativetoolthat supports a complete validated training curriculum with a veryusefulscoringsystem.TheSIMENDOcanbeappliedfromthe moment you received the system and is a great answer if youarelookingforaneffectiveandeasytrainingsolution.Thesimulatoriscompact,light-weightedandcanbetransportedinasmall suitcase.
EAGLE SURGICAL PRODUCTS LLC #425615EagleAustin,TX78734Tel:512-261-3104 Fax:512-261-3893Website:www.eaglesurgicalproducts.com
ElectroLube™:Easytouseelectrocauterycoating.Reducescharringofcauterytip.Reducestissuestickingtocauterytip. Facilitates cutting and coagulation and helps protect cauteryprobesfromwear.Savestimeandimprovesqualityofelectrocautery performance.
ELSEVIER, INC. #11011600JohnF.KennedyBlvd.,Ste.1800 Philadelphia,PA19103Tel:215-239-3900 Fax:215-239-3494Website:www.elsevierhealth.com
ELSEVIER,acombinedpremierworldwidehealthsciencepublishingcompany,incorporatingSAUNDERS,MOSBy,CHURCHILLLIVINGSTONE,BUTTERWORTHHEINEMANNandHANLEy-BELFUSpresentsourlatesttitlesinGastroenterology.Visitandbrowsethroughourcompleteselectionofpublicationsincludingbooks,periodicals,andsoftware.
ENDOCONTROL #10375avenueduGrandSablonLaTronche38700-FranceTel:+33476637583 Fax:+33476549561Website:www.endocontrol-medical.com
EndoControlisaninnovativecompanyspecializedinroboticassistanceforminimallyinvasivesurgery.ViKy®ourmainproduct, is a compact motorized endoscope holder for laparoscopic surgery which role is to maintain and move the endoscope according to surgeon orders with a footswitch control.
ENDOGASTRIC SOLUTIONS #920555TwinDolphinDrive,Suite620RedwoodCity,CA94065Tel:650-226-2225 Fax:650-226-2201Website:www.endogastricsolutions.com
EndoGastricSolutions,(EGS)isthepioneerinincisionlesssurgicalprocedures for the treatment of upper gastrointestinal diseases. TIF(TransoralIncisionlessFundoplication)withEGS’EsophyX™device creates a valve between the stomach and esophagus, reduceshiatalhernia,andrestorestheanatomytoreduce/preventgastroesophagealreflux.
ETHICON ENDO-SURGERY, INC. #7114545CreekRoadCincinnati,Ohio45242Tel:800-USE-ENDO Fax:800-873-3636Website:www.ethiconendo.com
EthiconEndo-Surgery,Inc.developsandmarketsadvancedmedical devices for minimally invasive and open surgical procedures.Thecompanyfocusesonprocedure-enablingdevicesfor the interventional diagnosis and treatment of conditions in general and bariatric surgery, as well as gastrointestinal health, plastic surgery, orthopedics, gynecology, and surgical oncology.
GENERAL SURGERY NEWS #907545West45thStreetNewyork,Ny10036Tel:212-957-5300 Fax:212-957-7230Website:www.generalsurgerynews.com
GeneralSurgeryNewsisamonthlynewspaperdesignedtokeepgeneral surgeons abreast of the latest developments in the field. The publication features extensive meeting coverage, analysis of journal articles, educational reviews, and information on new drugs and products.

70 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
IPEG 2009 ExhibitorsGI DYNAMICS #441OneMcGuireRoadLexington,MA02421Tel:781-357-3306 Fax:781-357-3301Website:www.gidynamics.com
GIDynamics,foundedin2003,isdevelopingtheEndoBarrier™GastrointestinalLiner,anovelendoscopictechnologyfortreatingObesityandType2Diabetes.GIDynamicsisledbyanexperienced management team and a scientific advisory board comprised of internationally recognized leaders in bariatric surgery, gastroenterology, obesity medicine, endocrinology, andmedicalweightloss.Thecompany’sfirsttechnology,theEndoBarrier™gastrointestinalliner,isbeingstudiedinclinicaltrials for the treatment of obesity and type 2 diabetes in the U.S.,Europe,andSouthAmerica.GIDynamicshasreceivedCEMarkapprovalfortheirfirstproductandisplanningtoinitiateaPivotalStudyintheU.S.
GORE & ASSOCIATES #401P.O.Box2400Flagstaff,AZ86003Tel:928-779-2771/800-437-8181Website:www.goremedical.com
GoreMedicalProductsDivisionhasprovidedcreativetherapeuticsolutions to complex medical problems for three decades. The extensiveGoreMedicalfamilyofproductsincludesvasculargrafts, endovascular and interventional devices, surgical materials for hernia repair, soft tissue reconstruction, staple line reinforcement, and sutures for use in vascular, cardiac and general surgery.
H & H SURGICAL TECHNOLOGIES #8034437 Robertson RoadMadison,WI53714Tel:608-222-2776 Fax:608-222-2604Website:www.hhsurgical.com
H+HSurgicalTechnologiesisaleaderinpre-ownedmedicalequipmentsales.Wespecializeinflexibleendoscopy,laparoscopyandrelatedinstrumentation.Wearededicatedtoprovidinghighqualityandcustomersatisfaction.Wefeelthatour prices are unbeatable and we stand behind every piece.
