Embed Size (px)
Citation preview

Descriptive Epidemiology of Colorectal Cancerin the United States, 1998–2001, Utilizing Data
from the NPCR and SEER ProgramsSupplement to Cancer
Excess Risk of Subsequent Primary Cancers AmongColorectal Carcinoma Survivors, 1975–2001
Faruque Ahmed, PhD1
Marc T. Goodman, PhD, MPH2
Carol Kosary, MA3
Bernardo Ruiz, MD, PhD4
Xiao-Cheng Wu, MD, MPH4
Vivien W. Chen, PhD4
Catherine N. Correa, PhD, MPH4
1 Cancer Surveillance Branch, Division of CancerPrevention and Control, Centers for DiseaseControl and Prevention (CDC), Atlanta, Georgia.
2 Cancer Research Center, University of Hawaii,Honolulu, Hawaii.
3 Cancer Statistics Branch, Surveillance ResearchProgram, Division of Cancer Control and PopulationSciences, National Cancer Institute (NCI), Rockville,Maryland.
4 Louisiana Tumor Registry, Epidemiology Program,School of Public Health, Louisiana State UniversityHealth Sciences Center, New Orleans, Louisiana.
BACKGROUND. Studies of persons with colorectal cancer have reported increased
risk of subsequent primary cancers. Results have not been consistent, however,
and there is little information about such risk in specific races and ethnic popu-
lations.
METHODS. Using 1975–2001 data from the Surveillance, Epidemiology, and End
Results (SEER) Program, we assembled 262,600 index cases of colorectal carci-
noma to assess the occurrence of subsequent primary cancers in 13 noncolonic
sites. Observed (O) subsequent cancers were compared with those expected (E)
based on age-/sex-/race-/year-/site-specific rates in the SEER population. The
standardized incidence ratio (SIR) and the absolute excess risk (AER) represent
‘O 7 E’ and ‘O – E,’ respectively.
RESULTS. Colorectal carcinoma patients had significantly elevated SIRs for small
gut, stomach (males), kidney, and corpus uteri cancers, ranging from 1.13 for sto-
mach cancer in males to 3.45 for small gut cancer in females. Elevated SIRs for
additional sites were seen in certain population subgroups: pancreas and ovary
in persons aged <50 years, and prostate in black males. The excess burden, as
assessed by AER, was notable for prostate cancer in black males and for corpus
uteri cancer in females aged <50 years (26.5 and 9.5 cancers per 10,000 person-
years, respectively), and it persisted beyond 5 years of follow-up.
CONCLUSIONS. Although significantly elevated SIRs were found for several cancers,
the excess burden was notable only for cancer of the prostate in black males and of
the corpus uteri in females under age 50. Cancer 2006;107(5 Suppl):1162–71.
� 2006 American Cancer Society.
KEYWORDS: colorectal neoplasms, second primary neoplasms, uterine neoplasms,ovarian neoplasms, stomach neoplasms, gastrointestinal neoplasms, pancreaticneoplasms, prostatic neoplasms, kidney neoplasms, breast neoplasms.
M ore effective screening and treatment regimens, coupled with
more cancer diagnoses because of an aging population, have
resulted in increasing numbers of cancer survivors who are at risk
for subsequent cancers.1 In 2002, there were an estimated 1.1 mil-
lion colorectal cancer survivors in the United States.2 The increased
risk of a second primary cancer among colorectal cancer patients,
when compared with the risk of persons without colorectal cancer,
may result from environmental or genetic factors shared between
the two cancers or from treatment effects.3,4 However, it is possible
that the intensive medical follow-up of colorectal cancer patients
may produce an artifactual association.3,4 A unidirectional altered
risk of a given cancer following colorectal cancer suggests a treat-
The findings and conclusions in this report arethose of the authors and do not necessarilyrepresent the views of the Centers for DiseaseControl and Prevention.
Address for reprints: Faruque Ahmed, PhD, Divi-sion of Cancer Prevention and Control, Centersfor Disease Control and Prevention, 4770 BufordHwy NE, MS K-53, Atlanta, GA 30341; Fax: (770)488-4759; E-mail: [email protected]
We appreciate the in-kind support from all the con-tributors to this monograph and also are grateful forthe contributions of Jessica King for the preparationof analytic files and to Faruque Ahmed for his lea-dership of the colorectal cancer monograph project.
Supported in part by the Centers for DiseaseControl and Prevention’s National Program ofCancer Registries.
Received March 2, 2006; accepted March 21,2006.
ª 2006 American Cancer SocietyDOI 10.1002/cncr.22013Published online 12 July 2006 in Wiley InterScience (www.interscience.wiley.com).
1162

ment effect or an artifactual association. A bidirec-
tional, mutually increased risk between two cancers
following each other suggests shared environmental
or genetic risk factors.4 Assessment of the risk of sub-
sequent primary cancers can facilitate strategies for
the prevention or early detection of second cancers.
Previous population-based studies on persons
with colorectal cancer, including those based on data
from one or more Surveillance, Epidemiology, and
End Results (SEER) cancer registries, have reported
increased risks of subsequent noncolonic primary
cancers of the stomach, small gut, gallbladder, pan-
creas, kidney, urinary bladder, brain, thyroid, pros-
tate, breast, corpus uteri, cervix uteri, and ovary.5–19
However, results have not been consistent, and there
is little information specific to race and ethnicity.
