Embed Size (px)
Citation preview

Applied Radiation and Isotopes 72 (2013) 16–29
Contents lists available at SciVerse ScienceDirect
Applied Radiation and Isotopes
0969-80
http://d
n Corr
E-m
journal homepage: www.elsevier.com/locate/apradiso
Feasibility study of gamma-ray medical radiography
Abdalmajeid M. Alyassin a,n, Hamza A. Maqsoud b, Ahmad M. Mashat b, Al-Sayed Al-Mohr b, Subhan Abdulwajid b
a Physics Department, Faculty of Science, Yarmouk University, PO Box 566, Irbid 21163, Jordanb Nuclear Engineering Department, Faculty of Engineering, King Abdulaziz University, PO Box 80204, Jeddah, 21589, Saudi Arabia
H I G H L I G H T S
c Characterized the performance of gamma-ray radiography.c Displayed medical images of humanoid phantoms using gamma radiography.c Am-241 has the right inherent parameters to be used in diagnostic medical imaging.c Outlined the main advantages and disadvantages of using gamma-radiography.c Production of a pure Am-241 will help in making the exposure times more clinically reasonable.
a r t i c l e i n f o
Article history:
Received 9 March 2012
Received in revised form
15 October 2012
Accepted 5 November 2012Available online 9 November 2012
Keywords:
Gamma-ray radiography
Am-241
Medical imaging
Computed radiography
43/$ - see front matter & 2012 Elsevier Ltd. A
x.doi.org/10.1016/j.apradiso.2012.11.001
esponding author.
ail address: [email protected] (A.M. Al
a b s t r a c t
This research explores the feasibility of using gamma-ray radiography in medical imaging. We will
show that gamma-ray medical radiography has the potential to provide alternative diagnostic medical
information to X-ray radiography. Approximately one Ci Am-241 radioactive source which emits
mono-energetic 59.5 keV gamma rays was used. Several factors that influence the feasibility of this
study were tested. They were the radiation source uniformity, image uniformity, and image quality
parameters such as contrast, noise, and spatial resolution. In addition, several gamma-ray and X-ray
images were acquired using humanoid phantoms. These images were recorded on computed radio-
graphy image receptors and displayed on a standard monitor. Visual assessments of these images were
then conducted.
The Am-241 radioactive source provided relatively uniform radiation exposure and images. Image
noise and image contrast were mainly dependent on the exposure time and source size, whereas spatial
resolution was dependent on source size and magnification factor. The gamma-ray humanoid phantom
images were of lower quality than the X-ray images mainly due to the low radioactivity used and not
enough exposure time. Nevertheless, the gamma-ray images displayed most of the main structures
contained in the humanoid phantoms. Higher exposure rates and thus lower exposure times were
estimated for different pure Am-241 source sizes that are hypothesized to provide high quality images
similar to X-ray images. For instance, a 10 mm source size of pure Am-241 with 7 s exposure time
should produce images similar in contrast and noise to X-ray images. This research paves the way for
the production and usage of a highly radioactive Am-241 source with the potential to lead to the
feasibility of acceptable quality medical gamma-ray radiography.
& 2012 Elsevier Ltd. All rights reserved.
1. Introduction
Medical images may be formed and constructed by severalmedical imaging modalities. Each imaging modality providesunique image features. For instance, X-ray planar imaging pro-vides higher spatial resolution than computed tomography (CT)
ll rights reserved.
yassin).
imaging. However, CT images provide a better low contrastresolution (Bushberg et al., 2002). In addition, X-ray imageacquisition is fast, easy to use, and may be portable, whereas,CT provides tomography images which allow for the construc-tion of 3D data (Alyassin, 2009; Fournier et al., 2007).
Unlike CT, the magnetic resonance imaging (MRI) modalityuses non-ionizing radiation to form medical images that providean excellent soft tissue contrast (Hendee and Ritenour, 2002).However, MRI requires longer acquisition time, is more expen-sive, has lower bone and calcification visualizations, and is less

A.M. Alyassin et al. / Applied Radiation and Isotopes 72 (2013) 16–29 17
quantitative than CT (Alyassin, 2009). All these modalities com-plement each other. Currently there is a revolution in multi-modality medical data such as positron-emission-tomographyPET and CT, single photon emission computed tomography(SPECT) and CT, X-ray and Ultrasound (US), PET and MRI.Multimodality-data has proven to provide better diagnosticinformation than an individual medical modality (Kapur et al.,2002; Krug et al., 2010; Liu et al., 2011; Pichler et al., 2008).
In ionizing radiation imaging modalities images may beacquired through transmission or emission scans. X-ray and CTprovide transmission scans which mean the X-ray source islocated outside the patient and the X-ray field transmittedthrough the patient records the final image on the image receptor.Unlike CT and X-ray, nuclear medicine (NM) images are formedthrough an emission scan which means the source of radiation islocated inside the patient and the radiation emitted from thesource is recorded on the detectors that are located outside thepatient. NM imaging mainly provides functional informationwhereas the transmission scans mainly provide the anatomicalinformation (Raan et al., 2000). The sources of radiation that areused in diagnostic NM imaging are radioactive sources thatmainly emit gamma-rays with energies in the diagnostic range(Huda and Slone, 2003; Bushberg et al., 2002).
Radioactive sources have been reported in literature to providetransmission scans to show some anatomical structures. Howeverthese scans have either been used for special procedures or withspecial dedicated detectors. They have not addressed the require-ments or the needs of general diagnostic medical imagingprocedures with gamma-rays. For instance, some researchershave used gamma-ray scans for attenuation correction in PET(Bailey et al., 2005; Kaplan and Hynor, 1999; Raan et al., 2000).Other researchers have generated beta particle images andgamma-ray images with a special digital probe that was used inradioguided surgery (Tipnis et al., 2004). Some researchers havedeveloped a special radiation-imaging device for imaging withlow-intensity gamma-ray sources (Woodring et al., 1999) whileothers have used gamma-ray imaging with a multiple pinholeimager in NM (Meng et al., 2003).
