Embed Size (px)
DESCRIPTION
Experimental Clearance of TSE Infectivity in Plasma-derived FVIII Products. TSE Advisory Committee December 15, 2006 Dorothy Scott, M.D. Office of Blood Research and Review/CBER. 4. Risk Characterization Importance Analysis (slide from S. Anderson). -. +. Questions to the Committee. - PowerPoint PPT Presentation
Citation preview

Experimental Clearance of TSE Infectivity in Plasma-derived FVIII
ProductsTSE Advisory Committee
December 15, 2006Dorothy Scott, M.D.
Office of Blood Research and Review/CBER

Importance AnalysisMajor risk drivers: Clearance, FVIII usage
Efficiency of Donor Deferral Policy
Yield of FVIII from plasma (IU/L plasma)
Quantity Infectivity in Blood (ID50/ml)
Efficiency of i.c. versus i.v. route
Prevalence UK vCJD (cases/million)
FVIII used per yr (IU/yr, person)
Log Manufacture Reduction vCJD Agent
4. Risk Characterization Importance Analysis (slide from S. Anderson)
- +

Questions to the Committee1. Based on available scientific knowledge, please discuss whether a
minimum TSE agent reduction factor, demonstrated using an exogenous (spiking) model in scaled-down manufacturing experiments, can be identified, that would enhance vCJD safety of the products.
a. If yes, what TSE agent reduction factor is most appropriate?
2. If the Committee identifies a minimum TSE reduction factor that would enhance vCJD safety what actions should FDA consider in cases when a licensed pdFVIII has a lower reduction factor:
a. Labeling that would differentiate the higher clearance products from other products;
b. Recommending addition of TSE clearance steps to the manufacturing method;
c. Performance of TSE clearance experiments using endogenous infectivity models;
d. Any other actions?

TSE Spike Plasma(e.g. – infected brain, brain subfractions, spleen) Cryoprecipitation Cryoprecipitate
(FVIII) – assay for infectivity
Cryopoor Plasma Supernatant
Assay for infectivity
TSE Clearance Evaluation: Exogenous(“Spiking Experiment”) Model

Exogenous Clearance Studies – Spiking Material
– “Ideal” spiking material• Physically/chemically replicates blood infectivity• Easy to prepare, widely available• High-titer material
– Committee discussion 9/18/06 (What would be optimal spiking material and its preparation?)
• Brain subfractions may be better than whole homogenate• Can higher titer infectivity fractions relevant to blood infectivity be
generated?– LDL//VLDL bound fraction from plasma
– Other purification methods (e.g. solublized homogenate)
– “There is no pending resolution of the physical form of [blood] infectivity”
• Spiking studies use human plasma and intermediates - highly process-relevant (animal plasma may fractionate differently)

