Embed Size (px)
Citation preview
Examination of the Thorax and Lungs
Janet M.Galiczewski Janet M.Galiczewski RN,CCRN, MSN, ANPRN,CCRN, MSN, ANP
Thorax and Lungs
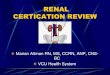
Thoracic cageThoracic cage is a bony structure defined by the is a bony structure defined by the sternum: 12 pairs of ribs, 12 thoracic vertebrae.sternum: 12 pairs of ribs, 12 thoracic vertebrae.
Floor is the Floor is the diaphragm diaphragm (musculotendinous (musculotendinous septum separates the thoracic cavity from septum separates the thoracic cavity from abdomen).abdomen).
First seven ribs attach directly to the sternum via First seven ribs attach directly to the sternum via costal cartilages. Ribs 8, 9, 10 attach to costal costal cartilages. Ribs 8, 9, 10 attach to costal cartilage above. Ribs 11 & 12 “floating” with free cartilage above. Ribs 11 & 12 “floating” with free palpable tips costochondral junctions are points palpable tips costochondral junctions are points where ribs join their cartilages (not palpable).where ribs join their cartilages (not palpable).
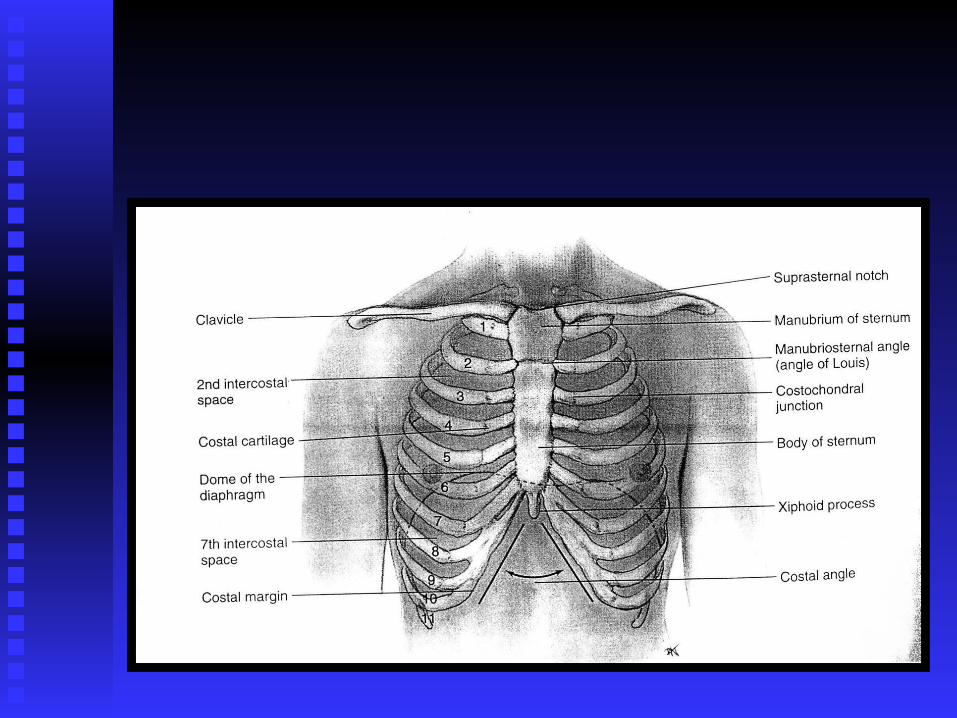
Anterior Landmarks
Suprasternal Notch:Suprasternal Notch: “U” shaped “U” shaped depression above sternum-between depression above sternum-between clavicles.clavicles.
Sternum:Sternum: “Breastbone” 3 parts: “Breastbone” 3 parts: Manubrium, Body, Xiphoid ProcessManubrium, Body, Xiphoid Process ““Angle of Louis” Marks site of tracheal Angle of Louis” Marks site of tracheal
bifurcation into Right and Left main bifurcation into Right and Left main bronchi. Approximately 2.5 cm below bronchi. Approximately 2.5 cm below sternal notch.sternal notch.
