Embed Size (px)
Citation preview

"Experience is the worst teacher; it gives the test first before presenting the lesson."
--Vernon Sanders "Deacon" Law, 1930 - Pitcher, Pittsburgh Pirates: 1950 – 1967
Case 1: A 48 year-old male victim of a high speed motor vehicle crash (MVC) arrives in the trauma bay with a Glasgow Coma Score (GCS) of 7, blood pressure 90/60 mm Hg., pulse rate 120 beats/minute, and respirations of 8 per minute. Initial pulse oximetry is 84%, with decreased breath sounds noted at both bases. The cervical spine is immobilized. After placing the patient on 100% oxygen via a non-rebreather mask, two 16-gauge intravenous lines with normal saline are inserted. The patient continues to deteriorate hemodynamically, and the decision is made to intubate him utilizing Rapid Sequence Intubation with cervical spine precautions. During the second attempt, the intubating physician recounts visualizing the endotracheal tube (ETT) passing into the trachea. Auscultation of both axilla records "good air entry," and condensation of water vapor in the tube is observed. Neither an end tidal CO2 monitor (ETCO2) nor an esophageal detector device are used. Chest and lateral cervical spine x-rays are taken prior to transporting the patient to the Operating Room. Due to the urgency of transfer, the attending physician does not review the films. Upon arriving in the OR, the patient's condition quickly deteriorates into pulseless electrical activity (PEA). A grossly distended abdomen is noted, and reinspection of the airway reveals an esophageal intubation, which is quickly corrected. Despite all efforts, resuscitation proves unsuccessful.

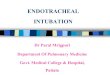
Figure 1. Frontal radiograph demonstrates an endotracheal tube in the esophagus. Note the large amount of gastric insufflation.

Fig 2: Lateral radiograph of the same patient shows a malpositioned
endotracheal tube in the esophagus
Table 1: Complications related to endotracheal tube placement Malposition Oral and Dental Trauma In esophagus Tracheal laceration In bronchus Laryngeal laceration
In glottis Esophageal laceration/perforation
Ensuring proper endotracheal tube placement is paramount in emergency airway management. In attempting to acquire a definitive airway, it is not uncommon to inadvertently misplace the tube or cause injury to the oral or laryngeal tracheal airway. One of the most serious complications of conventional endotracheal intubation is unidentified placement of the tube in the esophagus (3). Even the most experienced Emergency Physician accidentally intubates the esophagus at least once in his or her career. However, Esophageal Intubation (EI) is considered to be a problem of recognition as opposed to prevention (4). EI occurs relatively frequently in the emergency setting, with incidences ranging from 1 to 20% (5-7). This complication becomes of critical consequence when it remains unrecognized. Resultant unrecognized esophageal intubation triggers devastating consequences as evidenced by the closed claim study by Caplan et al. (8). Overlooked esophageal intubation produces severe hypoxemia progressing to permanent brain damage or cardiac arrest and ultimately death. Care was judged substandard in more than 80% of the inadequate ventilation and esophageal intubation claims (8). The problem of inadequate airway

management and missed esophageal intubation appears to be of even greater magnitude in children (10). Various outcome studies during the past two decades outline the extent and persistence of this problem. Failure to recognize esophageal intubation is not limited to junior residents or inexperienced personnel (11). However, recent studies suggest that unintentional esophageal intubation appears to occur more frequently in out-of-hospital situations. Contributing factors to this relatively high incidence of esophageal intubation include intubation under less than optimal conditions, unavailability of medication to assist intubation, lack of appropriate monitoring equipment, and less skilled personnel attempting intubation. Adverse Respiratory Events in Anesthesia: A Closed Claim Analysis (8): Studied 1541 adverse anesthetic outcomes based on closed claim files from 20 insurance carriers:
• Undetected esophageal intubations: 94 (6%). • 1/5 occurred during emergent intubation. • >95% felt to be preventable with proper monitoring. • 77% occurred in patients where intubation was not noted to be difficult. • 48% had equal breath sounds documented on chart. • 97% were not detected until over 5 minutes had transpired.
Clinical Outcomes (Esophageal intubations):
• 81% died. • 17% permanent brain damage. • 1% other permanent injury. • 1% Temporary injury. • 0% No injury.
Litigation outcomes:
• 82% resulted in a malpractice payment. • Median payment $217,000; Maximum $3.4 million.
In Hospital Emergent Intubation Schwartz, Anesthesiology 1995 (5):
• 297 emergent in-hospital intubations. • Performed by anesthesiologist • 25 (8%) were esophageal: 3 (1% overall, 12% of all esophageal tubes) undetected
with clinical exam.
Kasper, Anesthesiology 1998 (12):
• 300 emergent in-hospital intubations. • Performed by anesthesia resident (MD). • 19 (6%) were esophageal: All were detected with Esophageal Detection Device and
End-Tidal CO2.

Bozeman, Ann Emerg Med 1996 (13):
• 1% of Emergency Department intubations initially undetected esophageal intubations. • All were detected with Esophageal Detection Device
Sakles, Ann Emerg Med 1998 (14):
• 610 Emergency Department intubations: inadvertent esophageal tube placement found in 5.4%.
Prehospital Intubation Jenkins, Am J Emerg Med 1994 (15):
• 5% of field intubations were undetected (clinically) esophageal intubations.
Katz, Ann Emerg Med 2001 (16):
• 25% of patients had pharyngeal or esophageal intubation. • 17% of all field-intubated patients delivered to their ED had esophageal intubation. • Rate was higher in major trauma victims.
Esophageal intubations can remain undetected despite examination methods that seem to confirm proper tube placement (17-19). After emergent intubation, confirmation of the intratracheal location of an endotracheal tube is essential to airway management in critically ill patients. Over the years, a number of clinical signs and bedside maneuvers have been described to corroborate correct tube placement. Disappointingly there are inherent limitations to these techniques. Nonetheless, many physicians continue to rely solely on these error-prone clinical detection methods, unaware of their insensitivity (3,9). Over-reliance on traditional indicators contributes to the problem of delayed recognition of esophageal intubation. Direct visualization of the endotracheal tube passing through the vocal cords is purported to be the gold standard for confirming correct placement of the endotracheal tube. This method is fraught with potential risk. Physicians erroneously may believe that he or she observed the ETT pass through the larynx. However, distraction of the operator at the last moment prior to tube passage may trigger failure to accurately identify the anatomy, or the tube can become displaced into the esophagus post-tracheal intubation (9,20-22). This becomes particularly problematic in that a clinician convinced of proper tube placement would more likely explore other causes for hypoxia first, leading to delayed recognition of the true etiology. In Human Factor safety analysis this is known as a fixation error where there is a failure to revise a diagnosis or plan despite contradictory evidence and the persistent belief that no problem is occurring despite abundant evidence to the contrary (23). Frequently, the sole method used by clinicians to verify proper tube placement is auscultation of the chest. Confirming the location of the ETT by this method often proves erroneous. Air flowing through the esophagus has been shown to easily mimic respiratory airflow (18). Auscultation of the axillary region alone is recognized to be insensitive for a misplaced ETT. Andersen and coworkers demonstrated this method failed to identify esophageal intubation in 5 of 40 cases (18). Clearly unaided auscultation cannot be relied upon as the singular method of verification. Observing for condensation of water vapor in the tube during expiration is also extremely undependable. Haridas reported 42 of 60 esophageal intubations displaying condensation (24).

It is well documented that condensation can occur from gas emanating from the stomach (18). Therefore the presence of a vapor trail should not be used as supporting evidence for endotracheal intubation (17). Additional cited clinical techniques for ETT confirmation also reveal fallibility. Observation for symmetric bilateral chest excursions during compression of the reservoir bag can be deceptive in obese patients, women with large breasts and patients with a rigid chest wall. More disturbingly, upper chest wall movements simulating ventilation of the lungs can be seen and felt with an esophageally placed tube (25). Likewise, depending on reservoir bag compliance to differentiate esophageal from tracheal intubation is unreliable as is palpation of the cuff in the neck (26). While pulse oximetry should be continuously monitored during the intubation process, its use as a rapid detector of esophageal intubation remains limited. Although unrecognized esophageal intubation ultimately leads to a decrease in oxygen saturation, minutes may lapse before this is detected by pulse oximetry. This is especially true if the patient was pre-oxygenated prior to intubation. Delayed desaturation may then mislead the clinician into mistakenly believing the endotracheal tube is correctly positioned (27,28). The ideal device for corroboration of correct tracheal tube placement ought to be simple, quick to perform, dependable, safe, inexpensive, and reproducible (22). It should not require any elaborate equipment or extensive expertise. Ideally, it should demonstrate high specificity and sensitivity. While no such device yet exists, there are intubation confirmation devices that prove reliable in the emergency setting. These are the esophageal intubation detector, colorimetric end-tidal CO2, capnometry, and capnography. Such devices are accepted standards of care in the emergency setting. Intubation Confirmation Devices
• EID®: Esophageal Intubation Detector • Colorimetric End-Tidal CO2 • Capnometry • Capnography
STANDARD OF CARE
American Society of Anesthesia - Early 1990's:
• Waveform ETCO2 monitoring is mandatory in all intubated patients in the operating room.
Advanced Cardiac Life Support- 2000:
• Secondary confirmation devices following intubation (ETCO2, EDD) are now standards in the ACLS and PALS guidelines.
Esophageal detection devices (EDDs) are easy to use, inexpensive, and generally demonstrate good efficacy in detecting esophageal intubations. EDDs rely on anatomical differences in the rigidity of the tracheal and esophageal walls, with the trachea remaining consistently patent because of C-shaped rigid cartilaginous rings. The device consists of a 60-ml syringe fitted by an adaptor that can be attached to a tracheal tube adaptor. If the tube is

