Embed Size (px)
Citation preview

1
Evidence into Practice Supporting partners to quit smoking

1
Introduction
This briefing should support the delivery of interventions to reduce smoking prevalence among pregnant
women's partners or other household members. It reviews the evidence base for interventions targeting
partners and includes case studies from programmes currently underway in England.
The briefing sets out:
» Impact of smoking and exposure to secondhand smoke during pregnancy
» Addressing partners' smoking: National guidance
» What interventions to support partners and other household members to quit look like
» Current evidence base for supporting partners to quit: before, during and after pregnancy
» Creating smokefree homes
» Conclusions
1. Impact of smoking and exposure to secondhand smoke during
pregnancy
Smoking and exposure to secondhand smoke (SHS) during pregnancy increases the risk of stillbirth,
miscarriage, preterm birth, heart defects, low birth weight and sudden infant death (SIDS).
Source: Smoking in Pregnancy Challenge Group. Review of the Challenge 2018. July 2018.1
The focus of most work to reduce rates of smoking in pregnancy has been on the women who smoke, not on
the environments in which they live. For many women struggling to quit throughout pregnancy the home
environment will play a crucial role in whether they are smoking at conception, if they are able to successfully
quit, whether they relapse to smoking once the baby is born and if they and the baby are exposed to SHS.1
Women who live with a smoker are 6 times more likely to smoke throughout pregnancy and those who live
with a smoker and manage to quit are more likely to relapse to smoking once the baby is born. An estimated
20% of women are also exposed to SHS in the home throughout their pregnancy, leading to an increased
risk of many of the same adverse birth outcomes experienced by women who smoke.1
There is, therefore, an opportunity for services to intervene to support families and communities to become
smokefree as part of addressing rates of smoking in pregnancy. Reaching into households and communities
requires a new way of working with different kinds of professionals. There are many professionals who have
regular contact with families and prospective parents who could play an important role in highlighting the
need to quit smoking, the benefits to children and signpost mothers, fathers and other household members
to cessation support. Such groups include maternity professionals such as midwives, health visitors, and
paediatricians but also professionals in children’ services, social housing providers, family planning and
sexual health services, and mental health service providers.1 Services also need to consider other, potentially
more effective ways to engage fathers before, during and after pregnancy. This means trialling different types
of health messaging that focuses on fathering and men’s experiences and considering the role that online
stop smoking and health promotion programmes can play in reaching men who are less likely to access other
services.

2
2. Addressing partners' smoking: National guidance
NICE guidance PH26 ‘Smoking: stopping in pregnancy and after childbirth’ and the NCSCT ‘Briefing for
maternity care providers’ and ‘Standard Treatment Programme for Pregnant Women’ recommend a tailored
approach to treating smoking among partners and other household members. 2 3 4
In line with this guidance, all pregnant women should be asked whether their partner smokes or if there are
other smokers in their home. Exhaled breath carbon monoxide (CO) monitoring – which should take place at
the booking and 36-week antenatal appointments and as appropriate throughout pregnancy – can help to
identify if a pregnant woman has been exposed to SHS and can provide a route into conversations about
household smoking. If the woman does live with a smoker, it is important that she understands that:
» Exposure to SHS significantly reduces the chances of a healthy pregnancy.
» Living with a smoker or being around smokers will make it harder to quit and stay smokefree.3
» Introducing a smokefree home can increase the likelihood that their partner/household member will
be able to quit smoking successfully.5 6
Partners who smoke should be given clear advice about the harms of SHS to the pregnant woman and the
baby, and informed that they should not smoke around the pregnant woman or baby, especially in the home
or car. They should be offered a tailored intervention comprising of three or more elements (very brief advice,
behavioural support and pharmacotherapy) and multiple contacts. The intervention should consider partners’
preferences, the likelihood that they will follow the course of treatment, and their previous experience of stop
smoking aids to ensure they are recommended the approach most likely to help them quit.2
Additionally, the NHS Long Term Plan commits to offering NHS-funded tobacco treatment services to the
partners of pregnant women who smoke, as part of an adapted smokefree pregnancy pathway.7
3. What interventions to support partners and other household members to
quit look like
Interventions to reduce smoking among partners and other household members typically have three key
outcomes:
» To protect pregnant women and children from SHS exposure by creating and maintaining a smokefree
home.
» To support partners and other household members who smoke to quit, or if they are unable to quit,
moderate their smoking behaviour by smoking outside the home and away from pregnant women and
children.
» To support pregnant women who have quit or are trying to quit to have a smokefree home.
Although approaches which are effective for increasing quitting among adults in general are likely to be
effective for treating smoking partners, there is currently no standardised approach for engaging partners
with stop smoking interventions. Some interventions aimed at partners are delivered solely to the partner
while others are delivered to both the partner and the pregnant woman. The methods and outcome measures
are highly variable from one scheme to another and are heavily determined by the cultural context of the
target population. 8 9 General features of these interventions include:
» Educational interventions, typically based in health care settings (e.g. antenatal appointment), using
direct teaching or counselling, brochures, posters, role-play and/or videos;
» Tailored approaches targeting high prevalence population groups;
» Pharmacological and behavioural support offered to fathers and other household members. This
support should address the specific barriers and facilitators for quitting among fathers;
» Clear messaging around the harms of SHS exposure and the importance of maintaining a smokefree
home. This should include advice about what works (not allowing smoking inside) and what doesn’t
(opening windows).

