Embed Size (px)
DESCRIPTION
fern test
Citation preview

Fern Test - Amniotic Fluid Crystallization Test MCL Procedure for Waived Applications Specimen: Vaginal swab obtained from the posterior vaginal pool.- avoid the use of any lubricants or antiseptics- use a sterile swab and do not touch the mucus plug- prepare a thin smear on a glass microscope slide by spreading evenly.Testing:
Allow the slide to air dry- do not apply heat and do not coverslip the slide. Examine the fully-dried slide microscopically, using the 10X objective Observe for "fern-like" crystals. Presence of crystals indicates that the fluid is amniotic fluid. Record the results: Write your name, the date, time and findings on the patient record.
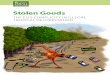
Positive Fern Test- note crystal formations Negative Fern test- no "fern-like" cytstalsInterfering Substances/ limitations:If present, blood, urine or cervical mucus can result in a false positive finding.False negative findings can result from prolonged rupture of membranes (>24 hr). Quality control:
Follow the procedural instructions exactly. There are no external(nor internal) quality controls to be performed at the unit level.
A simple and inexpensive test is described which permits positive identification of amniotic fluid by its fern-type crystallization. It permits a rapid and certain differential diagnosis between leukorrhea, hydrorrhea, urinary incontinence and spontaneous amniotomy. The crystallization test was shown to be most reliable and the few sources of error are easily avoided. The test is inhibited by cellular debris or blood when it is in a concentration greater than 1:10. Centrifugation permits the reappearance of fern-leaf crystallization. The typical image resembles that of the crystallization of cervical mucus. However, amniotic fluid crystallizes on the entire smear, whereas mucus crystallizes in a linear fashion. Cervical mucus crystallization is normally absent during pregnancy. It may occur in cases of threatened abortion. The authors have performed the test in combination with a nitrazin paper test in a series of 192 patients. In their hands it has given nearly perfect results.Ferning of amniotic fluid contaminated with blood. Rosemond RL, Lombardi SJ, Boehm FH. Obstet Gynecol. 1990 Mar;75(3):338-40.
“Amniotic fluid was obtained from 38 patients between 16-38 weeks’ gestational age who underwent amniocentesis. Amniotic fluid
was immediately mixed with freshly obtained, heparinized fetal cord blood in varying concentrations (blood to amniotic fluid 1:5,
1:10, 1:20). The slides were examined microscopically for the presence of ferning. All samples were fern-positive, but many had
atypical ferns described as “skeletonized.” As the concentration of blood to amniotic fluid increased, the number of atypical ferns
increased (32 of 38 at 1:5, 22 of 38 at 1:10, and nine of 38 at 1:20). We conclude that the presence of blood may alter the
morphology of the fern, but does not act as a contaminant that would affect the accuracy of the test.”
Amniotic fluid arborization: effect of blood, meconium, and pH alterations. Reece EA, Chervenak FA, Moya FR, Hobbins JC.. Obstet
Gynecol 1984 Aug;64(2):248-50
“Thirty-six specimens of amniotic fluid across gestational ages (16 to 42 weeks) were tested. The fern test was unaffected by
meconium at any concentration and by blood at dilutions of 1:10 or greater. When blood and amniotic fluid were mixed in equal
amounts, ferning was not present. Arborization of amniotic fluid was unaffected by pH alterations.”
The ferning and nitrazine tests of amniotic fluid between 12 and 41 weeks gestation. Bennett SL, Cullen JB, Sherer DM, Woods JR Jr.
Am J Perinatol. 1993 Mar;10(2):101-4
“Samples were obtained from amniocenteses between 14 and 42 weeks. Part I: Of 112 samples allowed to dry on a slide for 3
minutes only, 86.6% were ferning positive and 100% were nitrazine positive. Flame-drying increased the presence of ferning to
96.4%. Part II: 363 samples were allowed to dry completely for up to 10 minutes. All samples were ferning and nitrazine
positive….These tests may be reliably performed at gestations of 12 to 41 weeks.”
MORAL: Amniotic fluid will fern at any gestational age, in varying pH, and in the presence of a moderate amount of blood. If you
have fluid on the slide, and the slide doesn’t fern, you need to seriously doubt the diagnosis of ruptured membranes.
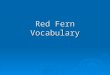
Fern test refers to detection of a characteristic 'fern like' pattern of cervical mucus when a specimen of cervical mucus is allowed to dry on a glass slide and is viewed under a low power microscope. Fern test is used to provide indirect evidence of ovulation and fertility, however this test does not predict the time of ovulation.