Anterior Landmarks (Cont).
Costal Angle:Costal Angle: Right and Left costal margins form an angle Right and Left costal margins form an angle where they meet at the Xiphoid Process. where they meet at the Xiphoid Process. Usually 90 degrees or less, greater Usually 90 degrees or less, greater emphysema.emphysema.
Posterior Landmarks
Vertebra Prominens:Vertebra Prominens: Most bony spur Most bony spur protruding at the base of the neck. This is protruding at the base of the neck. This is the spinous process of C7.the spinous process of C7.
Thoracic Cavity Mediastinum:Mediastinum: Middle section of the thoraic Middle section of the thoraic
cavity-contains esophagus, trachea, heart, great cavity-contains esophagus, trachea, heart, great vesselsvessels
Pleural cavities:Pleural cavities: R & L lung R & L lung Lung BordersLung Borders:: Anterior chestAnterior chest: : ApexApex-highest point lung tissue. -highest point lung tissue.
2-4 cm above inner third clavicles. 2-4 cm above inner third clavicles. Base Base lower lower border, rests on diaphragm 6border, rests on diaphragm 6thth rib midclavicular. rib midclavicular.
LaterallyLaterally lung tissue goes from the apex of the lung tissue goes from the apex of the axilla down to the 7axilla down to the 7thth or 8 or 8thth rib. rib.
Lobes of the Lungs
Right lungRight lung shorter than left because of the liver. shorter than left because of the liver. Right lungRight lung has 3 lobes. has 3 lobes. Left lungLeft lung has 2 lobes. has 2 lobes. LobesLobes are stacked in diagonal sloping segments are stacked in diagonal sloping segments
separated by fissures that run obliquely throughout separated by fissures that run obliquely throughout the chest.the chest.
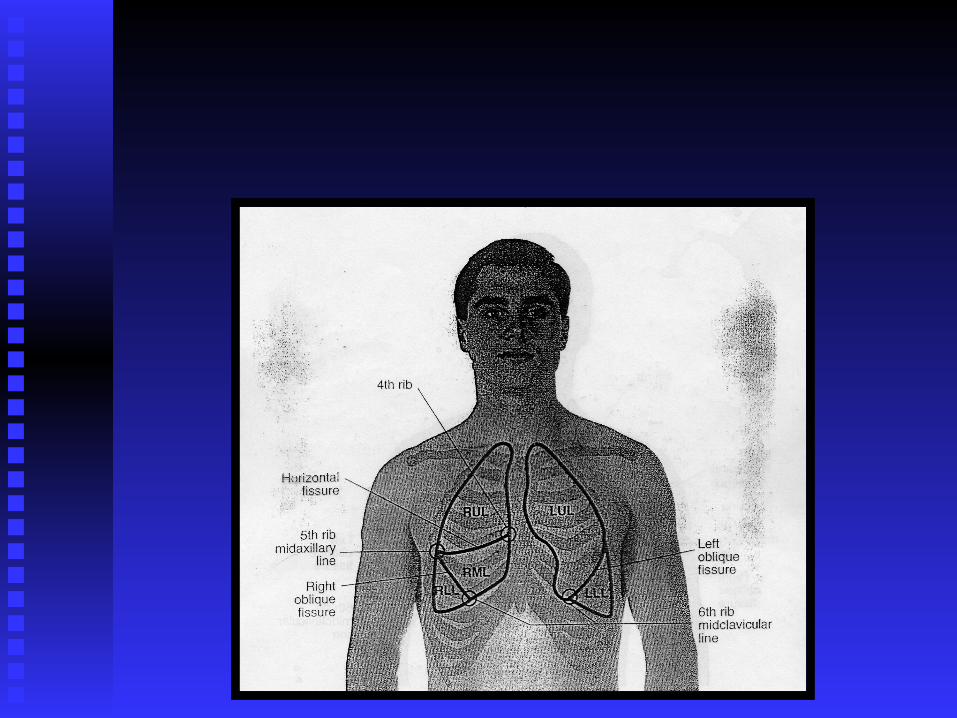
Anterior chestAnterior chest almost all upper and middle lobe almost all upper and middle lobe with very little lower lobe.with very little lower lobe.
