Embed Size (px)
Citation preview

Evidence That D-dimer Levels Predict Subsequent Thromboembolic and Cardiovascular Events in Patients with Atrial Fibrillation during Oral Anticoagulant Therapy
Tsuneaki SADANAGAUeki Hospital, Kumamoto, Japan

【 Purpose 】
Atrial fibrillation is associated with hemostatic abnormality even during oral anticoagulant therapy.
Hypothesis: elevated D-dimer levels predict thromboembolic and cardiovascular events in patients with atrial fibrillation during oral anticoagulant therapy

0123456789
10
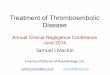
Control 28 – 457 days ( INR 1.5-3.7)
Oral anticoagulant therapy decreased D-dimer levels (30 paroxysmal Af, 13 chronic Af, n=43)
p <0.01
0.5µg/ml
12/43=28%
, however…
29/43=67%
(µg/ml)
D-d
imer
leve
ls

【 Methods】
Single center, prospective, observational study
Patients with atrial fibrillation (269 patients, 74±9 y/o, 152 male, 157 paroxysmal, 20 prosthetic valve) receiving anticoagulant therapy with warfarin are included. Exclusion: aortic aneurysm, deep vein thrombosis, malignancy (terminal stage), non-compliance (dementia)
Entry periods: January 2006 - April 2007Observational periods: January 2006 - December 2008Follow-up duration: 756±221 (1-1091, median: 736) days
D-dimer was measured only during entry periodsPT-INR was measured every 1-2 month during observational periods

End points1. Thromboembolic events (cerebral infarction,
transient ischemic attack, peripheral embolism)2. Combined cardiovascular events (thromboembolic events, cerebral hemorrhage,
myocardial infarction, cardiovascular death)
Secondary analysis Bleeding complications (intracranial bleeding,
gastrointestinal bleeding requiring transfusion)
The study protocol was approved by the institutional Ethics Committee and informed written consent was obtained from all the patients included in this study.

6 lost to followFollow-up 385-700 day → included in the analysis
4 discontinuation of warfarinFollow-up 374-630 day → included in the analysis
1 bleeding (accidental fall) 3 physician’s decision (no recurrence of pAf)
259 (96%) completed follow-up at the end of observational periods or reached endpoints
【 Follow-up 】

HHD IHD Valve HCM DCM None
HHD: hypertensive heart disease, IHD: ischemic heart disease, Valve: valvular heart disease, HCM: hypertrophic cardiomyopathyDCM: dilated cardiomyopathy
Underlying heart disease(%)

CHF HBP Age>75y/o DM Stroke Prosthetic Valve
Risk Factors for embolism
CHF: Congestive heart failure. NYHA≧II, HBP: systolic BP 140, ≧diastolic BP 90 mmHg, or medication, DM: Diabetes mellitus. fasting ≧blood glucose 126mg/dl, HbA1c 6.1%, medication, or insulin use≧ ≧
(%)

CHADS2 score distribution
C: Congestive heart failure, H: Hypertension, A: Age 75y/o≧
D: Diabetes mellitus, S: Stroke, * 26 patients. 24: Age 65y/o≧
(%)
*
(n=245, 24 valvular AF are excluded)

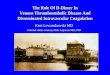
Relationship between D-dimer levels and PT-INR
0.5µg/ml
63(23%)
PT-INR
(µg/ml)
1 2 3 4
230 (86%)
D-d
imer
leve
ls

D-dimer (+) (n= 63) D-dimer (-) (n=206) (≥ 0.5 μg/ml ) (< 0.5 μg/ml ) p value
Gender ( Male,%) 56 57 n.s.
Age (y/o) 79±8 72±9 p<0.01
Chronic Af (%) 49 39 n.s.
INR 2.0±0.8 1.9±0.5 n.s.
D-dimer (μg/ml ) 1.4±1.3 0.2±0.2 p<0.01
CHADS2 score (n=245)* 2.7±1.4 (n=55) 1.7±1.2 (n=190) p<0.01
CHF(%) 67 35 p<0.01
Hypertension (%) 52 57 n.s.
Age≥ 75y/o (%) 71 39 p<0.01
Diabetes mellitus(%) 25 23 n.s.
History of Stroke (%) 21 9 p=0.014
【 Characteristics of patients with high D-dimer levels 】
* 24 patients with valvular AF are excluded

【 Determinants of high D-dimer levels by logistic regression analysis 】
Univariate Analysis Gender p=0.86Chronic Af p=0.16PT-INR (entry) p=0.36 CHF p<0.01 Hypertension p=0.54Age≥75 y/o p<0.01Diabetes mellitus p=0.67History of stroke p<0.01
Multivariate Analysis Odds ratio (95% CI)
Age≥75 y/o p<0.01 3.14 (1.66-5.94)CHF p<0.01 2.87 (1.54-5.36)History of stroke p=0.045 2.29 (1.02-5.16)

