Embed Size (px)
Citation preview

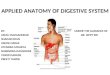
APPLIED ANATOMY OF DIGESTIVE SYSTEM
BY- UNDER THE GUIDANCE OFASMA MAZGAONKAR DR. SIPPY SIRSHADAB KHANASHISH UBALEJITENDRA MOURYANARENDRA DAUNDKARVINOD DARADEPREETI TAWDE

Ludwig's Angina
• Is a skin infection that occurs on the floor of the mouth, underneath the tongue.
• Complications can be life threatening.
Causes:-• Ludwig’s angina is a bacterial infection. It is usually caused by
the bacterium Streptococcus or Staphylococcus and often follows a mouth injury or infection such as a tooth abscess.
• Poor dental hygiene, lacerations in the mouth or a recent tooth extraction.

Symptoms:- Ludwig’s angina often follows a tooth infection or other infection or injury in the mouth.
Symptoms include:• pain in the floor of your mouth• problems with speech• neck pain• swelling of the neck• redness on the neck• weakness, fatigue• earache• swollen tongue pushing against your palate• fever, chills

Diagnosis:-• Physical exam:-Head, neck and tongue will appear red and
swollen.• Imaging tests:-Contrast-enhanced magnetic resonance
imaging (MRI) or computed tomography (CT) images.• Fluid cultures :-Fluid from the affected area may tested to
identify the bacterium.
Complications:-• Blocked airway.• Sepsis (a severe reaction to bacteria or other germs)• Septic shock(infection that leads to dangerously low blood
pressure).

Treatment:-• Blocked airway
- Insert a breathing tube through your nose or mouth into your lungs.
- Tracheotomy.• Surgery.• Antibiotics.
Prevention:-• Practicing good oral hygiene.• Having regular dental checkups.• Seeking prompt treatment for tooth and mouth infections.

Oral Mucositis• Oral Mucositis (OM) refers to an inflammatory, erosive and
ulcerative process inside the mouth, which is usually caused by radiation or chemotherapy.
Causes:-• Side effect of cancer treatment. Increased risk:-• Smoking.• Drinking alcohol.• Eating spicy foods.• Dehydration.• Dry mouth–is another side effect of radiotherapy and
chemotherapy.• Receiving a higher dose of chemotherapy.

Symptoms:-The symptoms of oral Mucositis usually begin five to 10 days after starting chemotherapy or 14 days after starting radiotherapy.
• Burnt sensation while eating very hot food. • Develop white patches or ulcers on the lining of mouth, on
tongue and around lips.• Red and inflamed oral mucosa. • Ulcerations may cause severe pain.
Conditions look like Oral Mucositis:-• Candidiasis (oral thrush);• Herpes simplex virus (HSV); and• Graft-versus-host disease (GVHD).

Diagnosis:-• Examining your mouth.• Diagnosis symptoms of pain.• Checking ability to eat and drink properly.
Complications:-• Severe pain and trouble eating .• Dry mouth.• Alterations in taste that can lead to Anorexia.• Weight loss.• Weakness due to poor nutrition.• Severe inflammation and injury to the oral mucosa also
increases the chance of other infections in the mouth and body.
• Cause a reduction in dose of treatment.

Treatment• Self-care- Avoid tobacco, alcohol and hot & spicy foods.- Drink plenty of fluids.• Palifermin is given by injection which encourages the growth
of new cells on the lining of the mucous membrane.

Adenoiditis• Adenoiditis is an inflammation of
the adenoids. • Adenoids are masses of lymph
tissue that help the body fight infection.
• Adenoids are found in the pharynx (throat) just behind the nose and are the first line of defense in your throat.
Causes:-• Adenoiditis can be caused by a
bacterial infection, such as Streptococcus, or by viruses such as the Epstein-Barr virus.

Risk:- Certain risk factors are:• Recurring infections in the throat, neck, or head.• Infections of the tonsils.• Contact with airborne viruses, germs and bacteria.
Symptoms:-. • Difficult to breathe through nose.• Sounding “nasal” when speaking.• Sore or dry throat from breathing through the mouth.• Snoring during the night or any time you sleep.• Signs of infection, such as a runny nose that produces green
or discolored mucus.

