Embed Size (px)
Citation preview

Federal Ministry of Health
Task SharingPolicy change and implementation in
Nigeria
Dr. Kayode AfolabiHead, RH Division, FMoH

|
Ø Country context Ø Enabling factors and other issues on task shifting Ø Task shifting policy development process Ø FP services shared under the task shifting Ø Operationalization of TS-policyØ Quality assurance & Supervision Ø Achievements Ø Recommendations
Outline

|
Population estimate 184,000,000Women of Reproductive Age 42,320,000% married women 67%Married WRA 28,354,400Fertility/Contraception
Total Fertility Rate 5.5Contraceptive use (Any method) 15.1%Contraceptive use ( Modern method) 9.8%Unmet need 16.1%Births/Safe Motherhood
Total number of Births 6,606,079MMR (Maternal Mortality Ratio) per 100,000 live births 576
Antenatal coverage 51.1%% of births with SBA 38.1%% of Births to adolescents (15-19) 14.90%National CPR goal by 2018 36%
Country Context

|
Ø Community health workers (CHEWs) are those who have undergone a 36-month course in a training institution approved by the FMOH through the Community Health Practitioners Registration Board of Nigeria (CHPRBN)
Ø CHEWs curriculum covers 90 hours of didactic -lectures and competency-based trainings
Background

|
Human resources shortage in addition to inequitable distribution.
Higher number of CHEWs -36,737 at PHCs compared to 5,604 Nurse/Midwives.
Freeze on employment due to funding constraints Preference for CHEWs
employment due to availability and lower remuneration package.
Enabling factors for task sharing

|
Ø Statutory responsibilities of CHEWs were limited, but in remote PHC locations performed lifesaving procedures without previous formal training.
Ø Scientific evidence demonstrated that CHEWs could be trained to proficiency in basic essential maternal services including family planning.
ØWHO recommendation for countries deficient in HRH is to embrace a task shifting and sharing policy.
Other existing issues on task sharing

|
Ø Advocacy and consensus building among all stakeholders including professional regulatory bodies, state and non-state actors, pre-service institutions, service providers etc.
Ø Review of examples of task shifting in country as well as evidence from other counties with similar health systems.
Ø Engagement with stakeholders for a more comprehensive essential health services package.
Ø Approval of the policy at the 55th NCH meeting in Uyo, Akwa Ibom State in 2014.
Task-shifting Policy Development Process

|
Task CHEWsProvide FP education/counseling and help women choose preferred method of contraception
√
Promote dual protection for HIV positive women √Provide contraceptive method or refer as necessary √Perform tubal ligation NOPerform vasectomy NOInsert and remove contraceptive implant √Insert and remove intrauterine contraceptive device (IUCD) √
Initiation and maintenance of injectable contraceptives √
FP services shared under the Policy

|
Reviewed pre-service curriculum to incorporate
LARCs training
Ongoing in-country studies to validate that CHEWs could be trained to competency and documenting lessons learned
Revision of all policy documents including training
curriculum – training methodology for nine days.
Development of a national implementation framework and roll out plan – in progress.
Operationalization of the Task Shifting policy

|
ØSupervision§ Structure: Mentoring for proficiency§1 Clinical Trainer assigned to 5 CHEWs.
§ Tools: Supportive Supervision Checklist.
§ Methodology: The Clinical Trainer visits the CHEWs on agreed dates
Ø Quality Assurance:§ Accreditation using Competency based approach.
§ Each service provider (CHEWs inclusive) has a qualified supervisor/master trainer attached to them.
§ Feedbacks are also received from exit interview on level of satisfaction with quality of service received.
How is quality assured?

|
Ø Review of policy documents including training curriculum.
Ø Training of 80 master trainers at the national level who stepped down training to state and service providers .
Ø Review quantification of commodities in anticipation of surge in uptake
Ø Training of 334 CHEWs from nine states.Ø Partners commitment to support training of CHEWs in their focal states
Achievements

|
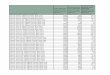
CHEWs/CHO LARC training so far…
Source: 1Nigeria FP dashboard 2016, 2State tracker.

|
Snapshot of National, Rivers and Zamfarastates Implant AMC
Source: DHIS2, Nigeria FP dashboard 2016, State FP facility register.
10899
21304
National
Quarterly National Implant AMC (period of CHEW trainings)
(Baseline =Q2,2015;; Endline = Q2,2016
Q1 , 2015 Q1 , 2016
35 41
693
410
Rivers Zamfara
Quarterly implant AMC in facilities trained in Rivers and Zamfara states
(Baseline =Q3,2015;; Endline = Q1,2016)
Pre Training Q3 2015 Post Training Q1 2016

|
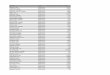
National HR Data: Trained LARC Providers
Source: Nigeria FP dashboard.
5301
3428National
Number of Trained LARC Providers.Q1 , 2015 Q1 , 2016
Additional 1873 LARC providers trained from Q1 2015-Q12016
4967
334National
Trained LARC Providers by CadreCHEWs/CHOs Doctors/Nurse/Nurse Midwives

|
Ø Operations research needed to identify local implementation standards and processes
Ø Buy-in of all strata of government for ownership, funding and sustainability
Ø Development of operation and implementation plans Ø Coordination of partners to ensure implementation is standardized, supervised and monitored
Recommendations

|
Thank you for your attention!