Embed Size (px)
Citation preview

12/13/2012
1
Subra Kugathasan, MDProfessor of Pediatrics & Human genetics
Marcus Professor of Pediatric Gastroenterology
Emory University & Children’s Healthcare of Atlanta
Evolution of IBD: Research Lessons Learned
I have the following financial relationships to disclose:JanssenUCB
IBD: The Pediatric Burden & the impact of Pediatric IBD research
• 1.2 million people with IBD in the US, estimated 80‐100,000 children with IBD
• About 20‐25% of all IBD is diagnosed during the pediatric age
• Identification of BIOTYPE = Genotype + Phenotype+ Immunotype + Bacteriotype + ??? clearest in pediatric IBD leading to Risk stratification and personalized therapy in IBD.
• The cause of IBD !• Differential diagnosis between CD and UC (colonic disease)
• Limited endoscopic approaches & lack of good small bowel imaging
• Surgery: the only answer to failure of medical therapy (sulfasalazine and steroid)
• Complete lack of studies in the pediatric age group while knowing pediatric disease is different from adult disease?
• Inability to induce long lasting remission (& mucosal healing)
Major Issues in IBD Diagnosis and TherapyPlagued us over the last few decades!
• IBD epidemiology & natural history
• Pediatric disease activity index: PCDAI & PUCAI
• TNF in stool leading to discovery of anti‐TNF as groundbreaking therapy in IBD
• Gene discoveries and therapeutic targets
• Microbiome, diet and intestinal inflammation
• Risk Prognostication in IBD
• Evolution of collaborative research in pediatrics compared to single center/investigator effort
Evolution of IBD:What have we learned in the last 50 years?
Agenda for the talk
Evolution of IBD epidemiology and natural History

12/13/2012
2
Rising Incidence‐global trends
Crohn’s disease Ulcerative Colitis
Molodecky, Gastroenterology, 2012
Worldwide IncidenceCrohn’s disease Ulcerative colitis
Benchimol, Inflamm Bowel Dis, 2011
Rising Incidence, becoming stablein Omstead county, MN
•Incidence rates of CD and UC increased after 1940•Incidence stable recently
Crohn’s disease Ulcerative Colitis
Loftus, Inflamm Bowel Dis, 2007
Incidence: Pediatric IBD
Overall incidence of IBD: 9.5 per 100,000 Incidence stable over last 8 years
Adamiak, Inflamm Bowel Disease, in press 2012
Rising incidence of UC in Korea
Yang S‐K et al, J Gastroenterol Hepatol, 2000
• Incidence in Korea increased 3‐4 decades after North America and Western Europe• Might this be due to “Westernization”?
Incidence in Indian Migrants to UK
Probert CS, et al. Gut, 1992 Jayanthi et al, Quarterly J of Medicine, 1992Carr I, Am Journal of Gastroenterol Yang S, Inflamm Bowel Dis, 2001
IBD incidence in South Asian migrants ≥ Western‐born population

12/13/2012
3
Regional Variation: Crohn’s disease prevalence
200 (192‐209) * 213 (206‐220) * 211 (204‐217) *
180 (174‐186)
Kappelman, Clin Gastroenterol Hepatol, 2007
Evolution of IBD epidemiology and natural History
Research Lessons learned• World-wide increase in IBD
• Globally, IBD is still raising• Incidence stabilized in western countries!• Increasing in developing countries & new
populations – where the research should be targeted!!
