Embed Size (px)
Citation preview
Fairness and Legitimacy of decisions during delivery of malaria services and ITN interventions in ZambiaAuthors: Mary Tuba¹ ², Ingvild Sandoy2, Paul Bloch3, Bruno Marchal4, Seter Siziya1, Øystein Olsen2 5, Jens Byskov6,
1 The Department of Community Medicine, School of Medicine, University of Zambia, PO Box 50110, Lusaka – Zambia, 2 Center for International Health, University of Bergen, PO Box 7804, N-5020 Bergen, Norway, 3Department of Public Health, Prince Leopold Institute of Tropical Medicine, Antwerpen, Belgium, 5Haydom Lutheran Hospital, Mbulu, Manyara, Tanzania, United Republic of, 3DBL - Centre for Health Research and Development, Faculty of Life Sciences, University of Copenhagen, Thorvaldsensvej 57, DK 1871 Frederiksberg, Denmark
Presentation Outline
– Background– Rationale for the study or paper– Objective of paper– Methodology– Results– Conclusion– Implications
Background 1
• An estimated 74% of the population in the Africa live in malaria endemic areas, 19% in epidemic-prone areas (WHO 2006)
• 75% out of annual malaria cases in sub-Sahara Africa, are in children <5 (WHO 2006)
• 80% of malaria in sub-Sahara Africa is managed at home (Breman et al 2004)
• In Zambia, malaria accounts for up to 40% of all infant mortality rates and up to 20% of all maternal mortality rate (MoH, 2008)
• Malaria accounts for 45% of hospitalizations and outpatients department visits (MoH, 2008)
Background 2
• REsponse to ACcountable priority setting and Trust in health system (REACT), aims to strengthen the fairness and legitimacy of priority setting at district level in Zambia, Tanzania and Kenya (Byskov et al 2009)
• Within REACT and between 2006 and 2008, fairness and legitimacy of decisions during delivery of malaria services and ITN interventions were evaluated
• Legitimacy refers to the moral authority of the people or institutions who exercise priority setting authority and how that authority is derived (Kapiriri and Martin 2007).
• Fairness refers to processes of making priority setting decisions (Kapiriri and Martin 2007) based on a balance of relevant locally acceptable wider stakeholder values in specific time and within a given context (own additional)
• Explicit use of the Accountability For Reasonableness (AFR) framework to isolate behaviours influencing fair and legitimacy of decisions during provision of malaria services and ITNs in public health institutions of Zambia
Objective of paper
• Describe and evaluate fairness and legitimacy of decisions during delivery of malaria services and ITN intervention in a rural district of Zambia
Methodology
• Study site – Kapiri-Mponshi District, rural Zambia
• A matrix was produced to identify eligible informants, who were occupying decision-making positions and were involved in priority setting processes
• 38 In-depth Interviews administered among decision makers at district, facility and community levels
• 9 Focus Group Discussions were conducted with District Health Management Team (DHMT) Officers, outpatient male and female attendees above 15 years, antenatal women and adolescents male and female 18-24 years
Methodology: Accountability For Reasonableness Framework
