Embed Size (px)
Citation preview

EXPERIMENTAL STUDIES OF THE LACRYMAL PASSAGEWAYS.
BY
K. G. PLOMAN. A. ENGEL AND F. KNUTSSON.
It is a well-known fact that the mechanism for the convey- ance of the lacrymal secretion from the eye into the nasal cavity has not yet been conclusively explained. Most authors agree, however, that contractions of the musculus orbicularis provide the active power. Schirmer’s observation that the tears do not run down into the nose when the movements of the eyelids are suppressed has been generally confirmed by other investigators; paresis of the facial nerve is sometimes accompanied by an overflow of tears before any eversion of the lower lid can be seen. Opinions differ, however, as to which part or parts of the tear-conducting apparatus, and which phase of the movement of the lids, the opening or the closing, are most essential for the transportation of the tears.
A large number of investigators, mainly older ones, attribute the greatest importance to the lacrymal sac, and maintain that its variations in volume, resulting from the movements of the eyelids, constitute the mechanism. Arlt, Aubaret, Rochat and Benjamins and some others maintain that the lacrymal sac is compressed, and its contents emptied into the naso- lacrymal duct by the contraction of the orbicularis, i. e., when the eyelids approach each other in winking, and in closing or forcibly contracting the lids. The canaliculi are closed during this phase by, among other factors, the sphincter muscles around the puncta lacrymalia. When the orbicularis relases

56
and the eye is opened, the lacrymal sac becomes distended and the tears are sucked into it through the now opened canaliculi. Hyrtl, uon Craefe, Doiiders, Schirmer and some others have a diametrically opposite opinion, viz., that the contraction of the orbicularis expands the lacrymal sac, which then sucks in the tears from the conjunctival sac, and that the relaxation of the muscle fibers leads to a purely elastic contraction of the lacrymal sac, the contents of which are thereby passed on into the nasal cavity.
While these two theories do not attribute any great importance to the canaliculi, there is a third, supported by Frieberg and others, which does. The mechanism is supposed to be the following: when the eye is closed, the canaliculi are compressed, and empty their contents into the lacrymal sac for further conveyance into the nasal cavity; when the eye is opened, their lumina are distended and the tears drawn in from the conjunctival sac. This view gains support from the clinical experience of recent years. A success- ful dacryocystorhinostomy thus shows that the tears, when they do not pass through the lacrymal duct, may still be conveyed into the nasal cavity by the action of the canaliculi alone. This observation certainly gives probability to the supposition that the canaliculi play a great rdle in the removal of the surplus lacrymal secretion in the case of normal passageways as well.
We have access to no clinical experience to illustrate the importance of the lacrymal sac in a similar way, although the absence of an overflow of tears after slitting up the lower canaliculus as completely as possible, indicates that the lacrymal sac is not entirely functionless in this connection. For clinical experience has shown that the upper canaliculus alone, when the lower one is occluded, is not seldom in- sufficient. Nor does Frieberg deny the possibility of the functional cooperation of the lacrymal sac by means of changes in volume resulting from the movements of the eye- lids. He stresses the fact that the anatomical conditions can in that case hardly account For anything but compression

57
upon closing the eyes. Other authors also assume a coopera- tion between the canaliculi and the lacrymal sac.
It is deserving of mention, too, that some authors coiisider the musculus orbicularis non-essential. Thus for instance .I. L. Petit and Gad attribute a siphon effect to the lacrymal passageways. This view gains a certain amount of support from the observation made by Krehbiel in 1878, that a liquid which is carefully dropped into the eye will disappear in the inner corner, even if the movements of the eyelids are as far as possible suppressed. Frieberg has lately repeated this experiment on himself, and confirmed this siphon effect in an upright position of the head, which is in opposition to the common view that is based on investigations by Schirnier and others, that the movements of the eyelids are a necessary prerequisite for the conveyanct of the tears into the nasal cavity. It is possible that Krehbiel's experiment is successful only on certain individuals. E. H. Weber, Hasner and others hold that the changes of pressure in the nasal cavity on inhalation and exhalation produce a suction on the tears. Arlf has, in opposition to this view, correctly asserted that there would in consequence be an overflow of tears in mouth breathing. Another objection to this view is based on experience in cases of fistula lacrymalis, when the ductus naso-lacrymalis is closed, but the tears nevertheless conveyed from the eye to the fistular opening in winking.
The value of the numerous observations made in connec- tion with lacrymal fistule has given occasion for much dis- cussion. In some cases, the aspiration, upon closing the eye, of a drop of liquid situated in the opening of the M u l e has been observed, and has been thought. to be due to an expansion of the tear, sac followed by suction (Donders, 11. Graefe, Gilse and others). Arlt and others have, on the other hand, made the contrary observation that a drop of liquid has appeared in the fistule on closing the eye, and interpreted this as a result of a simultaneous compression of the tear sac. Schirmer has very correctly remarked that all these observations are of slight value in judging physiolo-

58
gical conditions, inasmuch as the fistule is a pathological phenomenon, in the production of which changes followed by extremely varying effects o n the function, may have taken place.
Our In uestigations. Our experiments, which are divided into a roentgenological
and a volumetrical group, have the object of ascertaining whether there are any changes in shape or volume in the lacrymal passageways, exclusive of the canaliculi, in connec- tion with the movements of the eyelids.
A. Roentgen Experiments. '
During the last few years, a number of investigations of the tear-conducting passages have been made with the aid of Roentgen rays, but their main purpose has been to throw light on pathological conditions. Aubaref, and above all, u. Szily have been foremost in this field. Sulphates of thorium and barium were first employed, suspended in water, oil or paraffin, but these substances, because of purely technical difficulties in their use, were gradually abandoned in favour of lipiodol.
The American scientists Campbell, Carfer, and Doub have made a comparative investigation of the lacrymal passageways of whites and negroes, but it seems that Roentgen rays were not employed in the funciional examination.
Those parts of the tear-conducting passages which one could hope to study with Roentgen rays are obviously the lacrymal sac and the naso-lacrymal duct. The canaliculi are too small to permit theii variations in volume to appear on the plates, and often they become insufficiently or not a t all filled with the opaque substance, in which case they are not visible on the plate. It would be desirable to employ a contrast of the same consistency as the tears. We have as a matter of fact, tried such a one, umbrenal, but found that it could not be used, because it was. so speedily conveyed into the nasal cavity that comparison between the different

plates was made impossible and its shadow, too vague. We have therefore used lipiodol, which gives a dense shadow and which, upon being slightly warmed in the syringe, is always easily injected. Lipiodol is, to be sure, slightly tough and viscous, for which reason it probably distends the lacrymal sac somewhat, and possibly prevents it from going through with natural speed the changes of shape which may be produced by different kinds of movements of the eyelids. This is, however, of little consequence, as the long exposure excludes the possibility of studying the influence of winking. We have instead directed our investigation to' the question of whether the roentgenogram differs in ordinary winking and in the forcible contraction of the orbicularis.
I n all cases, the subject has occupied a recumbent position during exposure, and where the contrary is not expressly stated, lipiodol was injected when the subject was lying down, since otherwise, as we learned from earlier unsuccesful ex- periments, the contrast passed too rapidly down into the nasal cavity. Hut this precautionary measure is not sufficient; it is also necessary that the tear sac during exposure occupies the lowest position in the passageways. When an exposure is made in the occipitofrontal direction, this position is obtained by supporting the forehead on the horizontally placed cassette, while the nose touches it very lightly. I n lying horizontally on the back, the tear sac will be higher than the duct, unless the head is strongly bent back (cf. p. 74). In l'ying on the side, there is also some slight risk of the lipiodol running too quickly into the nasal cavity (cf. p. 68, Case K. E. L., Exper. I). The individuals on whom these experiments were made are medical students, all of whom have entirely healthy and normally functioning tear-conducting passages.
Report of Experiments. It might be well to point out that in the following, the
designations lacrymal scxc and ncxso-lacrgmal duct are used for purely practical reasons, and not at all in order lo emphasize any well difrerentiated anatomical regions. One