In addition, much work has been published about industrialgamma-ray radiography (Verbinski and Orphan, 1997). However,the radioactive sources that are typically used in industrialgamma-ray radiography are Cs-137 and Co-60, which emit on
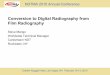
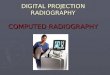
Fig. 1. The Americium-241 radioactive source. Part (A) shows the whole s
the average, high energy photons of 0.662 MeV and 1.25 MeV,respectively (IAEA, 1999). These energies are much higher thanthe diagnostic energy range. Amercium-241 (Am-241) emitsgamma-rays within diagnostic X-ray range (25–150 keV) andhas been used in brachytherapy (Muench and Ravinder, 1992;Randinder et al., 1990; Ravinder et al., 1987). It was brieflyintroduced in producing medical images (AbdulMajid, et al.,2010). Therefore, there is a tremendous lack of testing thefeasibility of using the Am-241 radioactive source in producinggamma-ray transmission scans that provide medically diagnosticinformation.
This research tackles the feasibility of using gammy rays informing medical images using Am-241 source. Am-241 sourceemits mono-energetic photons with energies that fall within thediagnostic range. It has also a very long half-life which reducesfrequency of replacement of the gamma-ray source. The Am-241gamma-ray imager should produce medical images with lowerdose than the dose delivered by an X-ray machine. It’s expectedthat the patient radiation dose will be lower when using adiagnostic mono-energetic photon beam than when using apoly-energetic photon beam with similar mean energies(Bushberg et al., 2002).
This article first lists the equipment used then describes themethods which consist of some estimated radiation exposurevalues for Am-241 and many experimental medical image qualitytests. Last, it discusses the results of this research and thenconcludes with the main achievements of this article.
2. Materials
The materials that were used in our research were; anAmercium-241 (Am-241) radioactive source, several 2 mm sheetsof lead with different circular size openings, three Kodak com-puted radiography (CR) image receptors, image quality phantoms,and several humanoid phantoms.
The activity of the Am-241 source at the time of our acquisi-tions was 0.965 Ci. The diameter of the source that was used toexpose and image our objects was roughly 29 mm (see Fig. 1).However, the thickness of the source was not measured becausethe source was permanently mounted into the source stand. TheAm-241 radioactive source emits 35.9% of the time a 59.5 keV and
tand and (B) shows a close up view of the source when it is opened.

Fig. 2. Sheets of lead with 2 mm thickness with circular openings. Part (A) shows the sheets of lead that represents the collimators. Part (B) shows the sheets of lead that
represents the source openings that will be aligned with center or one of the sides of the actual source.
A.M. Alyassin et al. / Applied Radiation and Isotopes 72 (2013) 16–2918
2.4% of the time 26 keV gamma photons. These energies fallclearly within the diagnostic range. Am-241 decays toneptunium-237 with 100% emission of alpha particles. Energiesof these alpha particles range from 4.758 to 5.545 MeV. The half-life of Am-241 is 432.2 years (Strain and Leddicottee, 1962).
Several 2 mm sheets of lead with openings were used ascollimators. The shape of the openings was roughly circular withdiameters of 2.3 cm, 4 cm, and 5.6 cm as shown in Fig. 2A.In addition, several 2 mm sheets of lead with circular openingswere used to define the source sizes. The diameter of the openingswere roughly 2 mm, 4 mm, 6 mm, 8 mm, 10 mm as shown inFig. 2B. The 2 mm thickness of lead was thick enough to blockmost of the gamma photons and of course the alpha particlesemitted from the Am-241 source (Strain and Leddicottee, 1962).This was also verified by a portable radiation survey meter.
The computed radiography (CR) image receptor was the KodakCR-140. Three different cassette sizes were used in the experi-ments. The dimensions were 800 �1000 with a 0.08 mm pixel size(6.25 lp/mm), 1000 �1200 with a 0.12 mm pixel size (4.2 lp/mm),and the 1400 �1700 with a 0.17 mm pixel size (2.94 lp/mm). Theseimage receptors will be referred to as high resolution CR, Mediumresolution CR, and low resolution CR, respectively.
The test objects used in the experiments were image qualityphantoms as well as humanoid phantoms. The image qualityphantom that was used to assess contrast and noise was a litersize plastic bottle that was filled with water. The resolutiontest phantom was the line-pair PTW-Freiburg phantom Model
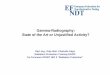
CN-31682 with spatial resolution that ranges from 0.25 lp/mmto a maximum 10 lp/mm with 41 steps as shown in Fig. 3A.A triangular prism phantom was built to develop the contrastdetail curve for gamma-ray imaging as shown in Fig. 4 (Bushberget al., 2002). The phantom dimensions were 13 cm�9 cm�2 cm.The diameters of the holes were 8 mm, 6 mm, 4 mm, 2 mm, and1 mm. These holes were filled with a common off the shelfcandle wax.
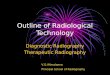
Several humanoid phantoms that are shown in Fig. 5 wereused to visually assess clinical image quality. The head of theRANDO man phantom was used for head imaging. The followingNuclear Associates’ human anatomical transparent phantomswere used; the chest model-76-083, the torso model-76-042,the elbow model-76-076. In addition, the SIB (PTW-Freibury TYP42001) mammography phantom was used. A RadCal Accu-Dose-2086 dosimeter was used to estimate the radiation exposure.
