Embed Size (px)
Citation preview

Critical care staff whomanage intubatedpatients often experiencedifficulties with one ofthe most basic human
functions: communication. Patientswith endotracheal or tracheostomytubes are unable to communicateverbally because of the placement ofthe tube and inflation of the tube’scuff, which prevents passage of airacross the vocal cords. Despite theinability to produce speech, thesepatients can communicate effectivelyvia other methods. Intubated patientscommunicate with nurses, other cli-nicians, and family members prima-rily through gestures, head nods,mouthing of words, and writing.1
Other communication methodsinclude letter/picture boards, lists
Promoting Effective Communication for Patients Receiving Mechanical Ventilation
of common words or phrases tailoredto meet individual patients’ needs,and high-tech alternative communi-cation devices. Various options forpatients with a tracheostomy tubeinclude partial or total cuff defla-tion and use of a speaking valve incertain patients who are in stablecondition. Specially designed tra-cheostomy tubes are also availableto allow speaking while the cuff ofthe tracheostomy tube is inflated.
Although communication withpatients in the intensive care unit(ICU) is usually focused on basicneeds related to physical comfortsuch as positioning or suctioning,communication is often an impor-tant component of end-of-life deci-sion making. Patients may need toexpress their final wishes to family,friends, and providers.2 The goal isto enhance a patient’s ability toexpress their needs and wishes tostaff and to their loved ones fullyand effectively. Various sophisticatedmethods are available for complex
Irene Grossbach, RN, MSNSarah Stranberg, MA, CCC-SLPLinda Chlan, RN, PhD
Feature
PRIME POINTS
• Communicating effectively with ventilator-dependent patients isessential to provide high-quality care.
• Various strategies canbe used to help patientsfully and efficiently expresstheir needs and wishes tostaff and loved ones.
• Nurses must assess thepatient’s communicationneeds; develop a commu-nication care plan with thepatient, the patient’s fam-ily, and other health careproviders; and ensure thatthe plan is visible andaccessible to all caregivers.
©2010 American Association of Critical-Care Nurses doi: 10.4037/ccn2010728
This article was published electronicallyon the CCN Web site. Some modificationsmay be made by the authors before thefinal version appears in printed form.
CriticalCareNurse OnlineFirst www.ccnonline.org
Crit Care Nurse Papers in Press. Published on August 31, 2010 as Manuscript ccn2010728
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from

cases. In this article, we review variousstrategies to promote effective com-munication between patients receivingmechanical ventilation, health carestaff, and patients’ family members.
Challenge of Effective Communication With Nonvocal Patients ReceivingMechanical Ventilation
Determining an alternative, effec-tive communication system requirescollaboration between staff, a patient’sfamily, and the patient. Difficultieswith communication often causeanxiety, frustration, and fear inpatients.3,4 Increased respiratory ratecan create breathing discomfort andthe need to make ventilator adjust-ments promptly to match the fasterbreathing pattern or provide optimalventilation support.4 Directing thepatient to calm down and breathewith the machine is inappropriateand usually ineffective.
Patients who have been emer-gently intubated may need initialreminders and short explanationssuch as “you have a tube in your throatto help you breathe” and “you can-not speak when the tube is in place.”Other simple words of encourage-ment and support may include “youare doing well,” “everything is OK—we are helping you get better,” and
“your breathing will feel better.”The patient may be able to commu-nicate basic responses more effec-tively if staff ask one question at atime to elicit a yes/no response andgive simple directions such as “nodyour head” or “squeeze my hand.” Acalming reassuring voice, confidentapproach, and therapeutic touchmay help alleviate this anxiety-pro-ducing situation.
More time is available to prepareelectively intubated patients andtheir family members. These patientscan be provided with detailed infor-mation about the location of theendotracheal or tracheostomy tube,why the patient will not be able tocommunicate verbally, and whatmethods to communicate can beused while receiving mechanicalventilation. An educational pam-phlet about the endotracheal or tra-cheostomy tube, the ventilator, andhow to communicate can be givento the patient’s family and the patientas appropriate (Table 1).
Nursing staff can improve apatient’s experience, frustration level,and outcome by using strategies toimprove communication3 with non-vocal patients and by creating orcustomizing a plan that meets thepatient’s needs. The patient careplan and specific methods should
be readily available for use by allmembers of the health care teamwho interact with the patient. It isalso essential to involve and educatethe patient’s family members so thatthey can communicate effectively.These efforts may help the patientand the patient’s family feel lessanxious and fearful.
Families want to be included ascaregivers when patients are in anICU. A familiar voice and touch canhave a calming effect on a frightenedor upset patient. Relatives have empa-thy for the patient and recognize thepatient’s nonverbal cues such asfacial expressions of fear and restlessphysical movements. They have adeep understanding of the patient’sneeds, which can be helpful to thehealth care team.5 However, whenrelatives experience difficulties com-municating with their loved one, theymay feel a sense of loss because ofthe lack of response from the patient.6
Appropriate, warm physical touchmay provide some benefit.7
Communication StrategiesNumerous strategies are avail-
able for improving communicationwith patients in the ICU. Many ofthese techniques are simple and/orinvolve very basic materials at thebedside. The following 6 strategiesfacilitate successful communicationwith patients receiving mechanicalventilator support: (1) Establish acommunication-friendly environ-ment. (2) Assess functional skillsthat affect communication. (3)Anticipate patients’ needs. (4) Facili-tate lipreading. (5) Use alternativeand augmentative communicationdevices. (6) Educate the patient, thepatient’s family, and staff aboutcommunication strategies. These
Irene Grossbach practiced as a pulmonary clinical nurse specialist for 28 years and is anadjunct assistant professor in the School of Nursing at the University of Minnesota inMinneapolis.
Sarah Stranberg is a speech-language pathologist and a clinical specialist at the Universityof Minnesota Medical Center, Fairview, in Minneapolis.
Linda Chlan is an associate professor in the School of Nursing at the University of Minnesotain Minneapolis.Corresponding author: Irene Grossbach, RN, MSN, 3043 East Calhoun Pkwy, Minneapolis, MN 55408 (e-mail:igrossbach@netscape,net).
To purchase electronic or print reprints, contact The InnoVision Group, 101 Columbia, Aliso Viejo, CA 92656.Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; e-mail, [email protected].
Authors
www.ccnonline.org CriticalCareNurse OnlineFirst
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from
CriticalCareNurse OnlineFirst www.ccnonline.org
Table 1 Patient Education Pamphlet: Ventilator
Your doctor has ordered a ventilator for you. This booklet will help answer questions you and your family may have.
What is a ventilator?A ventilator is a machine that helps your breathing. It is also called a respirator or a breathing machine. It is a large square machine that sits
at your bedside. The ventilator gives you a certain number of breaths every minute. The machine does the work your lungs usually do.
Why do I need a ventilator?You may need a ventilator if you do not have enough oxygen or if you have too much carbon dioxide in your bloodstream. It can help
decrease your shortness of breath and work of breathing so you feel more comfortable. If you are having surgery, the anesthesia mayprevent your breathing muscles from working. When the anesthesia wears off, normal breathing will return and you will not need theventilator. People may need the help of a ventilator for a variety of problems, including pneumonia, emphysema, asthma, and diseasesthat cause breathing muscles to become weak or paralyzed. You need a ventilator because ______________________________ ___.
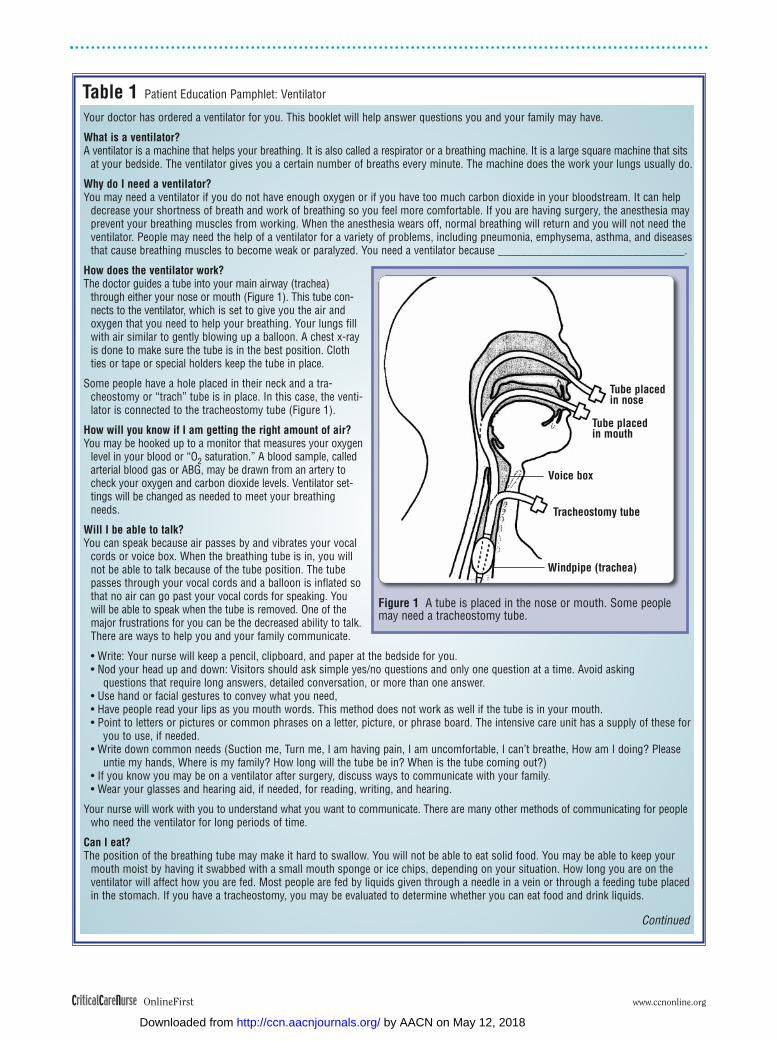
How does the ventilator work?The doctor guides a tube into your main airway (trachea)
through either your nose or mouth (Figure 1). This tube con-nects to the ventilator, which is set to give you the air andoxygen that you need to help your breathing. Your lungs fillwith air similar to gently blowing up a balloon. A chest x-rayis done to make sure the tube is in the best position. Clothties or tape or special holders keep the tube in place.
Some people have a hole placed in their neck and a tra-cheostomy or “trach” tube is in place. In this case, the venti-lator is connected to the tracheostomy tube (Figure 1).
How will you know if I am getting the right amount of air?You may be hooked up to a monitor that measures your oxygen
level in your blood or “O2 saturation.” A blood sample, calledarterial blood gas or ABG, may be drawn from an artery tocheck your oxygen and carbon dioxide levels. Ventilator set-tings will be changed as needed to meet your breathingneeds.
Will I be able to talk?You can speak because air passes by and vibrates your vocal
cords or voice box. When the breathing tube is in, you willnot be able to talk because of the tube position. The tubepasses through your vocal cords and a balloon is inflated sothat no air can go past your vocal cords for speaking. Youwill be able to speak when the tube is removed. One of themajor frustrations for you can be the decreased ability to talk.There are ways to help you and your family communicate.
• Write: Your nurse will keep a pencil, clipboard, and paper at the bedside for you.• Nod your head up and down: Visitors should ask simple yes/no questions and only one question at a time. Avoid asking
questions that require long answers, detailed conversation, or more than one answer.• Use hand or facial gestures to convey what you need, • Have people read your lips as you mouth words. This method does not work as well if the tube is in your mouth.• Point to letters or pictures or common phrases on a letter, picture, or phrase board. The intensive care unit has a supply of these for
you to use, if needed.• Write down common needs (Suction me, Turn me, I am having pain, I am uncomfortable, I can’t breathe, How am I doing? Please
untie my hands, Where is my family? How long will the tube be in? When is the tube coming out?)• If you know you may be on a ventilator after surgery, discuss ways to communicate with your family.• Wear your glasses and hearing aid, if needed, for reading, writing, and hearing.
Your nurse will work with you to understand what you want to communicate. There are many other methods of communicating for peoplewho need the ventilator for long periods of time.
Can I eat?The position of the breathing tube may make it hard to swallow. You will not be able to eat solid food. You may be able to keep your
mouth moist by having it swabbed with a small mouth sponge or ice chips, depending on your situation. How long you are on theventilator will affect how you are fed. Most people are fed by liquids given through a needle in a vein or through a feeding tube placedin the stomach. If you have a tracheostomy, you may be evaluated to determine whether you can eat food and drink liquids.
Continued
Figure 1 A tube is placed in the nose or mouth. Some peoplemay need a tracheostomy tube.
Tube placedin nose
Windpipe (trachea)
Tracheostomy tube
Voice box
Tube placedin mouth
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from

