Embed Size (px)
Citation preview

Factors influencing low uptake Factors influencing low uptake of breast screening services in of breast screening services in
DundeeDundee
Dr Rosemary Millar: StR NHS TaysideDr Rosemary Millar: StR NHS TaysideDr Julie Cavanagh: CPHMDr Julie Cavanagh: CPHM
Dr Elizabeth Magee: Public Health Dr Elizabeth Magee: Public Health OfficerOfficer
BackgroundBackground
Aims Aims
Literature ReviewLiterature Review
Focus GroupsFocus Groups
Conclusions Conclusions
Breast CancerBreast Cancer
Important public health problemImportant public health problem
1.38 million cases worldwide 1.38 million cases worldwide
Variation between countriesVariation between countries
Numerous risk factorsNumerous risk factors
Lifestyle and environmental factors Lifestyle and environmental factors probable given change in risk following probable given change in risk following migrationmigration
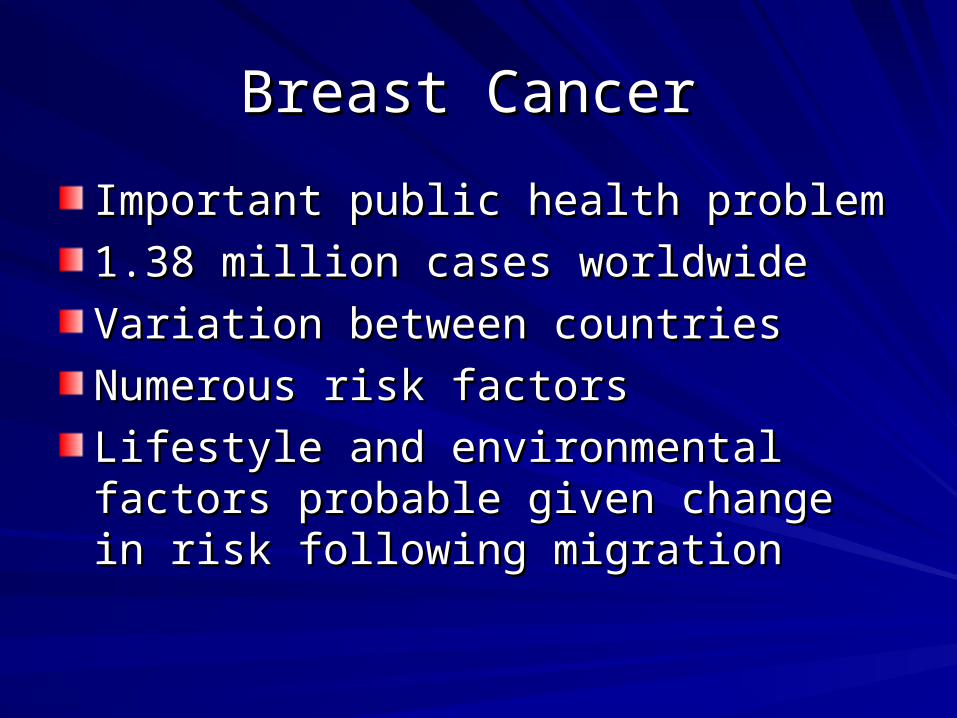
Breast cancer (C50), European Age-Breast cancer (C50), European Age-Standardised Incidence and Mortality Rates , Standardised Incidence and Mortality Rates ,
Females, Great Britain, 1975- 2008Females, Great Britain, 1975- 2008
DDownloaded from ownloaded from http://info.cancerresearchuk.org/cancerstats/types/breast/incidence/http://info.cancerresearchuk.org/cancerstats/types/breast/incidence/ access Aug 2011 access Aug 2011
0
20
40
60
80
100
120
1401
97
5
19
77
19
79
19
81
19
83
19
85
19
87
19
89
19
91
19
93
19
95
19
97
19
99
20
01
20
03
20
05
20
07
Year of diagnosis/death
Ra
te p
er
10
0,0
00
po
pu
lati
on
Incidence Rates Mortality Rates
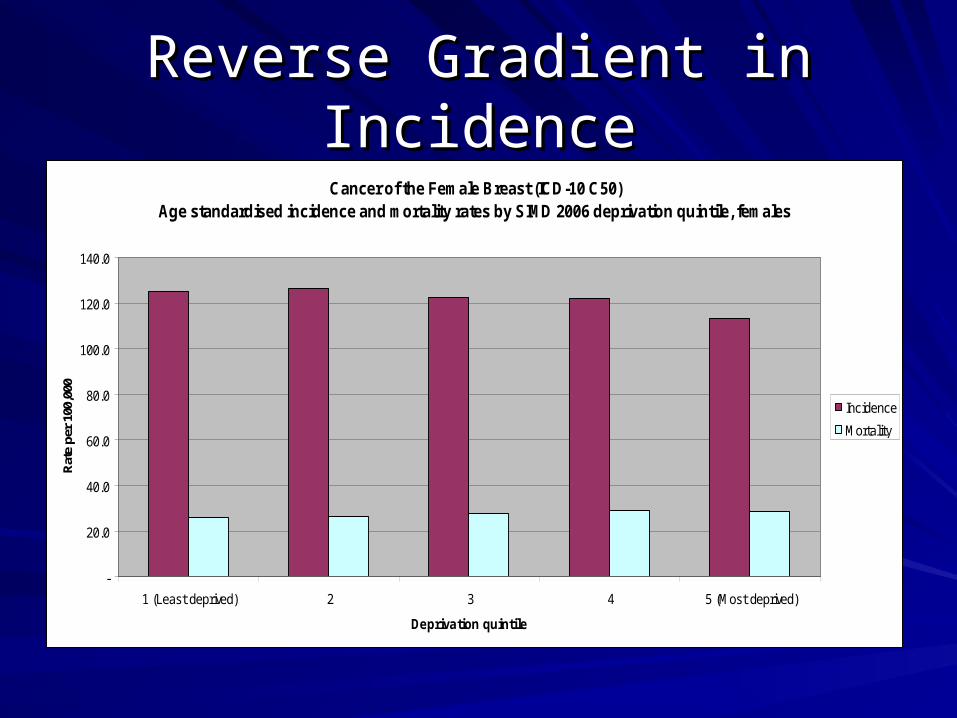
Reverse Gradient in IncidenceReverse Gradient in IncidenceCancer of the Female Breast (ICD-10 C50)
Age standardised incidence and mortality rates by SIMD 2006 deprivation quintile, females
-
20.0
40.0
60.0
80.0
100.0
120.0
140.0
1 (Least deprived) 2 3 4 5 (Most deprived)
Deprivation quintile
Rat
e pe
r 10
0,00
0
Incidence
Mortality
Breast ScreeningBreast Screening
Three yearly screening programme, Three yearly screening programme, established 1988established 1988Women aged 50-64 until 2003 when age Women aged 50-64 until 2003 when age extended to 70extended to 70High uptake needed if programme to High uptake needed if programme to reduce morbidity and mortalityreduce morbidity and mortalityMinimum screening uptake standard, 70% Minimum screening uptake standard, 70% with target of 80%with target of 80%Scottish average 76.2%, Tayside 80.3%Scottish average 76.2%, Tayside 80.3%