in the esophagus there is resistance to aspiration, with the esophagus collapsing when negative pressure its applied to its lumen. It is a rapid and reliable indicator of proper tube placement. Sensitivity and specificity have been reported to approach 100% (29,30). Reports of failure of the EDD to detect esophageal intubation have been attributed to prior air insufflation into the stomach (31). False negative readings (i.e., failing to detect tracheal intubation) have been attributed to chronic obstructive pulmonary disease, copious secretions and obesity (31-33). A potential advantage of the EDD over capnometry in the overall ED population may be in the setting of cardiac arrest, where it appears to be more sensitive (13,33). In the pre-hospital setting, the EDD has been found to be less reliable. In a prospective study by Pelucio and colleagues of 168 patients intubated in the field by paramedics, the EDD failed to identify 5 out of 10 esophageal intubations (34). Esophageal Intubation Detector Mechanism of Action:
• Applies vacuum to endotracheal tube. • Exploits anatomic difference between the trachea and the esophagus:
Device fills with air if ETT is tracheal. Device fails to fill with air if ETT is esophageal.
Literature support - Extensive:
• Exceedingly rare miss of esophageal tubes. • Approximately 3% misidentification of tracheal tubes:
Morbid Obesity. Right Mainstem intubation. Fluid filled airway.
Table 2: Esophageal Intubation Detector Advantages
Disadvantages
Very accurate Not a monitor
Immediate results Misses 3% of tracheal tubes Reduces aspiration risk
Reliable in cardiac arrest Very simple
Light, durable, portable No batteries
Not affected by airway contaminants
Inexpensive

Capnometry, capnography, and colorometric end-tidal CO2 monitors have emerged as the standard of care for anesthesia (end-tidal CO2 monitoring) to distinguish tracheal from esophageal intubation: "When an endotracheal tube is inserted, its correct positioning in the trachea must be verified by clinical assessment and by identification of carbon dioxide in expired gas" (35). Providing pulmonary perfusion is adequate, alveolar gas normally contains 5% carbon dioxide that can be reliably be detected in expired air from the intubated trachea, whereas CO2 is absent in gases emanating from a tube in the esophagus. False positive readings, reporting the tube to be in the trachea when it is actually in the esophagus are possible. This may occur when expired alveolar gas is introduced into the stomach during bag-valve-mask ventilation, or following the ingestion of carbonated beverages or antacids (30). Most false negative readings, reporting the ETT to be in the esophagus when it is actually in the trachea, occur in states of low cardiac output (e.g., cardiac arrest, severe hypotension), severe pulmonary disease or pulmonary embolism (30,37-39). In a meta-analysis, Li revealed capnography to express a sensitivity of 93% and specificity of 97% (30). This translates to a failed recognition of esophageal intubation in 3% of cases. Both qualitative colorimetric and quantitative digital end-tidal CO2 detector devices are available. The qualitative method simply measures the presence of CO2, whereas the quantitative method produces a waveform that can correlate with the respiratory cycle. A detectable waveform can be identified at lower levels of expired CO2, making it more sensitive in low flow states (40). Occurrence of a waveform, no matter how small, provides strong evidence of correct endotracheal tube placement in the trachea. Emergency Departments frequently make use of disposable colorimetric end-tidal carbon dioxide detectors. This detector contains filter paper impregnated with a colorless liquid based pH-sensitive indicator that reversibly changes from purple (‘problem’) to yellow (‘yes’) as a result of pH change when exposed to CO2. In general a purple color ("A" range) indicates a CO2 level < .5%; the "B" range is a dusty tan color reflecting CO2 levels between .5% and 2%; and when the detector is exposed to CO2 levels higher than 2% the color brightens to a yellow color, the "C" range (41). This device is quite reliable in the non-arrested patient. Colorimetric ETCO2 Mechanism of Action:
• pH sensitive paper changes color when exposed to CO2. • Color change indicates expired CO2 and confirms tracheal location.
Literature support - Extensive:
• Exceedingly rare miss of esophageal tubes. • Frequent misidentification of tracheal tubes: Cardiac arrest, fluid in airway,
bronchospasm, poor light conditions, shock.

Table 3: Colorimetric End-Tidal CO2 Detector Advantages
Disadvantages
Is a monitor Misses many tracheal intubations
Relatively simple Reliable only after seven breaths Inexpensive Aspiration risk higher than EDD
Light, durable, portable Often unreliable in cardiac arrest No batteries Affected by airway contaminants
Capnometry Mechanism of Action:
• CO2 absorbs infrared light at 4.26 um wavelength. Machine compares IR absorption in airway gas to IR absorption in CO2-free chamber.
• Differences in absorption are measured and reported: Qualitatively, semi-quantitatively, quantitatively.
Literature support - Extensive:
• Exceedingly rare miss of esophageal tubes. • Occasional misidentification of tracheal tubes: Cardiac arrest, fluid in airway, severe
shock.
Table 4: Capnometry Advantages
Disadvantages
Very accurate Aspiration risk higher than EDD Is a monitor Often unreliable in cardiac arrest
Affected by airway contaminants Expensive Requires power source
SUMMARY
• Esophageal Intubations occur relatively frequently. • Missed esophageal intubations increase in proportion to the difficulty of the clinical
situation. • Missed esophageal intubations guarantee a bad patient outcome. • Clinical judgment is inadequate to eliminate missed esophageal intubations. • Any undetected esophageal intubation or undetected ET-tube dislodgment is
inexcusable and constitutes medical malpractice.

Chest Radiographs While portable chest radiographs of intubated patients are routinely obtained in the Emergency Department setting, they should not be relied upon to quickly differentiate tracheal from esophageal intubation. In addition to the normal delay incurred in taking and developing the film, misreading the x-ray is possible due to projection of the esophagus over the tracheal air column (42). Primarily the utility of the chest x-ray is to ensure proper endotracheal tube position within the trachea.
Figure 3: Location of ETT tip above carina
When evaluating an endotracheal tube on a chest x-ray it is important to identify the location of the tube’s distal tip. The ET tube should be positioned so that the balloon is below the level of the vocal cords (about C6) and the distal tip is above the carina (43,44). The ideal position

for endotracheal tubes is in the midtrachea, 5 cm from the carina, with the head neither flexed nor extended. This allows for movement of the tip of the tube with head movements. The tip of the ET tube moves in the same direction as the patient’s chin. When the patient shifts his head to drop his chin from the neutral position, the ET tube tip can move 2cm more distal; when the patient lifts his chin from neutral, the ET tip can move 2cm more proximal. Remember the hose follows the nose. Thus, a general rule is to have the tip of the ET tube about 3-5cm above the carina. A previous chest ray can be used to estimate the position of the carina; it may be helpful to bear in mind that 95% of patients' carinas project over the T5 - T7 vertebral bodies. Alternatively, the Dee method for approximating the position of the carina can be used. This involves defining the aortic arch and then drawing a line inferomedially through the middle of the arch at a 45-degree angle to the midline. The vertical line is drawn down the center of the trachea. The intersection of the midline and the diagonal line is the most likely location of the carina.
Figure 4: Dee method of locating carina on radiograph
Approximately, 15% of endotracheal tubes are malpositioned (43). Because of the anatomy of the major bronchi, intubation of a bronchus is much more common on the right than on the

left side. When the tip of the tube is within a bronchus, a pneumothorax may occur on the intubated side and/or there may be collapse of the contralateral lung bypassed by the tube. Accidental esophageal intubation with positive pressure ventilation can also cause gastric rupture and pneumoperitoneum (45). Another uncommonly-mentioned malposition of the endotracheal tube is glottic location (46). Standard techniques such as absence of epigastric sounds, the presence of bilateral breath sounds, and even visualization of vapor in the tube for confirming endotracheal tube position prove unreliable in distinguishing tracheal placement from glottic placement. Additionally, objective measures of verifying tube position such as pulse oximetry readings and end-tidal CO2 are also undependable in distinguishing this inappropriate tube placement. Glottic intubation needs to be recognized and corrected, as it can be detrimental for a number of reasons. First it does not afford the same degree of airway protection as an appropriately placed endotracheal tube. Moreover, hypoventilation is possible since the tube is not actually in the tracheal lumen. Finally, if the patient were to regain consciousness his gag reflexes could become stimulated enough to cause the tube to become displaced or kinked, compromising ventilation completely (46). Malposition of the endotracheal tube may be noticeable on the chest x-ray or cross table lateral of the cervical spine. Additionally assess the cuff size of the endotracheal tube on the chest x-ray film. The endotracheal tube has an inflatable cuff that serves to stabilize the tube within the trachea as well as prevent aspiration of gastric contents into the trachea. Optimally, the diameter of the cuff should equal that of the trachea. However, if the cuff is overinflated and the diameter of the cuff greatly exceeds the diameter of the trachea (i.e., > 2.8 cm) distal to the cuff, there may be injury to the trachea, producing either rupture of the trachea or tracheomalacia (47). Additionally, distal prolapse of the balloon of the cuff is seen with tracheal rupture and esophageal intubation (47). The Emergency Physician also needs to review the chest x-ray for foreign bodies, especially teeth that may become dislodged during intubation. Teeth are often dislodged because of poor bony support structure. Patients tended to be older (in their fifth to seventh decade) with 86% of the injured teeth being the upper incisors (48).