【 Results 】
D-dimer (+) D-dimer (-) (n= 63) (n=206) p value
Thromboembolic events 8 2 p<0.01
Cardiovascular events 18 9 p<0.01
Total mortality 14 8 p<0.01
Bleeding complications 8 1 p<0.01
Thromboembolic events 10 1.8 % /year
Cardiovascular events 27 4.8 %/ year
Total mortality 22 3.9 %/year
Bleeding complications 9 1.6 %/year

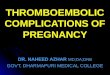
Follow-up duration (day)
Thromboembolic eventsD-dimer < 0.5μg/ml (n = 206)
Eve
nt f
ree
rate
p < 0.01 (Log rank test)
8 cerebral infarction, 1 transient ischemic attack, 1 peripheral embolism
D-dimer ≥ 0.5μg/ml (n = 63)
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 200 400 600 800 1000 1200

【 Risk factors for thromboembolic events by Cox proportional hazard analysis 】
Univariate Analysis D-dimer p<0.01INR<1.5 (at the time of event) p<0.01Gender p=0.30CHF p=0.012 Hypertension p=0.36Age≥75 y/o p=0.36Diabetes mellitus p=0.60History of stroke p<0.01
Multivariate Analysis Hazard ratio (95% CI)
D-dimer p=0.013 7.72 (1.53-38.8)History of stroke p<0.01 5. 67 (1.57-20.4)CHF p=0.059 7.66 (0.93-63.1)

Follow-up duration (day)
Combined cardiovascular eventsD-dimer < 0.5μg/ml (n = 206)
p < 0.01 (Log rank test)
Eve
nt f
ree
rate
10 thromboembolisms, 9 deaths from heart failure, 3 sudden deaths, 2 myocardial infarctions, and 3 cerebral hemorrhages
D-dimer ≥ 0.5μg/ml (n = 63)
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 200 400 600 800 1000 1200

【 Risk factors for combined cardiovascular events by Cox proportional hazard analysis 】
Univariate Analysis D-dimer p<0.01Gender p=0.35CHF p<0.01 Hypertension p=0.45Age≥75 y/o p<0.01Diabetes mellitus p<0.01History of stroke p<0.01
Multivariate Analysis Hazard ratio (95% CI)
D-dimer p<0.01 4.20 (1.83-9.68)CHF p<0.01 12.5 (2.92-53.7)Diabetes mellitus p=0.047 2.18 (1.01-4.71)History of stroke p<0.01 4.08 (1.84-9.08)

Follow-up duration (day)
Total mortality
D-dimer < 0.5μg/ml (n = 206)
D-dimer ≥ 0.5μg/ml (n = 63)
Eve
nt f
ree
rate
p < 0.01 (Log rank test)
18 cardiovascular deaths, 3 pneumonias, 1 lung cancer
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 200 400 600 800 1000 1200

【 Risk factors for total mortality by Cox proportional hazard analysis 】
Univariate Analysis D-dimer p<0.01Gender p=0.85CHF p<0.01 Hypertension p=0.46Age≥75 y/o p<0.01Diabetes mellitus p<0.01History of stroke p<0.01
Multivariate Analysis Hazard ratio (95% CI)
D-dimer p=0.046 2.67 (1.02-7.00)CHF p<0.01 22.7 (2.99-172)History of stroke p<0.01 5.52 (2.11-14.4)Diabetes mellitus p=0.064 2.25 (0.95-5.33)Age≥75y/o p=0.074 2.70 (0.91-8.03)

Follow-up duration (day)
Bleeding complications
4 intracranial hemorrhage, 5 gastrointestinal bleeding requiring transfusion
Eve
nt f
ree
rate
0 200 400 600 800 1000 1200
D-dimer < 0.5μg/ml (n = 206)
p < 0.01 (Log rank test)D-dimer ≥ 0.5μg/ml (n = 63)
0.4
0.5
0.6
0.7
0.8
0.9
1.0

【 Risk factors for bleeding complications by Cox proportional hazard analysis 】
Univariate Analysis D-dimer p<0.01INR>3.0(at the time of bleeding) p<0.01Gender (female) p=0.054CHF p=0.33 Hypertension p=0.98Age p<0.01Diabetes mellitus p=0.15History of stroke p<0.01
Multivariate Analysis Hazard ratio (95% CI)
D-dimer p<0.01 18.1 (2.2-150)INR>3.0(at the time of bleeding) p<0.01 26.4 (5.80-120)Gender (female) p=0.012 10.8 (1.69-68)History of stroke p=0.013 6.84 (1.51-31.1)

【 Conclusion 】
Persistent elevation of D-dimer Levels despite proper anticoagulant therapy can predict thromboembolic and cardiovascular events in patients with atrial fibrillation
Further larger scale, multicenter studies are needed to confirm these findings.