60
is generally able to make out an upper wider ssacg and a somewhat narrower >duct<, but sometimes there is only an indistinct demarkation or none at all, in which case only a comparison with roentgenograms of cases showing this de- markation motivates a differentiation between sac a n d duct. I n order to avoid repetition, it should be stated that the dimensions of the shadows on our plates were as a rule the following: the tear sac, vertical diameter (both in accipito- frontal and in biteniporal exposure) about 10 mm, frontal diameter (occipitofroi~tal exposure) 1 to 3 mm, sagittal dia- meter (bitemporal exposure) 5 to 7 mm; the naso-lacrymal duct just below the lacrymal sac, frontal diameter, 1 to 2 mm, sagittal diameter, 2 to 4 mm. Our roentgenograms beauti- fully illustrate the great variations in anatomical conditions which have been earlier demonstrated, especially by Aubaret's investigations.
Whenever, in the following, we mention >winking<, we mean that the subject during exposure performed the natural spontaneous movements of winking; by Bcontractione we mean that he kept the eyes firmely closed during exposure by a forcible contraction of the orbicularis. When nothing to the contrary is mentioned, the exposures have been made with only so short an interval of time as was absolutely necessary for the changing of the plates, or ':bout from two to three minutes.
F. K . , aged 25. I A. Two plates, the one of winking, the other of con-
traction, were bitemporally exposed with the, left tear sac, filled with lipiodol, nearest to the plate. These plates are not entirely comparable as the position of the head was slightly changed between exposures, but they plainly illustrate the interesting fact that the distinct shadow found in winking in the upper part of the lacrymal duct has become much weaker in contraction.
I B. Bitemporal exposure with the right tear sac, filled with lipiodol, nearest to the plate. (PI. I , Fig. 1 to 3).

P1. I CASE I=. li.
Experiment I B. Bitemporal exposure.
Fig. 1. Fig. 2. Fig. 3. Winking. Contraction, Winking.
Experiment IV A . Occipitofrontal exposure.
Fig. 4. Fig. 5. Winking. Contraction.
Experiment I17 11. Froiitooccipital exposwe.
Fig. 6. Win king.
Fig. 7 . Contraction.
Fig. 8. Winking.

CASE A . E. Experiment I B. Bitemporal exposure.
Fig. 9. Fig. 10. Fig. 11. Winking. Contraction. Winking.
Experiment II. Occipitofrontd exposure.
Fig. 12. Winking.
Fig. 14. Winking.
Fig. 13. Contraction.
Fig. 15. Contraction.
P1. I1

61
Plates 1 and 2, winking, show identical shadows, for which reason only Plate 2 is reproduced 'here (Fig. 1). The sac is shown to be divided by a constriction into an upper, smaller part, and a lower, larger one. The duct is well distended, but its shadow is not quite as dense as that of the sac.
Plate 3. Contraction. (Fig. 2). The picture is slightly indistinct be- cause of movement during exposure. Quite plainly, however, there is an increase in the sagittal dimension in the upper division of the sac, while a slight decrease in the same dimension is visible in the lower division at the entrance to the duct. At the same time, the shadow in the upper part of the duct has disap- peared. The lower part of the sac on this plate has a shape like an inverted cone, resembling that found in Case K. 0. G., p. 66 (Fig. 17).
Plate 4. Winking. (Fig. 3). The shadow 'of the sac has now again the appearence found on Plates 1 and 2 (Fig. l), and the duct is again filled with impervious material.
Comment: The most striking facts demolistrated by these roentgenograms are the following: that the sagittal diameter increases in the upper part of the sac during contraction, that the duct is simultaneously emptied of contrast,. and that when the eyes are opened, the sac and duct again appear as before.
11. Occipitofrontal exposure, recumbent position, face down- ward, the ' t ear sac lowest.
Plate 1. Winking. The right sac gives a shadow of equal breadth throughout, while the right duct gives no shadow. The shadow of the left sac is somewhat narrower in the upper part than in the lower, with dimensions of 2.5 mm and 3 m m respectively. Just below the sac there is no shadow for the duct, but it begins 3 mm further down.
Plate 2. Contraction, The shadow of the right sac is on the whole somewhat smaller than before, and narrower in the lower part than in the upper. The shadow of the left sac also shows some diminution in size as well as a great change of shape, the lower part tapering very much and continuing directly into the narrow but distinct shadow of the duct.

62
Comment: This exposure shows some diiiiinution in the shadows during contraction, and the shape is changed in that the lower part, which earlier was equal to or greater in width than the upper, is now smaller. Some of the contents of the left sac, which was probably more completely filled than the right one, were, as far as one can judge, pressed out into the duct by the contraction.
111. Occipitofrontal exposure, recumbent position, face down- ward, the tear sac lowest.
Plate 1. Winking. The shadow of the right sac is broader in its lower part than in its upper, the dimensions being 3 mm and 2 mm respectively. It continues directly into the narrow shadow of the duct. The left sac also has a shadow which is broader in the lower part, the dimensions being 2 ' / 2 mm and 2 mm. From a point a little above the lower pole on the nasal side, the shadow of the duct, 1 mm wide, proceeds.
Plate 2. Contraction. The shadow of the right sac is 'spindle-shaped and tapers down into a very narrow point connected with the extremely narrow shadow of the duct, discernable only with difficulty, and very much less dense than on the preceding plate. The shadow of the left sac is throughout narrower than on the preceding plate. It is now broader in the upper part than in the lower, the dimensions being 2 mm and l'/% mm respectively. The shadow of the duct just below the sac is considerably narrower than before.
Plate 3. Winking. The shadow of the right sac is again, as on Plate 1, broader below, and the upper part of the duct is also more distinct, although not as much as on the first plate. The shadow of the left sac is of about equal width throughout, and the upper part of the duct is again more distinct; just below the sac it is very narrow, but only a few millimeters further down it widens.
Plate 4. Contraction. The shadows of both sacs are of the same width in the upper part as on the preceding plate, hut in the lower part they are plainly narrower, the right one thus being of equal width throughout, while the left one is wider in the upper part. The upper part of the duct is hardly discernible on either side.

63
Comment: This series shows a progressive, slight diminution of the shadows in the course of tlie experiment. The difference between winking and contraction is here also discernible in that the lower part of the sac and the upper part of the duct are compressed in the frontal diameter during contraction, while they become wider again in winking. In this experiment contraction does not, however, lead to any visible expansion of the upper part of the sac. The opaque material is evidently conveyed toward the duct during contraction, and later it flows back into the sac by the force of gravity. Possibly there is also an active displacement toward the upper part of the sac. It is of some interest to note that in spite of the position of tlie head, nothing of the contrast flows back into the con- junctival sac by way of the canaliculi.
Exposure in one plane can not give definite information about the compression of the tear sac, but when the plates from this experinient are compared to the profile photo- graphs in experiment 1 B, it becomes evident that there is a compression of the sac in all diameters; this is found to be true of the duct also. I V A. Occipitofrontal exposure, recumbent position, face downward, the tear sac lowest. (PZ. I, Fig. 4 to 8).
Plates 1 to 4 were exposed in winking (Plate 4 is reproduced in Fig. 4), plates 1 to 3 in the fastest succession possible; between the third and fourth, there was an interval of three niinutes. The shadows on all the plates are practically identical; the sacs tapering upward and broader in the lower part, where they are joined by the shadow, 5 inm in length, of the duct.
Plate 5. Corilraction. (Fig. 5). The shadows of both sacs are now of about equal width throughout, and it is therefore mainly the left sac, which was previously cone-shaped, which has changed considerably. The shadows of the ducts are very much narrower than in winking. IV R. After new injection with lipiodol, exposure was made in the recumbent position, face zipward, the tear sac highest. Because of the increased distance from the plate, the shadows are now larger than before.