Figure 5: Radiograph of tooth aspirated during intubation.
The upper arrowhead identifies the end of the ETT.
Clues to esophageal intubation on chest x-ray (47):
• Projection of any part of the endotracheal tube outside the tracheobronchial air column • An enlarged tracheal balloon cuff (transverse diameter > 2.8 cm) • New extrapulmonary gas collections (marked gastric dilation, pneumoperitoneum,
pneumomediastinum) • Distal prolapse of the tracheal balloon (distal margin < 1.2 cm proximal to the
endotracheal tube tip)

Case 2: A 45-year-old male was found unresponsive in a city park. The patient has a GCS 6. After applying cervical spine precautions, the patient was orally intubated with an 8-0 endotracheal tube. Upon arrival at the hospital, the patient demonstrated spontaneous respirations with a rate of 26 breaths/min, and oxygen saturation was 87%. Decreased air entry was noted on the right side of the chest with palpable subcutaneous emphysema on the neck and upper part of the chest, but there were no clinically detectable rib fractures.
Figure 6: Radiograph demonstrates massive subcutaneous
emphysema, a right mainstem intubation, and a large gastric bubble
Tracheal trauma is a rare but devastating consequence of endotracheal intubation (49). The incidence of this condition is difficult to establish since many tracheal lacerations may be undetected clinically. Several anatomic and mechanical factors have been proposed to play a role. Clinical clues include persistent air leak around the endotracheal tube cuff despite adequate cuff inflation, subcutaneous emphysema over the neck and chest, mediastinal emphysema causing Hamman's crunch, difficulty ventilating the lungs, cyanosis, hemoptysis, and, less commonly, clinical signs of pneumothorax (50). The most common radiographic findings are pneumomediastinum, subcutaneous emphysema, and pneumoperitoneum (50). Early radiographic signs of tracheal rupture as described by Rollins and Tocino include: (1) orientation of the distal portion of the endotracheal tube to the side relative to the lumen; (2) an overdistended balloon cuff; (3) migration of the balloon towards the endotracheal tube tip; and (4) combined subcutaneous emphysema and pneumomediastinum (51).

Factors Predisposing to Tracheal Laceration during Intubation Mechanical causes of tracheal injury during intubation • Overinflation of the endotracheal tube cuff • Multiple attempts at intubation • Repositioning of the tube without deflating the cuff • Stylet protruding from the endotracheal tube • Patient coughing while intubated • Abrupt head and neck movement while intubated Anatomical factors associated with tracheal injury • Congenital tracheal abnormalities • Weakness of the membranous trachea • Chronic obstructive airway disease • Chronic steroid use
Case 3: A 36 year-old male with a history of intravenous drug abuse presents to the ED febrile, hypotensive and confused. The attending Emergency Physician inserts a central venous catheter (CVC) due to poor peripheral IV access. The procedure was performed at the right internal jugular site. At the end of the procedure, the ED physician reported excessive bleeding from the catheter site that was eventually controlled with manual pressure. A chest radiograph obtained after the procedure is interpreted as revealing the catheter lying in the distal right jugular vein. Twelve hours later, the patient developed dysarthria, dysphagia, and left hemiplegia. A MRI of the brain showed new cerebral infarctions in the right frontal, parietal, and temporal lobes. A carotid ultrasound rules out carotid stenosis. However, the ultrasound does confirm the CVC within the lumen of the right carotid artery. The catheter was immediately removed. The patient suffered permanent neurological deficits, including left sided hemiplegia. He was eventually discharged to a long-term skilled nursing facility.

Figure 7: Subclavian line passing into internal carotid artery
Central venous catheter insertion is one of the most frequent invasive procedures performed by Emergency Physicians (for an excellent review see The Difficult Vascular-Access Patient: Site Selection and Advanced Troubleshooting Pearls by Michelle Lin, MD). Selection of the central line access site is crucial to success or failure. There are multiple approaches for internal jugular, subclavian, and femoral venous catheterization (52). For the most part, femoral venous catheterization should be avoided except in emergencies because it is associated with an increased risk of infectious and thrombotic complications (53,54). The subclavian vein is the preferred site, especially in patients with indistinct landmarks for internal jugular catheterization, as it is purported to have the lowest rates of overall complications (53-56). Surprisingly, there is no difference in the rates of pneumothorax for internal jugular versus subclavian vein placement (56). Internal jugular lines are associated with a higher incidence of inadvertent arterial puncture (56). However, bleeding is more difficult to control when it arises at the subclavian site. Importantly, patients generally find subclavian catheters more comfortable than the internal jugular catheters.

Table 5: CVC Insertion (McGee, et al.) (57) Complication Frequency Internal Jugular (%) Subclavian (%) Femoral (%) Arterial puncture 6.3 to 9.4 3.1 to 4.9 9.0 to 15.0 Hematoma <0.1 to 2.2 1.2 to 2.1 3.8 to 4.4 Hemothorax NA 0.4 to 0.6 NA Pneumothorax <0.1 to 0.2 1.5 to 3.1 NA Total 6.3 to 11.8 6.2 to 10.7 12.8 to 19.4
While the rate of complications is greater for inexperienced practitioners, even seasoned clinicians endure complications and some degree of failure (58). Given the close proximity of other vital organs and vessels to the central veins, successful catheterization by either the internal jugular or the subclavian route relies on a thorough understanding of the anatomy of the neck. The internal jugular vein is located at the apex of the triangle formed by the heads of the sternocleidomastoid muscle and the clavicle. The subclavian vein crosses under the clavicle just medial to the midclavicular point. When the landmarks for one site of insertion prove problematical to identify, consider an alternative site. Of maximum relevance to this article are mechanical complications reported to occur in 5% to 19% of patients (53,55,58). Specifically, the following complications will be reviewed:
• Arterial puncture/ cannulation • Vessel Perforation • Malposition • Air embolus • Pneumothorax
Understandably, experience is important in limiting the risk of complications and when inexperienced physicians are performing central venous catheterization they need to be closely supervised (60). Fifty appears to be a strategic number as insertion of a CVC by a physician who has performed 50 or more catheterizations is half as likely to result in a mechanical complication as introduction by a physician who has performed fewer than 50 CVCs (55). Inability of the physician to insert the CVC after three attempts suggests the need for the operator to abandon any additional efforts and to seek assistance rather than continue the procedure. There is a six-time increase in the incidence of mechanical complications after three or more insertion attempts versus one attempt (58).

Table 6: Risk Factors for Mechanical Complications of CVC Insertion (57) • Patient factors
Extremes in weight Prior surgery or catheter at catheter site
Skeletal deformities: Severe scoliosis, upper extremity or neck contractures
• Inability to cooperate
• Operator factors:
Experience Physicians who have performed > 50 catheterizations have 1/2 as
many complications 3 or more unsuccessful passes with the needle is a marker for
increased complications
Arterial puncture complicates approximately 5% to 10% of internal jugular catheterization attempts (55,60). In patients with normal blood pressure and normal arterial oxygen tension, inadvertent arterial puncture, hitting "Big Red," provokes pulsatile flow of bright-red colored blood into the syringe. However, these findings are not as clear-cut in patients who are volume overloaded and breathing 100% oxygen, who may display pulsatile venous blood flow that appears quite red; patients with profound hypotension or marked arterial desaturation, may reveal minimally pumping arterial blood flow that is unexpectedly dark. Obviously, the key to preventing serious injury to the artery is recognizing an arterial puncture prior to dilating the vessel (57). If there is any uncertainty as to whether the introducer needle is in the artery or the vein, insert an 18-gauge, single-lumen catheter (included in most kits) over the wire and into the vessel and avoid using the dilator. It is usually more difficult to slide a catheter into an artery than vein because of the thick elastic properties of the arterial wall. Once the catheter is successfully placed, connect it to a pressure transducer. Venous waves are easily distinguished from arterial waves. Alternatively, a manometer can be constructed with a 20-cm to 30-cm piece of sterile IV tubing flushed with saline. After cannulation, connect the tubing to the needle and hold it upright. With arterial puncture the saline column does not drop and blood will pulsate to the top of the tubing. In contrast, with venous cannulation there is an immediate plunge in the column of saline. Sending a blood sample from the catheter for blood gas analysis is another option. Simultaneous analysis of the radial artery blood improves the accuracy of this technique. There should be a substantial difference in the oxygen tension if the catheter is located in a vein. The major drawback to blood gas analysis is time delay, which can be minimized when point-of-care testing is available. If the large central venous catheter inadvertently pierces the carotid artery, an airway-threatening hematoma can form even with application of external pressure (apply for a minimum of ten minutes). In addition to monitoring the patient’s airway and hemodynamic status, it may be prudent to leave the catheter in place and consult a vascular surgeon. Inadvertent subclavian arterial puncture is a relatively common complication of subclavian venipuncture. The overall reported incidence is in the range of 1 - 13% with 2 - 5% being typical. This incidence increases to about 40% if multiple attempts are made (61). Consequences of subclavian arterial puncture are not as potentially serious as the consequences of inadvertent internal carotid puncture as the risk of a cerebral

thromboembolic event or airway compromise is practically nil with accidental subclavian arterial injury. However, bleeding from the subclavian artery is much more difficult to control by pressure alone and if bleeding occurs, it may be more easily missed because the blood may track into the pleural cavity. It is for this reason that the subclavian route is generally thought to be the least suitable approach to the central circulation in the anticoagulated patient. Perforation of a great venous vessel is an uncommon, but potentially lethal, complication of central venous line placement (62). Catheter perforation may result in pleural effusion, hydrothorax, hemothorax, hydromediastinum, pneumothorax and pneumomediastinum (63). Most complications occur with the right subclavian vein approach and are thought to result from guidewire kinking during advancement of a vessel dilator. Another possible fatal problem arising from vascular trauma is cardiac tamponade (64).
Figure 8: Widened mediastinum from inadvertent puncture of subclavian vein