Most investigations have been small, and it is diffi-
cult to reconcile disparate findings because of differ-
ences in population characteristics, environmental
factors, and cancer management practices across
countries; differences in case-ascertainment, report-
ing, follow-up, and coding practices; and differences
in the criteria for defining and including multiple
primary cancers. Some studies have included all
multiple primary cancers regardless of the time-lapse
between diagnoses, whereas others have excluded
cancers diagnosed on the same day or within 1, 2, 6
months, or 1 year of the index cancer. For this study,
we analyzed data from nine SEER cancer registries,
which consistently use SEER rules for reporting and
coding multiple primary cancers.20 Our objectives
were 1) to ascertain the effect of using various inclu-
sion criteria on the excess risk of subsequent nonco-
lonic primary cancers among persons with colorectal
carcinoma and 2) to assess the excess risk of subse-
quent cancers among population subgroups.
MATERIALS AND METHODSDataThe SEER Program collects data on age, year of
diagnosis, sex, race, tumor characteristics, and other
variables among cancer cases diagnosed in the geo-
graphic areas it covers.21 Nine registries have contrib-
uted data to the National Cancer Institute’s SEER
database since 1975: Connecticut, Hawaii, Iowa, New
Mexico, Utah, Atlanta, Detroit, San Francisco-Oak-
land, and Seattle-Puget Sound.22 These SEER regis-
tries cover about 9% of the U.S. white population and
8% of the black population.23 As described previously,
all cancer patients in the SEER Program are actively
followed according to standard methods.24 Lympho-
mas of the colorectum and other sites, which are
categorized separately according to the SEER site
recodes, were excluded from our study.25 Multiple pri-
mary cancers are defined by the SEER Program as
tumors diagnosed �2 months apart, regardless of his-
tology or site, and tumors diagnosed within 2 months
of each other if they are of different histologies or if
they arise at different sites. The detailed guidelines on
identifying multiple primaries, including the excep-
tions to these general rules, are provided in the SEER
Program code manual.20 Extensions, recurrences, or
metastases of a single primary are not considered
new primaries. For comparability of stage at diagnosis
over time, we used SEER historic stage.26
Index CasesA total of 279,313 first primary invasive colorectal
cancer cases were recorded between 1975 and 2001
in the nine SEER registries. These cases did not have
prior in situ or invasive reported cancers of any site.
We excluded 16,713 (6%) cases that were a) identified
by death certificate or autopsy only, b) not microsco-
pically confirmed, c) not classified as carcinomas,27
or d) categorized as carcinoids (International Classifi-
cation of Diseases for Oncology, third edition, ICD-
O-3, histology codes 8240–8246, 8249).28 Thus, there
were 262,600 eligible index cases of colorectal carci-
noma.
Subsequent Primary CancersOn the basis of significant associations reported in
�1 previous studies (see earlier-mentioned text), we
assessed the excess risk of subsequent invasive pri-
mary cancers at 13 noncolonic sites. Because pre-
vious studies have shown no association between
colorectal and esophageal cancer, we included eso-
phagus as a control site. The subsequent cancers
included death certificate- and autopsy-only cases,
nonmicroscopically confirmed cases, and cancers of
any histologic type. Death certificate-only cases
accounted for �1% of cancers at each site. Autopsy-
only cases represented 14% of thyroid cancers, 4% of
kidney cancers, 3% of gallbladder cancers, 2% of
prostate and pancreatic cancers, and �1% of the
other cancers. Microscopic confirmation rates were
�95% for cancer sites other than kidney (87%), brain
(78%), and pancreas (72%). Carcinoids accounted for
45% of small gut cancers and �1% of cancers at the
other sites. We conducted sensitivity analysis by vary-
ing the definitions of subsequent primary and index
cancers to assess the robustness of our findings.
Statistical AnalysisDetection of a second primary for a given individual
did not preclude the counting of a subsequent pri-
mary cancer at another site. However, repeated pri-
Multiple Primary Cancers/Ahmed et al. 1163

mary cancers of the same noncolonic site were
excluded. Person-years (PY) at risk for subsequent
development of cancers were computed for each
noncolonic site from the date of diagnosis of colorec-
tal carcinoma to the date of diagnosis of the nonco-
lonic cancer, date of death, date of loss to follow-up,
or end of the study period (December 31, 2001),
whichever was earlier. The expected number of each
noncolonic cancer among index cases was calculated
by multiplying PY (stratified by sex, race, and 5-year
intervals of age and calendar year) by the strata-spe-
cific cancer incidence rates of the corresponding
sites for the population covered by the nine SEER
registries and then summing. The ratio of the
observed (O) to the expected (E) number denotes the
standardized incidence ratio (SIR). The SIR is an esti-
mate of the relative risk—adjusted for age, sex, race,
and calendar year—of developing cancer in colorec-
tal carcinoma patients when compared with that of
persons without colorectal carcinoma.
