Embed Size (px)
Citation preview
QuickTime™ and a decompressor
are needed to see this picture.
Expectations and individual differences in cognitive and affective control
CollaboratorsColumbiaKevin Ochsner Ed SmithMartin LindquistEmily SternJoy Hirsch
University of MichiganChristian WaughBarb Fredrickson Steve TaylorIsrael LiberzonKen CaseyDoug NollTom NicholsJon-Kar Zubieta
MBBH Brain GroupJim RillingJonathan Cohen Bob RoseEd SmithSteve KosslynRichie DavidsonMargaret Kemmeny
One who has control over the mind is tranquil in heat and cold, in pleasure and pain, and in honor and dishonor.
– Bhagavad Gita
If you are distressed by anything external, the pain is not due to the thing itself, but to your estimate of it; and this you have the power to revoke at any moment
– Marcus Aurelius
Abraham, sacrificing his son
Iago, manipulating Othello
Structure
• What is control? – Define terms: goals, expectations, and control– Control theory and principles of self-regulation
• Brain mechanisms of expectancy– Expectations in the control of attention– Expectations in the control of pain– Expectations in the control of emotion
What is control?• Control: The use of goals to regulate a process
• Goal: A representation of an ideal state to be achieved– May change depending on current state– Two ways goals shape regulation: by comparison with feedback and/or
expectations
• Feedback: A representation of a state or process to be regulated• Expectation: A prediction about a future state of the world or self
• Control: The comparison of feedback and/or predictions with ideal states, and the use of comparison information to alter an ongoing process
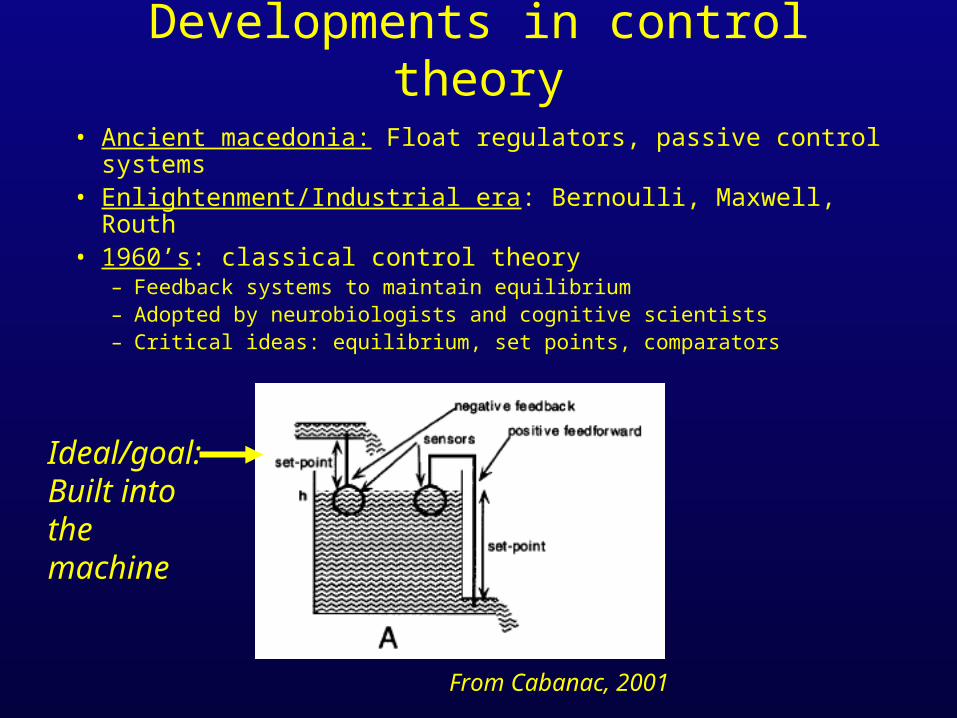
Developments in control theory
• Ancient macedonia: Float regulators, passive control systems• Enlightenment/Industrial era: Bernoulli, Maxwell, Routh• 1960’s: classical control theory
– Feedback systems to maintain equilibrium– Adopted by neurobiologists and cognitive scientists– Critical ideas: equilibrium, set points, comparators
From Cabanac, 2001
Ideal/goal:Built into the machine
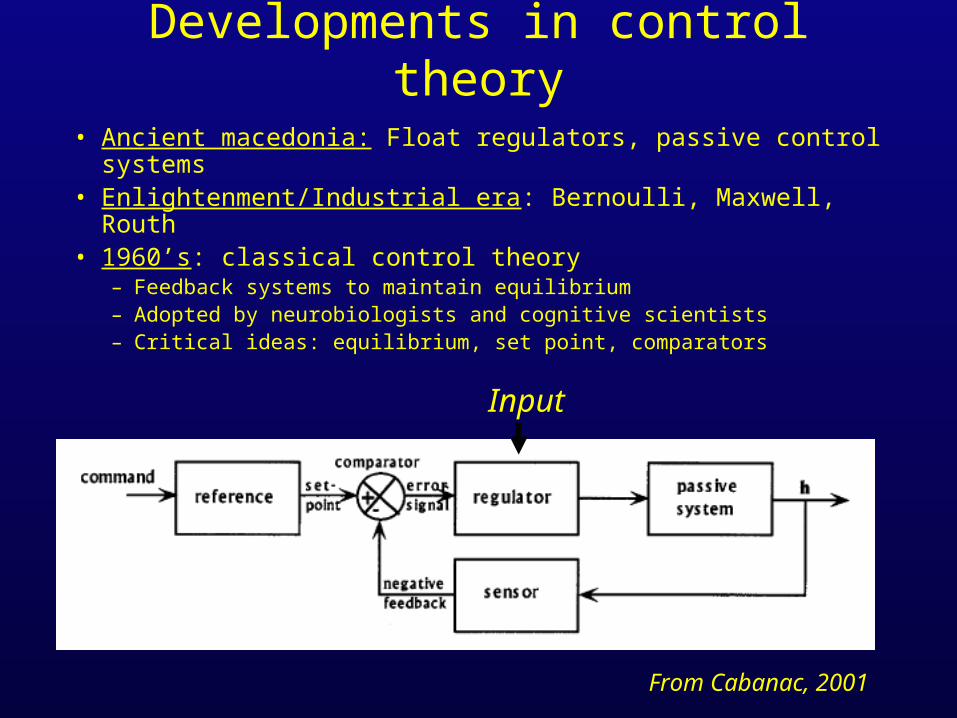
Developments in control theory
• Ancient macedonia: Float regulators, passive control systems• Enlightenment/Industrial era: Bernoulli, Maxwell, Routh• 1960’s: classical control theory
– Feedback systems to maintain equilibrium– Adopted by neurobiologists and cognitive scientists– Critical ideas: equilibrium, set point, comparators
From Cabanac, 2001
Input
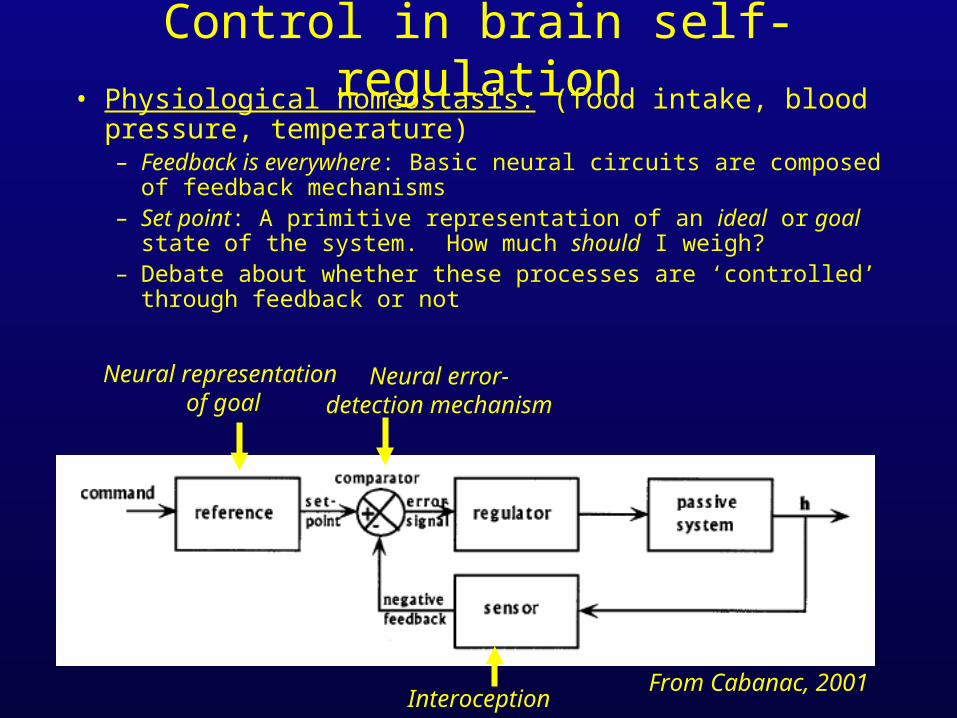
Control in brain self-regulation• Physiological homeostasis: (food intake, blood pressure,
temperature)– Feedback is everywhere: Basic neural circuits are composed of feedback
mechanisms– Set point: A primitive representation of an ideal or goal state of the system.
How much should I weigh? – Debate about whether these processes are ‘controlled’ through feedback or
not
From Cabanac, 2001
Neural representation of goal
Neural error-detection mechanism
Interoception
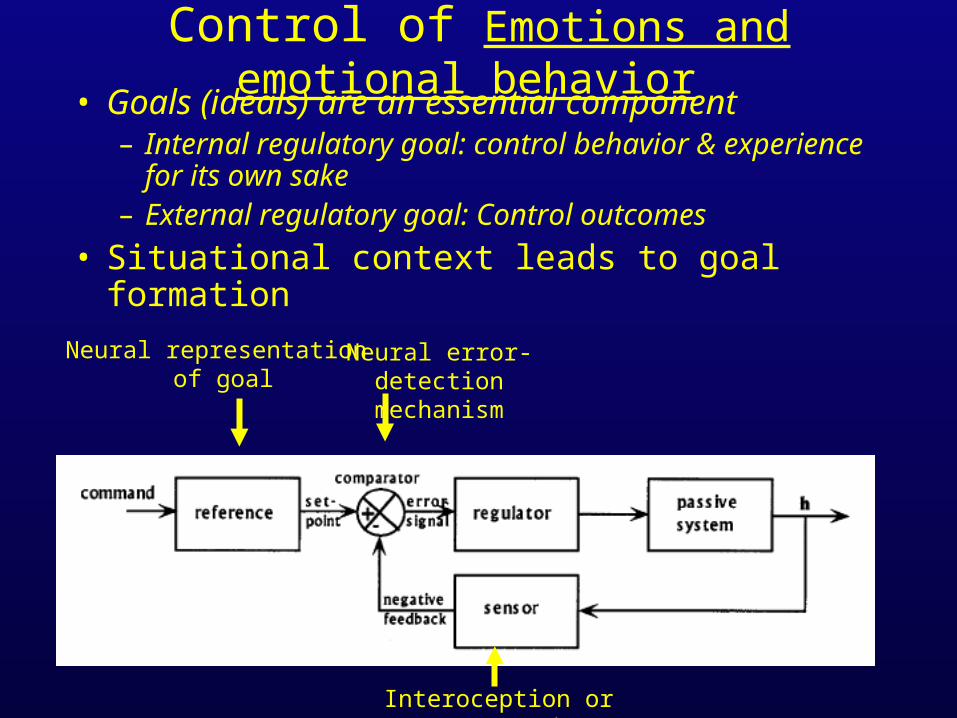
Control of Emotions and emotional behavior • Goals (ideals) are an essential component
– Internal regulatory goal: control behavior & experience for its own sake
– External regulatory goal: Control outcomes
• Situational context leads to goal formation
Neural representation of goal
Neural error-detection mechanism
Interoception or exteroception
Developments in control theory
• Ancient macedonia: Float regulators, passive control systems• Enlightenment/Industrial era: Bernoulli, Maxwell, Routh• 1960’s: classical control theory
– Feedback systems to maintain equilibrium– Adopted by neurobiologists and cognitive scientists– Critical ideas: equilibrium, set point, comparators
• Modern control theory– Adaptive control: control settings adjust to optimize performance(Analogue to strategy)– Neural networks– Borrows concepts from neurobiology– Focus on reactive control; Expectations largely absent
Structure
• What is control? – Define terms: goals, expectations, and control– Control theory and principles of self-regulation
• Brain mechanisms of expectancy– Expectations in the control of attention– Expectations in the control of pain– Expectations in the control of emotion
Control of attention
• Cognitive science/neuroscience– Use tasks that tap basic information processing– Highly controlled tasks– Identify mechanisms for voluntarily focusing
attention and selecting responses– Assumed to generalize: ‘free will’ or ‘cognitive
flexibility’
Control of attention
• Instructions: If the center letter you are about to see is an H, raise one index finger. If the center letter is an S, raise two fingers.
Control of attention
HHH
Control of attention
SSS
Control of attention
SHS

Comparing Response Interference Tasks
B
X
M
S-R Compatibility Flanker Go-No/go
blocked compatible or incompatible
responses
blocked congruent or incongruent
flankers
blocked 80% “go” versus 50% “go”
responses;Event related
analysis
Wager, T. D., Sylvester, C. C., Lacey, S., Nee, D. E., Franklin, M. S., and Jonides, J. (2005), Neuroimage
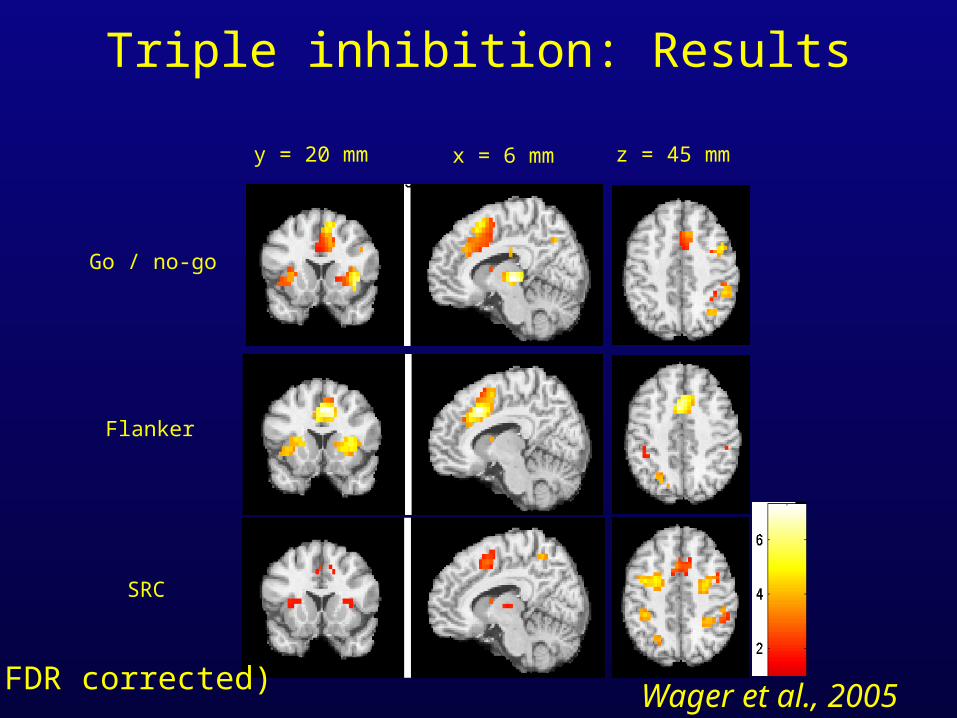
Triple inhibition: Results
Go / no-go
Flanker
SRC
y = 20 mm x = 6 mm z = 45 mm
(FDR corrected) Wager et al., 2005
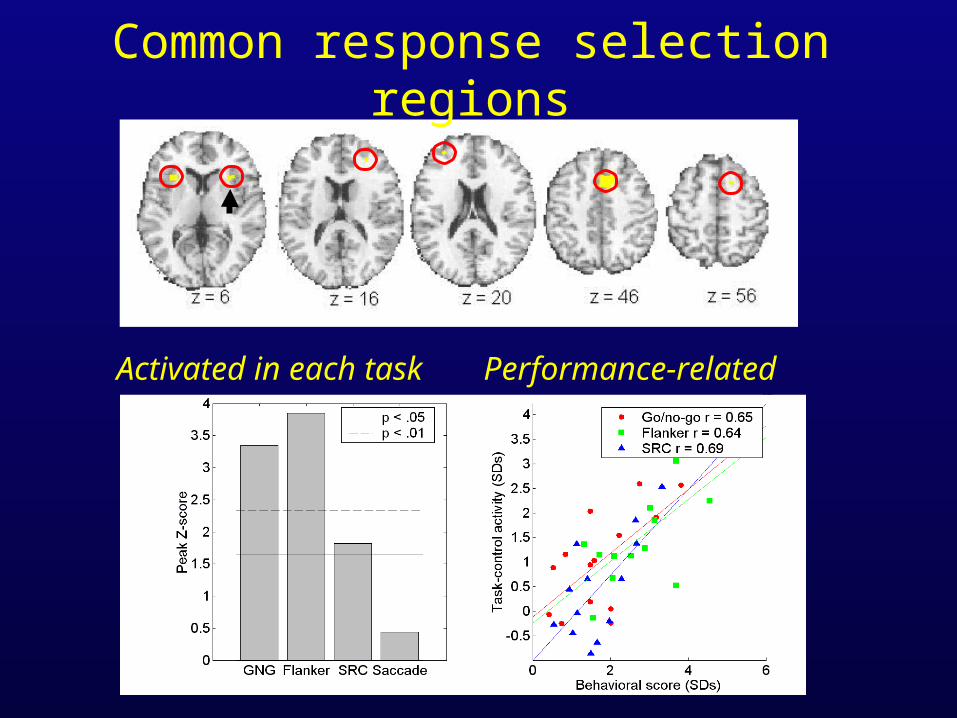
Common response selection regions
Activated in each task Performance-related
Control of attention• How did you perform the task?