Familiarity with normal and variant vascular anatomy is crucial for catheter positioning. Current guidelines strongly advise that the CVC tip be positioned in the superior vena cava (SVC) and outside the pericardial sac (64). Roughly, the tip should project over the superior vena cava beyond the anterior right second rib but above the cardiac border. Collier and colleagues recommend avoiding any location of the CVC tip that can be seen inside the cardiac silhouette on CXR (64). Placement beyond the superior vena cava may provoke arrhythmias or cause a cardiac perforation. Catheter tip malposition occurs in up to 14% of cases of IJ insertion and 11% of subclavian vein (56,65). For subclavian vein insertion the most common misplacement is in the ipsilateral IJ vein. The rate of misplacement of subclavian lines can be greatly reduced by the simple, noninvasive maneuver of placing a finger in the supraclavicular fossa during guide wire introduction. More specifically, the "finger-in-fossa" technique - having an assistant place a sterile finger in the patient's ipsilateral supraclavicular fossa or placing your own middle finger in the fossa - prevents the guide wire from traveling into the IJ vein. Interestingly, when the catheter tip unintentionally navigated up the IJ vein many patients complained of either ear pain or a trickling throat sensation during catheter insertion (66). In one study, the rate of catheter tip malposition was less than 1% with the supraclavicular route versus 10.8% with the infraclavicular route (67). Other common misplaced line locations are in the right atrium and ventricle, the inferior vena cava, the subclavian vein, internal jugular vein and azygos vein 68. Less frequently misplaced locations include a persistent left superior vena cava, the hepatic vein, the internal mammary veins, and arterially in the aorta, subclavian or internal carotid artery (68).

Figure 9: Central venous catheter lying beyond the superior vena cava. The smaller arrow points to the right ventricle.
Chest X-ray and CVC placement
• Radiographic confirmation of catheter position is generally reliable Can also identify other complications such as pneumothorax or hemothorax
• When correctly positioned, tip of catheter lies in the cavo-atrial junction, at the level of the right main stem bronchus

Figure 10: Central venous catheter passes from the right subclavian vein through the innominate veins to the left subclavian veins
One of the most serious complications of central venous catheterization is an air embolism, a potentially fatal event caused by the sudden entry of air into the heart or pulmonary artery. The true incidence of this complication is unknown. However, the frequency of air embolism during central venous access procedures is probably underestimated because the signs and symptoms are nonspecific and may be transient (69,70). A spontaneously breathing patient generates negative intrathoracic pressure during inspiration. If a catheter is left open to room air, the negative intrathoracic pressure can draw air into the vein, resulting in an air embolism. The sudden entry of a bolus of air into the right ventricle is thought to act as an "air lock," serving as a mechanical barrier to the right ventricular outflow tract. To prevent this complication, occlude the catheter hubs at all times, place the patient in the Trendelenberg’s position during the procedure, and ask the patient to exhale during insertion. If air embolism does occur, place the patient in a left lateral decubitus tilt to prevent movement of air into the right ventricular outflow tract, then administer 100% oxygen to help speed the resorption of the trapped air.

Figure 11: Air embolus in heart demon stared on CT scan
Pneumothorax is one of the more common complications resulting from central venous catheter insertion. The overall incidence is typically quoted as between 1% and 2% (71,72) but this increases to about 10% if multiple attempts at venipuncture are made (61). Pneumothorax is generaelly stated to occur more frequently with subclavian vein puncture than with internal jugular vein insertion. This is anticipated since the apex of the lung is only 0.5 cm from the subclavian vein and is therefore vulnerable. However, one study indicates a relatively similar rate for hemo/pneumothorax for internal jugular insertion as compared to subclavian insertion (57). Pneumothorax occurs more commonly in thin patients and in those with hyperexpanded chests. Depending on the size of the pneumothorax, treatment may range from expectant management with administration of oxygen (to enhance resolution) to formal tube thoracostomy. However, most pneumothoraces arising from central venous catheter miscues remain asymptomatic. Generally this complication is apparent on post procedural chest radiographs but occasionally may not manifest for several days after catheter placement (71). A meta-analysis by Plewa et al. revealed that delayed pneumothorax complicated approximately 0.4% of all central venous access attempts, was much more common after subclavian than internal jugular approaches, was asymptomatic in about 22% of cases and resulted in a tension pneumothorax in a similar proportion (73). A small simple asymptomatic pneumothorax can rapidly become a serious tension pneumothorax if the patient undertakes mechanical ventilation. A sonographically-guided internal jugular vein approach to central venous catheterization has been shown to improve procedural success and lower complication rates compared to the

traditional external landmark-guided puncture technique (74-76). In terms of complications, arterial puncture and hematoma formation occur in only 1.7% and 0.2% of patients, respectively, with ultrasound-guidance as compared to 8.3% and 3.3% with the landmark-based insertion (74). Reducing CVC-related Complications
• Limit catheter insertion to experienced operators or closely supervise inexperienced physicians
• Preferentially use the subclavian site • Use ultrasound guidance to identify target vessel when internal jugular approach
necessary • Optimize patient positioning prior to insertion

Case 4: A 33 year-old female arrives in the ED via ambulance with a report of 3 days of vomiting and diarrhea. On presentation she was found to be diaphoretic and hypotensive. Attempts at peripheral venous access failed. Using a standard kit, the right femoral vein was accessed via the Seldinger technique. The resident reported no complications. However, a routine admitting chest x-ray done two hours later revealed a guide wire in the thorax.
Figure 12: Loss of guide wire in chest
(Reprinted from Lum TE, Fairbanks RJ, Pennington EC, Zwemer FL. Misplaced Femoral Line Guidewire and Multiple Failures to Detect the Foreign Body on
Chest Radiography. Acad Emerg Med. 2005 Jul;12(7):658-62., with permission from Society for Academic Emergency Medicine)
Loss of the guide wire is a recognized complication of central line placement using the Seldinger technique and is considered to represent a systems problem rather than just an individual mistake (78). Despite traditional teachings to "never let go of the guide wire" this may become impractical during the course of the procedure (78). While there are no exact statistics on the complications associated with lost guide wires, such a foreign body could potentially cause arrhythmias, vascular damage, thrombosis and embolism (79). Guide wires ought to be removed as quickly and completely as possible once discovered misplaced in the body cavity. Interventional radiology is the method of choice

Predisposing factors for lost guide wire include:
• Inattention • Inexperienced operator-either in method (i.e. Seldinger technique) or actually central
venous cannulation per se • Inadequate supervision of trainees • Overtired staff
Signs of guide wire loss include:
• The guide wire is missing • Resistance to injection via the distal lumen • Poor venous backflow from the distal lumen • Guide wire visible on a radiograph
Case 5: A 48 year-old male with worsening dyspnea presents to the ED. A chest x-ray reveals a large pleural effusion. Subsequent to speaking to the consultant, the decision is made to insert a thoracostomy tube. The patient is prepped and a 24-F tube is inserted. However, no drainage is noted from the tube. This patient remained symptomatic after chest tube insertion. A chest x-ray showed a failure of the tube to drain the pleural effusion.
"There is no organ in the thoracic or abdominal cavity that has not been pierced by a chest drain" (80).
Tube thoracostomy is an invasive procedure that is often life saving, but by no means innocuous. Usually a chest tube is inserted in the Emergency Department for a spontaneous or traumatic pneumothorax involving greater than 25% collapse. Other potential indications include hemothorax or hemopneumothorax or a significant pleural effusion (malignant, complicated parapneumonic). The aim of drain insertion is to restore and maintain the negative intrathoracic pressure necessary for lung expansion and drainage of the pleural cavity. Etoch reported a complication rate of 21%, which he partly attributed to tube thoracostomies being performed by non-surgeons (81). Chan rebutted this claim by demonstrating no significant difference in complication rates between thoracostomy tubes inserted in the Emergency Department, operating room, and in-patient wards (82).

Figure 13: Nonfunctioning chest tube
Position the chest tube in the "safe triangle". This is the triangle bordered by the anterior border of the latissimus dorsi, the lateral border of the pectoralis major muscle, a line superior to the horizontal level of the nipple, and an apex below the axilla. Immediately before the procedure the site and side for insertion of the chest tube should be confirmed by reviewing the clinical signs and the chest radiograph (83).

Figure 14 : Safe triangle
(Reproduced with permission from the BMJ Publishing Group, D Laws, E Neville and J Duffy, BTS guidelines for the insertion of a chest drain. Thorax 2003;58:ii53.)
Complications arising from chest tube insertion can be divided into 3 categories (84):
Insertional:
• Esophageal perforation • Partial aortic obstruction • Laceration of internal organs and vessels • Acute diaphragmatic paralysis • Avulsion injury to stomach • Chylothorax • Lung perforation • Diaphragmatic perforation • Subcutaneous placement

Positional:
• Horner’s syndrome • Arteriovenous fistula • Reexpansion pulmonary edema • Contralateral pneumothorax • Cardiogenic shock from displacement of right ventricle
Miscellaneous:
• Pulmonary infarction • Empyema • Subcutaneous emphysema • Necrotizing fasciitis • Osteomyelitis • Site infection
A variety of complications have been associated with chest tube insertion (85). The most common of these complications is tube malposition. In a study by Deneuville, 144 chest tubes were placed for either blunt or penetrating thoracic trauma (86). The overall total complication rate was 25%, including 7% erroneous positioning, causing iatrogenic injuries to lung and subclavian vein. There is also a definite inherent risk of chest tube positioning outside the targeted pleural space. Morbidity and mortality increase substantially with chest tube malposition (87). Bleeding from the chest wall and damage to breast tissue have been described (87). More unusual complications include esophageal perforation (88), cardiac perforation89 subclavian vein obstruction (90). Many of these serious problems were associated with the closed technique that used a trocar. Insertion of the chest tube employing an open technique as described in the ATLS manual eliminates many of these potential complications (91).