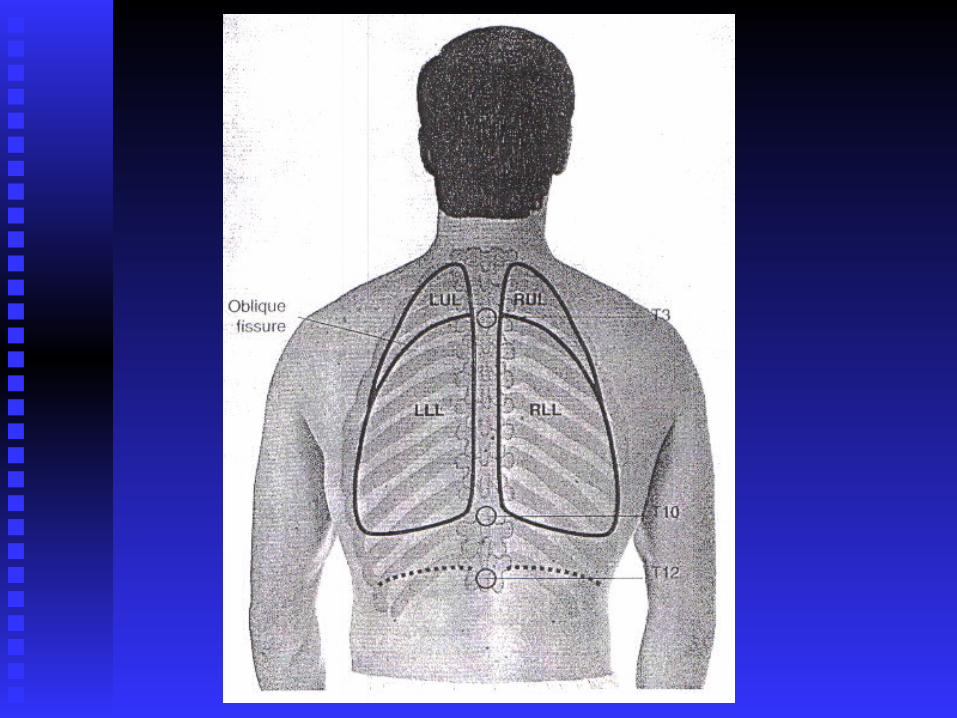
Posterior chestPosterior chest contains almost all lower lobe. contains almost all lower lobe.
Pleura of The Lungs
Parietal Pleura: Parietal Pleura: The outer lining of eachThe outer lining of each lung. It lung. It is attached to the chest wall.is attached to the chest wall.
Viseral Pleura:Viseral Pleura: The inner lining of each lung. It is The inner lining of each lung. It is attached to the lung itself.attached to the lung itself.
Pleural Space: Pleural Space: Is the space createdIs the space created between these between these two linings and it is filled with a small amount of two linings and it is filled with a small amount of lubricating fluid called lubricating fluid called Pleural Fluid.Pleural Fluid.
Negative PressureNegative Pressure holds lungs tightly against holds lungs tightly against chest wall and maintains inflation.chest wall and maintains inflation.
Trachea & Bronchial Tree TracheaTrachea is anterior to the esophagus & is anterior to the esophagus &
transports air to the bronchi.transports air to the bronchi. Bronchi Bronchi are large “air tubes” leading from are large “air tubes” leading from
the trachea that conducts air into lungs.the trachea that conducts air into lungs. Trachea & bronchiTrachea & bronchi transport gases transport gases
between environment and lung parenchyma.between environment and lung parenchyma. AlveoliAlveoli are the primary site of gas are the primary site of gas
exchange.exchange.
