Embed Size (px)
Citation preview

6/1/2016
1
Evolving Trends in Cardiac Arrest
Michael W. Donnino, MDEmergency Medicine and Critical Care
Director of the Center for Resuscitation ScienceBeth Israel Deaconess Medical Center
Disclosures
• Consultant: Paid Consultant for the AHA
• Research Grants: AHA, NIH, Kaneka, General Electric, Bristol-Myers Squibb
• American Heart Association (paid and volunteer)• 2015 ACLS guidelines editor (paid)• Member, Research Task Force and Clinical – GWTG• Member, ACLS task force for ILCOR

6/1/2016
2
The 2015 ACLS Guidelines
• Focused update
• ILCOR � GRADE � AHA writing groups
• The path forward � ongoing continuous update
• Assessment sequence
• Chest compression rate and depth
• Advanced airway ventilation rate
• Targeted temperature management
• Vasopressors for resuscitation: vasopressin and epi
• Consideration of ECPR (not routine but in certain settings)
• Consideration of ETCO2 as one element of determining when to stop resuscitative efforts
• Neuroprognstication at 72 hours post TTM
• Timing of C-section “modifier”
Changes to ACLS Guidelines

6/1/2016
3
Philosophy of Changes• Keep things simple � removal of vasopressin from
algorithms, change in respiratory rate to avoid a range
• Recognize differences between arrest scenarios:• IN-hospital and OUT-of-hospital arrest � some split
recommendations, change in chain of survival, assessment sequence flexibility
• Different management for shockable and non-shockable
• More formalized and critical evaluation of the studies with GRADE approach and push to “try” to take a stand one way or another though often difficult…
NEW AHA ADULT CHAINS OF SURVIVAL
IN-HOSPITAL(note new Surveillance and Prevention link)
OUT-OF-HOSPITAL,Including EMS

6/1/2016
4
Philosophy of Changes• Keep things simple � removal of vasopressin from
algorithms, change in respiratory rate to avoid a range
• Recognize differences between arrest scenarios:• IN-hospital and OUT-of-hospital arrest � some split
recommendations, change in chain of survival, assessment sequence flexibility
• Different management for shockable and non-shockable
• More formalized and critical evaluation of the studies with GRADE approach and push to “try” to take a stand one way or another though often difficult…
The Pyramid of Learning
No Clue

6/1/2016
5
The Pyramid of Learning
No Clue
Know the “sound bite” or “rule”
The Pyramid of Learning
No Clue
Know the “sound bite” or “rule”
Know “the study”

6/1/2016
6
The Pyramid of Learning
No Clue
Know the “sound bite” or “rule”
Know “the study”
Literature
The Pyramid of Learning
No Clue
Know the “sound bite” or “rule”
Know “the study”
Literature
Clinical Practice

6/1/2016
7
Try Not to Live in the “Sound Bite” !!
No Clue
Know the “sound bite” or “rule”
Know “the study”
Literature
Clinical Practice
Perimortem Ceasarean Delivery (PMCD)
Sound Bite:

6/1/2016
8
Perimortem Ceasarean Delivery (PMCD)
Sound Bite: PMCD should be consideredat 4 minutes after onset of maternal cardiac arrest or resuscitative efforts (for the unwitnessed arrest) if there is no maternal ROSC
Perimortem Ceasarean Delivery (PMCD)
Sound Bite: PMCD should be consideredat 4 minutes after onset of maternal cardiac arrest or resuscitative efforts (for the unwitnessed arrest) if there is no maternal ROSC
Deeper Dive: The clinical decision to perform a PMCD—and its timing with respect to maternal cardiac arrest—is complex because of the variability in level of practitioner and team training, patient factors (e.g., etiology of arrest, gestational age of the fetus), and system resources.