64
Plate 6. Winking. (Fig. 6). The sacs, which are now again well filled, are as before in winking narrower in the upper part than in the lower, and continue into the broad, distinct shadows of the ducts.
Plate 7 . Contraction. (Fig. 7). The shadows of the sacs are in coniparison with those on the last plate, broader in the upper part, and narrower in the lower, while the ducts show con- siderably narrower shadows.
Plate 8. Winking. (Fig. 8). The upper part of both sacs is almost emptied of opaque material, and the. shadows of the ducts are again broad as on Plate 6.
Comment: When the tear sac occupies the lowest position, winking produces hardly any change whatever, as shown by €he four practically identical Plates 1-4 (Fig. 4). Con- traction produces the characteristic change, a narrowing i n the lower part of the sacs and a diminution of the opaque substance in the upper part of the ducts. When the tear sac is highest, the opaque material is gradually conveyed into the nasal cavity, so that it becomes impossible to judge the changes of shape. Rut as in the other experiments, we find here too, that contraction leads to a compression of the upper part of the duct, which in winking becomes filled again, but in this case from the sac instead of from its own lower part, because of the position of the head.
A . E., aged 26. I A: Occipitofrontal exposure, recumbent position, face downward, the tear sac lowest.
Four plates exposed in winking, three minutes between each exposure, show shadows of sac and duct of identical shape and size. During the course of the experiment, none at all or at any rate extremely little of the opaque substance was thus conveyed into the nasal cavity.
I B. Bitemporal exposure with the right tear sac, filled with lipiodol, nearest to the plate. (PI. II, Fig. 9 to 11).
Plates 1 and 2. Winking. (Plate 2 is reproduced on Fig. 9). Both the tear sac and the duct seem to be well filled on both plates. Above the sac there are some small spots and streaks, probably

65
from opaque material dropped into the conjunctival sac. There is an angle pointing forward, which perhaps represents the boundary between sac and duct, 10'/e mm from the top of the shadow.
Plate 3. Contraction. (Fig. 10). The shadow above the angle just mentioned has increased to 12 mm, and with the exception of its uppermost part, it appears less dense. The sagittal diameter appears slightly diminished, and the anterior and posterior contours of the shadow are straighter. The shadow of the tear sac now extends up to the small shadows which probably repre- sent contrast in the conjunctival sac, and which on this plate appear to have run together.
Plate 4. Winking. (Fig. 11). This plate agrees in all essentials with Plates 1 and 2 (Fig. 9).
Comment: In contraction, the lower part of the sac is com- pressed both in the sagittal and frontal diameters, the latter fact being evident from the fading of the shadow. The opaque material i s evidently pressed up into the upper- most part of the sac, which was not earlier filled with it. There is no marked change -in the contents of the duct.
11. Occipitofrontal exposure, recumbent position, face down- ward, the tear sac lowest. (PZ. 11, Fig. 12 to 15).
Plate 1. Winking. (Fig. 12). The shadow of the right sac is throughout about 2'/2 i!im wide, and continues into the short shadow of the duct, which resembles a peg. The shadow of the left sac is also of the same width throughout, but narrower than the right one, its diameter being only slightly more than 1 mm. The shadow continues into the shadow of the duct, the uppermost part of which is very narrow.
Plate 2. Contraction. (Fig. 13). The shadow of the right sac has in its upper part increased in width to 3 mm; below, i t is slightly narrower and less dense thaii before. The duct gives a more distinct shadow. The shadow of the left sac is spindle-shaped and I'/Y nim wide across the middle. The upper part of the duct contains practically no opaque material.
Plate 3. Winking. (Fig. 14:. The shadow of the right sac has, on the whole, the same shape as on Plate 1 (Fig. 12), and the duct is again less distinct. The shadow of the left sac has now lost its spindle-shape. and appears of inore equal width throughout,
5

66
as on Plate 1. The upper part of the duct contains no impervious material,
Plate 4. Contraclion. (Fig. 15). Both sacs and ducts give very much the same appearance as on Plate 2 (Fig. .13).
Comment: W e find with respect to the sac the same con- ditions in this case as in case F. I<. The shadow is of equal breadth throughout in winking, but in contraction, it is narrower in the lower part and broader in the upper. The duct on these plates also shows the same changes as in case F. K., experiment 11, in that a small amount of the opaque material in contraction is pressed from the sac into the duct.
K . 0. G., aged 25. I. Bitemporal exposure, with the left tear sac, filled with lipiodol, nearest to the plate. (PI. ZZI, Fig. 16 to IS).
In this experiment, three 'exposures were made: Plates 1 and 3, Winking (Fig. 16 and 18). Plate 2, Contraction (Fig. 17), exposure made after Plate 1. Fig. 16 and 18 are on the whole much alike, each showing a distinct, dense shadow of both sac and duct. At the top, it ends in a less dense, hook-shaped shadow which probably belongs to the sac. In its neighbourhood there are some small shadows which no doubt are those of particles of lipiodol in the canaliculi or the conjunctival sac.
The similar shadows on Fig. 16 and 18 have on Fig 17 under- gone a considerable change. In a region 7 or 8 mm long, visibly located at the transition between sac and duct, the shadow has diminished very much in width. But in the upper part, the shadow has been lengthened a distance of about 3 nun, and here it is distinctly broader. The hook-shaped shadow visible in winking has changed into a denser arched shadow, connected with the main shadow by means of a very narrow string of contrast.
We repeated this experiment and found fairly good agreement in the appearence of the shadow of the sac, wherefore we feel justified in supposing that the upper hook-shaped or arched shadow really belongs to the sac. Case K. 0. G evidently has a division of the left tear sac, similar to that shown in the right sac of Case F. K. (PI. I, Fig. 1 to 3).
11. Occipitofrontal exposure, recumbent position, face down- ward. the tear sac lowest. (Pl. 111, Fig. 19 to 23).

67
Plates 1 to 3. Winking. These present identical shadows, for which reason only the latter is reproduced (Fig. 19). The shadow of the right sac is about 1 mm broad throughout, and continues into the very narrow shadow of the duct. The shadow of the left sac is about 2 mm broad throughout, and continues into the shadow of the duct, which is shaped like a corkscrew and has about the same width as the shadow of the sac.
Plate 4. Contraction. (Fig. 20). The shadows of both sacs have changed shape, become broadest at the upper end, and taper down into a point. On the right, the upper part of the duct is no longer visible, on the left, the duct just below the sac is as narrow as a thread for a distance of 1 cm, to widen again further down.
Plate 5. Winking. (Fig. 21). The shadows of the sacs again resemble those on Plate 3 (Fig. 19); the right one is about 1 mm broad throughout, the left one is narrower in the upper part than in the lower. The upper end of the right duct is not visible, the corresponding part on the left is broader than on the preceding plate, but somewhat fragmented.
Plate 6. Confraction. (Fig. 22). On the whole the same as Plate 4 (Fig. 20). The right sac is spindle-shaped, the upper end of the right duct not visible. The left sac is broadest at the upper end, and tapers down into a point. The upper part of the duct contains no opaque material for a distance of 7 mm.
Plate 7. Winking (Fig. 23). Great resemblance to Plates 3 and 5 (Fig. 19 and 21), although the shadows of the sacs are slightly reduced in size. On the right, the upper part of the duct still contains no opaque material, while the corresponding part on the left side is well filled.
Comment: The last two experiments show very distinctly, particularly in the left tear sac, how the transition region between sac and duct becomes compressed in contraction, while the contrast is pressed into the upper part of the sac and distends it. When contraction ceases, the shadows again take a shape very similar to the one they had before contraction.
Possibly the tear sac was not at the beginning of the first experiment completely filled, which may account for the difference in the appearence of the upper part in Fig. 16 and 18 and in Fig. 17.
rJ*