3. Methods
Fig. 6A shows the basic geometry that was used in thisresearch. The openings of the radioactive source were varied byplacing lead sheets with different circular openings attachedclosely to the source as shown in Fig. 2B. These lead sheets withsource circular openings (SCO) simulate different focal spot sizes.Similarly, the sheets of lead with different collimator circularopenings (CCO) represent the collimators as shown in Fig. 2A.

Fig. 4. The contrast detail phantom. The phantom dimensions were 13 cm length by 9 cm width by 2 cm height. The diameters of the holes were 8 mm, 6 mm, 4 mm,
2 mm, and 1 mm. Part (A) shows the phantom without fillings. Part (B) shows the phantom with the candle fillings.
Fig. 3. The spatial resolution phantom and its gamma-ray radiographic image.Part (A) shows the spatial resolution line-pair phantom. Part (B) shows the gamma-ray
radiographic image, which by visual inspection was estimated to have a 2.75 lp/mm spatial resolution.
A.M. Alyassin et al. / Applied Radiation and Isotopes 72 (2013) 16–29 19
The collimators were placed 12 cm away from the source. A CR-140 image receptor was placed further at different source toimage distances (SIDs) as needed in the experiments. The experi-ments in this research did not use an anti-scatter grid.
3.1. Exposure times estimates
Estimate of exposure times for different SCOs were prepared at80 cm SID as a general timing guideline. This estimation wasbased on determining the exposure time needed to obtain a500 mR radiation exposure. It is suggested in the literature thatthis exposure value was adequate to obtain a satisfactory X-rayimage (Huda and Slone, 2003). The calculation assumed also thatthe source was a point Am-241 radioactive source that emitsonly 35.9% of the time 59.5 keV gamma rays (Khan, 2010).The exposure rate was estimated using Eq. (1) (Khan, 2010):
X�
¼GA
SID2
mR
hr
� �ð1Þ
where C is the gamma ray constant, A is the activity of the source,and SID is the source to image distance. The gamma ray constantwas calculated using Eq. (2).
G¼ 0:5� E� fR �m2
Ci� hr
� �ð2Þ
where E is the energy of the gamma ray emitted by the Am-241source which is equal to 0.0595 MeV, and f is the probability of the
gamma decay which is equal to 0.359. The exposure time required to
obtain a 500 mR radiation exposure was estimated using the exposure
rate calculated in Eq. (1).Additionally, an estimate of the unblocked activity for the
different SCOs (10 mm, 8 mm, 6 mm, 4 mm, and 2 mm) was
estimated. The effective activity was expected to be reduced
when the SCO was reduced leading to a lower exposure and
longer times. The reduction in radioactivity was estimated based
on the ratio of the SCO diameters squared and a known activity as

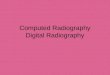
Fig. 5. The humanoid phantoms. Part (A) shows the head phantom (part of the Rando man phantom). Part (B) shows the chest phantom. Part (C) shows the torso phantom.
Part (D) shows the elbow phantom. Part (E) shows the mammography phantom.
Fig. 6. The basic geometry setup. Part (A) shows the SID and the general setup. Part (B) shows a close up view of the collimator opening and the source opening.
A.M. Alyassin et al. / Applied Radiation and Isotopes 72 (2013) 16–2920
shown in Eq. (3).
A2 ¼ A1d2
d1
� �2
ð3Þ
where A1 is the known activity, A2 is the expected activity, and d1
and d2 are the diameters of the SCO1 and SCO2, respectively.
Knowing the estimated activity for each SCO, the expectedradiation exposure as demonstrated earlier.
3.2. Field and source uniformities
Source uniformity was tested by measuring the exposurerate of the gamma-ray field at three different source-to-image

Table 1Estimate of expected exposure times for different source sizes of Am-241 to obtain
a 500 mR radiation exposurea.
Source circular
opening SCO [mm]
Activity [Ci] Exposure rate at
SID¼80 cm [mR/h]
Exposure time to
obtain 500 mR [min]
29 0.956b 15.95 1.9
10 0.114 1.90 15.8
8 0.073 1.21 24.7
6 0.041 0.68 43.9
4 0.018 0.30 98.8
2 0.005 0.08 395.4
a The source was assumed to be a point source and emits only 35.9% 59.5 keV
photons.b This is the actual activity. All other activities are estimated using Eq. (3).
A.M. Alyassin et al. / Applied Radiation and Isotopes 72 (2013) 16–29 21
distances SID (40, 80, and 120 cm). This experiment was repeatedwith five different source circular openings (SCO) (2 mm, 4 mm,6 mm, 8 mm, 10 mm). In addition, for each experiment the SCOwas either aligned with the center or with one of the four sides(above, below, right, and left) of the Am-241 source center.The exposure of the gamma ray field was measured with aportable dose rate meter type PDR1 positioned at the center ofthe image receptor location. The survey meter was calibrated tomeasure air-kerma-rate for Am-241.
The radiation field uniformity was tested by acquiring severalimages of the field of view without an object at three differentSIDs of 40, 80, and 120 cm. The images were acquired with a side-aligned SCO. Exposure times for the 40, 80, and 120 cm SIDs were60, 240, and 540 s, respectively. The difference in the exposuretime was to counter effect the inverse square law while obtainingroughly the same exposure. The low resolution CR image receptorwas used in this experiment. CR images were then analyzed usinga circular region of interest (ROI) with 120 pixel diameter. The ROIwas positioned in center of the image, and in the 3-clock, 6-clock,9-clock, and 12-clock positions and then the ROI’s mean grayvalues were estimated.
Table 2Shows the measured air-kerma rate [mGy/h] at SID¼40 cm.