HAPTICA INC #636101FederalStreet,Suite1900Boston,MA,02110Tel:6173427270 Fax:6173427080Website:www.haptica.com
Haptica’saward-winningProMIS™SurgicalSimulatoristhebestvalidatedsimulatorfortraininginlaparoscopicskillsandprocedures.ProMIS’‘mixedreality’approachhasbeenshowntobebetterthanVRandpreferredbyusers.Hapticaalsodevelopscustomsimulationsolutionstoaccelerateuptakeofnewsurgicaldevices
HCA PHYSICIAN RECRUITMENT #10063MarylandFarms,Suite150Brentwood,TN37027Tel:866.889.0203Website:www.PracticeWithUs.com
HCAownsandoperates169healthcarefacilitiesin20stateswithopportunitiescoasttocoast.Wearecommittedtothecareandimprovementofhumanlife.Westrivetodeliverhighquality,cost effective healthcare that meets the needs of communities.
HRA RESEARCH #836400LanidexPlazaParsippany,NJ07054Tel:973-240-1200Website:www.hraresearch.com
Ourteamofexperiencedinterviewerswillbedistributingcarefullydevelopedquestionnaires.We’llbegatheringtheanswerstovitalmarketingandclinicalquestions-answersthatcan affect the introduction of new products or the continuation of existing healthcare products and services.
I-FLOW CORPORATION #102520202WindrowDriveLakeForest,CA92630Tel:800-448-3569 Fax:949-206-2600Website:www.iflo.com
ON-Q®islabeledtosignificantlyreducepainbetterthannarcoticsandtosignificantlyreducenarcoticsintakeaftersurgery.ON-Qwasupheldasabestpracticeforpost-surgicalpain relief and its widespread use was encouraged as part of anindependentstudypublishedintheprestigiousJournalofAmericanCollegeofSurgeons.
IMMERSION #93155WestWatkinsMillRoadGaithersburg,MD20878Tel:800-929-4709 Fax:301-984-2104Website:www.immersion.com
Immersion’sMedicallineofbusinessdesigns,manufactures,andmarketscomputer-basedsurgicalsimulationtrainingsystemsworldwide. The medical and surgical simulators integrate proprietarycomputersoftwareandtactilefeedbackroboticsto create highly realistic medical simulations that help train clinicians.Thecompany’skeyproductlinesaretheVirtualIVsystem,EndoscopyAccuTouch®simulator,CathLabVRsurgicalsimulator,andLaparoscopyVRsurgicalsimulationsystem.
INTUITIVE SURGICAL, INC. #4291266 Kifer RoadSunnyvale,CA94086Tel:408-523-2100 Fax:408-523-1390Website:www.intuitivesurgical.com
IntuitiveSurgical,Inc.istheglobaltechnologyleaderinrobotic-assisted,minimallyinvasivesurgery.TheCompany’sdaVinci®SurgicalSystemenablesgeneralsurgeonstoofferanew,minimally invasive approach to patients.
JLJ MEDICAL DEVICES INT’L #9156585EdenvaleBoulevard,Suite150EdenPrairie,MN55346Tel:952-929-3881 FAX:952-929-3984Website:www.JLJMedicalDevices.com
JLJMedicalDevicesInt’lprovidestheSeeClear®MAX™patentedlaparoscopicsmokeevacuationfiltersystem.Itprovidescontinuous,automaticclearanceofsmokeandbioaerosols–without loss of pneumoperitoneum. No suction is required. Maintains visual clarity and prevents exposure to surgical plume.

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 71
IPEG 2009 ExhibitorsKARL STORZ ENDOSCOPY-AMERICA, INC. #7212151E.GrandAvenueElSegundo,CA90245Phone:800-421-0837Website:www.ksea.com
KARLSTORZEndoscopy-America,Inc.,theleaderinendoscopyequipment and instrumentation, offers a comprehensive line ofproductsforLaparoscopyandGI.OurImage1®FULLHDplatform that acquires and displays wide 16x9 1080p60 images provides the optimal viewing experience in minimally invasive surgery.
LAPAROSCOPIC TECHNOLOGIES, INC. #410140075thStreetKenosha,WI53143Tel:262-658-3914 Fax:262-658-2699Website:www.lapforceps.com
LaparoscopicTechnologies,Inc.isasurgicalinstrumentmanufacturing company committed to design, manufacturing, andmarketingofdevicesforminimallyinvasivesurgicalprocedures.Specifically,SchellpfefferForcepsaremanufacturedto facilitate removal of laparoscopically resected tissue specimens and laparoscopic tissue retrieval sacs.
LEXION MEDICAL #8005000TownshipParkwaySaintPaulMN55110Tel:877-9LEXION Fax:651-635-0090Website:www.lexionmedical.com
LEXIONMedical,aleaderofinnovativemedicaltechnologiesimprovingpatientsafety,offerstheInsuflow®LaparoscopicGasConditioningSystemsandthePneuVIEW®LaparoscopicSmokeEliminationSystem.
LIFECELL #1002OneMillenniumWayBranchburg,NJ08876Tel:908-947-1100 Fax:908-947-1087Website:www.lifecell.com
LifeCellisaleadingproviderofherniarepairandbreastreconstructionproductsincludingAlloDerm®andStrattice®.LifeCellTissueMatricessupporttissueregenerationthroughrapid revascularization, cell repopulation and white cell migration; may help to optimize aesthetic outcomes in breast applications;andmayminimizetherisksofsomecomplications.LifeCellislaunchingStratticeforbreastplasticsurgeryrevisionsin 2009.