Complications :- Complications may chronic or severe inflammation that spread to other locations of the head and neck.
• Ear Infections• Glue Ear• Sinusitis• Infections of the Chest
Diagnosis:-• Physical examination• Throat examinations• Blood tests• X-rays

Treatment:-• Antibiotics• Surgery
Prevention:-• Healthy foods.• Plenty of fluids.

OesophagusCongenital Anomalies
Muscular dysfunctions
Haematemesis of oesophageal origin
Inflammatory Lesions
Tumours of Oesophagus

Congenital Anomalies
Oesophageal Atresia and Tracheo-oesophageal Fistula
1 in 4425 live births.Congenital esophageal atresia (EA) represents a failure of the esophagus to develop as a continuous passage. Instead, it ends as a blind pouch. Tracheoesophageal fistula (TEF) represents an abnormal opening between the trachea and esophagus

Clinical FeaturesHypersalivationRegurgitation of every feedAttacks of coughCyanosis
Death usually results fromAsphyxiaAspiration pneumoniaFluid-electrolyte imbalance
The most immediate and effective treatment in the majority of cases is a surgical repair to close the fistula/s and reconnect the two ends of the esophagus to each other.

OthersAgenesisDuplication of OesophagusStenosis

Musular DysfunctionAchalasia Cardia (Cardiospasm)
Hiatus Hernia
Oesophageal Diverticula
Oesophageal Webs and Rings

Achalasia Cardiaa neuromuscular dysfunction Cardiac sphincter fails to relax during swallowingProgressive dysphagiaDialatation of the oesophagus

Signs and symptomsDysphagia (difficulty in swallowing),Regurgitation of undigested food, Chest pain behind the sternum,Weight loss. Coughing when lying in a horizontal position.Cardiospasm. It can be extremely painful in some sufferers. Food and liquid, including saliva, are retained in the esophagus and may be inhaled into the lungs (aspiration).
Investigations
Barrium swallowEndoscopy

ManagementForceful pneumatic dialatation using a 30-35mm diameter endoscopically postioned balloon disrupts the oesophageal sphincter and improves symptoms in 80% of patients
Endoscopically directed injection of botulinum toxin into the lower oesophageal sphincter induces clinical remission,but late relapse is common.

SurgicalSurgical Myotomy (Heller’s Operation)

Hiatus Hernia Hiatus hernia or hiatal hernia is the protrusion (or herniation) of the upper part of the stomach into the thorax through a tear or weakness in the diaphragm.
ClassificationSliding (Oesophago-Gastric) Hiatus Hernia- 90%Rolling (Paraoesophageal) Hiatus Hernia- 5%Mixed (Transitional) Hiatus Hernia- 5%

EtiologyFailure of the muscle fibres of the diaphragm that forms the margin of the oesophageal hiatus
Short oesophagus
Degenaration of muscle due to aging
Increased intra-abdominal pressure
Recurrent Oesophageal regugitation and spasm causing inflammation and fibrosis
Increase in fatty tissue in obease people causing decreased muscular elasticity of diaphragm

Signs and symptomsHiatal hernia has often been called the "great mimic" because its symptoms can resemble many disorders.
Dull pains in the chest,shortness of breath(caused by the hernia's effect on the diaphragm),
Heart palpitations (due to irritation of the vagus nerve),
Swallowed food "balling up" and causing discomfort in lower esophagus until it passes on to stomach.
Heartburn (retrosternal burning sensation)
Regurgitation of gastric juice into the mouth

Management1.To minimise gastro-oesophageal reflux
Elevate bed head by 20cmAvoid posture precipitating reflux,bending or stooping forwards,sitting in a low chairAvoid large mealNo food or drink for 3-4 hours before bedtimeReduce weight if possibleNo smokingAvoid all non dteridal anti-inflammatory drugsAvoid food which provoke syptoms eg: pastries, coffee
2.Reduce gastric acidity and pepsin secretion(Renitidine,Cimetidine, Famotidine)
3.Increase tone of lower oesophageal sphincterMetoclopramide 10 mg tds

Surgical
Restoration of intra-abdominal segment of oesophagus into abdomen and anchoring it,repairing the hiatus and enveloping the lower oesophagus by gastric fundus.( Nissen fundoplication)
)

Oesophageal DiverticulaCongenital Diverticula(Upper end of the oesophagus or at the bifurcation of the trachea)
Acquired Diverticula
Pulsion (Zenker’s) Type(in the region of hypopharynx)
Traction Type(Occurs in the lower third of oesophagus from contraction of fibrous tissue such as from pleural adhesions,scar tissue of healed tuberculous lesions in the hilum,silicosis etc.