Figure 15: Chest tube malpositioned below left hemidiaphragm with gastric distention. Endotracheal tube is positioned in right mainstem bronchus
On a single AP or PA view of the chest, the chest tube may appear to be within the thorax but actually may lie in the subcutaneous tissue, behind the consolidated lung, in a lung fissure, or within the substance of the lung. For example, a chest tube that overlies the right lung base may be in the pleural cavity, hepatic parenchyma, or soft tissues. If the chest tube is not draining adequately or the chest radiograph is equivocal regarding position, then a lordotic view of the chest can be ordered or even more optimally a computerized tomography (CT) scan of the chest should be performed (92). CTs of the chest demonstrate marked superiority over plain radiography in the assessment of chest tube position, often resulting in changes of management (93). As in our example, if the patient remains symptomatic after chest tube insertion, the first step is to recall if air or fluid drainage occurred immediately on entering the chest. If not, then the chest tube probably is positioned incorrectly in the pleural space or is not in the pleural cavity at all. Next evaluate the chest film. In situations where the chest x-ray does not conclusively determine the position of the chest tube, obtain either a lordotic or lateral view of the chest,

or a chest CT, depending on the situation, resources, and patient’s stability. If the additional imaging reveals the chest tube to be misplaced then the thoracostomy tube must be repositioned. The consequences of an improperly positioned chest tube range from ineffectual drainage to vital-organ damage. While the former may require only the repositioning or replacement of the chest tube, the latter may necessitate extensive surgical exploration and repair. In order for thoracostomy tubes to function properly all of the fenestrations in the tube must be within the thoracic cavity. The last side-hole in a thoracostomy tube is indicated by a gap in the radiopaque line. If the chest tube is kinked in the pleural space and is occluding the lumens, retracting the tube a few centimeters may untangle the tube and allow proper drainage. If the distal drain is in the pleural space, but the proximal port is in the subcutaneous tissue near the thoracic wall, advance the chest tube until both ports enter the pleural space. The chest tube may be located within the soft tissues of the chest, not in the pleural space. This is particularly common with chest tube placements at the bedside in obese patients (94). If the entire chest tube is in the subcutaneous tissue, replace the chest tube. Thoracostomy tubes placed in a fissure usually function adequately but potentially can cause delayed problems such as infection or erode into the pulmonary parenchyma resulting in a bronchopleural fistula (95). Before the chest tube is repositioned or replaced, the risks of the intervention must be weighed against the benefits.

Figure 16: Malpositioning of the chest tube (black arrows) within the soft tissues of the left chest wall
Intrapulmonary placement of a chest tube can be catastrophic. The absence of air or fluid exiting the tube or the occurrence of sudden hemoptysis on chest tube insertion is a clue to this complication. Consequences include severe bleeding (such as hemoptysis), respiratory failure, ineffectual functioning of the chest tube, and formation of a large bronchopleural fistula. In this scenario, first pay attention to the ABCs. Endotracheal intubation proves effective in controlling hemoptysis as well as assuring adequate ventilation. Emergently consult thoracic surgery for a possible thoracotomy (87). If there is no bleeding and a symptomatic pneumothorax persists, it is likely that both drainage ports are in the lung parenchyma. This can be identified on CT scan (93). CT reveals a large number of previously unsuspected intraparenchymal chest tube placements. Remove the chest tube a few centimeters to allow one drainage port to enter the pleural space and decompress the air. Once the acute situation is controlled, replace the chest tube. Attentively observe the patient carefully for bleeding and respiratory compromise. Generally chest tubes inserted too far do not cause acute organ damage, although patients may complain of intractable pain. Instead complications like Horner’s syndrome (96), and injury to the great vessels or esophagus (97) tend to be delayed. A sudden loss of the pulse may signify that the chest tube is impinging on the subclavian artery. Retract the chest tube a

few centimeters, and obtain a chest film to reevaluate its position. If symptoms continue, consider a stat angiogram (90). An additional concern arises when the chest tube encroaches on the mediastinum compressing the coronary arteries possibly provoking angina type symptoms 98. Again, if it appears that the chest tube is too close to the heart withdraw the tube a few centimeters. If the chest tube is in a good position, the anginal symptoms may be secondary to a sympathetic surge. The most severe complication from chest tube malposition is bleeding from damage to the vital organs or the diaphragm. This usually results from either insertion of the chest tube below the fifth intercostal space, or occurs when the diaphragm is paralyzed or when a large effusion masks the exact location of the diaphragm. Immediate treatment involves clamping the tube and consulting surgery. Uncontrolled bleeding may also result from the underlying condition that made chest tube insertion necessary or from an iatrogenic complication (89). If catheterization of the heart or great vessels is suspected, clamp the chest tube and consult thoracic or vascular surgery stat for an emergent thoracotomy.
Figure 17: Extensive liver laceration caused by a misplaced, low chest tube

Patients who undergo emergent tube thoracostomy are at risk for complications. The most common of these complications is chest tube misplacement that can cause potentially life-threatening problems. It is important that the Emergency Physician be familiar with these complications, and appreciates how to manage them. Summary:
1. Be certain of landmarks (‘safe triangle’) when inserting chest tube 2. Once the tube is inserted carefully review the film for proper tube placement. If a
standard anteroposterior radiograph does not conclusively determine does not conclusively determine the position, obtain a lateral or lordotic view of the chest or proceed to chest CT. CT is more useful than plain radiography for establishing chest tube malposition.
3. Anticipate complications before they occur and develop an action plan on how you will manage them.
Case 6: A 30 year-old-woman with a history of depression presents to the ED after being discovered by her family unconscious. They believed that the patient ingested an unknown quantity of her medications (Xanax®, Vicodin®, ibuprofen, Lexapro®, and Respiridol®). The time of the overdose is unknown. Because of the patient's altered mental status, the Emergency Physician decided to protect the airway via endotracheal intubation. Subsequently, a nasogastric tube was inserted in order to instill a charcoal with sorbitol suspension. Soon after the charcoal infusion, the patient began to cough and her oxygenation deteriorated. A chest radiograph demonstrated a new infiltrate in the right mid-lung field just distal to the tip of the NG tube, which clearly was in the right mainstem bronchus. The tube was promptly removed. The patient was treated for aspiration pneumonitis, but multiple complications developed including progressive pneumonia and she ultimately died. In most commercially available nasogastric tubes, the side port is approximately 9 cm from the tip of the tube and both the side port and the tip should be in the stomach. Traditionally the nasogastric tube is inserted blindly into one of the nares. Presuming the average distance from the anterior nasal spine to the cricopharyngeus (tracheoesophageal junction) to be about 20 cm, the esophagus to be 25 cm long, and aiming for the tip of the tube to be positioned 10 cm below the gastro-esophageal junction, secure the nasogastric tube at the 50 to 60 cm mark at the nasal vestibule. After introducing the first 15-20 cm of tubing, flex the head bringing the chin closer to the chest. This maneuver narrows the trachea and opens the esophagus (100). It is also recommended to rotate the patient's head towards either shoulder. This causes the deviation of the feeding tube tip away from the midline laryngeal opening (101). Alternatively, the distance from the nose to the pinna and from the pinna to the xiphoid process, and adding another 5 cm, will place the tip in the fundus . NG tubes may become coiled in the hypopharynx, esophagus, or stomach. If a nasogastric tube forms a loop or coil in its course, it is necessary to straighten out the catheter prior to any further attempts at advancing it. The loop establishes the point of least resistance, and advancing the catheter proximally will only widen the loop, it does not advance the tip. The 'victorious' placement of the tube to its full length is not a good practice. Knots may develop in the stomach when excess tubing is advanced, allowing the tubing to loop back on itself. During tube removal, there should be a low threshold for aborting the procedure if any resistance develops (102).

Figure 18: Nasogastric tube, in the right pleural cavity.
(Reproduced with permission, Pillai JB, Vegas A, Brister S, Thoracic complications of nasogastric tube: review of safe practice. Interact CardioVasc Thorac Surg 2005;4:429-433)
Since insertion of a nasogastric tube entails an element of blindness, there is a real potential for tube misplacement. It is important for physicians inserting nasogastric tubes to be aware of potential dangerous complications. Generally problems arising from nasogastric tube mishaps are divided into thoracic and non-thoracic complications. Reported complication rates range from 0.3% to 15% (100,103-105).