LIPPINCOTT WILLIAMS & WILKINS #6073013E.SouthForkDrivePhoenix,AZ85048Tel:480-704-1995 Fax:480-704-1995Website:www.lww.com
ComebyandseesomeofthelatestbooksfromLWWandalsorepresentingSpringer,Thieme,McGraw-Hill&BCD.
MARKET ACCESS PARTNERS #8053236 Meadowview RoadEvergreen,CO80439Tel:303-526-1900 Fax:303-526-7920Website:www.marketaccesspartners.com
MarketAccessPartnersprovidesmarketresearchconsultingtothemedicaldeviceandPharmaceuticalindustries.Weuse innovative qualitative and quantitative methodologies to researchopinionsofphysicians,nursesandpatients.Weofferamanagement-orientedapproachtoproductdevelopmentandmarketing.
MARY ANN LIEBERT, INC., PUBLISHERS #426140HuguenotStreetNewRochelle,Ny10801Tel:914-740-2100 Fax:914-740-2101Website:www.liebertpub.com
MaryAnnLiebert,Inc.publishesauthoritativejournalsinpromising areas of science and biomedical research, including JournalofLaparoendoscopic&AdvancedSurgicalTechniques,(www.liebertpub.com/lap).TheJournalfocusesonsurgicaltechniquesandadvancedsurgicaltechnologies.ComplimentaryCopies@Booth#426.
MAST BIOSURGERY, INC. #4326749TopGunStreet,Suite108SanDiego,CA92121Tel:858-550-8050 Fax:858-550-8060Website:www.mastbio.com
TheSurgiWrap®BioresorbableProtectiveSheetisdesignedtosupportandreinforcesofttissues&minimizeunwantedpost-surgicalsofttissueattachmentstothedevice,FDAClearedforbothopenandlaparoscopicprocedures.MASTBiosurgeryisa leader in the development and production of bioresorbable polymer implants.
MEDIFLEX SURGICAL PRODUCTS #1021250GibbsRoadIslandia,State:NyZip:11749Tel:800-879-7575 Fax:631-582-8487Website:www.mediflex.com
Forover30years,MediflexhasledthewayindesigningandmanufacturinguniquelyengineeredproductsusedinOperatingRoomsaroundtheworld.MediflexoffersanexpandedlineofTableMountedRetractorSystemsprovidingthewidestrangeofBookwalterT™compatibleproductsavailabletoday.
MEDTRONIC, INC. #706710MedtronicParkwayMinneapolis,MN55432-5604Tel:763-514-4000 Fax:763-514-4879Website:www.medtronic.com
Medtronicisthegloballeaderinmedicaltechnology–alleviating pain, restoring health and extending life for millionsofpeoplearoundtheworld.Medtronic’sU-CLIP®Devicesimplifiessuturingbyeliminatingknot-tyingandsuturemanagement in open, robotic and laparoscopic procedures.

72 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
IPEG 2009 ExhibitorsMICROLINE PENTAX, INC. #637800CummingsCenter,Suite166TBeverly,MA01915Tel:978-922-9810 Fax:978-922-9209Website:www.microlinepentax.com
Microline-Pentaxmanufacturesinnovativelaparoscopicreposable instruments bringing together the best in cutting, dissecting,grasping,cauterizingandligating:ReNew™universalreusablehandpiecewithdisposabletips;ClipAppliers:GeminiLargeandM/L-10reusablemulti-firewithdisposableclipcartridges;Visu-Loc™5mmfullydisposable.
MICROMEDICS #6381270EaganIndustrialRoadSt.Paul,55121Tel:800-624-5662 Fax:651-452-1787Website:www.micromedics.com
FibriJet®BiomaterialsApplicatorsallowcontrolledapplicationof single or dual component biomaterials; six syringe sizes and various tip designs facilitate the precise placement of biomaterials(suchasthrombin,plateletgel,tissuesealants)forgeneral, gastrointestinal, endoscopic and minimally invasive surgery.
MINNESOTA MEDICAL DEVELOPMENT, INC #9361430521stAvenueNorthPlymouth,MN55447Tel:763-354-7105 Fax:763-354-7101Website:www.2mdinc.com
TheReboundHRD™isaself-expandingNitinolframedherniarepair device designed for the laparoscopic repair of both inguinalandventralhernias.Thesuper-elasticNitinolframeallows the device to be folded and inserted laparoscopically. Oncedeployed,thedevicefullyunfurlsor“rebounds”backtoitsoriginalshape–readyforquickandeasyplacementoverthehernia defect.
MOSS TUBES INC. #6431929 Route 9Castleton,Ny12033Tel:800-827-0470 Fax:518-674-8067Website:www.mosstubesinc.com
Since1986MossTubesInc.hasmanufacturedthemostefficientfeeding/decompressiontubesavailable.Immediatefeedingwithdecompression allows for faster recovery and greater patient comfort.TheyareavailableindividuallyorinaPercutaneousEndoscopicGastrostomyKit.
NASHVILLE SURGICAL INSTRUMENTS #9062005 Kumar LaneSpringfield,TN37172Tel:615-382-4996 Fax:615-382-4199Website:www.NashvilleSurg.com
KumarPRE-VIEW*CholangiographyClampandKumarPRE-VIEW*CholangiographyCathetersallowCysticDuctMarkingtoPreventCommonBileDuctInjury.ThereisNoCysticDuctCannulation!KumarT-ANCHORS*HerniaSetallowseasyHerniaMesh Fixation by eliminating the need to grasp and feed sutures withSuturePasser.
