Embed Size (px)
Citation preview

Laurent J SALOMON
Fetal growth standards:TheIntergrowth approach
Onbehalf oftheINTERGROWTH-21stProject.Many thanks toArisPapageorghiou,JoseVillar andallother contributors

• Growth monitoring (GM) is an integral and undisputedcomponent of evidence-based antenatal and new-born careworldwide, as it is for infants and children.
• Public Heath problem associated with short, medium and longterm adverse outcomes
• Poor screening results
IUGR AND FETAL BIOMETRY…
Villar et al Am J Obstet Gynecol 2015; 213: 494-9

• A comprehensive set of fully integrated anthropometric measures toevaluate human growth from conception to infancy so that consistentjudgments can be made about the appropriateness of fetal and infantgrowth.
• Homogeneous standards before and after birth, developed using thesame adequate methodology across a large sample of fetuses andnewborns appropriately selected…
• Consensus about definitions, cut-offs and management policies.
WHAT IS DESIRABLE…?

• Reference charts that are heterogeneous: they are derived from local,unselected samples with inadequate methods and poor characterization oftheir putatively healthy populations.
• Management policies are variable: different charts, different definitions forIUGR, different thresholds, different managements…
WHAT WE HAVE…

TOO MANY DIFFERENT REFERENCES
Crown-rump length / gestational age estimation• 29 published charts• Only 4 charts satisfied minimum quality criteria
Napolitano et al (2014) BJOGFetal growth monitoring by ultrasound• 83 published charts• Only 12 charts used reliable dating method
Ioannou et al (2012) BJOGBirth weight charts• 102 published charts• Only 8 charts satisfied minimum quality criteria
Giuliani et al (2015) Acta PaediatricaPreterm postnatal growth charts• 61 published longitudinal charts• Limitations in GA estimation, anthropometric measures, feeding
Giuliani et al (2016) AJCN

28 weeks 32 weeks 36 weeks Author 10th
centile 50th centile
SD 10th centile
50th centile
SD 10th centile
50th centile
SD
Chitty25 212.92 230.57 13.77 248.97 269.71 16.18 282.59 306.41 18.58 Verburg91 224.30 239.40 11.78 261.10 278.60 13.65 292.10 312.20 15.68 Leung60 218.95 233.90 11.66 256.61 273.56 13.22 290.68 309.64 14.79 Sunsaneevithayakul86 217.04 232.58 12.12 254.89 273.26 14.33 289.72 309.12 15.13 Johnsen52 223.00 240.00 13.26 262.00 282.00 15.60 299.00 321.00 17.16 Jeanty48 208.01 225.24 13.44 245.13 262.36 13.44 276.07 293.30 13.44 Paladini73 218.20 239.30 16.46 252.30 275.00 17.71 284.30 307.00 17.71 Kurmanavicious55 213.21 231.78 14.49 249.60 270.61 16.39 283.33 306.78 18.29
Descriptive charts reflect how fetuses growunder particular conditions
Ioannou et al. BJOG, 2012Salomon et al., UOG, 2005
THE IMPACT OF THE CHOICE OF REFERENCE CHARTS

3rd centile15th centile
Gestational age
Feta
lHC

- Many are developed with poor methodology
- Population distributions ARE NOT standards
- May mask aberrations from optimal growth
- Assume SGA is the same in each population
- Show how fetuses have grown
Ioannou et al 2012
De Onis et al 2004
Stirnemann et al 2016
LOCAL DESCRIPTIVE REFERENCES

Human growth worldwide should be evaluated using international standards describing how individuals should grow’
“
Report of WHO Expert Committee 1995Physical Status: The Use and Interpretation of Anthropometry, Technical Report
Series No. 854
WHO RECOMMENDATIONS (1995)

• The distribution of biometry within a population does not constitute areference
• Local charts describe growth at a given time point and under preciseconditions
• ”Prescriptive” growth standards describe how babies should grow whennutritional, environmental and health constraints on growth are minimal.
.
LOCAL DESCRIPTIVES CHARTS VS PRESCRIPTIVE STANDARDS

‘The new growth standards are referable to all children everywhere, clearly show that all children in the world can and should grow equally well, and also demonstrate that in today’s world adequate nutrition, environment, and health are stronger determinants of growth than are gender or ethnicity’.
20th April 2006
1 year 2 years 3 years 4 years 5 years
WHO Child Growth StandardsDe Onis et al. Acta Paediatr 2006;450:1-101, De Onis et al (2004) Food Nutr Bull
INTERNATIONAL « PRESCRIPTIVE » WHO CHILD GROWTH STANDARDS