3
4. Preconception
Rates of smoking have a strong social and age gradient with poorer and younger women much more likely
to be smokers. As women get older, they are more likely to give up smoking before getting pregnant.10 Rates
of smoking for young (18-34) white women in routine and manual occupations are currently more than double
(27.7%) that of women on average (12.5%).11 This inequality for all women is reflected in pregnant women.12
While some women give up smoking because of pregnancy, the data suggests that for others, particularly
younger women, smoking can become entrenched during pregnancy.10
Rates of smoking among young men are similarly skewed, with 31.2% of young (18-34) white men in routine
and manual occupations smoking, compared to 16.4% of men overall.11 Consequently, women living with
these men are more likely to be exposed to SHS and less likely to have a home environment that is facilitating
quitting.
4.1 Reaching young men
Reaching these groups may require a targeted, innovative approach and working with different professionals
across a broader range of settings. There is some evidence to suggest that preconception health information
provided by GPs or health professionals or from other sources (including online) has the potential to increase
positive pre-pregnancy health behaviour in men.13 Family planning and fertility services could train staff to
identify smokers and deliver very brief advice (VBA) as well as specific messaging around the harms of SHS,
and offer referral to stop smoking services.14
However, it is recognised that men have less direct contact with family planning services and are less likely
to access healthcare in general.13 This is likely to be particularly salient for men working in routine and manual
occupations who are less likely to be able to take time off work to attend appointments. Digital health
interventions targeted at men may be effective for reaching partners from more deprived socio-economic
groups, although further research is needed.13
Localities need to consider whether there are there particular workplaces employing lots of young men locally
and whether this group is accessing other services (e.g. mental health). Partnering with social housing
providers is also likely to be an effective way of reaching this cohort. Smoking rates among people living in
social housing are more than double the national average at approximately 35%15 so improving reach into
these communities is likely to be an effective way to reach young smokers. Localities must consider which
professional groups are best placed to deliver these messages and what types of intervention are likely to be
most effective. Other settings relevant to this population include primary care services and sexual health
services, or education settings like further education and vocational colleges.
4.2. Ensuring consistent service provision
ASH’s annual tobacco control reports detail the variation in stop smoking services available in different
areas.16 In 2019, all areas responding to the survey commissioned stop smoking support for pregnant women,
however this support is not necessarily available to women or their partners pre-conception. Local Maternity
System’s (LMS) should engage with local authority public health teams and stop smoking services to identify
the service offer available to women and their partners before pregnancy and ensure that other healthcare
providers are delivering consistent, evidence-based messages around the importance of quitting smoking.
Reducing prevalence among all men and women in this age group through population-level and targeted
interventions will be crucial to achieving specific reductions in smoking during pregnancy and pregnant
women’s exposure to SHS.
Useful resources
» Smoking in Pregnancy Challenge Group. LMS Smokefree Pregnancy Pathway. 2020.
» Planning a pregnancy resources developed by Tommy’s for women and families.
» Public Health England. Preconception care: making the case. 2019.