For assessing the effect of various inclusion cri-
teria, we chose the cutoffs of 0, 1, 2, 6, and 12
months that were used in previous studies.5–19 SIRs
by time since diagnosis of the index cancer were
based on the appropriate PY. Subsequent cancers
that were reported within the first 2 months of diag-
nosis of the index cancer were termed synchronous,
whereas cancers reported �2 months after the index
diagnosis date were termed metachronous. For sensi-
tivity analysis, the expected number of subsequent
cancers was computed using the same case defini-
tion as that of the observed subsequent cancer. For
determining whether SIRs differed from 1, statistical
significance was assessed with an a level of 0.05 (2-
sided) on the basis of the assumption that O fol-
lowed a Poisson random distribution.29 Because a
high SIR for a rare noncolonic cancer may not trans-
late into a high cancer burden, we also computed
the absolute excess risk per 10,000 PY (AER) using
the formula ‘[(O – E) 7 PY] � 10,000.’ SEER*Stat
software was used for the analysis.30
RESULTSIndex Case CharacteristicsAmong the 262,600 eligible index cases of colorectal
carcinoma, 51% involved males and 86% involved
whites (Table 1). Male and female index cases were
similar with respect to race, year of diagnosis, histo-
logic type, and stage at diagnosis (Table 1). However,
female index cases were more likely to be older and
to have tumors in the colon than males. The average
age at diagnosis of colorectal carcinoma was 68 years
for males and 71 years for females. The average PYs
of follow-up were 5.2 for males and 5.5 for females,
with 36% of males and 38% of females followed for
�5 years.
Excess Risk by Follow-Up PeriodThe excess risk of subsequent cancers was substan-
tially higher within the first 2 months of follow-up
than in later periods (Tables 2 and 3). For metachro-
nous cancers, small gut cancer showed significantly
elevated SIRs for all follow-up intervals (Tables 2 and
3). The SIR for stomach cancer was significantly ele-
vated after an interval of 60 months. Cancers of the
prostate and female breast showed significantly ele-
vated SIRs during the follow-up period of 2–5
months, whereas corpus uteri cancer showed signifi-
cantly elevated SIRs for the follow-up intervals 12–59
and �60 months.
Effect of Using Various Cutoffs for IncludingSubsequent CancersCancer sites some showed significantly increased SIRs
only when cancers reported during the first 1 or 2
TABLE 1Features of Index Cases of Colorectal Carcinoma,SEER Program, 1975–2001
VariableMale, %(n = 133,004)
Female, %(n = 129,596)
Race
White 85.8 86.2
Black 7.3 8.4
Other 6.7 5.2
Unknown 0.3 0.2
Age at diagnosis (yr)
<50 7.5 6.8
50–64 29.5 22.9
�65 63.0 70.3
Year of diagnosis
1975–1987 46.1 46.7
1988–2001 53.9 53.3
Subsite
Colon 67.3 74.1
Rectum 32.7 25.9
Histology*
Adenocarcinoma 98.2 97.9
Epidermoid carcinoma 0.2 0.4
Other specified carcinomas 0.2 0.2
Carcinoma, not otherwise specified 1.4 1.5
Stage at diagnosisy
Localized 37.9 36.6
Regional 38.1 40.2
Distant 19.6 19.0
Unstaged 4.4 4.3
Average person-years of follow-up 5.2 5.5
SEER: Surveillance, Epidemiology, and End Results.
* Classified using Berg’s principal histologic grouping for digestive cancers.27
y SEER Historic Stage.26
1164 CANCER Supplement September 1, 2006 / Volume 107 / Number 5

months of follow-up were included; the sites were
urinary bladder, thyroid, prostate, female breast, cer-
vix, and ovary (Table 4). Kidney cancer showed no
increased risk when cancers occurring during the
first year of follow-up were excluded. Cancer sites
with significantly increased SIRs regardless of the in-
clusion criteria were stomach (males), small gut, and
corpus uteri. Cancer sites that showed no elevated
risk, regardless of the criteria used, were esophagus,
gallbladder, pancreas, and brain. A significant protec-
tive association was found for gallbladder cancer
when synchronous cancers were excluded. The effect
of using various cutoffs (Table 4) was marked when
synchronous cancers, particularly those reported
during the first month of follow-up, were included.
Relative Excess Risk of Metachronous CancerSIRs for metachronous cancers were significantly ele-
vated for stomach (males), small gut, kidney, and
corpus uteri (Table 4). For small gut cancers, SIRs
were substantially higher for noncarcinoids (4.18 for
males and 4.91 for females) than carcinoids (1.52 for
males and 1.54 for females) (data not shown); approx-
imately 92% of the noncarcinoid small gut cancers
were adenocarcinomas.
