Embed Size (px)
Citation preview

Abstract of thesis entitled
“Evidence-based Guidelines of Using Cryotherapy
in Reducing Pain, Knee Swelling and Improving
Range of Motion for Patients after Total Knee
Replacement”
Submitted by
Lui Pui Ling
for the degree of Master of Nursing at The University of Hong Kong
in July 2012
Introduction: Knee osteoarthritis is one of the common causes leading to
musculoskeletal disability of the elderly around the world. Total knee replacement
(TKR) is an effective and common treatment for end stage knee arthritis. Most
papers suggest that early rehabilitation could improve postoperative knee function.
However, postoperative pain and local swelling are the complications that
diminish range of motion (ROM) and inhibit patients’ recovery. A comprehensive
review of the literature reveals that cryotherapy is an effective and safe method to
overcome these complications. In this paper, a guideline of using cryotherapy in

reducing postoperative pain and knee swelling so as to improve the ROM of
patients and promote recovery after TKR has been developed.
Objectives: The objectives of this translational research are: (1) to look for
relevant papers that related to cryotherapy in reducing postoperative pain and
knee swelling so as to improve the ROM of patients after TKR; (2) to gather and
criticize the data obtained; (3) to develop a guideline of using cryotherapy in
reducing pain, knee swelling and improving ROM of patients after TKR based on
the evidence from the reviewed literature; (4) to assess the implementation
potential of the newly developed guidelines; and (5) to establish the
implementation and evaluation plans for the new innovation.
Methods: An empirical literature search published from 2001 to 2011 by several
searching engines regarding cryotherapy in reducing postoperative pain and knee
swelling with the aim to improve the ROM of patients after TKR has been
conducted. After that, the qualities of relevant studies were retrieved and
criticized by using the appraisal checklist of the SIGN (2004). The derived
evidences were then be summarized and synthesized. An evidence-based
guideline was established with reference to the evidence from the reviewed
literatures and the results of the quality assessment. Recommendations are graded
by SIGN (2004). The implementation potential including transferability,

feasibility and cost-benefit ratio of the innovation were assessed as well. Lastly,
implementation and evaluation plans have been developed to assess and appraise
the effectiveness of the new guideline.
Results: Finally, seven studies were chosen as final references after
methodological quality assessment. Four main types of comparison were made
from these seven reviews including: (1) continuous compressive cryotherapy vs.
compressive crepe bandage; (2) comparison in different temperature of
cryotherapy; (3) outcome measures; and (4) complications in cryotherapy. After
the summary, six main categories of recommendations were synthesized: (1)
continuous compression cryotherapy; (2) effective temperature; (3) potential
complications; (4) regular assessment; (5) duration; and (6) intermitted ice pack
regimen. Based on these syntheses and recommendations, a guideline of using
cryotherapy for patients after having TKR was developed.
Conclusion: With the implementation of the newly developed evidence-based
cryotherapy guidelines for patients after having TKR in local clinical settings, the
improvement in the ROM of the knee joint will be anticipated as a result of the
reduction in postoperative pain and knee swelling.

Evidence-based Guidelines of Using Cryotherapy in
Reducing Pain, Knee Swelling and Improving Range of
Motion for Patients after Total Knee Replacement
by
Lui Pui Ling
Bachelor of Nursing (Honors) H.K.U.
A thesis submitted in partial fulfillment of the requirements for
the Degree of Master of Nursing
at The University of Hong Kong
July 2012

Declaration
i
Declaration
I declare that the thesis and the research work thereof represents my own
work, except where due acknowledgement is made, and that it has not been
previously included in a thesis, dissertation or report submitted to this University
or to any other institution for a degree, diploma or other qualifications.
Signed ______________________________
Lui Pui Ling
Acknowledgements
ii
Acknowledgements
First of all, I owe my deepest gratitude to my thesis supervisor – Dr.
William Li. Without his encouragement, guidance and support in the preparation
and completion of this study, this dissertation would not have been possible.
Secondly, I would like to offer my heartily thankful to Dr. Daniel Fong and
Dr. Sharron Leung for their inputs and assistances in rendering tutorials and
comments.
Last but not the least, I offer my regards and blessings to my family, friends,
classmates and colleagues who supported me in any aspects throughout my study
of the Master Programme.

Contents
iii
Contents
Declaration i
Acknowledgements ii
Table of Contents iii
Lists of Appendices viii
Abbreviations ix
CHAPTER 1: INTRODUCTION
1.1 Background 1
1.2 Affirming Needs 3
1.3 Significance of the Study 4
1.4 Purpose of the Study 5
1.4.1 Research Questions 5
1.4.2 Objectives 5
1.4.3 Hypothesis 6
CHAPTER 2: CRITICAL APPRAISAL
2.1 Search Strategies 7
2.1.1 Study Selection Criteria 7
2.1.1.1 Inclusion Criteria 7
2.1.1.2 Exclusion Criteria 7
2.1.2 Searching Engines and Keywords Used 8
2.1.3 Extraction of Evidence 9
2.2 Appraisal Strategies 9
Contents
iv
2.3 Results 9
2.4 Summary and Synthesis of the Data 11
2.4.1 Data Summary 12
2.4.1.1 Continuous Compressive Cryotherapy vs.
Compressive Crepe Bandage
12
2.4.1.2 Continuous Cryotherapy vs. Intermitted
Cryotherapy
13
2.4.1.3 Cryotherapy vs. Epidural Anaesthesia 14
2.4.1.4 Comparison in Different Temperature of
Cryotherapy
15
2.4.1.5 Outcome Measures 16
2.4.1.6 Complications in Cryotherapy 17
2.4.2 Data Synthesis 17
2.4.2.1 Continuous Compression Cryotherapy 18
2.4.2.2 Effective Temperature 19
2.4.2.3 Potential Complications 20
2.4.2.4 Regular Assessment 20
2.4.2.5 Duration 21
2.4.2.6 Intermitted Ice Pack Regimen 22
2.4.2.7 Conclusion 22
CHAPTER 3: IMPLEMENTATION POTENTIAL
3.1 Target Settings and Audiences 23
3.1.1 Target Settings 23
3.1.2 Target Audiences 24

Contents
v
3.2 Transferability of the Findings 24
3.2.1 Proposed Setting 24
3.2.2 Proposed Audiences 25
3.2.3 Philosophy of Care 25
3.2.4 Popularity of the Innovation 27
3.2.5 Implementation and Evaluation Time 27
3.2.5.1 Implementation Time 27
3.2.5.2 Evaluation Time 28
3.3 Feasibility 29
3.3.1 Autonomy 29
3.3.2 Interfere Current Staff Functions 29
3.3.3 Support from Administration 30
3.3.4 Potential Barriers 30
3.3.5 Availabilities of Essential Equipments and Measuring Tools 32
3.4 Cost-Benefit Ratio of the Innovation 33
3.4.1 Potential Risks 33
3.4.2 Potential Benefits 33
3.4.3 Risks of Maintaining Current Practices 34
3.4.4 Cost for Implementation of New Protocol 34
3.4.4.1 Material Costs 34
3.4.4.2 Non-material Costs 35
3.4.5 Costs for Maintaining Current Practice 35
3.5 Conclusion 36