4
5. Intervening during pregnancy
An estimated 20% of women are exposed to SHS in the home throughout their pregnancy, leading to an
increased risk of many of the same adverse birth outcomes experienced by women who smoke. Interventions
to reduce both smoking and non-smoking pregnant women’s exposure to SHS during pregnancy need to be
further developed.
5.1 Targeting interventions at pregnant women
There is limited evidence around the effectiveness of smokefree home interventions which target fathers,
because most existing research focuses on women’s experiences of smoking behaviour change in these
settings. 8 9 These interventions tend to lay the responsibility for SHS avoidance/reduction on the pregnant
woman, rather than focussing on the role of other smoking household members to prevent exposure to the
pregnant woman.
In a systematic review of nine interventions which aimed to reduce pregnant women’s exposure to SHS,
seven targeted the intervention solely at the pregnant women. 8 This was done primarily through education
materials, counselling or guidance around the health effects of SHS and how best to avoid SHS exposure in
the home or workplace.
However, evidence has shown that encouraging pregnant women to provide counselling and encouragement
to their partners to help them quit does not increase quit rates. 8 17 Interventions which put the onus on the
woman to change the smoking behaviour of their partners are particularly problematic in households with
gender power imbalances.9 There is consequently a need for approaches which directly encourages partners
to quit smoking and engage with all members of smoking households to create a smokefree home.
5.2 Whole-family approaches
Approaches which involve partners and the wider household are likely to be more effective for reducing SHS
exposure among pregnant women and children, although further research is needed.
An intervention involving 60 smoking men, based on providing education on the effects of SHS, reduced
exposure among their non-smoking pregnant wives.18 The men in the intervention group received a 30-45
minute face-to-face education session based on the health belief model (HBM), which used photos to
emphasise the impact SHS exposure during pregnancy has on the foetus. The HBM is based on the
understanding that a person will take a health-related action if they feel greater susceptibility to the risk of
experiencing negative health outcomes. Messages with educational tips were sent to the participants for the
following 6 weeks. 18
Participants were surveyed on their health beliefs shortly before and after the education session, and then
again 6 weeks later. The researchers found that women in the intervention group reported significantly lower
SHS exposure (mean number of cigarettes per week they were exposed to) 6 weeks following the intervention
(35.63 compared to 12.87). However, the total number of cigarettes smoked weekly (self-report) by men was
not significantly different. Although maintaining the health of the pregnancy was not sufficient motivation for
men to quit smoking, it was effective for creating smokefree homes by encouraging men to smoke away from
their pregnant wives. 18
Research suggests that encouraging women to change the behaviour of their partners is not effective. 8 9
Providing men with education on the impact of their smoking behaviour appears to have some impact, at
least in the short term, but there is a need for further research. Future work should examine the potential
effectiveness of NRT provision (both for creating a smokefree home and for cessation purposes) and/or
financial incentives for partners in helping to reduce the exposure of pregnant women (both smokers and
non-smokers) to SHS. 8 19 The case studies below highlight that interventions which involve partners/family
members can be an effective way to engage pregnant smokers and increase quit rates, particularly when
combined with financial incentives and NRT provision.

5
Case study 1: Supporting a Smokefree Pregnancy (SaSFPS) in Greater Manchester (GM): The
influence of Significant Other Support
Strategic aim
The GM SaSFPS includes an option for the pregnant woman to recruit ‘Significant Other Support’ (SOS). The inspiration to include SOS within the GM SaSFPS was initially based on research showing that the combination of reinforced social support and financial incentives significantly increased the likelihood of a higher-than-usual quit rate among high risk pregnant women. 20 Analysis of a previous scheme in the North West (Supporting a Smokefree Pregnancy Scheme, 2010 – 2013) found that the odds of achieving a four-week quit was increased by 55% when participants received support from a significant other, compared to those did not.21
Design
The significant others (SO) within the GM scheme receive £60 worth of high street vouchers if the woman they are supporting remains smokefree up to 12 weeks postpartum. If the woman relapses when on the scheme the SO receives no vouchers. The SO can be anyone the woman nominates so long as they are 16yrs or over and are CO validated as smokefree*. The SO can be someone who is also quitting and does so along with the pregnant woman. They are expected to be CO validated:
» at time of quit commencement;
» at the end of the 4-week quit period;
» and there on every 4 weeks up until 12 weeks postpartum.
If the SO relapses they are no longer eligible for the vouchers, but the pregnant woman can remain on the scheme as long as she is still smokefree. The SO is required to sign a contract agreeing to the terms and conditions of the scheme.
* Scores less than 4ppm (parts per million) on a CO breath test
Outcomes
The initial outcomes are generated from participants on the original GM SaSFPS over a period of 18 months (Feb 2018 – July 2019).
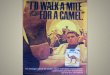
54% (386/710) of the women recruited onto the scheme identified an SO. Women with SOS were almost twice as likely to achieve a 4-week quit than those without. This trend continued through to delivery and 12 weeks postpartum, although the overall numbers of women who maintained their quit decreased throughout pregnancy and postpartum.
Fig 1. Percentage of women who are quit at 4 weeks, 36 week’s gestation and 12 weeks postpartum with and without SOS support
62%
64%
65%
38%
36%
35%
4-week quit
Still quit at delivery
12 weeks post-partum
Without SOS With SOS