NEW INTERNATIONAL “PRESCRIPTIVE” FETAL, NEWBORN & PRETERM POSTNATAL STANDARDS
1 year 2 years 3 years 4 years 5 years
INTERGROWTH-21st Project

>300 27 18Health care providers
& researchersOrganisations worldwide Countries

INTERGROWTH STUDY
Seattle, USA
Pelotas, Brazil
Oxford, UKTurin, Italy
Beijing, China
Nairobi, Kenya
Muscat, OmanNagpur, India
INTERGROWTH-21st sites

• CENTER CRITERIA : Low BW<10%, mean BW>3100g, perinatal mortality <20 / 1000births, >75% of mother with predefined socio-economic and educational status, noenvironmental toxic, altitude <1600m
• INDIVIDUAL CRITERIA : Health indicators (age, weight, height, BMI, no pathologies…..)
• CRITERIA AT INCLUSION: regular cycles, certain LMP, no hormonal treatment orbreastfeeding over the past 3 months, first trimester US measurements in accordancewith LMP …
Villar et al. BJOG, 2013
NUTRITIONAL, ENVIRONMENTAL AND HEALTH CONSTRAINTSON GROWTH ARE MINIMAL...

“Healthy” mother criteria for Fetal Growth Longitudinal Study
a) aged ≥18 and ≤35 years; b) BMI ≥18.5 and <30 kg/m2; c) height ³ 153 cm;d) singleton pregnancy; e) a known LMP with regular cycles (defined as a 26-30 day cycle in the previous 3 months), without hormonal contraceptive use, pregnancy or
breastfeeding in the 3 months before pregnancy; f) natural conceptiong) no relevant past medical history (refer to screening form), with no need for long-term medication (including fertility treatment and over-the-counter
medicines, but excluding routine iron, folate, calcium, iodine or multivitamin supplements);h) no evidence of socio-economic constraints likely to impede fetal growth identified using local definitions of social risk;i) no use of tobacco or recreational drugs such as cannabis in the 3 months before or after becoming pregnant; j) no heavy alcohol use (defined as > 4 units (40ml pure alcohol) per week) since becoming pregnant;k) no more than one miscarriage in the 2 previous consecutive pregnancies; l) no previous baby delivered pre-term (<37 weeks) or with a birth weight <2500g or >4500g; m) no previous neonatal or fetal death, previous baby with any congenital malformations, and no evidence in present pregnancy of congenital disease or
fetal anomaly; n) no previous pregnancy affected by pre-eclampsia/eclampsia, HELLP syndrome or a related pregnancy-associated condition; o) no clinically significant atypical red cell alloantibodies; p) negative urinalysis; q) systolic blood pressure <140 mmHg and diastolic blood pressure < 90 mmHg; r) haemoglobin ≥11 g/dl; s) negative syphilis test and no clinical evidence of any other sexually transmitted diseases, including clinical Trichomoniasis; t) not in an occupation with risk of exposure to chemicals or toxic substances, or very physically demanding activity to be evaluated by local standards.
Also women should not be conducting vigorous or contact sports, as well as scuba diving or similar activities
Criteria defining a low-risk study population as healthy and well-nourished (both before and during pregnancy) to ensure that fetal growth is optimal
Villar et al. BJOG, 2013

Low-risk pregnancies
Medium-high risk pregnancies
Fetal Growth Longitudinal Studyn = 4,607
Low-risk pregnancies
Medium-high risk pregnancies
è International Fetal Growth Standards
Low risk pregnanciesn = 20,324
POPULATION IN THE INTERGROWTH STUDY

Training
Standardisation• CRL• Biometry
Audit & quality control• Data • Image• External review
Papageorghiou et al. BJOG, 2013
QUALITY CONTROL

• Biparietal diameter • Occipito-frontal diameter• Head circumference• Transverse abdominal diameter• Anterio-posterior abdominal diameter• Abdominal circumference• Femur length
Measurements at each scan >14+0 weeks, every 5 +/- 1 week:
Measurements obtained 3 times from 3 separately obtained images ofeach structure in blinded fashion (no measurement visible) andsubmitted electronically
Philips HD9
Papageorghiou et al. BJOG, 2013
PRENATAL MEASUREMENTS

Fat-freemassindicatorsare:
• Resistanttoskewinginresponseto�excessivenutrition�
• Affectedbyunder-nutritionorinfectionbuttheseareunlikelytoberelevantinhealthypopulations
• Normallydistributed(unlikefat-relatedindicators)
• Moreprecisethanfat-relatedmeasures
• UsedintheWHOgrowthstandards
• Ex:CRL,HC…
Adapted from: WHO/MGRS, Acta Paed, 2006