strategies are addressed in detail inthe following sections.
Establish a Communication-Friendly Environment
Staff working in a critical careenvironment often become accus-tomed to the abundant sensorystimulation. Most critical care nurseshave mastered the ability to focusattention on a specific task or inter-action despite a multitude of distrac-tions. Patients and their families maynot be familiar with this environ-ment, which can significantly affectcommunication. The followingadaptations may be helpful.
Adjust your proximity and posi-tion so that you are visible to thepatient. Staff often attempt commu-nicating with patients when theyare across the room or behind otherequipment, such as ventilators.
Speak directly to the patient. Itis often easy to look up and speak
facing family members who are ableto participate in conversations eas-ily. Facing the patient directly mayrequire repositioning the patient ifmedically possible.
Ensure that the lighting is ade-quate for the patient to see thespeaker and/or communicationboards. Improve lipreading bymaking light fall on the patient’sface. Reduce background noise andactivity, perhaps by turning off thetelevision or radio, decreasing addi-tional conversations occurring inthe room, and closing the door.
Assess Functional Skills ThatAffect Communication
In addition to their current con-ditions, patients enter the ICU withpersonal characteristics and func-tional abilities that can affect theirability to communicate and interactin this challenging environment.Areas to assess include auditory and
visual acuity, whether the person isright- or left-handed, muscle strengthfor writing, and language for speak-ing and literacy. Table 2 presents auser-friendly and comprehensive com-munication assessment tool we devel-oped for use with nonvocal patients.
Auditory Acuity. The acute careunit is a difficult environment forpatients with any degree of hearingimpairment because of the variedbackground noises emitted by equip-ment. Although necessary equipmentcannot be eliminated, it is importantto establish a communication-friendly environment. Determine ifthe hearing-impaired patient wearshearing aids and whether the hear-ing aids are at the hospital and work-ing properly. Ensure that thehearing aid that is in place has noaudible feedback, a common prob-lem due to patients’ positioning.Hearing aid batteries and basic sup-plies for cleaning should be readily
www.ccnonline.org CriticalCareNurse OnlineFirst
Table 1 Continued
Will I feel pain?Some people are given medication so they do not remember the tube being put in. Other people may be uncomfortable while the
breathing tube is being put in. A medicated spray will numb your nose and mouth before the breathing tube is placed. This spray willhelp make you more comfortable. Your doctor may order a sedative or pain medication for you while you are on the ventilator.
Can I get out of bed?You should stay in bed. Your position will be changed at least every 2 hours or more often if you desire. You may sit up in bed and turn
from side to side. Sometimes people can get out of bed, stand, walk, and sit on a chair.
Will I be able to cough?You will be able to cough but will need help clearing secretions. The nurse or respiratory therapist will put a catheter (a small flexible tube)
into the breathing tube and suction out the secretions. This may need to be done often, depending on the amount of secretions in the tube.
Can I wear dentures?If the breathing tube is in your mouth, you cannot wear your dentures. If the breathing tube is in your nose, you can wear your dentures
if wearing them makes you feel better.
How long will I need the ventilator?This depends on your condition. Some people need ventilator support for only a few hours, while other people need support for days or
weeks or months. The nurses, respiratory therapists, and doctors will work to improve your condition so you spend as little time aspossible on the ventilator. When your condition improves, a process of discontinuing the ventilator or “weaning” is done. The machineis set so you are doing the breathing on your own. If your breathing is comfortable and your arterial blood gas looks good, thebreathing tube is removed.
Being on a ventilator may cause anxiety, fear, and discomfort. If needed, the doctor will order a sedative or pain medication for you.Understanding why you are on the ventilator, what to expect when you are on the ventilator, and how to communicate your needs canbe very helpful to calm and reassure you. Your nurses and doctors will try to make this a less frightening experience for you. Pleaseshare this booklet with your family. Feel free to ask your doctor or nurse any questions you may have.
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from