6
Case study 2: Poole Hospital NHS Foundation Trust and Public Health Dorset: Improving
Patient Care in a Tobacco Dependency Programme (IPCTD) A Quality Improvement Pilot for
Smoking Cessation Support to Family Members Wishing to Quit Smoking to Improve the Quit
Environment of the Smoking Pregnant Woman
Strategic aim
The key aim of the pilot was to contribute to a reduction in the prevalence of smoking in pregnancy to 6% or less by the end of 2022. This will be achieved by:
» Increasing engagement of pregnant smokers from 52% to 75% and maintain or improve the current
quit rate of 75%;
» Increasing the partner engagement rate from 4% to 30% and increasing the quit rate from 2.2% to
30%;
» Improving health outcomes for the 20-45 target age group who smoke and are less likely to access
health care;
» Reinforcing the simple prevention strategy that prevention is better than cure.
Design
This project is led by the Smoking in Pregnancy Midwifery services at Poole Hospital Foundation Trust. Specialist smoking in pregnancy liaison midwives provide pharmacotherapy and combined behavioural counselling sessions to the pregnant smoker and smoking partners/family members for the duration of the 12-week programme. This happens through a variety of contact methods including home visits and clinics to ensure good engagement.
The pregnant smoker, partner other household family members who smoke are seen “in tandem” to gain additional support from each other during the program. Both pregnant smokers and their smoking partners/family members are offered direct pharmacotherapy, avoiding the need for two separate pathways to be offered. Participants are CO monitored throughout the scheme to validate the quit and provide additional motivation.
Initial outcomes
1. Engagement of pregnant smokers setting a quit date has remained static at 52% (pilot target 75%)
but quit rates of those engaged has increased from 75% to 82%;
2. Partner engagement rate has increased from 4% to 39% (pilot target 30%);
3. Partner quit rates have increased from 2.2% to 60% (target 30%) and interestingly 90% opted for
Varenicline as their first choice of pharmacotherapy;
4. Two thirds of the partners engaged are from the targeted 20-45 age group.
5.3 Lessons for practice
» Interventions which are delivered at the household level can be effective for engaging smoking
partners, as they frame smoking as a household responsibility, with family-wide impact.
» Significant others need to be involved not just as providers of social support but as participants with
a stake in the change process.22
» Using financial incentives to recruit partners/significant others to support the pregnant woman’s quit
attempt can be an effective way to increase quit rates.
» Providing behavioural support and pharmacotherapy jointly to pregnant smokers and their smoking
partners/family members can increase quit rates among pregnant women and partners and could be
beneficial for creating a smokefree home.

7
6. Intervening beyond pregnancy
As of 2019, around 7% of all children in England were exposed to tobacco smoke in the home, increasing
their risk of sudden infant death (SIDS), chest infections, asthma and meningitis, and making them 90% more
likely to start smoking themselves.23 24 25 There is also emerging evidence of an association between home
smoking restrictions and reduced adolescent smoking behaviours.26
Evidence suggests that becoming a father is a significant transition period which provides a window of
opportunity to engage and support fathers in quitting smoking or creating a smokefree home.27 28 29 As adults
become parents, the decision to reduce or quit smoking becomes more prominent, influenced by:
» The de‐normalisation of tobacco use during pregnancy for women, and;
» The negative effects of SHS on children.27
Smoking is increasingly incongruent with fathers’ views of themselves as a role model and protector to their
children, with reducing and quitting smoking constructed as part of the process of engaging in fatherhood.27
There are challenges in effectively engaging fathers with stop smoking interventions. A study of new fathers’
narratives around reducing and quitting smoking, found that fathers are reluctant to rely on stop smoking aids
and medications; instead self‐reliance, willpower, and autonomy figured more prominently in their
narratives.27 Another study found that many men were more likely to deny or conceal their smoking rather
than seek support to quit, and found that online stop smoking materials which provide anonymity and are
tailored to men’s experiences could be an effective method for engaging smoking fathers.30
6.1 Gender appropriate approaches: reaching new fathers
FACET (Families Controlling and Eliminating Tobacco), based at the University of British Columbia in
Canada, is engaged in several programmes to find original ways to support young families in their efforts to
become smokefree, including work to help new fathers quit smoking.31
Booklet: The right time… The right reasons… Dads talk about reducing and quitting smoking (2010)
FACET’s ‘The right time… The right reasons…’ booklet is based on fathers’ experiences of reducing and
quitting smoking and is designed to provide fathers who smoke with information and advice to encourage
quitting.32 It includes quotes from expectant/new fathers who smoke or have successfully reduced/quit
smoking, advice about the best ways to quit, and a Q&A which highlights facts about the harms of SHS and
the benefits of quitting. The booklet presents becoming a father as a key opportunity to quit smoking and
emphasises the positive impact on the child/family, in terms of improved health and improved household
finances. The booklet portrays the decision to quit/cut down as a way of being a responsible father who
provides for his family.32
“I actually have a kid now and my smoking is not just about me anymore. My smoking also makes it harder
for my partner to quit.”
“Taking my smoking outside helps my baby stay healthy. But I keep thinking about what I’m missing when
I’m outside smoking. The guys at work understand that I want to be a good example for my child.”