6/1/2016
9
KEY AND UPDATED RECOMMENDATOINS:
BLS
ASSESSMENT SEQUENCE
• Check for responsiveness (tap and shout)
• Shout for nearby help upon finding a patient unresponsive/activate emergency response system/get AED
• Check breathing and pulse simultaneously
• Use defibrillator as soon as it is available

6/1/2016
10
CHEST COMPRESSION RATE: UPDATED
Recommendation: • Compression rate: 100-
120/minute(2010:at least 100/min)
Why? • Absolute number of
compressions delivered/minute linked with survival
• Actual compression rate often well below 100/minute
• Rates below 100/min or above 120/min adversely affect outcomes
MO2
ADULT CHEST COMPRESSION DEPTH: UPDATED
Recommendation: •Compress at least 2 inches (5cm) for average adult•Avoid excessive compression depth, i.e., greater than 2.4 inches (6cm)
Why? •Small study: more injuries with compressions greater than 2.4 inches (6cm). (Hellevuo et al, Resuscitation, 2013)
Note:•Difficult to judge depth without devices•Rescuers typically don’t “push hard” enough

Slide 19
MO2 Gen session slideMaureen Ortega, 11/23/2015

6/1/2016
11
ADVANCED AIRWAY VENTILATION RATE
• Deliver 1 breath every 6 seconds (10 breaths per minute) while continuous chest compressions are being performed
• Single rate for adults should be easier to learn, remember, and perform
MECHANICAL CHEST COMPRESSION DEVICES
Recommendation:• Manual chest compressions remain standard of care
over mechanical chest compression devices.
• Mechanical piston/compression devices may be a reasonable alternative to conventional CPR in specific settings (eg, where the delivery of manual compressions may be
challenging or dangerous to the provider).
Why?• Three large randomized trials comparing mechanical
chest compression devices to conventional CPR demonstrated survival similar to that with conventional CPR. Such devices may enable continuation of high-quality chest compressions in a vehicle or during PCI, etc.
6/1/2016
12
KEY NEW AND UPDATED
RECOMMENDATIONS:
ACLS
VASOPRESSORS FOR RESUSCITATION: VASOPRESSIN
• Vasopressin in combination with epinephrine offers no advantage as a substitute for standard-dose epinephrine in cardiac arrest
• Efficacy of the two drugs is similar, and there is no demonstrable benefit from administering both epinephrine and vasopressin as compared with epinephrine alone
• For simplicity, vasopressin has been removed from the algorithm

6/1/2016
13
VASOPRESSORS FOR RESUSCITATION: EPINEPHRINE
• Administer epinephrine as soon as feasible after the onset of cardiac arrest due to an initial nonshockable rhythm
• Association between early administration of epinephrine and increased ROSC, survival to hospital discharge, and neurologically intact survival
Epinephrine Versus Placebo
Jacobs et al. Resuscitation 82 (2011) 1138-1143.
“Patients receiving adrenaline during cardiac arrest had no statistically significant
improvement in the primary outcome of survival to hospital discharge although there was a
significantly improved likelihood of ROSC.”

6/1/2016
14
Epinephrine Versus Placebo
• Pre-hospital ROSC: 8.4% (placebo) vs 23.5% (epinephrine)
• ED to hospital admission: 13% (placebo) vs 25.4% (epinephrine)
• Hospital discharge: 1.9% (placebo) vs 4% (epi) [NS] (50% relative reduction in mortality though not enough patients for statistical significance – thus, caution with interpretation of “negative” trial)
Jacobs et al. Resuscitation 82 (2011) 1138-1143.
VF/VT versus PEA/asystole
Jacobs et al. Resuscitation 82 (2011) 1138-1143.