Scatter plot showing the relationship between breast screening Scatter plot showing the relationship between breast screening uptake and percentage of patients for LEAST deprived SIMD uptake and percentage of patients for LEAST deprived SIMD
quintiles for Dundee GP practices.quintiles for Dundee GP practices.
Data from Patient Data Base, NHS Tayside via Business Objects (Tayside, Data from Patient Data Base, NHS Tayside via Business Objects (Tayside, Fife & Forth Valley Consortium, excluding any Grampian patients - linked Fife & Forth Valley Consortium, excluding any Grampian patients - linked to A-CHI System)to A-CHI System) Extracted July 2010Extracted July 2010
Scatter Plot of percentage breast screening uptake by proportion of patients in the least deprived SIMD quintiles (4 and 5) for each Dundee
GP practice over 3 rounds.
0
1020
30
4050
60
7080
90
0 10 20 30 40 50 60 70 80 90 100
Proportion of patients in SIMD 4 and 5 ( least deprived) for each Dundee GP practice
Bre
ast
scre
enin
g u
pta
ke (
%)
Round 5: 2002-04
Round 6: 2005-07
Round 7: 2008-10
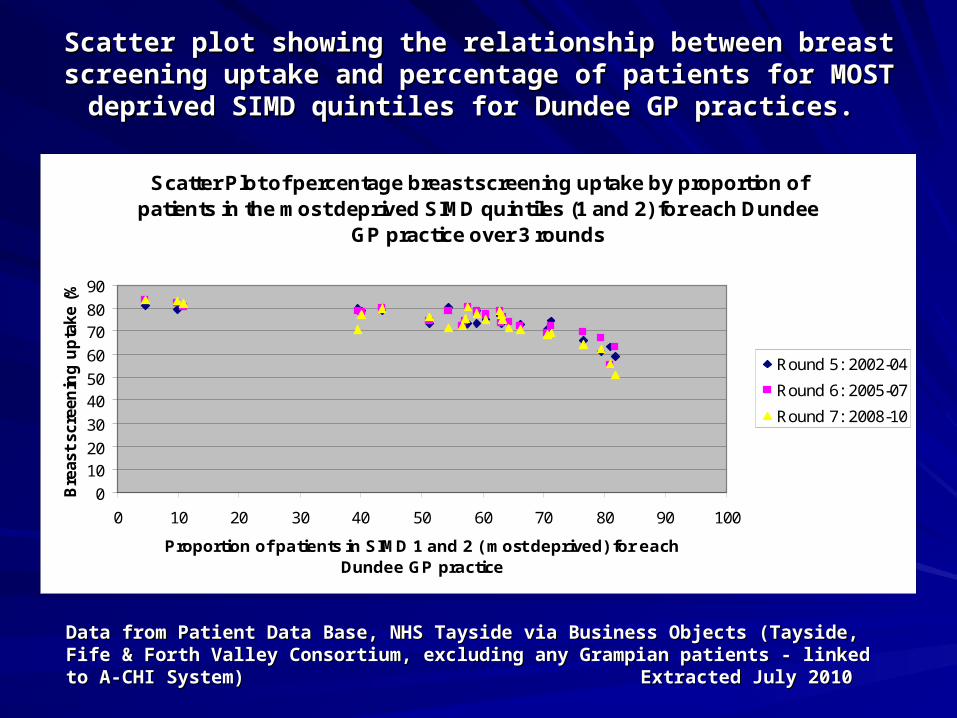
Scatter plot showing the relationship between breast screening Scatter plot showing the relationship between breast screening uptake and percentage of patients for MOST deprived SIMD uptake and percentage of patients for MOST deprived SIMD
quintiles for Dundee GP practices.quintiles for Dundee GP practices.
Data from Patient Data Base, NHS Tayside via Business Objects (Tayside, Data from Patient Data Base, NHS Tayside via Business Objects (Tayside, Fife & Forth Valley Consortium, excluding any Grampian patients - linked Fife & Forth Valley Consortium, excluding any Grampian patients - linked to A-CHI System)to A-CHI System) Extracted July 2010Extracted July 2010
Scatter Plot of percentage breast screening uptake by proportion of patients in the most deprived SIMD quintiles (1 and 2) for each Dundee
GP practice over 3 rounds
0
1020
30
4050
60
7080
90
0 10 20 30 40 50 60 70 80 90 100
Proportion of patients in SIMD 1 and 2 ( most deprived) for each Dundee GP practice
Bre
ast
scre
enin
g u
pta
ke
(%)
Round 5: 2002-04
Round 6: 2005-07
Round 7: 2008-10