– Instruction: “Respond to the center item”– Goal: make a correct response– Generate expectation: Important information in center, irrelevant
information peripheral. – Maintain expectation: activity in brain must be maintained to interact
with later stimulus processing– Bias perceptual mechanisms: Subgoal: enhance perception of center,
block periphery
– Expectancy generation = establishing a task set– This expectation of relevance, and the subsequent shaping of perception,
is ‘attention’
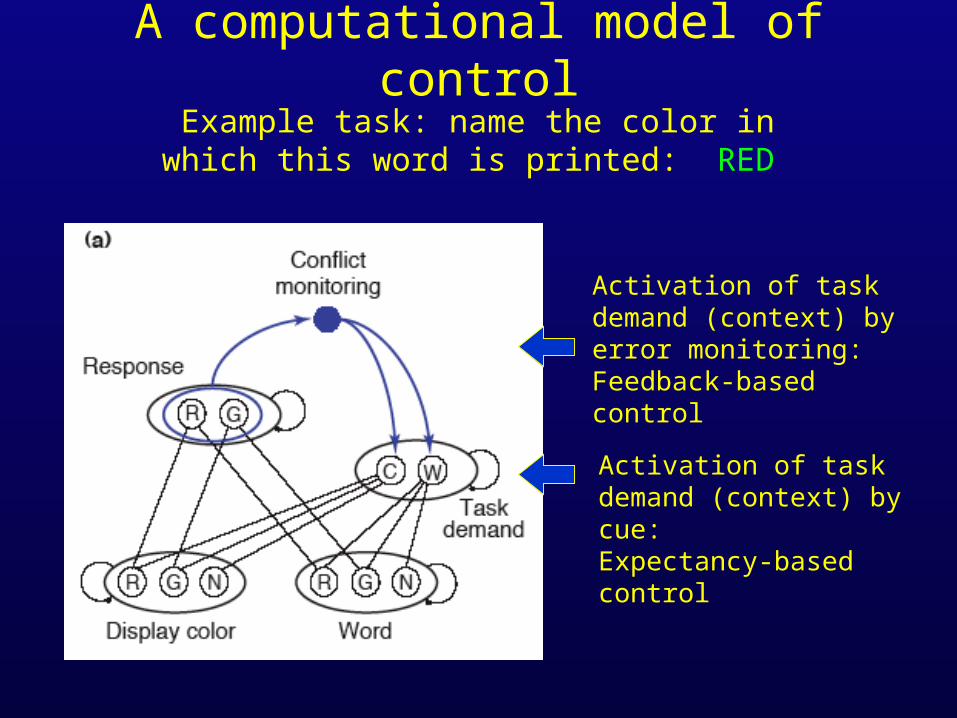
A computational model of controlExample task: name the color in which this word is
printed: RED
Activation of task demand (context) by cue:Expectancy-based control
Activation of task demand (context) by error monitoring:Feedback-based control
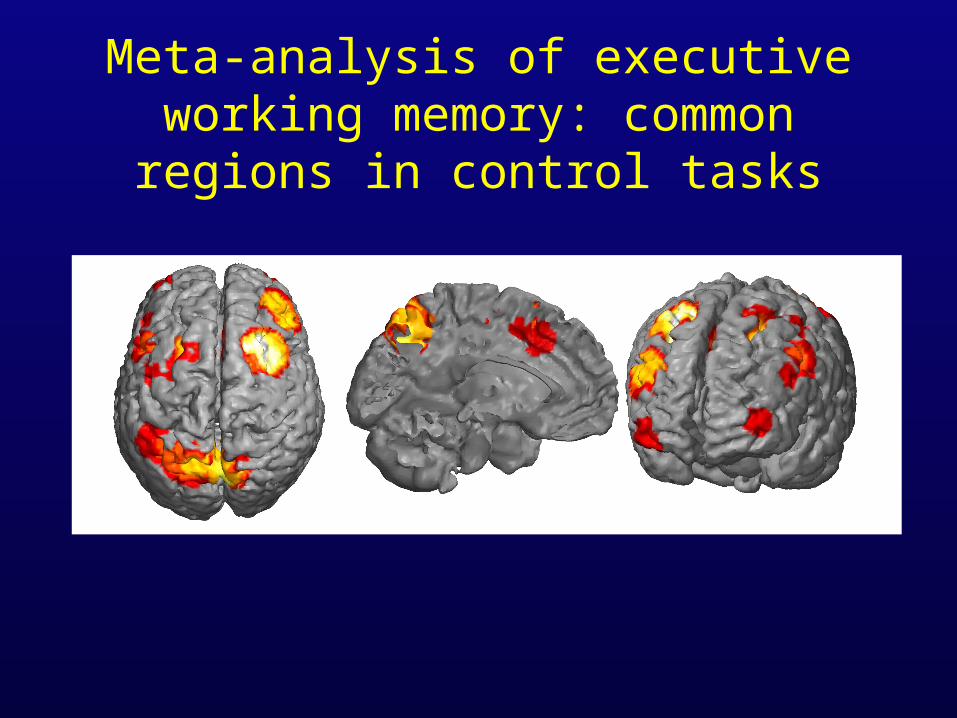
Meta-analysis of executive working memory: common regions in control
tasks
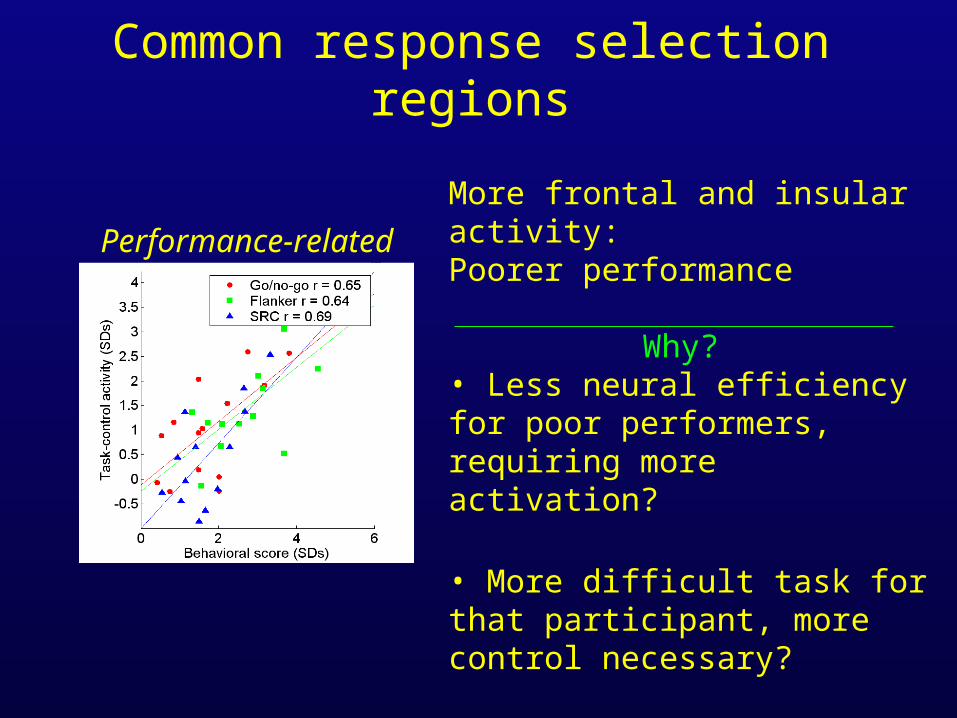
Common response selection regions
Performance-related
More frontal and insular activity:Poorer performance
Why? • Less neural efficiency for poor performers, requiring more activation?
• More difficult task for that participant, more control necessary?
• Activations reflect reactive control needed more in poor performers?
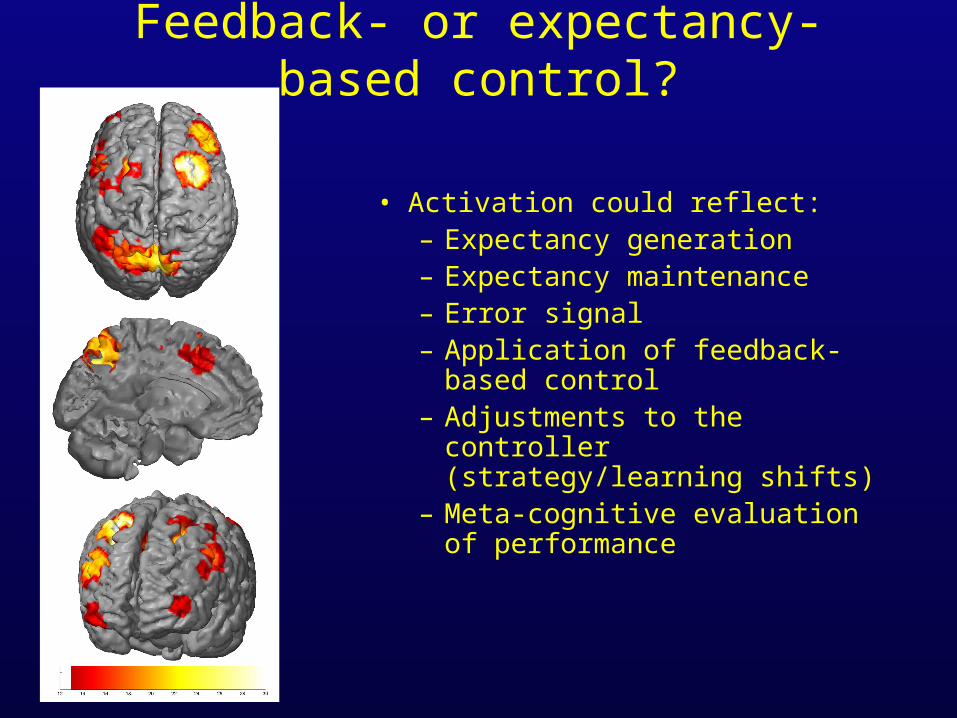
Feedback- or expectancy-based control?
• Activation could reflect: – Expectancy generation– Expectancy maintenance – Error signal– Application of feedback-based
control – Adjustments to the controller
(strategy/learning shifts)– Meta-cognitive evaluation of
performance
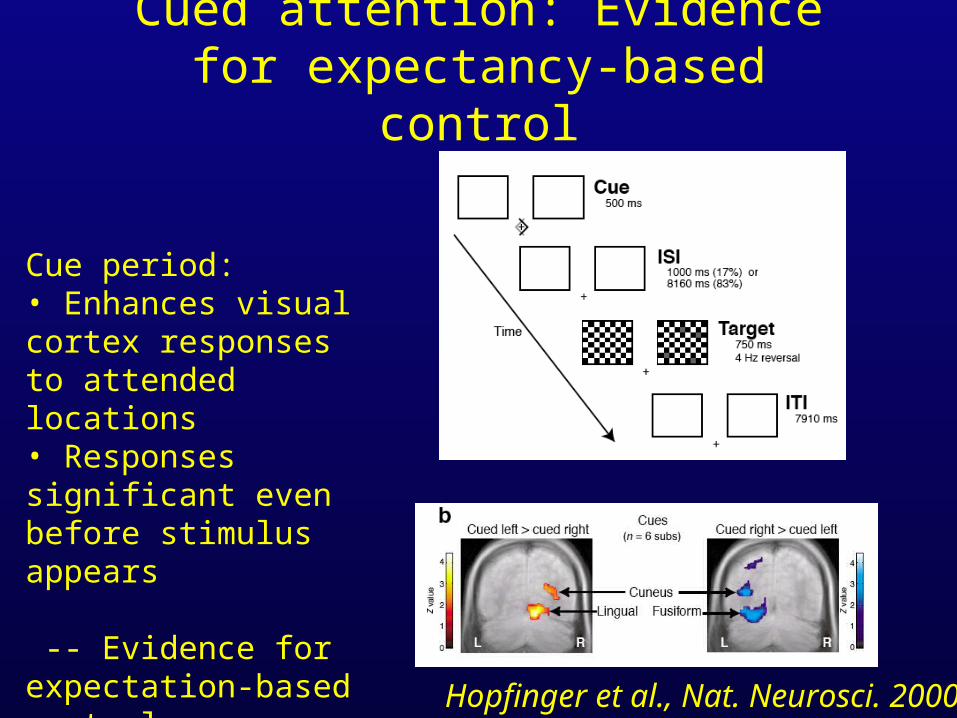
Cued attention: Evidence for expectancy-based control
Cue period:• Enhances visual cortex responses to attended locations• Responses significant even before stimulus appears
-- Evidence for expectation-based control
Hopfinger et al., Nat. Neurosci. 2000
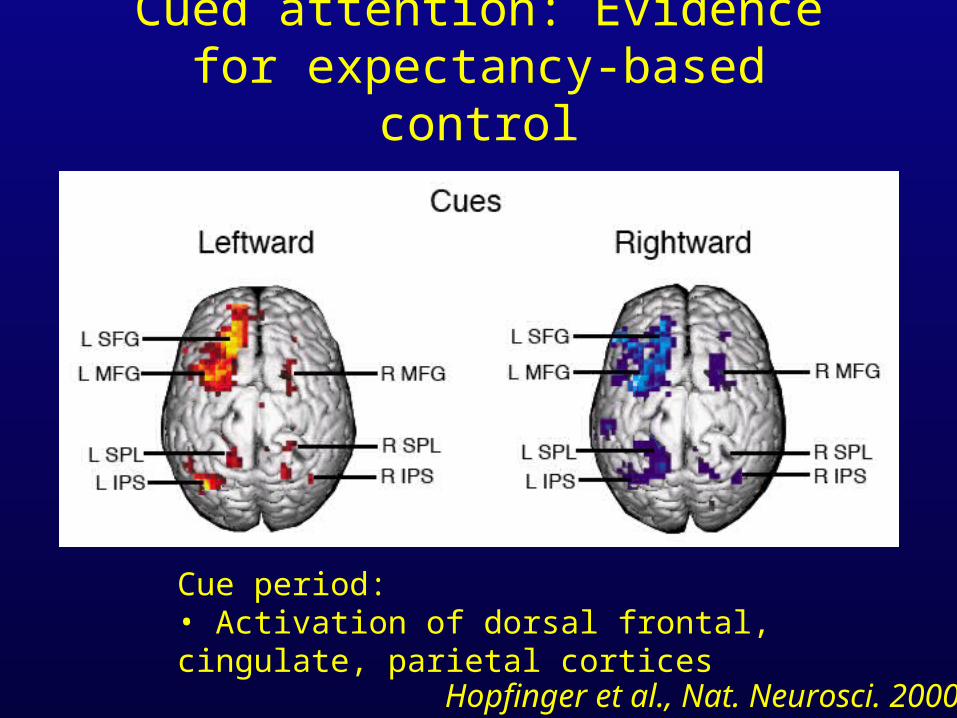
Cued attention: Evidence for expectancy-based control
Cue period:• Activation of dorsal frontal, cingulate, parietal cortices
Hopfinger et al., Nat. Neurosci. 2000
Feedback- or expectancy-based control?
• Activation likely to reflect: – Expectancy generation
– Expectancy maintenance
• But is frontal activity due to a general alerting response, or to specific task preparation?
6 s
Response:UP
Response:UP
No response
2200ms
N
W UP
W
W UP
Informative trials(P or W)
Non-informative trials
(N/P or N/W)
6 s
6 s
XControl trials
+
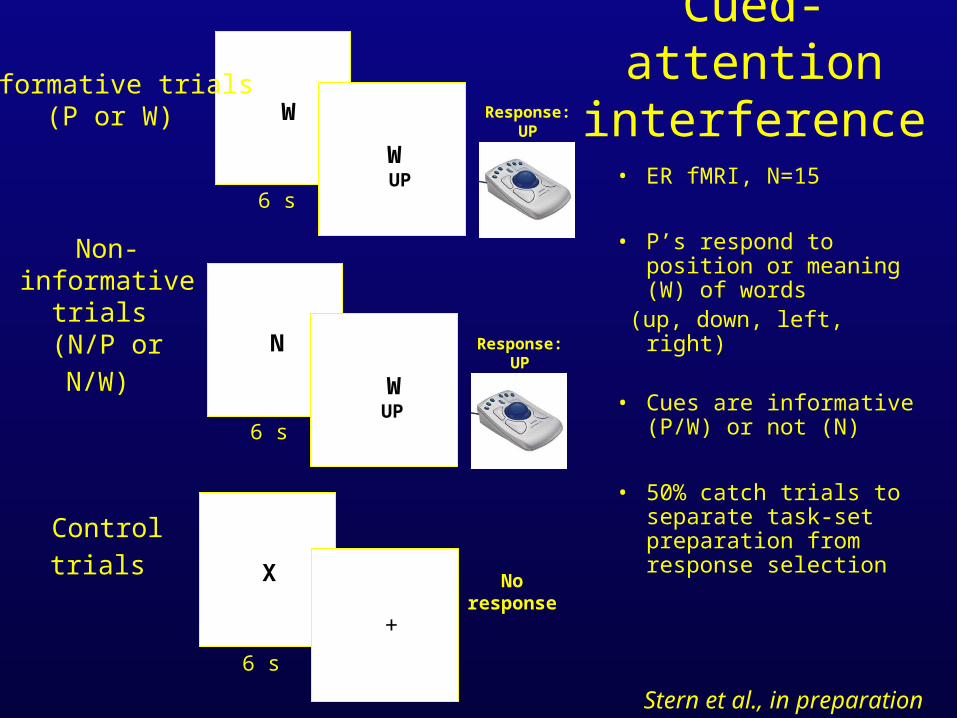
Cued-attention interference
• ER fMRI, N=15
• P’s respond to position or meaning (W) of words
(up, down, left, right)
• Cues are informative (P/W) or not (N)
• 50% catch trials to separate task-set preparation from response selection
Stern et al., in preparation
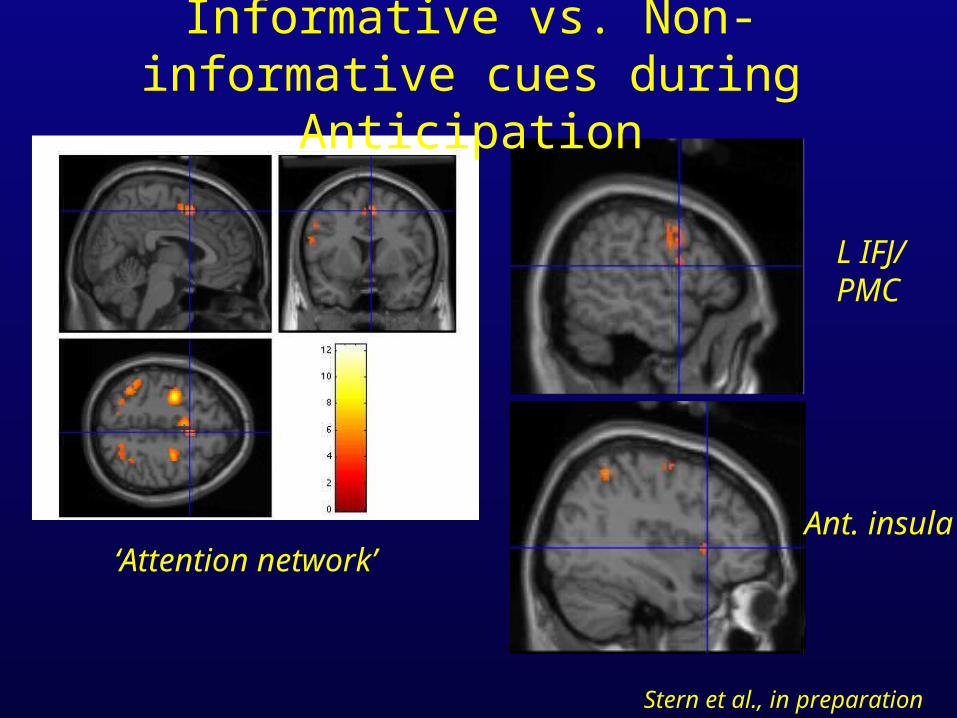
Informative vs. Non-informative cues during Anticipation
‘Attention network’
L IFJ/PMC
Ant. insula
Stern et al., in preparation
Control of attention
• Anterior prefrontal, insular, cingulate, and parietal cortices
• Commonly activated in many tasks that require ‘controlled’ response selection and attention
• All regions can be activated by expectations, even anterior insula / frontal operculum; but most frequently superior frontal regions.
• Failure to exercise expectancy-based control (poor performers) may result in reactive, feedback-based activation
Structure
• What is control? – Define terms: goals, expectations, and control– Control theory and principles of self-regulation
• Brain mechanisms of expectancy– Expectations in the control of attention– Expectations in the control of pain– Expectations in the control of emotion
Control of pain
• Does ‘cognitive control’ over attention generalize to other domains, like pain and emotion?
• Does affective information activate the ‘attention network,’ and is this information linked to affective regulation?
