Embed Size (px)
Citation preview

Hadeel Al-Jarhi
Murad
2
9/2/2015
Periodontics
Lecture No.
Date:
Doctor:
Done by:
Sheet
Slide
s
Hand Out
University of Jordan
Faculty of Dentistry
Fourth year –2nd semester 2014-2015

9/2/2015 perio sheet#2 Hadeel Al Jarhi
2
Examination and diagnosis of periodontal diseases :
Lecture outline:
- Patient interview
- Periodontal examination and charting
- Periodontal probing
- Mobility
- Recession
- diagnosis
When you examine a patient , especially for the first time ,always look at the big picture of the case, do not
focus on small details .
These gingival diseases were or will be covered in the lectures :
There's another table in the slides show each disease features .
Patient interview
Chief complain
- History of chief complaint :
in perio clinic it could be ( pain , mobility , bleeding , bad breath , recession , diastema formation ,
spacing between teeth , esthetics ;black triangles which form because of the papillary recession)

9/2/2015 perio sheet#2 Hadeel Al Jarhi
3
you then investigate the chief complain ( onset , location , duration , aggravating and relieving
factors & nature of the complaint )
*ask smart questions
*do not use scientific terms with the patient , use simple words instead .
Eg:
2 patients have bleeding of the gum as a chief complaint :
Case 1 : stated 2 weeks ago , not associated with swelling and the bleeding stops shortly after teeth
brushing .
Case 2 : started 2 weeks ago , associated with generalized swelling , and the bleeding lasts for
several hours
Which case is more ominous ? case 2
Case 1 is more like plaque induced gingivitis
Case 2 as the bleeding last for several hours , that’s indicate that it's something different than the
plaque induced gingivitis
In the gingival index , 3 = spontaneous bleeding which is not an accurate description , as almost
there's no real spontaneous bleeding ( it has to be stimulated even by a fine touch of the gingiva )
Eg . If a patient has mobility as a chief complain , you could ask him :
1- When did you first feel it
2- Did it start after a specific incident
3- has the nature of the complaint changed recently
chief complain could appear after a restorative treatment , so occlusal changes happen and lead to
changes in teeth
Medical history :
-Investigate systematically
-ask the patient if he/she is regularly attending a physician
- it's important to determine if the patient is prone to infective endocarditis ( patients with prosthetic heart
valve and congenital heart diseases are usually aware that they should stop the warfarin before visiting a
dentist )
- you can't probe for these patients without using an antibiotic prophylactically as probing induces
bacterial invasion and infection.
- it's important to ask about smoking ( what type of tobacco , amount per day and for how long he/she has
been smoking )

9/2/2015 perio sheet#2 Hadeel Al Jarhi
4
Smoking is a risk factor for periodontitis
-using the medical screening form is recommended ( as you could let the pt fill
it and investigate the positive answers only )
- you can consult a physician if you need to ( ask specific questions )
Eg : never ask the physician how to manage my patient , ask questions like
please update me with the cardiovascular status of the pt , or please advise if
we can use epinephrine in the LA
You should be cautious in using epinephrine with patients having diseases like
hypertension , ( the quantity per time )
If you gave him 2 carpools of LA , after 2 hours you should be aware of giving
him LA again as we have endogenous adrenaline secretion .
- Social an family history
Social Hx : smoking , alcohol use , recreational drugs use
Family Hx : for medical conditions and periodontal diseases
Eg. Do you have any relatives who have lost their teeth in an early age ?or have mobility in teeth ? or have
any gum disease
- Dental history
Previous perio treatment :
- It could impact the way you diagnose the condition
Eg. A pt who has been treated of chronic periodontitis (recession and exposure of the roots and you had
done scaling and root planning for him ) , when he has been examined for the next time he may have
bleeding upon probing and that doesn’t mean that he has active periodontitis , he may have gingivitis on a
reduced periodontium.
In any periodontitis case , the bone loss is an irreversible process , so when you treat it , you relieve the
symptoms , after the treatment , having bleeding on probing doesn’t mean that he/she still have active
periodontitis or bone loss , its gingivitis on the reduced periodontium
So you have to ask about the previous treatment to have good diagnosis , ant it could be helpful if you can
get the previous perio charting