68
I t is plainly evident, when one compares Fig. 19 and 23, that some of the lipiodol in the course of the rather long experiment has been displaced, and definitely removed into the .nose.
K . E . L., aged 27. I. Biteinporal exposure, the left tear sac, filled with lipiodol, nearest to the plate. (PI. ZV, Fig. 24 to 26).
Plate 1. Winking. (Fig. 24). The shadow of the tear sac is pear- shaped, the narrower part pointing upwards. The beginning of the duct well filled with opaque material.
Plate 2. Contraction. (Fig. 25). The shadow of the tear sac is unchanged in the vertical diameter, but the broader part is now higher up and the lower part tapers into the shadow of the duct, which is narrower and less dense than on the preceding plate.
Plate 3. Winking. (Fig. 26). The shadow of the sac is considerably diminished, the upper end pointed and the lower part broad. The beginning of the duct is still visible on the plate, but it is nar- rower than before.
11. New injection of lipiodol, occipitofrontal exposure, recumbent position, face downward, the tear sac lowest. (PI. ZV, Fig. 27 to 31).
Plates 1 to 3. Winking. Almost identical shadows. (Plate 3 is re- produced in Fig. 27). The shadow of the right sac is of equal width throughout and very narrow. It continues without any definite boundary into the somewhat broader shadow of the duct, which in the transition region makes an angle pointing laterally. The shadow of the left sac is considerably broader in the lower part than in the upper. There appears no duct on this side.
Plate 4. Contmcfion. (Fig. 28). The shadow of the right sac has changed its shape and is now broader in the upper part thanin the lower. The shadow of the duct is much narrower and less dense than on the preceding plate, and its course is straighter. The shadow of the left sac is unchanged in the upper part, but the lower part has diminished so that it is narrower than the upper. The beginning of the duct is barely indicated.
Plate 5. Winking. (Fig. 29). Shows about the same conditions as Plate 3 (Fig. 27). The shadow of the right sac is considerably

P1. 111
CASE K . 0. G . Experiment I . Bitemporal exposure.
Pig. 16. Fig. 17. Fig. 18. Win king. Contraction. Winking,
Experiment II . Occipitofrontal exposure.
Fig. 19. Winking.
Fig. 21. Winking.
Fig. 20. Contraction.
Fig. 22. Contraction.
Fig. 23. Winking.

P1. IV CASE K . E . I,.
Experiment I . Ritemporal exposure.
Fig. 24. Fig. 25. Fig. 26. Winking. Contraction. Winking.
Experiment II . Occipitofrontal exposnre.
Fig. 27. Winking.
Fig. 29. Winking.
Fig. 28. Contraction.
Fig. 30. Contraction.
Fig. 31. Winking.

less marked in the upper part than on Plate 4 (Fig. 28), and the shadow of the left sac is broader in the lower part than in the upper. The duct on the right side also appears as on Plate 3; on the left, it is not visible.
Plate 6. Contraction. (Fig. 30). Almost identical with Plate 4 (Fig. 28).
Plate 7. Winking. (Fig. 31). On the whole like Plates 3 and 5 (Fig. 27 and 29).
Comnient: On contraction, the shadows of both sacs are diminished, both in the sagittal and _frontal diameters, while there appears on the right side a simultaneous ex- pansion of the upper part. The right duct evidently be- comes compressed, while conditions on the left are more
/difficult to interpret. In profile, the shadow of the left duct appears to become narrower and less dense on con- traction, but it does not fill out again on winking. This is possibly due to the subject’s lying on his side. The opaque inaterial which on contraction has been moved towards the nasal opening of the duct can not so easily return, and possibly some of it has already run down into the nasal cavity. In occipitofrontal exposure there is on con- traction the slight indication of a shadow in the left duct, while in winking nothing is visible. Evidently some mate- rial is pressed out from the sac on contraction, which runs back again in winking.
. S n n i m rrry . Our roe:] tgenoglams o l the lacryinal passages thus show
that: 1. in most cases an upper, somewhat wider part, the tear
sac, can be distinguished from a lower, narrower one, the naso-lacrymal duct; and that the former in ordinary winking is usually slightly narrower in its upper part;
2. the shadow of the tear sac, when the orbicularis is forcibly contracted, undergoes a characteristic change in shape, its upper end either expanding or remaining as before, while the lower one becomes narrower, the sac thus being of equal width throughout or narrower below;

7 0
3 .
and that in rnost cases the shadow of the naso-lacrymal duct under the same conditions becomes narrower and less dense or entirely disappears. In some instances when the beginning of the duct in winking has been l'ound to contain no opaque material, contraction has caused a narrow shadow to appear in this region, which is evidently due to the fact that a siiiall quantity of opaque material has been pressed out of the tear sac. (Case I:. I < , Experiment 11; Case A. E., Experiment 11; Case I<. E. L. , Experiment 11). This shadow has, however, never been so broad or dense that its presence need contradict our supposition that the upper part ol' the duct is compressed in the forcible contraction of the orbicularis; linally, when the orbicularis is no longer strongly con- tracted, the shadow of the tear sac reappears with a narrowing upper part as described in 1, while the upper part of the duct not seldom becomes refilled with opaque in a terial .
The changes here described are so constant and typical that one can see immediately whether an exposure of winking or of contraction has been made. And this is so in spite of the fact that the various plates representing the same action in one and the same case are not exactly alike. The difyeren- ces are due, partly to the fact that it is impossible always to make the exposures in exactly the same diameter, and partly to the fact that there may be differences in the com- pleteness of filling with the opaque material. This would be a serious source of error which might easily jeopardize the value of the investigations, if the changes observed were not, as already stated, so constant and typical, that they give a guarantee for the slight importance of these errors. Inasmuch as the changes in shape are shown in both the sagittal and the frontal diameters, they can probably be explained only as a decrease of the space in the lower part of the sac and the upper part of the duct, the opaque material being thereby

71
displaced in the direction of least resistance, viz., to the upper part of the sac or the lower part of the duct, or in hoth these directions.
Since no striated muscle Iibers are found in the parts coin- pressed, the change in shape must be tlie result of extraneous pressure, which can hardly be any but the increased pressure in the orbita when the eyelids in forcible contraction seek to force the bulb inwards. The orbital content is then pressed against the fossa sacci lacrymalis, which has the efyect described on the sac and duct. The dif€erent eflects 011 the upper and lower parts of the sac are probably, due to the protection accorded to tlie former by the ligainentum palpebrale internuni, which, just because of the contraction, is quite taut, and thus prevents the compression of the upper part of the sac.
€f, by studying dissection material, one desires to find out how large a part of the duct may be exposed to the eiects of the orbital content, one finds that the distance from the top of the sac to the floor of the orbita at the entrance of the bony canal varies between 13 and 15 mm. On the roentgenogranis representing contraction, a section of the duct of which the lower boundary is at a distance of from 10 to 15 mni from the top of the sac, is found to be compressed, and this section quite certainly faces the orbita, even if the enlargement 011 the plates is taken into account (in occipito- frontal exposures, this enlargement is about 10 : 9).
In order to be still surer that this region of the duct really may be influenced by pressure from the orbita, we have made the following experiment. In Case F. K., after filiing with lipiodol as usual, we made occipitofrontal exposures with the tear sac lowest. In one of the exposures, the subject exercised pressure by means of a probe on the region below the liga- mentum palpebrale mediale i n the nasal, posterior direction I).
') I n a similar experiment tried in Case A. E., the probe was applied at a spot somewhat too high up, and as a result the tear sac was almost completely emptied and nothing of interest for tlie present discussion was evolved, wherefore the plates are not reproduced.