• Strategy: Manipulate expectancies about pain, examine neural correlates of expectancies and their impact on pain processing
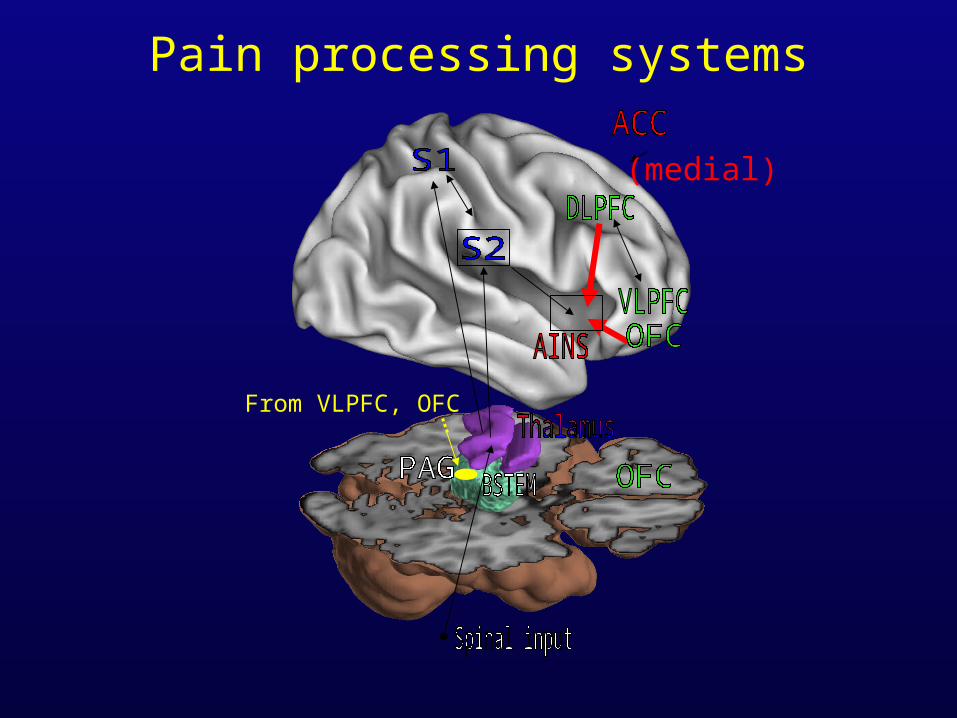
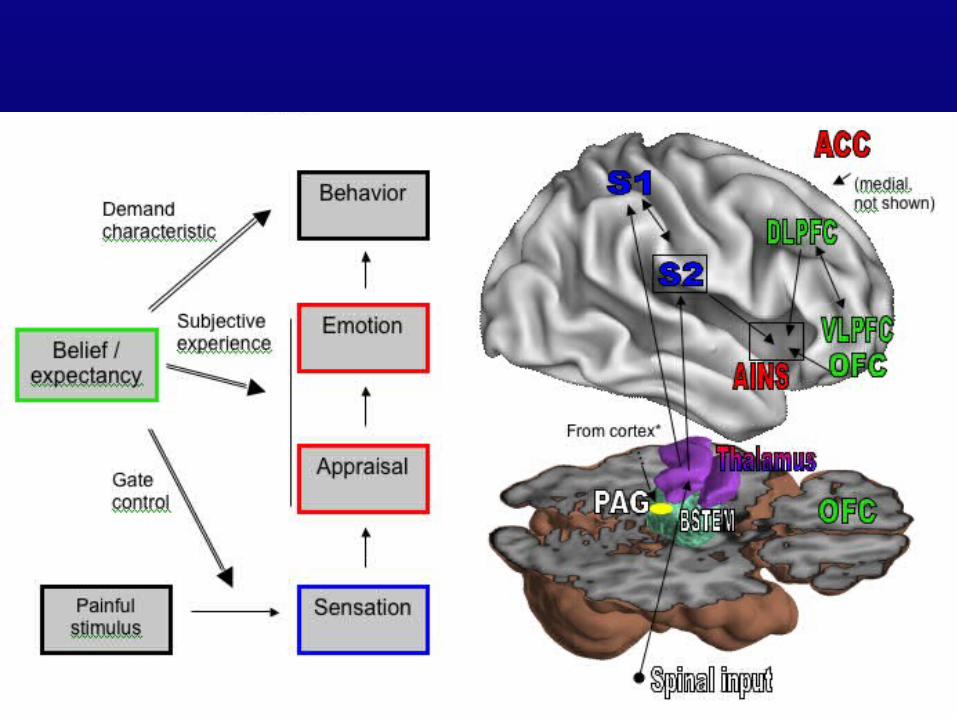
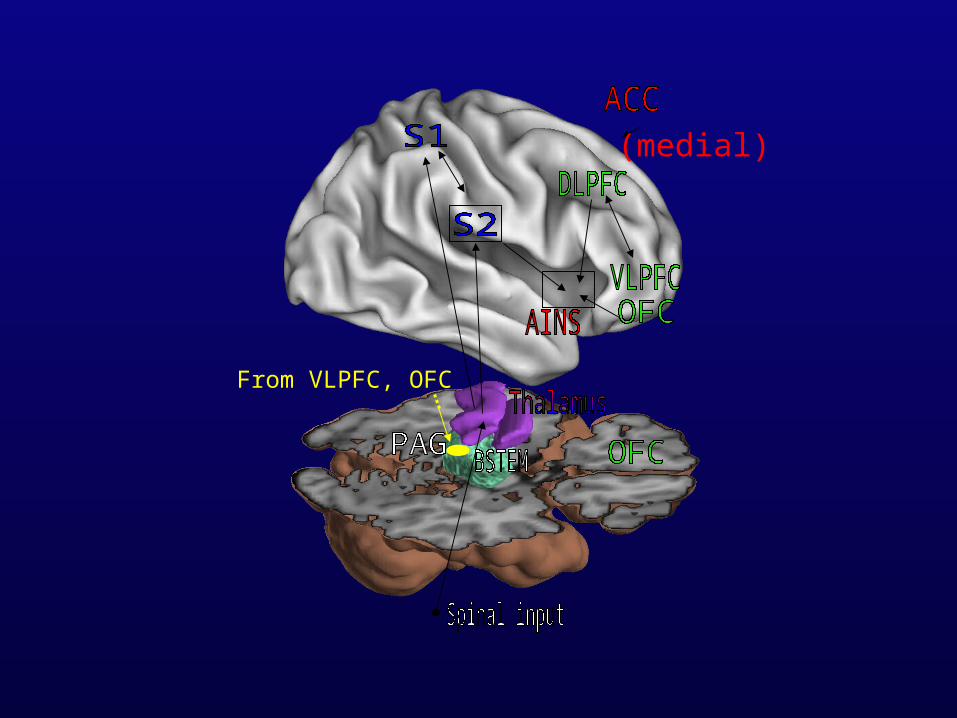
Pain processing systems
From VLPFC, OFC
(medial)
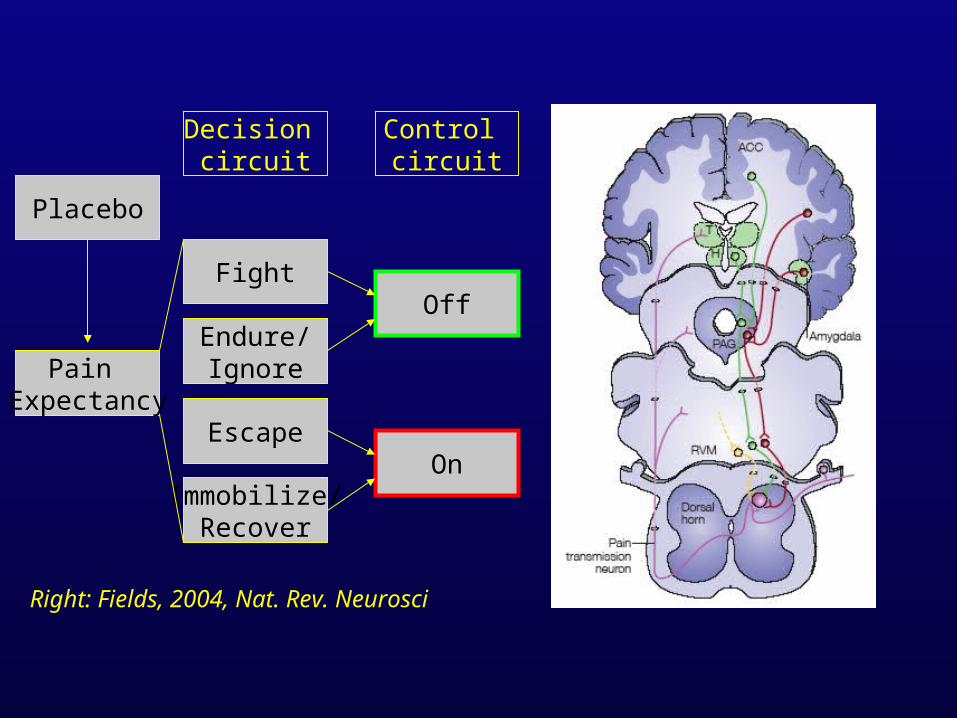
Pain Expectancy
Escape
Endure/Ignore
Fight
Decision circuit
Immobilize/Recover
Control circuit
Off
On
Right: Fields, 2004, Nat. Rev. Neurosci
Placebo
What is the placebo effect?• Placebo effect: Improvement of signs or symptoms caused by administration of a treatment with no intrinsic
beneficial effects.
• In pain, analgesia caused by a sham treatment (e.g., an injection of saline, an inert ointment)
• Placebo treatment is a manipulation of expectancy and appraisal of meaning. – A tool for studying meaning generation, mechanisms of belief, and brain-body interactions
The placebo panacea
• Over 4,000 ancient remedies, largely placebo Shapiro; in Harrington, Anne (ed.), The placebo effect
• Modern placebo effects in major clinical disorders: heart disease, arthritis, pain, depression, Parkinson’s disease
Are placebo effects real?
• Many things have been called ‘placebo effects’(Klein, Shapiro, Kirsch, Hrobartsson)
• Natural history• Spontaneous symptom fluctuation• Regression to the mean• Sampling bias• Hawthorne effects • Demand characteristics in reporting
Active mechanisms?
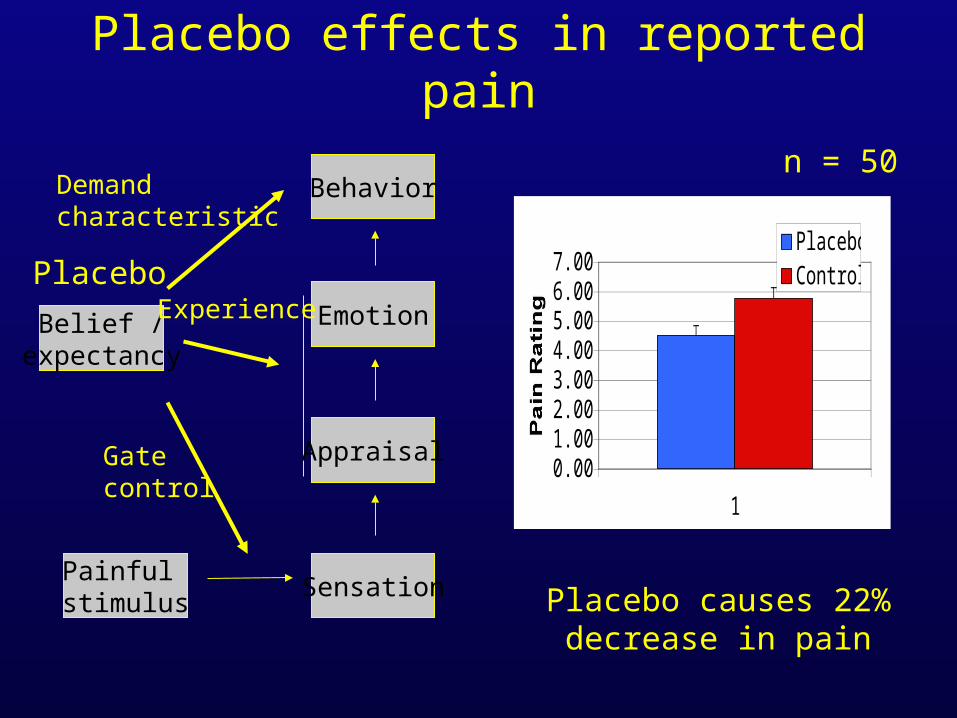
Placebo effects in reported pain
Behavior
Appraisal
Sensation
Emotion
Painful stimulus
Belief /expectancy
Gate control
Experience
Demandcharacteristic
n = 50
Placebo causes 22%decrease in pain
0.001.002.003.004.005.006.007.00
1
Pain Rating
PlaceboControlPlacebo
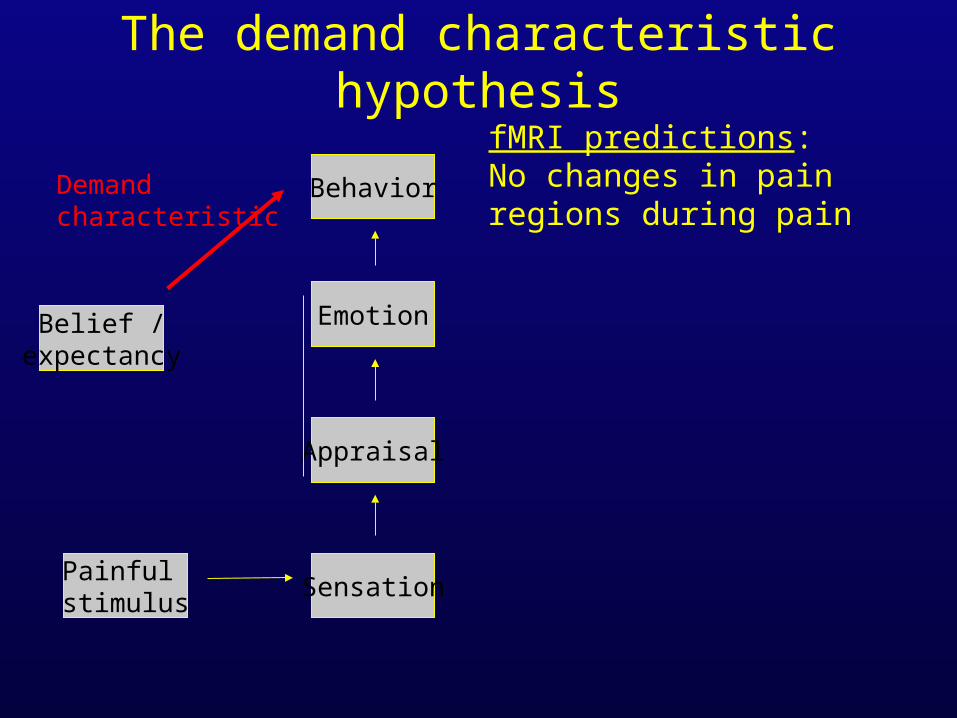
The demand characteristic hypothesis
Belief /expectancy
Appraisal
Sensation
Emotion
Behavior
Painful stimulus
Demandcharacteristic
fMRI predictions:No changes in pain regions during pain
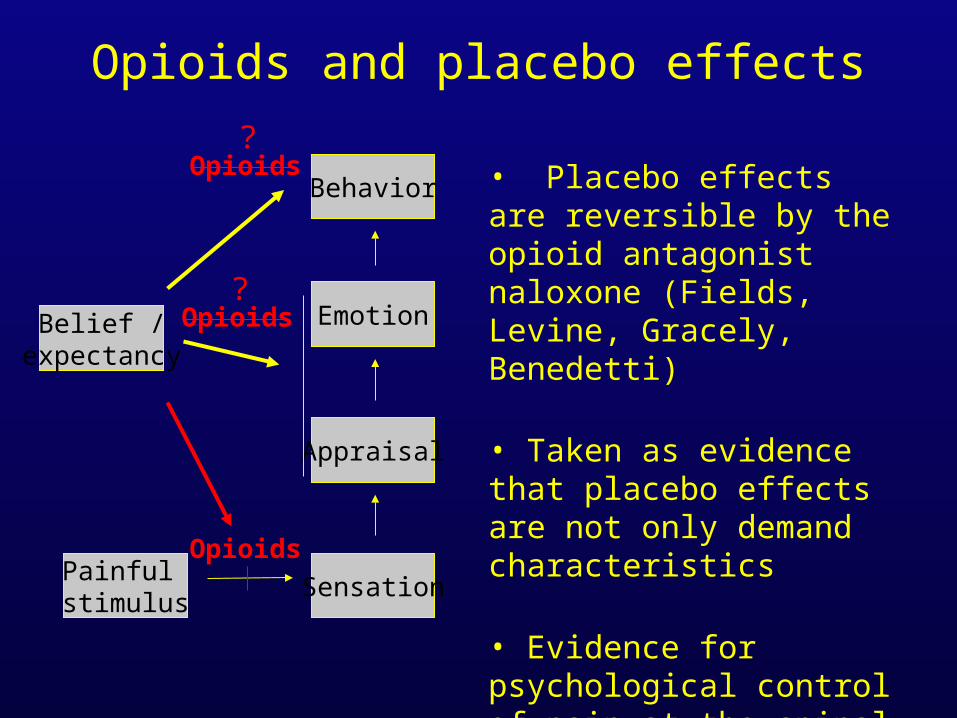
Opioids and placebo effects
Belief /expectancy
Appraisal
Sensation
Emotion
Behavior
Painful stimulus
• Placebo effects are reversible by the opioid antagonist naloxone (Fields, Levine, Gracely, Benedetti)
• Taken as evidence that placebo effects are not only demand characteristics
• Evidence for psychological control of pain at the spinal level? (Melzack and Wall, 1965)
Opioids
Opioids
Opioids?
?