8
The ‘Dads in Gear’ (DIG) programme 28 33
FACET has also trialled a ‘Dads in Gear’ (DIG) 8-week, gender-sensitized smoking cessation programme
targeting fathers. The DIG programme design is based on three integrated components: smoking cessation,
physical activity and fathering.
The programme was delivered in 5 community sites by trained male facilitators to fathers who smoked and
wanted to quit. The programme consisted of weekly 2-hour face-to-face group sessions which focused on
increasing men's cessation self-efficacy and providing peer and facilitator support. Materials to support the
delivery of the programme, recruitment of participants, and facilitator training were provided via the DIG
website.34
21 fathers completed the programme, with 35.5% of participants being abstinent (self-reported) at 3-month
follow up.33
See the FACET website for more information: http://facet.ubc.ca/
6.2 Lessons for practice
» Becoming a father is a significant transition period which provides a window of opportunity to engage
and support fathers in quitting smoking or creating a smokefree home.
» Evidence suggests that smoking is inextricably linked to the social relationships and environments in
which it occurs.22 Positive social support from peer groups may be effective for helping fathers quit
smoking i.e. messages from Dads may be more effective with Dads.
» Peer to peer approaches which focus on increasing men's cessation self-efficacy should be explored
further.

9
7. Creating smokefree homes
There are currently too few published studies assessing smokefree home interventions with fathers to draw
conclusions regarding effective approaches. However, several interventions have been trialled which merit
further exploration.
7.1 Using air quality measures to engage parents
There is some evidence to suggest that approaches which utilise feedback on air quality measures may be
effective for engaging parents around household smoking, although further work is required to identify the
best approach for engaging more deprived households.35 36 37 8
Under the AFRESH programme researchers have specifically developed interventions aimed at supporting
disadvantaged households.38 This intervention consists of 6 modules, each module addressing a particular
aspect of behaviour change, and is designed to be delivered face-to-face by healthcare professionals to
parents and other household members who smoke. It includes up to five meetings with parents, two sets of
five days’ air quality monitoring for concentrations of PM2.5 – fine particulate matter found in tobacco smoke
– with personalised feedback, and the option to involve other household members in creating a smokefree
home using educational, motivational, and goal setting techniques. This intervention is based on the current
evidence around smokefree homes interventions, including the REFRESH (reducing families' exposure to
secondhand smoke in the home) intervention.35 37 38 A small-scale pilot of AFRESH found that the intervention
was acceptable for the target population and may help participants to create smokefree homes, however the
resources required for the delivery of AFRESH do not match with the resources typically available in third-
sector organisations.39
The ‘First Steps 2 Smoke-free’ intervention trialled the use of air quality feedback with new mothers living in
deprived households, using an approach delivered as part of health professionals’ routine work.40 Women
reported that the intervention had increased their awareness of SHS risks to their children, and their
motivation to change home-smoking behaviours. However, the intervention was ineffective at creating actual
change, as attempts to create a smokefree home were often constrained by lack of access to suitable, safe
outdoor space; the challenges associated with looking after young, mobile children; and others’ smoking in
the home.40 Using NRT or an e-cigarette for temporary abstinence in the home could address some of these
complexities, alongside the development of smokefree home interventions that work with men and other
family members, framing household smoking as a collective responsibility.40
A 12-week smokefree homes intervention with primary caregivers of children aged under 5 years, who
reported smoking in the home and were not motivated to quit found feedback on air quality could motivate
quitting behaviours.41 The intervention comprised of feedback on the air quality measured in the home
(PM2.5); behavioural support on how to create a smokefree home; and provision of NRT for temporary
abstinence or for cutting down tobacco smoking. The intervention successfully reduced children’s exposure
to SHS in the home, resulting in improved home air quality, lower child salivary cotinine, lower cigarette
consumption in the home and increased likelihood of having made a quit attempt, compared to ‘usual care’.
Although the intervention did not specifically target smoking partners, this approach could be tailored for the
whole household.41
Feedback on air quality (PM2.5) in the home may be effective for engaging those who smoke inside the home.
However, the evidence to date suggests that air quality feedback and VBA have not been sufficient to change
household smoking behaviour in more deprived households.37 Personalised feedback may be more effective
if combined with behavioural support and perhaps with the additional provision of NRT or e-cigarettes.38 41
7.2 Considering cultural contexts
A review of fathers’ views and experiences of creating a smokefree home found that attitudes and knowledge,
along with cultural and gender norms play a significant role in shaping fathers’ beliefs and knowledge
regarding the health risks of SHS exposure to children and the importance associated with creating a
smokefree home.9 The review primarily focused on Asian countries where smoking is not the cultural norm
for women, and children are largely exposed to SHS through the father. In this context, there is some
evidence that community-wide interventions which aim to change smoking norms could be effective, although
further research is needed.42 43 The authors concede that different approaches may be required in countries