Inadvertent insertion of a nasogastric tube into the tracheopulmonary system during placement is associated with significant morbidity and mortality, especially if left unrecognized (103,106). Both airway penetration and introduction of various chemicals into the lung and pleural spaces may occur prior to recognition of tube misplacement and can be fatal (103,107). Rassias reported a 2% incidence of tracheopulmonary complications among 740 tube insertions with a 0.3% mortality rate (108). Pneumothoraces accounted for approximately 60% of the complications with fifty percent of those affected requiring a chest tube. In 15%, the misdirected bronchial tube did not cause any complications108. To place the risks associated with nasogastric tube placement into perspective, the probability of pneumothorax with central line insertion is in the 1-2% range (109). Nasogastric tubes are contraindicated in the presence of severe facial trauma (cribriform plate disruption), due to the possibility of inserting the tube intracranially (110). In this instance, an orogastric tube may be an alternative.
Figure 19: NG coiled in right nares

Furthermore, anatomic variants of the nasopharynx facilitate malposition of nasogastric tubes. A case report describes a nasogastric tube penetrating the right internal jugular vein at the height of the soft palate, ultimately navigating down the superior vena cava into the right atrium. The tube tracked the concave contour of a deviated nasal septum, perforating the lateral oropharyngeal wall (111). The physicians involved in the initial care of the patient mistakenly assumed the blood in the tube aspirate to be from a gastric bleed. Continued free drainage led to hemodynamic collapse. The eventual diagnosis was made on computerized tomography. Additionally, arbitrary insertion of a nasogastric tube into a patient with a known aberrant right subclavian artery needs to be avoided as this has been reported to cause fatal hematemesis (112).
Figure 20: Coiled NG tube removed by endoscopy

Figure 21: Contrast-filled nasogastric tube runs paravertebrally on the right side and ends in the right atrium
(Reprinted with permission, Duthorn L, Schulte Steinberg H, Hauser H, Neeser G, Pracki P. Accidental intravascular placement of a feeding tube. Anesthesiology 1998;89:251-253.)

Figure 22: Endotracheal tube with knotted orogastric tube.
(Reprinted with permission, Pousman, Robert M. DO; Koch, Stephen M. MD. Endotracheal Tube Obstruction after Orogastric Tube Placement Anesthesiology: Volume 87(5) November
1997 pp 1247-1248)
Less common complications have included nasopharyngeal, esophageal and gastric perforation (113-115), esophageal obstruction (116), and submucosal dissection (117). Signs of such injury are often subtle and require a high degree of suspicion. The appearances of subcutaneous air in the neck on chest radiograph, and the presence of cervical crepitance on physical examination, are valuable signs in the early diagnosis of perforation of the cervical esophagus.
Thoracic complications (108)
• Tracheobronchopleural complications
Bronchial placement leading to atelectasis, pneumonia and lung abscess Bronchial perforation and pleural cavity penetration (i.e., pneumothorax, isocalothorax, empyema and sepsis, pulmonary hemorrhage)

• Intravascular penetration
Erosion into retroesophageal aberrant right subclavian artery Right Internal Jugular vein to right atrium
Non-thoracic complications (108)
• Tube knotting and impaction • Tube obstruction and rupture with syringing • Enteric perforation (esophageal, and duodenum) • Intracranial entry:
Following maxillofacial trauma Following repair of choanal atresia and transnasal transphenoidal surgery
Most clinical indicators of proper tube placement prove too variable to be solely relied upon. Auscultation of air insufflated through the nasogastric tube (the so-called "whoosh" test) is notoriously inaccurate and there are many reports of its ineffectiveness (103,118,119). In several cases where results suggested correct tube placement, feedings were started with disastrous consequences (118). Additionally, care needs to be exercised in injecting air through a feeding tube until proper placement is verified. If a feeding tube is placed directly into the pulmonary parenchyma and then air is injected in order to verify the tube's position, it is theoretically possible to induce a local airway disruption and a pneumothorax. Also one can only speculate the outcome if air had been injected into the nasogastric tube that was inadvertently inserted into the right atrium (111). Similarly, aspiration of gastric contents for confirmation can also be misleading. Research and anecdotal evidence indicate that relying upon the appearance of feeding tube aspirate to rule out nasogastric tube misplacement is fraught with problems as gastric contents can easily mimic respiratory secretions (120). Additional suggested bedside methods employed to confirm proper nasogastric tube placement also reveal pitfalls. Interpreting an absence of respiratory distress following nasogastric tube placement, i.e., lack of coughing and choking, often proves ineffectual, particularly in patients with a decreased level of consciousness or with neurological debilitation where gag and cough reflexes may be suppressed (118). Case reports reveal that large bore nasogastric tubes can enter the respiratory tract without producing symptoms (121). A memo from the Medicines Healthcare products Regulatory Agency (MHRA) warned that blue litmus paper to test acidity/alkalinity of gastric aspirate is not sensitive enough to distinguish between bronchial and gastric secretions (122). Finally, observing for bubbling at the proximal end of the tube is unreliable since the stomach also contains air and could falsely indicate respiratory placement (118). Radiographic imaging is commonly utilized to confirm nasogastric tube position and is strongly recommended prior to initiation of enteral feeding or to the instillation of drugs or other material through the tube, especially as in this case in any patient with an altered mental status or at high risk for malposition (103,123). However, misinterpretation of the radiograph can happen. Hendry reported that of 11 patients with malpositioned nasogastric tubes (all of which had radiography for tube placement confirmation) the malposition was not identified in three (27%) (103). Nasogastric tube positioning in the left costophrenic sulcus is difficult to distinguish from intragastric placement especially on a supine anterior-posterior chest radiograph such as those commonly obtained in the ER or ICU (124).

Capnography, usually used to confirm correct endotracheal tube placement by documenting expired carbon dioxide, has been suggested as a quick test to also verify suitable nasogastric tube position. A small study utilized this phenomenon in a reverse manner to confirm the placement of the nasoenteric tube into the alimentary tract rather than the tracheobronchial tree by demonstrating the absence of CO2 within the tube lumen (125). Another study by Araujo confirmed these results in a report of 53 patients (126). An erroneous notion is that the intubated patient is protected from accidental misplacement of the nasogastric tube into the lung. The endotracheal tube, instead of deflecting the feeding tube, may actually increase the risk of pulmonary entry by preventing glottic closure and inhibiting swallowing. Nasogastric tubes can readily squeeze past the low-pressure endotracheal cuffs. Additionally, altered mental status and sedation increase the risk of tube misplacement, as does a prior episode of a misdirected nasogastric tube. As previously mentioned it is probably prudent to confirm nasogastric tube position with a chest x-ray prior to infusing any solution through the tube. High risk patients include:
• Intubated and sedated • Elderly • Mentally obtunded • Following Lung transplantation • Repeated attempt after earlier pulmonary misadventure
Summary Points
1. Traditionally, nasogastric tubes have been inserted blindly. 2. The X-ray remains the gold standard to verify the correct placement 3. Traditional bedside 'confirmatory' signs of gastric placement may not be reliable and
should not be used as a substitute to the X-ray. 4. Pneumothorax is the commonest pulmonary complication. 5. Initial 30 cm is the crucial damage limiting distance, as it is at the tracheoesophageal
transition zone. 6. The final nasogastric-position is ideally at 50-60 cm from the incisor teeth. 7. Insertion of excess tubing is to be avoided. 8. Tracheal entry can be detected using small, disposable capnometers.

References: 1. Schenkel S. Promoting patient safety and preventing medical error in Emergency Departments. Acad Emerg Med 200;7 (11):1204-1221) 2. Accessed http://www.psa.state.pa.us/psa/site/default.asp November 15, 2005 3. Knapp S. Kofler J. Stoiser B. Thalhammer F. Burgmann H. Posch M. Hofbauer R. Stanzel M. Frass M. The assessment of four different methods to verify tracheal tube placement in the critical care setting. Anesthesia & Analgesia. 1999; 88(4):766-70. 4. Wilson CW, Benumof JL. Respiration in anaesthesia pathophysiology and clinical update. Anesth Clin North Am 1998;16:29-75. 5. Schwartz DE, Matthay MA, Cohen NH: Death and other complications of emergency airway management in critically ill adults. Anesthesiology 1995; 82:367-76; 6. Conley JM, Smith DJ: Emergency endotracheal intubation by respiratory care personnel in a community hospital. Respir Care 1981; 26:336-8; 7. Stauffer JL, Olson DE, Petty, TL: Complications and consequences of endotracheal intubation and tracheotomy: A prospective study of 150 critically ill adult patients. Am J Med 1981; 70:65-76. 8. .Caplan RA, Posner KL, Ward RJ, et al. Adverse respiratory events in anesthesia: a closed claims analysis. Anesthesiology 1990;72:828-833. 9. Birmingham PK, Cheney FW, Ward RJ: Esophageal intubation: A review of detection techniques. Anesth Analg 65:886-891, 1986. 10. (Morray JP, Geiduschek JM, Caplan RA, et al: A comparison of pediatric and adult anesthesia closed claims. Anesthesiology 1993;78:461-467. 11. Gannon K; Mortality associated with anesthesia: a case review study. Anesthesia 1991:46;962-6. 12. Kasper C, Deem S The Self-inflating Bulb to Detect Esophageal Intubation during Emergency Airway Management. Anesthesiology 1998; 88(4):898-902. 13. Bozeman WP, Hexter D, Liang HK, Kelen GD. Esophageal detector device versus detection of end-tidal carbon dioxide level in emergency intubation. Ann Emerg Med 1996;27:595-9. 14. Sakles JC, Laurin EG, Rantapaa AA, Panacek EA. Airway management in the Emergency Department: a one-year study of 610 tracheal intubations. Ann Emerg Med. 1998;31:325-32. 15. Jenkins WA, Verdile VP, Paris PM. The syringe aspiration technique to verify endotracheal tube position. Am J Emerg Med 1994;12:413-416. 16. Katz SH, Falk JL. Misplaced endotracheal tubes by paramedics in an urban emergency medical services system. Ann Emerg Med 2001; 37(1): 32-37. 17. Kelly JJ, Eynon CA, Kaplan JL, et al. Use of tube condensation as an indicator of endotracheal tube placement. Ann Emerg Med. 1998;31:575-578.