72
Plate 1 . Winking. (Fig. 32). Shows a well-iilled tear sac of the usual shape, narrower in the upper part. The duct shadow is not quite 1 mm broad in the upper part.
Plate 2. Pressure with a probe. (Fig. 33). It is evident that the pres- sure of the probe has affected the lower part of the sac and the upper part of the duct. The upper part of the shadow of the sac has been very slightly diminished, while the lower part is very much diminished; the upper part of the duct is hardly visible.
Plate 3. Winking. (Fig. 34). The shadow of the tear sac on the whole resembles that in Plate 1, and the duct is again filled in the upper part.
CASE 1'. K .
Fig. 32. Fig. 33. Fig. 34.
Fig. 32. Conditions a t the 'beginning of the experiment. Fig. 33. Pressure with a probe (a) on the region of the tear. sac.
Fig. 34. Exposure immediately after compression.
One is inimediately struck by the great similarity between the plate exposed while the subject exercised pressure with the probe, and the plates exposed during forcible contraction of the orbicularis. This simple experiment thus shows that the upper part of the duct may be influenced by forces in

73
the orbita, and is therefore a reliable support for our opinion that the compression of the lower part of the sac and the upper part of the duct, here roentgenologically demonstrated, is probably the result of an increase in orbital pressure.
13. l~oliimetrical Experinients. Our roentgenograms have thus shown that a forcible con-
traction of the orbicularis leads to a compression of certain parts of the tear sac and the naso-lacrymal duct. They give, to be sure, an indication that there is at the same time a diminution of the volume of the tear sac as a whole, but there is no definite proof of this. By the Roentgen method one can not, moreover, demonstrate possibly occuring changes in the volume of the tear sac in connec.tion with the rapid movements in winking. To show these changes, another, more sensitive method is needed, which must, in addition, arrange for an absolute exclusion of the influence of the canaliculi.
Experinien tal Techn iqiie. The subject lies on his back with the head either bent
very far back or hanging over the edge of the table, so that the tear sac is lower than the opening of the naso-lacrymal duct into the nose. After careful anaesthetizing of the eye with cocaine, a so-called gutta-percha point - a conical inslrument made of gutta-percha and used in dentistry - is introduced as far as possible into the upper canaliculus, which is thus completely tamponed. Into the lower cana- liculus, a cahnulo is introduced which is connected with a narrow glass tube. We have thus a system of two com- municating tubes, of which the one is the glass tube, hence- forth called the graduated tube, and the other, the tear sac and naso-lacrymal duct. If this system is filled with a liquid (in our experiments, physiological salt solution), the variations in volume in the tear sac will immediately produce a change in the level of the liquid in the graduated tube.

74
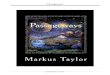
Fig. 35 gives an illustration of the preparations for these experiments. I n order that the naso-lacrynial duct, which io the erect position of the liead runs downward and slightly I~ackward, may run horizontally, a backward inclination of the head is necessary, which must iiaturally be increased
Fig. 35. General view of volurnetrical experiment.
considerably if the sac is to lie lower than the opening of the duct into the nasal cavity. In our experiments, the line connecting the forehead with the tip of the nose formed an angle of 70° with the horizontal plane. In Case F. K., we measured the angle between the line of the duct and the line from the forehead to the tip of the nose on a roentgenogram on which the duct had been made visible by filling with contrast. We found this angle to be 29O in this case, and it

75
is evident from this that the angle which the naso-lacryiiial duct formed with the horizontal plane in this case was about 40' during these experiments. A s the subjects have always had the head bent back to the same degree during the ex- periments, this calculation should afford a satisfactory guarantee that the tear sac in all cases occupied a position lower than the opening of the duct into the nose.
The cannula introduced into the lower canaliculus (Fig. 36), which had an outer diaineter of 0.75 mm, and which, hegin-
Fig. 36. ning at the point, was carefully gra- CaI111lU graduated duated in millimeters, was bent in two
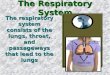
angles, so that it should not during the experiments interfere with the movements of the upper lid. The free opening of the cannula was joined by means of a thin rubber tube (see below) to a flexible, finely bored, leaden tube one decimeter in length. This in its turn was joined by means of another rubber tube to the graduated tube which was supported on a tripod. Into this connecting rubber tube a T-shaped tube was introduced, the free end of which was joined to a burette, also supported on the tripod. In Fig. 37, a diagram is given of the tear-conducting passages and their connections with the graduated tube; a and b are pinch clamps to shut off the flow, c is a tap for the same purpose. The rubber tubes were, with the exception of the one con- necting the cannula and the lead pipe, thick-walled tubes with a lumen about 1 1 / 2 mm in diameter. As a measuring tube we used an ordinary 0.1 c. c. pipette, graduated in 100 lines, the distance between each two lines being 2.25 mm. We intentionally selected fine-bored rubber and glass tubes so that the possible movements of the tear sac should have as small a mass of liquid as possible to work upon.
To find a suitable manner of connecting the end of the cannula with the end of the connecting tube was no easy matter. In our earlier experiments, not reported, we drew the end of the vacuum tube over the outer end of the can- nula. But this arrangement had two disadvantages. In the
in millimeters.

first place, the movements of the lower lid were somewhat affected, and in the second, they caused pendular movements
G
I
Fig. 37. Diagram of volumetric experiment.
a and b pinch clamps; c tap. C caiiiiula; G P gutta-percha-point; L lead tube: B burette for refilling;
G graduated tube.
in the rubber tube, movements which led to fluctuations in the liquid in the graduated tube. This last source of error was avoided by introducing into the tube system the leaden tube mentioned above, which was fastened by adhesive plaster

77
to the forehead. The cannula was connected to this tube hy means of a thin rubber tube in such a manner as to leave a space of only 1 mm between their ends, and this arrange- ment allowed the subject, after some practice, to carry out fairly unobstructed movements of winking, an important consideration in these experiments. We also ascertained that intentional movements in the joint between the cannula and the leaden pipe led to no fluctuations in the liquid in the graduated tube.
After the cannula had been introduced into the lower canaliculus, a opened, and b closed, the liquid was poured into the tube-system by opening the tap of the burette. The absence of a flow from the burette implied the presence of some obstruction in the system, which was usually due to the fact that the point of the cannula pressed against the walls of the canaliculus or tear sac, and this was corrected by changing the position of the cannula. After closing a and opening b, the graduated tube became entirely filled with liquid, after which c was closed. After a had again been opened, the liquid in the graduated tube sank - but only when the passage was free - to a point a few centimeters higher than the point where the opening of the naso-lacrymal duct was computed to be, the reason for the difference in level being the capillary force in the narrow graduated tube, which force, as experiment has shown, can raise the liquid a distance of from 4.2 to 4.5 cm in this tube.
There was in each winking, a moment's cessation in the process of sinking of the liquid in the graduated tube. When the liquid had ceased sinking and remained at a level which was constant except for oscillations occurring in connection with winking or other movements of the eyelids, the experi- ment was begun. When there appeared any obstruction for the passage of the liquid, the oscillations mentioned would immediately cease, a fact of importance, as it showed that displacement of the cannula, caused by motion of the eyelids, and the movements between the cannula and the leaden tube alone produced no visible oscillation. This we further demon-

78
strated by causing exagerrated movenients of the cannula or tapping the leaden tube with the finger, while the subject kept his eyes closed ; these manipulations produced no oscil- lation. One of our films illustrates this control experiment. The syiichronisin of the oscillations in the graduated tube with the movements of the eyelids, as well as the proportio- nalism between the size of the waves and the intensity of the orbicularis contraction (see below), also serve to justify the following assertion: the changes of volume which are evidenced by the movements of the meniscus in the graduated tube are changes occurring within the lacrymal passageways, and have a definite relation to the different movements of the eyelids, viz., winking, closing, or strongly contracting them.
The changes of volume in the lacrynial passages, which produced the oscillations, have evidently produced oscillations in the naso-lacrymal duct as well. Probably in the course of the experiments, some slight quantity of liquid ran over into the nasal cavity, which led to a slight sinking of the level of the liquid in the graduated tube in the course of the more prolonged experiments. When this was found to have occurred, more liquid was immediately introduced into the tube-system. One might suppose that a gap between the cannula and the lower canaliculus might be responsible for the decrease in the liquid, but this is not likely. The eye was well exposed to inspection, and we would immediately have seen any liquid that escaped from the lower punctum lacrymale. This we sometimes observed in connection with manipulations of the cannula, but not otherwise.
In order to find out to what extent we had managed to exclude the influence of the canaliculi, we have in all cases tried to measure their length. For that purpose we introduced a narrow probe, graduated in millimeters through the cana- liculus until it was felt to touch the medial wall of the tear sac. The distance was read off in this position, the contact with the wall of the sac being as light as possible. The figure obtained of course gives the length of the canaliculus