Ferning is due to the presence of sodium chloride in the mucus under estrogen effect. When high levels of estrogen are present, just before ovulation, the cervical mucus forms fern-like patterns due to crystallization of sodium chloride on mucus fibers. This pattern is known as arborization or 'ferning'.When progesterone is the dominant hormone, as is just after ovulation, fern pattern is no longer discernible. Fern pattern is completely absent by 22nd day of cycle. Disappearance of fern pattern after 22nd day suggests ovulation and its persistence throughout menstrual cycle suggests an-ovulation (infertility).The pH test involves sampling vaginal fluid to see how acidic or alkaline it is. Normal pH for vaginal fluid is between 4.5 and 5.5, and normal pH of amniotic fluid usually falls between 7.0 and 7.5. (When measuring pH, the higher the number, the more alkaline the substance.) If a sample of your vaginal fluid is more alkaline than normal vaginal pH, then it is very likely that the membranes have ruptured and amniotic fluid has leaked into thevagina.The Nitrazine test involves placing small amounts (a drop or two) of vaginal fluid onto paper strips prepared with Nitrazine dye. A chemical reaction occurs and the strips change color, indicating the pH of the vaginal fluid. If the color shows the pH is greater than 6.5, it's likely the membranes have ruptured. False readings can occur, however. Women with blood-tinged mucus, for example, can test positive on the Nitrazine test because blood has a pH closer to amniotic fluid than vaginal fluid. Some vaginal infections can also increase the pH of fluid in the vagina, and so can recent intercourse, because semen has a high pH.Your doctor can also confirm that your water has broken by checking for ferning (a fern-like pattern that can be seen on microscopic exam when estrogen and amniotic fluid mix together and cause salt crystallization).Other tests for diagnosing ruptured membranes have fallen in and out of favor among obstetricians and include:
Measuring the levels of glucose, fructose, prolactin, alpha-fetoprotein, or diamine oxidase in the fluid thought to be amniotic fluid. High levels of these chemicals indicate that the membranes have broken.
Staining the supposed amniotic fluid with nile blue sulfate. The resulting color will indicate whether amniotic fluid is present.
Injecting dye into the amniotic sac (by way of a needle into a woman's abdomen). If membranes have ruptured, the dyed fluid can be seen in the vagina.These other tests, though they work, are no more practical than the Nitrazine test and have some risk. These risks include rupture of the membranes (if this hasn't occurred already), trauma to the baby, infection, and possible adverse effects from the dye.
Procedure: Nitrazine paperProduct: Apothecon Nitrazine paper
PURPOSE
Nitrazine (Phenaphthazine ) paper is used to measure the vaginal pH of expectant mothers.
PRINCIPLE
Nitrazine paper is impregnated with an indicator dye Phenaphthazine. The color changes as pH changes, giving a broad range of colors from yellow through blue.
SUPPLIES
Phenaphthazine reagent strip.
Back to top
STORAGE
Store Phenaphthazine reagent strips at room temperature.
PATIENT PREPARATION
No patient preparation other than that required by a written protocol.
PROCEDURE
Standard Precautions must be adhered to by testing personnel.
Obtain a strip of Nitrazine paper approximately three inches long from the dispenser.

Wrap the paper around the ends of the fingers of one hand.
Insert the fingers and paper into the birth canal.
Remove the paper and excess fluid.
Compare the resulting color to the paper dispenser’s pH scale.
Record results on the patient chart.
Reports results as:
6.5 -6.5 =positive.6.0 and below = negative.
Back to top
Criteria for Unacceptable Specimens:
The specimen is estimated to be stable for 2-5 minutes at room. Contamination with blood will interfere with the reading. Bloody specimens should be read with caution, as it is difficult to interpret the color reaction.
EXPECTED VALUES
Normal vaginal pH is acidic (below 7.0). pH results above 7.0 ( basic) indicate that amniotic fluid is present. Bring results to the attention of the attending physician.
QUALITY CONTROL
Supplies:
pH calibrating buffers; pH 6.0 and pH 8.0 Store buffers at room temperature. Buffers are stable until the expiration date on the bottles.
Policy:
Both controls are run once each day of use.
Back to top
Procedure:
1. Add one drop of buffer to Nitrazine test paper.
2. Compare color to the paper dispenser's pH scale. The pH must be within 0.5 of the designated pH to be acceptable.
3. Document all results on the Control Sheet. If controls are out of range do not report any patient results until corrective action has been taken:
Repeat the procedure
Repeat using a different Nitrazine test packet
If controls are still out of range, call the Laboratory for assistance
SPECIFIC PERFORMANCE CHARACTERISTICS
The Nitrazine paper measures pH values generally to within 1 pH unit in the range of 4.5-7.5 visually.
REFERENCES
Apothecon, Princeton, NJ, Nitrazine Paper, p0083-00, p0084-00 52520.Communication from Bristol-Myers Squibb Company, March 28,1997.Hellman, L.M., et. al., Williams Obstetrics. 14th edition, New York, Appleton-Century-Crofts;
1971, p 405-406.