18. Andersen KH, Hald A. Assessing the position of the tracheal tube. The reliability of different methods. Anaesthesia. 1989;44:984-985. 19. Pollard BJ, Junius F. Accidental intubation of the oesophagus. Anaesth Intensive Care. 1980;8:183-186. 20. Cummings RO, Hazinski MF. Guidelines based on the principle "first, do no harm": new guidelines on tracheal tube confirmation and prevention of dislodgment. Circulation. 2000;102(8 Suppl):I380-I384. 21. Williamson JA, Webb RK, Cockings J, et al. The Australian Incident Monitoring Study. The capnograph: applications and limitations - an analysis of 2000 incident reports. Anaesth Intensive Care. 1993;21:551-557. 22. Clyburn P, Rosen M. Accidental oesophageal intubation. Br J Anaesth 1994;73:55-63. 23. DeKeyser V, Woods D: Fixation errors: Failures to revise situation assessment in dynamic and risky systems, Systems Reliability Assessment. Edited by Coloumbo A, Bustamante A. Dordrechty, Khiver Academic, 1990, pp 231-51. 24. Haridas RP. Condensation on tracheal tubes is commonly seen with oesophageal intubation. Br J Anaesth 1995;75:115-6. 25. Charters P. Normal chest expansion with oesophageal placement of a tracheal tube [letter]. Anaesthesia. 1989;44:365. 26. Howells TH, Riethmulller RJ. Signs of endotracheal intubation. Anaesthesia 1980 ;35(10):984-6. 27.Guggenberger H, Lenz G, Federle R. Early detection of inadvertent oesophageal intubation: pulse oximetry vs. capnography. Acta Anesthesiol Scand. 1989;33:112-115. 28. Vaghadia H, Jenkins LC, Ford RW. Comparison of end-tidal carbon dioxide, oxygen saturation and clinical signs for the detection of oesophageal intubation. Can J Anaesth. 1989;36:560-564. 29. Wee MYK. The esophageal detector device: a rapid and accurate method for assessing tracheal versus esophageal intubation in the porcine model. Ann Emerg Med 1992;21:1073-6. 30. Li J. A prospective multicenter trial testing the SCOTI device for confirmation of endotracheal tube placement. J Emerg Med 2001;20:231-9. 31. Andres AH, Langenstein H. The esophageal detector device is unreliable when the stomach has been ventilated. Anesthesiology 1999;91:566-8. 32. Ardagh M, Moodie K. The esophageal detector device can give false positives for tracheal intubation. J Emerg Med. 1998;16:747-749. 33. Kasper CL, Deem S. The self-inflating bulb to detect esophageal intubation during emergency airway management. Anesthesiology. 1998;88:898-902. 34. Pelucio M, Halligan L, Dhindsa H. Out-of-hospital experience with the syringe esophageal detector device. Acad Emerg Med. 1997;4:563-568.

35. Ornato JP, Shipley JP, Racht EM, et al. Multicenter study of a portable, hand size, calorimetric end-tidal carbon dioxide detection device. Ann Emerg Med 1992;21:518-23. 36. Standards for Basic Anesthetic Monitoring" of the American Society of Anesthesiologists (ASA) pages 462-463 of the ASA’s 1999 Directory of Members and on the ASA website: http://www.asahq.org accessed December 3, 2005. 37. Sayah AJ, Peacock WF, Overton DT. End-tidal C02 measurement in the detection of esophageal intubation during cardiac arrest. Ann Emerg Med. 1990;19:857-860. 38. Hayden SR, Sciammarella J, Viccellio P, et al. Colorimetric end-tidal C02 detector for verification of endotracheal tube placement in out-of-hospital cardiac arrest. Acad Emerg Med. 1995;2:499-502; 39. Bhende MS, Thompson AE, Cook DR, et al. Validity of a disposable end-tidal C02 detector in verifying endotracheal tube placement in infants and children. Ann Emerg Med. 1992;21:142-5. 40. O'Connor RE, Swor RA. Verification of endotracheal tube placement following intubation. Prehosp Emerg Care 1999;3:248-50. 41. MacLeod BA, Heller MB, Gerard J, et al. Verification of endotracheal tube placement with colorimetric end-tidal CO2 detection. Ann Emerg Med. 1991;20:267-70. 42. Smith GM, Reed JC, Choplin RH. Radiographic detection of esophageal malposition of endotracheal tubes. AJR 1990;154:23-6. 43. McCoy EP, Russell WJ, Webb RK. Accidental bronchial intubation. An analysis of AIMS incident reports from 1988 to 1994 inclusive. Anaesthesia. 1997;52:24-31. 44. Chan YK. Radiological diagnosis of accidental oesophageal intubation. Singapore Med J. 1994;35:327-8. 45. Ballester EE, Torres A, Rodriguez-Roisin R, Agusti-Vidal A. Pneumoperitoneum: an unusual manifestation of improper oral intubation. Crit Care Med 1985;13:138-9. 46. Werman HE, Falcone RE. Glottic positioning of the endotracheal tube tip: A diagnostic dilemma. Ann Emerg Med 1998;31 (5):643-646. 47. Brunel W. Coleman DL. Schwart DE, et al. Assessment of routine chest roentgenograms and the physical examination to confirm endotracheal tube position. Chest 1989;96:1043-1045. 48. Owen H, Waddell-Smith I. Dental trauma associated with anaesthesia. Anaesth Intensive Care 2000; 28: 133–45. 49. Fan CM, Chow-In Ko, P, Tsai KG, et al. Tracheal rupture complicating emergent endotracheal intubation. Am J Emerg Med 2004;22:289-293. 50. Chen EH, Logman ZM, Glass PS, et al. A case of tracheal injury after emergent endotracheal intubation: a review of the literature and causalities. Anesth Analg. 2001;93:1270-1271. 51. Rollins RJ, Tocino I. Early radiographic signs of tracheal rupture (1987). Am J Roentgenol.;148:695-698.

52. Mickiewicz M, Dronen SC, Younger JG. Central Venous Catheterization and Central Venous Pressure Monitoring, in Roberts JR, Hedges JR (eds): Clinical Procedures in Emergency Medicine, 4th ed. Philadelphia: Saunders: 413-440. 53. Merrer J, De Jonghe B, Golliot F, et al. Complications of femoral and subclavian venous catheterization in critically ill patients: a randomized controlled trial. JAMA. 2001;286:700-7.; 54. Durbec O, Viviand X, Potie F, Vialet R, Albanese J, Martin C. A prospective evaluation of the use of femoral venous catheters in critically ill adults. Crit Care Med. 1997;25:1986-9. 55. Sznajder JI, Zveibil FR, Bitterman H, Weiner P, Bursztein S. Central vein catheterization: failure and complication rates by three percutaneous approaches. Arch Intern Med. 1986;146:259-61. 56. Ruesch S, Walder B, Tramer M. Complications of Central Venous Catheters: Internal Jugular versus Subclavian access-A Systematic Review. Crit Care Med. 2002;30:454-60. 57. McGee DC, Gould MK. Preventing complications of central venous catheterization. N Engl J Med. 2003;348:1123-33. 58. Mansfield PF, Hohn DC, Fornage BD, Gregurich MA, Ota DM. Complications and failures of subclavian-vein catheterization. N Engl J Med 1994;331:1735-1738. 59. Fares LG II, Block PH, Feldman SD. Improved house staff results with subclavian cannulation. Am Surg 1986;52:108-111. 60. Martin C, Eon B, Auffray JP, Saux P, Gouin F. Axillary or internal jugular central venous catheterization. Crit Care Med. 1990;18:400-2. 61. Lefrant JY, Muller L, Nouveoon E et al When subclavian vein cannulation attempts must be stopped? Anesthesiology Supplement 1998. ASCCA abstract B11. 62. Robinson JF, Robinson WA, Cohn A, Garg K, Armstrong JD. Perforation of the great vessels during central venous line placement. Arch Intern Med 1995; 155(11): 1225-8. 63. Duntley P, Siever J, Korwes ML, Harpel K, Heffner JE. Vascular erosion by central venous catheters. Chest 1992; 101: 1633–8. 64. Collier PE, Ryan JJ, Diamond DL. Cardiac tamponade from central venous catheters. Report of a case and review of the English literature. Angiology 1998; 35: 595–600. 65. Slonim A, Landucci DL, et al. Cannulation of the Internal Jugular Vein: Is Postprocedural Chest Radiography Always Necessary? Crit Care Med. 1999; 27: 1819-1823. 66. Ambesh SP, Dubey PK, Matreja P, et al. Manual Occlusion of the Internal Jugular Vein During Subclavian Vein Catheterization: A Maneuver to Prevent Misplacement of Catheter into Internal Jugular Vein. Anesthesiology. 2002; 97(2): 528-529. 67. Sterner S, Plummer DW, Clinton J, et al. A Comparison of the Supraclavicular Approach and the Infraclavicular Approach for Subclavian Vein Catheterization. Ann Emerg Med. 1986; 15: 421-424. 68. Dunbar R.D., Mitchell R., Lavine M., Aberrant locations of central venous catheters. Lancet 1981; 1 : 711-715.