Screen detected compared to Screen detected compared to symptomatic breast cancersymptomatic breast cancer
Screen detected cancers higher probability of Screen detected cancers higher probability of being smaller, lower grade, node negative, in the being smaller, lower grade, node negative, in the EPG/GPG, oestrogen receptor positive and less EPG/GPG, oestrogen receptor positive and less likely to be HER2 positive (true across all likely to be HER2 positive (true across all deprivation quintiles and ages)deprivation quintiles and ages)
Screening reduces inequalities???Screening reduces inequalities???
Survival rates higher for women with screen Survival rates higher for women with screen detected cancer compared to symptomaticdetected cancer compared to symptomatic

AimsAims
Identify barriers and facilitators to Identify barriers and facilitators to attending breast screeningattending breast screening
MethodsMethods
Literature review to identify barriers and Literature review to identify barriers and facilitators to uptakefacilitators to uptake
Invitations to all non attending Dundee Invitations to all non attending Dundee women from 2 GP practices to attend women from 2 GP practices to attend focus groupsfocus groups

Results of literature reviewResults of literature review
15 papers on barriers and facilitators, 15 papers on barriers and facilitators, including 2 systematic reviews although including 2 systematic reviews although majority descriptive studiesmajority descriptive studies
13 papers on interventions to improve 13 papers on interventions to improve uptake including 2 systematic reviews, 1 uptake including 2 systematic reviews, 1 meta analysis, 2 Cochrane reviews and 2 meta analysis, 2 Cochrane reviews and 2 RCT’sRCT’s

Literature review findings: Literature review findings: Barriers and FacilitatorsBarriers and Facilitators
Socioeconomic deprivationSocioeconomic deprivation
Sociodemographic factorsSociodemographic factors
Attitudes and beliefsAttitudes and beliefs
Previous experience breast screeningPrevious experience breast screening
Access to servicesAccess to services

Literature review findings: Literature review findings: Interventions to improve uptakeInterventions to improve uptake
Combined, access enhancing interventions and Combined, access enhancing interventions and individual directed interventions achieved the individual directed interventions achieved the best improvement in uptake 26.9% [9.9%-best improvement in uptake 26.9% [9.9%-43.9%] 43.9%]
Interventions to improve uptake Interventions to improve uptake contd.contd.
IMPROVE ACCESSIBILITYIMPROVE ACCESSIBILITYMailed invitation letter:- OR 1.66 [1.43-1.92]Mailed invitation letter:- OR 1.66 [1.43-1.92]Mailed education material:- OR 2.81 [1.96 -4.02]Mailed education material:- OR 2.81 [1.96 -4.02]Letter of invitation combined with phone call:- Letter of invitation combined with phone call:- OR 2.53 [2.02-3.18]OR 2.53 [2.02-3.18]Phone call:- OR 1.94 [1.70-2.23]Phone call:- OR 1.94 [1.70-2.23]Training activities plus a reminder:- OR 2.46 Training activities plus a reminder:- OR 2.46 (1.72-3.50](1.72-3.50]Reduce travel distanceReduce travel distanceRemoval of financial barriersRemoval of financial barriers