Mechanics of Respiration The The Mechanism of BreathingMechanism of Breathing maintains PH of maintains PH of
the blood by supplying oxygen & eliminating the blood by supplying oxygen & eliminating excess carbon dioxide.excess carbon dioxide.
With With InspirationInspiration the size of the thoracic container the size of the thoracic container increases creating a slightly negative pressure in increases creating a slightly negative pressure in relation to the atmosphere, air rushes in.relation to the atmosphere, air rushes in.
Major muscle responsible for this increase is the Major muscle responsible for this increase is the diaphragm.diaphragm.
InspirationInspiration – contraction of the diaphragm causes – contraction of the diaphragm causes it to descend and flatten.it to descend and flatten.
Expiration Expiration – passive, relaxation of the diaphragm– passive, relaxation of the diaphragm
Inspiration & Expiration
InspirationInspiration: Intercostal muscles lift the sternum : Intercostal muscles lift the sternum and elevate the ribs, diaphragm descends.and elevate the ribs, diaphragm descends.
ExpirationExpiration is primarily passive. As diaphragm is primarily passive. As diaphragm relaxes - it is forced to dome up.relaxes - it is forced to dome up.
This results in air flowing out due to positive This results in air flowing out due to positive pressure within the alveoli.pressure within the alveoli.
Respiratory centerRespiratory center in the brain stem (Pons & in the brain stem (Pons & medulla).medulla).
Normal stimulus to breathe is an increase in CO2 Normal stimulus to breathe is an increase in CO2 (Hypercapnia).(Hypercapnia).
Review Of Systems
Smoking HistorySmoking History Exposure to SmokeExposure to Smoke Environmental ExposuresEnvironmental Exposures OccupationOccupation Sleeping PatternSleeping Pattern Nutritional StatusNutritional Status Medical/Surgical HistoryMedical/Surgical History MedicationsMedications
Inspection
General AppearanceGeneral Appearance Restless or agitatedRestless or agitated Flaring nostrilsFlaring nostrils Supraclavicular retractionsSupraclavicular retractions Intercostal retractionsIntercostal retractions Use of accessory musclesUse of accessory muscles
Inspection (cont). Cyanosis:Cyanosis: Central Cyanosis:Central Cyanosis: Circumoral (around Circumoral (around
mouth), check lips, tongue, buccal mucosa.mouth), check lips, tongue, buccal mucosa. Peripheral Cyanosis:Peripheral Cyanosis: check nail beds and check nail beds and
extremities.extremities. Check nails for clubbing.Check nails for clubbing. Cough: Cough: productive or non-productiveproductive or non-productive Inspect appearance of Inspect appearance of sputum: sputum: Mucoid vs Mucoid vs
PurulentPurulent
Inspection (cont). Musculature: Musculature: Check accessory muscles: Check accessory muscles:
Sternomastoid, Intercostals, Scalene, Ala NasiSternomastoid, Intercostals, Scalene, Ala Nasi Symmetry:Symmetry: Check symmetrical expansion of Check symmetrical expansion of
chest wall.chest wall. Bilateral diminished expansion may be due to Bilateral diminished expansion may be due to
acute pleurisy, pleural fibrosis, atelectasis, chest acute pleurisy, pleural fibrosis, atelectasis, chest pain (fx. ribs), Costochondritis.pain (fx. ribs), Costochondritis.
Unilateral diminished expansion may be due to Unilateral diminished expansion may be due to pneumothorax.pneumothorax.
Check for asymmmetry of spine:Kyphosis, Check for asymmmetry of spine:Kyphosis, Lordosis, Scoliosis.Lordosis, Scoliosis.
Inspection (cont).