HC : UK, USA, ITALY
5010
015
020
025
030
035
0
HC (m
m)
10 15 20 25 30 35 40 45Gestational age (weeks)
UK 616 USA 184 Italy 426

5010
015
020
025
030
035
0
HC (m
m)
10 15 20 25 30 35 40 45Gestational age (weeks)
UK 616 USA 184 Italy 426 China 606
HC: UK, USA, ITALY, CHINA

5010
015
020
025
030
035
0
HC (m
m)
10 15 20 25 30 35 40 45Gestational age (weeks)
UK 616 USA 184 Italy 426 China 606 India 598
HC: UK, USA, ITALY, CHINA, INDIA

5010
015
020
025
030
035
0
HC (m
m)
10 15 20 25 30 35 40 45Gestational age (weeks)
UK 616 USA 184 Italy 426China 606 India 598 Kenya 595
HC: UK, USA, ITALY, CHINA, INDIA & KENYA

5010
015
020
025
030
035
0
HC (m
m)
10 15 20 25 30 35 40 45Gestational age (weeks)
UK 616 USA 184 Italy 426 China 606India 598 Kenya 595 Oman 554
HC: UK, USA, ITALY, CHINA, INDIA, KENYA, OMAN

5010
015
020
025
030
035
0
HC (m
m)
10 15 20 25 30 35 40 45Gestational age (weeks)
UK 616 USA 184 Italy 426 China 606India 598 Kenya 595 Oman 554 Brazil 304
HC: UK, USA, ITALY, CHINA, INDIA, KENYA, OMAN, BRAZIL

SITE STANDARDISED DIFFERENCES(FETAL GROWTH LONGITUDINAL STUDY)

INTERGROWTH CHARTS ARE PRESCRIPTIVE STANDARDS, THEY REPRESENT ‘HEALTHY’ GROWTH OF A NORMAL POPULATION
IT SUGGESTS A TARGET TO ACHIEVE
INTERGROWTH STUDY


Equations for the mean and SD (mm) of each fetal biometry measurement according to exact gestational age (weeks)
Regressionequation
Mean −28.2849+1.69267xGA2−0.397485xGA2xlog(GA)
SD 1.98735+0.0136772xGA3−0.00726264xGA3xlog(GA)+0.000976253xGA3xlog(GA)2
Mean 5.60878+0.158369xGA2−0.00256379xGA3
SD exp(0.101242+0.00150557xGA3−0.000771535xGA3xlog(GA)+0.0000999638xGA3xlog(GA)2)
Mean −12.4097+0.626342xGA2−0.148075xGA2xlog(GA)
SD exp(−0.880034+0.0631165xGA2−0.0317136xGA2xlog(GA)+0.00408302xGA2xlog(GA)2)
Mean −81.3243+11.6772xGA−0.000561865xGA3
SD −4.36302+0.121445xGA2−0.0130256xGA3+0.00282143xGA3xlog(GA)
Mean −39.9616+4.32298xGA−0.0380156xGA2
SD exp(0.605843−42.0014xGA-2+0.00000917972xGA3)
HeadCircumference
BiparietalDiameter
OccipitofrontalDiameter
AbdominalCircumference
FemurLength

• Growth differs among population because of genetic/ethnic differences. Not because ofhealth, nutrition or socio-economic differences.
• The proportion of abnormal growth (either over or undergrowth) is 10 % (or 5%) all overthe world.
• Local references should be updated every X years as a results of change in normal growthrather than as a results of an improve or decrease in health status…
• Screening and management policies among different populations cannot be compared
DESCRIPTIVE CHARTS: SOME ERRONEOUS UNDERLYING HYPOTHESIS…

• At least 116 definitions of self-reported race or ethnicity inthe biomedical literature
• Most populations have large genetic admixture due toglobal migration, invasions, refugees etc.
• Actually, the variability in skeletal growth WITHIN apopulation is larger than the variability BETWEENpopulations when nutrition and health needs are met(Lancet Diabetes Endocrinol 2014; 2: 781-92)
HOW TO JUSTIFY LOCAL CHARTS ?
Nature 2014; 513: 409-412

FETAL CRL FETAL HC
NEWBORN LENGTH
PRETERM INFANT LENGTH
INFANT LENGTH
WHO-MGRS (2006)
CHILD HEIGHT
HABICHT (1974)
VARIANCE BETWEEN STUDY SITES 1.9% 2.6% 3.5% 0.2% 3.4% 3.0%
VARIANCE AMONG INDIVIDUALS WITHIN A SITE
- 18.6% - 57.1% 70.0% -
UNEXPLAINED VARIANCE 98.1% 78.8% 96.5% 42.7% 26.6% -
VARIANCE ANALYSIS
Villar et al Am J Obstet Gynecol 2015; 213: 494-9