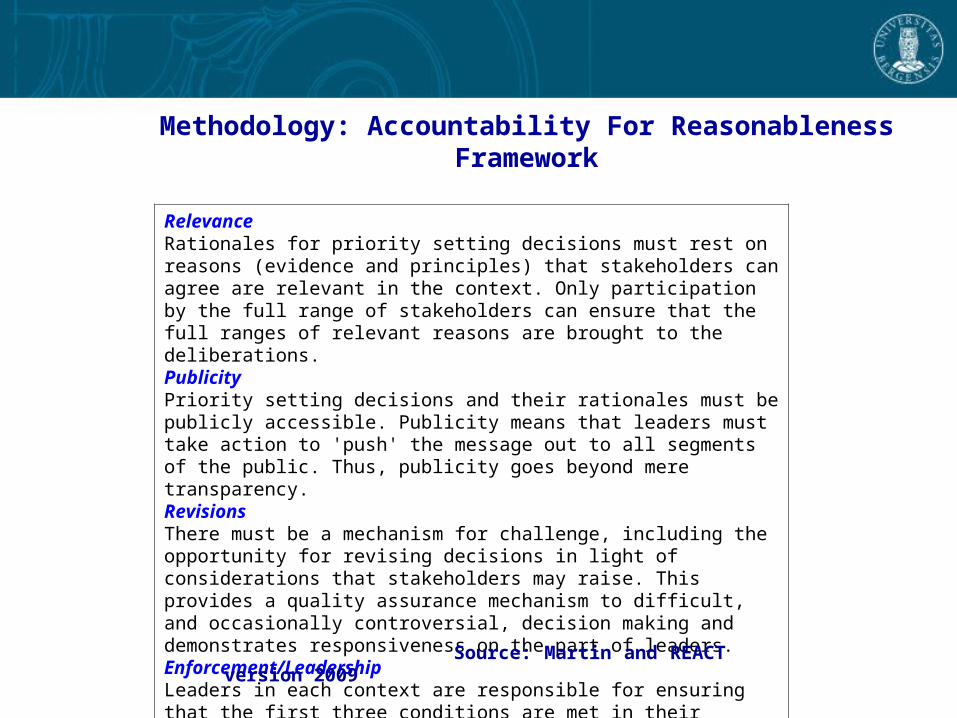
RelevanceRationales for priority setting decisions must rest on reasons (evidence and principles) that stakeholders can agree are relevant in the context. Only participation by the full range of stakeholders can ensure that the full ranges of relevant reasons are brought to the deliberations.PublicityPriority setting decisions and their rationales must be publicly accessible. Publicity means that leaders must take action to 'push' the message out to all segments of the public. Thus, publicity goes beyond mere transparency.RevisionsThere must be a mechanism for challenge, including the opportunity for revising decisions in light of considerations that stakeholders may raise. This provides a quality assurance mechanism to difficult, and occasionally controversial, decision making and demonstrates responsiveness on the part of leaders.Enforcement/LeadershipLeaders in each context are responsible for ensuring that the first three conditions are met in their context and adequately represent and facilitate public regulation .
Source: Martin and REACT version 2009
Methodology II
• Analysis was manually done using the code sheet approach • Same or similar phrases describing fairness and legitimacy of
decisions were coded using standardized codes• To check for reliability of phrases, frequencies and occurrences of
common phrases within single IDIs and FGDs and across the IDIs and FGDs, transcripts were repeatedly read through
• Different standardized codes were assigned to phrases that were describing emerging themes
• Further classification of common phrases was done using the Accountability For Reasonableness (AFR) conditions of relevance, publicity, appeals/revisions and leadership/enforcement.
Results for the period 2006 and 2008
• Disagreements existed concerning fairness and legitimate decision-makers to involve during delivery of malaria services and ITNs between decision-makers and communities (patients).
• Decision-makers believed there was fairness and legitimate decision-making practices during delivery of malaria services and ITNs.
• Strongest and priority recurring calls for improving fairness and legitimacy were found in the leadership/enforcement condition
Results: Decision-makers’ perspectives
• Decision-makers perceived fairness from cost, supply of malaria medicines, ITNs, type and number of people accessing and presence of health-providers.
• Legitimate decision-makers included the District medical officer (head of district), health-providers, financial officers, public regulatory bodies (civil service) to deploy and retain health-providers, donors for supply of ITNs and Medical stores of Zambia (national parastatal institution) for supply of medicines including malaria medicines and other biomedical consumbles.
Results: Decision-makers’ perspectives
“But of course we know that drugs (including malaria drugs) come from Medical Stores. Sometimes you may go there, you find the drugs are not there because they come on scheduled times. Sometimes they will say they will bring themselves” (FGD with Decision-makers district level, Male participant 3: 49 years old, 22 years of service).