Contents
vi
CHAPTER 4: EVIDENCE BASED PRACTICE PROTOCOL
4.1 Background 37
4.2 Name of the Protocol 37
4.3 Objectives of the Protocol 37
4.4 Target Population of the Protocol 38
4.5 Rating System for the Recommendations 38
4.6 Practice Recommendations 39
4.7 Conclusion 45
CHAPTER 5: IMPLEMENTATION PLAN
5.1 Communication Plan 46
5.1.1 Identifying Stakeholders 46
5.1.2 Communication Plan with Stakeholders 47
5.1.2.1 Communication with Decision Makers 47
5.1.2.2 Communication with Project Team 48
5.1.2.3 Communication with Nurses in the Target Wards 51
5.1.2.4 Communication with Orthopaedic Doctors 52
5.1.2.5 Communication with Allied Health Professionals 52
5.2 Pilot Testing 53
5.2.1 Objectives 53
5.2.2 Target Setting and Target Population 53
5.2.3 Sampling Plan 54
5.2.4 Implementation 54
5.2.5 Outcomes to be Measured 55
5.2.6 Data Collection and Analysis 55

Contents
vii
5.2.7 Conclusion 56
CHAPTER 6: EVALUATION PLAN
6.1 Outcome to be Achieved 57
6.1.1 Primary Outcomes 57
6.1.2 Secondary Outcomes 59
6.2 Nature And Number Of Clients 61
6.2.1 The Nature of the Clients to be Involved 61
6.2.2 The Number of the Clients to be Involved 61
6.3 Time and Frequency of Taking Measurements 63
6.3.1 Primary Outcomes 64
6.3.2 Secondary Outcomes 64
6.4 Data Analysing Methods 65
6.5 Effectiveness of the Protocol 66
6.6 Conclusion 68
CHAPTER 7: SUMMARY 69
APPENDICES 70
REFERENCES 103

List of Appendices
viii
List of Appendices
Appendix 1: Table of Electronic Databases 70
Appendix 2: Tables of Evidences 72
Appendix 3: Levels of Evidences 79
Appendix 4: Grades of Recommendations 79
Appendix 5: Table of Critical Appraisals 80
Appendix 6: Summary of Levels of Evidences 95
Appendix 7: Criteria for Evaluating the Implementation Potential of an
Innovation under Scrutiny
96
Appendix 8: Cryotherapy Protocol Flow Chart 97
Appendix 9: Gannt Chart of Implementing the Protocol 98
Appendix 10: Pain Management Record Chart 99
Appendix 11: Knee Circumferences Record Chart 101
Appendix 12: Range of Motion Record Chart 102

Abbreviations
ix
Abbreviations
APN(s) Advance Practice Nurse(s)
BNI British Nursing Index
BNIA British Nursing Index and Archive
CB Compression Bandage
CINAHL Plus Cumulative Index of Nursing and Allied Health Literature
Plus
COS Chief of Service
CPM continuous passive motion devices
cryo cryotherapy
CT Cold Therapy
CTC Continuous temperature-controlled cryotherapy
D Postoperative Day
DOM Departmental Operational Manager
DVT deep vein thrombosis
EDA epidural anaesthesia
e.g. exempli gratia
etc. et cetera
Ev. evidence
F female
FPS-R Faces Pain Scale Revised
gp group
hr(s) hour(s)
IKDC International Knee Documentation Committee
kg kilogram
Lv. level
M male
mg milligram
min(s) minute(s)

Abbreviations
x
ml milliliter
mm millimeter
NCBI National Centre for Biotechnology Information
NO Nursing Officers
NRS Numerical Rating Scale
O&T Orthopaedics and Traumatology
OT operation
P level of significance
PCA patient controlled anaesthesia
post-op postoperative
pre-op preoperative
PT physiotherapist
RCT(s) randomized controlled trial(s)
ROM range of motion
SD standard derivation
SIGN Scottish Intercollegiate Guidelines Network
TKR total knee replacement
US United States
VAS Visual Analogue Scale
vs. versus
W / wk(s) Week(s)
WM Ward Manager
WOL Wiley Online Library
yr(s) old year(s) old

Chapter 1: Introduction
1
CHAPTER 1
INTRODUCTION
1.1 Background
Knee osteoarthritis is one of the common causes leading to musculoskeletal
disability of the elderly around the world. About 12% of the elderly aged over 65
in US as well as 15% of women and 6% of men in Beijing had symptomatic knee
osteoarthritis (Yan, Chiu, & Ng, 2011). Total knee replacement (TKR) is an
effective and common treatment for end stage knee arthritis. In the recent years,
the number of TKR performed each year is increasing rapidly in most developed
countries. The total number of TKR operations performed had increased by 150%
in the past decade in Australia (Lin et al., 2009) and increased by 69% from 1997
to 2005 in US (Yan, et al., 2011). According to Yan, et al. (2011), the annual
number of TKR operations performed had increased nearly double from 2000 to
2009 in Hong Kong. Moreover, Lin, et al. (2009) anticipated that the TKR
operations would continue to increase at least double in the following decade.
In view of the increasing number of TKR surgery, its complications
reported are also increased and become significance. There are numerous
complications reported from Coordinating Committee in Orthopaedics &
Traumatology (2011) including deep vein thrombosis, knee stiffness, wound or

Chapter 1: Introduction
2
chest infection, etc. Most studies proved that early mobilization or rehabilitation,
e.g. the use of CPM machine and postoperative exercise, could reduce the
postoperative complications (Brander & Stulberg, 2006; Pearse, Caldwell,
Lockwood, & Hollard, 2007) and improve the postoperative knee function
(Brander & Stulberg, 2006; Grella, 2008).
However, postoperative pain and local swelling are the great barriers that
inhibit patients’ recovery (Adie, Naylor, & Harris, 2010; Barry, Wallace, & Lamb,
2003). Some studies reported that the patients after operation would suffer from
acute and severe pain (Bonica, 1990; Crutchfield, Zimmerman, Nieveen,
Barnason, & Pozehl, 1996) as well as local swelling (Chou & Liu, 2008; Schroder
& Passler, 1994) during the early postoperative period and resulting in lowering
the motivation of the training adherence (Naylor, Harmer, Fransen, Crosbie, &
Innes, 2006). If the patients cannot participate in the training and perform the
activities of daily living after TKR, they cannot achieve the basic function of knee,
especially sitting on or getting out of a chair or sofa; going up or down stairs, etc.
Thus, their qualities of life would be affected. Finally, it will increase the
suffering of patient and affect the length of convalescence. In view of these,
adequate pain management and controlling localized swelling are necessary and
important.