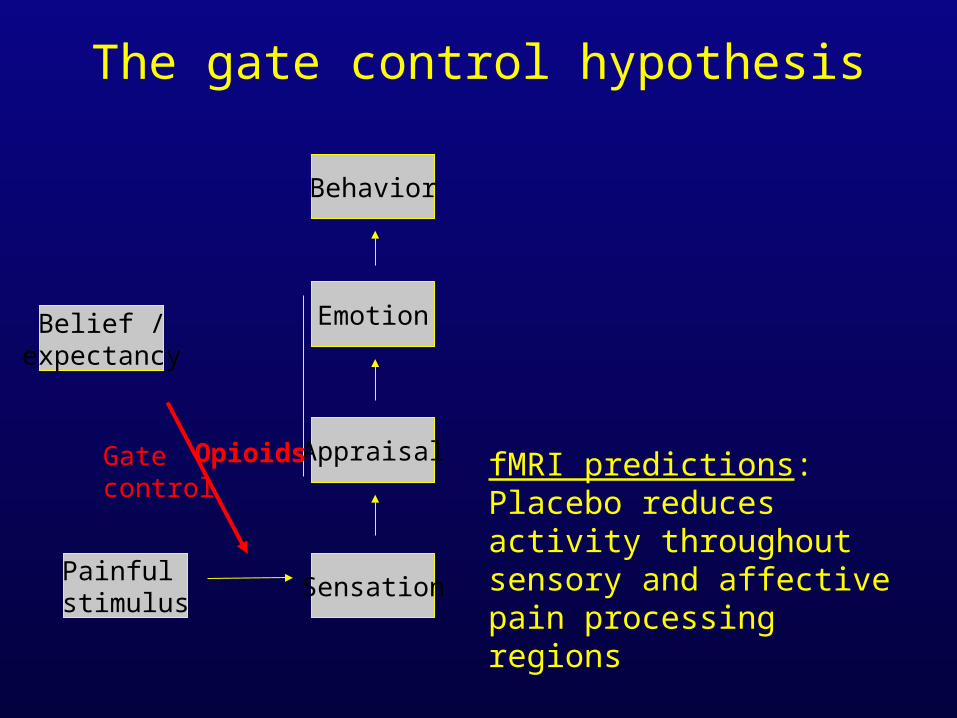
The gate control hypothesis
Belief /expectancy
Appraisal
Sensation
Emotion
Behavior
Painful stimulus
Gate control
fMRI predictions:Placebo reduces activity throughout sensory and affective pain processing regions
Opioids
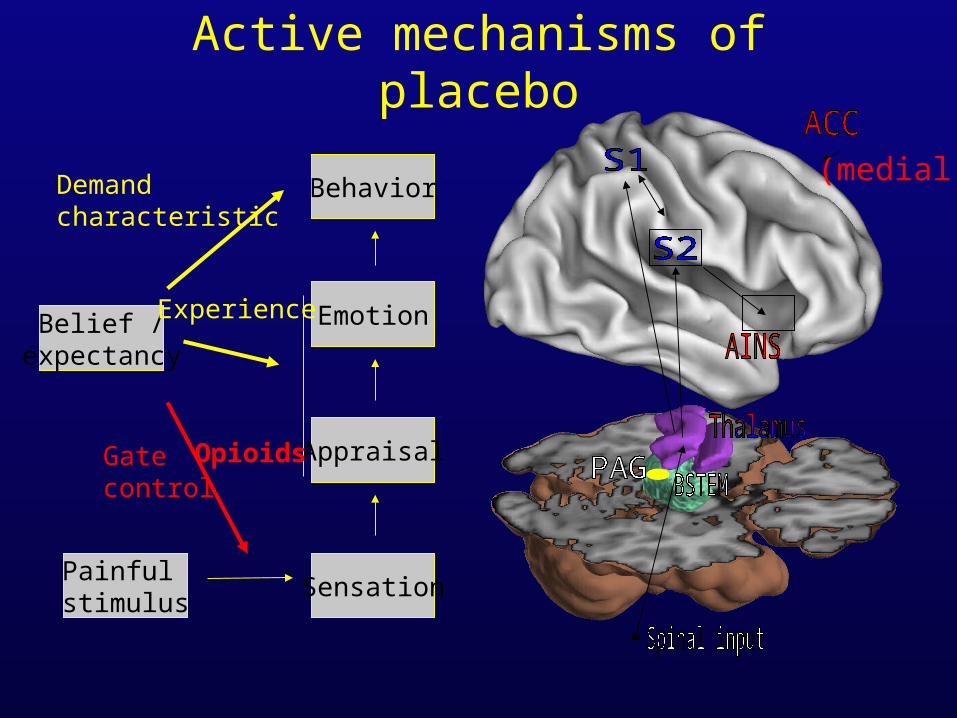
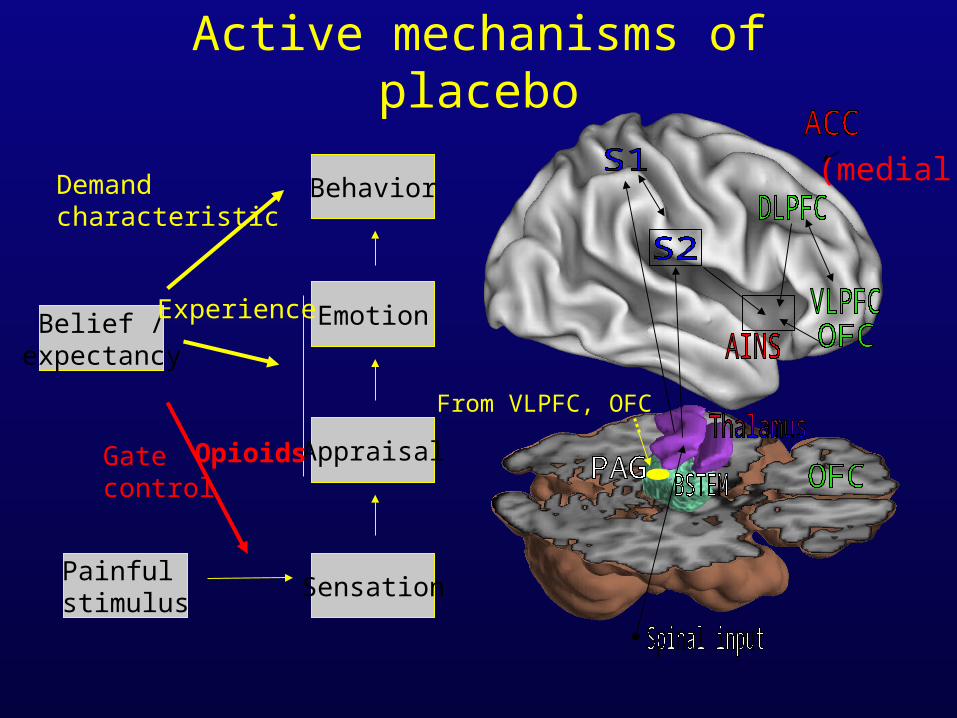
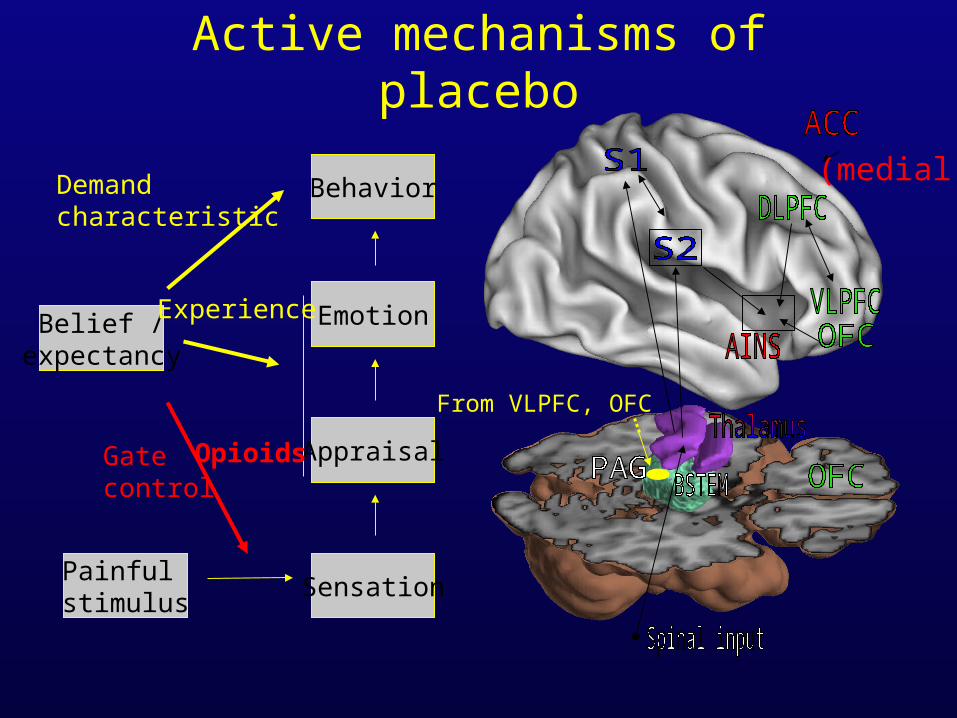
Active mechanisms of placebo
Belief /expectancy
Appraisal
Sensation
Emotion
Behavior
Painful stimulus
Gate control
Experience
Demandcharacteristic
Opioids
(medial)
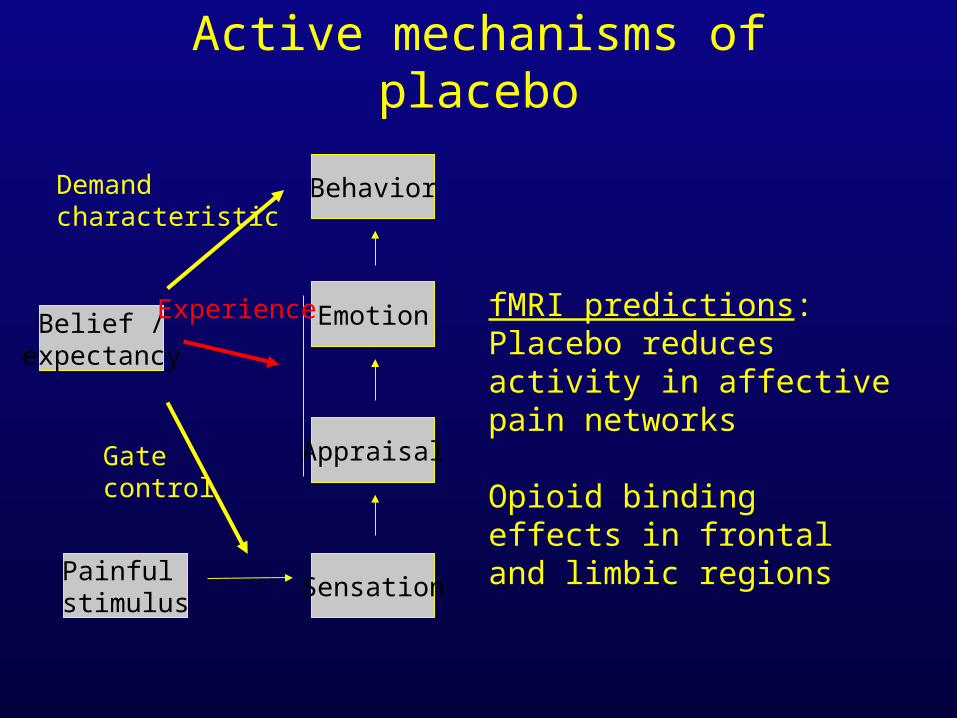
Active mechanisms of placebo
Belief /expectancy
Appraisal
Sensation
Emotion
Behavior
Painful stimulus
Gate control
Experience
Demandcharacteristic
fMRI predictions:Placebo reduces activity in affective pain networks
Opioid binding effects in frontal and limbic regions
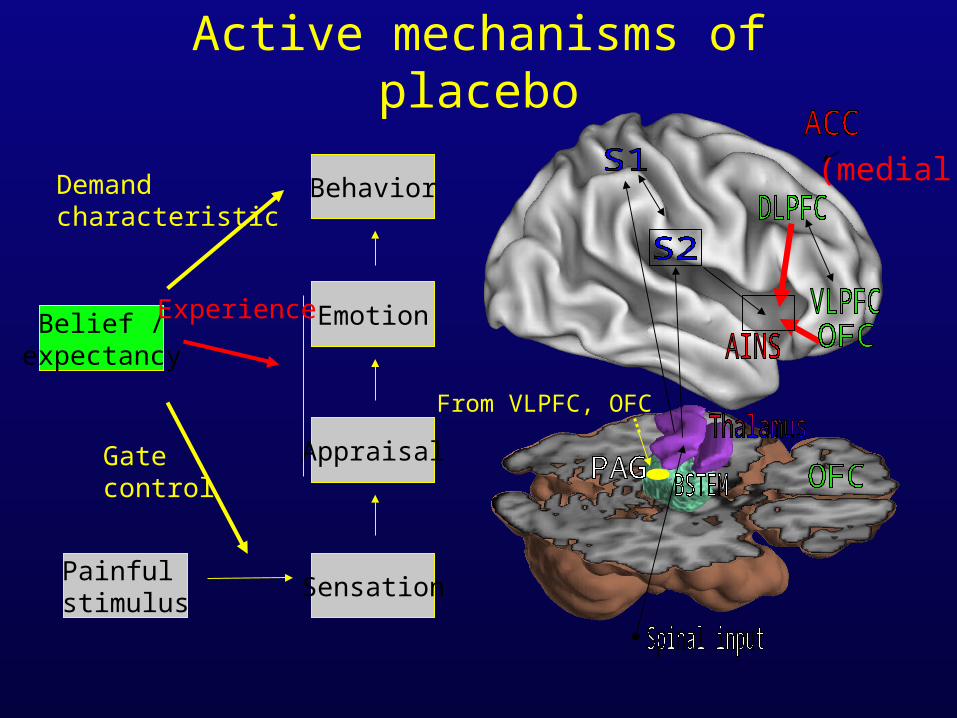
Active mechanisms of placebo
Belief /expectancy
Appraisal
Sensation
Emotion
Behavior
Painful stimulus
Gate control
Experience
Demandcharacteristic
From VLPFC, OFC
(medial)
fMRI studies
• Study 1: Shock on R forearm (n = 24)
• Study 2: Heat on L forearm (n = 23, selected placebo responders)
• Treatment with an inert ointment (Vasoline)– Placebo treatment: participants told that treatment was lidocaine– Control treatment: participants told that treatment was a ‘control cream’ to control for having ointment applied to skin
• Testing on placebo and control-treated skin
• fMRI design: Separate anticipation from experience of pain
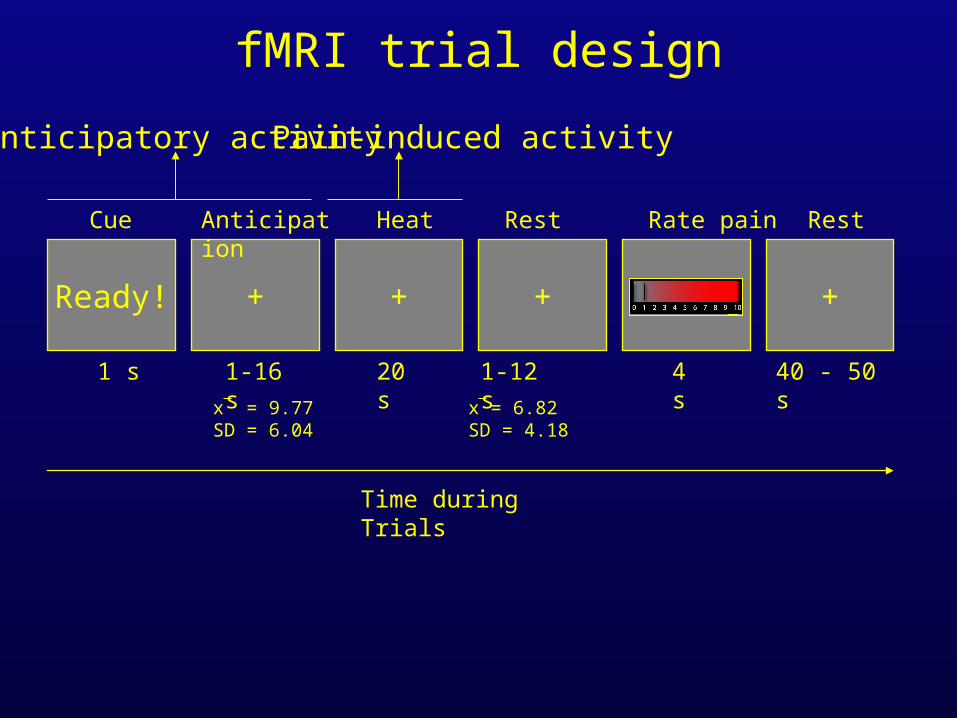
fMRI trial design
Time during Trials
+
20 s
Heat Rate pain
rating
4 s
Rest
+
40 - 50 s
Ready!
1 s
Cue
+
1-16 s
Anticipation
x = 9.77SD = 6.04
x = 6.82SD = 4.18
+
1-12 s
Rest
Anticipatory activity Pain-induced activity
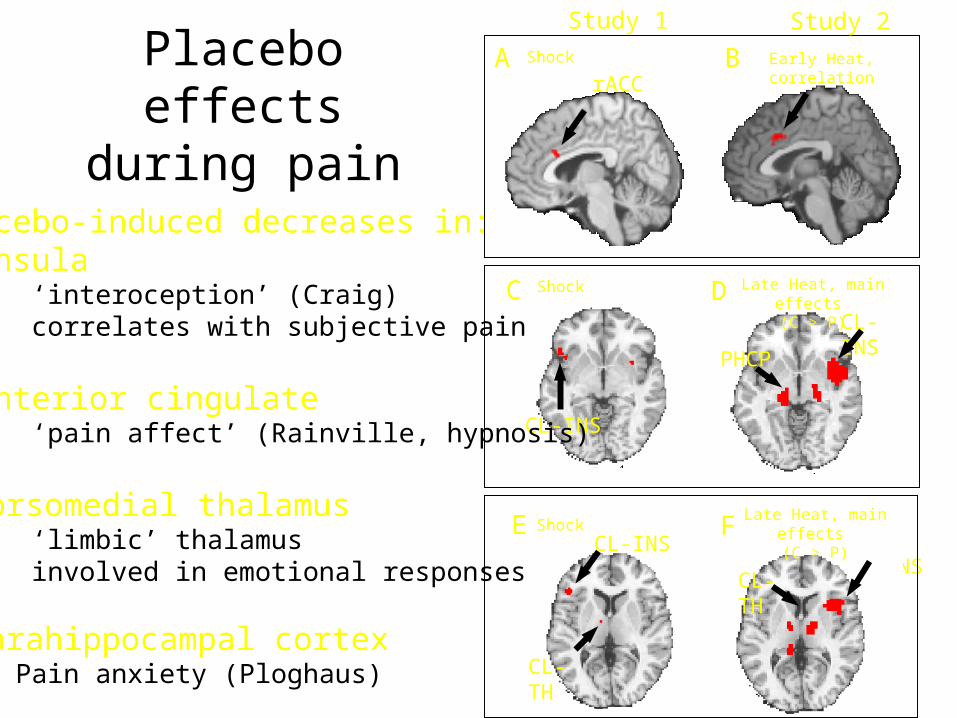
Placebo effects during pain
CL-INS
Shock
Early Heat, correlation Shock
Late Heat, main effects (C > P)
A B
C
rACC
CL-INS
CL-INS
CL-TH
CL-TH
CL-INS
D
E FShockLate Heat, main effects
(C > P)
PHCP
Study 1 Study 2
Placebo-induced decreases in:• Insula
• ‘interoception’ (Craig)• correlates with subjective pain
• Anterior cingulate• ‘pain affect’ (Rainville, hypnosis)
• Dorsomedial thalamus• ‘limbic’ thalamus• involved in emotional responses
• Parahippocampal cortex• Pain anxiety (Ploghaus)
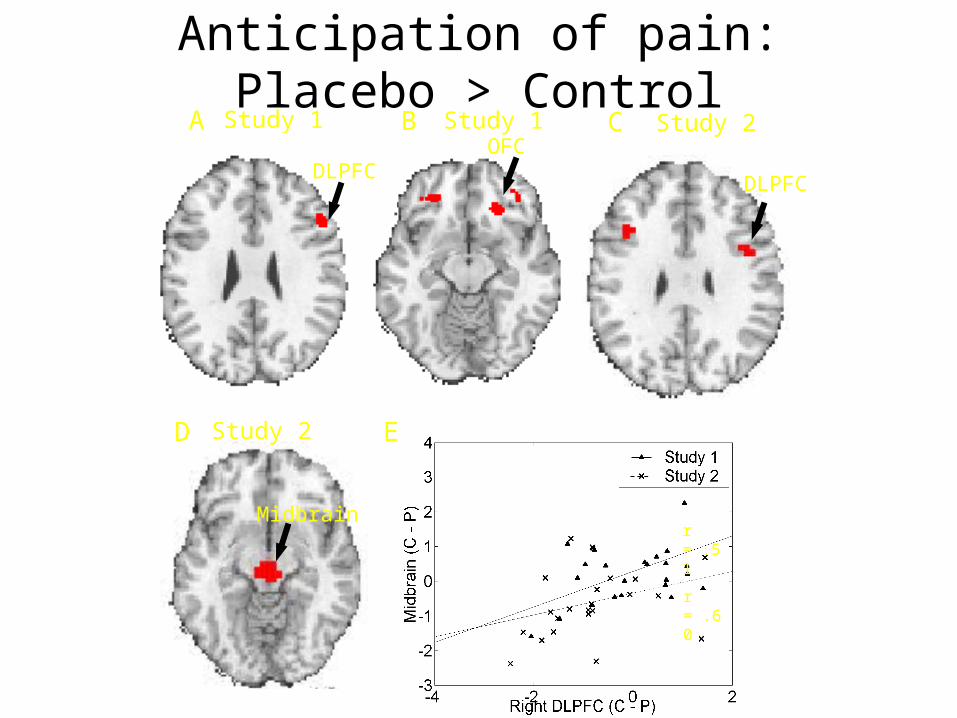
Anticipation of pain: Placebo > ControlB Study 1
OFCStudy 1A
Midbrain
DLPFC
C Study 2
DLPFC
r = .51
r = .60
Study 2D E
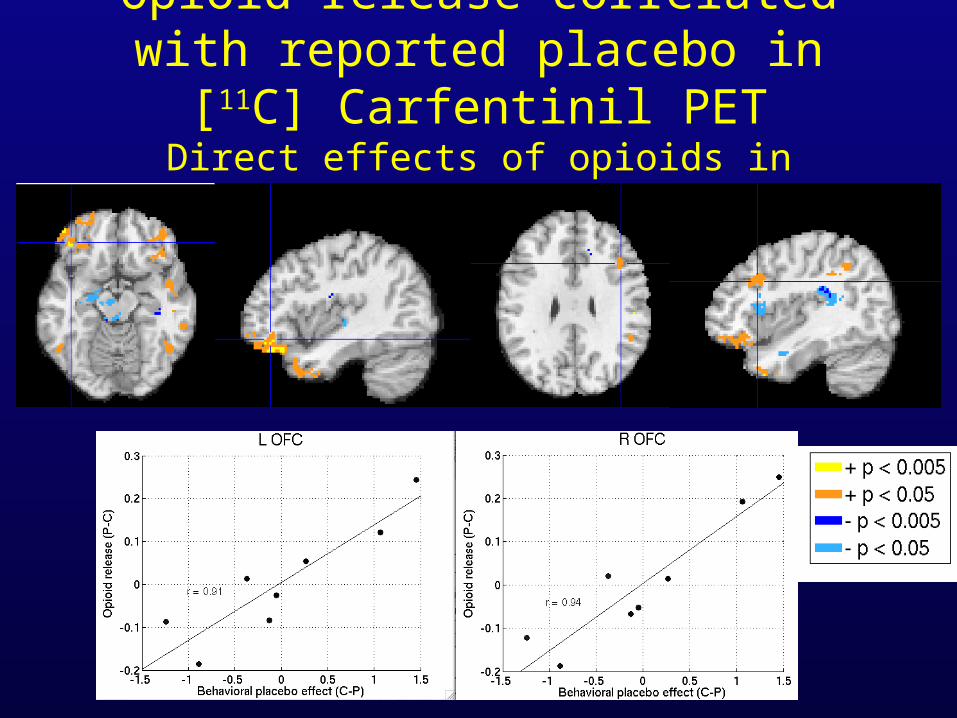
Opioid release correlated with reported placebo in [11C] Carfentinil PET
Direct effects of opioids in appraisal
Expectancy-induced control
• DLPFC activation, as in cognitive control
• OFC activation: Generation of expectancies– Expectancies of pain relief– Altered significance of incoming nociceptive stimuli– Opioid activity directly altered by placebo in OFC
• PAG activation– Opioid activity elicited in expectation of placebo (?)– ‘Affective decision’ circuit– Opioid activity correlated with placebo in PAG
Structure
• What is control? – Define terms: goals, expectations, and control– Control theory and principles of self-regulation
• Brain mechanisms of expectancy– Expectations in the control of attention– Expectations in the control of pain– Expectations in the control of emotion
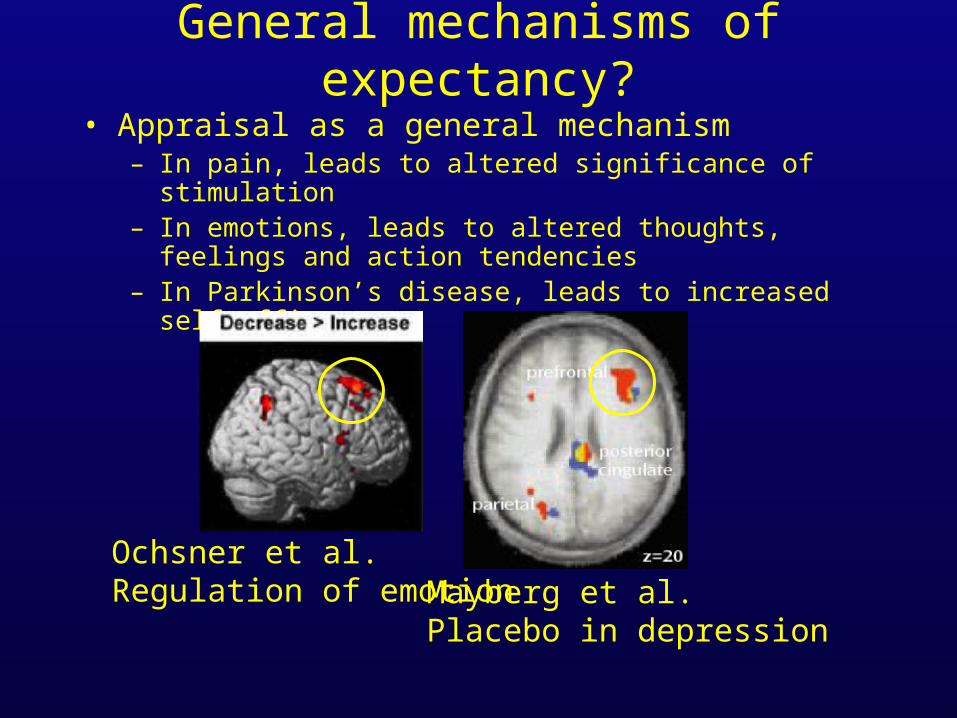
General mechanisms of expectancy?