6/1/2016
15
Time To Epinephrine – PEA/Asystole
(Donnino et al. British Medical Journal 2014 )
(Donnino et al. British Medical Journal 2014 )
Time To Epinephrine – PEA/Asystole

6/1/2016
16
(Donnino et al. British Medical Journal 2014 )
Time To Epinephrine – PEA/Asystole
Figure 3. Time to epinephrine and survival
(Andersen et al., JAMA, 2015)
Time To Epinephrine – PEA/Asystole in pediatrics

6/1/2016
17
Very Early Epinephrine in VF/VT
)Early administration of epinephrine in patients with cardiac arrest and initial shockable rhythm. Andersen LW, Kurth T, Chase M, Berg KM, Cocchi MN, Callaway C, Donnino MW; BMJ. 2016 6;353
6/1/2016
18
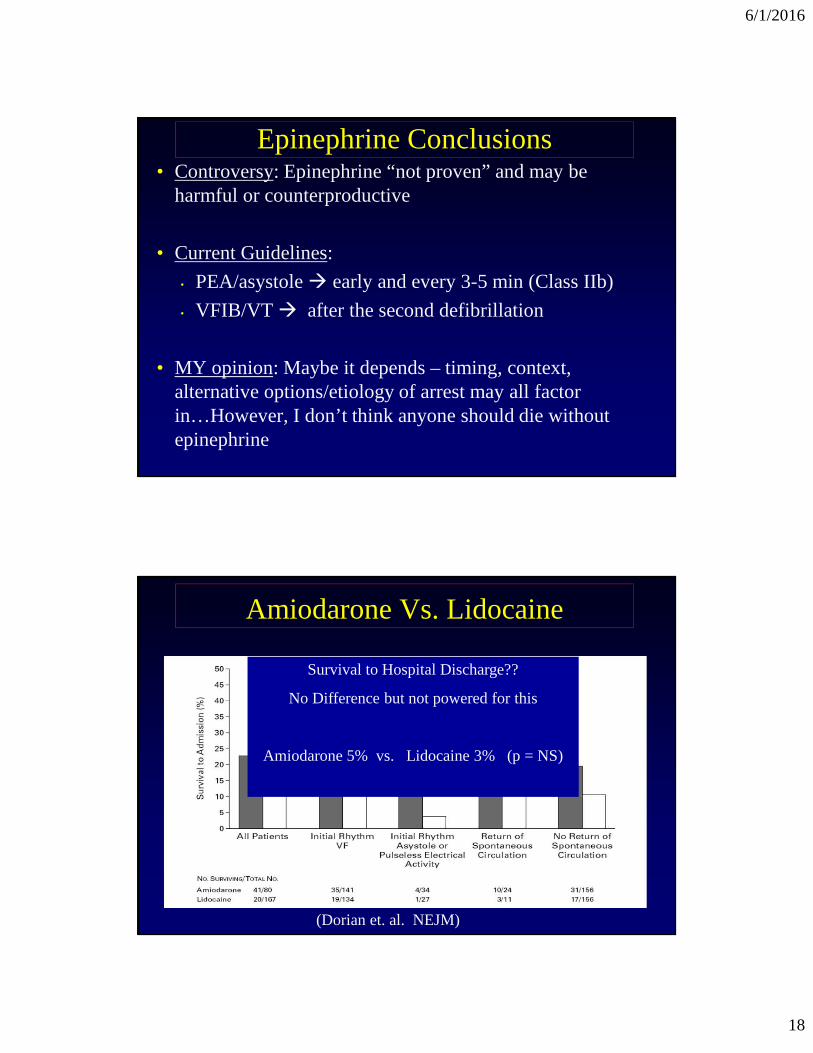
Epinephrine Conclusions• Controversy: Epinephrine “not proven” and may be
harmful or counterproductive
• Current Guidelines:
• PEA/asystole � early and every 3-5 min (Class IIb)
• VFIB/VT � after the second defibrillation
• MY opinion: Maybe it depends – timing, context, alternative options/etiology of arrest may all factor in…However, I don’t think anyone should die without epinephrine
Amiodarone Vs. Lidocaine
Survival to Hospital Discharge??
No Difference but not powered for this
Amiodarone 5% vs. Lidocaine 3% (p = NS)
(Dorian et. al. NEJM)