Chapter 1: Introduction
3
1.2 Affirming Needs
Oral, intravenous or intramuscular analgesics are the common methods in
relieving postoperative pain for patients after TKR. However, most patients
reported dizziness and poor appetite which resulted from nausea and vomiting
after administrating the analgesics. Consequently, the wound healing progress will
be affected due to poor nutrition absorption. Also, patients will refuse
mobilization due to dizziness, as a result, slow down their rehabilitation.
Cryotherapy is one of the non-pharmacological methods to reduce the
traumatic or postoperative pain and swelling (Adie, et al., 2010). It is a therapy
that decreases the temperature of the skin surface by using ice bags or cold water
and applies on the injured tissues. The decreased the temperature of inner
structures (Martin, Spindler, Tarter, & Detwiler, 2002) and the conduction of
nerve signals (Abramson et al., 1966), the transmission of harmful signals and
inflammatory response will be suppressed (Matsen, Questad, & Matsen, 1975).
Consequently, the pain sensation and swelling will be reduced. In addition,
cryotherapy is a safe and economical way to manage the postoperative pain. Most
patients have positive comments in using cryotherapy (Lombardi, Drouillard,
Mallory, & Vaughn, 1993).
Cryotherapy is often used in early postoperative phase after orthopaedic

Chapter 1: Introduction
4
surgery in order to promote healing in British and Australia (Barry, et al., 2003;
Naylor, et al., 2006). However, it is not a common practice in other countries,
such as Hong Kong. In the proposed wards, it is not a routine practice to apply
cryotherapy for patients after TKR. Also, there is still controversial in the
advantages of this practice for the patients following TKR (Adie, et al., 2010).
Besides, the benefit of different interventions in cryotherapy is less justifiable, for
example, bandaging vs. cryotherapy, continuous vs. intermittence cryotherapy,
cryotherapy in acute phase vs. cryotherapy in whole recovery phase, the
effectiveness in different temperature of cryotherapy, etc. Moreover, as discussed
as above, the postoperative rehabilitation and range of motion (ROM) of knee are
associated with the effectiveness of postoperative pain management and knee
swelling. The consequence of poor pain control will affect the patients’ activities
of daily living and qualities of life after TKR. In consideration of the problems, a
study about the effectiveness of cryotherapy for patients after TKR in reducing
pain, knee swelling and promoting ROM of knee is important.
1.3 Significance of the Study
The pain and rehabilitation is in directed relationship: the poor pain control,
the lower motivation in rehabilitation. Thus, the patients’ activities of daily living
and qualities of life will be affected. As discussed, cryotherapy is a safe,

Chapter 1: Introduction
5
economic and effective practice compared with administrating analgesics alone.
In view of this, it seems that cryotherapy is one of the most feasible interventions
performed by nurses in reducing postoperative pain for patient with TKR. Based
on Melnyk and Fineout-Overholt (2005), the evidence-based practice would guide
to the highest quality of care. Therefore, the study of the effectiveness of
cryotherapy should be developed to improve practice for the patients’ best
interests.
1.4 Purpose of the Study
The purpose of the study is to evaluate the effectiveness of cryotherapy and
develop a cryotherapy protocol in reducing postoperative pain and knee swelling
for patients after TKR in order to improve the ROM of knee.
1.4.1 Research Questions
Is the cryotherapy effective in reducing postoperative pain, knee swelling
and improving the ROM of knee for patient after TKR?
1.4.2 Objectives
The objectives of this project are:
1. to gather the searched evidences on cryotherapy for patients after TKR.
2. to apply the findings and develop an evidence-based protocol on
cryotherapy in reducing postoperative pain and knee swelling for

Chapter 1: Introduction
6
patients after TKR.
3. to assess the feasibility of implementing the proposed protocol
4. to plan for the implementation of the protocol
5. to evaluate the effectiveness of the protocol in reducing pain and knee
swelling.
1.4.3 Hypothesis
The patients who receive the cryotherapy will share of having less pain
sensation verbally and less differences in bilateral knee circumference as well as
improving ROM of knee for patients after TKR.

Chapter 2: Critical Appraisal
7
CHAPTER 2
CRITICAL APPRAISAL
After affirming the needs and significances of the study in the previous
chapter, the following step is to search the relevant evidences as well as criticize
and synthesize the selected data. In this chapter, the searching strategies, its results,
appraisal strategies as well as the summary and the synthesis of the searched data
will be presented.
2.1 Search Strategies
2.1.1 Study Selection Criteria
2.1.1.1 Inclusion Criteria
This review would comprise the studies involving patients who had
performed knee surgeries, especially those with TKR. The studies about the
cryotherapy interventions in reducing postoperative pain and swelling would be
included as well. The interventions were able to implement by nurses in ward or
clinic settings. The studies which were published in English language, accessible
full text and the publication year after 2001 would also be included. Furthermore,
only controlled trials studies would be selected.
2.1.1.2 Exclusion Criteria
The studies which targeted on the postoperative treatment of other parts of
Chapter 2: Critical Appraisal
8
the body except knee would be excluded. The interventions which could not be
performed by nurses were also expelled. Moreover, the studies that were not
related in reducing pain and swelling of injured knee were ignored. This project
would reject the studies with participants who were disorientated or suffering
from psychiatric disorders as which could be a factor affecting the results.
2.1.2 Searching Engines and Keywords Used
Several electronic databases were used for the systematic search in this
paper, including MEDLINE via Ovid (1948 – 2011), British Nursing Index (BNI)
via Ovid (1994 – 2011), British Nursing Index and Archive (BNIA) via Ovid
(1985 – 2011), Cumulative Index of Nursing and Allied Health Literature Plus
(CINAHL Plus) via EBSCOhost, PubMed via National Centre for Biotechnology
Information (NCBI) and the Cochrane Library via Wiley Online Library (WOL).
An integrated search were applied through several attempts and
combinations with the use of keywords “total knee arthroplasty”, “total knee
replacement”, “cryotherapy”, “cold therapy” and “pain”. The related articles from
reference list of the selected studies were also assessed for suitability. The
searches were performed before 5th September 2011. Details of the database and
keywords used for searching are presented in Appendix 1.

Chapter 2: Critical Appraisal
9
2.1.3 Extraction of Evidence
The useful data would be extracted into tables by using the reference table
from “SIGN 50: A Guideline Developer's Handbook - Annex D: Completed
Evidence Table” of Scottish Intercollegiate Guidelines Network (2008) to develop
tables of evidences. The details of the table are listed in Appendix 2.
2.2 Appraisal Strategies
The “Controlled trial” critical appraisal tool in “SIGN 50: A Guideline
Developer's Handbook - Annex C: Critical appraisal - Notes and checklists” from
Scottish Intercollegiate Guidelines Network (2008) would be used to appraise the
quality of the identified paper. The details of the critical appraisal will be given in
Appendix 5.
The rating system for the hierarchy of evidence in “SIGN 50: A Guideline
Developer's Handbook - Annex B: Key to Evidence Statements and Grades of
Recommendations” from Scottish Intercollegiate Guidelines Network (2008) was
used to evaluate the level of evidence (see Appendix 3) and the grades of
recommendations (see Appendix 4).
2.3 Results
After matching with the above selection criterion, seven studies (see
Appendix 1) were chosen and analyzed in light of the table of evidence and

Chapter 2: Critical Appraisal
10
critical appraisal tool from Scottish Intercollegiate Guidelines Network (2008).
Five studies were selected by using MEDLINE via Ovid (1948 – 2011) (Gibbons,
Solan, Ricketts, & Patterson, 2001; Kullenberg, Ylipää, Söderlund, & Resch, 2006;
Morsi, 2002; Radkowski, et al., 2007; Smith, Stevens, Taylor, & Tibbey, 2002).
One study was identified in both British Nursing Index (BNI) via Ovid (1994 –
2011) and British Nursing Index and Archive (BNIA) via Ovid (1985 – 2011)
(Smith, et al., 2002). From Cumulative Index of Nursing and Allied Health
Literature Plus (CINAHL Plus) via EBSCOhost, one study was chosen (Smith, et
al., 2002). In PubMed via National Centre for Biotechnology Information (NCBI),
five studies were found (Holmström & Härdin, 2005; Kullenberg, et al., 2006;
Morsi, 2002; Radkowski, et al., 2007; Smith, et al., 2002). Finally, no study was
picked out from the Cochrane Library via Wiley Online Library (WOL).
Moreover, one study was discovered from the reference lists (Woolf, Barfield,
Merrill, & McBryde, 2008).
There was one prospective controlled trial (Morsi, 2002), whereas others
were randomized controlled trial (Gibbons, et al., 2001; Holmström & Härdin,
2005; Kullenberg, et al., 2006; Radkowski, et al., 2007; Smith, et al., 2002; Woolf,
et al., 2008). Among the six RCT studies, however, two of them did not clearly
stated the randomization and concealment method (Gibbons, et al., 2001;