Configuration & Contour:Configuration & Contour: Check AP Check AP diameter (AP to transverse diameter).diameter (AP to transverse diameter). Abnormal:Abnormal:
Barrel chestBarrel chest
Pectus CarinatumPectus Carinatum
Pectus ExcavatumPectus Excavatum
Inspection (cont). Movement:Movement: Breathing patterns, smooth & even Breathing patterns, smooth & even
breathing.breathing.
Passive breathing:Passive breathing: normal rate12-20 normal rate12-20
Inspiration > Expiration Inspiration > Expiration
Check Character of Breathing: Check Character of Breathing: type, rate, type, rate, rhythmrhythm
ApneaApnea
Hyperventilation/TachypneaHyperventilation/Tachypnea
KussmaulKussmaul
Hypoventilation/respiratory depressionHypoventilation/respiratory depression
Cheyne Stoking/Dying SighsCheyne Stoking/Dying Sighs
Palpation
Trachea: Check for deviationTrachea: Check for deviation Thorax: Check for crepitus, tenderness.Thorax: Check for crepitus, tenderness. Check for chest wall excursionCheck for chest wall excursion Check for tactile or vocal Check for tactile or vocal
fremitus:Vibrations produced in the larynx fremitus:Vibrations produced in the larynx that are transmitted to the chest wall.that are transmitted to the chest wall. Technique: palpate with ball of handTechnique: palpate with ball of hand Ask Pt. to say “99”Ask Pt. to say “99”
Tactile fremitus (cont).
Normal finding is a mild purrlike sensation.Normal finding is a mild purrlike sensation. IncreasedIncreased tactile fremitius occurs in conditions tactile fremitius occurs in conditions
where solid conducts vibrations better than air. where solid conducts vibrations better than air. Ex. Pneumonia, tumor, pulmonary fibrosisEx. Pneumonia, tumor, pulmonary fibrosis
DecreasedDecreased tactile fremitus occurs when there is tactile fremitus occurs when there is increased distance that sound has to travel increased distance that sound has to travel before it reaches chest wall. Ex. Pleural before it reaches chest wall. Ex. Pleural Effusion, pneumothorax, COPD.Effusion, pneumothorax, COPD.
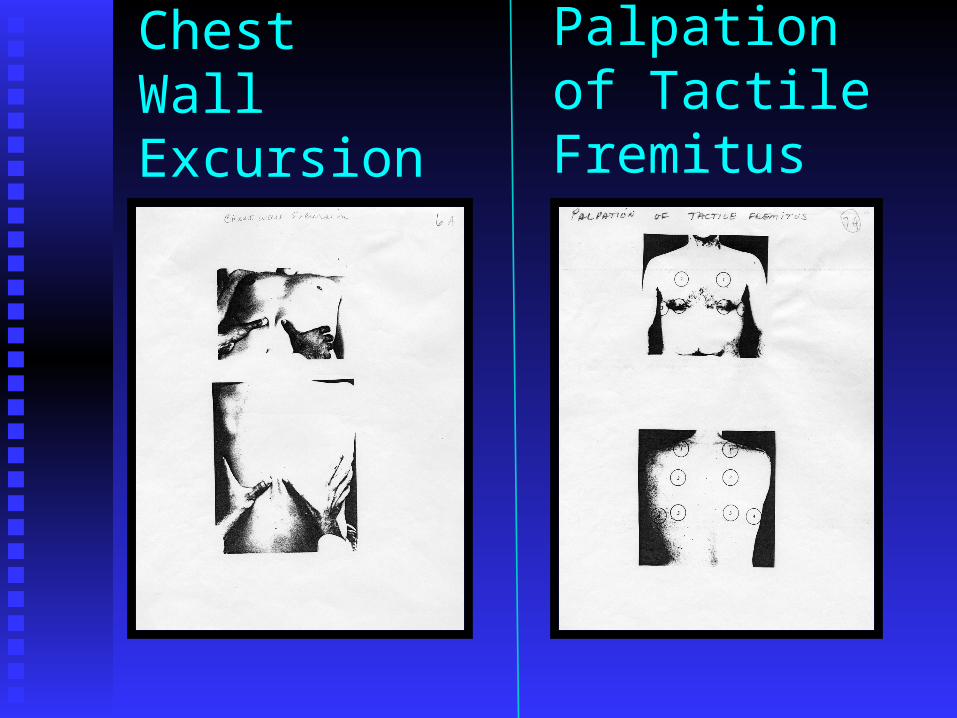
Chest Wall Excursion
Palpation of Tactile Fremitus
Palpation (cont).