SIRs for selected cancers by race, age at diagno-
sis, colon and rectum subsite, and year of diagnosis
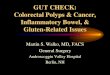
of the index case are shown in Figures 1–4. Blacks,
but not whites, were at a significantly elevated risk of
prostate cancer (SIR, 1.26; P < .05). Among persons
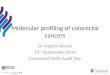
aged <50 years, SIRs were significantly elevated for
cancers of the stomach (males), small gut, pancreas,
kidney (males), corpus uteri, and ovary. Prostate can-
cer showed a significantly elevated association with
colon cancer but a protective association with rectal
cancer. The results were generally similar for the
1975–1987 and 1988–2001 diagnosis years. For meta-
chronous breast cancer, no significant associations
were seen in any of the subgroup analyses (data not
shown). For urinary bladder cancer, a significantly
elevated risk was found only among black males
TABLE 2Subsequent Primary Cancers among Colorectal Carcinoma Patientsby Time since Initial Diagnosis, Males, SEER Program, 1975–2001
Subsequent
primary
cancer
Follow-up period (mo)
Synchronous Metachronous
<1 1 2–5 6–11 12–59 �60
Esophagus SIR 4.57* 2.40 0.73 0.74 0.95 0.98
O 14 7 8 11 78 101
Stomach SIR 8.30* 3.04* 1.04 1.06 1.06 1.20*
O 52 18 23 32 175 242
Small gut SIR 161.56* 57.16* 6.76* 3.70* 3.17* 2.38*
O 107 36 16 12 58 58
Gallbladder SIR 18.92* 13.38* 3.58* –y – 0.44*
O 9 6 6 – – 7
Pancreas SIR 7.79* 2.86* 0.76 0.53* 1.01 0.93
O 46 16 16 15 159 184
Urinary bladder SIR 4.74* 2.79* 1.27 1.00 1.03 0.96
O 79 44 75 81 474 578
Kidney SIR 23.43* 10.85* 3.71* 1.42 1.20* 1.00
O 111 49 63 33 156 167
Brain SIR – – – 0.70 0.82 0.78
O – – – 7 45 52
Thyroid SIR 8.42* – 2.34 1.72 1.11 1.01
O 6 – 6 6 21 22
Prostate SIR 5.39* 3.88* 1.36* 0.89* 0.95* 1.00
O 382 260 341 308 1861 2522
SEER: Surveillance, Epidemiology, and End Results; SIR: standardized incidence ratio; O: number of
observed cancers.
* SIR differs significantly from 1 (P < 0.05).y Dashes indicate that data are suppressed if there are <6 observed cancers.
TABLE 3Subsequent Primary Cancers among Colorectal Carcinoma Patientsby Time since Initial Diagnosis, Females, SEER Program, 1975–2001
Subsequent
primary
cancer
Follow-up period (mo)
Synchronous Metachronous
<1 1 2–5 6–11 12–59 �60
Esophagus SIR –* – – 1.67 1.15 1.02
O – – – 8 31 38
Stomach SIR 14.88y 1.97 0.79 0.78 1.07 1.24y
O 48 6 9 12 91 140
Small gut SIR 151.30y 39.12y 5.80y 2.98y 4.61y 2.51y
O 73 18 10 7 62 50
Gallbladder SIR 32.45y 9.13y – – 0.57y 0.71
O 30 8 – – 14 22
Pancreas SIR 5.76y 1.88 1.06 0.87 0.96 0.92
O 29 9 19 21 132 177
Urinary Bladder SIR 5.71y 2.78y 1.05 0.78 1.10 1.06
O 26 12 17 17 137 185
Kidney SIR 25.38y 14.71y 3.67y 1.02 1.21 0.98
O 56 31 29 11 74 85
Brain SIR – – 1.26 0.93 0.93 1.20
O – – 6 6 33 56
Thyroid SIR – 5.84y 1.82 – 1.07 1.25
O – 6 7 – 30 43
Breast SIR 4.97y 1.79y 1.18y 0.78y 1.01 0.97
O 192 66 164 147 1043 1313
Cervix uteri SIR 11.82y – 1.01 1.52 0.97 0.96
O 23 – 7 14 46 49
Corpus uteri SIR 6.31y 2.47y 0.91 0.95 1.16y 1.27y
O 56 21 29 41 267 357
Ovary SIR 23.32y 4.24y 0.51y 1.38 1.11 0.83y
O 115 20 9 33 146 141
SEER: Surveillance, Epidemiology, and End Results; SIR: standardized incidence ratio; O: number of
observed cancers.
* Data are suppressed if there are < 6 observed cancers.y SIR differs significantly from 1 (P < 0.05).
Multiple Primary Cancers/Ahmed et al. 1165

(SIR, 1.37; P < .05) (data not shown). Metachronous
cancers of the gallbladder, brain, thyroid, and cervix
were too few to conduct meaningful subgroup analysis.
Absolute Excess Risk of Metachronous CancerThe AER of metachronous cancer was greatest for
small gut in males (1.44) and corpus uteri in females
(1.58) (Fig. 5). Substantially higher AERs were ob-
served for certain population subgroups (Figs. 1,2).