Killiance Dehiscenceis a triangular area in the wall of the pharynx between the thyropharyngeus part of the inferior constrictor of the pharynx and the cricopharyngeus muscle, also of the inferior constrictor muscle of the pharnyx
It represents a potentially weak spot where a pharyngoesophageal diverticulum (Zenker's diverticulum) is more likely to occur.

Oesophageal Webs and Rings
Esophageal webs are thin (2-3mm) membranes of normal esophageal tissue consisting of mucosa and submucosa that can partially protrude/obstruct the esophagus.
A Schatzki ring or Schatzki-Gary ring
is a narrowing of the lower part of the esophagus that can causedifficulty swallowing (dysphagia). The narrowing is caused by a ring of mucosal tissue (which lines the esophagus) or muscular tissue.

Heamatemesis Of Oesophageal OriginVomiting Of Blood
1.Oesophageal Varices2.Mallory- Weiss Syndrome3.Rupture Of The Oesophagus
4. Other CausesBursting of aortic aneurysm into the lumen of oesophagusOesophageal CancerPurpurasHeamophiliaZollinger-EllisonDisease

Inflammatory LesionsOesophagitisReflux of the gastric juice is the commonest cause of oesophagitis

Barrett’s Oesophagus
Infective Oesophagitis
Other Causes of oesophagitisIntake of certain drugsIngestion of hot, irritating fluidsRadiationCrohn’s disease

PEPTIC ULCER• Peptic ulcer disease refers to painful sores or ulcers in the lining of
the stomach or first part of the small intestine, called the duodenum.
CAUSES OF PEPTIC ULCER• ulcer is the end result of an imbalance between digestive fluids in
the stomach and duodenum. Ulcers can be caused by:• Infection with a type of bacteria called Helicobacter pylori (H.
pylori)• Use of painkillers called no steroidal anti-inflammatory drugs
(NSAIDs), such as aspirin, naproxen (Aleve, Anaprox, Naprosyn, and others), ibuprofen (Motrin, Advil, Midol, and others), and many others available by prescription. Even safety-coated aspirin and aspirin in powered form can frequently cause ulcers.
• Excess acid production from gastrinomas, tumors of the acid producing cells of the stomach that increases acid output

Symptoms of peptic ulcer
• Bloating• Heart Burn• Vomiting blood (that can look like "coffee-grounds")• Severe pain in the mid to upper abdomen

TREATMENT AND DIAGNOSIS
DIAGNOSIS:The diagnosis of an ulcer is made by either a barium upper
gastrointestinal X-ray (Upper GI series) or an Upper GI endoscopy
Treatment:• The goal of ulcer treatment is to relieve pain, heal the ulcer,
and prevent complications. .• The first step in treatment involves the reduction of risk
factors (NSAIDs and cigarettes).and second is medications:• Antacids• Proton-pump inhibitors (PPIs)

Gastric ulcer
• A gastric ulcer is a sore in the lining of your stomach. CAUSES:• Upsets in the balance of stomach acid and digestive juices can
lead to an ulcer. This can be caused by:• Helicobacter pylori (H. pylori) infection• NSAIDsRisk Factors:• Taking NSAIDs for a long time and at higher doses• Cigarette smoking• Alcohol abuse

Symptoms:• Gnawing pain• Bloating• Burping• Weight lossDiagnosis: Physical examination
Treatment:Talk to your doctor about the best treatment plan for you. Treatment options may
include one or more of the following:• Medication
• Lifestyle Changes
• Surgery and Endoscopy