• Appraisal as a general mechanism– In pain, leads to altered significance of stimulation– In emotions, leads to altered thoughts, feelings and action
tendencies – In Parkinson’s disease, leads to increased self-efficacy
Ochsner et al.Regulation of emotion Mayberg et al.
Placebo in depression
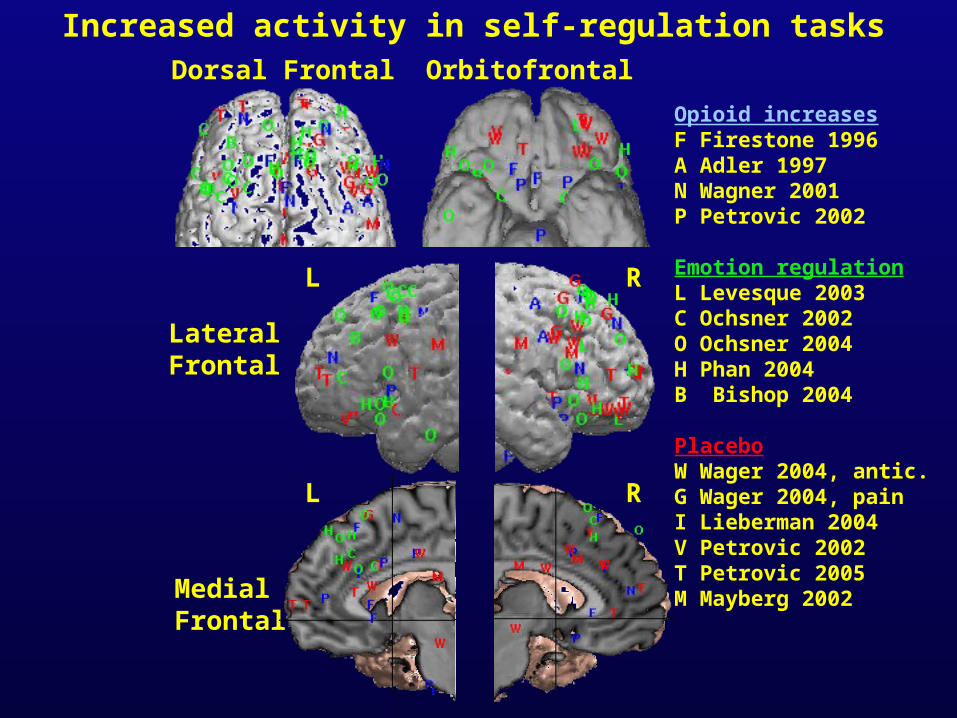
Opioid increasesF Firestone 1996A Adler 1997N Wagner 2001P Petrovic 2002
Emotion regulationL Levesque 2003C Ochsner 2002O Ochsner 2004H Phan 2004B Bishop 2004
PlaceboW Wager 2004, antic.G Wager 2004, painI Lieberman 2004V Petrovic 2002T Petrovic 2005M Mayberg 2002
Dorsal Frontal Orbitofrontal
Lateral Frontal
Medial Frontal
Increased activity in self-regulation tasks
L R
L R
Expectations and Emotion
• How does expectation of an emotional picture influence neural responses?
• Do patterns of expectancy distinguish emotionally resilient individuals from nonresilient ones?
• Resilience: Ability to deal effectively with life adversity• Sample: 15 resilient and 15 nonresilient individuals
picked from extremes of sample on ego resilience scale (e.g., Block 1989).
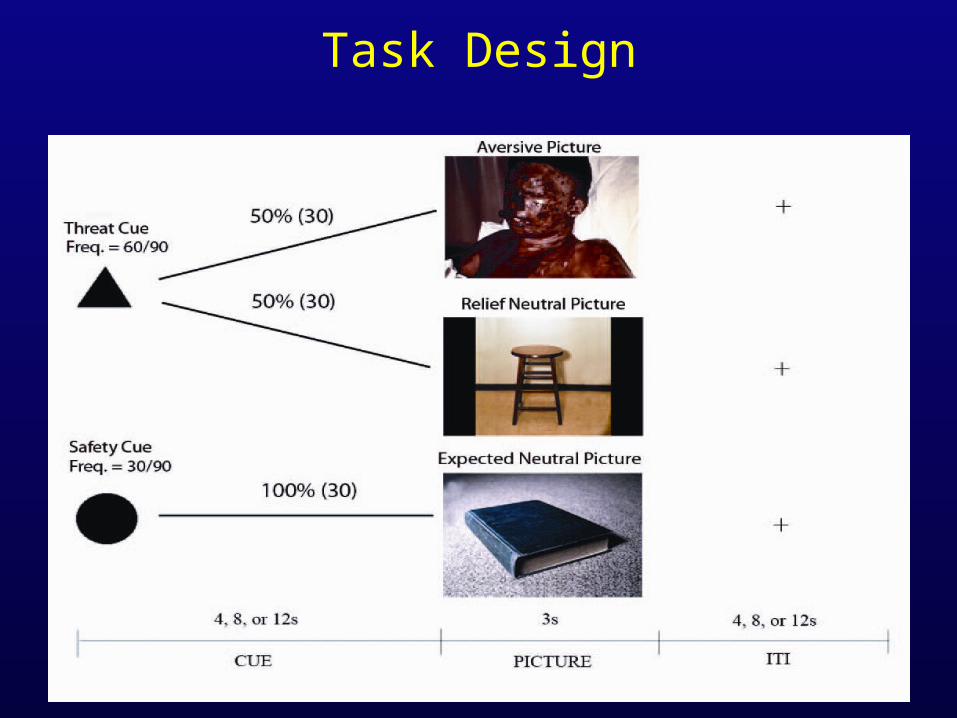
Task Design
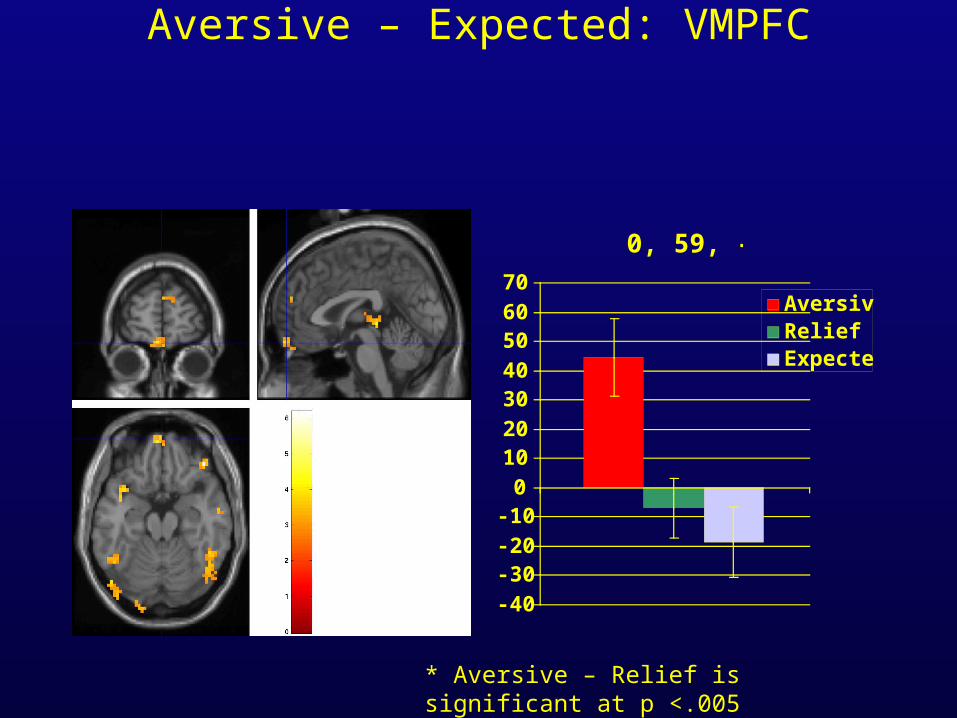
Aversive – Expected: VMPFC
0, 59, -21
-40
-30-20
-100
1020
3040
5060
70AversiveReliefExpected
* Aversive – Relief is significant at p <.005
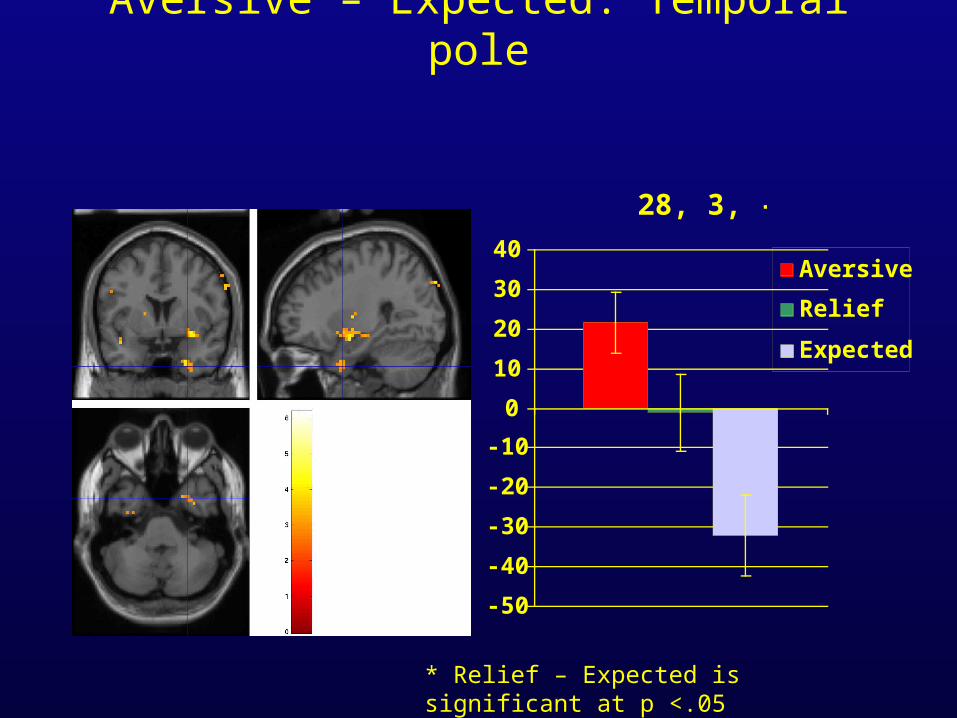
Aversive – Expected: Temporal pole
28, 3, -39
-50
-40
-30
-20
-10
0
10
20
30
40Aversive
Relief
Expected
* Relief – Expected is significant at p <.05
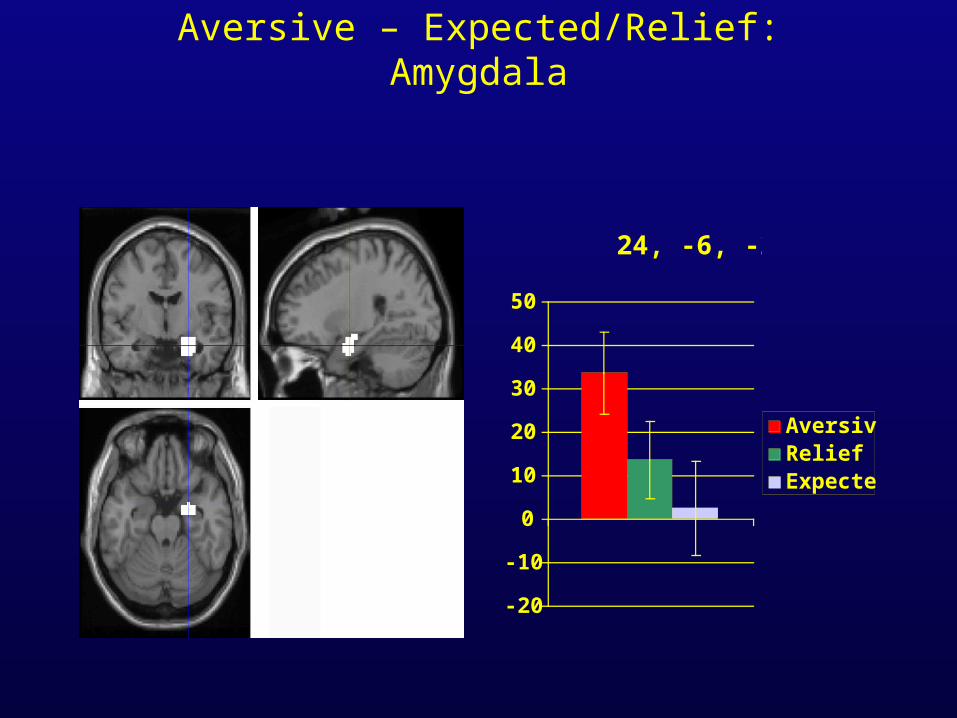
Aversive – Expected/Relief: Amygdala
24, -6, -22
-20
-10
0
10
20
30
40
50
AversiveReliefExpected
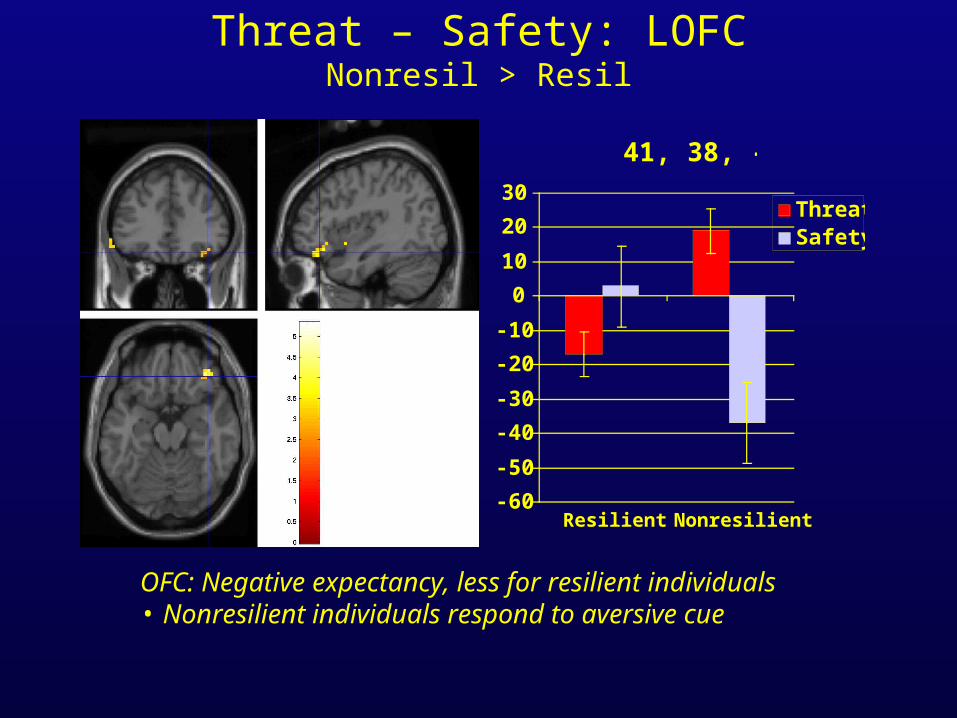
Threat – Safety: LOFCNonresil > Resil
41, 38, -18
-60
-50
-40
-30
-20
-10
0
10
20
30
Resilient Nonresilient
ThreatSafety
OFC: Negative expectancy, less for resilient individuals• Nonresilient individuals respond to aversive cue
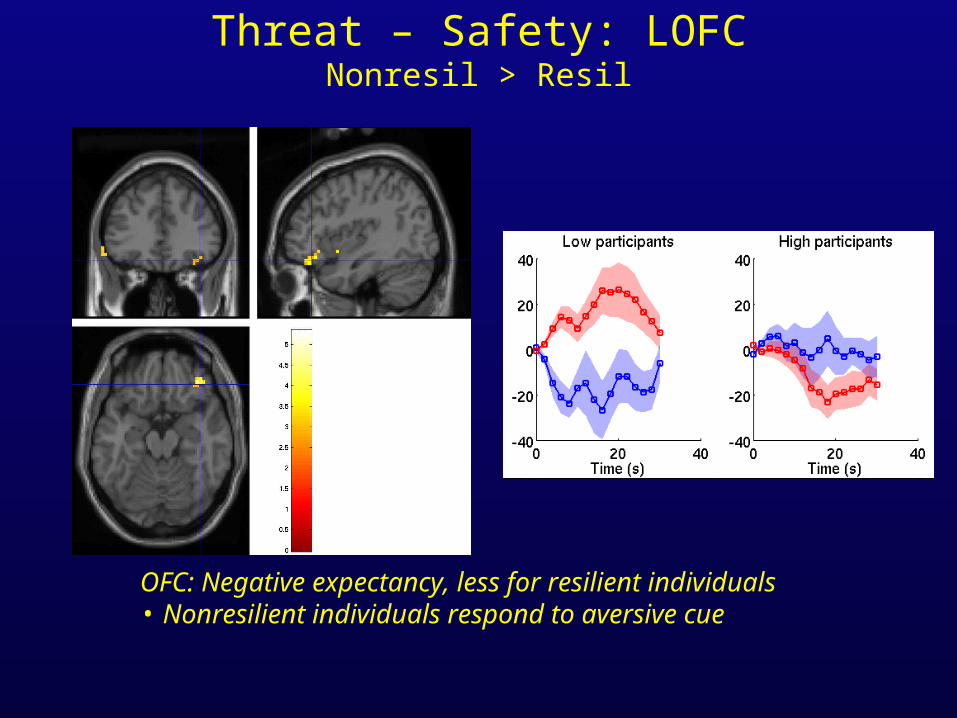
Threat – Safety: LOFCNonresil > Resil
OFC: Negative expectancy, less for resilient individuals• Nonresilient individuals respond to aversive cue
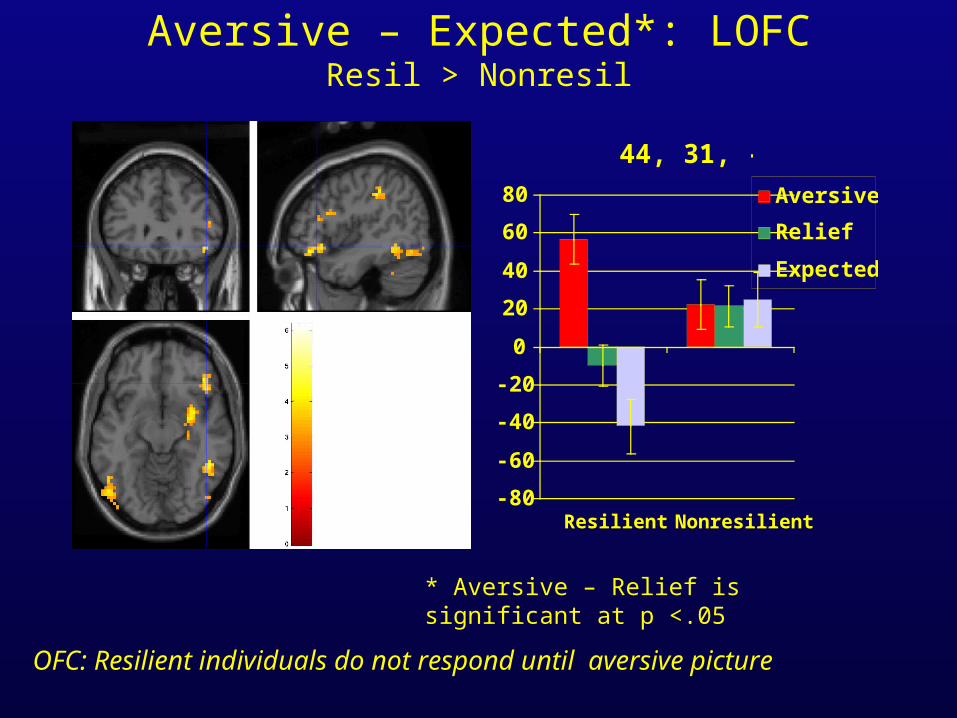
Aversive – Expected*: LOFCResil > Nonresil
44, 31, -12
-80
-60
-40
-20
0
20
40
60
80
Resilient Nonresilient
Aversive
Relief
Expected
* Aversive – Relief is significant at p <.05
OFC: Resilient individuals do not respond until aversive picture
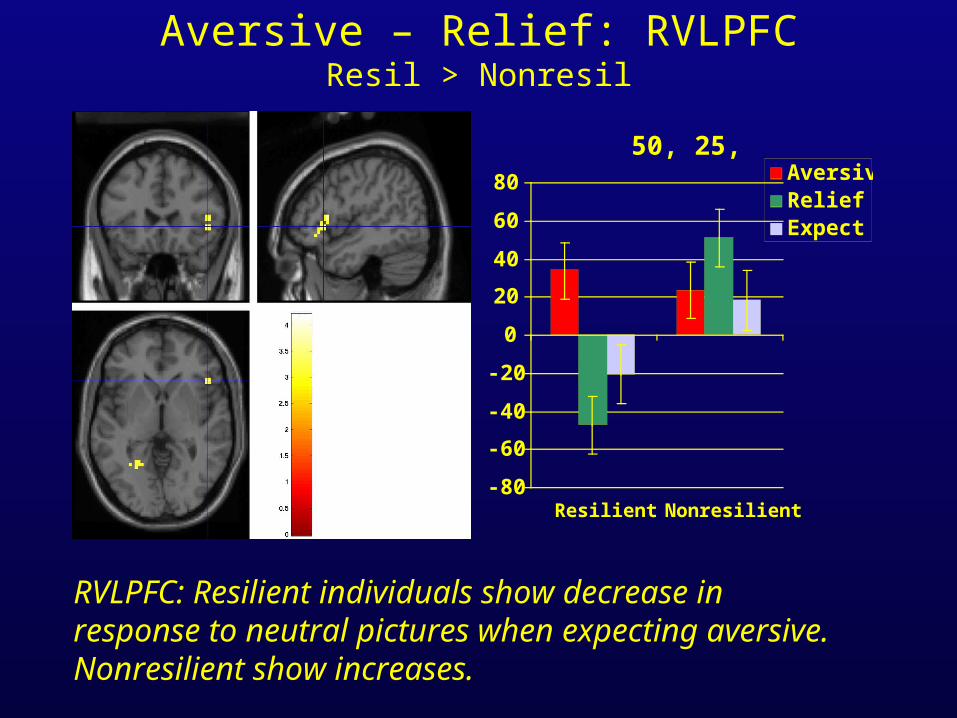
Aversive – Relief: RVLPFCResil > Nonresil
50, 25, 0
-80
-60
-40
-20
0
20
40
60
80
Resilient Nonresilient
AversiveReliefExpect
RVLPFC: Resilient individuals show decrease in response to neutral pictures when expecting aversive. Nonresilient show increases.