The highest AERs were for prostate cancer among
black males (26.48) and for corpus uteri cancer
among females aged <50 years (9.53). Among black
males, the AER of prostate cancer was elevated for
both colon and rectal index cancers (AERs of 30.43
TABLE 4Standardized Incidence Ratio (SIR) of Subsequent Primary Cancers Reported after Diagnosis of Colorectal Carcinomaby Follow-Up Interval, SEER Program, 1975–2001
Subsequent
primary cancer
Follow-up period (mo)
Male Female
�0 �1 �2 �6 �12 �0 �1 �2 �6 �12
Esophagus 1.01 0.96 0.94 0.95 0.96 1.10 1.10 1.10 1.12 1.08
Stomach 1.26* 1.15* 1.13* 1.13* 1.14* 1.32* 1.13 1.12 1.14 1.16*
Small gut 5.79* 3.68* 2.98* 2.79* 2.72* 5.73* 3.88* 3.45* 3.33* 3.36*
Gallbladder 0.99 0.73 0.56* 0.39* 0.42* 1.20 0.75* 0.64* 0.64* 0.65*
Pancreas 1.04 0.95 0.92 0.93 0.96 1.01 0.95 0.94 0.93 0.93
Urinary bladder 1.08* 1.03 1.00 0.99 0.99 1.14* 1.08 1.06 1.06 1.08
Kidney 1.67* 1.37* 1.24* 1.11* 1.09 1.68* 1.37* 1.20* 1.07 1.08
Brain 0.78* 0.77* 0.78* 0.79* 0.80* 1.06 1.06 1.08 1.07 1.08
Thyroid 1.36* 1.25 1.18 1.11 1.06 1.29* 1.26* 1.19 1.16 1.17
Prostate 1.09* 1.03 0.99 0.97* 0.98 – – – – –
Breast – – – – – 1.05* 0.99 0.98 0.97 0.99
Cervix uteri – – – – – 1.22* 1.04 1.01 1.01 0.97
Corpus uteri – – – – – 1.28* 1.20* 1.19* 1.20* 1.22*
Ovary – – – – – 1.31a 1.00 0.96 0.98 0.95
SEER: Surveillance, Epidemiology, and End Results.
* SIR differs significantly from 1 (P < 0.05).
FIGURE 1. Standardized incidenceratio (SIR) and absolute excess risk
(AER) of selected metachronous can-
cers by race, SEER Program, 1975--
2001. SIR represents the ratio of the
observed (O) to the expected (E) num-
ber of subsequent cancers, adjusted
simultaneously for age, sex, race, and
calendar year. AER denotes O � E
per 10,000 person-years of follow-up.
1166 CANCER Supplement September 1, 2006 / Volume 107 / Number 5

and 14.38, respectively), as well as for all age groups
(11.26, 26.00, and 32.52 for the <50, 50–64, and �65
age groups, respectively) and for the 1975–1987 and
1988–2001 diagnosis years (29.30 and 23.06, respec-
tively) (data not shown).
The substantial burden of prostate cancer among
black males and corpus uteri cancer in younger (aged
<50 years) females persisted beyond 5 years of the
index diagnosis date; AERs for the follow-up period of
�60 months were 36.15 and 11.22 for cancers of the
prostate and corpus uteri, respectively (data not
shown). Analysis by attained age (i.e., age at diagnosis
of the subsequent cancer) showed that the elevated
AER of corpus uteri cancer among females aged <50
years was found up to the attained age of 60 years (for
the attained age categories of<45, 45–49, 50–54, 55–59,
and �60 years, AERs were 11.57, 10.42, 11.81, 13.31,
and�3.86, respectively) (data not shown).
FIGURE 2. Standardized incidenceratio (SIR) and absolute excess risk
(AER) of selected metachronous can-
cers by age at diagnosis of colorectal
carcinoma, SEER Program, 1975--2001.
SIR represents the ratio of the observed
(O) to the expected (E) number of sub-
sequent cancers. AER denotes O � E
per 10,000 person-years.
FIGURE 3. Standardized incidenceratio (SIR) and absolute excess risk
(AER) of selected metachronous can-
cers by subsite, SEER Program, 1975--
2001. SIR represents the ratio of the
observed (O) to the expected (E) number
of subsequent cancers. AER denotes O
� E per 10,000 person-years.
Multiple Primary Cancers/Ahmed et al. 1167

Sensitivity AnalysisRepeating the analysis after expanding the index case
definition to include all colorectal cancers (n ¼279,313) did not change the results (data not shown).
For subsequent cancers, excluding cancers diagnosed
by death certificate and autopsy only, or excluding non-
microscopically confirmed cancers, yielded similar
results with the exception that the risk of metachro-
nous stomach cancer among females was significantly
elevated in both sets of analysis (SIRs of 1.14 and 1.20,
respectively; P<.05) (data not shown).
Bidirectional AssociationFor assessing possible mechanisms of carcinogenesis,
we ascertained whether the associations were present
in the reverse direction (Table 5). There was a signifi-
cant association between corpus uteri cancer and
subsequent colorectal cancer, which was more pro-
nounced among persons aged <50 years (SIR, 3.06;
P < .05). For prostate cancer, there was a significantly
elevated risk of subsequent colorectal cancer among
black males. Among persons aged <50 years, an ele-
vated risk was found with ovarian cancer (SIR, 2.52;
P < .05); it was not possible to assess the association
with pancreatic cancer because of poor survival of
pancreatic cancer patients. For small gut cancer,
there appeared to be an excess risk of colorectal can-
cer for the noncarcinoid subgroup only. For stomach
or kidney cancer, no excess risks were found.