• The Medical Stores and not the DHMT are responsible for supply of medicines in the facilities – fairness and legitimacy (relevance, leadership or enforcement)

Results: Decision-makers’ perspectives
“I am a medical personnel also, there are times when you find that I can’t just call somebody immediately and that person will be available as it used to be. So in human resource, we are not enough, it’s a very big challenge, under that concept” (FGDs with District level decision-makers, male participant 7: 54 and half years, 29 years service)
• Inadequate health personnel, but not communicated to patients – Legitimacy (relevance, publicity)
Results: Decision-makers’ perspectives
• “One staff at one of the rural health centres, the chief took him to the provincial Permanent Secretary (PS). He didn’t want him. A decision related to health, they are supposed to follow the channel, by seeing the District Director of Health (DDH), then let the civil service handle the issue, than the politicians or the chief” (FGD with Decision-makers district level, Male participant 3: 49 years old, 22 years of service).
• Chiefs and politicians regulating deployment of health-provider – legitimacy and fairness (relevance, leadership/enforcement)

Results: Decision-makers’ perspectives – Promotion of ITNs use
“We are not doing much concerning our primary prevention strategies, the use of ITN, sourcing of funds to purchase those ITNs, you know the spraying (In-door Residual Spraying in the district) and ensuring that we cut the grass around. (District level decision-maker, male Informant 36 years, 2 years service)
• Costs and supply of ITNs difficulties hindered implementation according to planned activities – fairness (Enforcement condition)
Results: Decision-makers’ perspectives – malaria services
“The community we are serving, many of them are appreciating the service. People have written letters appreciating what we have done, they are passing very good comments. We look at people who are accessing the service, we have seen that there are so many that come in for the service. For us we are saying, definitely we are doing fine with the communities that are working with us,
yes” (FGDs with District level decision-makers, male participant 7: 54 and half years, 29 years service)
• Fairness was defined by number and type of people accessing services, good comments recieved and information from letters (suggestion boxes) – fairness and legitimacy (relevance, revisions, leadership)
Results: Community (Patients’) perspectives
Community perceptions of fairness and legitimacy combined different criteria.
• Fairness criteria included time, cost of malaria medicines and ITNs, availability of responsive appeal mechanisms, practices, attitudes of providers, accessibility or adequacy of malaria medicines, ITNs, providers and the way they were received (reception).
• Legitimate decision-makers included health-providers, patients, suppliers of medicines (Medical Stores), indigenous healing system (healers), indigenous leadership (chiefs), political position holders
Quote relating to availability of ITNs: Patients’ perspectives
“The problem here is that the ones who receive the mosquito nets, those in offices, you find they get many and they go to sell somewhere else”. (PARTICIPANT4: FGD with Male
Adolescent 18-24 years)
• No mechanisms to challenge deviation of subsidized ITNs elsewhere - fairness and legitimacy (appeals and leadership)
Results: Quote relating to adequacy of health-provider. Patients’ perspectives
“There are no doctors in most of the rooms, so every time we come here, it’s congestion. They do not perform their jobs to satisfaction. Nakumukoshi kulafita (literally translated as “even my throat becomes dark”). No desire (referring to herself) to receive a particular service despite going to the hospital.” (PARTICIPANT1, G6 schooling: FGD with Out Patient Females 35 years and above)