10
with greater emphasis on gender equality compared to Asian countries – Western European countries for
example – to support fathers to effectively create and maintain a smokefree home.9 These findings could be
useful for informing smokefree homes interventions in minority ethnic communities with high rates of paternal
smoking.
Case study 3: Dorset HealthCare University NHS Foundation Trust and Public Health Dorset:
Exploring the use of CO screening by health visitors to support smoking cessation in
pregnancy and the postpartum period
Strategic aim
Health visitors in Dorset are piloting a new project to engage with families around the harms of CO (carbon monoxide) and smoking with the aim of reducing the prevalence of smoking households.
Design
The health visitors received a three-hour training session on delivering a smoking cessation brief intervention and using a CO monitor.
When visiting a household, the health visitor offers all members of the household a personal exhaled breath CO test. Offering CO testing as part of the routine pathway enabled the conversation about smoking behaviours to be more meaningful and helps to facilitate a conversation about SHS and the risk to the baby and others in the household.
Following the CO test, household members with elevated CO levels (4ppm and above) receive Very Brief Advice (VBA) and are offered a referral to the local stop smoking service. Those declining support or indicating that they do not wish to quit, will be informed of the benefits of switching to vaping in line with the advice from Public Health England.44
Health visitors reported that they wanted further training to cover cessation methods and e-cigarettes to support those who did not want to be referred to smoking cessation services.
Initial outcomes
Results from the early stages of the pilot found that almost half (48%) of the 33 participants managed to quit smoking during pregnancy. Of these, 69% remained smokefree up to 6-8 weeks postpartum. Health visitors reported they were able to help have more meaningful conversations with mothers and their partners using the CO monitor as an engagement tool. Those partners present during the visit were also screened for CO.
7.3 Lessons for practice
» Interventions which combine personalised feedback on home air quality with behavioural and
pharmacological support could help new parents keep a smokefree home.
» Feedback on home air quality can be an effective way to engage women and partners around smoking
cessation.
» Evidence suggests that parents living in disadvantaged households require a tailored approach that
not only acknowledges the limited opportunities that they have to take their smoking outside, but
provides a practical means to overcome these limitations (e.g. NRT).
» Carbon monoxide (CO) testing can be an effective tool for engaging and motivating smoking partners.
» Ethnic groups with low rates of maternal smoking where children are largely exposed to SHS through
the father may require tailored interventions which take into account cultural and gender norms.

11
8. Conclusions
» Population level interventions to reduce smoking prevalence among young men and women from
more deprived groups are likely to be effective for reducing rates smoking and exposure to SHS during
pregnancy.
» Interventions to reduce partner smoking at preconception are currently lacking and should be
developed.
» Current evidence suggests that encouraging women to change their partner’s behaviour is not an
effective approach to reduce exposure to SHS in the home.
» Interventions which encourage men to take responsibility for their smoking behaviour appear to be
more effective, particularly when delivered at the household level.
» Significant others need to be involved not just as providers of social support but as participants with
a stake in the change process.
» Interventions which offer partners pharmacotherapy and financial incentives can be effective for
increasing quit rates among pregnant women and partners, although further research is needed.
» Carbon monoxide (CO) testing can be an effective tool for engaging and motivating smoking partners.
» Peer-to-peer approaches which focus on increasing men's cessation self-efficacy as used by FACET
in Canada should be explored further.
» There is some evidence that interventions which combine personalised feedback on home air quality
with behavioural and pharmacological support could help new parents keep a smokefree home.
» Ethnic groups with low rates of maternal smoking where children are largely exposed to SHS through
the father may require tailored interventions which take into account cultural and gender norms.
» Parents living in disadvantaged households require a tailored approach that not only acknowledges
the limited opportunities that they have to take their smoking outside, but provides a practical means
to overcome these limitations.
» There is a lack of agreement within published research on how best to assess non-smoking pregnant
women’s exposure to SHS, both pre- and post-intervention. Objective measures such as salivary
cotinine or hair nicotine are expensive and time consuming whereas self-report measures of SHS
exposure or partner smoking are inherently unreliable.
» The quality of future interventions would be improved by validated questionnaire tools and a
standardised measure to assess pre- and post-intervention exposure to SHS.
» There is a need to build the evidence base and identify an effective intervention which can be
replicated at a population level. The case studies included in this briefing should inform the design of
future interventions to reduce partner smoking.