Chapter 2: Critical Appraisal
11
Holmström & Härdin, 2005); two of them only stated the randomization method
(Smith, et al., 2002; Woolf, et al., 2008), while another study stated with
concealment method only (Kullenberg, et al., 2006).
All of target participants underwent TKR, except one paper which target
groups was those performed knee arthroscopy (Woolf, et al., 2008). Holmström &
Härdin (2005) had two experimental groups and one control groups, while the
remaining studies had one experimental group and one control group. The sample
size of the studies were ranged from 60 to 86.
The levels of evidence of seven selected studies were ranged from 1++ to
1 – and the summary is listed in Appendix 6. All the RCTs were rated at level 1
according to the definition of the levels of evidence in Appendix 3. One study was
rated as 1 – (Morsi, 2002), one study was rated as 1++ (Radkowski, et al., 2007)
and the remaining studies were rated as 1 + (Gibbons, et al., 2001; Holmström &
Härdin, 2005; Kullenberg, et al., 2006; Smith, et al., 2002; Woolf, et al., 2008).
2.4 Summary and Synthesis of the Data
According to the results of the tables of evidence, critical appraisals and the
levels of evidence from the identified articles, the summary and synthesis of data
will be shown in this paragraph.

Chapter 2: Critical Appraisal
12
2.4.1 Data Summary
Four main types of comparison could be categorized from these seven
papers and the details of the summary are listed as follow:
2.4.1.1 Continuous Compressive Cryotherapy vs. Compressive Crepe
Bandage (3 Studies)
Three studies, which purposes were to compare the differences between
continuous compressive cryotherapy and compressive crepe bandage in reducing
postoperative pain and ROM, were identified (Gibbons, et al., 2001; Morsi, 2002;
Smith, et al., 2002). From Gibbons, et al. (2001), the continuous compressive cold
therapy was applied to the intervention group by an inflated cryocuff that filled
with ice water to provide compression and cold therapy on the affected knee,
while, modified Robert Jones bandage with compression effect only was applied
to the control group. The subjective pain sensation was mild decreased and the
ROM of knee was a bit wider in the cold compression group. However, the results
were less statically significant. In Morsi (2002), both intervention and control
group were wrapped with compressive crepe bandage on the operation site. Only
extra cooling flow was applied in the intervention group. It suggested that the
continuous compressive cryotherapy had significant improvement in pain control
with less subjective pain score and analgesic used as well as ROM compared with

Chapter 2: Critical Appraisal
13
compressive crepe bandage. For Smith, et al. (2002), continuous cryotherapy was
applied in the first 24 hours after operation for the intervention group; on the other
hand, crepe bandage was kept intact for the control group in the first 24 hours. It
stated a bit decrease in swelling and more flexion in intervention group. The pain
score was similar in both intervention and control group in the first 24 hours. But
the results were less statically significant as well.
To sum up, all three studies revealed that continuous compressive
cryotherapy had greater benefits in reducing postoperative pain, swelling and
improving ROM of knee for patients after TKR although two studies (Morsi, 2002;
Smith, et al., 2002) with less statically significant. Moreover, no complication
such as adverse effect on wound healing was exposed in these three studies.
2.4.1.2 Continuous Cryotherapy vs. Intermitted Cryotherapy (1 Study)
A study was distinguished to compare the difference between continuous
cryotherapy and intermitted cryotherapy (Woolf, et al., 2008). The researchers set
the continuous cryotherapy machine for patient in intervention group. For control
group, the patient was applied ice bag with compressive dressing for 20 minutes
in every two hours at daytime. It showed the continuous cryotherapy was better in
pain control than intermitted ice pack regimen at first two postoperative days.
Besides, the patients had less pain at night time significantly. However, in latter

Chapter 2: Critical Appraisal
14
postoperative period, the participants told that intermitted ice pack regimen has a
bit lower pain sensation than continuous cryotherapy.
Overall, continuous cryotherapy had better pain control, especially during
night time, than intermitted ice pack regimen in the early postoperative stage after
knee surgery. Also, it was a safe procedure without developing thermal skin injury,
nerve palsy or infection in the study.
2.4.1.3 Cryotherapy vs. Epidural Anaesthesia (2 Studies)
Two studies compared the differences between cryotherapy and epidural
anaesthesia (Holmström & Härdin, 2005; Kullenberg, et al., 2006). There were
three experimental groups in Holmström & Härdin (2005) study. They suggested
using cryocuff to provide cold therapy for one of the experimental groups and
continuous epidural anaesthesia infusion for another experimental group. Also, a
control group with traditional analgesics only was introduced to compare with the
two experimental groups. The results inferred that no significant different
observed about subjective pain scores at rest or on motion in the three groups.
However, there was significantly decrease in the used of morphine in both
continuous cryotherapy and epidural anaesthesia which compared to the control
group. Also, it revealed that the patients in cryotherapy group decrease morphine
consumption constantly even after discontinuous the cryotherapy and no

Chapter 2: Critical Appraisal
15
morphine was requested after postoperative day 4, while the other group
consumed morphine continuously until postoperative day 7. There was a bit
reduced in knee swelling for patients in the cryotherapy group. But no significant
different observed in passive or active ROM in all three groups of participants.
Kullenberg, et al. (2006) compared the variation between cold compression
therapy and epidural analgesia therapy. The cyrocuff was applied for patients in
the intervention group and the epidural analgesia was used in the comparsion
group. The patients had less pain sensation and morphine consumption in the cold
compression group. Moreover, the ROM improved significantly in the cold
compression group.
In short, both studies said that the cryotherapy had better advantages in pain
controls which used less analgesic than epidural anaesthesia. One study
(Kullenberg, et al., 2006) believed cryotherapy would improved the ROM and
shorten the rehabilitation period, whereas, another study (Holmström & Härdin,
2005) showed less differences in knee swelling and ROM between the two
groups.
2.4.1.4 Comparison in Different Temperature of Cryotherapy (1
Study)
Only one study (Radkowski, et al., 2007) verified the effectiveness in

Chapter 2: Critical Appraisal
16
different temperature of cryotherapy. The researchers set the temperature of
cryocuff at 45°F in intervention group and at 75°F in the comparison group. The
results reported that there were no significant differences or improvement of
patients with colder temperature cryotherapy devices in pain sensation, opioid
consumption and ROM.
2.4.1.5 Outcome Measures (All Studies)
All studies using similar visual analogue pain scale with variable range to
measure the subjective pain sensation, including 0 – 100 (Gibbons, et al., 2001),
0 – 10 (Holmström & Härdin, 2005; Radkowski, et al., 2007), 1 – 10 (Morsi, 2002;
Smith, et al., 2002) and 5-point scale (Woolf, et al., 2008), while one study did not
stated its range clearly (Kullenberg, et al., 2006).
For knee swelling, two studies had dabbled in this category. One study
described the measurement method in details (Holmström & Härdin, 2005),
whereas another study only stated to measure the swelling by physiotherapists at
the same time for three days from pre-operation to day 2 (Smith, et al., 2002).
For range of motion, there were five studies which looked into this aspect.
One study illustrated the measurement method in details (Holmström & Härdin,
2005), whereas others studies just presented with measuring time or measurement
tools briefly (Kullenberg, et al., 2006; Morsi, 2002; Radkowski, et al., 2007;