6/1/2016
19
Amiodarone vs. Lidocaine• Bottom Line: Amiodarone currently has “the
nod” but the study was small and had some flaws including provision of lipoprotein with deleterious effects to lidocaine group. Thus, giving lidocaine is acceptable alternative
• Currently, being reproduced with very large trial
Amiodarone vs. Lidocaine• Bottom Line: Amiodarone currently has “the
nod” but the study was small and had some flaws including provision of lipoprotein with deleterious effects to lidocaine group. Thus, giving lidocaine is acceptable alternative
• Currently, being reproduced with very large trial

6/1/2016
20
Amiodarone vs. Lidocaine• Bottom Line: Amiodarone currently has “the
nod” but the study was small and had some flaws including provision of lipoprotein with deleterious effects to lidocaine group. Thus, giving lidocaine is acceptable alternative
• Currently, being reproduced with very large trial
Amiodarone vs. Lidocaine

6/1/2016
21
LOW ETCO2 FOR PREDICTING FAILED RESUSCITATION
Recommendation:• In intubated patients, failure to achieve an ETCO2
greater than 10 mm Hg by waveform capnography after 20 minutes of CPR may be considered one component of a multimodal approach to decide when to end resuscitative efforts, but it should not be used in isolation
Why?• Failure to achieve an ETCO2 greater than 10 mm
Hg after 20 minutes has been associated with poor outcome in case series
A patient is unresponsive and in ventricular fibrillation. A shock is delivered. The team leader orders the continuation of 2 minutes of compressions but before the "compressor” begins, another member of the team detects a carotid pulse. In this case, you should:
a) Cease CPRb) Provide an additional 2 minutes of chest compressions but do not deliver any medications during this periodc) Provide an additional 2 minutes of chest compressions and consider providing 1 mg or epinephrine or 40 Units of vasopressind) Provide an additional 2 minutes of chest compressions and consider providing 300 mg of amiodaronee) Both 3 and 4

6/1/2016
22
CPR in patients with ROSC??
(Giberson, Journal of Intensive Care Medicine, 2014)

6/1/2016
23
Well, not everyone was happy…
2010 AHA Recommendations
Treatment Recommendation 1: “We recommend that comatose (i.e., lack of meaningful response to verbal commands) adult patients with ROSC after out-of-hospital VF cardiac arrest should be cooled to 32oC to 34oC for 12 to 24 hours”
(Class I, LOE B)

6/1/2016
24
2010 AHA Recommendations
Treatment Recommendation 2: “Induced hypothermia also may be considered for comatose adult patients with ROSC after out-of-hospital cardiac arrest with an initial rhythm of pulseless electric activity or asystole”
(Class IIb, LOE B)
Targeted Temperature Management (TTM)1 - Should we perform TTM?
- Shockable versus non-shockable rhythms- Out-of-hospital versus in-hospital
2 - If so, what temperature should we choose?
3 - If so, when should we start? Prehospital?
4 - How long should we go?
5 – What do we do about fever after TTM is done?

6/1/2016
25
Targeted Temperature Management (TTM)1 - Should we perform TTM?
- Shockable versus non-shockable rhythms- Out-of-hospital versus in-hospital
2 - If so, what temperature should we choose?
3 - If so, when should we start? Prehospital?
4 - How long should we go?
4 – What do we do about fever after TTM is done?