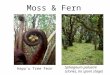
The lecithin–sphingomyelin ratio (aka L-S or L/S ratio) is a test of fetal amniotic fluid to assess for fetal lung immaturity.[1][2][3] Lungs require surfactant, a soap-like substance, to lower the surface pressure of the alveoli in the lungs. This is especially important for premature babies trying to expand their lungs after birth. Surfactant is a mixture of lipids, proteins, and glycoproteins, lecithin andsphingomyelin being two of them. Lecithin makes the surfactant mixture more effective.Evaluation[edit]The lecithin–sphingomyelin ratio is a marker of fetal lung maturity. The outward flow of pulmonary secretions from the fetal lungs into the amniotic fluid maintains the level of lecithin and sphingomyelin equally until 32–33 weeks gestation, when the lecithin concentration begins to increase significantly while sphingomyelin remains nearly the same. As such, if a sample of amniotic fluid has a higher ratio, it indicates that there is more surfactant in the lungs and the baby will have less difficulty breathing at birth. An L–S ratio of 2 or more indicates fetal lung maturity and a relatively low risk of infant respiratory distress syndrome, and an L/S ratio of less than 1.5 is associated with a high risk of infant respiratory distress syndrome.If preterm delivery is necessary (as evaluated by a biophysical profile or other tests) and the L–S ratio is low, the mother may need to receive steroids such as betamethasone to hasten the fetus' surfactantproduction in the lungs.Procedure[edit]An amniotic fluid sample is collected via amniocentesis and the sample is spun down in a centrifuge at 1000 rpm for 3–5 minutes. Thin layer chromatography (TLC) is performed on the supernatant, which separates out the components. Lecithin and sphingomyelin are relatively easy to identify on TLC and the predictive value of the test is good.[4]
Phosphatidylglycerol is a glycerophospholipid found in pulmonary surfactant.[1]
The general structure of phosphatidylglycerol consists of a L-glycerol 3-phosphate backbone ester-bonded to either saturated or unsaturated fatty acids on carbons 1 and 2. The head group substituent glycerol is bonded through a phosphomonoester. It is the precursor of surfactant and its presence (>0.3) in the amniotic fluid of the newborn indicates fetal lung maturity.Approximately 98% of alveolar wall surface area is due to the presence of type I cells, with type II cells producing pulmonary surfactant covering around 2% of the alveolar walls. Once surfactant is secreted by the type II cells, it must be spread over the remaining type I cellular surface area. Phosphatidylglycerol is thought to be important in spreading of surfactant over the Type I cellular surface area. The major surfactant deficiency in premature infants relates to the lack of phosphatidylglycerol, even though it comprises less than 5% of pulmonary surfactant phospholipids. It is synthesized by head group exchange of a phosphatidylcholine enriched phospholipid using the enzyme phospholipase D.
AMNIOTIC FLUID SHAKE TESTThe shake test is a qualitative measurement of the amount of pulmonary surfactant contained in the amniotic fluid. It is quick and inexpensive. It is a bedside test of lung maturity. In an obstetric emergency, an immediate decision about delivery can be made. The advantages of this test over the others are that a physician, technician or must can perform it and the test are highly reliable as
¨ It evaluates the ability of pulmonary surfactant to generate a stable foam in the presence of ethanol.¨ Ethanol, a nonfoaming competitive surfactant, eliminates the contributions of protein, bile salts and
salts of free fatty acids to the formation of a stable foam.¨ At an ethanol concentration of 47.5 percent, stable bubbles that foam after shaking are due to
amniotic fluid lecithin.¨ Positive tests, a complete ring of bubbles at the meniscus with a 1:2 dilution of amniotic fluid, are
rarely associated with neonatal RDS.¨ It is a screening test that gives useful information if mature.
Reference ValuesNormalPositive: persistence of a foam ring for 15 minutes after shaking (at an amniotic fluid – alcohol dilution of 1:2) indicates lung maturity.Procedure:
1. Test is based on the ability of amniotic fluid surfactant to form a complete ring of bubbles on the surface of the amniotic fluid in the presence of 95% ethanol.
2. Place a mixture of 95% ethanol and amniotic fluid in an appropriate container and shake for 15 seconds. A commercial kit is also available.Clinical implications:
1. If a complete ring of foam forms and persists for 15 minutes the test is positive.2. If no ring of bubbles forms, the test is negative.3. The test has a high false – negative rate but a low false – positive rate. The L/S ratio must be >4:1
for this test to be positive.

Interfering Factors1. Blood or meconium contamination can alter results.2. Contamination of glassware or reagents can alter test results.
InterventionsPretest patient care
1. Obtain informed consent.2. Explain the procedure and the reason foe testing.3. Use sterile techniques.
Posttest patient care1. Interpret test outcome counsel appropriately.2. Provide counseling if test is negative.3. Provide future treatment modalities.
Foam stability test Definition: a test for fetal pulmonary maturity, determined by the ability of pulmonary surfactant in amniotic fluid to generate stable foam in the presence of ethanol after mechanical agitation.Synonym(s): shake test