9/2/2015 perio sheet#2 Hadeel Al Jarhi
5
Eg. A pt who has been treated from periodontitis previously but still have active signs of the disease (
suppuration , severe pocketing , sub gingival calculus ) that indicate it's such a tough case that didn’t
respond to treatment as it was predicted ,
- Oral hygiene attitude ( what he/she use ,how many times and so )
- Orthdontic tx history ( could cause root resorption r blunting , recession )
Examination :
- extra oral examination ; muscles of mastication , TMJ , skin , lips , symmetry , lymph nodes
- intra oral examination ; caries , prominent wear facets , uneven marginal ridges , failing restorations ,
evidence of food impaction , tenderness to percussion , fremitus
Fremitus : tooth mobility upon function ; when the pt bite , the first tooth to come in contact with the
opposing , move a little to allow for maximum intercuspation .
Its seen most commonly in the maxillary anterior teeth but could be anywhere , it could happen upon
either centric or eccentric movement .
Fremitus in eccentric movement happen in the posterior teeth ;
In normal occlusion , when we have eccentric movement , there's no non- working side contact , but in
some cases
A non-working side contact happens , which lead to excessive load and mobility of teeth upon function
(fremitus).
Periodontal examination :
Visual inspection
Periodontal probing
Assessment of mobility
Assessment of plaque and calculus
Visual inspection

9/2/2015 perio sheet#2 Hadeel Al Jarhi
6
Check color
size(presence of swelling)
changes in the position of gingival margins ( like gingival recession )
loss of stippling ; it's not a sensitive indicator unless you know that the patient had stippling
before as many people don't have stippling in their gingiva.
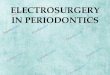
this pt had gingival swelling , sub gingival calculus ,
the chief complaint : bleeding
she had scaling and polishing but she wasn't improving
after a good perio treatment ( removing of sub gingival calculus ) she improved
the formation of black triangles was a result of the bone loss she
had, it was there before the treatment but was masked by the swelling , but
you can do either restorative Tx or veneers to hide the black triangles
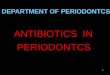
and by visual inspection you can see if there's any necrotic areas
or gingival recessing
(localized )
Generalized gingival recession

9/2/2015 perio sheet#2 Hadeel Al Jarhi
7
Check the miller classification for gingival recession form the
slides
Visual inspection includes root caries , or severe recession as seen here
- Periodontal probing
Probing depth vs. pocket depth
Probing depth : The degree of penetrating of the periodontal probe (clinical measure )
Pocket depth : histological term refers to the depth from the gingival margin to the most coronal cell of the
gingival sulcus
The difference is there because the tip of the probe does not stop at the most
coronal cell of the junctional epithelium ( it just enters it )
The degree the penetration depend on :
1. The level of inflammation ( if the tissues are inflamed the probe tip
penetrates all the way through junctional epithelium and lands in the
connective tissue , after treating the pt , the tissues resist the penetration
of the probe tip and it stops more coronally)
2. The size of the probe
3. The angle of penetration
4. The presence of sub gingival calculus
5. The presence of certain anatomical varieties like enamel pearl or grooves
There're interoperator , intraoperater and intraobservor variability of measurement
We use either
Perio probes

9/2/2015 perio sheet#2 Hadeel Al Jarhi
8
Naber probes : for furcation areas
Probing in the interproximal areas :
You have to probe under the contact into the Midproximal , (not at the line
angles of the tooth)
Probing at the line angle , subgingival calculus , bulky restoration could cause an
error in determining the probe depth .
Furcation assessment
- Aim to determine the amount of bone loss
Horizontally ( in the furcation )
- So we measure the horizontal penetration by naber 's
Probe which is divided to increments f 3 mm
When the periodontal disease progress to the root trunk , the plaque extends to the root surface , so the
infection spreads to the furcation making bone loss ( furcation invasion ) , and that worsens the prognosis of
the tooth and makes it more difficult to treat .
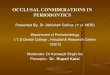
We use Hamp classification of furcation involvement :
Grade I - The furcation can be probed to a depth of 3 mm horizontally . Using the probe, the
anatomic fluting between the roots can be felt, but cannot engage the roof of the furcation.
Grade II - The furcation can be probed to a depth greater than 3 mm, but not through and through.
Grade III The furcation can be completely probed through and through subgingivally regardless of
the soft tissues .
Grade IV The probe goes completely through the furcation and is supragingival.