Chapter 2: Critical Appraisal
17
Smith, et al., 2002).
2.4.1.6 Complications in Cryotherapy (6 Studies)
Six studies had reported about the complication of cryotherapy in their
papers (Gibbons, et al., 2001; Holmström & Härdin, 2005; Kullenberg, et al.,
2006; Morsi, 2002; Radkowski, et al., 2007; Woolf, et al., 2008). Among these
researches, four studies reported there was no cryotherapy-related complication
observed (Gibbons, et al., 2001; Morsi, 2002; Radkowski, et al., 2007; Woolf, et
al., 2008). From Holmström & Härdin (2005), they mentioned that one patient
requested to take off the cryocuff during the expirmental period and one patient
had cold sensation but continue the procedure. Kullenberg, et al. (2006) told there
was one patient with deep vein thrombosis and one patient with superficial
infection of unknown reason in the cryotherapy group. Overally, cryotherapy was
a harmless treatment which compared with other analgesics especially epidural
anaesthesia.
In conclude, cryotherapy was a safe and effective procedure in reducing
postoperative pain, swelling and improving ROM of knee for patients after TKR.
2.4.2 Data Synthesis
After extracting and summarizing the data, cryotherapy seemed to be
recommended for patient after TKR. In this part, the evidences in previous

Chapter 2: Critical Appraisal
18
paragraph are synthesized and presented as follow to maximize the benefit of
cryotherapy:
2.4.2.1 Continuous Compression Cryotherapy
Three studies used cryocuff as a means to provide cryotherapy for the
patients in the intervention groups (Gibbons, et al., 2001; Holmström & Härdin,
2005; Kullenberg, et al., 2006). Cryocuff was a device with an inflated cuff that
consisted of cold and compression effects at the same time. Among these three
studies, two studies proved cryotherapy with cryocuff had significantly decreased
in the use of analgesics and postoperative swelling as well as improved ROM for
patient with TKR (Holmström & Härdin, 2005; Kullenberg, et al., 2006), whereas
another study showed little improvement in pain control and ROM. Comparing
with Morsi (2002), the researcher used two bottles which connected with a plastic
tube and coiled around the affected knee. The cold therapy was given from the
cold water in a bottle which hanged at higher level to a lower empty bottle via the
coiled plastic tube. To sustain the cryotherapy, the two bottles needed to change
frequently. This research proved continuous cryotherapy was beneficial to the
patients with TKR as well. Among these studies, cryocuff was recommended to be
the device for continuous compressive cryotherapy comparatively. Not only the
proven advantages in pain control and reduced postoperative swelling, but also

Chapter 2: Critical Appraisal
19
less labour involved in managing the cold treatment. Ice water was just needed to
change when it melted. Some cryocuff instruments even could maintain the
required temperature and it saved extra manpower to manage the system.
2.4.2.2 Effective Temperature
Four studies had mentioned about temperature used of cryotherapy in their
studies (Holmström & Härdin, 2005; Morsi, 2002; Radkowski, et al., 2007; Smith,
et al., 2002). Holmström & Härdin (2005) tried 10°C to 15°C cold therapy in their
study. Morsi (2002) kept the skin temperature at 7°C ±2°C for two hours after
surgery and then kept at 12°C±3°C in the remaining time. Smith, et al. (2002) set
the cryotherapy machine at 2°C to 5°C in their experiment. One of the studies
even compared two different temperatures (45°F and 75°F) in the research
(Radkowski, et al., 2007). From the above studies, two studies showed the
cryotherapy with temperature from 7°C to 15°C had significant advantages on
pain control and ROM (Holmström & Härdin, 2005; Morsi, 2002). However,
Radkowski, et al., (2007) believed that there was no great difference of
cryotherapy with warmer or cooler temperature. Moreover, a study warned that
low temperature may increase the risk of tissue damage (Farry, Prentice, Hunter,
& Wakelin, 1980). Thus, to balance the pros and cons, cryotherapy which kept at
12°C to 15°C would be suggested and regular checking should be implemented to

Chapter 2: Critical Appraisal
20
prevent complications.
2.4.2.3 Potential Complications
Five studies raised the potential complications that would occur for patients
with cryotherapy (Kullenberg, et al., 2006; Morsi, 2002; Radkowski, et al., 2007;
Smith, et al., 2002; Woolf, et al., 2008). Kullenberg, et al., (2006) revealed one
patient in the cryotherapy group suffered from deep vein thrombosis whereas the
remaining studies did not discover any complications from the researches.
However, the studies had mentioned about the potential complication in their
studies, including discomfort feelings (Smith, et al., 2002), frostbite (Morsi, 2002;
Woolf, et al., 2008), nerve palsy (Morsi, 2002; Radkowski, et al., 2007; Woolf, et
al., 2008), wound dehiscence (Radkowski, et al., 2007), infection (Woolf, et al.,
2008), blisters (Smith, et al., 2002) and compartment syndrome (Smith, et al.,
2002). Therefore, regular assessment was highly recommended to prevent the
undesired complications.
2.4.2.4 Regular Assessment
Nurses would approach the patients regularly to re-chill the device or
change ice water for the reason of maintaining the cryotherapy in two researches
(Holmström & Härdin, 2005; Kullenberg, et al., 2006). Holmström & Härdin
(2005) recommended nurses should approach the patients every six hours or more

Chapter 2: Critical Appraisal
21
often in order to change the ice water and assess the patients for any discomfort.
Kullenberg, et al. (2006) just suggested nurses should encounter the patients for
re-chilling the device every 60 minutes and changing ice water every four hours
with checking of any complications. Combining these two suggestions, regular
assessment of complications and patients’ discomfort every four hours minimally
would be proposed in order to minimize the nurses’ workload and prevent the
unwanted complications.
2.4.2.5 Duration
All studies had discussed about the suitable length of applying cryotherapy
(Gibbons, et al., 2001; Holmström & Härdin, 2005; Kullenberg, et al., 2006;
Morsi, 2002; Radkowski, et al., 2007; Smith, et al., 2002; Woolf, et al., 2008).
However, different studies suggested different durations. Gibbons, et at., (2001)
thought the cryocuff should be placed at least six hours during the daytime until
discharge. Holmström & Härdin (2005) believed the cold therapy should be
continued for 48 hours. Kullenberg, et al. (2006) said the cryotherapy should be
applied for three days. Morsi (2002) instructed to coil the continuous cooling
device for six days. Radkowski, et al., (2007) advised to continue the cryotherapy
upon discharge. Smith, et al., (2002) told the cryo treatment should be performed
for the first 24 hours and then followed by intermitted ice pack regimen for the

Chapter 2: Critical Appraisal
22
next 24 to 48 hours. Woolf, et al. (2008) recommended to wrap the cryocuff for
minimum four days. Moreover, they proved that continuous cryotherapy had
better pain control, especially during night time, on the second postoperative day.
After synthesizing the advices and considering the manpower required, the
continuous cryotherapy would be suggested at the first 48 hours for patients with
TKR.
2.4.2.6 Intermitted Ice Pack Regimen
Two studies used intermitted ice pack regimen in their researches (Smith, et
al., 2002; Woolf, et al., 2008). Smith, et al., (2002) suggested to apply ice pack in
plastics bag and wrapped with a towel three times a day for 15 minutes. Woolf, et
al., (2008) proposed to provide ice pack with compressive dressing for 20 minutes
every two hours. In view of the advantages of cold therapy and labour intensive,
ice pack regimen was advised to be given four times per day for 20 minutes after
ceasing the continuous cryotherapy machine.
2.4.2.7 Conclusion
To sum up, cryotherapy, whatever continuous or intermitted, had benefits
for patients with TKR in reducing postoperative pain, swelling and improve
postoperative ROM. Therefore, developing a cryotherapy protocol for patients
after TKR is necessary.