DISCUSSIONThe excess risk of synchronous cancers (i.e., cancers
reported within the first 2 months of follow-up) in
colorectal carcinoma patients was elevated for all
sites other than brain. For metachronous cancers,
increased excess risks were observed for stomach,
FIGURE 4. Standardized incidenceratio (SIR) and absolute excess risk
(AER) of selected metachronous can-
cers by year of diagnosis of colorectal
carcinoma, SEER Program, 1975–2001.
SIRs represent the ratio of the observed
(O) to expected (E) numbers of sub-
sequent cancers. AERs denote O � E
per 10,000 person-years.
FIGURE 5. Absolute excess risk of selected metachronous cancers, SEERProgram, 1975–2001.
1168 CANCER Supplement September 1, 2006 / Volume 107 / Number 5

small gut (particularly noncarcinoid tumors), kidney,
and corpus uteri cancers. Elevated excess risks for
additional sites were seen in certain population sub-
groups: pancreas and ovary in persons aged <50
years and prostate in black males. A protective asso-
ciation was found for gallbladder cancer. A bidirec-
tional association was seen for noncarcinoid small
gut cancer (males) and for cancers of the corpus
uteri, ovary, and prostate (black males). A substantial
excess burden was found for subsequent cancers of
the corpus uteri in younger females and prostate in
black males.
It is well documented that intensive medical scru-
tiny can result in an apparent increase in risk of subse-
quent cancers followed by a deficit.3,31 The elevated
risk of synchronous cancers among persons with col-
orectal carcinoma might have resulted from ‘lead time
bias’: through increased medical scrutiny, second
tumors were detected before they would normally
have become clinically apparent. Although the occur-
rence of multifocal cancers is biologically plausible, it
is more likely that direct extension of the index cancer
to adjacent organs was sometimes misclassified as a
new primary.2–34 This misclassification is probably
unlikely in our study because of the experienced staff
and high quality data of the SEER registries. Also, for
the two cancers diagnosed at the same time, it may be
arbitrary which is designated as the index cancer.29 To
reduce the possibility of artifactual association, some
investigators have excluded cancers diagnosed during
the first 6 or 12 months of follow-up. Excluding can-
cers detected during the early follow-up period may
bias the study towards the null.3 Our results were very
similar (with the exception of kidney cancer) for the 2-
month comparable to the 12-month cutoff.
There are certain potential limitations to our
study. First, possible underreporting of subsequent
cancers among index cases who moved outside of the
SEER areas could result in underestimation of excess
risks, particularly with increasing time since diagnosis
of the index cancer. However, the fact that SIRs for the
esophageal cancer control group were close to unity
suggests that such underreporting was likely minimal.
Second, it is plausible that persons with advanced col-
orectal carcinoma may have incomplete reporting of
subsequent cancers. Still, similar results were obtained
when the analysis was restricted to localized or regio-
nal stage index cancers (data not shown). Finally,
because of the large number of comparisons per-
formed, associations that have not been previously
reported should be considered suggestive.35
Previous population-based studies have typically
reported the relative excess risk (i.e., the SIR) of
developing subsequent primary cancers but have not
assessed the absolute excess risk.5–19 Some of these
studies have not differentiated between synchronous
and metachronous cancers. We believe that synchro-
nous cancers should be excluded to avoid possible
bias. For corpus uteri and small gut cancers, previous
studies have consistently reported elevated excess
risks.6,7,12,15,16,18 We extend these finding by reporting
that the association is stronger for noncarcinoid
small gut cancers and that younger female colorectal
carcinoma patients have a substantial excess burden
of corpus uteri cancer. For prostate cancer, certain
studies have reported an increased risk whereas
others have not; for studies reporting an increased
risk, a bidirectional association was not found or
reported.5,6,10,12,13,15,18 To our knowledge, our study is
the first to report that black colorectal carcinoma
patients have a higher excess risk of prostate cancer
and that the association is bidirectional. For ovarian
cancer,5,6,14,15,18 an increased excess risk has been
reported. For pancreatic cancer, some studies have
found an increased risk, but others have not.6,7,15,18
We found increased excess risks for ovarian and pan-
creatic cancers only among younger persons. An ear-
lier study reported a protective association with
gallbladder cancer, which is in accord with our find-
ing.7 Results have not been consistent for cancers of
the stomach,5,6,12,15,18 kidney,7,12,15,18 breast,5,12,15,18
cervix uteri,6,7,15,18 urinary bladder,5,6,12,15,18 brain,7,18,19
and thyroid.6,7,15 We found an elevated excess risk for
stomach cancer after a lag of 5 years and for kidney
cancer only during the early follow-up period. We
did not find elevated risks for cancers of the breast,
cervix uteri, urinary bladder, brain, and thyroid.
The elevated risk of metachronous cancers of the
corpus uteri, ovary, small gut, and pancreas may be
TABLE 5Standardized Incidence Ratio (SIR) of Metachronous ColorectalCancer by Site of First Cancer, SEER Program, 1975–2001
First cancer site Male Female
All ages
Stomach 1.01 1.04
Small gut 1.20 1.19
Carcinoid 0.60 1.08
Noncarcinoid 2.07* 1.35
Kidney 1.00 0.97
Corpus uteri – 1.05*
Age <50
Corpus uteri – 3.06*
Ovary – 2.52*
Blacks
Prostate 1.09* –
SEER: Surveillance, Epidemiology, and End Results.