available. If the hearing loss is newand unexplained, the attendingphysician and pharmacist should benotified to determine whether thepatient is experiencing ototoxiceffects from prescribed medications.The ear canal should be inspectedand cleaned of wax.
Most hospitals have basic ampli-fier equipment, or assistive listen-ing devices, to improve hearing. Acommon assistive listening device isthe Pocketalker Personal Amplifier(Williams Sound Corp, Eden Prairie,
Minnesota), which consists of head-phones for the hearing-impairedperson to wear and a microphonedevice that can amplify the speechof the other talker (Figure 2).
Visual Acuity. Glasses may beessential to visualize items on acommunication device. Evaluatewhether the patient wears glassesfor reading and if they are available.Clean and position properly, espe-cially if a patient requires bifocallenses. Screen patients for neuro-logical deficits such as field cuts or
visual neglect, which may interferewith their ability to communicate.
Handedness. Determine whichhand is used for writing or use of acommunication board. If the patienthas a new hemiparesis affecting thedominant hand, it can affect the abil-ity to point to items on some boards.
Assess Muscle Strength. Commu-nication boards may need to bemodified to accommodate theselimitations, including locating themost common needs at an “easy-topoint-at” spot on the board. Use of
CriticalCareNurse OnlineFirst www.ccnonline.org
Table 2 Communication Assessment Tool for nonvocal patients
Directions: Communication plan should be kept at the bedside and/or designated computer location so it is readily available to all healthcare team members and the patient’s family. Update as needed.
Date assessed: ______ with patient ______ with family member _______ both _____
Mental status: alert, appropriate----lethargic, confused----comatoseLanguage: English: Yes No Other (List) ____________Hearing: Normal Impaired (R,L) Hearing aid: Yes NoVision: Normal Impaired Needs glasses for reading: Yes NoWriting: Right Left Grasps writing device: Yes No Unable due to hands: weak--- swollen---paralyzedLiteracy (reads, spells): Yes No Aphasia: Yes No (If yes, consult speech therapy)Neuromuscular weakness, paralysis: Yes (Explain) _________________ NoAble to use standard call light system Yes No (Select adaptive system)_______________________________________________________________Effective communication system(s) for this patient:____Nods head up, down to yes/no questions____Clipboard, pad, pencil _____hand____Lip-read____Picture board____Letter board____Word board____Regular call light system____Needs adaptive call light system. Proper placement for use __________________
Severe weakness, paralysis_____Blinks eyes 1 blink = yes, 2 blinks = no_____Moves eyes toward head for yes, closes eyes for no_____Needs advanced system; speech consult sent________________________________________Details of effective communication system for Mr/Ms ____________________Example:12/6/08 Mr L communicates by nodding head to yes/no ?, needs glasses for reading and writes with right hand-elevate HOB at least
40°, points to picture board—usual issues have been pain, needs frequent position change, likes ROM to legs and wants radio on(AM 1500 or FM 100)
12/10 Update—same communication system as 12/6 except patient unable to write because hands swollen, weak, can’t grasp. Discon-tinue pad, pencil for now
12/13 Bilateral hearing loss—MD notified, no ear wax—use Pocketalker in room12/15 No change
Abbreviations: HOB, head of bed; L, left; R, right; ROM, range of motion exercises.
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from

restraints on a patient’s dominanthand will hinder their ability to write,gesture, or point to items on a com-munication board.
Language. If a patient does notspeak/understand English, a hospi-tal interpreter can be extremelyhelpful for developing communica-tion tools. Picture boards may workbetter than word/phrase/letterboards for non-native English speak-ers or aphasic patients because pic-tures do not rely on language skills.
Literacy. A patient’s impairedability to read/spell can be a com-plicating factor if staff membersattempt to use a letter board orphrase lists. In these situations, useof pictures may be more appropri-ate to facilitate communication.
Anticipate Patients’ NeedsGestures have been identified as
the communication method usedmost often by ventilator-dependentpatients.2 Gestures can be misinter-preted as anxiety8 when the patientis really just attempting to convey amessage and be understood. A rest-less, diaphoretic, and grimacingpatient with a high respiratory ratemay be in pain. A frustrated patient
trying to com-municatebecomes moreanxious.
The nursemay administera sedativeand/or applyrestraints whenthe more appro-priate manage-ment would beto identify andimplementcommunication
strategies that meet the particularneeds of that patient and enable thepatient to communicate effectively.The following strategies are helpfulin resolving problems to ensure suc-cessful communication.
Use of Inquiry. When routinelyassessing patients, anticipate basiccare needs by asking simple questionsrelated to personal care and comfort,such as: “Do you want to be turned?”“Do you need to be suctioned?” “Doyou need to use the bedpan?” “Uri-nal?” “Do you have pain?”
Ask yes/no questions rather thanopen-ended questions. Instead ofasking “Where are you having pain?”ask “Are you having pain in yourchest?” “Do you have a headache?”or “Does your back hurt?” Staff canalso use pictures of the body or havethe patient point to the area of pain.Accurate assessment and pain man-agement are essential to qualitycare. A nonverbal pain scale at thebedside or taped to the head of thebed reminds nurses of the rating scaleand the policy for pain assessment.9
Ask only one question at a time.For example, do not ask “Are youhaving pain in your chest or inyour hip?”
Implement a consistent methodfor yes/no responses and communi-cate the plan to all staff. Consistencyis particularly important for patientswith neuromuscular impairment orparalysis, where eye blinks, headmovements, and gestures are com-monly their “lifeline” to communi-cate needs effectively. Identify thetopic if the patient’s communicationis unclear. “Are you asking about theventilator?” “Are you talking aboutyour family?” Knowing a specifictopic/context of the patient’s mes-sage may significantly increaseunderstanding of the message andimprove questions that you ask inefforts to resolve the problem.
Identification and Validation ofNonverbal Responses. Identify andvalidate the meaning of facial expres-sions and other nonverbal commu-nication. For example, you couldverbalize to the patient your obser-vation that he appears angry, upset,scared, sad, or happy. Empathizeand attempt to identify possiblecauses for feelings and solutions.
Maintain eye contact, preferablyat the patient’s level. Be aware ofcultural factors that may precludeeye contact.
Convey a calm, confident, reas-suring manner. Maintain patienceif the patient is angry or frustratedat not being able to communicateneeds. Empathize with the patientand convey willingness to under-stand. Allow time for the patient toconvey a message. Obtain additionalassistance, if needed, in situationswhere time is limited.
Facilitate LipreadingReading lips is a specialized skill
and may be difficult, particularly ifthe tube is orally placed. The tube,
www.ccnonline.org CriticalCareNurse OnlineFirst
Figure 2 Pocketalker Personal Amplifier. Courtesy Williams Sound Corporation, Eden Prairie, Minnesota.
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from