• Adequacy and access to qualified health-providers for diagnosis. No appeal mechanisms to challenge attitudes, practices identified – legitimacy, fairness (relevance and appeals)
Priority and decision-making regarding delivery ITNs
“We have already said, the service for us in rural area, the information is not reaching the people. Like we hear that there are mosquito nets, sometimes we hear that in such an area they were selling at 10,000 or K3, 000, now this is another way to prevent for us who are out there and the hospital is far.” (PARTICIPANT6, G1 schooling: FGD with Out Patient Male 15-34 years, community level)
• Ineffective communication mechanisms regarding information on ITNs – fairness (publicity condition)
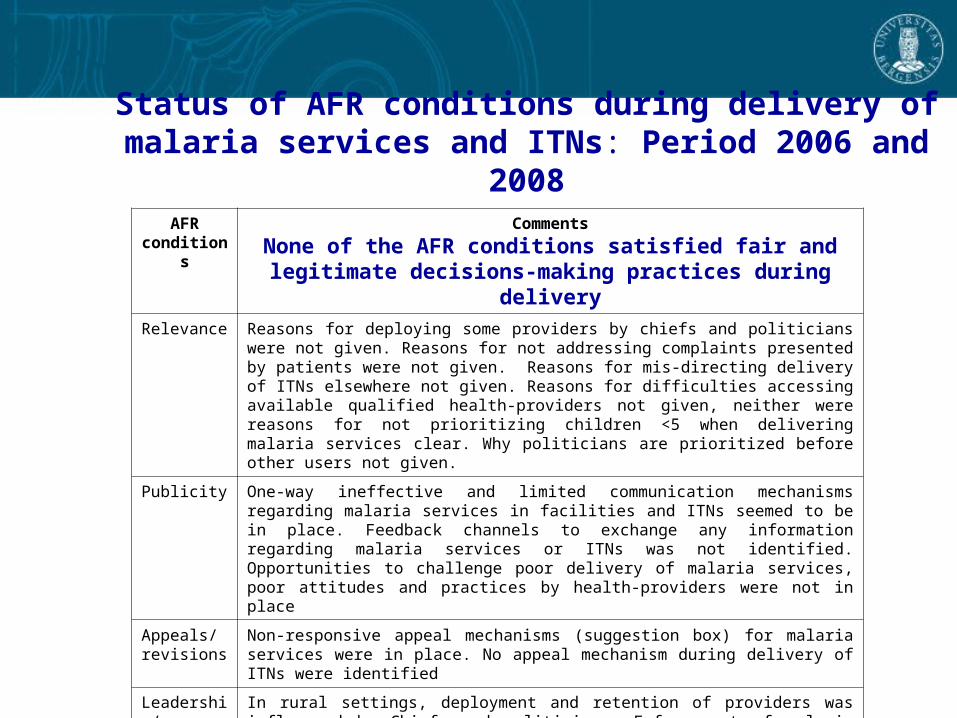
Status of AFR conditions during delivery of malaria services and ITNs: Period 2006 and 2008
AFR conditions
Comments
None of the AFR conditions satisfied fair and legitimate decisions-making practices during delivery
Relevance Reasons for deploying some providers by chiefs and politicians were not given. Reasons for not addressing complaints presented by patients were not given. Reasons for mis-directing delivery of ITNs elsewhere not given. Reasons for difficulties accessing available qualified health-providers not given, neither were reasons for not prioritizing children <5 when delivering malaria services clear. Why politicians are prioritized before other users not given.
Publicity One-way ineffective and limited communication mechanisms regarding malaria services in facilities and ITNs seemed to be in place. Feedback channels to exchange any information regarding malaria services or ITNs was not identified. Opportunities to challenge poor delivery of malaria services, poor attitudes and practices by health-providers were not in place
Appeals/ revisions
Non-responsive appeal mechanisms (suggestion box) for malaria services were in place. No appeal mechanism during delivery of ITNs were identified
Leadership/enforcement
In rural settings, deployment and retention of providers was influenced by Chiefs and politicians. Enforcement of malaria services delivery was a monopoly of health-providers, yet fair and legitimate characteristics such as responsiveness, open-mindedness, caring, leadership over supply of medicines, availability and accessibility to providers, monitoring performance of health-providers were weak. Due to cost of purchasing ITNs and supply challenges, enforcement of ITNs delivery according to DHMT activity plan was difficult. Enforcing the first three conditions was a challenge

Conclusion
• Fairness and legitimacy of decisions during delivery of malaria services and promotion of ITN utilization, was weak. The weak application of AFR conditions could have been precipitated by conflicting criteria used to construct fairness and legitimate decision-makers to involve during delivery between decision-makers and communities (patients).
Implications
• Need to resolve conflicts through application of approaches such as AFR, which among other aspects promotes legitimacy, fairness and leadership during priority setting processes.
QUOTE
• ”The time has come to say goodbye to the simple solutions” Holm, 1998
Acknowledgement
• REACT – REsponse to ACcountable priority setting for Trust in health systems project, recieved financial support from EU.
• We are indebted to the Ministry of Health, Zambia, for authorising this rare research to be implemented in the country.
• We are thankful to The District Health Management Team (DHMT) at Kapiri-Mponshi, for their willingness to implement this work.
• We would not be fair or accountable if we did not also acknowledge important contributions from informants and participants residing in the district, without whose willingness to be interviewed or have discussions, we could not have collected the data.