* SIR differs significantly from 1 (P < 0.05).
Multiple Primary Cancers/Ahmed et al. 1169

attributed, in part, to genetic conditions such as her-
editary nonpolyposis colorectal cancer syndrome and
familial adenomatous polyposis, which are asso-
ciated with both multiple cancers and younger age.36
Acquired defects in mismatch repair genes may also
be involved.37 Hormonal factors may contribute to
the association between colorectal and corpus uteri
cancer.7 Similarly, dietary risk factors and obesity
may also account for the association of these two
malignancies.38 For prostate cancer, the elevated risk
in black men could be an artifact if black colorectal
carcinoma patients undergo more testing for prostate
cancer, which often remains asymptomatic, than do
black men in the general population. However, the
elevated risk was observed even before 1987, a time
when prostate-specific antigen screening for prostate
cancer was uncommon.39 Similar genetic mutations
have been reported in colorectal and prostate can-
cers, and saturated fat intake has been reported to
be a risk factor for both cancers.13 For kidney cancer,
the fact that the association was unidirectional and
that an elevated risk was found for the early follow-
up period only suggests that the elevated risk may be
an artifact. For stomach cancer, the finding of an ele-
vated risk after a lag of 5 years suggests that a treat-
ment-related effect may have a role.3 The risk of
gallbladder cancer could be reduced because gall-
bladders, particularly those containing gallstones, are
often removed at the time of colon cancer surgery.4
Our study has several implications. First, many
synchronous cancers were observed. Further research
is needed on the effect of early detection of concur-
rent cancers on survivorship. Second, increased risks
for metachronous cancers of the pancreas, ovary,
and prostate were seen in certain population sub-
groups only. This finding underscores the fact that
the composition of the study population can affect
the results. Third, the risks for metachronous cancers
of the female breast and cervix uteri were similar to
those risk levels in the general female population.
This observation emphasizes the importance of con-
tinued breast and cervical cancer screening in
women with colorectal carcinoma. Finally, although
significantly elevated relative excess risks were found
for several subsequent cancers, the absolute excess
risk was notable only for cancers of the prostate
among black males and the corpus uteri among
younger females. Our findings may be useful in the
formulation of strategies to improve survivorship.
REFERENCES1. Cancer survivorship––United States, 1971–2001. MMWR
Morb Mortal Wkly Rep. 2004;53:526–529.
2. Ries LAG, Eisner MP, Kosary CL, et al. SEER Cancer Statistics
Review, 1975–2002, Bethesda, MD: National Cancer Institute,
2005. Available at http://seer.cancer.gov/csr/1975_2002,
based on November 2004 SEER data submission, posted to
the SEERweb site 2005, accessed April 18, 2005.
3. Hemminki K, Boffetta P. Multiple primary cancers as clues
to environmental and heritable causes of cancer and mech-
anisms of carcinogenesis. IARC Sci Publ. 2004;157:289–297.
4. Su Y, Ahsan H, Neugut AI. The association between biliary
tract cancers and cancers of other sites. Am J Gastroenterol.
1999;94:2256–2262.
5. Buiatti E, Crocetti E, Acciai S, et al. Incidence of second
primary cancers in three Italian population-based cancer
registries. Eur J Cancer. 1997;33:1829–1834.
6. Enblad P, Adami HO, Glimelius B, Krusemo U, Pahlman L.
The risk of subsequent primary malignant diseases after
cancers of the colon and rectum. A nationwide cohort
study. Cancer. 1990;65:2091–2100.
7. Evans HS, Moller H, Robinson D, Lewis CM, Bell CM,
Hodgson SV. The risk of subsequent primary cancers after
colorectal cancer in southeast England. Gut. 2002;50:647–
652.
8. Hoar SK, Wilson J, Blot WJ, McLaughlin JK, Winn DM,Kantor AF. Second cancer following cancer of the digestivesystem in Connecticut, 1935–82. Natl Cancer Inst Monogr.1985;68:49–82.
9. Lynge E, Jensen OM, Carstensen B. Second cancer follow-ing cancer of the digestive system in Denmark, 1943–80.Natl Cancer Inst Monogr. 1985;68:277–308.
10. Levi F, Randimbison L, Te VC, Rolland-Portal I, Franceschi S,
La Vecchia C. Multiple primary cancers in the Vaud Can-
cer Registry, Switzerland, 1974–89. Br J Cancer. 1993;67:391–
395.
11. Slattery ML, Mori M, Gao R, Kerber RA. Impact of familyhistory of colon cancer on development of multiple pri-maries after diagnosis of colon cancer. Dis Colon Rectum.1995;38:1053–1058.
12. Teppo L, Pukkala E, Saxen E. Multiple cancer––An epide-miologic exercise in Finland. J Natl Cancer Inst. 1985;75:207–217.
13. Moot AR, Polglase A, Giles GG, Garson OM, Thursfield V,Gunter D. Men with colorectal cancer are predisposed toprostate cancer. ANZ J Surg. 2003;73:289–293.