Gastritis• Gastritis occurs when the lining of the stomach becomes
inflamed or swollen.• Gastritis can last for only a short time (acute gastritis), or
linger for months to years (chronic gastritis).Causes:• Alcohol abuse• Eating or drinking caustic or corrosive substances (such as
poisons)• Extreme stress• Certain medications, such as aspirin

SYMPTOMS:• Loss of appetite• Nausea and vomiting• Black stoolsDIAGNOSIS:• CBC• H. pylori tests• Stool test to check for small amounts of blood in the stools,
which may be a sign of bleeding in the stomachTREATMENT:MEDICATIONS• Antacids may be used to treat chronic gastritis caused by
infection with Helicobacter pylori bacteria.• H2 antagonists: famotidine (Pepsid), cimetidine

SMALL INTESTINE

Problems with the small intestine can include:
1.Bleeding2.Celiac disease3.Crohn's disease4.Infections5.Intestinal cancer6.Intestinal obstruction7.Irritable bowel syndrome8.Ulcers, such as peptic ulcer

Crohn's diseaseIt causes inflammation of the digestive system. It isone of a group of diseases called inflammatory boweldisease. It most commonly starts between the ages of13 and 30.
Location- Crohn's can affect any areafrom the mouth to the anus.It often affects the ileum.

Causes-The exact cause of Crohn’s disease is unknown.
Most researchers think that it is caused by acombination of factors.1.Genetics2.The immune system3.Smoking4.Previous infection5.Environmental factors

The five types of Crohn's disease-1. Ileocolitis: Most common type of chron’s disease. Affects
the mouth and colon2. Ileitis: affects the ileum3. Gastroduodenal Crohn's disease: Affects the stomach and
duodenum4. Jejunoileitis: affects the jejunum5. Crohn's colitis: Affects only the colon

Symptoms1. Pain in the abdomen2. Diarrhea3. Bleeding from the rectum4. Weight loss5. Fever
Diagnosis-• Barium enema• Colonoscopy• CT scan of the abdomen• Endoscopy• MRI of the abdomen

Complications of Crohn's disease-1.Intestinal blockages2.Ulcers in the intestine3.Problems getting enough nutrients4.Joint pain and skin problems5.Growth problems (in children)
Treatment-There is no cure for Crohn's.Treatment to control symptoms1.Medicines2.Nutrition supplements3.Surgery

Medicines:1. Anti-inflammatory drugs • Sulfasalazine• Mesalamine• Corticosteroids
2. Immune system suppressors • Azathioprine• Remicade• Adalimumab
3. Antibiotics• Metronidazole• Ciprofloxacin

Other medications:1. Anti-diarrheals2. Laxatives3. Pain relievers4. Iron supplements5. Nutrition (special diet given via a feeding tube)6. Vitamin B-12 shots
Surgery: Removes a damaged portion of your digestivetract
Limitations of surgery-1. temporary benefits2. Recurrence of chron’s3. Post surgery medication’s required

Ulcerative colitis

Ulcerative colitis is a disease that causes inflammation and sores, called ulcers, in the lining of the rectum and colon.
The main symptom of active disease is usually constant diarrhea mixed with blood, of gradual onset. It is a form of inflammatory bowel disease (IBD).
Ulcerative colitis is a form of colitis, a disease of the intestine, specifically the large intestine or colon, that includes characteristic ulcers, or open sores, in the colon
INTRODUCTION


SYMPTOMS :-• The most common symptoms of ulcerative colitis are
abdominal pain and bloody diarrhea. Patients also may experience.
• Anemia• Fatigue.• Weight loss• Loss of appetite• Rectal bleeding• Loss of body fluids and nutrients • Skin lesions• Joint pain• Growth failure (specifically in children)

DIAGNOSIS
• Many tests are used to diagnose ulcerative colitis. A physical exam and medical history are usually the first step.
• Blood tests may be done to check for anemia, which could indicate bleeding in the colon or rectum .
• In addition, a stool sample allows the doctor to detect bleeding or infection in the colon or rectum caused by bacteria, a virus, or parasites.