6/1/2016
26
Mortality
Neurologic
Study Limitations
1 – Non-blinded assessors
2 – One “pseudo-randomized”
3 – Unclear attention to temp management in the control arm
4 – No report of longer term neuro outcomes or granular neurologic outcomes

6/1/2016
27
ILCOR Recommendation
We recommend TTM as opposed to no TTM for adults with OHCA and initial shockable rhythm who remain
unresponsive after return of spontaneous circulation.
(Strong recommendation, low quality evidence)
ILCOR Recommendation
We suggest TTM as opposed to no TTM for adults with OHCA and initial non-shockable rhythm who remain unresponsive after return of spontaneous circulation.
(Weak recommendation, low quality evidence)

6/1/2016
28
ILCOR Recommendation
We suggest TTM as opposed to no TTM for adults with IHCA and any initial rhythm who remain unresponsive after
return of spontaneous circulation.
(Weak recommendation, low quality evidence)
Targeted Temperature Management (TTM)1 - Should we perform TTM?
- Shockable versus non-shockable rhythms- Out-of-hospital versus in-hospital
2 - If so, what temperature should we choose?
3 - If so, when should we start? Prehospital?
4 - How long should we go?
5 – What do we do about fever after TTM is done?

6/1/2016
29
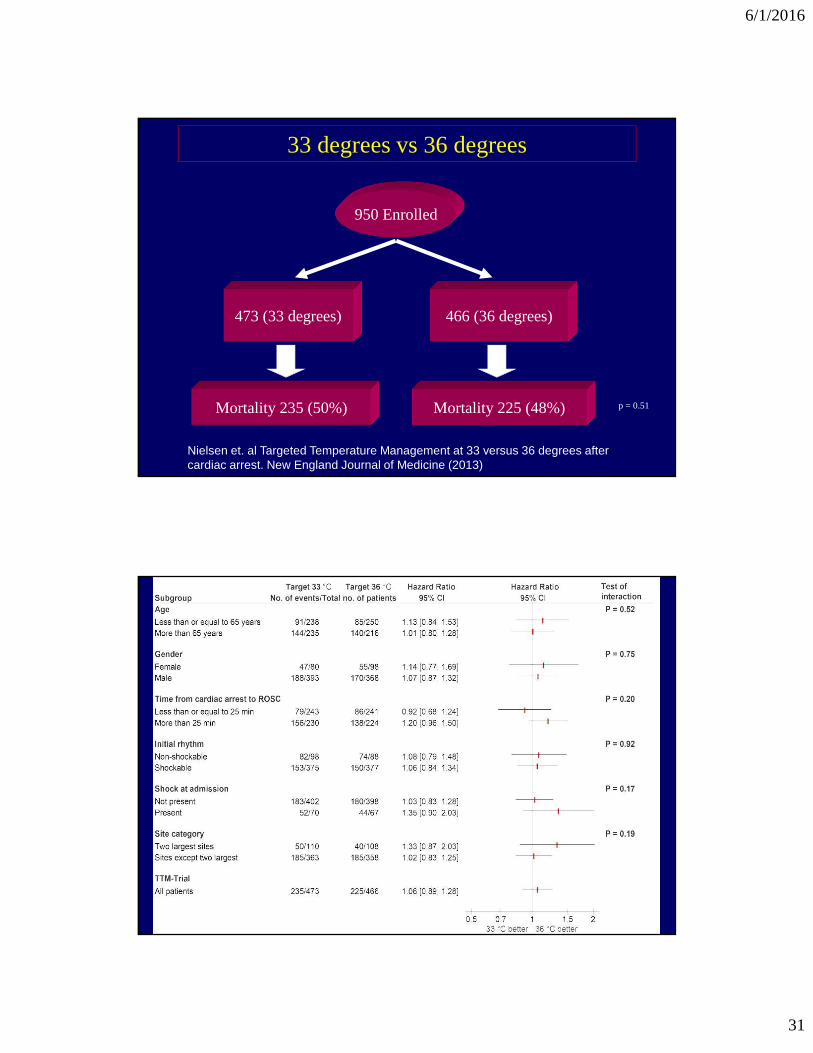
950 Enrolled
473 (33 degrees) 466 (36 degrees)
Mortality 235 (50%) Mortality 225 (48%) p = 0.51
33 degrees vs 36 degrees
950 Enrolled
473 (33 degrees) 466 (36 degrees)
Mortality 235 (50%) Mortality 225 (48%) p = 0.51
33 degrees vs 36 degrees