*TrademarkandPatent
NDS SURGICAL IMAGING #10075750HellyerAvenueSanJose,CA95138Tel:408-776-0085 Fax:408-776-9878Website:http://www.ndssi.com
NDSSurgicalImaging(NDSsi)deliversvisualizationsystemsthatenableimaginginformaticsforsurgicalandPACSmarkets.NDSsiproducts have revolutionized medical imaging applications globallyforover12years.NDSsiisaprivatelyheldcompanywithpresence in more than 35 countries.
NEW WAVE SURGICAL #533CoralSpringsCorporatePark,Suite1353700N.W.124thAvenueCoralSprings,Florida33065Tel:866-346-8883 Fax:866-586-6793Website:www.newwavesurgical.com
NewWaveSurgicalofferscutting-edgedevicesthatincreasethesafety and efficiency of laparoscopic surgery.
NOVADAQ TECHNOLOGIES #8412585SkymarkAvenue,Suite306,Mississauga,Ontario,Canada,L4W4L5Tel:905-629-3822Website:www.novadaq.com
NovadaqTechnologiesmarketsfluorescenceimagingsystemsdesigned to improve outcomes of complex surgical procedures. Novadaq’sSPyscopeSystemenablessurgeonstosimultaneouslyobserveHDvisuallightandreal-timefluorescenceimagesofbloodflowinvesselsandtissueperfusionduringendoscopicprocedures.
NOVARE SURGICAL SYSTEMS, INC. #92710440BubbRoad,SuiteACupertino,CA95014Tel:877-668-2730 Fax:4088733168Website:www.novaresurgical.com
RealHand®HighDexterity(HD)InstrumentscontinuetoadvanceminimallyinvasivesurgeryincludingapplicationsinSinglePortSurgeryandNOTES.RealHanddeliversgreaterdexterityandsurgical control with 7 degrees of freedom of movement and tactilefeedbackinconvenienthand-heldinstruments.
Olympus-Gyrus ACMI #7273500CorporateParkwayCenterValley,PA18034Tel:800-548-5515 Fax:800-833-1482Website:www.olympussurgical.com
Whileoptimizingclinicalcareandfinancialoutcomes,OlympusandGyrusACMI,leadingsuppliersofmedicalvisualizationandenergysystems,deliversthebest-in-classtissuemanagementandminimally invasive, ergonomically designed surgical endoscopy equipment with outstanding optics for you and your patients.

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 73
IPEG 2009 ExhibitorsPADT MEDICAL #8457755S.ResearchDrive,Suite110Tempe,Arizona85284Tel:480-813-4884 Fax:480-813-4807Website:www.padtinc.com
PADTMedicalhelpsemergingmedicaldevicecompaniesthatarecommercializing new products and need funding support and outsideengineeringexpertise.Weprovideservicesthatenableinnovators to achieve design goals, implement manugacturing, andtaketheirconceptstomarket.Weenablereducedtime-to-marketbyutilizingcomputersimulationandrapidprototypetestingtoquicklyconvergeoninnovativedesignsolutions.PADTMedicalisdedicatedtoEngineeringyourMedicalDeviceInnovations.
PAJUNK MEDICAL SYSTEMS #8375126SouthRoyalAtlantaDriveTucker,GA30084 Tel:770-493-6832 Fax:770-934-3384Website:www.pajunk.com
AstrongcommitmenttoinnovationandreliabilityhasenabledPAJUNK®tobecomeoneofthemosttrustedcompaniesservingaworld-widemarket.FeaturingLapVision,analternativemethod for diagnostic laparoscopy, using local anesthesia and a balloon-system.Providingclearimageswithoutinsuflation.
PARÉ SURGICAL INC. #8017332S.AltonWay,SuiteHCentennial,CO80112Tel:303-689-0187 Fax:303-689-0579Website:www.PareSurgical.com
PARE’srecognizedandprovensuturingtechnologyutilizesbothstraight and curved needles with reusable and disposable closure devicesthatdeliverapre-tiedlockingRoederknotforsecuretissueapproximationinadvancedLaparoscopic,SinglePortandFlexibleEndoscopicprocedures.TheQuik-Stitch®isasimpleand secure method for gastric band placement as well as gastric bypass,especiallyforover-sewingstaplelines.Sinceitdoesnotrequiretriangulation,theQuik-Stitch®isidealforallSinglePortProcedures.InFlexibleEndoscopicProcedures,thegi-Stitch™readily achieves serosa to serosa tissue penetration to tighten the dilated stoma of a gastric bypass.
PATTON SURGICAL #7446300BridgepointParkwayBuildingTwo,Suite420Austin,TX78730Tel:512-329-0469 Fax:512-328-9113Website:www.pattonsurgical.com
PattonSurgicalimprovespatientcarethroughadvancementsinsurgicalinstrumentation.ThePassPort®Double-ShieldedTrocaris endorsed by renowned laparoscopic surgeons for providing superiorprotectionandcontrol,drasticallyreducingtheriskofcatastrophic vessel and organ injury associated with laparoscopic procedures.
PRACTICE PARTNERS IN HEALTHCARE, INC. #8022ChaseCorporateDrive,Suite15Birmingham,AL35244Tel:205-824-6250 Fax:205-824-6251Website:www.practicepartners.org
PracticePartnersinHealthcareisanASCdevelopmentandmanagementcompany,bringingsuccess-provenmanagementexpertise, enhancing the clinical and financial aspects of the operations.PPHacquiresminorityequitypositionallowingthepartnership to capitalize on existing value and maintain control.