Exogenous Experiments – Selection of TSE strains and animal model (TSEAC
discussion 9/18/06)
• Most relevant strains may be BSE/vCJD-related, but well-characterized and practical vCJD model in rodents not yet available
• Transgenic mice (PrP-transgenic for specific TSE strain) may provide greater sensitivity/shorter incubation periods) – e.g. BSE into “bovinized” mice; scrapie into “ovinized” mice
• Human TSE’s studied in “humanized” mice – continue to be developed
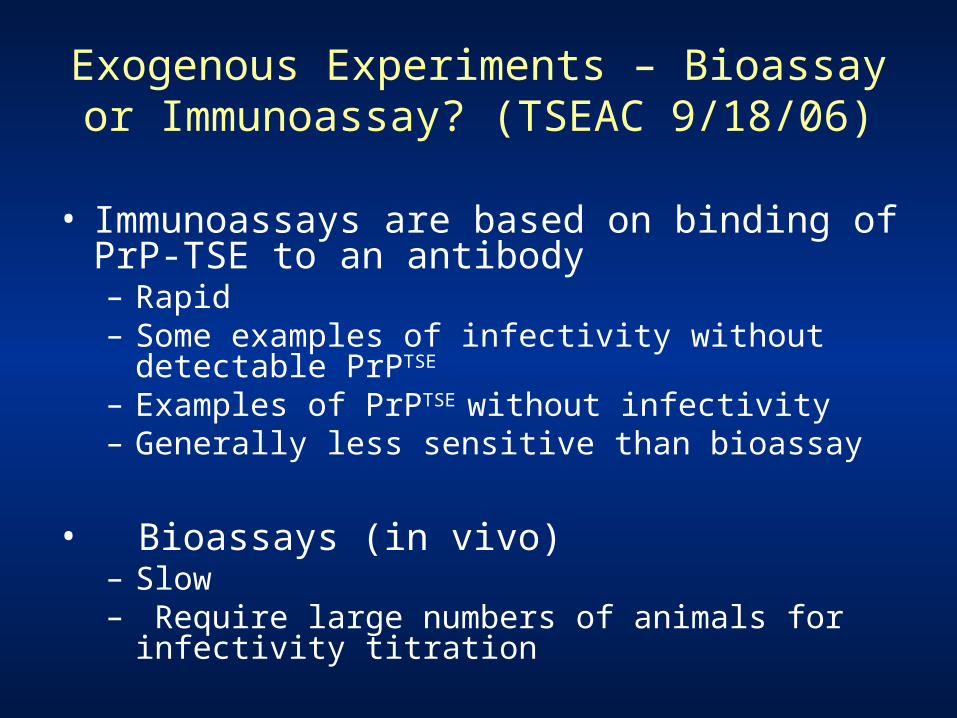
Exogenous Experiments – Bioassay or Immunoassay? (TSEAC 9/18/06)
• Immunoassays are based on binding of PrP-TSE to an antibody– Rapid– Some examples of infectivity without detectable
PrPTSE
– Examples of PrPTSE without infectivity– Generally less sensitive than bioassay
• Bioassays (in vivo)– Slow– Require large numbers of animals for infectivity
titration

Exogenous Experiments – Bioassay or Immunoassay?
• TSEAC discussion 9/18/06– Enhancement of binding assay sensitivity with
PMCA* may be possible– Replacement of bioassay with binding assays
• Would require very careful validation• Still currently important to assay infectivity
• Tissue culture bioassay models – not fully developed for use in titrating infectivity in clearance studies, but may eventually be rapid (30 day incubation)
* protein misfolding cyclic amplification

“We are never going to have the best assay. That is the nature of science. We keep moving ahead
and making things better.”
R. Colvin, TSEAC 9/18/2006

TSE Agent Reduction Factor
• What is a reasonable minimum clearance that would enhance vCJD safety of pdFVIII products?
• Viral validation analogy – how is viral safety demonstrated?
• Information from FDA pdFVIII risk assessment – sensitivity analysis for clearance levels

Viral Safety – amount of clearance• Experiments are similar to TSE clearance –
spiking of infectious virus into plasma or intermediate, and assessing removal
• Viremia ranges higher than blood infectivity range estimated for TSE’s– 4-9 Log10/ml for HCV, HIV-1, HBV– 7 Log 10/ml for HAV; 13 log10/ml for B19 virus – 2-30 i.c. IU/ml estimated for TSE’s
• TSE infectivity estimate in plasma (based on animal models): 2-30 IU/ml x 800 ml plasma = 3.2-4.4 log10 IU total
• Viral clearance usually at least for the maximum amount of virus expected + “margin of safety”

Viral Safety – amount of clearance
• Margin of safety (at least 2-3 additional logs of clearance) may be prudent because – – Manufacturing conditions cannot be identical
in every respect for every lot (critical parameters are within specified ranges)
– Viremia range could be higher than reported – Virus model is not identical to field viruses
(e.g., HCV cannot be studied due to lack of culture methods; similar model viruses are used to demonstrate clearance)