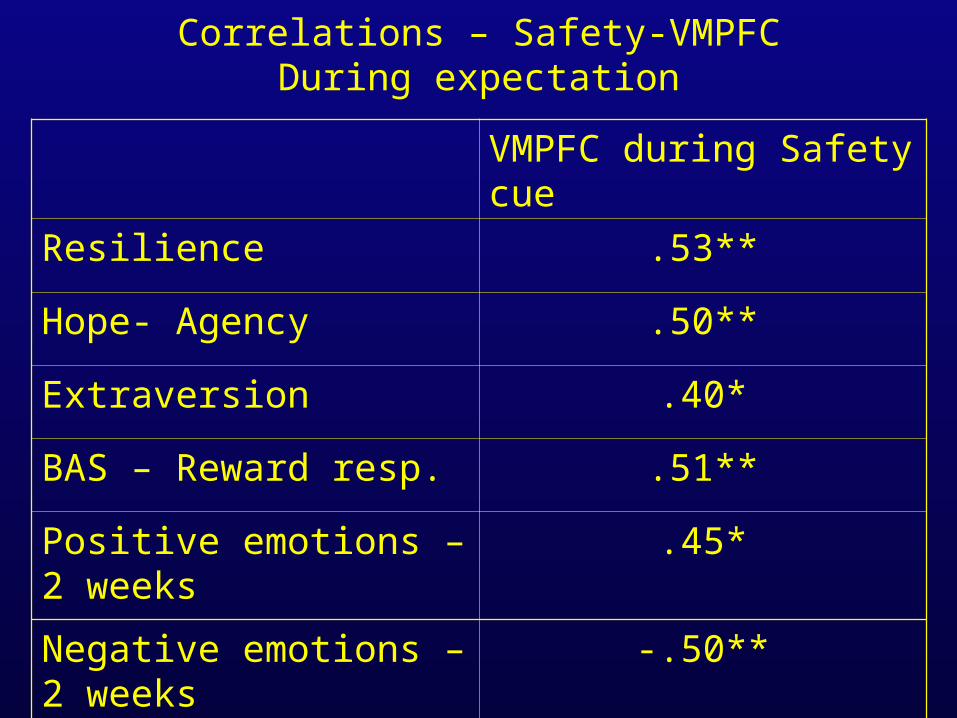
Correlations – Safety-VMPFCDuring expectation
VMPFC during Safety cue
Resilience .53**
Hope- Agency .50**
Extraversion .40*
BAS – Reward resp. .51**
Positive emotions – 2 weeks .45*
Negative emotions – 2 weeks
-.50**
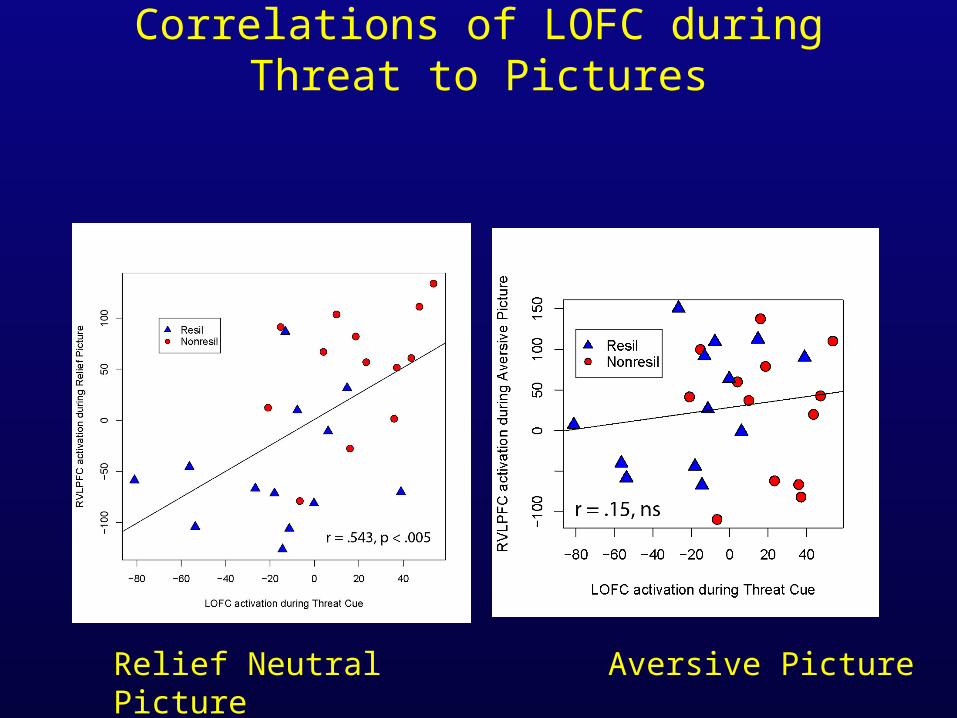
Correlations of LOFC during Threat to Pictures
Relief Neutral Picture
Aversive Picture
Emotion and expectancy
• Expectation of aversive stimuli elicits OFC activity. More expectancy in nonresilient individuals.
• Co-localized with expectancy effects in pain
• Lower aversive OFC expectancy effects correlated with greater deactivation of VMPFC to ‘relief’ pictures, and with broad measures of optimism
• Resilience: shift away from aversive expectations
Final conclusions• Expectancy, or predictions about future states (including emotional
experiences) is an important factor in shaping experience.
• Expectations provide ways of controlling behavior without experiencing adverse consequences first.
• Emerging circuit in ventrolateral PFC/anterior insula and orbitofrontal cortex links expectancies across cognitive and emotional domains
• Much more to learn! Underlying functions of these regions; impact on emotional health and cognitive ability; ways of modifying expectations and their effects in the brain.
Thank you!
Threat cues in the brain
QuickTime™ and aTIFF (LZW) decompressor
are needed to see this picture.
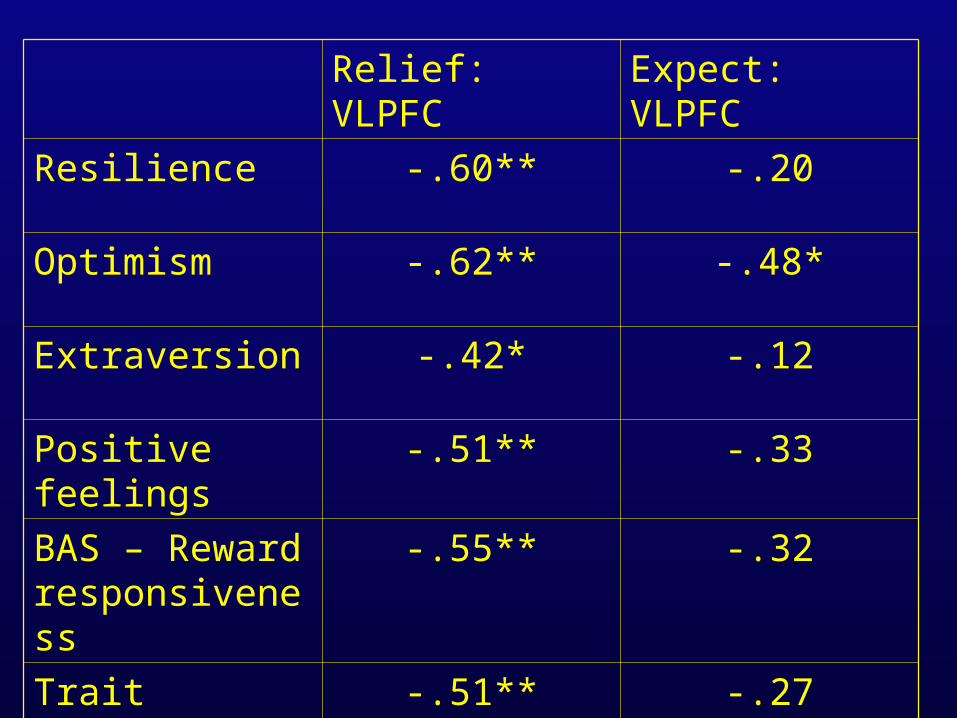
Relief: VLPFC Expect: VLPFC
Resilience -.60** -.20
Optimism -.62** -.48*
Extraversion -.42* -.12
Positive feelings -.51** -.33
BAS – Reward responsiveness
-.55** -.32
Trait positivity -.51** -.27
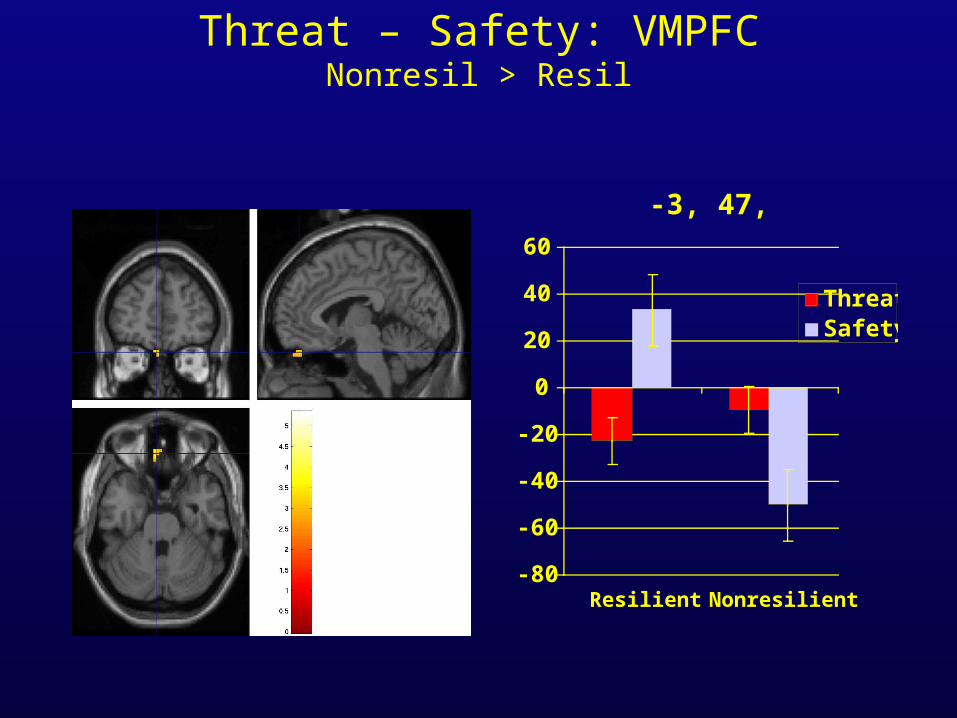
Threat – Safety: VMPFCNonresil > Resil
-3, 47, -27
-80
-60
-40
-20
0
20
40
60
Resilient Nonresilient
ThreatSafety
Conclusions
• Nonresilient activate more MPFC/LOFC in response to the threat cue
• Nonresilient activate more RVLPFC to relief pictures than Resilient
• This activation in the LOFC to the threat cue predicts RVLPFC response to the relief neutral pictures
• If LOFC -> negative expectations and RVLPFC -> negative labelling, then for NR, their negative expectations drive their negative labelling of a neutral picture.