PROSURGICS INC. #43710121MillerAvenue,Suite205Cupertino,CA95014Tel:1-877-ROBOT11Website:www.freehandsurgeon.com
TheFreeHandRoboticCameraControlleristhefirstofProsurgics’newgenerationofaffordablesurgicalrobotics.FreeHand is your most dependable laparoscopic assistant, helping you achieve new levels of efficiency and patient throughput.Takingonlymomentstosetup,FreeHandgivesyousimpleanddirecthead-movementcontrolofscopeposition.Nowyoucanbenefitfromtremor-freevisualizationofunparalleled clarity, no matter how long the procedure.
RG MEDICAL USA / MAHE INTERNATIONAL, INC. #1020468CraigheadStreetNashville, TN 37204 Tel:615-269-7256 Fax:615-269-4605Website:www.rgmedical.com
RGMedicalUSA,Inc.specializesinawidevarietyofequipment,instrumentsandancillaryproductsforArthroscopy,Bronchoscopy,Cystoscopy,Hysteroscopy,Laparoscopy,Laryngoscopy,Resectoscopy,andSinuscopy.Theproductlineincludesrigidandflexibleendoscopes,videosystems,surgicalinstruments and disposables
RICHARD WOLF MEDICAL INSTRUMENTS #631, 1107353CorporateWoodsParkwayVernonHills,IL60061Phone:847.913.1113Fax:847.913.6959Website:www.richardwolfusa.com
RichardWolfMedicalInstruments(RWMIC)manufacturesanddistributeslaparoscopicandthoracoscopicinstruments.RWMICalsomanufacturesscopes,insufflatorsandacompletelineof instruments and optics designed specifically for bariatric andcolorectalsurgery.RWMICofferstheonlystereoscopeonthemarket,designedspecificallyforTransanalEndoscopicMicrosurgery.
SALIX PHARMACEUTICALS, INC #7421700PerimeterParkDriveMorrisville,NC27560Tel:919-862-1000 Fax:919-862-1095Website:www.salix.com
SalixPharmaceuticals,Inc.followsacompetitivestrategyofin-licensinglate-stagepharmaceuticalproductstotreatGIdiseases.TheSalixportfolioincludesAPRISO™COLAZAL®,XIFAXAN®,OsmoPrep®,MOVIPREP®,AZASAN®,ANUSOL-HC®,PROCTOCORT®,PEPCID®OralSuspension,andDIURIL®OralSuspension.
SANDHILL SCIENTIFIC #8069150CommerceCenterCircle#500HighlandsRanch,CO80129Tel:303-470-7020Toll-Free:800-468-4556Fax:303-470-2975Website:www.sandhillsci.com
SandhillScientific,aworldleaderinGIdiagnosticsfor25years,providesTotalRefluxMonitoringtohelpquantifyacidandnon-acidrefluxactivityandproducecomprehensivesymptomassociationdatawiththeintroductionoftheZepHr™Systemwith(Z)technology.

74 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
IPEG 2009 ExhibitorsSIERRA SCIENTIFIC INSTRUMENTS, INC. #9175757W.CenturyBlvd.Suite660LosAngeles,CA90045 Tel:866-641-8492 Fax:310-872-5558Website:www.sierrainst.com
SSIproducesHigh-Resolutionsolid-statemanometrysystemsforgastrointestinalmotilitystudy.OurManoScan360™dramatically simplifies clinical procedures and provides intuitive pressure images that reveal diagnostically significant conditions notseenwithconventionalmanometry.TheManoScan360™isnowupgradeabletoHigh-ResolutionManometrywithImpedance.AlsoavailablearethenewAccuTrac™pH&Impedancemonitoringsystems,ManoShielddisposablecathetersheaths for both esophageal and anorectal catheters, and small diameteradultandpediatricsolid-statecatheters.
SILIMED #1045(Silicone&InstrumentalMedicalCenter&HospitalLTDA)FigueiredoRochaStreet,374-VigárioGeralRioDeJaneiro21.240-660-BrazilTel:55(21)3687-7000Fax:55(21)3687-7140Website:www.silimed.com.br
SilimedisthefirstandonlycompanythatmanufacturessiliconeimplantsinLatinAmericaandranksthirdintheworldranking.Ourlineofproductsforaestheticandreparatorypurposesisthemostwide-ranginganddiversifiedinthemarketandtheonlyonethatshowstheserialnumberoneachproduct manufactured, thus assuring 100% security in product traceability since its manufacturing.
SIMBIONIX USA CORP. #101411000CedarAvenue,Suite210Cleveland,OH44106Tel:216-229-2040 Fax:216-229-2070Website:www.simbionix.com
Simbionixisagloballeaderinmedicalsimulationandeducationtechnologies.SimbionixLAPMentor™andGIMentor™provideadvancedsimulationexperienceofcompleteMISprocedures.SimbionixiscurrentlydevelopingtheSAGESFundamentalsofEndoscopicSurgery(FES)TrainingandAssessmentProgram.
SONY ELECTRONICS, INC. #7431SonyDriveParkRidge,NJ07656Tel:201-930-1000Website:www.sony.com/medical
SonyElectronicsisaleadingproviderofinnovativemedicalimagingproducts.OurofferingsincludeHighDefinitioncameras,displays,capturesystemsandprinters.Sony’smedicalgroupisrecognizedforitscommitmenttofine-tuningitsproducts to meet the demands for healthcare professionals.