Interventions to improve uptake Interventions to improve uptake contd.contd.
SYSTEM EFFECTSSYSTEM EFFECTS
More accurate patient registersMore accurate patient registers
Financial incentives to GP’s with practice Financial incentives to GP’s with practice screening lead screening lead
Enhance screening service with increased Enhance screening service with increased capacity for calls and customer service capacity for calls and customer service improvementsimprovements
Interventions to improve uptake Interventions to improve uptake contd.contd.
UNDERSTANDING AND INFORMED UNDERSTANDING AND INFORMED CONSENT CONSENT
Personalised risk information helps a little Personalised risk information helps a little
Person to person communicationPerson to person communication
Tailored telephone counsellingTailored telephone counselling

Focus GroupsFocus Groups
We undertook focus groups with our target We undertook focus groups with our target population to discover what their perceived population to discover what their perceived barriers were. barriers were. Selected 2 GP practices with deprived Selected 2 GP practices with deprived catchments, who were shortly to be screenedcatchments, who were shortly to be screenedAll women who had missed their most recent All women who had missed their most recent appointment had an invitation letter included with appointment had an invitation letter included with their reminder letter from SBSS.their reminder letter from SBSS.400 letters posted over 2 separate rounds in 400 letters posted over 2 separate rounds in early 2011early 2011£10 offered as token of appreciation to cover £10 offered as token of appreciation to cover transport costtransport cost

Awareness raisingAwareness raisingPosters published in Posters published in house and delivered to house and delivered to local shops near to the local shops near to the surgeries.surgeries.
Displayed in Displayed in participating surgeries participating surgeries and concourse of and concourse of Ninewells Hospital.Ninewells Hospital.
Posted to top ten Posted to top ten frequented pharmacies frequented pharmacies for each practicefor each practice

Subject recruitmentSubject recruitment
11 respondents indicated a willingness to 11 respondents indicated a willingness to attend, with 6 in the first tranche and 5 in attend, with 6 in the first tranche and 5 in the second. the second. 2 groups held: 5 attendees in March 2011, 2 groups held: 5 attendees in March 2011, however only 2 of the 6 attended the however only 2 of the 6 attended the second group in June 2011second group in June 2011Both researcher and scribe attended the Both researcher and scribe attended the first group, and researchers only for the first group, and researchers only for the second groupsecond groupConsent forms signedConsent forms signed

Main themes: Main themes: Barriers and FacilitatorsBarriers and Facilitators
• Fear and AnxietyFear and Anxiety• Fear of the processFear of the process• Fear of outcome/bad news Fear of outcome/bad news • Worry about radiationWorry about radiation• Delay inducing anxietyDelay inducing anxiety
• Individual and Life Individual and Life Circumstances:Circumstances:• Issues of childcare/ Issues of childcare/
dependants/ carers make it dependants/ carers make it hard to attend hard to attend appointmentsappointments
• Work Work responsibilities/Forgettingresponsibilities/Forgetting
• Poor healthPoor health• Loss of a friend or relative Loss of a friend or relative
through breast cancer through breast cancer
• AccessAccess• TransportTransport• Parking at HospitalParking at Hospital• Mobile location not Mobile location not
convenientconvenient• WeatherWeather
• Ardent Non attendersArdent Non attenders
Main Themes: Group perception of Main Themes: Group perception of what helps?what helps?
Mobile unitsMobile units
Recall serviceRecall service
Current advertising and marketingCurrent advertising and marketing
Changing attitudesChanging attitudes
Breast screening informationBreast screening information
Group Ideas for the FutureGroup Ideas for the Future
Local Champions for screeningLocal Champions for screening
Mobile units in the heart of communities Mobile units in the heart of communities
Drop in serviceDrop in service
More education about breast cancerMore education about breast cancer
Organisational changesOrganisational changes
ConclusionsConclusions
Focus group findings in keeping with those Focus group findings in keeping with those from the literature reviewfrom the literature review
We can look at interventions to increase We can look at interventions to increase uptakeuptake
Cost is a prime barrier to further interventionsCost is a prime barrier to further interventions
Further work needed to determine the Further work needed to determine the possible yield of extra cancers to ascertain possible yield of extra cancers to ascertain whether further interventions to increase whether further interventions to increase uptake would be cost effective. uptake would be cost effective.

Any questions?Any questions?