Check supra & infraclavicular nodes,check Check supra & infraclavicular nodes,check axillary nodes.axillary nodes.
Percussion Percuss:Percuss: Anterior chest, lateral chest, Anterior chest, lateral chest,
posterior chestposterior chest NormalNormal:: ResonanceResonance AbnormalAbnormal:: Dullness - consolidation, atelectasis, pleural Dullness - consolidation, atelectasis, pleural
effusion.effusion. Hyperresonance -Hyperresonance -
pneumothorax,emphysema, asthma.pneumothorax,emphysema, asthma.
Percussion (cont).
Diaphragmatic Excursion:Diaphragmatic Excursion: Checks ROM Checks ROM of the diaphragm.of the diaphragm. Procedure: Pt. sits upright.Procedure: Pt. sits upright.
Tell Pt. To Tell Pt. To EXHALEEXHALE and and HOLD ITHOLD IT..Percuss downward posterior chest at Percuss downward posterior chest at
scapular line.scapular line.Continue until tone changes resonance Continue until tone changes resonance
to dullness, mark with marker.to dullness, mark with marker.
Diaphragmatic Excursion (cont).
Tell Pt. To take a Tell Pt. To take a DEEP INHALATION ANDDEEP INHALATION AND HOLD ITHOLD IT..
Continue percussing from first mark until changes Continue percussing from first mark until changes from resonance to dullness.from resonance to dullness.
Mark with a marker, measure findings. DON’T Mark with a marker, measure findings. DON’T FORGET TO TELL PT. TO BREATH!!!FORGET TO TELL PT. TO BREATH!!!
Normal finding 4-6 cm. Repeat on other side.Normal finding 4-6 cm. Repeat on other side.
Auscultation
Pt. sit upright, breathe slowly through Pt. sit upright, breathe slowly through mouth.mouth.
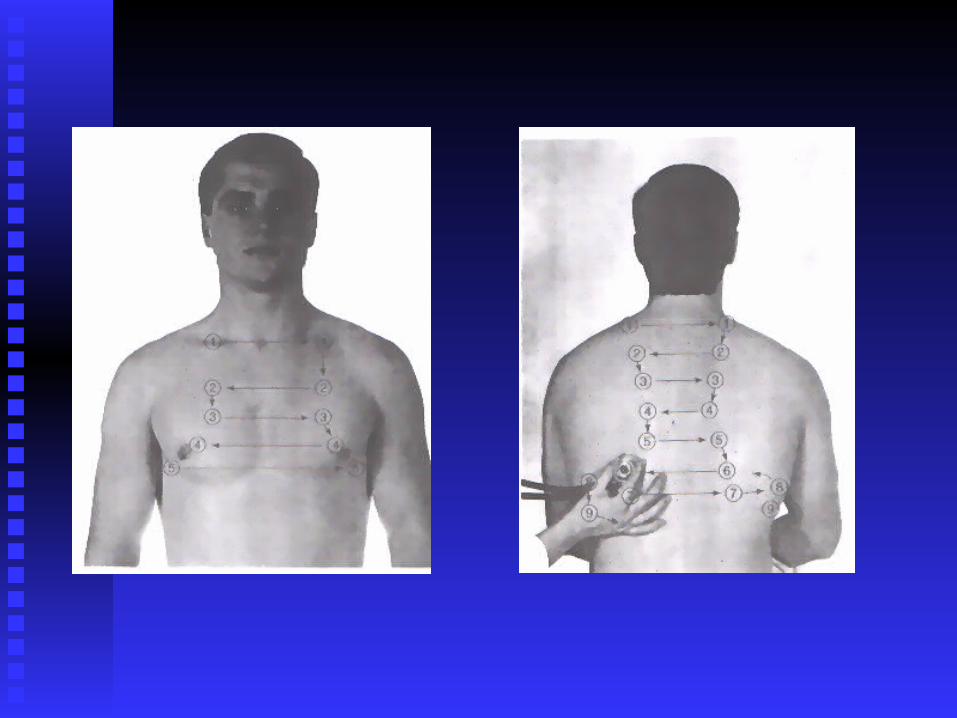
Use diaphragm.Use diaphragm. Auscultate anterior, lateral and posterior Auscultate anterior, lateral and posterior
chest.chest.