Development of Pediatric Disease Activity Indices:
PCDAI & PUCAI
ITEM POINTS
1. Abdominal pain No pain Pain can be ignored Pain cannot be ignored
0 5 10
2. Rectal bleeding None Small amount only in < 50% of stools Small amount with most stools Large amount (>50% of the stool content)
0 10 20 30
3. Stool consistency of most stools Formed Partially formed Completely unformed
0 5 10
4. Number of stools per 24 hours 0-2 3-5 6-8 >8
0 5 10 15
5. Nocturnal bowel movement (any diarrhea episode causing wakening)
No Yes
0 10
6. Activity level No limitation of activity Occasional limitation of activity Severe restricted activity
0 5 10
SUM OF PUCAI (0-85)
The PUCAI
Turner et al; Gastroenterology 2007;133:423‐432
• Abdominal pain (0‐10)• Stools/bleeding (0‐10)• Functioning/well being (0‐10)• Laboratory:
• Hct (0‐5• ESR (0‐5)• Albumin (0‐10)
• Weight (0‐10)• Height velocity (z score) (0‐10)• Abdominal exam (0‐10)• Perirectal disease (0‐10)• EIM (0‐10)
The PCDAI
Hyams et al. JPGN 1991;12:439 Turner et al. Gastroenterology 2007;133:423‐432
r=0.78; n=76
Gastroenterology 2007;133:423–432 and unpublished data (DT)
Colonoscopic Score
(0‐15)
PUCAI score
Correlation of the PUCAI with colonoscopy
Studies evaluating the PCDAI & PUCAI in different scenarios
• Inflamm Bowel Dis 2011; 17(8):1726‐30
• JPGN 2011;52: 708–713
• Gut 2010;59(9):1207‐1212
• Gastroenterology 2010;138(7):2282‐2291
• Inflamm Bowel Dis 2010; 16(4):651‐656
• J Clin Epidemiol 2010; 63(1):28‐36
• Clin Gastroenterol Hepatol2009;7(10):1081‐8
• Inflamm Bowel Dis 2009; 15(8):1218‐23
• J Clin Epidemiol 2009;62(4):374‐379
• J Clin Epidemiol 2009;62(7):738‐744
• Gut 2008; 57:331‐338
• Gastroenterology 2007;133:423‐432
• Gastroenterology 2007;132:863‐73
(Pediatric Infliximab trial)
• Gastroenterology 2012;143:365‐74
(Pediatric Adalilumab trial)
• J Pediatr Gastroenterol Nutr2007;44:185‐91
(Pediatric Natalizumab trial)

12/13/2012
4
TNF in stool leading to discovery of anti‐TNF as groundbreaking
therapy in IBD
Different anti‐TNF: comparable results(Years 2000 to 2006)
Response† Remission Response‡ Remission Response‡ Remission
27.0
51.0
21.0
39.0
Hanauer SB et al. Lancet. 2002;359:1541–1549.Colombel J et al. Gastroenterology. 2006;131:950.Schreiber S et al. NEJM. 2007;357:239‐50.
Week 26–30
26.0
52.0
17.0
40.0
62.8
36.2
47.9
28.6
Infliximab 5 mg/kg
ACCENT 1n = 113
CHARMn = 172
PRECiSE 2n = 215
Adalimumab 40 mg EOW Certolizumab pegol 400 mg every 4 weeks
Placebo Placebo Placebo
*
**
***
***
***
***
REACH: Pediatric CD infliximab trialAnti‐TNF therapy is highly efficacious in inducing remission
88
64
33
59 56
24
0102030405060708090
100
Week 10 Week 54 q8 Week 54 q12
Response Remission% of Patients
n = 99 n = 66 n = 29n = 33 n = 17 n = 12
p = 0.002
p < 0.001
Hyams J, et al. Gastro 2007;132:863‐873
Early aggressive biologic therapy induced more mucosal healing than conventional management of Crohn’s disease
(n=26)Early aggressive
(n=23)Conventional therapy
p=0.003
% Patients with m
ucosal healing
73
30
0
100
D’Haens G, et al. Lancet 2008;371:660‐7.
Lichtenstein GR, et al. Gastroenterology 2005;128:862
Anti‐TNF: fewer surgeries and post‐surgical recurrence
100
125 Placebo maintenance (n=99)
Cumulative number of surgeries and procedures
Weeks
Randomization0
25
50
75
2 6 14 22 30 38 46 54
Infliximab 5 mg/kg maintenance (n=96)
RegueiroM, et al. Gastroenterol 2009;136:441‐450.

12/13/2012
5
• 10 year old presented with rectal bleeding, perianal pain
• Growth failure and iron deficiency anemia
• Exam under anesthesia & MRI: recto‐labial fistula and perianal fistulae
• Endoscopy: severe left sided Crohn’s colitis & inflammation
• Induction with ‘top down’ biologic therapy rather than ‘step up’ therapy
Before After
Anti‐TNF: ‘Top down’ Evolution in the initial approach in pediatric IBD Crohn’s disease: therapeutic evolution
1979 SulfasalazineSteroids
1980Antibiotics6‐MP
1993 5‐ASA
1994Budesonide
1995 Methotrexate
1998 Infliximab
2005Second‐
generationbiologicals
Adapted from Rutgeerts PJ. Rev Gastroenterol Disord. 2004;4(suppl 3):S3‐S9.