tube holder, and/or tape over themouth limit lip movement and visu-alization. Becoming skilled at lipread-ing takes practice, and some peopleare naturally better at decipheringmouthed words. Persons with hear-ing loss generally are expert lip-readers,9 and it is especially helpfulif they are health care professionals,because they understand the healthissues. Identify other methods tocommunicate needs effectively. Alip-reader translating service elicitedpositive responses from patients andallowed health care providers tospend more time providing patient-centered care and less time attempt-ing to decipher patients’ messages.10
Several steps can be taken toimprove lipreading. Make sure thelight falls on the patient’s mouth, notin the patient’s eyes. Look for keywords, a pattern of words or phrasesthat give the sentence meaning andprovides clues so you can ask focusedquestions. Allow the patient to mouthwords in a full sentence to givethem context; do not isolate words.Avoid interruptions that break the
thought process and distract youfrom focusing on what the patientis saying. Obtain assistance fromskilled colleagues to help translatemouthed words.11
Use Alternative and AugmentativeCommunication Devices
Alternative and augmentativedevices to aid communicationrange from the basic to the high-tech. Patients can have success withstandard, generic tools, such as analphabet board, but patients mayfurther benefit from other assistivedevices. Identifying and implement-ing alterative and augmentativecommunication requires collabora-tion among nurses, respiratory ther-apists, and speech pathology staff.An effective communication systemincludes use of basic communicationtools and consultation with stafffrom the speech-language pathologyservice as needed.
Basic Communication Tools. Pro-vide each patient with basic suppliesfor note writing, including paper ona clipboard and a dark lead pencil
for easy visualization. Removerestraints as needed for writing.Table 3 lists the essential contentsfor communication tool kits. Maketools and supplies easily accessibleto all staff.
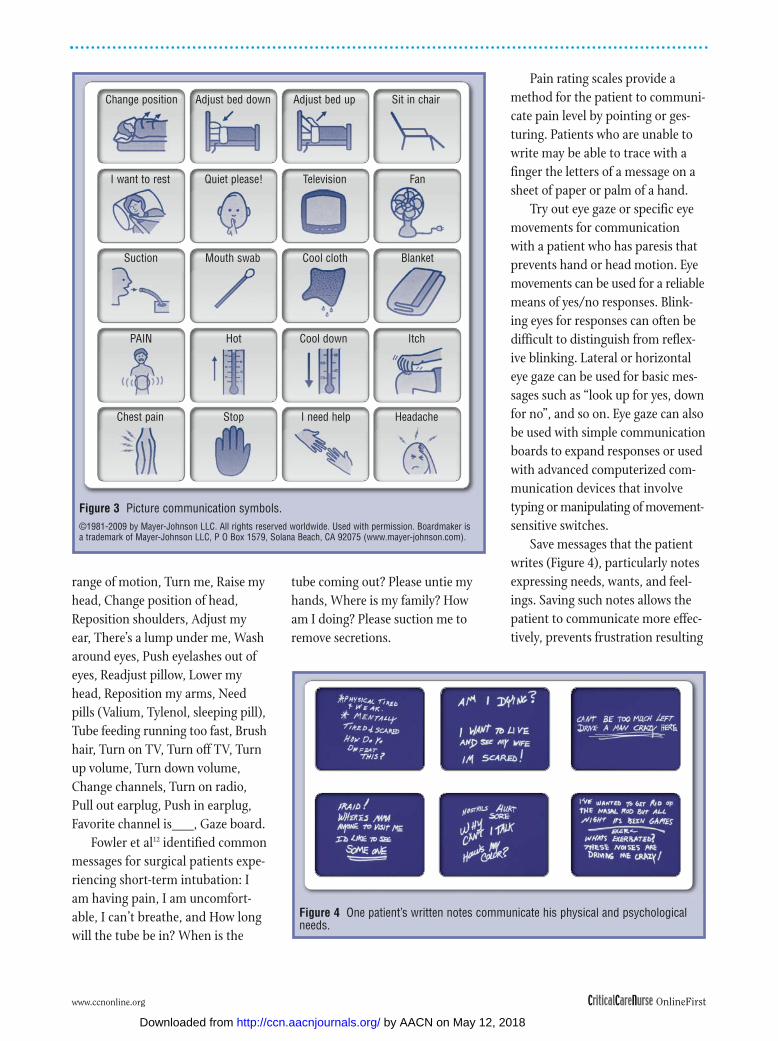
Provide basic communicationboards. These may include a letterboard, a picture board, and a list ofcommon phrases/messages as shownin Figure 3. Involve the patient, ashe or she is able, the patient’s fam-ily, and staff in determining a listof patient-specific needs or mes-sages and the best order of place-ment on the individualized board.Word/phrase boards can reduceoverall frustration with communica-tion.3 Boards can be laminated forlong-term use. Messages may varydepending on the clinical situationand the duration of intubation.Messages for a patient with neuro-muscular disease who is able onlyto blink eyes include the following:Suction, Urinal, Bedpan, Brushteeth, I am hot, I am cold, I can’thear you, I am biting my tongue,Mouth guard, Bend elbows, Do
CriticalCareNurse OnlineFirst www.ccnonline.org
Table 3 Essentials to include in a communication kit
Communication supplies should be readily available for all ventilator-dependent patients. These supplies can be easily assembled andplaced in clear plastic bags or plastic containers for individual use. Letter, word, and picture boards should be laminated for durabilityand trouble-free use. Adaptive call light systems and other aids for hearing impairment (eg, the Pocketalker) should be readily avail-able in a designated location. Speech pathologists should be consulted as needed to assist in determining effective communicationsystems for patients with complex communication problems or for seemingly simple cases where the nurse is unable to establish aneffective communication system.
Communication kit contentsClipboard 81⁄2 x 11 writing pad Pencil (#2)Washable fine-tip markerLetter boardWord board Picture boardPain rating scaleShortness of breath/dyspnea rating scaleAnxiety rating scale Communication Assessment Tool (Table 2)
A Pocketalker for hearing impaired patients and a magnifying glass should be readily available for use.
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from
range of motion, Turn me, Raise myhead, Change position of head,Reposition shoulders, Adjust myear, There’s a lump under me, Washaround eyes, Push eyelashes out ofeyes, Readjust pillow, Lower myhead, Reposition my arms, Needpills (Valium, Tylenol, sleeping pill),Tube feeding running too fast, Brushhair, Turn on TV, Turn off TV, Turnup volume, Turn down volume,Change channels, Turn on radio,Pull out earplug, Push in earplug,Favorite channel is___, Gaze board.
Fowler et al12 identified commonmessages for surgical patients expe-riencing short-term intubation: Iam having pain, I am uncomfort-able, I can’t breathe, and How longwill the tube be in? When is the
tube coming out? Please untie myhands, Where is my family? Howam I doing? Please suction me toremove secretions.
Pain rating scales provide amethod for the patient to communi-cate pain level by pointing or ges-turing. Patients who are unable towrite may be able to trace with afinger the letters of a message on asheet of paper or palm of a hand.
Try out eye gaze or specific eyemovements for communicationwith a patient who has paresis thatprevents hand or head motion. Eyemovements can be used for a reliablemeans of yes/no responses. Blink-ing eyes for responses can often bedifficult to distinguish from reflex-ive blinking. Lateral or horizontaleye gaze can be used for basic mes-sages such as “look up for yes, downfor no”, and so on. Eye gaze can alsobe used with simple communicationboards to expand responses or usedwith advanced computerized com-munication devices that involvetyping or manipulating of movement-sensitive switches.
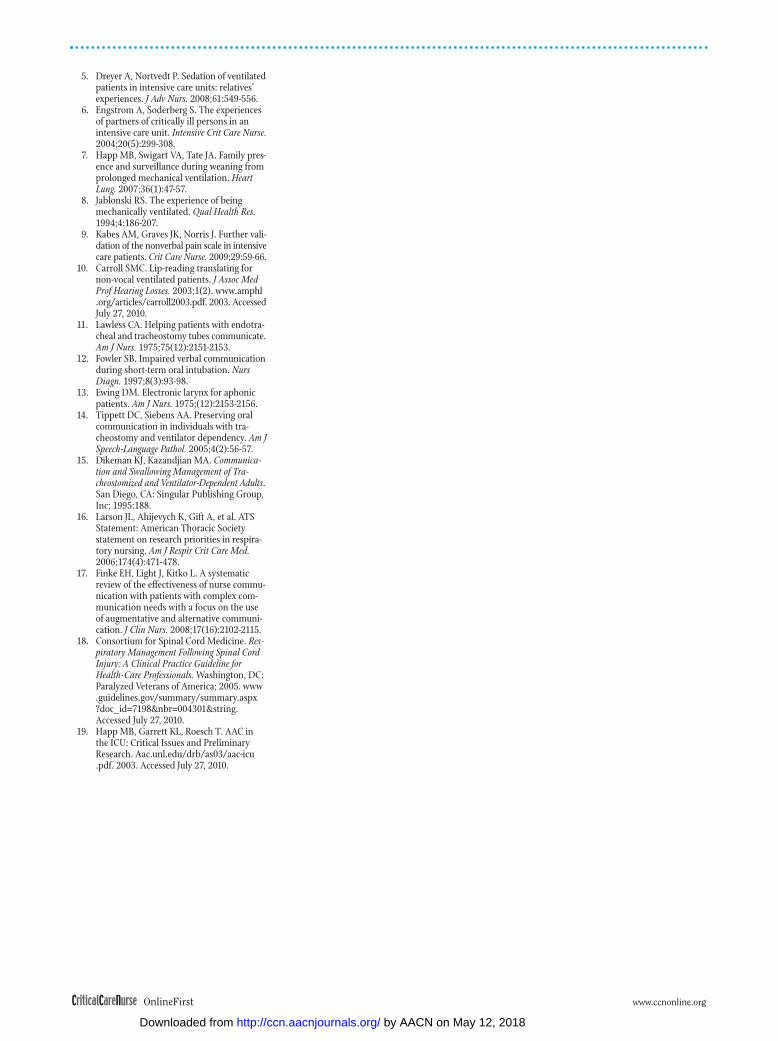
Save messages that the patientwrites (Figure 4), particularly notesexpressing needs, wants, and feel-ings. Saving such notes allows thepatient to communicate more effec-tively, prevents frustration resulting
www.ccnonline.org CriticalCareNurse OnlineFirst
Figure 3 Picture communication symbols. ©1981-2009 by Mayer-Johnson LLC. All rights reserved worldwide. Used with permission. Boardmaker isa trademark of Mayer-Johnson LLC, P O Box 1579, Solana Beach, CA 92075 (www.mayer-johnson.com).
Change position Adjust bed down Adjust bed up Sit in chair
I want to rest Quiet please! Television Fan
Suction Mouth swab Cool cloth Blanket
ItchCool downHotPAIN
Chest pain Stop I need help Headache
Figure 4 One patient’s written notes communicate his physical and psychologicalneeds.
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from