9/2/2015 perio sheet#2 Hadeel Al Jarhi
9
We assess the mobility using 2 instruments or our finger + an instrument Grade I : up to 1 mm Grade II : more than 1 mm in the buccolingual or mesiodistal direction Grade III : movement is greater than 1 mm in any direction and is depressible in the socket
Pus (suppuration) can be found upon probing
Calculus assessment :
- Visual inspection :
Used to detect the Supragingival calculus , or the subgingival calculus if the gingival margin was detached
- Tactile sensation
Using perio probe , periodontal explorer , curettes
The perio chart :
It shows the upper and lower teeth .
The facial and lingual surface of each tooth
Each part is divided into 3 sites as we probe 6 sites ( 3
facially and 3 lingually )
We have to probe to determine the gingival index and the
plaque index

9/2/2015 perio sheet#2 Hadeel Al Jarhi
10
We probe 6 sites for each tooth and determine the PSR .
( in the clinics we have to probe only the sextants which have the PSR value as 3 or 4 )
Charting guidelines :
1- Start by Eliminating the missing teeth from the chart
2- write roman latters on the crown to represent mobility of each tooth
3- if there's a furcation invasion use a ( < ) symbol to
refer to the root that has furcation invasion Grade I
4- if the furcation is grade II , used a triangle pointing to the root
that has it .
5- use a cycle to refer to impacted/ unerupted teeth
6- Use an arrow to indicate drifting

9/2/2015 perio sheet#2 Hadeel Al Jarhi
11
7- Outline the surfaces involved in any carious lesions , and color in the areas in red to be
restored and blue for already restored.
8- Charting includes 6 sites for each tooth
( GM = gingival margin ,normally it should be coronal to the CEJ , if it was 0 = at the CEJ
BOP=bleeding on probing ( use a dot if there's bleeding and leave it if no bleeding present )
PD= probing depth )
9- Chart recession and bleeding
Periodontal pocketing is usually 5 mm or above ( assuming that it's not a pseudo pocket )
In pseudo pocket : the gingival margin migrates coronally
In a healthy situation , connective tissue is attached to the CEJ of the
root , more coronally , the Junctional epithelium lies the base of the
gingival sulcus.
In a case of periodontitis / periodontal bone loss , this complex Migrates more apically , so the part of the root which was covered by connective tissue will be exposed ( loss of attachment ) , but still there will be a part of the root covered by junctional epithelium
This is clinical attachment loss
Eg. If the probing depth was 8mm , and the clinical recession was 1mm , the clinical attachment loss will be
9mm
General rules :
When recession of the gingival margin is present, the CAL is calculated by adding the probing depth to the
gingival margin level
Example:

9/2/2015 perio sheet#2 Hadeel Al Jarhi
12
Probing depth measurement: 4 mm Gingival margin level: +2 mm* Clinical attachment loss: 6 mm
When the gingival margin is coronal to the CEJ, the CAL is calculated by subtracting the gingival margin level from the probing depth. Example: Probing depth measurement: 9 mm Gingival margin level: -3 mm* Clinical attachment loss: 6 mm
When the gingival margin is slightly coronal to the CEJ, no calculations are needed since the probing depth and the clinical attachment level are equal. Example: Probing depth measurement: 6 mm Gingival margin level: 0 mm* Clinical attachment loss: 6 mm
Remember : the root (cementum) of any healthy tooth should all be covered by PDL fibers
The bone is 1-2 mm away from the CEJ and attached to it by dentogingival fibers (PDL fibers )
The exposed part of the root represents the clinical attachment loss ( exposed doesn’t mean recession away , it's
any loss of attachment detected by probing )
Radiographic examination
- Used to detect horizontal or vertical bone loss )

9/2/2015 perio sheet#2 Hadeel Al Jarhi
13
- An imaginary line is drawn between the CEJ of adjacent teeth , if the contour of the alveolar bone
is parallel its either normal situation or horizontal bone loss , if its perpendicular to the contour it’s
a vertical bone loss .
- the presence of radiolucency in the furcation area doesn’t mean
that
there's furcation invasion unless its proved clinically
as this radiolucency could be caused by a perforation after endo
Tx
- A full mouth series is usually needed ( panorama x-ray can be used too)
- Vertical bitewings are used to detect the bone loss
- The major difference between gingivitis and periodontitis is the plaque induced attachment loss
- Gingivitis is not progressive , periodontitis is a progressive
disease causing bone loss
- In this case the patient has periodontitis , if the patient was left
without treatment , the disease will progress , he/she will have
more bone resorption and attachment loss , even if he/she
doesn't have pockets
- Pockets presence is a very important periodontal parameter but its not the primary difference
between gingivitis and periodontitis
*I added extra informations to clarify some points*
Good Luck .