6/1/2016
30
950 Enrolled
473 (33 degrees) 466 (36 degrees)
Mortality 235 (50%) Mortality 225 (48%) p = 0.51
33 degrees vs 36 degrees
EQUALLY MATCHED GROUPS
950 Enrolled
473 (33 degrees) 466 (36 degrees)
Mortality 235 (50%) Mortality 225 (48%) p = 0.51
33 degrees vs 36 degrees
EQUALLY MATCHED GROUPS
Median Time BLS: 1 min [0-2] 1 min [0-2]
6/1/2016
31
950 Enrolled
473 (33 degrees) 466 (36 degrees)
Mortality 235 (50%) Mortality 225 (48%) p = 0.51
33 degrees vs 36 degrees
Nielsen et. al Targeted Temperature Management at 33 versus 36 degrees after cardiac arrest. New England Journal of Medicine (2013)
Other Differences• Hypotension criteria
• Rhythm inclusion differences
• Sedation/NMB strategies
• Targeted temperature control for 3 days (no fevers in all patients both groups in latest study)
• Follow-up protocol for neuro-prognostication

6/1/2016
32
Survival Curve Differences
Temperature Differences

6/1/2016
33
Temperature Differences
Other Differences• Hypotension criteria
• Rhythm inclusion differences
• Sedation/NMB strategies
• Targeted temperature control for 3 days (no fevers in all patients both groups in latest study)
• Follow-up protocol for neuro-prognostication

6/1/2016
34
Other Differences• Hypotension criteria
• Rhythm inclusion differences
• Sedation/NMB strategies
• Targeted temperature control for 3 days (no fevers in all patients both groups in latest study)
• Follow-up protocol for neuro-prognostication
ILCOR Recommendation
We recommend selecting and maintaining a constant target temperature between 32-36o Celsius for those for whom
TTM is being used.
(Strong recommendation, moderate quality evidence)

6/1/2016
35
Theoretical Complications from TTM1 – Bleeding – no increase in the RCTs but…
2 – Infection (Pneumonia) – trend toward increase
3 – Bradycardia – occurs but is this harmful?
4 – Hypokalemia – yes, increased incidence
Targeted Temperature Management (TTM)1 - Should we perform TTM?
- Shockable versus non-shockable rhythms- Out-of-hospital versus in-hospital
2 - If so, what temperature should we choose?
3 - If so, when should we start? Prehospital?
4 - How long should we go?
5 – What do we do about fever after TTM is done?