1980 1990 2000
Steroids vs 6-MP for maintenance of remission in pediatric Crohn’s
30
40
50
60
70
80
90
100
0 50 100 150 200 250 300 350 400 450 500 550 600
Days Since Remission Induction
% o
f P
atie
nts
in
Re
mis
sio
n
P<.007
91%
53%
At baseline, patients received prednisone plus either 6‐MP or placebo. Steroids were tapered after induction of remission.
Markowitz J et al. Gastroenterology. 2000;119:895.
Steroids & 6‐MP
Steroids only
Pediatric CD Registry and Wisconsin population-based cohort study
Time point N % on AZA/
6-MP/MTX
At diagnosis 578 21%
30 days 525 41%
3 months 515 56%
1 year 410 69%
2 years 276 76%
Adamiak et al. Inf lammatory Bowel Diseases 2012 (in press)
Increased time‐dependent exposure to immunomodulators
and anti‐TNF agents in pediatric IBD (2002‐2007)
Markowitz J et al. Clin Gastroenterol Hepatol. 2006;4:1124
Crohn’s disease
Ulcerative colitis
Infliximab: Cumulative Commercial Patient exposure by Indication
PSUR 23: August 24, 2010 – February 23, 2011
Total Patients TreatedWorldwide: 1,537,395
Hepatosplenic T‐cell Lymphoma in Infliximab‐treated Patients: Cumulative Review
• 27 reported/possible cases
– All were reported between 2002 and February 2011
– All patients had reported exposure to azathioprineor 6‐mercaptopurine
– 5 cases with another anti‐TNF‐α antagonist
– 26 confirmed cases reported to be HSTCL, all in IBD (22 CD, 4 UC)
– 23 cases have been fatal
Data on File, Janssen Biotech, Inc.

12/13/2012
6
The therapeutic “pendulum”
2004 – everyoneon combinationtherapy
2008 – everyone onbiologic or Immunomodulatormonotherapy
2012 – more use of combination therapy
Pediatric IBD; impact of HSTCLis HUGE
What we have:Fatal form of lymphoma Large, population-based FDA mandated
registry (DEVELOP -short and long-term) is ongoing.
What we need:More follow upRisk stratification and translational studies
Genetics of IBD and therapeutic targets
Timeline of genetic discoveries in IBD
1988 20011996 2006‐7 2012 beyond2008‐9 2010
Twin studies
Linkage studiesIDB1; IBD2
NOD2IBD5
CD GWASTNFSF15, IL23R;ATG16L1; IRMG;
NKX2.3
1st CD meta‐analysis:30 confirmed CD loci
UC GWAS: IL10, IFNγ, HNF4α Pediatric GWAS: IL27, CAPN10
2nd CD meta‐analysis:71 confirmed CD loci
1st UC meta‐analysis:47 confirmed CD loci99 confirmed IBD loci
Innate Immunity (CD)
• Th17 pathway (IBD)• Autophagy (CD)• Defective barrier
function (UC)
• Fine mapping of existing loci• Missing heritability• Genotype‐phenotype correlation• Metagenetics• Disease biology• Biomarker of disease severity• Pharmacogenomics• Genomic‐based therapeutic targets
Immunochip163 confirmed IBD lociloci overlap with mycobacterial infection.Pathways are shared with host response
Tysk et al. Gut 1988;29:990‐996Hugot JP et al. Nature 1996;379:821–3Ogura Y et al. Nature 2001;411:603–6Barrett JC et al. Nat. Genet; 40:955‐962Franke A et al. Nat. Genet; 42:1118‐25Anderson CA et al. Nat. Genet; 43:246‐52
Many loci are shared, few are specificLoci segregates specific disease mechanism
CDIBD
UC
Innate ImmunityNOD2; LRRK2
Function not clearly definedNKX2‐3; CREM; C11Orf30; ORMDL3; RTEL1; PTGER4; KIF21B; CDKAL1; ZNF365
Receptor Signaling pathwayMST1; IL10; CARD9; REL; PRDM1; TNFSF15; IL1R2; YDJC; SMAD3; PTPN2