from needing to rewrite commonneeds, and helps the health careteam more effectively understandand meet the physical and psycho-logical needs of the patient. A magicslate or dry erase board may not bethe best choice because everythingthe patient writes is usually erased.
Collaborate with the patient onhand signaling to convey basic needsor information. Communicate thisinformation in writing so that allstaff can interpret hand signals.
Make sure the call light is ineasy reach before leaving the room.Consult with the appropriate hospi-tal department as needed for modi-fied call light systems for weak orparalyzed patients. These include“easy-touch” switches and switchesthat patients can activate withmouth movement.
Consultation With the Speech-Language Pathology Service. Consultwith the speech-language pathologyservice for more complex alternativecommunication systems. Voice out-put communication aids are smallelectronic, computerized devicesthat can be used by typing or manip-ulating movement-sensitive switches.The cost of these devices usuallyprohibits most facilities from hav-ing a supply for use in the ICU.
An electronic larynx (electro -larynx) can enhance communica-tion for patients with temporary orpermanent voice loss. This hand-held device is easily operated bypressing the instrument to the neckto transmit sound into the pharynx,where the lips and tongue use it toform words. It is commonly used bypeople who have had a laryngec-tomy because it produces a “sound”that replaces the voice component ofspeech. Patients with a tracheostomy
could be considered for use of thedevice if they are able to articulateor mouth words to produce intelli-gible speech. Patients with weakspeech muscles are poor candidates.
Ewing13 reported that patientsrate use of an electronic larynx morefavorably than they rate use of padand pencil, lip movement, and signlanguage, indicating that the elec-tronic larynx was the least stressfulmethod, the easiest to use, and theclearest for self-expression. Use ofthe electronic larynx with criticallyill patients is often challengingbecause manual dexterity is requiredto place the electrolarynx against theneck and to coordinate the on/offmodes with speech attempts. Thenurse commonly manipulates thedevice in these situations. The speech-language pathologist should be con-sulted for instruction on correct use.
Consult with a speech-languagepathologist and a respiratory thera-pist to determine if a stable patientwith a tracheostomy is a candidatefor speech. Procedures include par-tial or total cuff deflation, use of a1-way speaking valve, and a special-ized tracheostomy tube with talkattachments, as discussed in thenext section.
Educate the Patient, the Patient’sFamily, and Staff in Communica-tion Strategies
The patient, the patient’s family,and staff must be educated on thecommunication strategies developedfor that specific patient. Communi-cation can be extremely frustrating,inefficient, and inaccurate if staffare each using different strategies.Such inconsistency can profoundlyaffect even simple movements foryes/no questions. A severely impaired
patient may be cued by one staff to“blink once for yes and blink twicefor no,” whereas a second staffmember may cue the patient in theopposite “blink once for no andblink twice for yes.”
Successful strategies includenoting the patient-specific commu-nication plan on the care plan andplacing it in an easily recognizedlocation for caregiver implementa-tion. Keep the patient-specific com-munication system at the bedsideon a clipboard for easy use. Be awareof patient privacy regulations thatmay limit postings. Assist anddemonstrate to the patient’s familyhow to communicate effectivelywith their loved one. Provide preop-erative education on the causes ofimpaired verbal communicationwhen a patient is intubated. Workwith the patient and the patient’sfamily members to identify effectivecommunication methods and ensurethat information is written on thecare plan. Table 4 summarizes thecommunication problem, causes,and management.
Speech With a Tracheostomy
Many patients with a tra-cheostomy, whether receivingmechanical ventilation support orbreathing spontaneously, can achievespeech with the tracheostomy tubein place. Determining a patient’scandidacy for speech should be acollaborative effort between mem-bers of the multidisciplinary team.Facilities vary in their practice, buttypically the physician orders anevaluation by the speech-languagepathologist, the pulmonary clinicalnurse specialist, and/or the respira-tory therapist.
CriticalCareNurse OnlineFirst www.ccnonline.org
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from

Several methods are available forachieving speech with a tracheostomy,and selection of the most effective,safe, efficient method should bebased on the patient’s clinical status.Five common methods are partialor complete cuff deflation, pluggingor capping the tube, use of a 1-wayspeaking valve, use of a tracheostomytube with a talk attachment, and useof a fenestrated tracheostomy tube.
Partial or Total Cuff Deflation Partial or total deflation of the
cuff is an option for clinically stabletracheostomy patients who are
receiving mechanical ventilation. Atracheostomy with the cuff inflatedprevents air from passing throughthe larynx for speech (Figure 5). Ifthe tracheostomy cuff is deflated byonly a few milliliters or completely,air leaks around the tube and passesthrough the larynx and out of themouth (Figure 6). The speech pro-duced with this technique is oftenreferred to as “leak speech.” Patientsoften need to work on coordinationof verbalizations with the inhalation/exhalation timing of the ventilatorin order to initiate speech/voiceduring the exhalation phase. They
can learn how to control air leakagethrough the mouth by occludingthe posterior pharynx area with thetongue and pharyngeal structure.
Plugging or Capping the TubeAnother option for patients
with a tracheostomy who are in sta-ble condition and do not requiremechanical ventilation is pluggingor capping the tube. Patients whoare breathing spontaneously orrequire partial ventilator supportcan be evaluated to determinewhether plugging the tube is appro-priate. Because the tube takes up
www.ccnonline.org CriticalCareNurse OnlineFirst
Table 4 Communication problem, causes, and management
Problem: Impaired ability to communicate verbally
Causes: Endotracheal tube, tracheostomy tube placement results in no air flowing past larynx when cuff is inflated, decreased ability toread lips if orally intubated, and tube-securing method occludes the patient’s mouth.
ManagementInitial evaluation/plan
1. Evaluate appropriate communication method(s) for client based on type and degree of physical disability and use of arms and hands,mental status, comprehension, language background, hearing, and vision. Refer to Table 2 (Communication Assessment Tool).
2. Communicate patient-specific plan on care plan and at bedside for easy implementation by caregivers. 3. Assist/Demonstrate effective communication methods to staff and patient’s family.
Interventions4. Maintain eye contact, preferably at patient’s eye level. Provide adequate room light. Make sure patient has glasses and hearing aid
if needed. 5. Ask yes/no questions one at a time, use pad/pencil, gestures, and word and alphabet board as appropriate. 6. Anticipate needs, ask questions related to personal care and comfort on a regular basis. Questions include the following: Do you
want to be turned? Do you need to be suctioned? Do you need to use the bedpan? Urinal? Do you have pain? 7. Initiate use of word board/phrase board appropriate for patient and tailored to meet individualized needs. Place in bold print on
communication board. Laminate if intended for long-term use.
Sample communication board for complex patient, total paralysisSuction, Urinal, Bedpan, Brush teeth, I am hot, I am cold, I can’t hear you, I am biting my tongue, Mouthguard, Bend elbows, Do
range of motion, Turn me, Raise my head, Change position of head, Reposition shoulders, Adjust my ear, There’s a lump underme, Wash around eyes, Push eyelashes out of eyes, Readjust pillow, Lower my head, Reposition my arms, Need pills (Valium,Tylenol, sleeping pill), Tube feeding running too fast, Brush hair, Turn on TV, Turn off TV, Turn up volume, Turn down volume,Change channels, Turn on radio, Pull out earplug, Put in earplug, Favorite channel is___, Gaze board.
Common messages of surgical patients experiencing short-term ventilator supportI am having pain, I am uncomfortable, I can’t breathe, How long will the tube be in?, When is the tube coming out?, Please untie
my hands, Where is my family? How am I doing? Please suction me to remove secretions.8. Convey calm, confident, reassuring approach. Maintain patience if patient gets frustrated or angry at not being able to communi-
cate needs. Empathize with patient.9. Seek assistance from other colleagues to help determine what the patient is trying to communicate. Avoid communicating your
frustration or blaming the patient for the problem. 10. Identify, validate meaning of nonverbal communication. Empathize with patient. 11. Involve family/significant other in plan of care as much as possible.12. Make sure call light is easy to reach before leaving room. Obtain modified call light system if patient is weak or paralyzed.13. Provide preoperative education about what to expect regarding impaired verbal communication when intubated. Identify effective
communication methods with patient/family and communicate specific information on care plan.14. Consult with speech therapy as needed to assist in providing effective communication methods.
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from

space in the trachea, plugging itcreates various degrees of airwayobstruction depending upon tubesize, tracheal size, and other possi-ble upper airway problems. Increasedairway resistance causes anxiety,respiratory distress, and potentialcardiopulmonary deterioration.
Before thetube is plugged,the cuff mustalways be com-pletely deflated.(See Table 6 forthe procedurefor cuff defla-tion.) Largertracheostomytubes cannot becontinuouslyplugged becauseof the increasedairway resistancethat results.Instead, thepatient may tol-erate intermit-tent plugging ofthe tube with afinger duringthe exhalationphase. Initiateplugging afterthe patient takesa breath, and dis-continue plug-ging the tube ifthe patient can-not exhale,speak, or com-plains of short-ness of breathand difficultybreathing.Teach capablepatients how tofinger occlude
the tracheostomy tube for speaking.In order to plug the tube success-fully and continuously, the tubemust be changed to a smaller diam-eter to decrease airway resistance byallowing more space for airflow inthe trachea. Changing to a tra-cheostomy tube with a cuff that
tightly collapses to the shaft of thetube may also improve space for air-flow in the trachea. Change to anuncuffed tube if a cuffed tube is nolonger needed. A 1-way speakingvalve may be attached to the tubeopening for speech.
1-Way Speaking ValveUse of a 1-way speaking valve is
a common method for achievingspeech with a clinically stablepatient with a tracheostomy who isbreathing spontaneously or receiv-ing mechanical ventilatory support.Although they are available fromseveral different manufacturers, 1-way valves have similar characteris-tics and functions. The Passy-MuirSpeaking Valve (Passy-Muir Inc,Irvine, California) is an example ofa 1-way valve that attaches to the15-mm hub of the tracheostomytube. The plastic valve opens oninspiration, allowing air to enterthe lungs. On exhalation, the valvecloses off and all air must exitthrough the upper airway (Figure 7).As it exits, exhaled air passes betweenthe vocal cords to produce the voicefor speech.
The cuff of the tracheostomytube must be completely deflatedfor all patients, regardless of whetherthey are receiving mechanical venti-lation, before attachment of the 1-wayvalve. Placing a 1-way valve on a tra-cheostomy tube with an inflatedcuff would allow a patient to inhalebut not exhale, a major error thatcan immediately lead to acute respi-ratory distress, barotrauma, andother life-threatening complications.Also, an improperly deflated cuffwith 1-way valve placement cancause an immediate and undesirableincrease in lung pressures and
CriticalCareNurse OnlineFirst www.ccnonline.org
Figure 5 When the cuff of the tracheostomy tube is inflated,air cannot pass through the larynx to generate speech. Reprinted with permission from Tippett and Siebens.14 Copyright 1995 by AmericanSpeech-Language-Hearing Association. All rights reserved.
Figure 6 When the cuff of the tracheostomy tube is partially orcompletely deflated, air can pass around the cuff and throughthe larynx, so speech is possible. Reprinted with permission from Tippett and Siebens.14 Copyright 1995 by AmericanSpeech-Language-Hearing Association. All rights reserved.
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from