TREATMENT• Drug Therapy:-• AMINO SALICYLATES• CORTICOSTEROIDS• IMMUNO SUPRESSIVE DRUGS• BIOLOGIC TREATMENT • SURGERY• OTHER SURGICAL ALTERNATIVES • DIET• BACTERIAL RE COLONIGATION

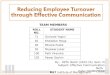
Appendicitis
McBurney’s pointSite of maximum tenderness in appendicitis

HEMORRHOIDS
• Hemorrhoids are swollen and inflamed veins in the anus and lower rectum.
Internal and External Hemorrhoids• Internal hemorrhoids located inside the rectum; • External hemorrhoids develop under the skin around the
anus.


CAUSES
• Too much pressure on the veins in the pelvic and rectal area causes hemorrhoids.
Factors that might cause increased pressure include: • Overweight• Pregnancy• Diarrhea or constipation• Sitting for long periods of time on the toilet• Diet low in fiber or fluids

SIGNS AND SYMPTOMS
• Extreme itching around the anus• Irritation and pain around the anus• Itchy lump located near your anus• Fecal leakage• Painful bowel movement • Blood on your tissue after having a bowel movement

Diagnosis• Digital rectal exam• Sigmoidoscopy
Treatment • Rubber band ligation• Sclerotherapy• Surgery : Hemorrhoidectomy

MEDICATION
• Ointments: as zinc oxide or petroleum jelly• Ointment that contains 1% hydrocortisone• Acetaminophen can help with pain.• Aspirin and other nonsteroidal anti-inflammatory drugs such
as ibuprofen (Motrin) and naproxen (Aleve) can help with pain and swelling.

COMPLICATIONS
• Blood clots within the swollen vein• Bleeding• Iron-deficiency anemia (caused by blood loss)

PREVENTION
• Avoid straining during a bowel movement.• Increase your water intake. Drinking adequate water can
keep your stool from hardening.

Disorders of Tongue• Glossodynia (burning mouth
syndrome)- spontaneous burning, discomfort, pain, irritation, or rawness of the tongue, has no identifiable etiology most of the time
• Etiology- – Idiopathic, Infection,
Allergic/contact hypersensitivity, Mechanical trauma
– Xerostomia, Geographic tongue/ Fissured tongue
– Vesiculobullous disease, temporomandibular dysfunction
– Referred pain from teeth or tonsils
– Drugs- Antibiotics, psychiatric medications, chemotherapy

Glossodynia Treatment
Treatment for burning mouth syndrome varies greatly between cases based on the severity of the symptoms, the underlying cause and the diagnosis of the physician. In many cases the symptoms will be associated with a psychological disorder such as depression and the burning mouth and the underlying cause will be treated together with anti-depressants. In other cases patients can try altering their medication, using different toothpastes, checking their dentures and increasing their consumption of vitamin B12.

Disorders of Tongue…• Macroglossia- congenital or
acquired process, tongue is disproportionately large relative to the patient’s jaw size
• Difficulty with mastication and speech and accidental tongue biting are common
• Differential- Down syndrome, hypothyroidism, Beckwith-Wiedemann syndrome, neurofibromatosis, infection by mycobacteria, filamentous bacteria or fungus, amyloidosis

Macroglossia treatment
Tongue Reduction Surgery
Speech Therapy

DISEASES OF LIVER

• Most common chronic blood-borne infection accounts for 50% of all patients with chronic liver disease in the US
• Flaviviridae family, genus Hepacivirus
• HCV RNA polymerase with poor fidelity inherently unstable (+) genomic instability & antigenic variability within one individual evade IFN-mediated anti-viral response repeated bouts of hepatic damage
Hepatitis C

• Persistent infection and chronic hepatitis are the hallmarks of HCV infection
• MOT: 1. inoculations 2. blood transfusions 3. hemodialysis
4. sexual transmission5. perinatal
Hepatitis C

Hepatitis C Therapy• Interferon Alone < 15%• Interferon/Ribavirin
– 12 months Genotype 1– 6 months Genotype 2 and 3
• Sustained response (Hep C PCR- 6 mos post therapy)– 5-15% monotherapy– 35-40% combo therapy– 45-70% PEG combo therapy
• Must use birth control--teratogenic