Adaptive immunityIL‐23 /Th17 pathwayIL23R; IL12B; TNFSF15; TYK2; JAK2; ICOSLG; STAT3; IL21
HLADRB103
Epithelial barrier
ECM1HNF4ACDH1LAMB1GNA12
AutophagyNOD2ATG16L1IRGM
Epithelial BarrierMUC19ITLN1
Cell migration
ARPC2LSP1
AAMP
Less organ‐specific, More mechanism/pathway oriented
Lees et al Gut 2011

12/13/2012
7
Clinical and therapeutic valueof genetic discoveries in IBD
Gut 2009;58:1612
Inflamm Bowel Dis 2010;16:2090
Inflamm Bowel Dis 2010;16:1357 Inflamm Bowel Dis 2011;17:179
Children carrying 34 or more of the common CD risk
alleles have a ~13-fold increased risk of developing CD,
and children carrying 20 or more of the common UC risk
alleles have a ~7-fold increased risk of developing UC
Imielinski M et al. Nat Genetics 2009;41:1335
Inflamm Bowel Dis 2011;17:1830
These initial findings need replication in large, well phenotyped and prospective cohorts
These initial findings need replication in large, well phenotyped and prospective cohorts
From gene discovery to IBD pathways
Gut 2011;60:1739‐1753
AutophagyNOD2; ATG16L1; IRGM; LRRK2PARK7; DAP
ER stressCPEB4; SERINC3
Cell migrationARPC2; LSP1; AAMP
Apoptosis /necroptosisFASLG; THADA; DAP
Oxidative stressPRDX5; BACH2; ADO; GPX4; GPX1; SLC22A4; LRRK2; NOD2HSPA6; DLO; PARK7
Epithelial barrierMUC19; ITLN1GNA12; HNF4A; CDH1; ERRF11
RestitutionSTAT3;PLA2G2A/E; HNF4A; ERRF11
Paneth cellsITLN1; NOD2; ATG16L1
Innate mucosal defenseNOD2; ITLN1; SLC11A1; FCGR2A/B
Antigen presentationERAP2; LNPEP; DENND18
IL‐23 / Th17STAT3; IL21
T‐cell regulationNDFIP1; TAGAP; IL2RIL2; TNFRSF9; PIM3; IL7R; TNFSFB; IFNG
B‐cell regulationIL5; IK2F1; BACH2;IL7R; IRF5
Immune toleranceIL27; SBNO2; NOD2; IL1R1 / IL1R2
Main pathways identified so far
Drug-mediated modulation of autophagy
Rubinzstein D et al. Nat Rev Drug Discovery. 2007;6:304
Massey D et al. Gut 2008;57:1294
Use of sirolimus (rapamycin) to treat refractory Crohn’s disease
Gene discovery can help in diagnosis and therapy
Allogeneic bone marrow transplantation could cure severe & early onset IBD
Gut 2012;61:7 1028‐1035
Glocker EO et al. The NEJM 2009;361:2033-2045
Muise, Snapper, Kugathasan. Gastroenterology, 2012
Evolution of IBD Genetics and therapeutic targets
Research Lessons learned
• CD and UC are very closely related.
• Genetics of IBD is shared with many other complex disorders. The genetic research has become less organ-specific, but focuses of molecular level and common pathways.
• Identification of clusters of ‘Bio-types’ can be used to target specific biological pathways.
• Firm genomic diagnosis can be used for definitive therapies to reverse the IBD

12/13/2012
8
Microbiome, diet and intestinal inflammation
Evidence for gut microbial dysbiosis in IBD
R Balfour Sartor and Sarkis K Mazmanian. Am J Gastroenterol 2012
Our environment determines the compositionof the gut microbiota
http://www.springerimages.com/Images/RSS/1‐10.1007_s12263‐011‐0226‐x‐0
Westernized lifestyle
Decreased microbial exposure
Reduced microbiota diversity
Chronic inflammatory diseases
Dysregulation of the immune system
Susceptible host
The hygiene hypothesis
Manichanh, C. et al. Nat. Rev. Gastroenterol. Hepatol. 9, 599‐608 (October 2012)
Changes in lifestyle alter the gut microbiota
Modern lifestyle in year 2012 !