Types of Breath Sounds
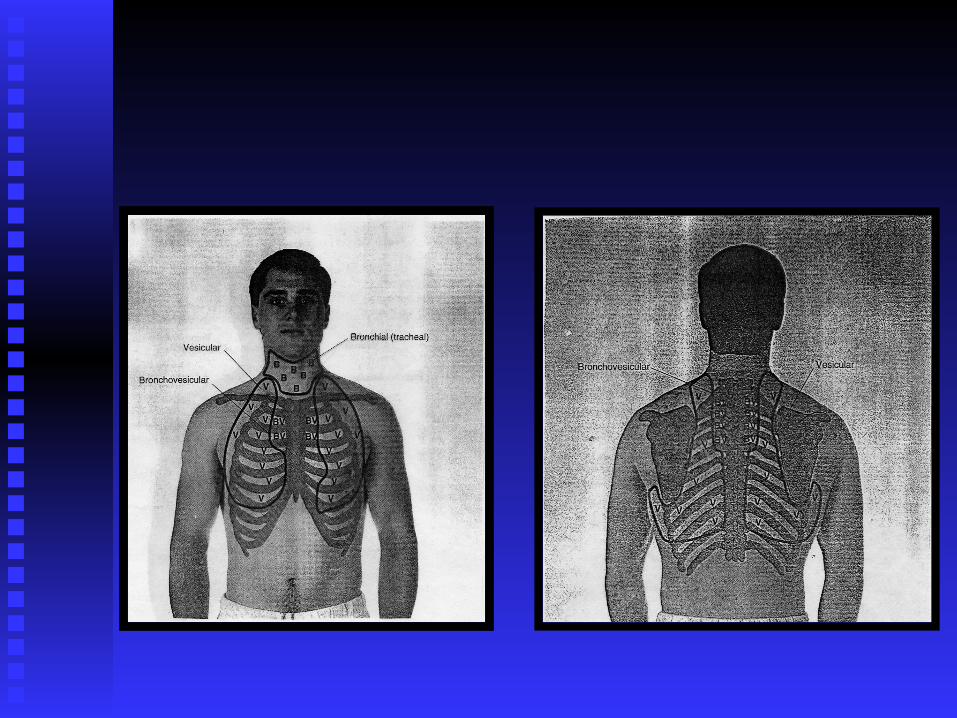
Vesicular Breath SoundsVesicular Breath Sounds Soft and low pitchedSoft and low pitched Fine rustling/swishing Fine rustling/swishing
sound.sound. Heard on inspiration Heard on inspiration
continuosly without pause continuosly without pause until expiration.until expiration.
Heard over all post. Lung Heard over all post. Lung fields and anterior periph. fields and anterior periph. Fields.Fields.