Chapter 3: Implementation Potential
23
CHAPTER 3
IMPLEMENTATION POTENTIAL
As talked in the previous chapters, TKR is a common orthopaedic surgery
in Hong Kong. Thus, the complications (e.g. postoperative pain, knee swelling
and ROM, etc.) after the surgery cannot be neglected. In view of this, it is
essential to develop an evidence-based protocol. However, before this can be
achieved, the implementation potential of the innovation should be evaluated.
Therefore, in this chapter, the implementation potential of the innovations
including transferability of the findings, feasibility and the cost-benefit ratio of the
innovation, which based on the criteria discussed by Polit & Beck (2008), will be
assessed and presented (see Appendix 7).
3.1 Target Settings and Audiences
The target settings and audiences should be identified at the beginning.
3.1.1 Target Settings
The target settings are the orthopaedics and traumatology (O&T) wards of a
public hospital from Hospital Authority. There are two O&T wards in this hospital,
one is a male ward and another is female ward. Each ward has 42 beds and serves
about 200 patients with TKR performed annually. The average length of stay in
hospital is about 12 – 16 days.

Chapter 3: Implementation Potential
24
3.1.2 Target Audiences
The target audiences are the patients who have undergone TKR in the target
wards, except those who have contraindication to cryotherapy such as circulatory
insufficiency (e.g. peripheral vascular disease), cold allergy (e.g. cold urticaria),
cutaneous sensory abnormalities, cryoglobulinemia, Raynaud’s phenomenon,
haemoglobinopathy and advanced diabetes, etc (Chatap, De Sousa, Giraud, &
Vincent, 2007; Nadler, Weingand, & Kruse, 2004). Furthermore, they should be
cognitive intact to follow the instructions and willing to apply the cryotherapy at
the postoperative stages after explanation.
All the nurses in the target wards are responsible for applying the
cryotherapy. They should understand the protocol thoroughly before delivering it.
Therefore, they should receive some training before delivering the interventions.
3.2 Transferability of the Findings
3.2.1 Proposed Setting
Although all the previous studies did not mention the target settings and the
conduction places, the entire target populations of the researches were performed
knee surgeries which usually took place in O&T wards. Therefore, the innovation
can be transferred to the proposed settings.

Chapter 3: Implementation Potential
25
3.2.2 Proposed Audiences
The subjects of the previous studies were similar to the proposed audiences.
The participants of five studies were undergone TKR (Gibbons, et al., 2001;
Kullenberg, et al., 2006; Morsi, 2002; Radkowski, et al., 2007; Smith, et al., 2002)
whereas the samples of one study was performed unicompartmental knee
arthroplasty (Holmström & Härdin, 2005) and the remained one was performed
knee arthroscopy (Woolf, et al., 2008). Also, the age of the reviewed studies was
around 63 to 72 years old, which was similar to the age of the target audiences
who generally aged over 60 years old. Moreover, the responsible staffs of
previous studies were also similar to the proposed settings as well. Three studies
presented that nurses were responsible staff (Holmström & Härdin, 2005;
Kullenberg, et al., 2006; Radkowski, et al., 2007) whereas two studies reported
that the physiotherapists were responsible for the interventions (Gibbons, et al.,
2001; Radkowski, et al., 2007).
To sum up, the populations involved are similar to the proposed audiences
and therefore the findings can be transferable.
3.2.3 Philosophy of Care
There are numerous philosophies of cares underlying the innovation which
are similar to the proposed setting.

Chapter 3: Implementation Potential
26
The innovation proposed is evidence-based which will improve the quality
of nursing care and enhance the professional image. Medical Service
Development Committee of Hospital Authority (2002) encourages the use of
clinical practice guideline which has the potential to align clinical practice to
scientific evidence. Hospital Authority (2002) also promotes high quality patient
care by striving for the highest standard of nursing practice. It supports the staff to
make clinical decision basing on evidence-based research. It will create an
environment with and for staff to enhance their potential as well.
The second philosophy of care of the innovation is to help the patients
relieve the undesired pain sensations after surgery. Hospital Authority (2002)
suggests the role of O&T nurses should identify and treat the acute and chronic
pain which frequently occur in the orthopaedic population.
The third philosophy of care of the innovation is to enhance the quality of
patient-centred services in order to improve the quality of life. The core value of
Hospital Authority is to provide quality patient-centred care through teamwork.
Hospital Authority (2002) believes that O&T nurses should provide
individualized and high quality nursing care for all clients and their families.
Lastly, the innovation proffers to provide cost-effective and safe nursing
practice to patients. Hospital Authority (2002) bolsters the O&T nurses to provide

Chapter 3: Implementation Potential
27
cost-effective nursing care to patients. Hospital Authority (2010) also encourages
promoting continuously service quality and safety.
In sum, the philosophy of care underlying the innovation is similar to the
philosophy prevailing in the proposed setting, and thus the findings of the
previous studies can be transferable.
3.2.4 Popularity of the Innovation
As discussed before, the target settings serve about 200 patients to undergo
TKR in each ward every year. There are two O&T wards in this hospital. Hence,
the total number of the patients who benefit from the innovation will be about 300
patients annually. There is sufficiently large number of clients to get the
advantages from the new protocol.
3.2.5 Implementation and Evaluation Time
3.2.5.1 Implementation Time
The first step of starting the evidence-based protocol is to get the approval
and support from the decision makers. The Chief of Service, General Manager
(Nursing), Departmental Operational Manager, Ward Manager and Nursing
Officers or Advance Practice Nurses should be communicated as well as to get
their approval and support before. It takes around two days to discuss with them.
The cooperation of orthopaedic doctors and allied health professionals are also

Chapter 3: Implementation Potential
28
important. After that, it needs about two months to develop this guideline by the
project coordinator. Time of preparing equipments (e.g. goniometer,
documentation charts, etc.) have to be counted as well. For the cryocuff and ice
maker which are already in wards, no extra time is required to prepare. Finally, it
requires about six to eight sessions to introduce the new protocol to the nurses in
the proposed settings which consumes about one to two week. Five to six nurses
will be attended in each training session. The duration of each session lasts for
about one to two hours.
3.2.5.2 Evaluation Time
The outcomes can be evaluated into three aspects. For the impact evaluation,
the attitudes, skills and understandings of the new protocol can be measured. It is
a short term evaluation. The perception and competency of implementing the new
protocol will be assessed after the introduction sessions by questioning staff in
question and answer session and getting verbal feedback from staff. For the
process evaluation, the utility of the proposed protocol and its quality will be
monitored. It is a long term evaluation which assures the staff putting the protocol
into practice efficiently and effectively as planned via regular review and
feedback from colleagues. For the outcome evaluation, the differences of pain
sensation, knee swelling and its ROM after implementing the protocol will be