Lifestyle: 50 yrs ago in Western world
Antibiotics and Pediatric IBD
Case control of all children born in Finland between 1994‐2008. • IBD diagnoses and antibiotic
ascertained through national registries
• For CD, repeated exposure increased risk
• No risk of abx during 1st year of life
Virta, Am. J. Epidemiology, 2012
CDN=233
UCN=362
Adjusted OR 2.1 (1.0‐4.4) 1.1 (0.7‐1.8)“Dirty” pigs
(Outdoor environment)
“Clean” pigs(Indoor environment + antibiotics)
Gut floraMore Firmicutes,
mostly LactobacillaceaeLess enterobacteria
Gut floraLess Firmicutes,
fewer LactobacillaceaeMore enterobacteriaGene expressioninflammation,
cholesterol synthesis
Gene expressionBalanced immunity
Mulder Iet al. BMC Biol 2009;7:79
Experimental evidence supporting the hygiene hypothesis

12/13/2012
9
Summary of gut microbiota main composition in IBD
Mulder I. et al. BMC Biol 2009;7:79
Phylotype Healthy Disease (IBD) ‘Clean’ Pigs ‘Dirty’ pigs
Firmicutes
Bacteroidetes
Proteobacteria
Frank et al PNAS 2007 Manichanh C et al Gut. 2006:205‐11
Diet shapes the gut microbiota
Proc Natl Acad Sci U S A. 2010 Aug 17;107(33):14691‐6
Rural Africa (Burkina Faso)
Urban Europe (Florence, Italy)
High carbohydrate, fiber and non‐animal protein Children breast‐fed up to the age of 2
Typical western diet high in animal protein.Children breast‐fed for up to age of 1.
Dietary patterns are associatedwith specific gut microbial patterns
Wu G et al. Sciencexpress / September 1, 2011 / 10.1126/science.1208344
CarbohydratesProtein & animal fat
Nickerson & McDonald (unpublished data)
Western diet (malto +)Normal diet (malto -)
FL82 AIEC biofilm formation
Maltodextrin: a common additive that improvestexture and palatability found in many foods, sweeteners (Splenda), drugs, cosmetics, etc.
Intestinal epithelial cells (HT29) infected with salmonella in the absence (normal diet) and presence (Western diet)of matodextrin: malto suppresses autophagy ➞ less killing ➞ more residual colonies ➞excess of bacteria
Modulation of bacterial function
by food additives
Different bacterial species induce different phenotypes of colitis in IL-10-deficient mice
Kim et al. Gastroenterology 2005
Germ-freeNo colitis
Commensal bacteria Pancolitis(Right sided)Onset 1 wk
E. faecalis Left sided10-12 wks
E. coli Right sided3 weeks
E. coli + E. faecalis Pancolitis1 week
D’ Haens G et al., Gastroenterology 114:262, 1998
Recurrence of ileal Crohn’s diseasebefore and after infusion of intestinal contents
12/13/2012
10
Evolution of collaborative researchin pediatrics compared to
single center/investigator effort
From single center/investigators to
multi‐center, multi‐investigator studies
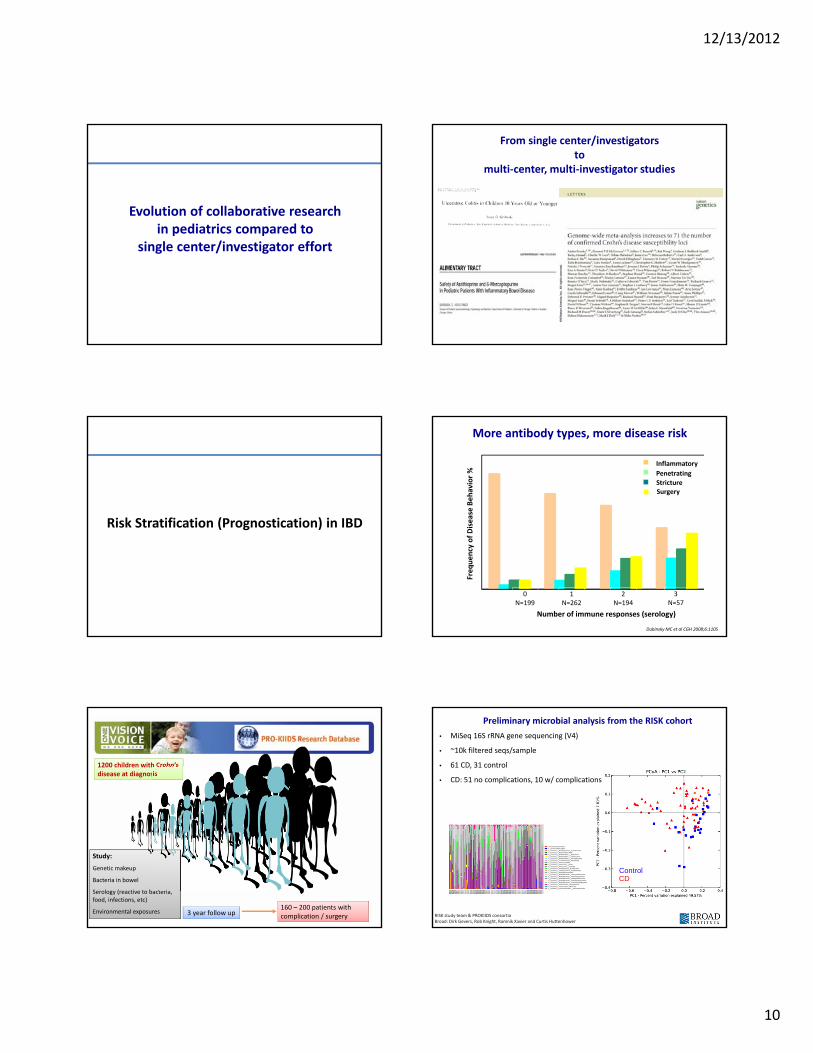
Risk Stratification (Prognostication) in IBD
Frequency of Disease Behavior %
Number of immune responses (serology)
More antibody types, more disease risk
Inflammatory
Penetrating
Stricture
0N=199
1N=262
2N=194
3N=57
Surgery
Dubinsky MC et al CGH 2008;6:1105
Study:
Genetic makeup
Bacteria in bowel