SPECIALTY SURGICAL INSTRUMENTATION (SSI) #938ADivisionofSyMMETRyMEDICAL,INC.200RiverHillsDriveNashville, TN 37210Tel:800-251-3000 Fax:615-883-9107www.ssiultra.com
SpecialtySurgicalInstrumentation(SSI)(DivisionofSymmetryMedical,Inc.)isproudtocarrythefulllineofACCESSSurgicalLaparoscopicInstruments.SSIwillfeaturetheNewACCESSSurgicalParallelJawGrasperalongwiththeJonesGastricBanding&BypassInstruments.
STARION INSTRUMENTS #737775PalomarAvenueSunnyvale,CA94085Tel:800-STARION(800-782-7466)Fax:408-522-5201Website:www.starioninstruments.com
Starion’sthirdgenerationThermalLigatingShears(TLS3)utilizesourproprietaryTissueWeldingtechnology,whichfocusesthermal energy to simultaneously seal and divide tissue while minimizing collateral damage. The ability to grasp and dissect soft tissue, as well as seal and divide, reduces the need for instrument exchange.
STRYKER ENDOSCOPY #5015900OpticalCourtSanJose,CA95138Tel:800-624-4422 Fax:800-729-2917Website:www.stryker.com
StrykerCorporationisoneoftheworld’sleadingmedicaltechnologycompanieswiththemostbroadly-basedrangeofproducts in orthopaedics and a significant presence in other medical specialties.
SURGICAL PRODUCTS MAGAZINE #804AdvantageBusinessMedia100EnterpriseDr.Ste.600Rockaway,NJ07866Tel:(973)920-7000Website:www.surgicalproductsmag.com
SurgicalProducts,amonthlyproductnewsmagazine,istheleading source of new product information to 60,000 surgeons and other medical and purchasing professionals in hospitals and surgi-centersacrossthecountry.SurgicalProductsmagazineisavailable in both hard and digital editions. The publication is also complemented by a stable of online offerings including a monthlye-newsletter,e-productshowcaseandcustom-designed,audience-directedE-Marketingblasts.
SURGICAL SCIENCE INC. #838206CrestmoorCircleSilverSpring,MD20901Tel:301.219.5159 Fax:866.428.9242Website:www.surgical-science.com
SurgicalScienceiscommittedtodevelopingcutting-edgesimulationtoolsthathelptrain‘SaferSurgeonsFaster’.OurvalidatedLapSim®systemhasshowntobuildskillsthatactuallytransferintotheoperatingroom.Pleasevisitbooth#838toexperienceLapSimandtheSimPraxis®CognitiveInteractiveSimulationTrainer!
SURGIQUEST, INC. #52712CascadeBoulevard,Suite2BOrange,CT06477Tel:203-799-2400 Fax:203-799-2401Website:www.surgiquest.com
SurgiQuest’sAirSeal™platformfacilitatesanunprecedenteddegree of operative freedom and superior visualization. The AirSealaccessporthasnointernalsealsorgaskets,therebyproviding unobstructed abdominal access and unimpeded specimenremoval.Nomorescopefogging.SurgiQuest’sAirSealSystemevacuatessmokeautomatically.

IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org 75
IPEG 2009 ExhibitorsSUTURTEK INCORPORATED #101351MiddlesexStreetNorthChelmsford,MA01863Tel:978-251-8088 Fax:978-251-8585Website:www.suturtek.com
SuturTekEndo360°MinimallyInvasiveSuturingDevicesenablelaparoscopicsurgeonstoeasilyandquicklyplacerunningorinterruptedstitchesandtieintracorporealknotsusingstandardtechnique, standard curved needles, and standard sizes and typesofsutures.Cost-effectivereusableprecisionstainlesssteelinstruments save hospitals hundreds of dollars in every case as comparedtocostlysingle-usedisposableplasticdevices.
SYNAPSE BIOMEDICAL INC. #532300ArtinoStreetOberlin,OH44074Tel:440-774-2488 Fax:440-774-2572Website: www.synapsebiomedical.com
SynapseBiomedicalInc.,aneurostimulationcompany,marketstheNeuRxDiaphragmPacingSystem(DPS)™.Thesystemisdesigned for laparoscopic implantation to address respiratory insufficiency or chronic ventilator dependency in high spinal cord injuryandALS(LouGehrig’sdisease)patients.
SYNOVIS SURGICAL INNOVATIONS #9112575UniversityAvenueWStPaulMN55114Tel:1-800-255-4018 Fax:1-651-642-9018Website:www.synovissurgical.com
SynovisSurgicalInnovations,adivisionofSynovisLifeTechnologies,Inc.,willfeatureVeritas®CollagenMatrix,aremodelablebiomaterial,forsofttissuerepairs.SynoviswillalsodisplayPeri-StripsDry®withVeritas®CollagenMatrix,itsremodelable circular and linear staple line reinforcement, for gastric, small bowel and mesentery applications.
TEI BIOSCIENCES #9407ElkinsStreetBoston,MA02127Tel:866-524-0022 Fax:888-623-2259Website:www.teibio.com
Aleadingbiomedicalcompany,TEIBiosceincesInc.hasappliedits expertise in regenerative medicine to develop novel biological products for a broad spectrum of soft tissue repair andreinforcementapplications-dura,tendon,herniarepairandplastic surgery.