There are no major differences in growth potential between populations

Fetal Head Circumference

Fetal Head Circumference

Fetal Head Circumference

Standardised Study Discrepancy

www.worldmapper.org, Sep 2014
THE WORLD…

www.worldmapper.org, Aug 2015
PERINATAL MORTALITY…

Implications:ratesofsmallforgestationalage(<10th centile)
0
10
20
30
40
50
60
70
Data from: Kozuki et al JAMA Ped 2015
LOCAL charts = 10%
% SG
A
INTERGROWTH-21st
Standards = 24%

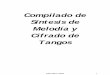
Implicationsfordevelopedpopulations:overweightatbirth

12.9 12.2 12.7 12.7 12.7 13.0
10.69.9 9.9
8.611.5
12.714.4
16.5
19.118.4
19.2
21.420.4
0
5
10
15
20
25
33 34 35 36 37 38 39 40 41 42
% LG
A
Gestational age at birth
Overweightatbirth (England2011-12)
INTERGROWTH-21st
identified 42,988 more overweight babies
Local chart: UK 1990
Hirst et al Lancet 2015; 386: 1039-40

• Similar growth across population under optimal health conditions
• Accordance with postnatal standards.
• Reproducibility of results (ex: French CFEF experiment)
PRESCRIPTIVE CHARTS: WHAT THE DATA SHOW

INTERGROWTH-21st WHO
Birth weight 3.3 (0.5) kg 3.3 (0.5) kg
Birth length 49.3 (1.8) cm 49.5 (1.9) cm
IN ACCORDANCE WITH WHO PAEDIATRIC REFERENCES

BOYS
0
2
4
6
8
Weigh
t (Kg)
32 34 36 38 40 42 44 46 48 50Post menstrual age (weeks)
INTERGROWTH-21st
WHO-MGRS
GIRLS
0
2
4
6
8
Weigh
t (Kg)
32 34 36 38 40 42 44 46 48 50Post menstrual age (weeks)
INTERGROWTH-21st
WHO-MGRS
INTERGROWTH 21st Newborn Standards (red lines) WHO Child Growth Standards (blue lines)
Villar et al Am J Obstet Gynecol 2015; 213: 494-9

§ 120 sonographers
§ 8,784 examinations over the 6weeks study period
§ 4858 (55.3%) with“INTERGROWTH-like” inclusioncriteria
§ Comparaison withINTERGROWTH prescriptivestandards
FLASH STUDY CFEF– INTERGROWTH (2016)
8784examinations
1090 (12.4%) maternal reason288 (3.3%) SGA/IUGR311 (3.5%) maternal symptoms1248 (14.2%) maternal age 961 (10.9%) abnormal BMI 28 (0.3%) measurements <-5SD or >5SD
4858examinations

FLASH STUDY CFEF – INTERGROWTH
Stirnemann et al. 2016

FLASH STUDY CFEF – INTERGROWTH (IN PRESS)
FRANCE
Stirnemann et al. 2016

DISCUSSION :
• LesmesuresdebiométriefœtaleenFrancesontcomparablesàcellesobservéesdansl’étudeINTERGROWTH.

INTERGROWTH-21st Project International standards
• Fetal growth by ultrasound (Lancet 2014)• Newborn size for gestational age and sex (Lancet 2014)• Symphyseal-fundal height (BMJ 2016)• Maternal weight gain in pregnancy (BMJ 2016)• Postnatal growth of preterms (Lancet Glob Health 2015)• Preterm phenotypes (JAMA Ped 2015)• SGA phenotypes (JAMA Ped 2015)• Late pregnancy dating (Ultrasound Obstet Gynecol 2015)• 1st trimester dating (Ultrasound Obstet Gynecol 2014)• Estimated fetal weight (Ultrasound Obstet Gynecol 2016)

Lancet, 2014; 384:857-68
Lancet, 2014; 384:869-79
SEVERAL UNIVERSAL STANDARDS FROM 1ST TRIMESTER TO DELIVERY

Conclusions
• Fetal, newborn and infant growth are similar across populations when constraints ongrowth are minimal, justifying the construction of International Growth Standards
• The INTERGROWTH-21st & WHO Child Growth Standards monitor growth up to 5years of age using the same instruments
• Growth monitoring promotes continuity of care from the womb to the classroomworldwide
• The use of such prescriptive standards avoids overlooking growth abnormalities andallows international research programs