Serology (reactive to bacteria, food, infections, etc)
Environmental exposures
1200 children with Crohn’sdisease at diagnosis
3 year follow up160 – 200 patients with complication / surgery
ControlCD
Preliminary microbial analysis from the RISK cohort
• MiSeq 16S rRNA gene sequencing (V4)
• ~10k filtered seqs/sample
• 61 CD, 31 control
• CD: 51 no complications, 10 w/ complications
RISK study team & PROKIIDS consortiaBroad: Dirk Gevers, Rob Knight, Ramnik Xavier and Curtis Huttenhower

12/13/2012
11
In patients with ileal CD Ruminococcaceae, and Faecalibacterium were dramatically decreasedcompared to control subjects
Fusobacteria - Fusobacteria - Fusobacteriales - Fusobacteriaceae - Fusobacterium
In patients with ileal CD Fusobacteria were dramatically increasedcompared to control subjects
Preliminary microbial analysis show bothdecreased and increased taxa in risk cohort Fecal microbiota transplant for IBD
17 case series: 41 patients with IBD (27 UC)
• reduction of symptoms: 76%
• cessation of IBD medications: 76%
• disease remission: 63%
• resolution of concurrent C. difficile: 100%
Anderson et al, Aliment Pharmacol Ther. 2012
Perhaps, we can do selective FMT based on individual's flora and genetics
Can the host’s mucosal gene expression at the time of diagnosis predict complications?
– Non IBD (control)Red – Inflammatory (B1)Blue – Stricturing and penetrating (B2/B3)
Clusters
Ted Denson & RISK study team
Evolution of IBD Risk Stratification
Research Lessons learned
• Small proportion (20%) of CD accounts for 80% of complicated disease (and healthcare needs)
• These high risk patients are identifiable at the time of diagnosis with relatively low cost
• Individualized care based on RISK• Best approach for risk/benefit ratio• Reduce overall cost in long term
Remember the Key note speech delivered by Dr Clark
IBD: The Pediatric Burden & the impact of Pediatric IBD research
• 1.2 million people with IBD in the US, estimated 80‐100,000 children with IBD
• About 20‐25% of all IBD is diagnosed during the pediatric age
• Identification of BIOTYPE = Genotype + Phenotype+ Immunotype + Bacteriotype + ??? Future of IBD management.
ImmuneResponse
I
ImmuneResponse
ll
ImmuneResponse
lll
Immune responses
Outcomebiotypes
IBD l
IBD ll
IBDlll
Hypothesis: IBD biotypes drive the IBD phenotype and outcome
Bacterial
Bacteriall
Bacterialll
Gene l
Genell
Genelll
Genetic variability
Microbial variability

12/13/2012
12
Exposome
Metabolome
Transcriptome
Epigenome
Proteome
MicrobiomeEpimmunome
Inflammasome
Genome
Resolvome
Apoptosome Phenome
Responsome
Antibodome
IBD patientand associated“omes” network
IBD patientand associated“omes” network
“How Everything is Connected to Everything”A-L Barabási. Plume Books 2003
The interactomeThe interactome
Stead WW. Beyond expert-based practice. IOM Institute of Medicine. Evidence-based medicine and the changing nature of health care:The National Academies Press 2008
Clinical featuresDeep ulcerations etc.