Inspiration> ExpirationInspiration> Expiration
Bronchial (Tracheal)Bronchial (Tracheal) Loud and high pitchedLoud and high pitched Tubular qualityTubular quality Expiration>InspirationExpiration>Inspiration Heard only anteriorly Heard only anteriorly
over trachea & larynxover trachea & larynx Expiration loudExpiration loud
Types of Breath Sounds
Bronchovesicular Breath SoundsBronchovesicular Breath Sounds Combination of vesicular and bronchial soundsCombination of vesicular and bronchial sounds Represent a mixture of sounds produced by Represent a mixture of sounds produced by
vibrations of bronchial and alveoli vibrations.vibrations of bronchial and alveoli vibrations. No pause between inspiration and expirationNo pause between inspiration and expiration Inspiration = ExpirationInspiration = Expiration Heard best anteriorly at 1&2 ICS, posteriorly Heard best anteriorly at 1&2 ICS, posteriorly
between scapula, anywhere else = consolidationbetween scapula, anywhere else = consolidation
Auscultation
DecreasedDecreased Breath Sounds: shallow Breath Sounds: shallow breathing, pleural effusion, COPD, breathing, pleural effusion, COPD, pneumothorax, asthma, atelectasis.pneumothorax, asthma, atelectasis.
IncreasedIncreased Breath Sounds:Consolidation- Breath Sounds:Consolidation-tumor, pneumonia.tumor, pneumonia.
Adventitious Sounds
Rales (Crackles):Rales (Crackles): Discontinuous sounds Discontinuous sounds highpitched.highpitched.
Sounds like hair being rubbed together Sounds like hair being rubbed together Sound produced by air passing through Sound produced by air passing through
fluid in air spaces (CHF, pneumonia).fluid in air spaces (CHF, pneumonia). Usually on inspiration / not expirationUsually on inspiration / not expiration Cough doesn’t clear.Cough doesn’t clear.
Adventitious Sounds (cont).
Rhonchi:Rhonchi: Deeper, rumbling sounds. Deeper, rumbling sounds. Low pitched, snoring qualityLow pitched, snoring quality > pronounced during expiration.> pronounced during expiration. Etiology: larger airways are obstructed with Etiology: larger airways are obstructed with
mucus or tumor in large airways.mucus or tumor in large airways. Clear with coughing.Clear with coughing.
Adventitious Sounds (cont). Wheezing:Wheezing: High pitched, musical, High pitched, musical,
whistling sounds.whistling sounds. Produced by narrowed airway.Produced by narrowed airway. R/t bronchospasm, asthma, tumor, foreign R/t bronchospasm, asthma, tumor, foreign
bodybody Can occur during inspiration or expiration.Can occur during inspiration or expiration. Stridor: Stridor: increased musical wheeze heard increased musical wheeze heard
over trachea on inspiration; cause over trachea on inspiration; cause obstruction = MEDICAL EMERGENCYobstruction = MEDICAL EMERGENCY
Adventitious Sounds (cont). Friction (Pleural) Rub:Friction (Pleural) Rub: Course, dry, grating Course, dry, grating
soundsound Etiology: Inflamed pleural surfaces rub.Etiology: Inflamed pleural surfaces rub. Sounds similar to cupping hand over ear, Sounds similar to cupping hand over ear,
scratching back of hand with other hand.scratching back of hand with other hand. Usually heard anteriolateral chest wallUsually heard anteriolateral chest wall Continuous during inspiration and expiration.Continuous during inspiration and expiration. Differentiate from cardiac origin: have Pt. hold Differentiate from cardiac origin: have Pt. hold
breath-if breath-if continues Cardiaccontinues Cardiac origin, if origin, if stops-Lungstops-Lung origin.origin.
Tests of Vocal Resonance BBRONCOPHONYRONCOPHONY: “99”: “99”
NL. Muffled soundNL. Muffled soundAbnormal: hear, clear loud “99” Abnormal: hear, clear loud “99”
(consolidation)(consolidation) WHISPERED PECTORILOQUAYWHISPERED PECTORILOQUAY
Whisper “99”Whisper “99”Normal-Don’t hear or very faintNormal-Don’t hear or very faintAbnormal hear “99” Abnormal hear “99”
EGOPHONYEGOPHONY Say “E” Say “E”Normal- hear “E”, Abnormal-hear “A”Normal- hear “E”, Abnormal-hear “A”