• Resilient people are better able to discriminate negative from neutral events -> may lead to quicker recovery
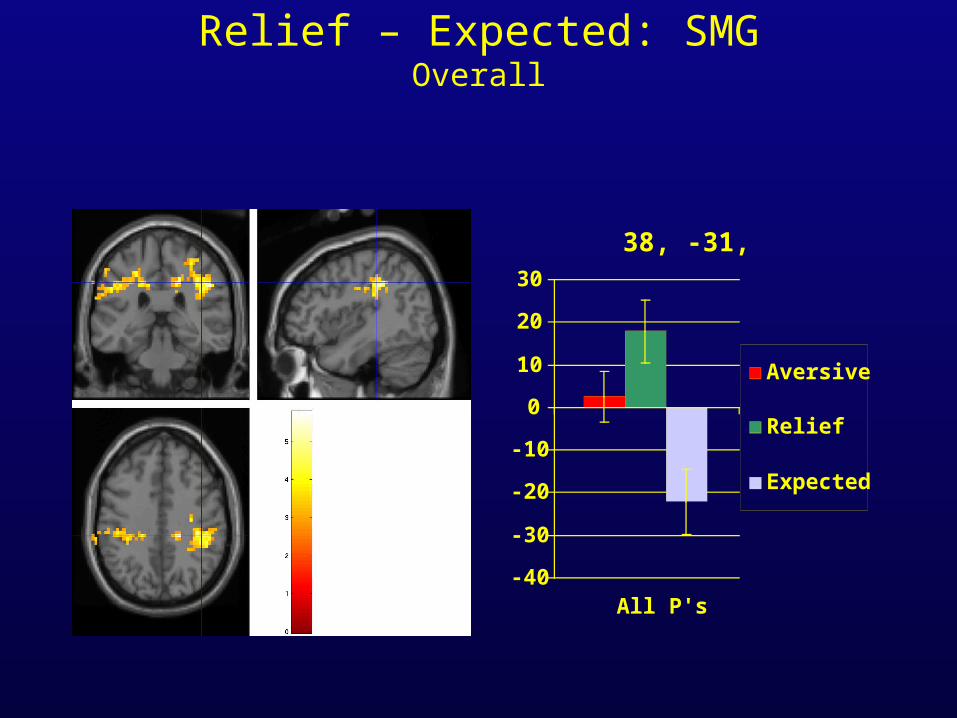
Relief – Expected: SMGOverall
38, -31, 39
-40
-30
-20
-10
0
10
20
30
All P's
Aversive
Relief
Expected
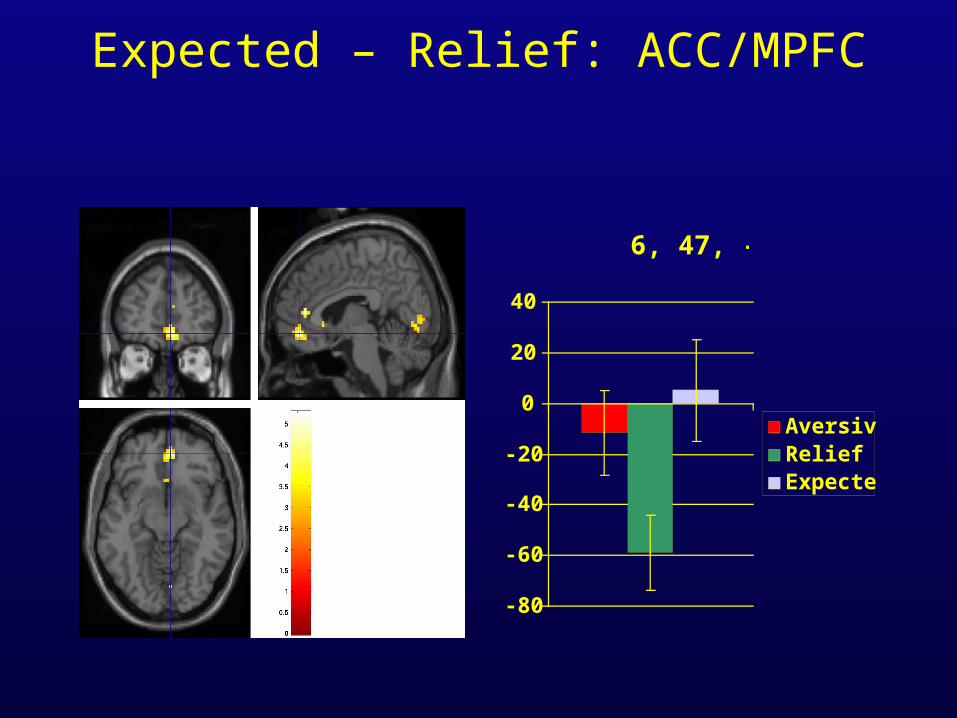
Expected – Relief: ACC/MPFC
6, 47, -9
-80
-60
-40
-20
0
20
40
AversiveReliefExpected
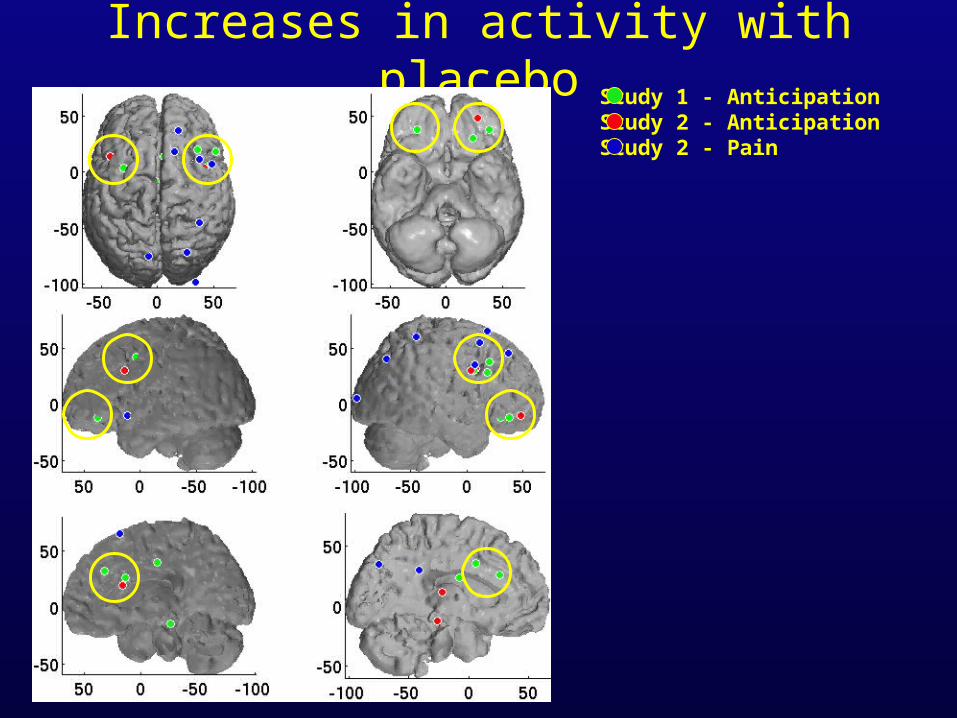
Increases in activity with placeboStudy 1 - AnticipationStudy 2 - AnticipationStudy 2 - Pain
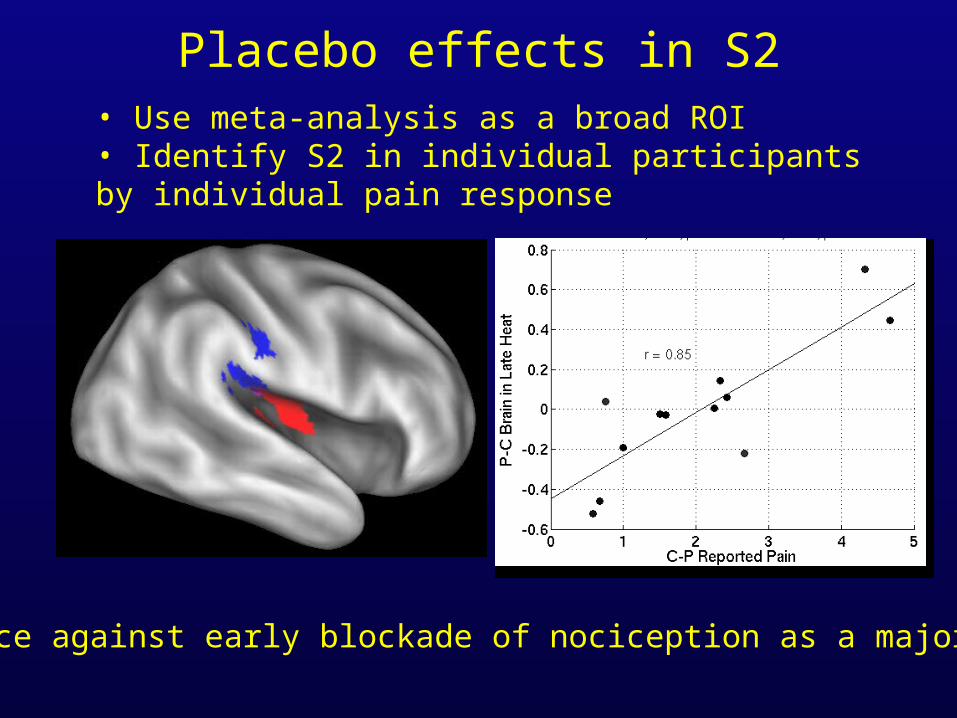
Placebo effects in S2• Use meta-analysis as a broad ROI• Identify S2 in individual participants by individual pain response
Evidence against early blockade of nociception as a major factor
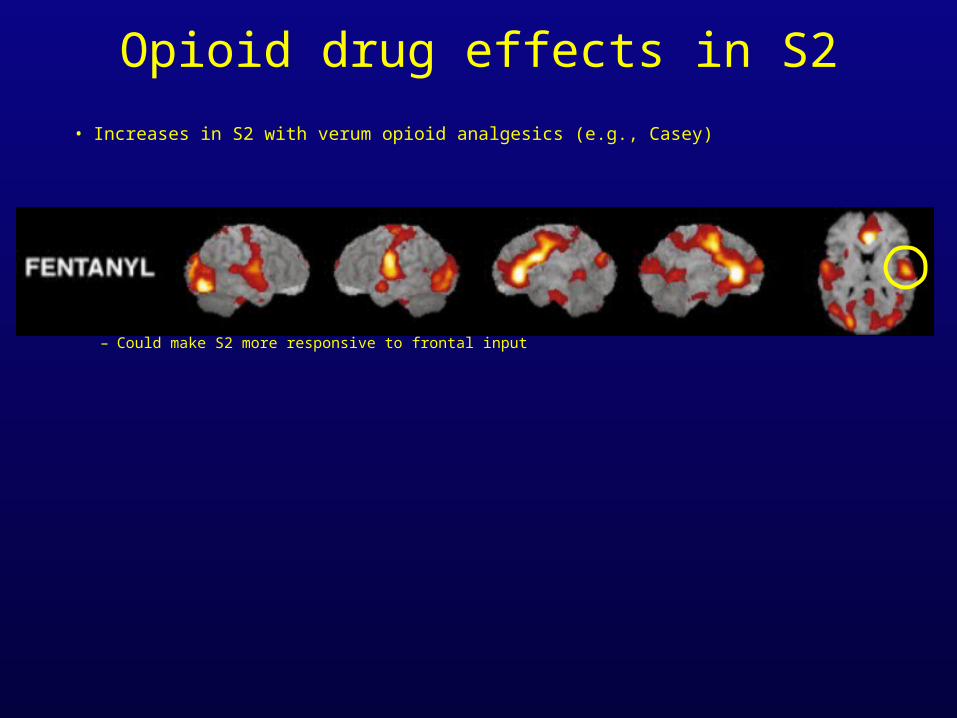
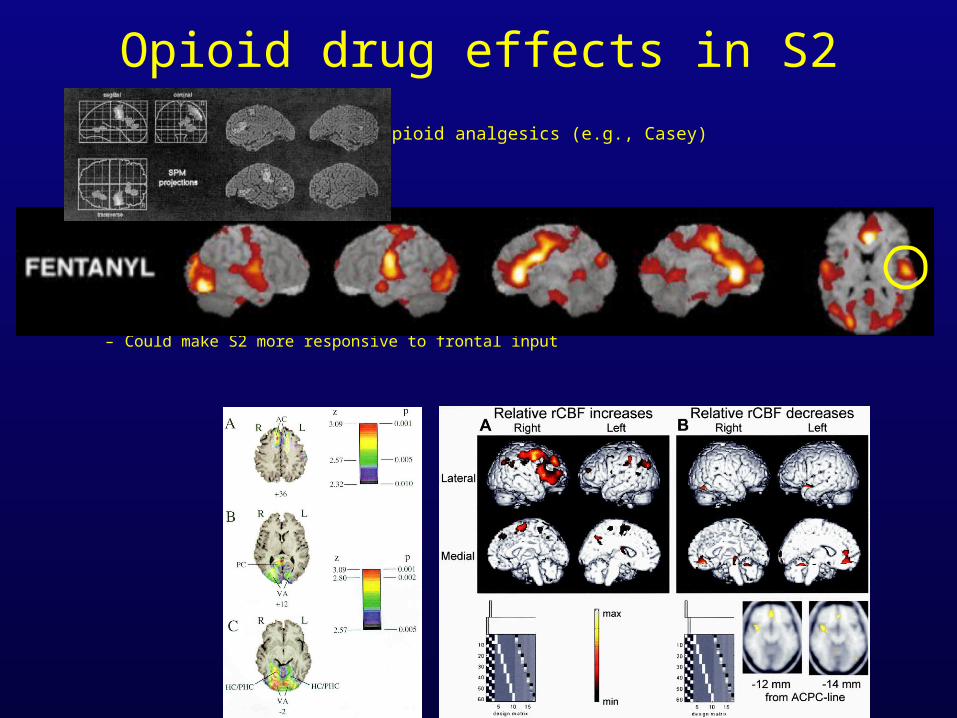
Opioid drug effects in S2
• Increases in S2 with verum opioid analgesics (e.g., Casey)
• Increased inhibitory input– Metabolic activity in interneurons -> Tonic increase– Could make S2 more responsive to frontal input
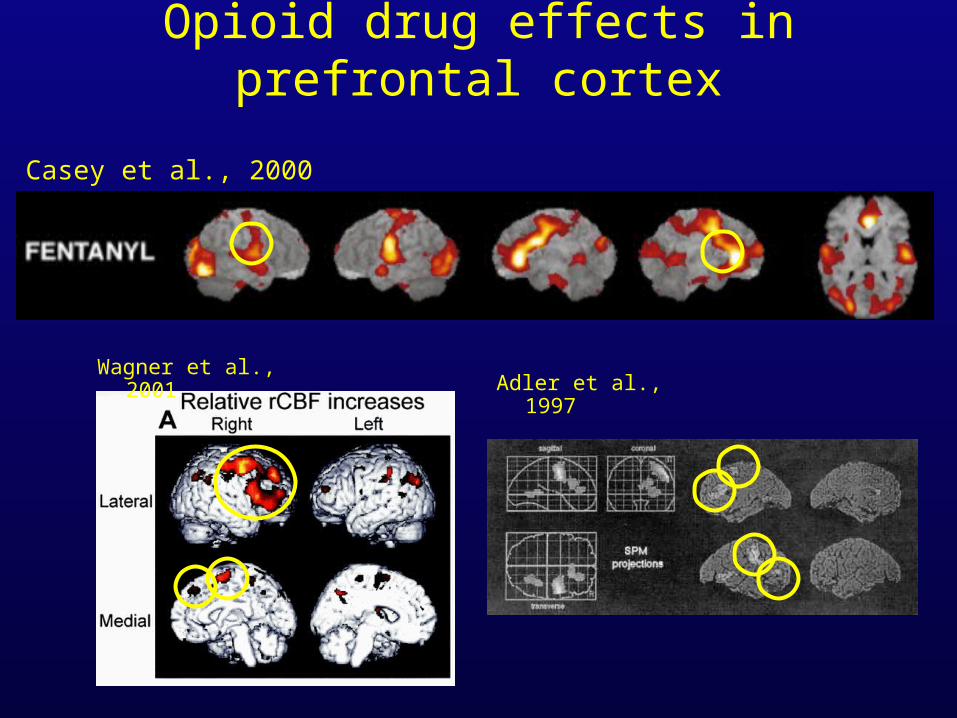
Opioid drug effects in prefrontal cortex
Casey et al., 2000
Wagner et al., 2001Adler et al., 1997
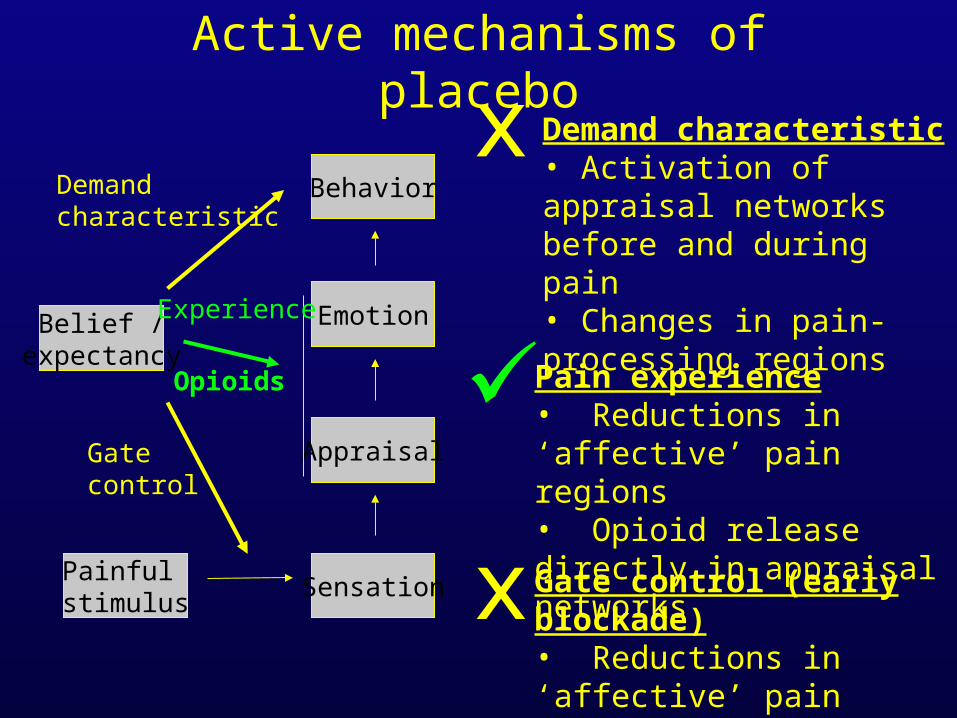
Active mechanisms of placebo
Belief /expectancy
Appraisal
Sensation
Emotion
Behavior
Painful stimulus
Gate control
Experience
Demandcharacteristic
Demand characteristic• Activation of appraisal networks before and during pain• Changes in pain-processing regions
Opioids
x
Pain experience• Reductions in ‘affective’ pain regions• Opioid release directly in appraisal networks
Gate control (early blockade)• Reductions in ‘affective’ pain regions• Increased activation in S2
x
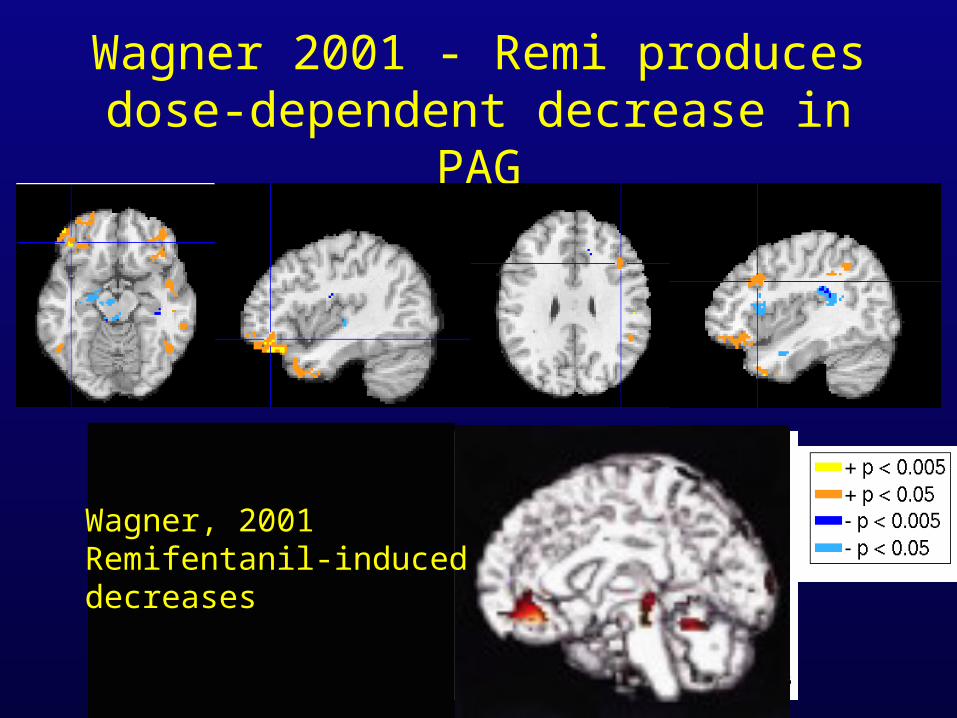
Wagner 2001 - Remi produces dose-dependent decrease in PAG
Wagner, 2001Remifentanil-induceddecreases
Opioid drug effects in S2
• Increases in S2 with verum opioid analgesics (e.g., Casey)
• Increased inhibitory input– Metabolic activity in interneurons -> Tonic increase– Could make S2 more responsive to frontal input
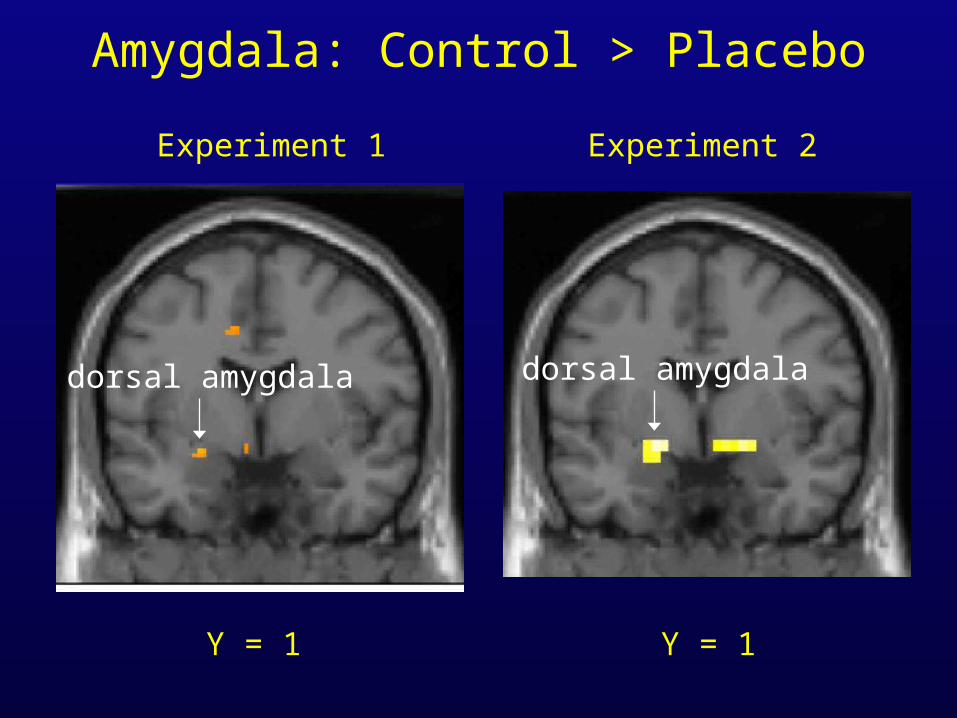
Y = 1 Y = 1
Experiment 1 Experiment 2
dorsal amygdala dorsal amygdala
Amygdala: Control > Placebo
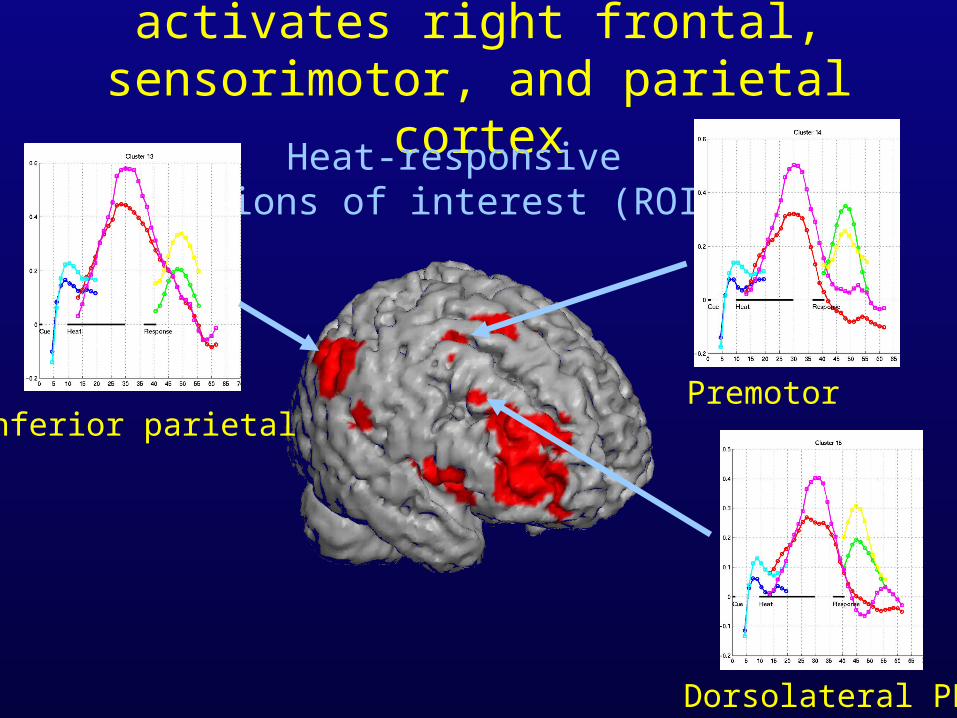
Peak Heat: Placebo activates right frontal, sensorimotor, and parietal cortex
Heat-responsiveRegions of interest (ROIs)
Inferior parietalPremotor
Dorsolateral PFC
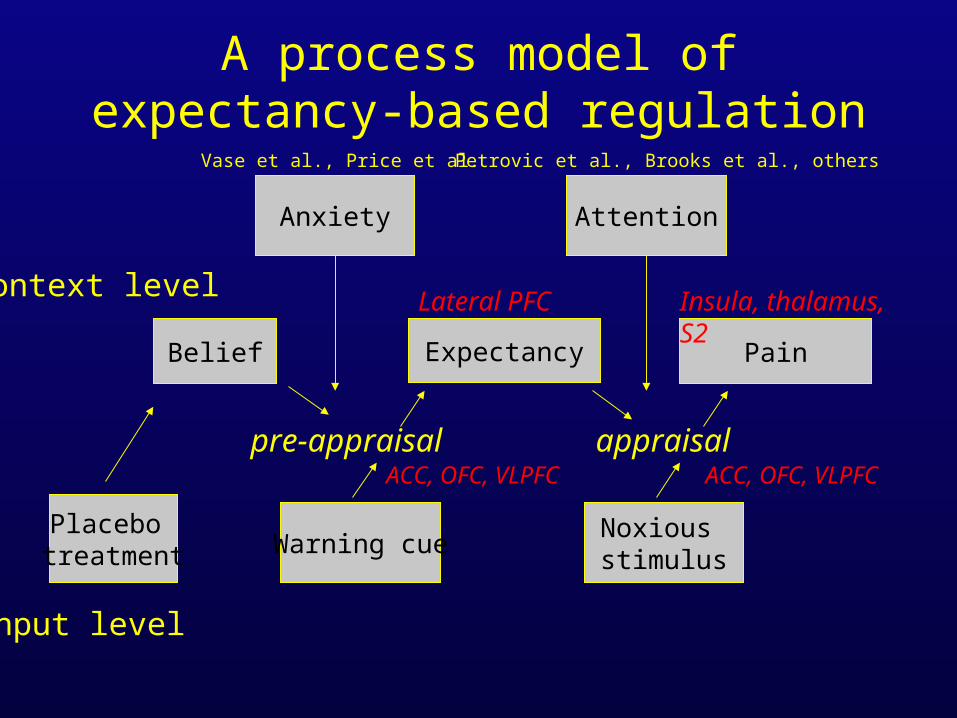
A process model of expectancy-based regulation
Warning cue
Belief
Placebo treatment
Expectancy
pre-appraisal
Noxious stimulus
Pain
appraisal
Context level
Input level
Lateral PFC
ACC, OFC, VLPFC ACC, OFC, VLPFC
Insula, thalamus, S2
Anxiety
Vase et al., Price et al.
