Embed Size (px)
Citation preview

Fair society, Healthy Lives
Michael Marmot
UCL Institute of Health Equity
Stockholm
July 2012

• Fairness at the heart of all policies.
• Health inequalities result from social inequalities – requires action on all the social determinants; the causes of the causes
• Focusing solely on the most disadvantaged will not reduce inequalities sufficiently – action is needed across the social distribution.

The health sector acting alone cannot tackle health inequalities
• Action is needed across the whole of government and the whole of society
• Health is an issue for all social workers, not just those working in health settings
• Recipients of social care services are likely to be the most socially disadvantaged and most will have a long-term illness or disability… over 50s age group are largest users of health and social care (Marmot Review p 159)

Social determinants of health across the lifecourse

A. Give every child the best start in life
B. Enable all children, young people and adults to maximise their capabilities and have control over their lives
C. Create fair employment and good work for all
D. Ensure healthy standard of living for all
E. Create and develop healthy and sustainable places and communities
F. Strengthen the role and impact of ill health prevention
Fair Society, Healthy Lives: 6 Policy Objectives

A. Give every child the best start in life
B. Enable all children, young people and adults to maximise their capabilities and have control over their lives
C. Create fair employment and good work for all
D. Ensure healthy standard of living for all
E. Create and develop healthy and sustainable places and communities
F. Strengthen the role and impact of ill health prevention
Fair Society, Healthy Lives: 6 Policy Objectives

Early child care and education
• Parenting and family support– Perinatal services– Care before and during pregnancy– Help for new mothers
• Pre-school education and care• Primary, secondary and tertiary education and
training

Links between socioeconomic status and factors affecting child development, 2003-4
Source: Department for Children, Schools and Families

Gaps in school readiness at 3 and 5 years by family income: UK
Ave
rage
per
cent
ile s
core
Waldfogel & Washbrook 2008

Country ranking: equality in child wellbeing - material, education, and health
Source: UNICEF Report Card 9, ranking 24 OECD countries by theirperformance in each of three dimensions of inequality in child well-being
Score Country8 Denmark, Finland, Netherlands, Switzerland 7 Iceland, Ireland, Norway, Sweden 6 Austria, France, Germany, Poland, Portugal 5 Belgium, Czech Republic, Hungary,
Luxembourg, Slovakia, Spain, United Kingdom
3 Greece, Italy

Children aged 36-59 months that do not attend any form of early education programme in selected CIS and CEE countries
0 20 40 60 80 100
Belarus
Ukraine
Albania
Georgia
Serbia
Kyrgyzstan
Montenegro
Uzbekistan
Kazakhstan
TFYR Macedonia*
Bosnia and Herzegovina
Tajikistan
Richest 20% Poorest 20%
Source: Unicef/MICS 2007

A. Give every child the best start in life
B. Enable all children, young people and adults to maximise their capabilities and have control over their lives
C. Create fair employment and good work for all
D. Ensure healthy standard of living for all
E. Create and develop healthy and sustainable places and communities
F. Strengthen the role and impact of ill health prevention
Fair Society, Healthy Lives: 6 Policy Objectives

Unemployment in EU 27 countries, 2002 - 2011

• Unemployment associated with poor mental and physical health

Mortality* of men aged 16-64 by social class and employment status at the 1981 census
1981 LS Cohort. *England & Wales: mortality 1981-92
* adjusted for age and salary
56
92102
82
118
86
118
97
139
112
176
74
50
70
90
110
130
150
170
190
Social class
Sta
nd
ardi
sed
Mo
rtal
ity R
ate
I II IIIN IIIM IV V I II IIIN IIIM IV V
Employed in 1981 Unemployed in 1981

Unemployment and Mortality1% rise in unemployment associated with:
- 0.8% ↑Suicide
- 0.8% ↑Homicide
- 1.4% ↓Traffic death
No effect on all-cause mortality
Source: Stuckler et al 2009 Lancet

Changes in adult unemployment and in age-standardised suicide rates (age 0–64 years) in old (pre-2004) and new European Union Member States
(Stuckler et al Lancet 2011)2007 is the index year, and y-axis values represent proportional change relative to that year
Unemployment
Suicides

Occupational stress in European countries
0
10
20
30
40
50
Very low Low High Very high
Effort rewardimbalance
Low control
Per cent
Occupational class

A. Give every child the best start in life
B. Enable all children, young people and adults to maximise their capabilities and have control over their lives
C. Create fair employment and good work for all
D. Ensure healthy standard of living for all
E. Create and develop healthy and sustainable places and communities
F. Strengthen the role and impact of ill health prevention
Fair Society, Healthy Lives: 6 Policy Objectives

• Social protection policies make a difference • Social and health benefits

Social Protections Help…
Each 100 USD per capita greater social spending reduced the effect on suicides by:0.38%, active labour market programmes
0.23%, family support
0.07%, healthcare
0.09%,unemployment benefits Spending> 190 USD no effect of
unemployment on suicide
Source: Stuckler et al 2009 Lancet

Copyright ©2010 BMJ Publishing Group Ltd.
Stuckler, D. et al. BMJ 2010;340:c3311
Relation between social welfare spending and all cause mortality in 18 EU countries, 2000

Responses to economic crisis and child poverty: UK

Projected relative AHC income poverty rates under current policies and without the coalition government’s tax and benefits reforms: UK
IFS 2010

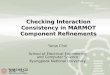
Social protection policies can mitigate intergenerational effects

0 10 20 30 40 50 60
Romania Latvia
Bulgaria Lithuania
Italy Greece
Spain Poland
Portugal Luxembourg
Hungary United Kingdom
Malta Estonia
Switzerland Ireland
Slovakia France
Belgium Netherlands
Germany Austria
Czech Republic Sweden Finland Cyprus
Slovenia Denmark
Norway Iceland
Poverty rate
Before social transfers After social transfers
Child poverty rates (% living in households <60% median income) before and after social transfers 2009
Source: EU SILC

• Health inequalities are not inevitable or immutable

SMRs by cause, all ages: Glasgow relative to Liverpool & Manchester
All ages, both sexes: cause-specific standardised mortality ratios 2003-07, Glasgow relative to Liverpool & Manchester, standardised by age, sex and deprivation decile
Calculated from various sources
112.2 111.9126.7
248.5
131.7
168.0
229.5
0
50
100
150
200
250
300
350
All cancers(malignantneoplasms)
Circulatory system Lung cancer External causes Suicide (inc.undetermined intent)
Alcohol Drugs-relatedpoisonings
Sta
ndar
dise
d m
orta
lity
ratio
Source: Walsh D, Bendel N., Jones R, Hanlon P. It’s not ‘just deprivation’: why do equally deprived UK cities experience different health outcomes? Public Health, 2010
from H Burns, CMO, Scotland

Health improvement in difficult times
• A major element of the excess risk of premature death seen in Scotland is psychosocially determined
• Study evidence of low sense of control, self efficacy and self esteem in population in these areas
Source: H. Burns, CMO Scotland

Health inequalities and policy strategies
• Health inequalities are not inevitable;• Not just a responsibility of the health care sector;• Whole of society, whole of government

• A Fair Society