SCO (mm) Air-kerma rate [mGy/h] Mean
sides/centerCenter Right Up Left Down Mean sides
2 3.0 4.0 4.0 5.0 5.0 4.5 1.5
4 10.0 10.0 15.0 17.5 17.0 14.9 1.5
6 35.0 30.0 35.0 35.0 40.0 35.0 1.0
8 55.0 40.0 60.0 72.5 58.0 57.6 1.0
3.3. Image quality parameters
Several tests were conducted to test the image quality para-meters such as spatial resolution, image contrast, and image noise(Fauber, 2008). In addition, a special phantom was developed tostudy the contrast detail curve for gamma-ray images that wereproduced by the radioactive Am-241 source.
10 75.0 75.0 84.0 105.0 95.0 89.8 1.2
Mean¼1.25
St dev ¼0.24
%COV ¼19%
Table 3Shows the measured air-kerma rate [mGy/h] at SID¼80 cm.
SCO (mm) Air-kerma rate [mGy/hr] Mean
sides/centerCenter Right Up Left Down Mean sides
2 0.6 1.2 1.3 1.0 1.5 1.3 2.1
4 2.5 3.0 4.0 4.0 4.0 3.8 1.5
6 5.0 8.5 9.5 8.5 9.5 9.0 1.8
8 13.0 10.0 17.5 17.5 17.5 15.6 1.2
10 22.5 20.0 21.0 25.0 24.0 22.5 1.0
Mean ¼1.52
St dev ¼0.44
3.3.1. Resolution
In the first part of this experiment, a line-pair phantom wasimaged with different SCO up to the full source size at SID¼40 cmwith an exposure time of 180 s. This was done with minimummagnification by attaching the line-pair phantom directly to theCR image receptor. In the second part, using the same experimentsetup but with the full SCO only, the phantom was imaged usingthe three different cassette sizes (high resolution CR, mediumresolution CR, and low resolution CR). In the third part, the sameexperiment was repeated with the high resolution CR but with anobject to image distance (air gap) of 0.6 cm which causedmagnification. In the last part, the latter experiment was repeatedbut with a smaller SCO of 6 mm. Additionally, its exposure timewas modified (increased approximately by the squared ratio ofthe source diameters) to compensate for the reduction in theradiation exposure.
%COV ¼29%
Table 4Shows the measured air-kerma rate [mGy/hr] at SID¼120 cm.
SCO (mm) Air-kerma rate [mGy/hr] Mean
sides/center
Center Right Up Left Down Mean sides
2 0.4 0.8 0.7 0.6 0.7 0.7 1.8
4 1.3 1.3 2.5 2.0 1.8 1.9 1.5
6 3.0 4.0 4.0 3.5 4.5 4.0 1.3
8 5.0 5.5 8.5 7.5 8.0 7.4 1.5
10 8.5 10.0 10.0 10.0 10.0 10.0 1.2
Mean ¼1.44
St dev. ¼0.21
%COV ¼15%
3.3.2. Contrast-to-noise ratio
A simple phantom of a water bottle was used to test thecontrast to noise ratio in gamma-ray images. Several images wereacquired at an 80 SID, with 10 mm SCO and different exposuretimes (30, 60, 120, and 180 s). A profile plot was drawn on theimages to show the contrast difference for different exposures.In addition, two square ROIs (each 40�40 pixels) were drawn oneach image. One ROI was drawn on the region that representswater and the other on the region that represents air. The meanand the standard deviation of the ROIs were calculated.The contrast was calculated as the difference in the mean grayvalue for water and the mean gray value for air. The noise wasestimated as the square root of the sum of the standard deviationssquared for air and water. The contrast to noise ratio was thencalculated from the images taken at different exposure times.
3.3.3. Contrast detail curves
The triangle prism phantom previously described and shownin Fig. 4 was developed to assess the contrast detail (CD) curve.

Table 5Shows image uniformity in terms of percent difference (PD) between the center
mean and the sides mean.
SCO SID
[cm]
Mean gray pixel value of ROI Mean
sides
PD
Center 12-
Clock
3-
Clock
6-
Clock
9-
Clock
Center
aligned
40 2808 2917 2900 2899 2960 2919 3.9
80 2991 3085 3040 3065 3130 3080 2.9
120 3280 3362 3314 3318 3375 3342 1.9
Side aligned 40 2814 2816 2935 2871 2860 2871 2.0
80 2960 2964 3044 3055 3023 3022 2.1
Table 6Contrast to noise ratio calculated from the water bottle images acquired at
different exposures times.
Exposure times [s] Water bottle Air Contrasta Noiseb CNR
Mean Stdev Mean Stdev
30 3736 11 3001 54 735 55 13
60 3668 20 2489 81 1179 83 14
120 3615 22 2047 88 1568 91 17
180 3423 28 1624 96 1799 100 18
a The contrast is calculated as the difference in the means of air and water gray
values.b The noise is calculated as the square root of the sum of the squared standard
deviations for air and water.
Fig. 7. Displays the air-kerma rates for different source circular openings at different SIDs when the source is center aligned and side aligned.
Fig. 8. Images of the gamma-ray field with a 4 mm source circular opening. Part (A) shows the image of the gamma ray field when the SCO aligned with the center of the
source. Part (B) shows the gamma-ray field when the SCO is aligned to the side (down) of the source. The small circles in (B) are the ROIs used to estimate the image
uniformity.
A.M. Alyassin et al. / Applied Radiation and Isotopes 72 (2013) 16–2922
At an SID of 40 cm with the full size source, several scans wereacquired of the CD phantom by placing it directly on the lowresolution CR image receptor. The scan times were equal to 10, 20,30, and 40 s. Then, a 1.5 cm thick Plexiglas plate was placed underthe CD phantom and another scan was acquired with a 40 sexposure time. The latter part was repeated two more times. Onescan was acquired with an SCO of 10 mm and a scan time of 260 sand the second scan was acquired with an SCO of 6 mm and ascan time of 690 s. The acquired images were analyzed visuallyand CD curves were manually drawn separating detectable andundetectable holes in the phantom. The region above and to the
right of a CD curve indicates the detectable holes, and the regionbelow and to the left indicates the undetectable holes (Bushberget al., 2002). During the CD curve analysis, all the images weredisplayed at the same window and level setting.