6/1/2016
36
Prehospital Hypothermia Trials
3551 Assessed

6/1/2016
37
6/1/2016
38
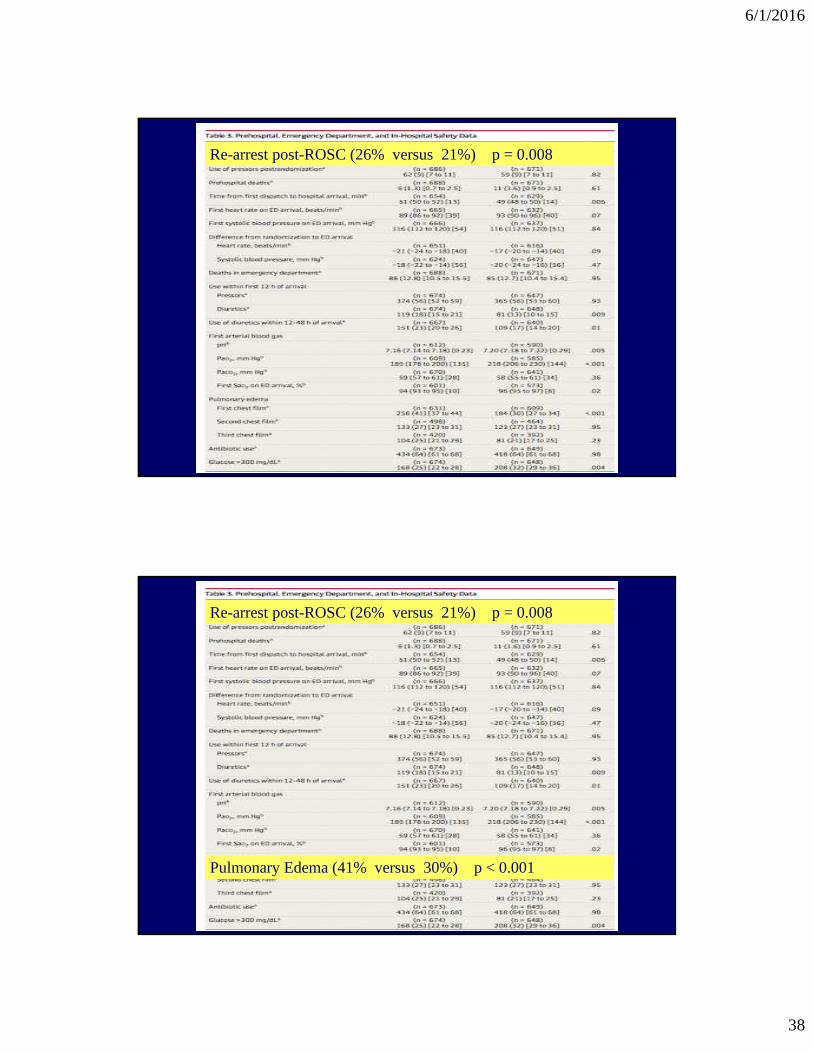
Re-arrest post-ROSC (26% versus 21%) p = 0.008
Re-arrest post-ROSC (26% versus 21%) p = 0.008
Pulmonary Edema (41% versus 30%) p < 0.001

6/1/2016
39
ILCOR Recommendation
We recommend against routine use of prehospital cooling with rapid infusion of large volumes of cold intravenous
fluid immediately after ROSC.
(Strong recommendation, moderate quality evidence)
Targeted Temperature Management (TTM)1 - Should we perform TTM?
- Shockable versus non-shockable rhythms- Out-of-hospital versus in-hospital
2 - If so, what temperature should we choose?
3 - If so, when should we start? Prehospital?
4 - How long should we go?
5 – What do we do about fever after TTM is done?

6/1/2016
40
ILCOR Recommendation
We suggest that if TTM is used, duration should be at least 24 hours as done in the two largest previous RCTs.
(Weak recommendation, low quality evidence)
Targeted Temperature Management (TTM)1 - Should we perform TTM?
- Shockable versus non-shockable rhythms- Out-of-hospital versus in-hospital
2 - If so, what temperature should we choose?
3 - If so, when should we start? Prehospital?
4 - How long should we go?
5 – What about fever after TTM is done?

6/1/2016
41
ILCOR Recommendation
We suggest prevention and treatment of fever in persistently comatose adults after completion of TTM between 32 and
36o Celsius.
(Weak recommendation, low quality evidence)
Keeping the Doctors Away Might Be Among One of the Most Important
Post-Cardiac Arrest Interventions

6/1/2016
42
Keeping the Doctors Away Might Be Among One of the Most Important
Post-Cardiac Arrest Interventions
• Non-TTM: 72 hours post-ROSC
• TTM: It is reasonable to wait 72 hours post return of normothermia before undergoing neuroprognostication
Case 1
• 65 year old male history of recent CABG surgery is on the hospital floor on POD #4
• A nurse obtaining vital signs witnesses the patient become unresponsive and ashen and calls for help…

6/1/2016
43
Case 1
Case 2
• 60 year old male presents with respiratory distress secondary to pneumonia and is intubated without complication (ETT confirmed by auscultation, end-tidal, and CXR)
• Patient initially stable after intubation with fluids/antibiotics and on low dose of vasopressors
• However, 2 hours later, nurse calls for help and…