Microbiome
Genetic variationand gene expression
Serology / immunotypes
RISK Stratification in the puzzle
of pediatric IBD
Close integration of 4 in‐depth
critical components
The Future
ACKNOWLEDGEMENT
Topics and contents I have chosen for the talk were suggested by the following IBD’ologists and scientists:
Francisco SylvesterJoel RoshJeff HyamsJim MarkowitzMarla DubinskyTed DensonAlex MuiseTim BoyleClaudio Fiocchi
12/13/2012
13
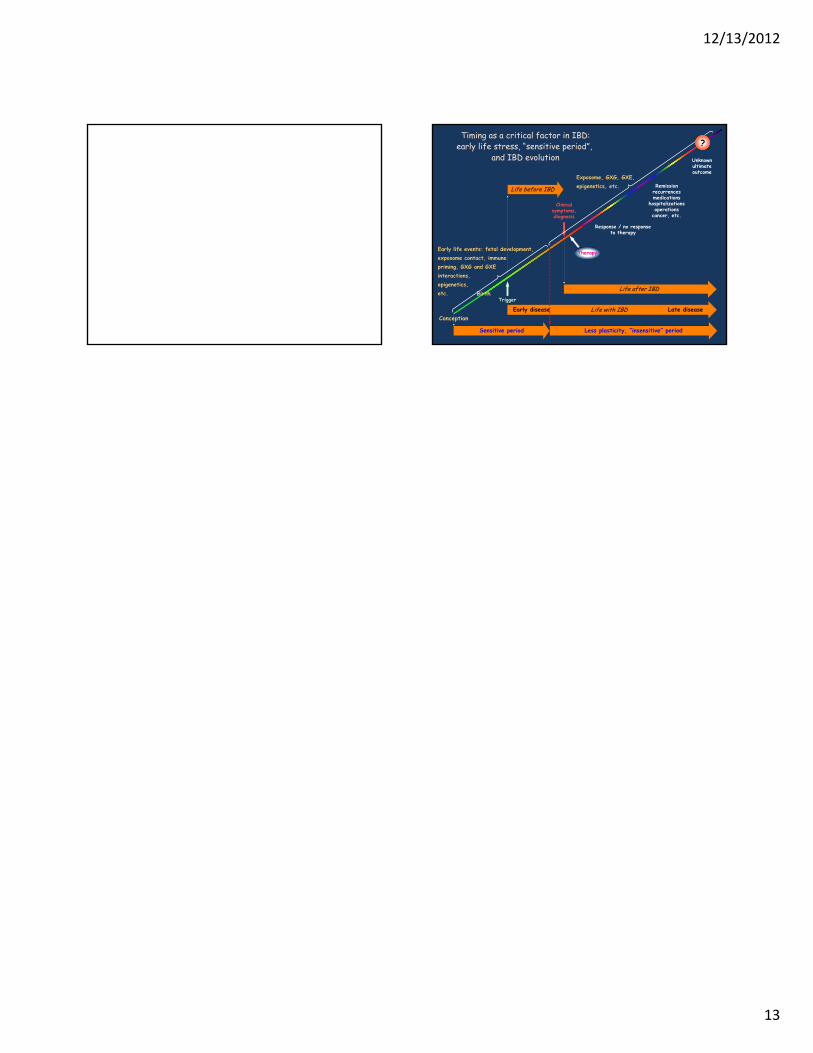
Timing as a critical factor in IBD:early life stress, “sensitive period”,
and IBD evolution
Life with IBDEarly disease Late disease
Less plasticity, “insensitive” period
Life before IBD
Trigger
Clinicalsymptoms,diagnosis
Exposome, GXG, GXE,epigenetics, etc.
Life after IBD
Therapy
Unknownultimateoutcome
Remissionrecurrencesmedications
hospitalizationsoperations
cancer, etc.
Response / no responseto therapy
?
Sensitive period
Early life events: fetal development, exposome contact, immune priming, GXG and GXE interactions, epigenetics, etc.
Conception
Birth





