What is cirrhosis?
• Cirrhosis is a condition in which the liver slowly deteriorates and malfunctions due to chronic injury. Scar tissue replaces healthy liver tissue, partially blocking the flow of blood through the liver

What causes cirrhosis?
• heavy alcohol consumption• chronic hepatitis C (the most common)• Obesity• Autoimmune inflammation of the liver• Metabolic disorders

What are the symptoms of cirrhosis?
Symptoms are hard to catch in the early stages of the disease. However, as the disease progresses, a person may experience the following symptoms:
• weakness• fatigue• loss of appetite• nausea• vomiting• weight loss• abdominal pain and bloating • itching• spiderlike blood vessels on the skin

Treatment and Prevention
Prevention•Stop drinking alcohol (or don’t start at all)•Limit salt in the diet•Eat a nutritious diet•Get vaccinated for influenza, hepatitis A and B.•Practice safe sexTreatment•Liver transplant•Antibiotics

DESEASES OF GALL BLADDER

Gallstones
Gallstones develop when cholesterol and other substances in the bile form crystals that become hard stones in the gallbladder. The gallbladder is a small sac located just under the liver. Gallstones can form when too much cholesterol is in the bile or when the gallbladder does not empty properly.

Symptoms
• Pain in the RUQ– Most common and typical symptom– May last for a few minutes to several hours– Mostly felt after eating a heavy and high-fat
meal
• Pain under right shoulder when lifting up arms
• Fever, nausea and vomiting • Jaundice (obstruction of the bile duct
passage)• Acute pancreatitis (gallstone enters the duct
leading to pancreas and blocks it)

Diagnosis• Ultrasound
– Most sensitive and specific test for gallstones
• Computerized tomography (CT) scan – May show gallstones or
complications, such as infection and rupture of GB or bile ducts
• Cholescintigraphy (HIDA scan) – Used to diagnose abnormal
contraction of gallbladder or obstruction of bile ducts
• Endoscopic retrograde cholangiopancreatography (ERCP) – Used to locate and remove
stones in bile ducts• Blood tests
– Performed to look for signs of infection, obstruction, pancreatitis, or jaundice

Treatment• Surgery:
Cholecystectomy (gallbladder removal) – 5 - 40% of patients develop
postcholecystectomy syndrome (gastrointestinal distress and persistent pain in the RUQ)
– 20% of patients develop chronic diarrhea
• Two surgical options– Open cholecystectomy– Laparoscopic
cholecystectomy

• Nonsurgical treatment:– Only in special situations
• When a patient has a serious medical condition preventing surgery
• Only for cholesterol stones
– Oral dissolution therapy• Ursodeoxycholic acid - to dissolve cholesterol
gallstones• Months or years of treatment may be necessary
before all stones dissolve
– Contact dissolution therapy • Experimental procedure• Involves injecting a drug directly into the
gallbladder to dissolve cholesterol stones

DIABETES MELLITUS• DM is a group of metabolic diseases in which a person has
high blood sugar, either because the pancreas does not produce enough insulin, or because cells do not respond to the insulin that is produced.
• Types :1. Type 1 DM results from the body's failure to produce insulin.2. Type 2 DM results from insulin resistance, a condition in
which cells fail to use insulin properly, sometimes combined with an absolute insulin deficiency.
3. Gestational diabetes

SYMPTOMS
• Polyuria• Polydypsia• Nocturia• Hyperphagia• Weight loss• Pruritis• Blurred vision• Giddiness• Numbness

Diagnosis• Random blood sugar test• Fasting blood sugar test
Treatment• Metformin - type 2 diabetes• Insulin and other medications e.g. regular insulin ,insulin
isophane.

COMPLICATIONS• Heart Disease• Stroke• Retinopathy• Chronic renal failure• Difficulty in passing urine in adults• Dehydration• Ketosis• Acidosis• Coma • Death

PREVENTION
• Avoid obesity• Quit Smoking• Elevated Cholesterol Level• Lifestyle changes• Appropriate Diet• Regular Exercise• In case of Diabetic patient wear diabetic sock, avoid higher
risk of serious diseases, weight loss, proper medication.

THANK YOU