79
plus the frontal diameter of the tear sac at the level of the inner opening of the canaliculus. It is possible that we might have obtained too high a figure as a result of the friction between the probe and the wall of the canaliculus, which might have led to a stretching of the latter, but we have in every way tried to eliminate this source of error. The figures which we have obtained are listed below, a detraction of 2 mm having been made, which is our estimate, based on the roentgenograms, of the frontal diameter of the tear sac.
Length in mm Case F. K. . . . . . . . 8 9-10 Case K. 0. G. . . . . 9 11 Case A. S.. . . . . . . . 9 11
The figures obtained agree fairly well with Chose given in reference books and monographs on the subject, viz., 7 to 10 mm.
Upper canaliculus Lower canaliculus Length in rnm
Report of Experiments. The experiments have shown that all contractions of the
orbicularis led to a distinct rise in the level of the liquid in the graduated tube, a rise which quite plainly coincided with the lowering of the upper eyelid. The movements of the meniscus in the graduated tube were studied by means of a binocular magnifying glass. In the table below, the rise OP the meniscus on contraction is recorded in millimeters, but it should be mentioned that its motion during winking was too rapid to allow of any exact reading. Only a few readings are given in each case, because they showed very slight variations. The distances to which the cannula was introduced into the lower canaliculus, and the gutta-percha point into the upper, the latter measure being taken when the point was removed, are also recorded in the table.
Winking was done as naturally as possible, only occasio- nally on special request. Contraction was forcible, but we had no way of estimating its intensity.

80
Case F. K., aged 25. The point introduced 9 mm into the upper canaliculus.
Cannula introduced Motion of the meniscus into the lower in in
canaliculus win king contraclion i n nim in mni in mm
11-12 m ' 12 2'12
5 about 1 about 2l/2
10 )) 1 n 2 ' / z 4 )I 1 n 2',a
Case K . 0. G., aged 25. The point introduced 7 mm into the upper canaliculus.
Cmnula introduced Motion of the menisciis into the lower in in
canaliculus win king contraction in mm in mni in mtn
8 nearly 2 6 )) 1 7 n 1 2 1
5 1
5 1
2 -3 lully 1
7' 2 1 ' / Y 2' lz
Case A. S., aged 25. The point was introduced 10 mm into the upper canaliculus. In repeated readings in winking the change in level was 1 mm. The cannula was introduced into the lower cana- liculus from 8 to 10 m m at different times.
These experiments show that the movements of winking as well as those of forcible contraction led to a decrease in volume of the lacrymal passage ways. Judging from the roentgenograms, this decrease in forcible contraction takes place in the lower part of the tear sac, and in that part of the naso-lacrymal duct which faces the orbita. Because con- traction leads to a very much greater change in the level of the liquid than the movement of winking, one might infer that the decrease in volume is in something like direct pro- portion to the force ol the contraction of the orbicularis. I1 i s then natural to suppose that the decrease in volume in

81
winking occurs at the same place as in contraction, i. e., that the changes of volume in the sac and the duct produced in winking and in contraction are not different in quality, only in quantity.
The table also shows that the distance to which the can- nula was introduced in the lower canaliculus did not affect the movements of the liquid. This seems at first rather strange when one considers the ability of the canaliculi to transport the tears, for instance after a successful dacryo- cystorhinostomy. On second thought it becomes evident, however, that the changes of volume of the minute canali- culus, a greater or smaller part of which was occupied by the cannula, would be very slight, possibly too slight for the method which we employed to give a record of them. The introduction of the cannula into a rather large part of the canaliculus would, moreover, be a hindrance for the function of the part which was free. Nor is it probable that any importance can be attributed to the circumstance, observed in Case F. K., in which upon removing the point in the upper canaliculus, there was found to be no change in the movements of the liquid. For the upper canaliculus, as is well known, has not seldom a considerably smaller functional activity than the lower one. I1 might even be possible that our tamponing of the upper canaliculus was an entirely superfluous detail in the experiments. But we have not con- sidered it necessary, merely for the elucidation of this detail, which is rather beside the main question, to repeat the expe- riments, which are quite unpleasant for the subjects.
An interesting observation made in contraction .deserves to be mentioned here. As said before, the graduated tube was, for the purpose of control, filled almost completely at the beginning of the experiments, and sometimes in the course of them, whereupon, after opening the connection from the graduated tube to the lacrynial passages, the liquid in the former would sink. This sinking was seen to cease imme- diately on contraction. Not until the orbicularis was again relaxed did the sinking start anew. This shows that con-
G

82
traction caused a closing of the passage. If this Observation is compared with the observation on the roentgenograms of a more or less pronounced compression of the upper part of the naso-lacrymal duct, it becomes very probable that the upper part of the duct is really closed in contraction. That this condition does not always appear on the roentgenograms, where indeed sonietimes a duct which has not given any shadow before, comes into view in contraction, may be due to the circumstance, referred to on p. 59, that the tear-con- diicting passages in the making of the roentgenograms were working under non-physiological conditions, the greater part of them being filled with the rather viscous oil which, be- cause of the position of the head, could not be pumped away by the natural mechanism. Neither in normal conditiens, nor in the volumetrical experiments, in which the cannula in the lower canaliculus allows the liquid to run back in the direction of the graduated tube, is the closing of the passage which we assume, prevented. Winking, as mentioned on p. 77, produced only a momentary cessation in the sinking of the meniscus, which indicates a process qualitatively similar to, but, as was to be expected, quantitatively different from that in contraction.
Cinemdogrnphic Records. We have indicated in the foregoing our opinion that the
different movements of the eyelids have an effect on the tear passages, which is different only quantitatively, not qualitatively. The short space of time occupied by each movement of winking, however, does not permit of any satisfactory analysis of the effects of the different phases of winking. In order to study these conditions in the most objective manner possible, and thus to escape the criticism which has been justly directed against most of the earlier investigators, we have made cinematographic records of some of the volumetrical experi- ments described above. To the liquid (ordinary physiological salt solution) in the tube-system, fluorescin was added i n such quantity as to make the liquid visible on the photo-

83
graphic plate. A cinematographic record made and shown with ordinary rapidity would not of course increase the time for making observations, but from the progress of events recorded on the film, we could select individual pictures to be enlarged for further study.
Fig. 38 (PI. 19, a to h, gives the enlargements of the series of pictures representing one movement of winking (Case F. K.), The camera made 20 exposures every second, and thus the interval of time between each two exposures was 0.05 sec. The process of winking occupied in all 0.4 sec. The lowering of the upper lid occupied 0.05 sec.; the eyelid remained in the lowered position for 0.15 sec.; lifting it occupied 0.2 sec. For comparison we give the figures of Garten and uaiz Gilse. In his investigation of winking, Garten recorded a duration of from 0.075 to 0.09 sec. for the lowering; the pupil was entirely covered by the upper lid for from 0.17 to 0.20 sec.; the lifting took from 0.14 to 0.18 sec.; the entire movement of winking occupied from 0.31 to 0.44 sec. Van Gilse ascer- tained the duration of one movement of winking by means of cinematographic records. The values he obtained were between 4/3a and 4/ao second. Lowering the upper lid took from ‘ / a 0 to V z o second; lifting it took a slightly shorter time. Between these two movements, the lid was motionless for ‘/:D
second. The movements of winking probably vary rather much in
duration, and it is possible that the arrangement of apparatus in our experiment somewhat retarded them.
These pictures thus show the following relations between the movements of the upper lid in ordinary winking and the meniscus in the graduated tube; with the sinking of the lid there occurs a rise in the meniscus, with the raising of the lid, a falling of the meniscus. The movements of the meniscus, however, lay slightly behind those of the eyelid, which no doubt is due to inertia, the transference of the effect of the contraction via the contents of the orbita to the tear passages, the friction in the graduated tube, etc. The meniscus thus continues to rise the entire time during which
6”