trauma due to difficulty exhalingair through the narrowed airway.
Use of the 1-way valve typicallyinvolves the collaboration of a mul-tidisciplinary team that includes thenurse, physician, speech-languagepathologist, respiratory therapist,and patient. It is essential that thehealth care team thoroughly under-stand the indications, contraindi-cations, correct procedure, andmonitoring that are required with useof a 1-way valve. Table 5 summarizescontraindications to use of the 1-wayspeaking valve. Patients unable to usethe Passy-Muir Speaking Valve may
tolerate partialcuff deflation asdiscussed earlier.
Procedure forUse of the Tracheostomy1-Way Speak-ing Valve
Health careproviders mustpossess theknowledge andskills to deter-mine appropri-ate candidatesfor use of the 1-way speakingvalve. They also
must be able to make appropriateassessments and ventilator adjust-ments and to implement otherstrategies for successful use of thiscommunication technique. Table 6lists a specific procedure for suc-cessful and safe use of a Passy-MuirSpeaking Valve.
Specialized Tracheostomy Tube With Feature Designed for Speaking
Many critically ill patients arenot in stable enough condition totolerate cuff leaks with tidal volumeloss or tracheal occlusion. Several
manufacturers of tracheostomytubes have produced tubes with afeature to allow speaking (Figure 8).These tubes have dimensions simi-lar to the dimensions of other cuffedtracheostomy tubes. The unique fea-ture of these specialty tubes is that asmall section of tubing with an open-ing for airflow is attached above thecuff. This tubing exits the stomaand can be attached to an additionalsource of airflow with the flow rateregulated on a wall flowmeter accord-ing to the manufacturer’s recom-mendations. The patient or staffmember occludes a port on theexternal airflow tubing so that theadditional airflow is routed throughthe airflow tubing and exits into thetrachea just above the inflated tra-cheostomy cuff. This airflow can thenpass through the vocal cords forspeech. The air used for speaking isnot the air being used for ventilation.
The main barrier to successfuluse of the speaking tube is obstruc-tion of the small holes of the tubingwith secretions, which blocks theairflow. The hole above the cuff isonly several millimeters large andcan easily be occluded by the copi-ous secretions that accumulate abovean inflated cuff. These secretionsshould be removed by applying asuction source to the airflow tubing
www.ccnonline.org CriticalCareNurse OnlineFirst
Table 5 Contraindications to use of a 1-way speaking valve
Patient in medically unstable condition and/or requiring significant ventilator support (high respiratory rate and minute ventilationrequirements, high fraction of inspired oxygen, positive end-expiratory pressure greater than 5 cm H2O, respiratory distress, fre-quent bronchospasm and air-trapping problems)
Pneumothorax with air leak and without air leak if there is any potential for increase in lung pressuresLarger diameter tracheostomy tubeTracheostomy tube with inflated cuff Tracheostomy tube with foam cuffAirway above tracheostomy not patent: obstruction can be caused by numerous factors including bilateral vocal cord paralysis, severe
tracheal or laryngeal stenosis, tumor obstruction, or secretionsCopious, excessive, or thick secretionsParalysis of lips, tongue, and other muscles involved in speechLaryngectomy
Figure 7 A 1-way speaking valve.
Larynx
Trachea
1-way valve
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from

and suctioningout the secre-tions. The tubemay also not fitproperly in thepatient’s tra-chea, causingblockage of theairflow port andan ineffectivetube for speak-ing. Patientswith handweakness orparalysis are
unable to occlude the port for initi-ating voice and must rely on thenurse for assistance and adjustmentof the wall airflow. This optionshould be considered for patientswho have not had success with themore common techniques for speechand need the cuff to remain inflatedfor optimal ventilation.
Fenestrated Tracheostomy Tubefor Patients Who Do Not RequireMechanical Ventilation
If the plan is to plug a tra-cheostomy tube for speaking, a
CriticalCareNurse OnlineFirst www.ccnonline.org
Table 6 Procedure for placement of a 1-way speaking valve
1. Evaluate the patient to determine whether the device is appropriate. The patient should be awake, attempting to communicate, andshould not have contraindications to use. Collaborate with the physician, speech pathologist, and respiratory therapist.
2. Explain the plan to the patient. Gather the necessary clinicians at the bedside, often including the bedside nurse and respiratory therapist and/or speech pathologist.
3. Verify that all equipment is readily available, including suction catheter, suction, manual resuscitation bag.4. Position patient for breathing comfort, usually with head of bed elevated.5. Deflate cuff completely.
a. Suction oral cavity and tracheostomy tube if needed.b. Completely deflate the cuff.c. Be ready to immediately suction the trachea and mouth of any secretions that may have pooled above the cuff and are forcedinto the mouth with coughing or ventilator airflow.
6. Attach valve to tracheostomy tube. If patient is ventilator dependent, attach flex tube adapter or swivel valve adapter; reattach venti-lator tubing.
7. Adjust, as needed, the ventilator tidal volume higher to compensate for leakage around tube, reset volume and pressure alarms, andmake other ventilator adjustments including turning off PEEP to prevent machine self-cycling.
8. Monitor tolerance including breathing comfort and ability to exhale easily. Immediately remove the valve if the patient complains ofrespiratory distress, breathing discomfort, or shortness of breath or if observations show difficulty with air exchange, inadequatechest deflation indicating impaired exhalation, the appearance of “air trapping,” increased respiratory rate, increased respiratorymuscle use, and various other signs of increased work of breathing. Readjust the ventilator to ensure adequate ventilation andreassess the patient for contraindications.
9. Caution: If the patient has difficulty exhaling, vocalizing will be difficult for the patient. The patient most likely is not a good candi-date for the valve because of significant airway resistance from the tube or other problems. Avoid placing the patient in a situationof uncomfortable breathing, which may affect future communication interventions.
10. Instruct ventilator-dependent patient to “notice that air fills your lungs with air when the machine gives you the breath of air. Breath-ing out will be through your nose and mouth.” Coach the patient to “take a breath in first, then speak.” Initially try vocalizing withsimple sounds like “Ahhhh…..” or count “1,2,3,4….” Provide direction and reassurance as needed.
11. Provide adequate oxygenation and monitor oxygenation status with pulse oximetry. Maintain SpO2 at 90% or greater or be alert toacute problems if SpO2 starts decreasing from the patient’s baseline level while on the ventilator.
12. Remove the valve and suction as needed to maintain a patent airway. Provide ventilation support as needed. Note: Secretions canobstruct air passage outside the tube, causing respiratory distress and valve intolerance. Although a 1-way speaking valve canimprove the strength of the cough, it may be difficult for the patient to cough secretions up to the mouth with the valve in placebecause of the small space between the tube and the trachea, thicker secretions, inability to take deep breaths, and the weak cough.
13. Provide an oral suction system for patients who can to suction the oral cavity.14. Remove the valve before starting nebulizers/ aerosol treatments to prevent damage of the valve. Remove the valve when the patient
is sleeping.15. Readjust the ventilator to previous settings after valve removal, and recheck the patient/ventilator system to ensure optimal ventilation.16. Spontaneously breathing patient: Provide ventilation assistance as needed with a manual resuscitation bag to assist with deep
breaths and secretion clearance.
Abbreviations: PEEP, positive end-expiratory pressure; SpO2, oxygen saturation as determined by pulse oximetry.
Figure 8 A tracheostomy tube with the feature that allowsspeaking while the cuff is inflated.Reprinted from Dikeman and Kazandjian,15 with permission from Delmar Learning,a part of Cengage Learning, Inc. ©1996.
Ventilator air
Speaking air
Air source
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from