12
References
1 Smoking in Pregnancy Challenge Group. Review of the Challenge 2018. 2018. 2 NICE. Smoking: stopping in pregnancy and after childbirth. Public health guideline [PH26]. 2010. 3 NCSCT. Stopping smoking in pregnancy: A briefing for maternity care providers. 2019 4 NCSCT. Standard Treatment Programme for Pregnant Women. 2019 5 Haardörfer R, Kreuter M, Berg CJ, Escoffery C, Bundy ŁT, Hovell M, Mullen PD, Williams R, Kegler MC. Cessation and reduction in smoking behavior: impact of creating a smoke-free home on smokers. Health education research. 2018 Jun 1;33(3):256-9. 6 Vijayaraghavan M, Messer K, White MM, Pierce JP. The effectiveness of cigarette price and smoke-free homes on low-income smokers in the United States. American journal of public health. 2013 Dec;103(12):2276-83. 7 NHS England. The NHS Long Term Plan. January 2019. 8 Nwosu C, Angus K, Cheeseman H, Semple S. Reducing second-hand smoke exposure among non-smoking pregnant women: a systematic review. Nicotine & Tobacco Research: Accepted for publication 9 O’Donnell R, Angus K, McCulloch P, Amos A, Greaves L, Semple S. Fathers’ Views and Experiences of Creating a Smoke-Free Home: A Scoping Review. International Journal of Environmental Research and Public Health. 2019 Jan;16(24):5164. 10 Public Health England. Health of women before and during pregnancy: health behaviours, risk factors and inequalities. 2019. 11 Public Health England. Smoking prevalence in young adults aged 18 to 34 years. 2019 12 NHS Digital. Infant feeding survey UK – 2010. 2012. 13 Shawe J, Patel D, Joy M, Howden B, Barrett G, Stephenson J. Preparation for fatherhood: A survey of men’s preconception health knowledge and behaviour in England. PloS one. 2019;14(3). 14 Rosenthal AC, Melvin CL, Barker DC. Treatment of tobacco use in preconception care. Maternal and child health journal. 2006 Sep 1;10(1):147-8. 15 Office for National Statistics. Smoking status and housing tenure, England and London, 2015 to 2017. 2018. 16 ASH and Cancer Research UK. A changing landscape: Stop smoking services and tobacco control in England. 2019. 17 Loke AY, Lam TH. A randomized controlled trial of the simple advice given by obstetricians in Guangzhou, China, to non-smoking pregnant women to help their husbands quit smoking. Patient Educ Couns. 2005;59(1):31–7. 18 Sahebi Z, Kazemi A, Loripour M, Shams N. An educational intervention to men for reducing environmental tobacco smoke exposure in their pregnant wives. The Journal of Maternal-Fetal & Neonatal Medicine. 2019 May 19;32(10):1595-601. 19 Pollak KI, Lyna P, Bilheimer AK, Gordon KC, Peterson BL, Gao X, Swamy GK, Denman S, Gonzalez A, Rocha P, Fish LJ. Efficacy of a couple-based randomized controlled trial to help Latino fathers quit smoking during pregnancy and postpartum: The Parejas Trial. Cancer Epidemiology and Prevention Biomarkers. 2015 Feb 1;24(2):379-85. 20 Donatelle RJ, Prows SL, Champeau D, Hudson D. Randomised controlled trial using social support and financial incentives for high risk pregnant smokers: Significant Other Support (SOS) program. Tobacco Control 2000;9(Supplement III):iii67‐iii69. 21 Healthier Futures. Supporting a Smokefree Pregnancy Scheme, What does the data tell us. Unpublished. 2014 22 NCSCT. Smoking cessation interventions involving significant others: the role of social support. 2012. 23 2019 ASH Smokefree GB Youth Survey. Total sample size was 2,523 respondents. Fieldwork was undertaken between 12th March - 3rd April 2019. The figures have been weighted and are representative of all GB children aged 11 to 18. 24 Royal College of Physicians. Passive smoking and children. A report by the Tobacco Advisory Group. London: RCP, 2010 25 Cancer Research UK Statistical Information Team. Calculation based on data from the Smoking, Drinking and Drug Use in Young People in England survey 2016. [Online] 2018. 26 Emory K, Saquib N, Gilpin EA, Pierce JP. The association between home smoking restrictions and youth smoking behaviour: a review. Tobacco Control. 2010 Dec 1;19(6):495-506. 27 Bottorff JL, Radsma J, Kelly M, Oliffe JL. Fathers’ narratives of reducing and quitting smoking. Sociology of health & illness. 2009 Mar;31(2):185-200. 28 Bottorff JL, Oliffe JL, Sarbit G, Caperchione C, Clark M, Anand A, Howay K. Assessing the feasibility, acceptability and potential effectiveness of an integrated approach to smoking cessation for new and expectant fathers: The Dads in Gear study protocol. Contemporary clinical trials. 2017 Mar 1;54:77-83. 29 Everett KD, Gage J, Bullock L, Longo DR, Geden E, Madsen RW. A pilot study of smoking and associated behaviors of low-income expectant fathers. Nicotine & Tobacco Research. 2005 Apr 1;7(2):269-76. 30 Bottorff JL, Oliffe JL, Sarbit G, Kelly MT, Cloherty A. Men’s responses to online smoking cessation resources for new fathers: The influence of masculinities. JMIR research protocols. 2015;4(2):e54. 31 Families Controlling and Eliminating Tobacco (FACET) website. Accessed 10/03/2020 32 Oliffe, J.L., Bottorff, J. L., & Sarbit, G. The right time... The right reasons… Dads talk about reducing and quitting smoking. 2010. Kelowna, BC: Institute for Healthy Living and Chronic Disease Prevention, University of British Columbia Okanagan, Canada. This publication is also available for download at: http://www.facet.ubc.ca and http://www.menshealthresearch.ubc.ca 33 Bottorff JL, Oliffe JL, Sarbit G, Huisken A, Caperchione C, Anand A, Howay K. Evaluating the feasibility of a gender-sensitized smoking cessation program for fathers. Psychology of Men & Masculinity. 2018 Nov 1. 34 The University of British Columbia. Dads in gear. Accessed 10/03/2020