69. Ely EW, Hite RD, Baker AM, Johnson MM, Bowton DL, Haponik EF. Venous air embolism from central venous catheterization: a need for increased physician awareness. Crit Care Med 1999; 27: 2113-2117. 70. Vesely TM. Embolism during Insertion of Central Venous Catheters. JVIR 2001. 12:1291-1295. 71. Tyburski, JG., Joseph, A.Thomas, G. Delayed pneumothorax after central venous access: a potential hazard. American Surgery 1993; 59(9), 587-589. 72. Walters, G., Kahn, A., Jescovitch, A. (1997, January). Efficacy of a central venous access service. Southern Medical Journal, 1997; 90(1), 37-39. 73. Plewa MC; Ledrick D Delayed tension pneumothorax complicating central venous catheterization and positive pressure ventilation. Am J Emerg Med,1995; 13:532-5. 74. Denys BG, Uretsky BF, Reddy PS. Ultrasound-assisted cannulation of the internal jugular vein: a prospective comparison to the external landmark-guided technique. Circulation 1993; 87: 1557-1662; 75. Skolnick ML. The role of sonography in the placement and management of jugular and subclavian central venous catheters. AJR 1994; 163: 291-295; 76. Hind D, Calvert N, McWIliams Ret al. Ultrasonic Locating Devices for Central Venous Cannulation: Meta-Analysis. BMJ. 2003; 327(7411): 361. 77. Lefrant JY, Cuvillon P, Benezet JF, et al. Pulsed Doppler ultrasonography guidance for catheterization of the subclavian vein: a randomized study. Anesthesiology 1998;88:1195-1201. 78. Lum TE, Fairbanks RJ, Pennington EC, Zwemer FL. Profiles in Patient Safety: Misplaced Femoral Line Guidewire and Multiple Failures to Detect the Foreign Body on Chest Radiography. Acad Emerg Med 2005; Vol. 12 (7): 658-662. 79. Schummer W, Schummer C, Gaser E, Bartunek R. Loss of the guide wire: mishap or blunder? Br J of Anaesth, 2002, Vol. 88,(1) 144-146. 80. accessed from www.trauma.org 12/18/05 81. Etoch SW, Bar-Natan MF, Miller FB, Richardson JD. Tube thoracostomy. Factors related to complications.Arch Surg. 1995; 130(5):521-5. 82. Chan L, Reilly KM, Henderson C, Kahn F, Salluzzo RF. Complication rates of tube thoracostomy. Am J Emerg Med. 1997 Jul;15(4):368-70. 83. Brasel KJ, Layde PM, Hargarten S, Evaluation of Error in Medicine: Application of a Public Health Model. Academic Emergency Medicine 2000; Vol 7 (11) 1298-1302. 84. Callop NA, Kim S, Sahn SA. Analysis of tube thoracostomy performed by pulmonologists at a teaching hospital. Chest 1997;112(3)709-713. 85. Miller KS, Sahn SA. Chest tubes: indications, techniques, management and complications. Chest 1987;91:258–264.

86. Deneville M. Morbidity of percutaneous tube thoracostomy in trauma patients. Eur J Cardiothorac Surg 2002; 22(5):673–678. 87. Millikan JS, Moore EE, Steiner E, Aragon GE, Van Way CW. Complications of tube thoracostomy for acute trauma. Am J Surg 1980; 140(6):738–741. 88. Shapira OM, Aldea GS, Kupferschmidj J, et al. Delayed perforation of the esophagus by a closed thoracostomy tube. Chest 1993;104:1897-8. 89. Rashid MA, Acker A. Cardiac Herniation with Catheterization of the Heart, Inferior Vena Cava, and Hepatic Vein by a Chest Tube. J Trauma 1998; 45(2):407-409. 90. Moskal TL; Liscum KR; Mattox KL. Subclavian Artery Obstruction by Tube Thoracostomy. J Trauma 1997; 43(2):368-369. 91. Committee on Trauma, American College of Surgeons. Advanced trauma life support. Chicago: American College of Surgeons, 1997. 92. Gayer G, Rozenman J, Hoffmann C, Apter S, Simansky DA, Yellin A, Itzchak Y CT diagnosis of malpositioned chest tube. Br J Radiol 2000; 3(871):786–790. 93. Baldt MM, Bankier AA, Germann PS, et al. Complications after emergency tube thoracostomy: Assessment with CT. Radiology 1995;539-543. 94. Miller KS, Sahn SA. Chest tubes. Indications, technique, management and complications. Chest. 1987;91:258-264. 95. Curtin JJ, Goodman LR, Quebbeman EJ, et al. Thoracostomy tubes after acute chest injury:m relationship between location in a pleural fissure and function. AJR 1994;163:1339-1342. 96. Bourque PR. Paulus EM. Chest-tube thoracostomy causing Horner's syndrome. Canadian Journal of Surgery.1986; 29(3):202-3. 98. Johnson JF. Wright DR. Chest tube perforation of esophagus following repair of esophageal atresia. Journal of Pediatric Surgery. 1990;25(12):1227-30. 99. Svedjeholm R, Hakanson E. Postoperative myocardial schemia caused by chest tube compression of vein graft. Ann Thorac Surg. 1997;64:1806-1808. 100. Pillai JB, Vegas A, Brister S, Thoracic complications of nasogastric tube: review of safe practice. Interact CardioVasc Thorac Surg 2005;4:429-433. 101. Phillips DE, Sherman IW, Asgarali S, Williams RS. How far to pass a nasogastric tube. J R Coll Surg Edinb 1994;39:295-296. 102. Dinsmore RC, Benson JF. Endoscopic removal of a knotted nasogastric tube lodged in the posterior nasopharynx. Southern Medical Journal 1999;92:1005-1007. 103. Hendry PJ, Akyurekli Y, Mclntyre R, et al.: Bronchopleural complications of nasogastric feeding tubes. Crit Care Med 1986, 14:892-894. 104. Harris MR, Huseby JS. Pulmonary complications from nasoenteral feeding tube insertion in the intensive care unit: incidence and prevention. Crit Care Med 1989; 17:917-919.

105. McWey RE, Curry NS, Schabel SI, et al. Complications of nasoenteric feeding tubes. Am J Surg 1988; 155:253-257. 106. Odocha O, Lowery RC, Mezghebe HM, et al.: Tracheopleuropulmonary injuries following enteral tube insertion. J Natl Med Assoc 1989, 81:275-281. 107. Balogh GJ, Adler SJ, VanderWoude J, Glazer HS, Roper C, Weyman PJ: Pneumothorax as a complication of feeding tube placement. AJR 1983; 141: 1275-1277. 108. Rassias AJ, Ball PA, Corwin HL. A prospective study of tracheopulmonary complications associated with the placement of narrow-bore enteral feeding tubes. Critical Care 1998;2:25-28. 109. Hagley MT, Martin B, Gast P, et al.: Infectious and mechanical complications of central venous catheters placed by percutaneous venipuncture and over guidewires. Crit Care Med 1992, 20:1426-1430. 110. Gregory JA, Turner PT, Reynolds AF: A complication of nasogastric intubation: Intracranial penetration. J Trauma 1978; 18:823-4. 111. Duthorn L, Schulte Steinberg H, Hauser H, Neeser G, Pracki P. Accidental intravascular placement of a feeding tube. Anesthesiology 1998;89:251-253. 112. Merchant FJ, Nichols RL, Bombeck CT. Unusual complication of nasogastric esophageal intubation-erosion into an aberrant right subclavian artery. J Cardiovasc Surg 1977;18:147-150. 113. Siemers PT, Reinke RT. Perforation of the nasopharynx by nasogastric intubation: a rare cause of left pleural effusion and pneumomediastinum. Am J Roentgenol 1976; 127:341-343. 114. Tiller HJ, Rhea WG. Iatrogenic perforation of the esophagus by a nasogastric tube. Am J Surg 1984; 147:423-425. 115. Ghahremani GG, Turner MA, Port RB. Iatrogenic intubation injuries of the upper gastrointestinal tract in adults. Gastrointest Radiol 1980; 5:1-10. 116. Iragu I, Fulda GJ. Esophageal obstruction secondary to concretions of tube-feeding formula. Crit Care Med 1995; 23:208-210. 117. Lind LJ, Wallace DH. Submucosal passage of a nasogastric tube complicating attempted intubation during anesthesia. Anesthesiology 1978; 49:145-147. 118. Metheny NA, Aud MA, Ignatavicius DD. Detection of improperly positioned feeding tubes. J Healthc Risk Management 1998;18(3):37-48; 119. Dobranowski J, Fitzgerald JM, Baxter F, Woods D. Incorrect positioning of nasogastric feeding tubes and the development of pneumothorax. Can Assoc Radiol J 1992;43(1):35-9. 120. Theodore AC, Frank JA, Ende J, et al. Errant placement of nasoenteric tubes. A hazard in obtunded patients. Chest 1984;86(6):931-3. 121. Torrington KG, Bowman MA. Fatal hydrothorax and empyema complicating a malpositioned nasogastric tube. Chest 1981;79(2):240-2. 122. MHRA Notice MHRS/MS/2004/026

123. Boyes RJ, Kruse JA: Nasogastric and nasoenteric intubation. Crit Care Clin 8: 865?878, 1992. 124. Valentine RJ, Turner WW Jr: Pleural complications of nasoenteric feeding tubes. J Parenter Enteral Nutr 9: 605-607, 1985. 125. Thomas BW, Falcone RE. Confirmation of Nasogastric Tube Placement by Colorimetric Indicator Detection of Carbon Dioxide: A Preliminary Report. Journal of the American College of Nutrition, 1998; 17 (2), 195-197. 126. Araujo P, Carlos E, Melhado ME, Gutierrez FJ, Maniatis T, Castellano MA. Use of capnometry to verify feeding tube placement. Critical Care Medicine 2002;30:2255-2259.