Impact of TSE clearance on mean potential vCJD risk/person/year (pdFVIII risk assessment table 5.3.A.)
Treatment interval + estimated UK vCJD prevalence
7-9 * 4-6 * 2-3
Episodic, no inhibitor, UK vCJD prevalence 1.8/106
1 in 3.2
billion
1 in 9.4 million
1 in 21,500
Episodic, no inhibitor, UK vCJD prevalence 1:4,225
1 in 100 million
1 in 105,000
1 in 159
Log10 TSE Clearance
* Available data suggests that all U.S.-licensed products are likely to have TSE clearance of > 4 log10

Question 2
If the Committee identifies a minimum TSE reduction factor that would enhance vCJD safety what actions should FDA consider in cases when a licensed pdFVIII has a lower reduction factor:
a. Labeling that would differentiate the higher clearance products from other products;
b. Recommending addition of TSE clearance steps to the manufacturing method,
c. Performance of TSE clearance experiments using endogenous infectivity models;
d. Any other actions?

Current FDA Recommendation: Labeling for Risk of CJD in Plasma Derivatives
“Because [this product] is made from human blood, it carries a risk of transmitting infectious agents, e.g. viruses, and, theoretically, the Creutzfeldt-Jakob disease (CJD) agent.”

Voluntary Labeling (based on submission of TSE clearance studies)
• In DESCRIPTION section: “Additionally, the manufacturing process was investigated for its capacity to decrease the infectivity of an experimental agent of transmissible spongiform encephalopathy (TSE), considered as a model for the vCJD and CJD agents.”– Characterizes study as investigational– Introduces the concept of models for vCJD
and CJD

Voluntary Labeling (continued)• In DESCRIPTION section “Several of the individual production
steps in the [product name] manufacturing process have been shown to decrease TSE infectivity of an experimental model agent. TSE reduction steps include [process][(logs)]), [process][(logs)], [etc.]. These studies provide reasonable assurance that low levels of CJD/vCJD agent infectivity, if present in the starting material, would be removed.”– States that clearance was observed, with specific logs
removal– Provides an estimation effectiveness in context of low levels
of infectivity

Plasma from TSE-infected animal
Cryoprecipitation Cryoprecipitate(FVIII) – assay for infectivity
Cryopoor Plasma Supernatant
Assay for infectivity
TSE Clearance Evaluation: Endogenous Infection model

Endogenous TSE studies: Relevance to Blood Infectivity
• Comparison of results from endogenous and exogenous infectivity studies suggest similar reductions for some precipitations– Limited number of endogenous studies
• Endogenous infectivity characteristics in plasma– Small size– Difficult to sediment (in its native form)– Poorly aggregated– May be lipid/plasma-protein associated

Endogenous TSE Clearance Studies
• Relevance to human blood highly likely• Limited clearance can be demonstrated because starting
infectivity is low (est. 2-30 IU/ml)– Large numbers of donor and assay animals may compensate
for low titers • Recipients – volume injectible i.c. for titration: 0.02 ml mice; 0.05 ml
hamsters• For 100 ml plasma: 5000 mice or 2000 hamsters
• Large animal models (Scrapie, BSE)• Experimental logistics - herd management, limited locations,
incubation time, availability• Scale-down logistics – dedicated pilot laboratories
• Can studies be done using large animal plasma donor with small animal assay?
• Animal plasma fractionation – equivalence to human plasma for studied clearance steps?

Questions to the Committee1. Based on available scientific knowledge, please discuss whether
a minimum TSE agent reduction factor, demonstrated using an exogenous (spiking) model in scaled-down manufacturing experiments, would enhance vCJD safety of the products.
a. If yes, what TSE agent reduction factor is most appropriate?
2. If the Committee identifies a minimum TSE reduction factor that would enhance vCJD safety what actions should FDA consider in cases when a licensed pdFVIII has a lower reduction factor:
a. Labeling that would differentiate the higher clearance products from other products;
b. Recommending addition of TSE clearance steps to the manufacturing method;
c. Performance of TSE clearance experiments using endogenous infectivity models;
d. Any other actions?