3.3.4. Imaging humanoid phantoms
Several human organ phantoms were imaged with gamma-rayand X-ray radiography. The Toshiba X-ray (T-RAD Plus) machine

A.M. Alyassin et al. / Applied Radiation and Isotopes 72 (2013) 16–29 23
was used in this research. Visual assessments of the acquiredimages were then conducted between the two acquisitions of thefollowing humanoid phantoms:
First, the head of the Rando phantom that is shown in Fig. 5Awas imaged with gamma-ray radiography at 60 cm SID, 2083 s(approx 35 min) exposure time, 6 mm SCO, and 5.6 cm CCO usingthe CR image receptor. The Rando head phantom was also imagedwith X-ray at 60 cm SID, 60 kVp, 20 mA, and 400 ms using asimilar CR image receptor. The radiation exposure was alsomeasured using a RadCal dosimeter at the center of the field ofview. Visual assessments of the two images were performed.
Second, the chest phantom that is shown in Fig. 5B wasimaged twice with gamma-ray radiography and once with X-rayradiography. The SID was set to 80 cm for all three acquisitions.The first gamma-ray radiography was imaged with an exposure
Gray Values
30 sec exposure
120 sec exposure
Position Profile
Fig. 9. Image pixel gray values versus the position along a horizontal profile for differ
Con
tras
t
Details
Fig. 10. Images of the CD Phantom acquired without magnification using the full sourc
smaller holes) and the vertical axis points down toward lower contrast holes. Fig. 10A–
the CD curve improves with the increase in exposure time.
time of 180 s with the full source size. The second gamma-rayradiography acquisition was set to 1920 s exposure time(approximately, 32 min), 4 mm SCO, and 4 cm CCO. The thirdacquisition of the chest phantom was acquired with ToshibaX-ray machine using 60 kVp, 20 mA, and 400 ms exposure time.CR image receptors were used for all acquisitions. The radiationexposure was also measured using a RadCal dosimeter at thecenter of the field of view. Visual assessments of the three imageswere performed.
Third, the abdomen phantom that is shown in Fig. 5C wasimaged with gamma-ray radiography at 80 cm SID, 1500 s(25 min) exposure time, 10 mm SCO, and 5.6 cm CCO using theCR image receptor. The Abdomen phantom was also imaged withX-ray at 60 cm SID, 60 kVp, 20 mA, and 400 ms using a similar CRphantom. Visual assessments of the two images were performed.
60 sec exposure
180 sec exposure
ent exposure times. The longer the exposure the time is, the higher the contrast.
e and an SID¼40 cm. In (A), the horizontal axis points to the left (higher details or
D show images with scan time equal to 10, 20, 30, and 40 s, respectively. Note that

A.M. Alyassin et al. / Applied Radiation and Isotopes 72 (2013) 16–2924
Fourth, the elbow phantom that is shown in Fig. 5D wasimaged with gamma-ray radiography at 60 cm SID, 1172 s(approximately 20 min) exposure time, 4 mm SCO, and 5.6 cmCCO using a CR image receptor. The Elbow phantom was alsoimaged with X-ray at 60 cm SID, 60 kVp, 20 mA, and 400 msusing a similar CR phantom. Visual assessments of the two imageswere performed.
Fifth, the SIB mammography phantom (PTW-Freiburg TYP42001) that is shown in Fig. 5E was imaged with gamma-rayradiography at 60 cm SID, 3120 s (approximately 52 min) expo-sure time, 4 mm SCO, and 4 cm CCO using a CR image receptor.The mammography phantom was also imaged with X-ray at60 cm SID, 60 kVp, 20 mA, and 400 ms using a similar CRphantom. Visual assessments of the two images were performed.
Con
tras
t
Details
Fig. 11. Shows images of the CD phantom all scanned at SID¼40 cm without and w
acquired with a scan time of 40 s. Using the same scan setting, (B) shows a lower quality
the use of smaller SCOs at 10 and 6 mm, respectively.
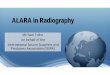
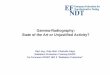
Fig. 12. Gamma-ray and X-ray radiography images of the Rando head phantom. Part (
image acquired with 60 cm SID, 60 KeV, 20 mA, and 400 ms.
3.4. Estimates of a pure Am-241 source
The radioactivity for a cylindrical shape pure Am-241 sourcewas calculated using Eq. (4).
Ap ¼ SA� r� V ð4Þ
where Ap is the pure activity, SA is the specific activity and r is thedensity and V is the volume. Since, the specific activity of Am-241is 3.5 Ci/gm and its density is 12 g/cc, manufacturing a pureAm-241 in a cylindrical shape with 10 mm diameter and 5 mmheight (volume¼393 mm3) would provide a radioactivity of approxi-mately 16.5 Ci (Strain and Leddicottee, 1962). The exposure rates andthe exposure times were estimated using Eqs. (1)–(3) as previouslydescribed for the estimates of pure Am-241 activities.
ith magnification. Part (A) shows the CD phantom image without magnification
C–D curve due to magnification. Parts (C) and (D) show improved C–D curves due
A) shows the gamma-ray radiography image, and (B) shows an X-ray radiography

Fig. 13. Gamma-ray and X-ray radiography images. Part (A) shows the gamma-ray radiography image with open source and 3 min exposure time. Part (B) shows the
gamma-ray radiography image with 32 min exposure time and 6 mm SCO. Part (C) shows an X-ray image with 60 KeV and 20 mA, and 400 ms exposure time.