fenestrated tracheostomy tube maybe placed to allow more airflowthrough the trachea and therebyhelp decrease airway resistance. Thefenestration is a hole located on theoutside of the tube that allows air totravel through the tube if the innercannula is removed and the fenes-tration is properly located in the tra-chea (Figure 9). Before the tube isplugged, the cuff must be com-pletely deflated.
Some fenestrated tubes do notfit properly in certain patient’sanatomies, and the hole may beblocked by the tracheal wall tissue.Such blockage can affect breathingand also place the patient atincreased risk for granulation tissueformation at the site of the fenestra-tion. The tube should always beevaluated for proper position of thefenestration by visual inspectionwith an endoscope by a specialisttrained to evaluate the tube prop-erly. Potential for this problem maybe evaluated simply by removingthe inner cannula and looking witha flashlight into the tracheostomytube to observe for an open holeversus a hole blocked by trachealwall tissue. If the hole is against thetracheal wall, it can be a source oftracheal irritation or tissue growthinto the fenestration and trachea.The tube should not be used if thefit is improper.
It may be difficult for somepatients, even patients with strongcoughs, to cough secretions throughthe narrow space in the trachea andthrough the fenestration, especiallyif secretions are thick and tenacious.The tracheostomy plug should beremoved and secretions suctionedas needed if sounds of secretions areaudible or the patient complains of
needing suctioning, feels short ofbreath, or has respiratory distress.Reevaluate the patient’s respiratorystatus after the tube is plugged.Close monitoring throughout tubeplugging is essential as mostpatients are unable to remove tracheostomy plugs on their own.When the patient needs to receivemechanical ventilation, the innercannula is replaced, the cuff isinflated, and the ventilator adapteris reattached to the ventilator, whichis properly set up and functioning.
Suggested Research Priorities for Effective Communication
Loss of speech is a frighteningexperience16 and can cause anxiety,agitation, and various other adversephysiological effects as well as adverseventilator effects. Although ICU
nurses commonly care for patientswith complex communication needs,nurses may receive little or no train-ing in facilitating or interpretingcommunication for ventilator-dependent patients or in usingdevices to improve the effectivenessof communication.15,16 Assistive andaugmentative devices are availableto improve communication; how-ever, it is not surprising that theyare rarely used.2 It is essential toassess the patient’s ability to com-municate, establish an effective careplan with strategies customized forthe patient’s needs, and ensure thatall staff can effectively interact withthe patient to determine needs andconcerns.17,18 The American ThoracicSociety Statement on Research Pri-orities in Respiratory Nursing16 rec-ommends the following:
Studies are needed toimprove nurse-patientcommunication, includinginterpretation of non-vocalbehaviors. In addition,studies are needed todetermine ways of bestassisting patients to useavailable communicationdevices. Strategies need tobe tested to improve healthcare provider communica-tion skills.
Testing combinations of alterna-tive augmentative technologies,consultation, and training of care-givers may create effective commu-nication options for nonspeakingpatients. Systematic research mayassist in determining the differen-tial effects of these treatments andprofiles of successful users of alter-native augmentative communica-tion systems.19
www.ccnonline.org CriticalCareNurse OnlineFirst
Figure 9 Fenestrated tracheostomytube for patients who do not requiremechanical ventilation.
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from

It is common for neuropsycho-logical and functional deficits tooccur in ICU patients receiving
mechanical ventilation because ofthe various sedative medicationscommonly used. Studies are needed
to test the frequency, severity, andpotential causes of these deficits withthe goal of testing interventions to
CriticalCareNurse OnlineFirst www.ccnonline.org
Table 7 Case management: meeting communication needs in a variety of situations
Case 1: Mary is a 60-year-old woman who had an elective knee replacement 3 days ago complicated by respiratory arrest that requiredemergent intubation and mechanical ventilation support. With every “sedation holiday,” she exhibits severe anxiety, bangs on siderails of her bed, attempts to speak, and pulls on the endotracheal tube. These behaviors made it necessary to use restraints and seda-tion to maintain Mary’s safety and comfort.
Assessment: Mary experienced adverse outcomes after surgery and was unfamiliar and unprepared for the experience of waking upbeing unable to communicate verbally and is most likely feeling uncomfortable and/or in pain from the surgery, the endotracheal tube,and the chest compressions. Her anxiety, restlessness, and various other undesirable behaviors are normal and expected in this fear-ful and uncomfortable situation.
Management: The nurse in the intensive care unit displayed a calm, confident, and reassuring approach and provided focused attentionto explain clearly and simply why Mary was unable to speak with the tube in place and that she would be able to speak when the tubewas removed. She worked with Mary to identify effective communication methods, which included nodding her head to yes/no ques-tions and removing restraints so the patient could write on a dry erase board and point to letters on an alphabet board. Implementingthese strategies allowed Mary to communicate basic wants, needs, and feelings and enabled the nurse to provide effective interven-tions, which then led to resolution of her undesirable behaviors and sedation use. She was successfully extubated several days later.
Case 2: Steve is a 17-year-old boy who was in a high-speed motor vehicle accident that resulted in multiple traumatic injuries includinga severe C5 spinal cord injury that required surgical stabilization, use of a halo, and tracheostomy placement. Steve’s family and staffare frustrated and saddened because they are unable to understand his attempts to communicate. Nursing and medical staff are hav-ing difficulty assessing his general mentation and mood.
Assessment: It is a normal response for Steve to feel very anxious, confused, and frightened when he woke up after such a traumaticseries of events. Shock, disbelief, and various emotions experienced by the patient and the patient’s family are also normal. Stressful situ-ations commonly result in the need to frequently repeat or clarify information provided to the patient or family. Steve and his family neededucation on many topics regarding spinal cord injury and its management. Spacing out their education is important to meet their needs,yet not make them feel more overwhelmed and stressed. Steve cannot write or gesture for communication because of quadraparesis. Heis unable to shake his head yes/no because of the halo. In his frustration to communicate, Steve has not been interactive with staff orfamily and is no longer attempting to express care needs. He can elicit distinct eye blink responses for a reliable yes/no answer.
Management: His nurse educated the family and other health care staff that Steve was using 1 blink for yes and 2 rapid blinks for no.As facial injuries resolved, it became easier for staff and family to read Steve’s lips, but he needed frequent reassurance and cues toslow down and not become frustrated with communication breakdowns. As a supplement to mouthing words, he used a communica-tion board with partner-directed scanning. For this technique, the listener holds a communication board/message board/alphabetboard and runs his or her finger across the rows and/or columns. When the target is pointed at, the patient makes a response such asan eye blink. As Steve’s respiratory status stabilized, ventilator support was needed only during the night with a tracheostomy domeused during the day. Speech pathology, working with respiratory therapy and nursing, helped him begin to use a Passy-Muir SpeakingValve (PMSV). As he started verbally communicating, he became more alert, increased interaction with staff and family, and was ableto discuss spinal cord issues with his multidisciplinary team.
Case 3: Herb is a 78-year-old man with a history of chronic obstructive pulmonary disease, hypertension, and coronary artery bypass.He suffered a severe postoperative head bleed that resulted in right hemiparesis and suspected language impairments. After severaldays of tracheostomy placement, Herb is successfully breathing spontaneously on a tracheostomy dome and receiving mechanicalventilation support only at night.
Assessment: Herb is very frustrated by communication deficits resulting from the neurologic lesion that caused expressive aphasia. Heis unable to speak with the tracheostomy in place and is unable to write because of right hemiparesis (patient is right handed) andaphasia. Herb is confused about the tube in his throat and his new functional deficits.
Management: Nursing and speech pathology staff explained the tracheostomy and speaking deficits to the patient and his family. Staffcommunicated by asking basic yes/no questions. Use of a picture board for communicating basic needs worked very well because itis picture based and does not rely on language skills. Staff placed a timely consult to the speech pathologist for evaluation of PMSVuse. Herb began speaking with the PMSV while on the tracheostomy dome and was able to communicate basic messages and partici-pate in language therapy for his aphasia. He continued to benefit from staff and his family adapting their communication styles to hisnew language deficits/aphasia.
Case 4: Beth was a 28-year-old patient with a rapidly growing malignant brainstem tumor that invaded several cranial nerves, causing arapid deterioration, over a 2-week period, in her ability to speak and move. Speech remained intact after her first surgery, but rapidonset of dysarthria with headaches required a second surgery.
Assessment: Tumor invasion to the cranial nerves and the brainstem resulted in Beth’s inability to voice, cough, and protect her airway.Staff and family were unable to read her lips because of the impaired oral motor function. She appeared frustrated, attempting to askquestions rather than just respond to staff’s questions. Rapidly progressing quadraparesis over several hours resulted in the need toimplement many different communication methods to meet her needs to actively participate in end-of-life decisions and communicatewith her loved ones.
Continued
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from