Chapter 3: Implementation Potential
29
checked. It is a long term evaluation. Pain sensation will be assessed regularly for
patients with standard pain assessment tools used in ward during their length of
stay; the knee swelling should be recorded regularly by measuring the knee
circumferences and the ROM of knee will be checked regularly by using
goniometer.
3.3 Feasibility
3.3.1 Autonomy
According to Hospital Authority (2002), nurses can make clinical decision
basing on nursing process, theory, research and specific orthopaedics knowledge.
Moreover, cryotherapy is a non-pharmacological procedure and safe practice
which is allowed to use by clinical judgement of nurses in the target setting. In
view of this, the nurses will have freedom to carry out and terminate the
innovation by their knowledge and judgement.
3.3.2 Interfere Current Staff Functions
As talked before, nurses have the autonomy to apply cryotherapy by their
clinical decision. Moreover, the cryocuff is applied after operation immediately in
the operation theatre. Therefore, the nurses are required regular assessment in
each shift only. During these times, they could assess the signs of complication
and the pain intensity of the patients as well as maintain the temperature of the

Chapter 3: Implementation Potential
30
cooler. For these reasons, the implementation of the innovation will not interfere
with the current staff functions.
3.3.3 Support from Administration
Hospital Authority supports clinical practice guideline to align clinical
practice with scientific evidence in local health care settings (MSDC, HA, 2002)
as well as create an environment with and for staff to enhance their potential. The
mission of the target hospital is “to provide a level of care and services good
enough for our own patients”, thus it supports good practices to improve the
quality of health care services. The orthopaedics department also advocates
individualized, high quality and cost-effective nursing care to all patients (HA,
2002). Furthermore, the wards are welcome evidence-based practice to improve
the quality of nursing. The staff can discuss concerns, share opinion and conclude
new workable procedure in the regular staff meeting. As a whole, the
administrations involved support the innovation.
3.3.4 Potential Barriers
There may be some potential barriers in implementing the innovation by
several parties. Firstly, approval and support from the decision makers, e.g. COS,
DOM, WM, NO and APN, ought to be obtained. The protocol cannot be
implemented if they turn down. The proposal including significances of pain

Chapter 3: Implementation Potential
31
management and effectiveness of cryotherapy with evidence support as well as
the advantages of changes such as reducing the length of stay, feasibility and
cost-effectiveness with a budget plan will be presented in the meeting and
persuade their support.
Next, the nurses who are responsible for the programme in the ward should
be informed for the details of the protocol. The compliance and acceptance of the
nurses are important in the success of implementation of the protocol. However,
most people are not willing to change the usual practice and adopt another new
protocol, besides, it benefit themselves and other people. Hence, advantages of
implementing new protocols, e.g. reducing the length of stay and increasing
professional image as well as clarification of misunderstand and uncertainties of
the protocol should be explained to the staff in advance in order to enhance their
acceptances and interests. Moreover, the skill of applying cryotherapy is ought to
be taught to new staff for promoting the compliance.
Then, the cooperation of orthopaedic doctors is also important as they are
responsible for applying the cryocuff after operation, prescribing the medications
and the post operation treatments for the patients. The responsible staff will
explain the details of the protocol and implementation strategies to the
orthopaedic doctors in their weekly meeting with a question and answer session to

Chapter 3: Implementation Potential
32
explain and clarify their concerns in order to invite their participance as well as
enhance their acceptances and cooperation.
Also, the allied health professionals such as physiotherapists and
occupational therapists are another leading factor in successful protocol
implementation. They play important roles in rehabilitation of patients after
surgery. Therefore, the cooperation of them is another hit to increase the
compliance of the protocol of the patients. The responsible staff will also explain
the details of the protocol and the implementation strategies to the allied health
professionals in their weekly meeting with a question and answer session to
explain and clarify their concerns in order to invite their participance as well as
enhance their acceptances and cooperation.
Except these, there are other unpredictable barriers which cannot be
identified previously. For the sake of preventing them, a pilot study is worth to
perform before the implementation. The pilot study will reveal the actual and
concrete problems or barriers in implementation of the proposed evidence-based
practice.
3.3.5 Availabilities of Essential Equipments and Measuring Tools
Although nearly all necessary instruments including cryocuff with
temperature control, ice maker, plastics bags, tape water and electricity are

Chapter 3: Implementation Potential
33
available in the ward, it is not a practice to apply cryotherapy after TKR in the
target setting. Therefore, it is worth to develop the new protocol in order to
increase the quality of nursing care. Besides, the measuring tools, e.g. pain score
assessment tools and measuring tools except goniometer, the knee circumferences
and ROM record charts are used in wards already as well.
3.4 Cost-Benefit Ratio of the Innovation
3.4.1 Potential Risks
The major potential risk of using cryotherapy is cold related complication
development, like intolerant cold sensation, frostbite, transient nerve palsy, wound
dehiscence and deep vein thrombosis. From the studies, the complication is rare.
Only two patients complaint of intolerant cold sensation and one patient develop
deep vein thrombosis (Gibbons, et al., 2001; Holmström & Härdin, 2005;
Kullenberg, et al., 2006; Morsi, 2002; Radkowski, et al., 2007; Smith, et al., 2002;
Woolf, et al., 2008). Most complication like intolerant cold sensation, frostbite or
transient nerve palsy can be relieved after stopping the cryotherapy. For wound
dehiscence, sufficient nutrition support can promote wound healing. For the DVT,
adequate limbs exercise can prevent it development.
3.4.2 Potential Benefits
Despite of the potential risks, there are some potential benefits of the

Chapter 3: Implementation Potential
34
innovation. For the patients, the decreasing of pain sensation and swelling will
promote their rehabilitation and reduce the complication. Hence, their quality of
life can be improved. For the health care providers, their professional image and
knowledge will be increased as well as decrease the length of stay and
complication development. As a result, their workload can be reduced. For the
hospital, the medical cost can be cut down because cryotherapy is a safe and
economical practice. Also, the length of stay and complication development will
be reduced. So, the medical cost can further be saved.
3.4.3 Risks of Maintaining Current Practices
If the current practice is still maintained, the consumption of other means of
pain control such as PCA, oral or injected painkillers might be increased.
Consequently, the side effects of drugs and their risks will be increased and the
rehabilitation will be affected. The less rehabilitation, the more length of stay and
complication developed. Finally, the medical cost and workload of staff will be
increased and the patients’ quality of life will be diminished.
3.4.4 Costs for Implementation of New Protocol
3.4.4.1 Material Costs
As discussed, nearly all the necessary equipments such as cryocuff with
temperature control, knee cuff, ice maker, plastic bags, tape water and electricity

Chapter 3: Implementation Potential
35
as well as evaluation measuring tools such as pain score assessment tools and
measuring tools except goniometer, the knee circumferences and ROM record
charts are available in ward . Therefore, not much extra time and budget are
needed to implement the innovation.
3.4.4.2 Non-material Costs
Besides, manpower is another cost that has to be considered. All nurses in
the proposed settings are responsible for running the programme. Although the
cryocuff is applied in the operation theatre by surgeons, the nurses still have to
assess the patients for tolerableness of cryotherapy and complication development
as well as check the proper operation of the cryocuff and re-chill the cryocuff to
maintain the temperature regularly. The nurses should spend extra time on
implementing the new protocol. However, the nurses need to examine patient
regularly in their daily work. So, the staff can make use of these times to look
over the pain intensity, signs of complication, tolerableness of cryotherapy of the
patients and maintain the function and temperature of the machine as well as
record the pain intensity, knee circumference and ROM.
3.4.5 Costs for Maintaining Current Practice
The most common used painkillers in the proposed settings are PCA
(morphine), oral (Panadol, Tramodol and NSAIDs) or injected (Tramadol and