Fig. 14. Gamma-ray and X-ray radiography images of the abdomen (torso) phantom.Part (A) shows the gamma radiography image.Part (B) shows an X-ray radiography
image scanned at 80 cm SID, 60 KeV, 20 mA, 0.4 s exposure time.
A.M. Alyassin et al. / Applied Radiation and Isotopes 72 (2013) 16–29 25

A.M. Alyassin et al. / Applied Radiation and Isotopes 72 (2013) 16–2926
4. Results and discussion
4.1. Exposure time estimates
Table 1 shows the estimates of the expected exposure time fordifferent SCOs at 80 cm SID. The estimate was based on a 500 mRradiation exposure and assuming the source was a point source.These results indicate that using our Am-241 source, that has anactivity of approximately 1 Ci, would require very long exposuretime to acquire an adequate gamma-ray image especially with asmall SCO.
4.2. Field and source uniformity
Tables 2–4 and Fig. 7 demonstrated that the radiation fieldsemitted by the radioactive source were not completely uniform.The radioactive source emitted on the average, higher radiationintensity from the sides than the center by more than 25% with alowest coefficient of variation of 15%. The reason for this varia-bility was probably due to the manufacturing technique of theradioactive source. As expected and shown in Fig. 7, as the SCOwas enlarged, the measured air-kerma rate and thus the radiationintensity became higher.
Table 5 and Fig. 8 demonstrated that the radiation fielduniformity was less than 4% percent difference for all SIDs setupswhen either the SCO was aligned with the center-source or withthe side-source. The uniformity was slightly better when the SCOwas side-aligned. In addition, these results indicated that thesource was not completely uniform because the sides of theimage received less radiation (higher pixel values) than the center(lower pixel values) and that was probably due to mainly thedistance inverse square law (Khan, 2010).
4.3. Image quality parameters
4.3.1. Resolution
The images of the line-pair phantom indicated that resolutionfor the first part was roughly 1.6 lp/mm regardless of the size ofthe SCO. This is expected because there was no magnification andthe resolution of the setup depended mainly on the resolution ofthe CR image receptor, as was verified in the second part(Hasegawa, 1987). In the second part of the experiment, the lowresolution CR provided a 1.6 lp/mm, the medium resolution CRprovided 1.75 lp/mm, and the high resolution CR provided a2.1 lp/mm. However, in the third part of the experiment, theresolution was reduced to 1.6 lp/mm for the high resolution CR.This was due to the image magnification of the phantom. In lastpart, the resolution was improved to 2.75 lp/mm when the sameexperiment was repeated with a smaller SCO of 6 mm (seeFig. 3B). This is because the spatial resolution also depends onthe size of the source. The smaller the source size the higher thespatial resolution. This factor has more effect when there is moreimage magnification. Magnification can improve to a certaindegree the image spatial resolution to take advantage of theinherent resolution of the image receptor when the source size issmall (Hasegawa, 1987).
Fig. 15. The Elbow phantom images. Part (A) shows the gamma-ray radiography
image, and (B) shows the X-ray radiography image at 60 kVp, 20 mA, 400 ms, and SID
of 60 cm.
4.3.2. Contrast-to-noise ratio
Table 6 shows clearly that as the exposure times increased,allowing for more radiation exposure, the mean pixel gray valuefor air and water decreased and became darker. The difference inthe mean gray value for water and the mean gray value for air, thedisplay contrast, increased and was clearly demonstrated in Fig. 9.Table 6 shows that the noise also increased, however, there was a
slight increase in the contrast to noise ratio with the increase inexposure time.
4.3.3. Contrast detail curve
The CD analysis is a qualitative procedure that estimates thecontrast and resolution at a certain noise level of an imagingsystem. Fig. 10 shows the CD images with different exposuretimes which lead to different noise levels. At a scan time of 40 sthe smallest hole was observed at the lowest contrast. InFig. 11B, a lower quality CD curve was observed because someof the holes disappeared which was due to the blurring causedby magnification. In Fig. 11C and D, better CD curves wereobserved and the smallest holes with lowest contrast reap-peared in the image because the source collimator openingswere reduced to minimize blurring.
4.3.4. Imaging humanoid phantoms
Fig. 12 shows the acquired images of the head phantom usinggamma-ray and X-ray radiography. The X-ray image showedmore details and superior quality than the gamma-ray image.However, the gamma-ray radiography image contained most ofthe head details such as the skull, some facial muscles, and eyeorbits.
Fig. 13 shows the acquired images of the chest phantom usinggamma-ray and X-ray radiography. The X-ray image showedsuperior quality than the gamma-ray image. However, thegamma-ray radiography image contained most of the chest

A.M. Alyassin et al. / Applied Radiation and Isotopes 72 (2013) 16–29 27
details such as the ribs, heart, and scapula. Fig. 13B showed moresuperior quality image than Fig. 13A due to the higher exposureand smaller SCO size.
Fig. 14 shows the acquired images of the abdomen phantomusing gamma-ray and X-ray radiography. The X-ray imageshowed more details and superior quality than the gamma-rayimage as shown in Fig. 14B. However, the gamma-ray radio-graphy image contained some of the abdomen phantom detailssuch as Ilium, Sacrum, some lumbar vertebras as shown inFig. 14A. The abdomen phantom was thick which lead to theincrease in the scatter that blurred the image further.
Fig. 15 shows the acquired images of the Elbow phantom usinggamma-ray and X-ray radiography. The X-ray image showedsomewhat more fine details than the gamma-ray image as shownin Fig. 15B. However, the gamma-ray radiography image con-tained most of the Elbow details such as the humerus, radius, andulna as shown in Fig. 15A.
