Embed Size (px)
Citation preview
In Canada the incidence of Fetal Alcohol Spectrum Disorder (FASD) has been
estimated to be 1 to 9 in 1000 live births.
Introduction
• Caused by prenatal exposure to alcohol
• FASD is the leading cause of developmental and cognitive disabilities among Canadian children
Etiology
• Alcohol readily crosses the placenta and results in similar levels in the mother and fetus
• Rate of elimination is slower in the fetus
• Most teratogenic effect during organogenesis and development of the nervous system
Etiology
When neuronal activity is abnormally suppressed during the developmental period, the timing and sequence of synaptic connections is disrupted, and this causes nerve cells to receive an internal signal to commit suicide, a form of cell death known as "apoptosis".
• Addiction Biology 2004 Jun;9(2):137-49.
Etiology
Alcohol suppresses neuronal activity, causing millions of nerve cells to commit suicide in the developing brain. This effect of alcohol provides a likely explanation for the diminished brain size and lifelong neurobehavioral disturbances associated with the fetal alcohol syndrome.
• Addiction Biology 2004 Jun;9(2):137-49.
Etiology
• Teratogenesis is grossly dose related, although the threshold dose is still unknown and related to maternal/fetal susceptibility
• Risk to fetus greatest with more than 7 or more standard drinks per week (1 standard drink = 13.6 grams of absolute alcohol)
• Binge drinking of more than 5 ounces ( 142 grams) on one occasion
Etiology
• No safe time to drink during pregnancy
• No known safe amount
Fetal Alcohol Spectrum Disorder: Defined
• Facial Anomalies
• Growth Restriction
• CNS Dysfunction
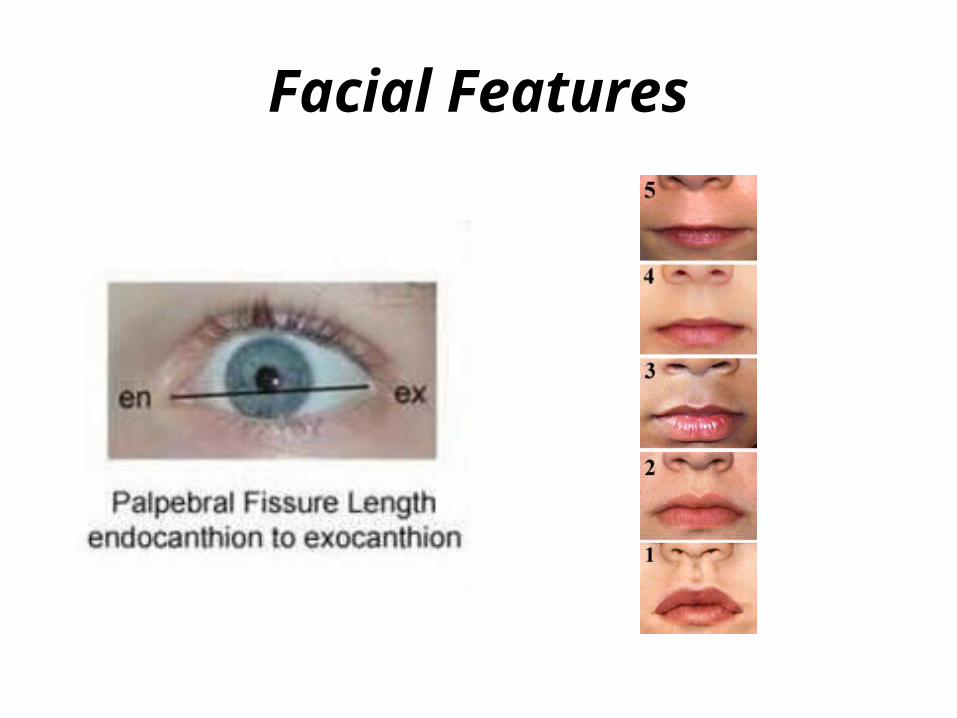
Facial Features
Growth Restriction
• Growth restriction is demonstrated by height and weight below the tenth (10th) percentile, and by microcephaly
• Growth restriction may be apparent prenatally and/or postnatally
Central Nervous System Dysfunction
• Decreased Cranial Size at Birth
• Structural Brain Abnormalities: microcephaly, partial or complete agenesis of the corpus callosum, cerebellar hypoplasia
• Neurobehavioral/Cognitive Signs
Neurobehavioral/Cognitive Signs:Infancy
• Tremors• Poor suck• Hypotonic/Hypertonic • Irritability• Feeding problems• Developmental delay
Neurobehavioral/Cognitive Signs:Beyond Infancy
• Cognitive problems• Fine motor issues• Hyperactivity• Restlessness • Poor ability to focus attention
Neurobehavioral/Cognitive Signs
• Cognitive problems:–Verbal IQ–Performance IQ–Scatter in Cognitive Skills–Specific Learning Disabilities–Memory Deficits–Executive Functioning
•
Executive functions ofthe prefrontal cortex
working memory
planning time
perception internal
ordering
self-monitoring
regulation of emotion
motivation
inhibition
Neurobehavioral/Cognitive Signs
• Poor Judgement
• Impulsiveness
• Sleep disturbances
• Extreme anxiety
• Depression
• Aggressiveness
• Other Behavioural Problems
Associated Anomalies
• Cardiac anomalies
• Joint and limb anomalies
• Neurotubal defects
• Anomalies of the urogenital system
• Hearing disorders
• Visual problems
• Severe dental malocclusions
Diagnosis: Diagnostic Criteria
Classification of FASD
1. FAS with confirmed maternal alcohol exposure
2. FAS without confirmed maternal alcohol exposure
3. Partial FAS with confirmed maternal alcohol exposure
4. Alcohol-Related Birth Defect (ARBD)
5. Alcohol-Related Neuro-Developmental Disorder (ARND).
• American Academy of Pediatrics, 1996.