decrease the impact of the deficits.16
One example is a study of the effectof implementing effective communi-cation strategies on decreasing theneed for sedative medications andthereby minimizing adverse neu-ropsychological consequences.
Communication assessmenttools should be evaluated to deter-mine whether they are user-friendlyand meet the desired outcome ofdetermining and implementingeffective communication strategies.The assessment tool (Table 2) devel-oped and presented in this articlerequires clinical evaluation.
Various types and sizes of letterboards, word boards, and phraseboards are available to enhancecommunication. Few descriptive orempirical studies have addressedthe content and format of these tools
or patients’ perspectives on decreas-ing frustration with communication.Research is needed to test the effectsof communication boards and variousother methods used to facilitate com-munication on outcomes, includingpatients’ anxiety and satisfaction,adequate pain management, andduration of mechanical ventilation.3
Research is also needed to determinethe types of communication toolsthat are most effective for individualtypes or categories of patients.
SummaryCommunicating effectively with
ventilator-dependent patients isessential for the provision of qual-ity care. Cases presented in Table 7summarize a variety of clinical situ-ations and highlight useful commu-nication strategies that effectivelymeet the needs of patients andtheir families. It is important fornurses to assess communicationneeds; identify appropriate alterna-tive communication strategies; cre-ate a customized care plan with thepatient, family, and other team
members; ensure that the care planis visible and accessible to all staffinteracting with the patient; andcontinue to collaborate with col-leagues from all disciplines to pro-mote effective communication withnonvocal patients. Patients’ familymembers also need to be educatedand supported in their efforts tocommunicate and care for theirloved ones. CCN
Financial DisclosuresNone reported.
References1. Happ MB, Tuite P, Dobbin K, Divirgilio-
Thomas D, Kitutu J. Communication ability,method, and content among nonspeakingnonsurviving patients treated with mechan-ical ventilation in intensive care unit. Am JCrit Care. 2004;13(3):210-222.
2. Happ MB. Communicating with mechani-cally ventilated patients: state of the science.AACN Clin Issues. 2001;12(2):247-258.
3. Patak L, Gawlinski A, Fung NI, et al. Com-munication boards in critical care: patients’views. Appl Nurs Res. 2006;19(4):182-190.
4. Grossbach I. Ventilator troubleshootingguide. In: Chulay M, Burns S, eds. AACNEssentials of Progressive Care Nursing. NewYork: McGraw-Hill; 2007:487-497.
www.ccnonline.org CriticalCareNurse OnlineFirst
Table 7 Continued
Management: Physicians discussed the severity of Beth’s disease with her family and questioned whether they wished to pursueaggressive treatment or more palliative care. Beth’s family felt that it was important for Beth to be awake without sedation in order toindicate her wishes to medical staff. The sedation was weaned and she was extubated to high-flow oxygen via a mask. Beth consis-tently indicated that she consented to trial radiation therapy and temporary intubation, if needed, but refused tracheostomy. Withinhours after extubation, she required reintubation. She allowed staff to intubate her on the condition that she be given breaks in seda-tion so that she could indicate to staff her desires to continue or withdraw treatments. She initially was able to reliably shake her headfor yes/no responses. A clipboard, paper, and pencil with hand grip were provided and she was able to write words with inconsistentlegibility. The speech pathologist known to Beth developed a specialized communication board with phrases regarding treatmentoptions, questions about treatment, and key phrases such as “I want…”, “I do not want…”, “Please stop…”. Phrases also addressedcomfort and emotional issues like “I am scared” and “I am anxious”. Within 2 days of starting radiation therapy, Beth was too weak towrite but was able to point to items on the letter board/phrase board. On day 4, her development of complete quadraparesis over sev-eral hours prevented her from pointing to the communication boards. She was able to shake her head for yes/no and to select an itemon the communication board while staff or family ran their fingers over the rows of letters/phrases. As the day progressed, she wasunable to move her head so staff implemented an eye-blink system (1 for yes, 2 rapid blinks for no). Her family and physiciansexplained her situation and Beth clearly indicated that she did not want to continue medical treatment. Within a couple hours, itbecame difficult to discern purposeful blinking from reflexive blinks, particularly as Beth became tearful with family and friends gath-ering at her bedside. Staff then adjusted communication to eye movements (look up for yes, down for no). With this method, Bethconsistently indicated that she would like to withdraw treatment. Family and staff felt confident that Beth’s decisions were consistentwith prior discussions despite use of a variety of alternative modes of communication. Beth was withdrawn from life support sur-rounded by family, friends, and staff.
Now that you’ve read the article, create or contributeto an online discussion about this topic using eLetters.Just visit www.ccnonline.org and click “Respond toThis Article” in either the full-text or PDF view ofthe article.
To learn more about patients receivingmechanical ventilation, read “Not-so-TrivialPursuit: Mechanical Ventilation RiskReduction” by Mary Jo Grap in the Ameri-can Journal of Critical Care, 2009;18:299-309. Available at www.ajcconline.org
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from
5. Dreyer A, Nortvedt P. Sedation of ventilatedpatients in intensive care units: relatives’experiences. J Adv Nurs. 2008;61:549-556.
6. Engstrom A, Soderberg S. The experiencesof partners of critically ill persons in anintensive care unit. Intensive Crit Care Nurse.2004;20(5):299-308.
7. Happ MB, Swigart VA, Tate JA. Family pres-ence and surveillance during weaning fromprolonged mechanical ventilation. HeartLung. 2007;36(1):47-57.
8. Jablonski RS. The experience of beingmechanically ventilated. Qual Health Res.1994;4:186-207.
9. Kabes AM, Graves JK, Norris J. Further vali-dation of the nonverbal pain scale in intensivecare patients. Crit Care Nurse. 2009;29:59-66.
10. Carroll SMC. Lip-reading translating fornon-vocal ventilated patients. J Assoc MedProf Hearing Losses. 2003;1(2). www.amphl.org/articles/carroll2003.pdf. 2003. AccessedJuly 27, 2010.
11. Lawless CA. Helping patients with endotra-cheal and tracheostomy tubes communicate.Am J Nurs. 1975;75(12):2151-2153.
12. Fowler SB. Impaired verbal communicationduring short-term oral intubation. NursDiagn. 1997;8(3):93-98.
13. Ewing DM. Electronic larynx for aphonicpatients. Am J Nurs. 1975;(12):2153-2156.
14. Tippett DC, Siebens AA. Preserving oralcommunication in individuals with tra-cheostomy and ventilator dependency. Am JSpeech-Language Pathol. 2005;4(2):56-57.
15. Dikeman KJ, Kazandjian MA. Communica-tion and Swallowing Management of Tra-cheostomized and Ventilator-Dependent Adults.San Diego, CA: Singular Publishing Group,Inc; 1995:188.
16. Larson JL, Ahijevych K, Gift A, et al. ATSStatement: American Thoracic Societystatement on research priorities in respira-tory nursing. Am J Respir Crit Care Med.2006;174(4):471-478.
17. Finke EH, Light J, Kitko L. A systematicreview of the effectiveness of nurse commu-nication with patients with complex com-munication needs with a focus on the useof augmentative and alternative communi-cation. J Clin Nurs. 2008;17(16):2102-2115.
18. Consortium for Spinal Cord Medicine. Res-piratory Management Following Spinal CordInjury: A Clinical Practice Guideline forHealth-Care Professionals. Washington, DC:Paralyzed Veterans of America; 2005. www.guidelines.gov/summary/summary.aspx?doc_id=7198&nbr=004301&string.Accessed July 27, 2010.
19. Happ MB, Garrett KL, Roesch T. AAC inthe ICU: Critical Issues and PreliminaryResearch. Aac.unl.edu/drb/as03/aac-icu.pdf. 2003. Accessed July 27, 2010.
CriticalCareNurse OnlineFirst www.ccnonline.org
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from

Irene Grossbach, Sarah Stranberg and Linda ChlanPromoting Effective Communication for Patients Receiving Mechanical Ventilation
http://ccn.aacnjournals.org/Published online ©2010 American Association of Critical-Care Nurses
10.4037/ccn2010728 2010;Crit Care Nurse
http://ccn.aacnjournals.org/cgi/external_ref?link_type=PERMISSIONDIRECTPersonal use only. For copyright permission information:
http://ccn.aacnjournals.org/subscriptions/Subscription Information
http://ccn.aacnjournals.org/misc/ifora.xhtmlInformation for authors
http://www.editorialmanager.com/ccn Submit a manuscript
http://ccn.aacnjournals.org/subscriptions/etoc.xhtmlEmail alerts
362-2049. Copyright ©2016 by AACN. All rights reserved. bimonthly by AACN, 101 Columbia, Aliso Viejo, CA 92656. Telephone: (800) 899-1712, (949) 362-2050, ext. 532. Fax: (949) Critical Care Nurse is an official peer-reviewed journal of the American Association of Critical-Care Nurses (AACN) published
by AACN on May 12, 2018http://ccn.aacnjournals.org/Downloaded from





