14. Crocetti E, Buiatti E, Falini P. Multiple primary cancer inci-
dence in Italy. Eur J Cancer. 2001;37:2449–2456.
15. McCredie M, Macfarlane GJ, Bell J, Coates M. Second pri-
mary cancers after cancers of the colon and rectum in
New South Wales, Australia, 1972–1991. Cancer Epidemiol
Biomarkers Prev. 1997;6:155–160.
16. Neugut AI, Santos J. The association between cancers of
the small and large bowel. Cancer Epidemiol Biomarkers
Prev. 1993;2:551–553.
17. Ahsan H, Neugut AI, Bruce JN. Association of malignantbrain tumors and cancers of other sites. J Clin Oncol.1995;13:2931–2935.
18. Hemminki K, Li X, Dong C. Second primary cancers aftersporadic and familial colorectal cancer. Cancer EpidemiolBiomarkers Prev. 2001;10:793–798.
19. Malmer B, Tavelin B, Henriksson R, Gronberg H. Primarybrain tumours as second primary: A novel association be-tween meningioma and colorectal cancer. Int J Cancer.2000;85:78–81.
20. National Cancer Institute. The SEER Program Code Manual,
3rd edn. Bethesda, MD: National Cancer Institute; 1998:7–
14.
1170 CANCER Supplement September 1, 2006 / Volume 107 / Number 5

21. Jackson-Thompson J, Ahmed F, German RR, Lai S, Friedman
C. Descriptive epidemiology of colorectal cancer in the Uni-
ted States, 1998–2001. Cancer 2006;107(5 Suppl):1103–1111.
22. SEER*Stat Database: Incidence-SEER 9 Regs Public-Use,
Sub (1973–2001) [computer program], version released
April 2004 (based on the November 2003 submission),
National Cancer Institute, DCCPS, Surveillance Research
Program, Cancer Statistics Branch, 2004.
23. Frey CM, McMillen MM, Cowan CD, Horm JW, Kessler LG.
Representativeness of the surveillance, epidemiology, and
end results program data: Recent trends in cancer mortal-
ity rates. J Natl Cancer Inst. 1992;84:872–877.
24. Inskip PD. Multiple primary tumors involving cancer of the
brain and central nervous system as the first or subsequent
cancer. Cancer. 2003;98:562–570.
25. SEER Site Recode ICD-O-3 (1/27/2003) Definition, National
Cancer Institute, 2003. Available at http://seer.cancer.gov/
siterecode/icdo3_d01272003, accessed July 8, 2005.
26. SEER Summary Staging Manual 2000: Codes and Coding
Instructions. Bethesda, MD: National Cancer Institute;
2001.
27. Histology of cancer incidence and prognosis: SEER popula-
tion-based data, 1973–1987 (dedicated to Dr. Harold LS).
Cancer. 1995;75(1 Suppl):139–421.
28. World Health Organization. International Classification of
Diseases for Oncology, 3rd edn. Geneva, Switzerland: World
Health Organization; 2000.
29. Schoenberg BS, Myers MH. Statistical methods for studying
multiple primary malignant neoplasms. Cancer. 1977;40(4
Suppl):1892–1898.
30. Surveillance Research Program, National Cancer Institute.
SEER*Stat software (www.seer.cancer.gov/seerstat) version
6.1.4. [computer program], Bethesda, MD: National Cancer
Institute, 2005.
31. Hemminki K, Li X. Familial carcinoid tumors and subse-
quent cancers: A nation-wide epidemiologic study from
Sweden. Int J Cancer. 2001;94:444–448.
32. Boice JD Jr, Storm HH, Curtis RE, et al. Introduction to the
study of multiple primary cancers. Natl Cancer Inst
Monogr. 1985;68:3–9.
33. Schottenfeld D. Multiple primary cancers. In: Schottenfeld
D, Fraumeni JF, eds. Cancer Epidemiology and Prevention,
2nd edn. New York: Oxford University Press; 1996: 1370–1387.
34. Schoenberg BS, Christine BW. The association of neo-
plasms of the colon and rectum with primary malignancies
of other sites. Am J Proctol. 1974;25:41–58.
35. Rothman KJ. Fundamentals of epidemiologic data analysis.
In: Rothman KJ, ed. Modern Epidemiology. Boston: Little,
Brown; 1986:147–150.
36. Lynch HT, de la CA. Hereditary colorectal cancer. N Engl J
Med. 2003;348:919–932.
37. Shureiqi I, Cooksley CD, Morris J, Soliman AS, Levin B,
Lippman SM. Effect of age on risk of second primary color-
ectal cancer. J Natl Cancer Inst. 2001;93:1264–1266.
38. Potter J. Epidemiologic, environmental, and lifestyle issues
in colorectal cancer. In: Young GP, Rozen P, Levin B, eds.
Prevention and Early Detection of Colorectal Cancer. Phila-
delphia: Saunders; 1996, 23–24.
39. Mettlin CJ, Murphy GP. Why is the prostate cancer death rate
declining in the United States? Cancer. 1998;82:249–251.
Multiple Primary Cancers/Ahmed et al. 1171