#1: Fetal Alcohol Syndrome with confirmed prenatal exposure to alcohol
is characterized by a triad of signs:
• Facial Anomalies: short palpebral fissures, flat philtrum, and thin vermillion border of the upper lip
• Growth Restriction: weight and height (length) at or below the 10th percentile
• Central Nervous System Dysfunction: Structural abnormalities of the brain, intellectual impairment, developmental delay and a complex pattern of behaviours including extreme hyperactivity, poor judgment and aggressiveness
#2: Fetal Alcohol Syndrome without confirmed prenatal exposure
to alcohol:
• If the triad of signs described in category 1 is present, an diagnosis of Fetal Alcohol Syndrome can be made without confirmed alcohol exposure during gestation.
#3: Partial Fetal Alcohol Syndrome (PFAS) with confirmed alcohol
exposure:
• This diagnostic term is used when the patient presents with central nervous system dysfunction and most (but not all of the growth and/or facial features of FAS), and has a confirmed prenatal alcohol exposure
#4: Alcohol-Related Birth Defects (ARBD)
• Patients in this category will have congenital malformations such as cardiac anomalies, joint and limb anomalies, and confirmed prenatal alcohol exposure
#5: Alcohol-Related Neuro-Developmental Disorder (ARND)
• Patients with ARND present with neuro-cognitive dysfunction and complex patterns of behaviour, and have a confirmed exposure to alcohol prenatally
• Patients with ARND may not demonstrate any of the facial features or growth restriction associated with the full syndrome
New Classification of FASD
1. FAS with or without confirmed maternal alcohol exposure
2. Partial FAS with confirmed maternal alcohol exposure
3. Alcohol-Related Neuro-Developmental Disorder (ARND).
4. Alcohol-Related Birth Defects (ARBD)
• CMAJ, March 2005.
Differential Diagnosis
A number of genetic and malformation syndromes can present with clinical features similar to FASD and must be ruled out
Differential Diagnosis
A number of genetic and malformation syndromes can present with clinical features similar to FASD:
Cornelia de Lange Syndrome
Dubowitz Syndrome
Fragile X
Velocardiofacial Syndrome
Williams Syndrome
When to Diagnosis?
A diagnosis of FASD can be made at any time during life but it is often most easily made at the age of 18 months to 4 years when the facial characteristics are most distinct
Why Diagnose?
Validation• New understanding leads to new strategies at home and
other environments• Funding in school and daycare• Opening doors for family services• Better medical management• Prevention of secondary disabilities• Prevention of future alcohol affected children
Primary Disabilities: Organ Anomalies
• Cardiac anomalies • Joint and limb anomalies• Neurotubal defects• Anomalies of the urogenital system. • Hearing disorders• Visual problems• Severe dental malocclusions
Primary Disabilities: Central Nervous System
• Tremors• Poor suck• Hypotonic/Hypertonic • Irritability• Feeding problems• Developmental delay
Primary Disabilities: Central Nervous System
• Cognitive problems
• Fine motor issues
• Hyperactivity
• Restlessness
• Poor ability to focus attention
Primary Disabilities: Central Nervous System
• Cognitive problems:–Verbal IQ–Performance IQ–Scatter in Cognitive Skills–Specific Learning Disabilities–Memory Deficits–Executive Functioning
•
Executive functions ofthe prefrontal cortex
working memory
planning
Time perception
internal ordering
self-monitoring
regulation of emotion
Motivation
inhibition
Primary Disabilities: Central Nervous System
• Poor Judgement
• Impulsiveness• Sleep disturbances • Extreme anxiety • Depression• Aggressiveness• Other Behavioural Problems

Interventions:Medical
Interventions: Medical
• Referral to appropriate specialist: Cardiologist
OrthopedicsNephrologist
• Hearing Testing• Visual Testing• Follow Growth• Dental Care• ?? Medication
Interventions:Neuro-Developmental
Interventions: Neuro-Developmental
• Developmental Assessment
• Early Intervention Programs – Cognitive & Fine Motor
• Pre-School Speech and Language Program
• Occupational Therapist
Interventions: Neuro-Developmental
• Neuro-developmental or Psychological Assessment
• Modification of School Programs– Decrease Class Size 8 to 10– Resource Teacher/Educational Assistant– Individual Educational Plan– Speech Therapist- through school board
Interventions: Neuro-Developmental
– Challenge – Don’t Overwhelm
– Ensure expectations are reasonable with opportunities to succeed
Interventions:Psycho-social
Interventions: Psycho-social
• Early Intervention Programs – Behavioural, Social
• Activities child enjoys that foster self-esteem and social development
• Psychiatry
• ? Medication
Interventions: Psycho-social – Family
• Listening & Support
• Counselling
• Depression not uncommon and may need treatment
• Support Groups



















![867 Standard[1]](https://img.pdfslide.us/doc/110x75/577cc0471a28aba7118f8355/867-standard1.jpg)