the eyelid is kept still, and it reaches its highest point just as the eyelid again begins to rise (Fig. 38 e), after which it rapidly falls to the level from which it started. These con- ditions are also found in our other numerous cinematographic records of winking.
Fig. 39 (PI. VZ), a to d, gives four out of a series of pic- tures taken in contraction (Case K. 0. G.), which could not, for lack of space, be reproduced complete. Here we also see that the meniscus rises when the upper lid is lowered, and sinks when it is raised. The rise of the meniscus is much greater than in winking. Here, also, the same conditions are found in other records. That the meniscus at the end of the experiment is at a somewhat lower level than a t ' the begin- ning is probably due to the fact that some of the liquid was emptied into the nasal cavity during contraction.
Experiment on a Pathological Lacrgmal Passagewag. We have performed a somewhat modified, volumetrical
experiment on a patient having stenosis of the naso-lacrymal duct and a large atonic tear sac. After the patient had been placed in a recumbent position and the cannula introduced into the lower canaliculus, the tear sac was filled with liquid from the burette. When the liquid began to run out of the upper canaliculus, a point was introduced into it to a depth of 8 mm. After the burette tap had been closed, the full tear sac was placed in communication with the graduated tube which had previously been filled to a level a little above that of the tear sac. In every winking, we then observed a rise of from 4 to 5 mm of the meniscus in the graduated tube. In contraction, the rise amounted to as much as 10 mm. We had the distinct impression that the rise occurred imme- diately after the eyelid had started on its downward motion, even though this, for reasons mentioned earlier, was not possible to ascertain with certainty. When the patient was told to wink at a certain time, the meniscus was seen to rise immediately after ,now< had been said and winking began. When the patient was told to wink somewhat more slowly,

PI. v
Fig. 38. Cinematographie record of winking.

P1. VI
Fig. 39. Pictures from a cinornatographic record of contraction.

85
the meniscus rose while the eyelid was being lowered. In contraction, the meniscus remained at its highest point as long as the eyelids were kept forcibly pressed together, and it sank at once when the contraction of the orbicularis was relaxed. The wery lightest pressure on the tear sac was able to cause the meniscus to rise rather high.
The experiment shows that in this pathological case also, the contraction of the orbicularis leads to a compression of the tear sac. In forcible contraction, this is beyond doubt proved to be the case, and although in winking one can not with certainty ascertain in which phace of the movement the compression occurs, there does not seem to be any reasonable cause to suppose that conditions in winking are different in principle from those .in contraction. Because of purely technical difficulties (mainly insufficient lighting arran- gements), we had to abstain from making cinematographic records in this case.
Conclusions ctnd F i n d Remarks.
justified in forming the following conclusions. On the basis of our experiments we. believe ourselves
1.
2.
3.
4.
A forc ib le c o n t r a c t i o n of t h e m u s c u l u s o r b i c u l a r i s p r o d u c e s a c h a r a c t e r i s t i c change i n t h e s h a p e of t h e t e a r s a c a n d t h e w i d t h of t h e u p p e r p a r t of t h e n a s o - l a c r y m a l duc t , vis ible o n t h e roentgeno- gram. T h e u p p e r p a r t of t h e s a c r e m a i n s u n - changed o r becomes d is tended , whi le t h e lower p a r t of t h e s a c a n d t h e u p p e r p a r t of t h e d u c t a r e compressed i n b o t h t h e sag i t ta l a n d f r o n t a l d iameters . Volumetr ica l e x p e r i m e n t s have s h o w n t h a t th i s c h a n g e involves a decrease i n volume. I n w i n k i n g there is , a s s h o w n by volumetr ica l exper iments , a l s o a decrease in volume, a l t h o u g h to a s l igh ter degree. C i n e m a t o g r a p h i c r e c o r d s of t h e v o l u m e t r i c a l ex- per iments , a n d a n a l i z a t i o n of t h e v a r i o u s p h a s e s

of t h e m o v e u i e n t h a v e s h o w n a q u i t e de f in i t e r e l a t i o n be tween t h e d e c r e a s e i n y o l u m e a n d t h e m o v e m e n t s 01 t h e eyel ids , i n t h a t t h e dec rease h e g i n s s i m u l t a n e o u s l y w i t h t h e c o n t r a c t i o n of t h e o r b i c u l a r i s , a n d ceases w h e n t h e musc le is r e l axed . I n o t h e r w o r d s , i t i s t h e c los ing p h a s e of t h e niovenient of t h e eye l id s w h i c h l eads to a c o m p r e s s i o n of t h e t e a r s a c a n d t h e u p p e r p a r t of t h e n a s o - l a c r y m a l d u c t , wh ich p a r t s ex l ) and aga in w h e n t h e e y e s a r e reopened.
Although our technique has not enabled us to make ally direct roentgenological observations of the possible changes of shape in the tear sac in the movements of zninking, everything seems to indicate the probability that the changes occurring in contraction, referred to in 1, take place in winking too, although to a less pronounced degree.
It is also probable that the naso-lacrymal duct beconies entirely closed in its upper part during a forcible contraction of the orbicularis.
The compression of the lower part of the tear sac and the upper part of the naso-lacrymal duct can not, we believe, be explained otherwise than as a result of an increase in pressure in the orbita reacting on the parts which are coni- pressible. This attempt at an explanation contains nothing new; it has previously been discussed by many authors, e. g. Frieberg, Rosengren and others. The upper part of the tear sac is shown to be protected against the increased pres- sure from the orbita, and tlie protection is, as we believe, with a very great degree of probability to be sought in the stretching of the ligamenturn palpehrale internuin upon muscular contraction.
The variations in volume which we have demonstrated i n the tear sac give an indication that the tear sac is not without importance in the physiological conveyance of tears, but our results give no grounds for any definite conclusions in this question. They do not in any way oppose tlie riew, supported

87
by clinical experience, as well as by experinienls, that the canaliculi play an important active part in the transportation of tears.
We wish to express our sincere thanks to Prof. A. Ihrl6ii for permission to carry out some of our experiments at the eye clinic a t Serafitnerlasarettet (Serafimer Hospital) in Stock- holm. We are greatly indebted to Prof. G. Forssell for permitting us to carry out our roentgenological experiments in the Roentgen Institute a t Serafimerlasarettet, and to Prof. P. Haglund, who has been kind enough to place a t our disposal the lighting arrangements for cinematographic work at the orthopedic clinic.
To our young colleagues who have kindly served a s sub- jects, and to the roentgenologists and assisting nurses, who have, with a great sacrifice of time, aided us in making the roentgenograms, we extend our heart,y thanks.
To the foundation BTherese och Johan Anderssons ininnee (>)To the Remembrance of Therese and Johan Anderssone), we are greatly indebted for financial support in carrying out the investigations.
Arlt, F. Hibliogruphy . Page 135. BUeber den Tranenschlauchu. (Arch. f. Ophth., 1855, I,
Page 64. DUeber den Ringmuskel der Augenlidere. (Arch. f. Ophth.,
SZum Mechanismus der Tranenableitungu. (Wien. med. Wochen-
2nd series.)
1863, IX, 1st series.)
schr., 1865, 6.) Aubaret, Ed.
Page Y7. nRecherches sur la morphologie du conduit lacrymo-
Page 172. PEmploi de la radiographie dans la skmiologie des nasal chez l'hommec. (Bibliographie anat., 1910, XX.)
voies lacrymalesu. (Recueil d'ophth., 1911, 33.) Bailey, John.
Page 665. ))Surgical anatomy of the lacrymal sac<. (Amer. Journal of Ophth., 1924, 6.)
Bockstein, F. S. Page 288. $Endonasale Fisteln des'rranensackesu. (Russki Ophthalm.
Journ., 1924, 111. - Russisch.) Quoted on page 141, Zbl. f. d. ges. Ophth., 1926, XV