USGI MEDICAL #937 1140CalleCordilleraSanClemente,CA92673Phone:(949)-369-3890 Fax:(949)369-3891Website:www.usgimedical.com
USGIMedicaliscommittedtothedevelopmentoftechnologiestoenableIncisionlessSurgeryforthetreatmentofdiseases.USGI’sEndoSurgicalOperatingSystem™providessurgeonstheoperating platform and specialized tools to perform surgery throughapatient’snaturalorifices.
V. MUELLER® AND SNOWDEN-PENCER® PRODUCTS #10011430WaukeganRoadMcGawPark,IL60085Tel:10800-323-9088www.cardinal.com/snowdenpencer
V.Mueller®andSnowden-Pencer®instrumentationincludesafulllineoflaparoscopicinstruments,withreusable,take-apartandreposableproductsolutions.GetagriponcomfortwiththeergonomicdesignofthenewDiamond-Line®instruments.Also,achieveflexibilitywithourarticulatinginstruments.
Ourintegratedapproachtoinstrumentation,FullCircleInstrumentation™,meansthatweareyoursourceforthepeople, selection, craftsmanship and solutions that encompass all of your instrumentation needs.

76 IPEG 18th Annual Congress for Endosurgery in Children | April 21 - 25, 2009 | www.ipeg.org
Long Term Research Fund Individual Contributors
$1,000 and AboveThomE.Lobe,MD
$300 and AboveJulioJustoBaez,MDCarrollM.Harmon,MD,PhDThomasH.Inge,MD,PhDMarcA.Levitt,MDStevenRothenberg,MDHolgerTill,MDVictorValda,MDAtsuyukiyamataka,MD
$100 to $300Taya Alami,MDMariArai,MDMarianaBachmannDeSantos,MDBehrouzBanieghbal,MDDouglasC.Barnhart,MDSimonA.Clarke,FRCSGiovanniCobellis,MDBenjaminDelRioHernandez,MDTakaoFujimoto,MD,PhDCharlesGoudie,MDMuntherJ.Haddad,MDGeorgeW.HolcombIII,MDAndrewJ.A.Holland,PhDTadashiIwanaka,MD,PhDTimothyD.Kane,MDSimonKenny,MDToanKhuc,MDVladamirKotlobovsky,MDMasashiKurobe,MDVinhT.Lam,MDColinLazarus,MDMaryH.Li,MDFrancoisI.Luks,MDGordonA.MacKinlay,MD,FRCSMarceloMartinezFerro,MDThomasMcGill,MDElizabethJ.McLeod,MDOliverJ.Muenster,MDAzadNajmaldin,MD,FRCSPeterF.Nichol,MDDanielJ.Ostlie,MDDariuszPatkowski,MDJoseL.PeiroIbanez,MDBhaskarN.Rao,MDMasahitoSato,MDJuergenSchleef,MDOsamuSegawa,MDJeong-MeenSeo,MDHeribertoL.Solano,MDJoséSousa,MDNorioSuzuki,MDRichardG.Weiss,MDC.K.yeung,MDJeffreyZitsman,MD
$50 to $100HosseinAllal,MDLindaABaker,MDKlaasMABax,MD,PhDFranciscoJoseBerchiGarcia,MDMarcosBettolli,MDPeterBorzi,MDTimJ.Bradnock,MBChBIoanaBratu,MDJuanI.Camps,MDA.AlfredChahine,MD
KelvinL.Choo,MD,FRACSRalphC.Cohen,ProfJean-FrancoisColombani,MDJohnConnor,MDCatherineM.Cosentino,MDSherifG.Emil,MDWalidA.Farhat,MDJoaoM.B.Fonseca,MDPiergiorgioGamba,MDCarlosGarcía-Hernández,MDB.J.Hancock,MDGretchenPurcellJackson,MD,PhDSaundraKay,MDAlfredP.Kennedy,MDDae-yeonKim,MDyoshihiroKitano,MDMasayukiKubota,MDJean-MartinLaberge,MDClemens-MagnusMeier,MDMarioMendoza-Sagaon,MDAntonioMessineo,ProfJorgeMogilner,MDFraserD.Munro,MDSadasivamMuthurajan,MDHollyL.Neville,MDGustavoNunez,MDElizabethC.Pohlson,MDMarkPowis,MDRahaminR.Pretto,MDMarioA.Riquelme,MDMaryC.Santos,MDKlausSchaarschmidt,ProfHidekiSoh,MDRichardJ.Stewart,MDHenriSteyaert,MDGerhardStuhldreier,MDDouglasy.Tamura,MDBurakTander,MDKristineJaneThayer,MDBennoUre,MD,PhDJean-StephaneValla,ProfDavidC.vanderZee,MD,PhDMartinVanNiekerk,MDRavindraVegunta,MDSuzanneM.yoder,MD