Attention
Petrovic et al., Brooks et al., others
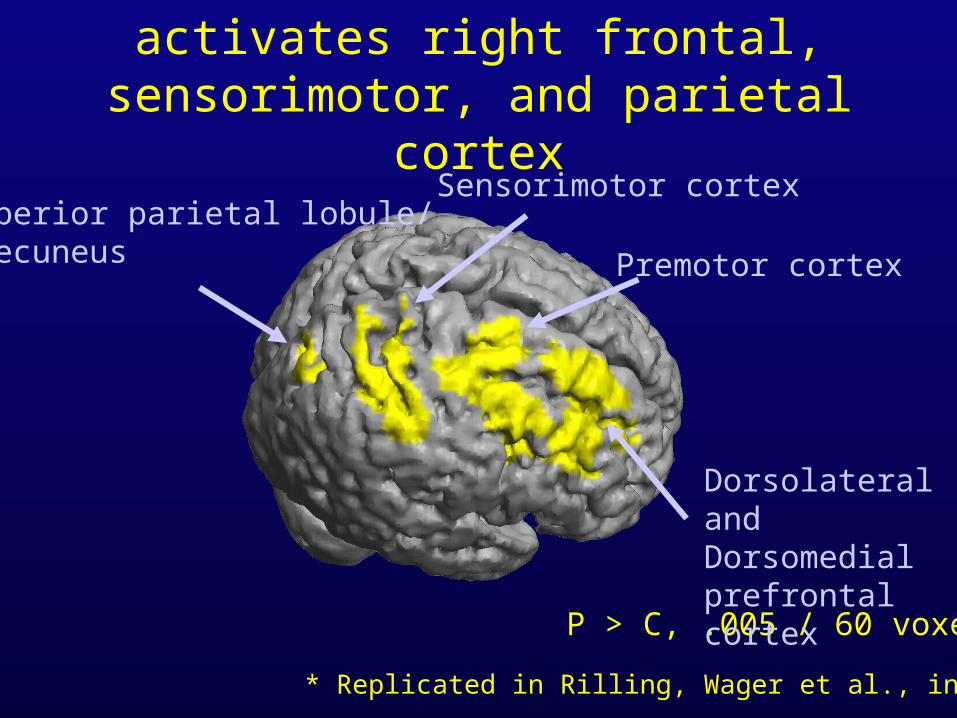
Peak Heat: Placebo activates right frontal, sensorimotor, and parietal cortex
P > C, .005 / 60 voxels
Superior parietal lobule/precuneus
Sensorimotor cortex
Dorsolateral andDorsomedial prefrontal cortex
Premotor cortex
* Replicated in Rilling, Wager et al., in prep.
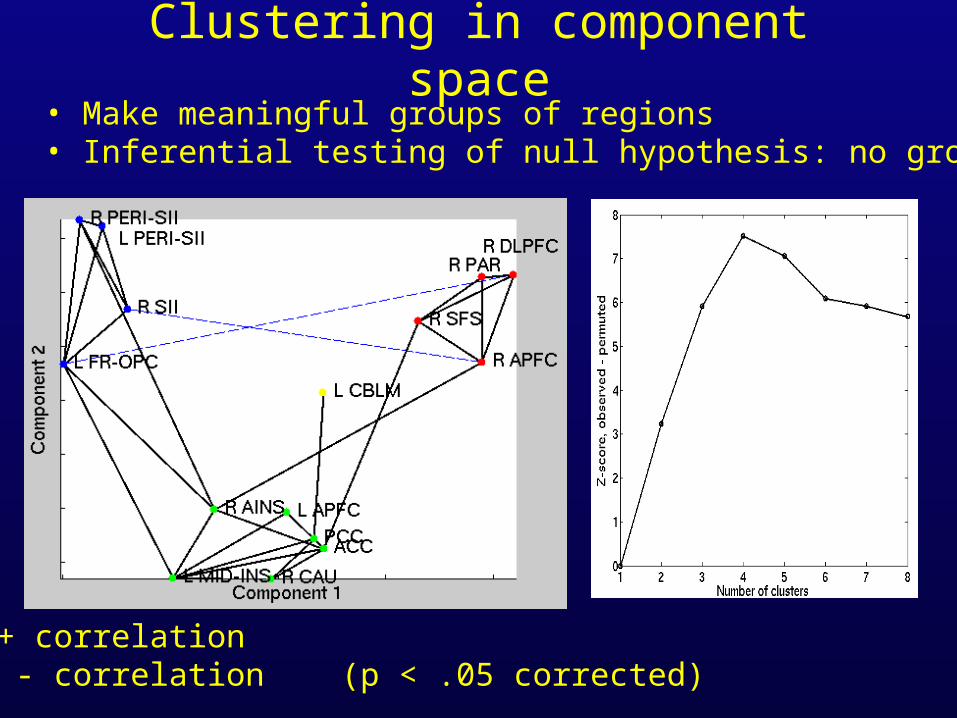
Clustering in component space• Make meaningful groups of regions• Inferential testing of null hypothesis: no grouping
Black: + correlation Blue: - correlation (p < .05 corrected)
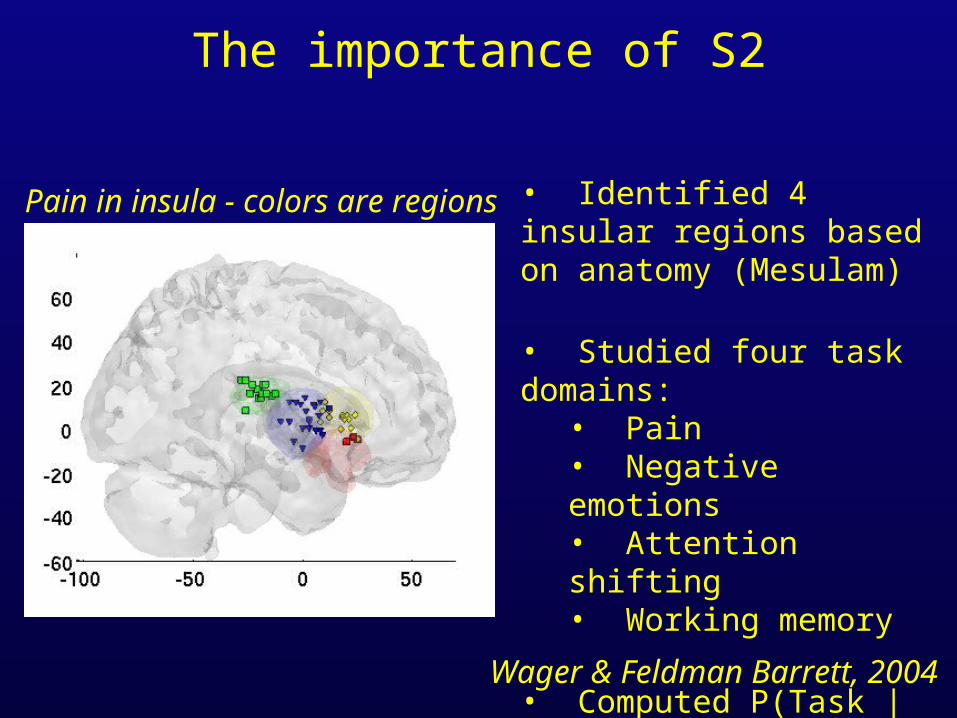
The importance of S2
Pain in insula - colors are regions
Wager & Feldman Barrett, 2004
• Identified 4 insular regions based on anatomy (Mesulam)
• Studied four task domains:• Pain• Negative emotions• Attention shifting• Working memory
• Computed P(Task | Activity) in each region
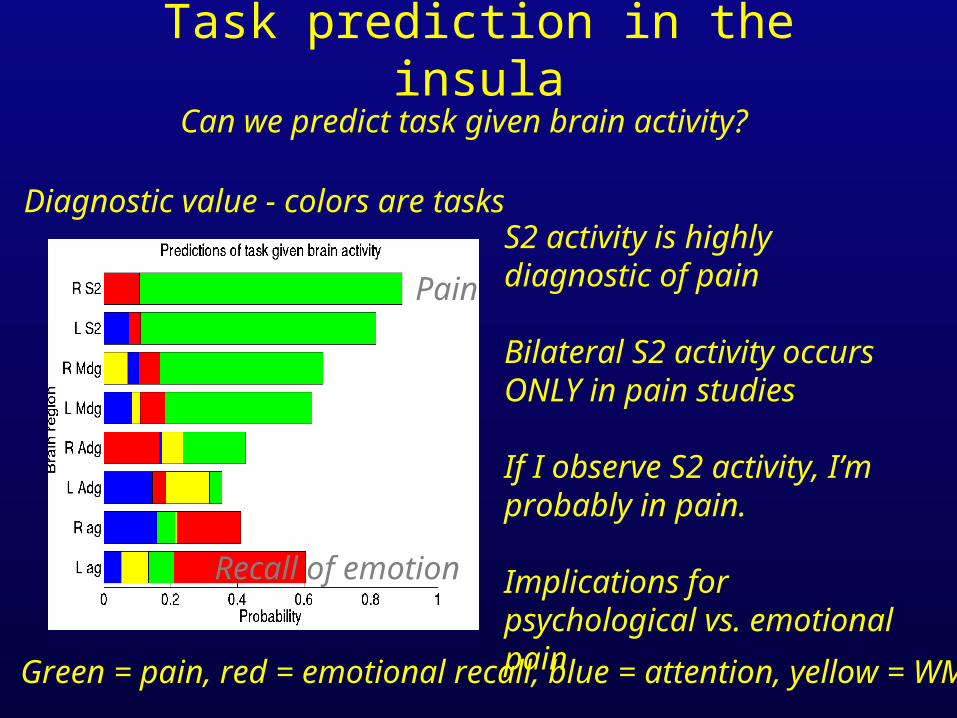
Task prediction in the insula
Pain
Recall of emotion
Diagnostic value - colors are tasks
Can we predict task given brain activity?
Green = pain, red = emotional recall, blue = attention, yellow = WM
S2 activity is highly diagnostic of pain
Bilateral S2 activity occurs ONLY in pain studies
If I observe S2 activity, I’m probably in pain.
Implications for psychological vs. emotional pain
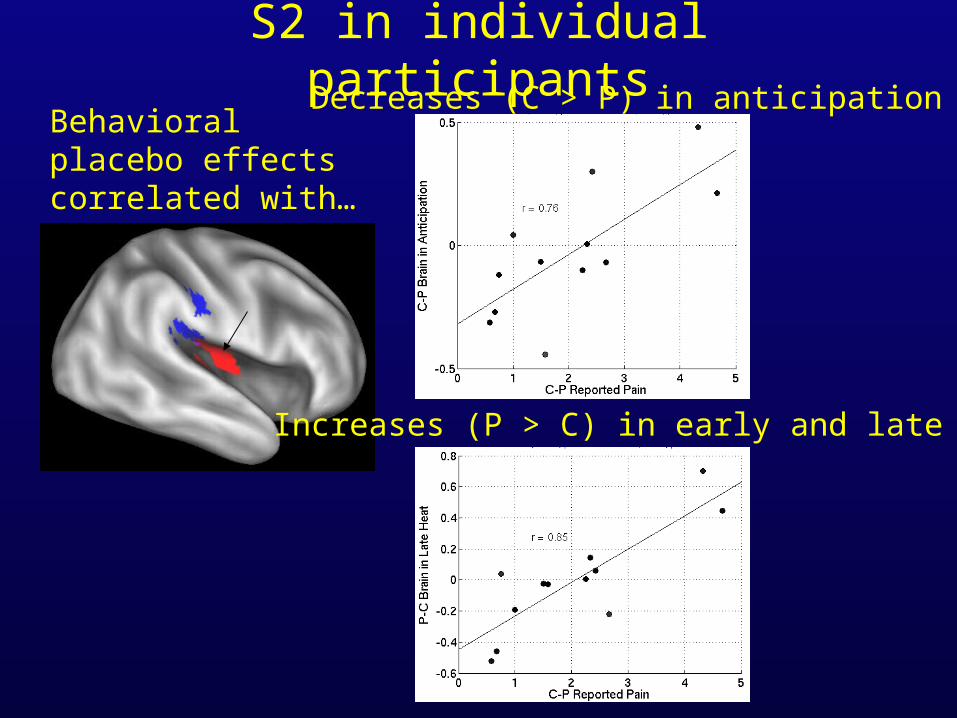
S2 in individual participantsDecreases (C > P) in anticipation
Increases (P > C) in early and late heat
Behavioral placebo effects correlated with…
Active mechanisms of placebo
Belief /expectancy
Appraisal
Sensation
Emotion
Behavior
Painful stimulus
Gate control
Experience
Demandcharacteristic
Opioids
From VLPFC, OFC
(medial)
Active mechanisms of placebo
Belief /expectancy
Appraisal
Sensation
Emotion
Behavior
Painful stimulus
Gate control
Experience
Demandcharacteristic
Opioids
From VLPFC, OFC
(medial)
From VLPFC, OFC
(medial)
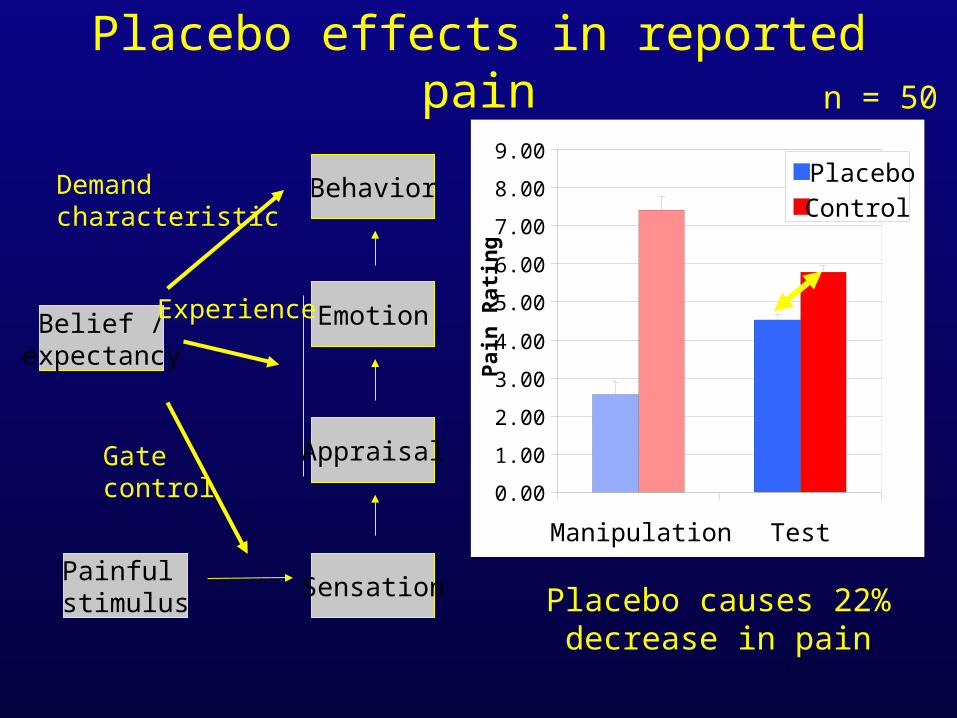
Placebo effects in reported pain
Behavior
Appraisal
Sensation
Emotion
Painful stimulus
Belief /expectancy
Gate control
Experience
Demandcharacteristic
n = 50
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
8.00
9.00
Manipulation Test
Pai
n R
atin
g
PlaceboControl
Placebo causes 22%decrease in pain







![[34] - Lindquist Lablindquistlab.wi.mit.edu/wp-content/uploads/2013/06/...Schirmer, C. Queitsch, A. S. Kowal, and S. Lindquist, submitted (1997). a" Y. Sanchcz and S. L. Lindquist,](https://img.pdfslide.us/doc/110x75/606c80b19bb7de31a926ace6/34-lindquist-schirmer-c-queitsch-a-s-kowal-and-s-lindquist-submitted.jpg)





