Fig. 16. Images of the SIB mammography phantom. Part (A) shows the gamma-ray rad
400 s exposure time, and 60 cm SID.
Fig. 16 shows the acquired images of the SIB mammographyphantom using gamma-ray and X-ray radiography. Although bothmodalities used higher energy than is typically used in mammo-graphy, the X-ray image showed more details than the gamma-rayimage. However, the gamma-ray radiography image contained someof the SIB mammography details as shown in Fig. 16A.
The X-ray images showed higher resolution details due to thesmaller focal spot in the X-ray tube than the used SCO in gamma-ray radiography. The X-ray exposures used in these images wereestimated by the RadCal dosimeter to be 690 mR at SID of 60 cmfor the head phantom, 399 mR at SID of 80 cm for the chestphantom, 399 mR at SID of 80 cm for the abdomen phantom,690 mR at SID of 60 cm for the mammography phantom.
The reason for gamma-ray poorer quality image was due to thelow exposure provided by the Am-241 radioactive source. Usingan anti-scatter grid should help improve the contrast in thegamma-ray image. Therefore, higher activity Am-241 source and
iography image and (B) shows an X-ray radiography image using 40 kVp, 20 mA,

Table 7Estimate of expected exposure times for different source sizes of pure Am-241 to
obtain a 500 mR radiation exposurea.
Source circular
opening—SCO
[mm]
Volumes of
cylindrical
source [mm3]b
Maximum
activity
[Ci]
Exposure rate
at SID¼80 cm
[mR/h]
Exposure
time to
obtain
500 mR [s]
30 3534.3 148.4 2477.2 0.7
20 1570.8 66.0 1101.0 1.6
10 392.7 16.5 275.2 6.5
8 251.3 10.6 176.2 10.2
6 141.4 5.9 99.1 18.2
4 62.8 2.6 44.0 40.9
2 15.7 0.7 11.0 163.5
1 3.9 0.2 2.8 654.0
a The source was assumed to be a pure point source and emits only 35.9%
59.5 keV photon.b The height of the cylindrical source is 5 mm.
A.M. Alyassin et al. / Applied Radiation and Isotopes 72 (2013) 16–2928
the use of an anti-scatter grid should provide a better qualitygamma-ray image with shorter scan time.
4.4. Pure Am-241 source
Table 7 shows a listing of the expected exposures and exposuretimes for a cylindrical shape previously described pure Am-241source. Note that exposure time can be reduced approximately from16 min to 7 s with a 10 mm SCO for the pure 241-Am source. Thescan time was longer for smaller SCO. The scan time for a SCO of1 mm is in the order of 11 min. Thus very high resolution medicalimages will be difficult to obtain in an acceptable clinical settingeven if a pure Am-241 was used. However, a reasonable scan time of18 s may be accomplished with 6 mm SCO.
In summary, on one hand gamma-ray radiography has severaladvantages over X-ray radiography. First, the use of a proper radio-active source that emits a monoenergetic photon beam will lead to alower radiation dose to the patient. Since the number of the X-rayprocedures has been on the rise and special X-ray CT proceduresrequires higher patient dose, then the exploration of using radioactivesources should be encouraged. Second, the use of a long half-lifesource lowers the maintenance and downtime of the machine. Third,it is expected to be less expensive since it does not require a highvoltage generator or an X-ray tube. Fourth, a gamma-ray radiographicsource can be fashioned in a small compartment, hand held, andmade portable. This may be useful in a war zone environment orremote areas. Fifth, it is possible to also use several radioactivesources that simultaneously emit different unique energies. Theseenergies are useful to suppress unwanted information and to stressuseful diagnostic information in the image (Bushberg et al., 2002). Onthe other hand, there are also challenges in gamma-ray radiography.The first challenge is to prepare a highly radioactive source that emitsdiagnostic photon energies. Although one may prepare mixed radio-active sources, there will also be a limited option of photon energiesin comparison to X-ray radiography. Additionally, the source has to besmall in size and highly radioactive to be able to generate highresolution images. Finally, shielding, contaminations, and handling ofradioactive sources will be of more concern, since, unlike X-raysource, radiation is continuously being emitted.
5. Conclusions
This research studied several factors that influence the feasi-bility of using gamma-ray radiography in medical imaging. Thesource uniformity test deduced that the radioactive sourceemitted higher radiation intensity from the sides than the actual
center. All the subsequent experiments focused on the side of theactual radioactive source to obtain smaller source sizes withhigher exposures. The exposure in the field of view was relativelyuniform and provided uniform images. The image quality para-meter tests indicated that the noise was dependent on theexposure time and the source size. Similarly, since we did notuse any anti-scatter grid in our experiments, contrast was alsodependent on both the exposure time and the source size. Spatialresolution depended on the source size and the magnificationfactor. The contrast detail analysis also reemphasized thesefindings.
The images of the human phantoms from both gamma-ray andX-ray radiography were visually assessed. Although, the X-rayimages showed superior quality because of higher number ofphotons and smaller focal spot size, the gamma-ray images wereable to show the main features of the humanoid phantoms. Thehead phantom image showed detailed information of the skull aswell as some facial muscles. The chest phantom image showed allthe basic information shown on the X-ray chest image. The elbowphantom image showed more detailed diagnostic information.The torso and the mammography phantom images showed lowerquality images. The torso was of lower quality because of highscatter to primary radiation caused mainly by the thickness of theobject. The mammography phantom image was also of lowerquality. This was due to several reasons, namely, the high energyemitted by Am-241 compared with the energy typically used inmammography, the source size compared with the very smallfocal spot size used in mammography, and the high scatterradiation that caused blurring to several small objects in thephantom.