$25 IvanAlcoholado,MDAayedR.Al-Qahtani,MDGabrielaAmbriz-Gonzalez,MDThomasBaesl,MDMariaMarcelaBailez,MDTahminaBanu,MDKatherineA.Barsness,MDRaimundoBeltraPico,MDThaneA.Blinman,MDChristopherJ.Bourke,MDBrendonBowkett,MDCharlesW.Breaux,MD,FACSNancyT.Browne,RN,MS,CPNPMarceloCalcagnoSilva,MDKarenC.Cartwright,MDSteveC.Chen,MDSalvatoreFabioChiarenza,MDLarsJ.Cisek,MDZahaviCohen,MDC.EricColn,MDMauricioCopete-Ortíz,MDJoseC.Cortez,MDRichardA.Courtney,MD
JosephCrameri,MDJosephI.Curry,MD,FRCSRobertCywes,MD,PhDPiotrS.Czauderna,MDMarc-HenriDeLaet,MDJamesM.DeCou,MDMariaRitaDiPace,MDKarenA.Diefenbach,MDAnthonyDilley,MDStevenDocimo,MDMartinDuebbers,MDArnisEngelis,PhDJamesW.EubanksIII,MDRichardA.FalconeJr,MDKenFalterman,MDVictorF.Garcia,MDKeithE.Georgeson,MDJustinGerstle,MDChristopherA.Gitzelmann,MDJamesGlasser,MDWojciechGorecki,MDJonathanI.Greenfeld,MDMiguelGuelfand,MDMohanSahebGundeti,MS,FRCSAnnaGunnarsdóttir,MDJamesK.M.Hamill,MDWilliamHardin,MDDanielH.Hechtman,MDHollyL.Hedrick,MDyvesHeloury,MDAmbrosioHernandez,MDCelesteHollands,MDAndrewRHong,MDJeffreyHorwitz,MDOlajireIdowu,MDSvetlanaV.Ionouchene,MDTetsuyaIshimaru,MDGirishJawaheer,MDMichaelJosephs,MDCarlosEduardoR.Junqueira,MDMichelJuricic,MDEdwardM.Kiely,MDHiroakiKomuro,MDKeithA.Kuenzler,MDJacobC.Langer,MDHubertLardy,MDyi-HorngLee,MDThomasS.Lendvay,MDToniLerut,MDPierreLingier,MDHannuT.Lintula,MDDeborahLoeff,MDMaurícioMacedo,PhDAtulK.Madan,MDAniesA.Mahomed,Mr.LucianoMastroianni,MDPeterMattei,MDDavidP.MeagherJr,MDJanetMeller,MDRobertK.Minkes,MD,PhDJesusD.Miranavarro,MDPhilippeMontupet,MDKevinP.Moriarty,MDPhilipN.Morreau,MDVolkerMueller,MDBommayyaNarayanaswamy,MDNamXuanNguyen,MDMichaelGlennNightingale,MBChBMasakiNio,MDDavidM.Notrica,MD
AlpNumanoglu,MDAnnO’Connor,MDSumiOlinski,MDMatthijsW.N.Oomen,MDAlejandraM.Parilli,MDJateenC.Patel,MDCarlosA.H.Peterson,MDPaulPhilippe,MDJ.DuncanPhillips,MDAgostinoPierro,ProfGuillaumePodevin,MDToddA.Ponsky,MDWilliamP.Potsic,MDD.DeanPotter,MDDavidM.Powell,MDRajeevPrasad,MDPremPuri,ProfHoracioA.Questa,MDTroyM.Reyna,MDDanielJ.Robertson,MDFrankM.Robertson,MD,FACSBradleyRodgers,MDDavidH.Rothstein,MDJanRutqvist,MDHananMohamedAhmedSais,MDJulianAlbertoSaldanaCortes,MDRicardoV.SantanaRamirez,MDRadhakrishnanSatheesan,MDUlrkeSchaarschmidt,MDMarcSchlatter,MDRobertSchlechter,MDMaxC.Schlobach,MDAkihiroShimotakahara,PhDEdwardShlasko,MDAlbertShun,MDSVSoundappan,TroyL.Spilde,MDWilliamW.Spurbeck,MDShawnD.StPeter,MDAmyB.Stanfill,MDHenrikSteinbrecher,MDMarshallM.Stone,MD,FACSGustavoStringel,MDWendyT.Su,MDMakotoSuzuki,MDBarbaraTadini,MDHirooTakehara,DOyukHimTam,MDTakemaruTanimizu,MDDavidTashjian,MDLesliTaylor,MDRejuJ.Thomas,MDBaranTokar,MDDaisyVieiraTravassos,MDJuanPabloValdivieso,MDRobertineVanBaren,MDFrancoisVarlet,PhDGeorgeM.Wadie,MDChristopherB.Weldon,MDHollyL.Williams,MD,FACSGuinevaJPWilson,MDAndrewL.Wong,MDKennethK.Wong,MDSimonK.Wright,MDMarkL.Wulkan,MDAydinyagmurlu,MDDaniyardeni,MD

Inside Back Cover Ad

April 21 - 25, 2009Phoenix Convention Center, Phoenix, Arizona
18th Annual Congress for Endosurgery in Children
2009 Surgical Spring Week
International Pediatric Endosurgery Group (IPEG)
11300 W. Olympic Blvd., Suite 600 Los Angeles, CA 90064Phone: 310-437-0553 Fax: 310-437-0585 Website: www.ipeg.org
IPEG Corporate Supporters
DIAMOND DONORS
KARL STORZ ENDOSCOPY-AMERICA
STRYKER ENDOSCOPY
PLATINUM DONORSCOVIDIEN
GOLD DONORSCHILDREN’S MERCY HOSPITALS AND CLINICS
BRONZE DONORSCHILDREN’S HOSPITAL CINCINNATI
ETHICON ENDO-SuRgERy, INC.
International Pediatric Endosurgery group