13
35 Wilson I, Semple S, Mills LM, Ritchie D, Shaw A, O'Donnell R, Bonella P, Turner S, Amos A. REFRESH--reducing families' exposure to secondhand smoke in the home: a feasibility study. Tob Control. 2013;22(5):e8. 36 Hovell MF, Bellettiere J, Liles S, Nguyen B, Berardi V, Johnson C, Matt GE, Malone J, Boman-Davis MC, Quintana PJ, Obayashi S. Randomised controlled trial of real-time feedback and brief coaching to reduce indoor smoking. Tob Control. 2019 Feb 15. 37 Semple S, Turner S, O’Donnell R, Adams L, Henderson T, Mitchell S, Lyttle S, Amos A. Using air-quality feedback to encourage disadvantaged parents to create a smoke-free home: Results from a randomised controlled trial. Environ Int. 2018;120:104–110. 38 O’Donnell, R, Dobson, R, de Bruin, M, Turner, S, Booth, L and Semple, S. Development of a smoke-free homes intervention for parents: An intervention mapping approach. Health Psychology Bulletin. 2019 Dec 11;3(1), 67-86. 39 Dobson R, O'Donnell R, De Bruin M, Turner S, Semple S. Using air quality monitoring to reduce second-hand smoke exposure in homes: the AFRESH feasibility study. Tobacco Prevention and Cessation. 2017 Jun 30;3. 40 O’Donnell, R, Amos, A, Turner, SW, Adams, L, Henderson, T, Lyttle, S, Mitchell, S, Semple, S. ‘They only smoke in the house when I’m not in’: Understanding the limited effectiveness of a smoke-free homes intervention. Journal of Public Health (in press). 2020. 10.1093/pubmed/fdaa042. Accepted for publication. 41 Ratschen E, Thorley R, Jones L, Breton MO, Cook J, McNeill A, Britton J, Coleman T, Lewis S. A randomised controlled trial of a complex intervention to reduce children’s exposure to secondhand smoke in the home. Tobacco control. 2018 Mar 1;27(2):155-62. 42 Nichter, M.; Padmajam, S.; Nichter, M.; Sairu, P.; Aswathy, S.; Mini, G.K.; Bindu, V.C.; Pradeepkumar, A.S.; Thankappan, K.R. Developing a smoke free homes initiative in Kerala, India. BMC Public Health 2015, 15, 480. 43 Mdege N, Fairhurst C, Ferdous T, Hewitt C, Huque R, Jackson C, Kellar I, Parrott S, Semple S, Sheikh A, Swami S. Muslim Communities Learning About Second-hand Smoke in Bangladesh (MCLASS II): Study protocol for a cluster randomised controlled trial of a community-based smoke-free homes intervention, with or without Indoor Air Quality feedback. Trials 2019, 20, 11. 44 McNeill A, Brose LS, Calder R, Bauld L & Robson D. Evidence review of e-cigarettes and heated tobacco products 2018. A report commissioned by Public Health England. London: Public Health England.

1
Bit.ly/sipchallenge