Campbell, Carter and Doub. Page 462. r Rontgen ray studies of the naso-lacrymal passageways..
(Arch. of Ophth., 1922, LI.) Dreuschnch, Fr. und Sacha, A.
Page 387. aRbntgenografie slznych cestx. - Die Rdntgenographie der Tranenwege. - (Bratislavske lekarske listy 1935, IV. - Tscheckisch mit englischer Ref.) Quoted on page 841, Zbl. f. d. ges. Ophth., 1926, XV.
Frieberg, T. IUeber die Mechanik der Tranenableitung U S W . ~ . (Ztschr. f. Aughk.,
1917, XXXVI.) Page 127. ))Om kanaliklarnas betydelse for thmekanismen(c. -
The Significance of the Canaliculi for the Conveyance of Tears. - (Hygiea, 1918, 80.)
Page 266. $Weitere Untersuchungen iiber die Mechanik der Tranen- ableitungu. (Ztschr. f. Aughk., 1918, XXXIX.)
Page 684. 8Bemerkungen zu der Diskussion iiber die Tranen- wegsphysiologiec. (Klin. Monatbl. f. Aughk., 1923, 70.)
Page 69. aEine Revision der Lehre von der Trlnenableitung und den Lidbewegungen<. (Arch. f. Anat. u. Physiol.; Physiol. section, Suppl., 1883.)
aEin Beitrag zur Kenntnis der Bewegung der Tranenfltksigkeit und der Augenlider des Menschenu. (Festschrift f. Fick, Braun- sehweig 1899.)
Gangelen, G. van.
Gad.
Page 399. ,Die Rdntgenuntersuchung der Triinenwegeu. (Ada otolaryng., 1921, 2.)
Garten. nZur Kenntnis des zeitlichen Ablaufes der Lidschllgea. (Pliigers
Arch., 1898, 71.) Gerlach.
1880. .Beitrag zur normalen Anatomie des menschlichen Augesu. Leipzig
Gilse, P. E. G. van. Page 1. nBeobachtungen Bber den Trhensackmechanisnius und
den Lidschlag. Kinematografische Registration.. (Klin. Monatbl. f. Aughk., 1922, 69.)
Graefe. A. von. Page 295. zNotiz iiber die Absorption der Thranen in den Thrlnen-
punkten.. (Arch. f. Ophth., 1854, I, 1st series.) Halben, R.
Page 61. aBeitrage zur Anatomie der Tranenwegec. (Arch. f. Ophth., 1904, 57.)

Hasner. Page 388.
Ilenke, W. Page 70. DDie Oeffnung und Schliessung der Augenlider und des
Tranensackesa. (Arch. f. Ophth., 1858, IV, 2nd series.) Page 363. SBeleuchtung des neuesten Fortschrittes in der Lehre
vom Mechanismus der Thrlinenableitungu. (Arch. f. Ophth., 1861, VIII, 1st series.)
DZur Frage iiber Thranenwege und Thranenableitungu. (Wien. med. Wochenschr., 1865.)
Henle. Page 264. aZur Anatomie der Tranenwege und zur Physiologie
der Tranenableitung.. (Zeitschr. f. rat. Med., 1865, XXXIII.) Hoewe, J. van der, und Steenhuis, D. J.
Page 671. BTranenwege im Rontgenbild nach Ffillung mit lipiodolc. (Klin. Monatbl. f. Aughk., 1925, 74.)
Hoppe. 2Untersuchungen iiber die Mechanik der Triinenableitunga. (Klin.
Monatbl. f. Aughk., 1909, 47.) Hyrtl.
Krehbiel. BTopographische Anatomies. 2 Aufl., 1853.
SUber die Musculatur der Trlnenwege und der Augenlider USW.~.
(1naug.-Diss., Miinchen 1878.) Lepage.
BRecherches sur la gouttikre lacrymo-nasale et le canal lacrymal chez l'homme et les mammifkresa. (ThQe de Bordeaux, 1909.)
Lesshaft, P. Uber den M. orbicularis orbitae und seinen Einfluss auf den Me-
chanismus der Tranenabsonderungc. (Arch. f. Anat. und Physiol., 1868.)
Meisner. Pages 465 to 470. ZKlinik und Therapie der Tranensackerkrankungenc .
(Zbl. f. d. ges. Ophth., 1923, IX.) Merkel.
SZur Anatomie, Physiologie und Pathologie der Tranenableitungs- organes. (1naug.-Diss., Erlangen 1859.)
Merkel und Kallius. SMakroskopische Anatomie des Augesu. (Graefe-Saemischs Hdb.,
2 edition, I, 1st series.) Michaescu, P.
Page 39. ,Die Rdntgenuntersuchung im Studium der Pathologie der Tranenwege.. (Clujul med. Jg. 6, 1925, "4. - Rumanisch.) Quoted on page 499, Zbl. f. d. ges. Ophth, 1926, XV.
Patton, J. Page 58. BHegional anatomy of the tear sacs. (Ann. of otol.,

rliinol. and laryngol., 1923, 32.) Quoted on page 139, Zbl. f. ci. ges. Ophth., 1924, XI.
Hochat, G. F. und Benjaniins, C. E. Page Y2 8Experimente iiber die Traoenableitung~. (Arch. f. Ophth.,
1916, XCI.)
1902.)
Hochon-Duvigneaud. Voies lacryniales chez l’adulte et le iiouveau-nea. (Arch. d’ophth.,
Hosengren, B. *). Page 388 aStudier iiver tirvagarnas komparativa fysiologiu. -
Studies in the coiuparative physiology of the tear passages. - (Hygiea, 1927, 89.)
Petit, J. L. Page 134. sSur Bstule la cry male^. (MMBmoires de I’Acad8mie des
Sciences de Paris, 1734) Scimemi, E.
Page 291. .Beitrag zur Lehre von der Tranenableitung~. (Arch. f. Physiol., 1892, 16.)
Schirmer, 0. Page 197. nStudien zur Physiologie und Patliologie der Tranen-
absonderung und Triinenabfuhra. (Arch. f. Ophth., 1903, LVl.) .Mikroskopische Aualomie und Physiologie der Tranenwegeu
(Graefe-Saemischs Hdb., 2 Edition, Part I, Vol. 1, Cbapt. VII.) Stock, W.
aPathologie der Triinenorgaiiec. (Graefe- Saemischs Hdb., 2 Edition, 1925, IX, Parts 3 and 4, Chapt. XV.)
Szily, A. v. BZur Rhlgendiagnostik der Erkrankungen der Tranenwegea.
Page 847. $Die Pathologie des TrPneiisacks und des Ductus naso- (Klin. Monatbl. f. Aughk., 1914, 52.)
Page 410. ))Die Pathologie der TrPnenwege irn Rontgenbilda. (Ber.
Page 392. BNeue Ueitrage zur Pathologie der Tranenableitungswege
Page 31. BZur Pathologie der Tranenwege in1 Hontgenbilds. (V.
(Deutsche med. Wochenschr., Febr. 1914.)
lacrimalis im Rontgenbildc.
der Ophth. Ges., Heidelberg, 1916.)
im Rontgenbilda. (Ibid. 1918.)
Mittheilung., Klin. Monatbl. f. Aughk.. 1920, 64.) Weber.
Pages 63,107,156. rUber das Triinenableitungssystema. (Ibid. 1863, I.)
’) After the cornpletioo of the investigation reported in this paper Rosengren published DStudien iiber die Trlinenableitung beini Menschen und einigen Siiugetierena (Svenska IAkaresBllskapets Handlingar - Trausactions of the Society of Swedish Physiciens - 1927).