6/1/2016
44
Case 3
• 66 year old female who presents with hypotension, urosepsis, and acute renal failure
5.6
90
13
191
133 80
3.3

6/1/2016
45
Case 3
!
Case 3
• 78 year old female history of COPD is on the hospital ward recovering from pneumonia
• She is found by nursing staff to be unresponsive and breathing at a rate of less than 8 breaths per minute
• She is obtunded and hypoxic but has a good pulse; you are called to intubate the patient…

6/1/2016
46
Conclusions • ACLS guidelines have stepped into a new era of
continuous review and online fluidity
• Most of the guidelines are based on expert opinion of limited evidence
• Don’t live in the sound bite – dive deeper than the one sentence recommendation….
Conclusions
• END
6/1/2016
47
Well, how about some stuff we got wrong?
• The “Earth is Flat”…
• Important items we did not cover: IO versus intravenous access
• Elements that may be misinterpretated: Beta blockers and lidocaine post-arrest
Re-arrest post-ROSC (26% versus 21%) p = 0.008
Pulmonary Edema (41% versus 30%) p < 0.001

6/1/2016
48
Prehospital Hypothermia Trials
3551 Assessed
ILCOR Recommendation
We recommend against routine use of prehospital cooling with rapid infusion of large volumes of cold intravenous
fluid immediately after ROSC.
(Strong recommendation, moderate quality evidence)

6/1/2016
49
Targeted Temperature Management (TTM)1 - Should we perform TTM?
- Shockable versus non-shockable rhythms- Out-of-hospital versus in-hospital
2 - If so, what temperature should we choose?
3 - If so, when should we start? Prehospital?
4 - How long should we go?
5 – What do we do about fever after TTM is done?
Targeted Temperature Management (TTM)1 - Should we perform TTM?
2 - If so, what temperature should we choose?
3 - If so, when should we start? Prehospital?
4 - How long should we go?
5 – What do we do about fever after TTM is done?
Donnino M, et al. Temperature Management after Cardiac Arrest: An Advisory Statement by the ACLS Task Force at ILCOR. Circulation 132 (25) 2448-56.2015

6/1/2016
50
What did we get right and do I know??
• “Known Knowns”
• Known Unknowns”
• “Unknown unknowns”
The Process
• ILCOR � evidence reviewing using GRADE and creation of the “Consensus on Science”
• AHA writing groups incorporate the findings from ILCOR into guidelines with levels of evidence to support…

6/1/2016
51
Could NMB be a confounder?
Salciccioli JD, Cocchi MN, Rittenberger JC, Ornato JP, Abella BJ, Callaway CW, Donnino MW. Continuous neuromuscular blockade is associated with decreased mortality in post-arrest patients. Resuscitation (2013) 84:1728-33
Amiodarone vs. Lidocaine
Survival to Hospital Discharge??
No Difference but not powered for this
Amiodarone 5% vs. Lidocaine 3% (p = NS)
(Dorian et. al. NEJM)

6/1/2016
52
Amiodarone vs. Lidocaine• Bottom Line: Amiodarone currently has “the
nod” but the study was small and had some flaws including provision of lipoprotein with deleterious effects to lidocaine group. Thus, giving lidocaine is acceptable alternative
• Currently, being reproduced with very large trial
ACLS Drugs - Summary� Epinephrine
� Vasopressin: removed from ACLS algorithms but is it magic when combined with steroids??
� Amiodarone versus Lidocaine versus placebo ???
� Sodium Bicarbonate: “Routine use” not recommended
� Calcium: “Routine use” not recommended
� Magnesium: “Routine use” not recommended
� Atropine: Remains out of pulseless ACLS algorithms –

6/1/2016
53
EXTRACORPOREAL CPR
• Extracorporeal CPR may be considered among select cardiac arrest patients who have not responded to initial conventional CPR, in settings where it can be rapidly implemented