The used low activity made the exposure time much longerthan X-ray radiography. However, the scan time in gamma-rayradiography can be much shorter if a pure Am-241source of highenough activity is used. Higher exposure rates and thus lowerexposure times were estimated for different pure Am-241 sourcesizes. For instance, a 10 mm source size of 16.5 Ci pure Am-241with 7 s exposure time should produce images similar to X-rayimages in the level of contrast and noise. However its low specificactivity may hinder the creation of a very small source size that isable to produce high resolution images similar to X-ray. Inconclusion, this research studied and demonstrated the feasibilityof gamma-ray medical radiography as a potential alternative toX-ray radiography.
References
AbdulMajid, S., Kollathodi, M., & Maimani, A., 2010. Am-241 radioactive source fordiagnostic medical imaging. Tenth Radiation Physics & Protection Conference,27–30.
Alyassin, A.M., 2009. Obstacle exclusion from X-ray CT angiography data for 3Dimage diagnosis. Jordan J. Phys. 2 (1), 59–72.
Bailey, D.L., Townsend, P.E., Valk, P.E., Maisey, M.N., 2005. Positron emissiontomography. In: N. Secaucus (Ed.), Basic Sciences, pp. 798–802.
Bushberg, J.T., Siebert, A.J., Leidholdt Jr., E.M., Boone, J.M., 2002. Essential Physics ofMedical Imaging, second ed. Lippincott Williams & williams.
Fauber, T.L., 2008. Radiographic Imaging & Exposure, first ed. Mosby.Fournier, L., Chatellier, L., Peureux, P., Djafari, M., Idier, J., 2007. 3D reconstruction
from narrow angles radiographs. AIP Conf. Proc., 680–687.Hasegawa, B., 1987. Physics of Medical X-Ray Imaging, second ed. Medical Physics
Pub Corp.Hendee, W.R., Ritenour, E.R., 2002. Medical Imaging Physics. Wiley-Liss, New York.Huda, W., Slone, R.M., 2003. Review of Radiologic Physics, second ed. Lippincott
Williams & Williams, Philadelphia.IAEA, 1999. Radiation protection and safety in industrial radiography. Safety
reports series No. 13. IAEA. IAEA , Austria.Kaplan, M.S., Hynor, D., 1999. Differential attenuation method for simultaneous
estimation of activity computed tomography. Med. Phys. 26 (11).Kapur, A., Thomenius, J.W., Eberhard, P.L., Goodsitt, C.M., Krucker, M.A.,
Roubidoux, H.M., et al., 2002. Co-registered digital mammography and 3Dbreast ultrasound imaging: design and initial evaluation of a new investigationdevice. RSNA.

A.M. Alyassin et al. / Applied Radiation and Isotopes 72 (2013) 16–29 29
Khan, F.M., 2010. The Physics of Radiation Therapy, fourth ed. Wolters Kluwer andLippincott William & Wilkins.
Krug, B., Crott, R., Roch, I., Lonneux, M., Beguin, C., Baurain, J.F., et al., 2010.Cost-effectiveness analysis of FDG PET-CT in the management of pulmonarymetastases from malignant melanoma. Acta Oncol. 49 (2), 192–200.
Liu, T., Cheng, T., Xu, W., Yan, W.L., Liu, J., Yang, H.L., 2011. A meta-analysis of18FDG-PET, MRI and bone scintigraphy for diagnosis of bone metastases inpatients with breast cancer. Skeletal Radiol. 40 (5), 23–31.
Meng, L.J., Rogers, W.L., Clinthorne, N.H., Fessler, J.A., 2003. Feasibility study ofcompton scattering enchanced multiple pinhole imager for nuclear medicine.IEEE Trans. Nucl. Sci. 50 (5), 1609–1617.
Muench, P.J., Ravinder, N., 1992. Dose distribution produced by shielded applica-tors using 241Am for intracavitary irradiation of tumors in the vagina. Med.Phys. 19 (5).
Pichler, B.J., Judenhofer, M.S., Pfannenberg, C., 2008. Multimodal imagingapproaches: PET/CT and PET/MRI. Handb. Exp. Pharmacol. 1, 32–109.
Raan, D.H., Toit, D.P., Lotter, M.G., Herbst, C.P., Walt, V.T., Otto, A.C., 2000.Implementation of Tc-99 m and Ce-139 scanning line source for attenuation
correction in SPECT using a dual opposing detector scintillation camera. Med.Phys. 27 (7).
Randinder, N., Park, C.H., Christopher, K.R., Muench, P., 1990. A dose computationmodel for 241Am vaginal applicators including the source-to-source shieldingeffects. Med. Phys. (5), 17.
Ravinder, N., Gray, L., Park, C.H., 1987. Dose distribution around cylindrical 241Amsource for a clinical intracavitary applicator. Med. Phys. 14 (5).
Strain, J.E., Leddicottee, G.W., 1962. The Preparation, Properties, and Uses ofAmericium-241, Alpha, Gamma, and Neutron Sources. Oak Ridge NationalLaboratory.
Tipnis, S.V., Nagarkar, V.V., Shestakova, I., Gaysinskiy, V., Entine, G., Tornai, M.P.,Stack Jr., B.C., 2004. Feasibility of a beta–gamma digital imaging probe forradioguided surgery. IEEE Trans. Nucl. Sci. 51 (1), 43–47.
Verbinski, V.V., Orphan, V.J., 1997. Gamma radiography cargo vehicle scanner.Proc. SPIE 112.
Woodring, M., Souza, D., Tipnis, S., Waer, P., Squillante, M., Entine, G., Ziock, K.P.,1999. Advanced radiation imaging of low-intensity gamma-ray sources. Nucl.Instrum. Methods Phys. Res. A 422, 709–712.