Chapter 3: Implementation Potential
36
Pethidine) painkiller. These painkillers have not only more serious side effects,
but also more expensive. According to Department of Pharmacy, TKOH (July
2011), the cost of morphine is $3.9 per 1ml per ampule. Most of the patient use
PCA for about three to four days postoperatively. The mean of oral painkiller is
around $0.19 per tablet and the mean of injected painkiller is about $2.69 per
ampule. Most of the patients use the oral or injected painkiller during their length
of stay. All the medications are consumable (~HK$ 50/each patient/each
hospitalization); however, most of the equipments for cryotherapy can be reused.
The studies also revealed that using cryotherapy can reduce the consumption of
painkiller (Holmström & Härdin, 2005; Kullenberg, et al., 2006; Morsi, 2002).
Thus, cryotherapy is a good way to reduce pain sensation and medical cost.
3.5 Conclusion
Overall, the anticipated benefits of using cryotherapy for patients after TKR
are outweighed its potential cost and risk. In addition, the innovation can be
transferable and feasible to the target settings and audiences. Thus, it is
worthwhile to develop a new evidence-based protocol.

Chapter 4: Evidence Based Practice Protocol
37
CHAPTER 4
EVIDENCE BASED PRACTICE PROTOCOL
Based on Melnyk & Fineout-Overholt (2005), the next step of Iowa Model
is to develop an evidence-based protocol about cryotherapy.
4.1 Background
As stated before, postoperative pain and local swelling are the great barriers
that inhibit patients’ recovery and resulting in lowering the motivation of the
training adherence and affecting the postoperative rehabilitation. Consequently,
their quality of life will be influenced. Nurses play an important role in restoring
the patients’ health and alleviating their suffering. On account of this, nurses have to
develop up-to-date evidence-based practices to improve the qualities of nursing cares.
4.2 Name of the Protocol
Evidence-based guidelines of using cryotherapy in reducing pain, knee swelling
and improving range of motion for patients after total knee replacement.
4.3 Objectives of the Protocol
To reduce postoperative pain and knee swelling for patients after TKR with
the use of cryotherapy
To optimize the pain management through a safe and cost-effective practice
Chapter 4: Evidence Based Practice Protocol
38
4.4 Target Population of the Protocol
The target population of the protocol are:
all the patients who have undergone TKR in the target wards
except those who have contraindication to cryotherapy
circulatory insufficiency (e.g. peripheral vascular disease)
cold allergy (e.g. cold urticaria)
cutaneous sensory abnormalities
cryoglobulinemia
Raynaud’s phenomenon
haemoglobinopathy
advanced diabetes
cognitive intact to follow the instructions
willing to apply the cryotherapy at the postoperative stages
4.5 Rating System for the Recommendations
According to the designated levels of evidence of the reviews in Appendix
6, the grades of each recommendation is assigned by “SIGN 50: A Guideline
Developer's Handbook - Annex B: Key to Evidence Statements and Grades of
Recommendations” from Scottish Intercollegiate Guidelines Network (2008) (see
Appendix 4).

Chapter 4: Evidence Based Practice Protocol
39
4.6 Practice Recommendations
The recommended practice will be divided into five stages: preoperative
stage, intra-operative stage, early postoperative stage, middle postoperative stage
and late postoperative stage. A brief flow chart of the recommendations is shown
in Appendix 8.
1. Preoperative Stage:
Recommendation 1.1
Use cryocuff as a mean to provide continuous compression cryotherapy
Supporting evidences:
Cryocuff was a device with an inflated cuff that consisted of cold
and compression effects at the same time. (Holmström & Härdin,
2005; Kullenberg, et al., 2006) (1+; 1+)
Continuous compression cryotherapy by cryocuff could reduce
the use of analgesics and postoperative swelling as well as
improved ROM for patients with TKR significantly. (Holmström
& Härdin, 2005; Kullenberg, et al., 2006; Radkowski, et al., 2007)
(1+; 1+; 1++)

Chapter 4: Evidence Based Practice Protocol
40
2. Intra-operative Stage:
Recommendation 2.1
Apply the cryocuff immediately on the affected knee after skin closure and
before releasing of the tourniquet
Supporting evidences:
Applying the cryocuff instantly after surgery could reduce the
blood flow and resulting in decreasing the local inflammatory
response and oedema formation.
The immediately anaesthetic effect of local cooling is produced
by the slowing or elimination of pain signal transmission as well
as inhibits the stretch reflex and reduces muscle spasm.
(Holmström & Härdin, 2005; Kullenberg, et al., 2006; Morsi,
2002) (1+; 1+; 1-)
Recommendation 2.2
Place the cryocuff on a light dressing wound
Supporting evidences:
The decrease the thickness of the dressing, the increase the
contact of cryocuff and the skin. As a result, the skin surface
temperature would be reduced and the cryotherapy effect of the

Chapter 4: Evidence Based Practice Protocol
41
affected site could be maintained. (Gibbons, et al., 2001; Morsi,
2002; Radkowski, et al., 2007; Woolf, et al., 2008) (1+; 1-; 1++;
1+)
Recommendation 2.3
Place the cryocuff on the anterior part of knee as well as leave patella and
popliteal space free of pressure
Supporting evidences:
Place the cryocuff directly on the anterior part of knee could
increase the effectiveness of cryotherapy for limiting pain and
swelling. (Holmström & Härdin, 2005; Kullenberg, et al., 2006;
Smith, et al., 2002) (1+; 1+; 1+)
Leaves patella and popliteal space free of pressure to prevent
complication, e.g. pressure sore or nerve function damage due to
ischemic. (Kullenberg, et al., 2006) (1+)

Chapter 4: Evidence Based Practice Protocol
42
3. Early Postoperative Stage:
Recommendation 3.1
Keep the cryocuff continuously on affected knee at least 48 hours after
operation
Supporting evidences:
Different studies suggested different suitable length of applying
continuous compression cryotherapy from one to six days
postoperatively. (Gibbons, et al., 2001; Holmström & Härdin,
2005; Kullenberg, et al., 2006; Morsi, 2002; Smith, et al., 2002;
Woolf, et al., 2008) (1+; 1+; 1+; 1-; 1+; 1+)
Continuous cryotherapy had better pain control, especially during
night time, on the second postoperative day. (Woolf, et al., 2008)
(1+)
Recommendation 3.2
Keep the temperature of cryocuff at 7°C to 15°C
Supporting evidences:
The cryotherapy with temperature from 10°C to 15°C had
significant reduced in using pharmacological method for pain
control. (Holmström & Härdin, 2005) (1+)

Chapter 4: Evidence Based Practice Protocol
43
The cryotherapy with temperature from 7°C to 12°C had
significant advantages on pain control and ROM. (Morsi, 2002)
(1-)
Recommendation 3.3
Re-chill the cryocuff regularly to maintain the cryotherapy
Supporting evidences:
Change the ice water in cryocuff when it is melted to keep its
function. (Gibbons, et al., 2001; Holmström & Härdin, 2005;
Kullenberg, et al., 2006; Morsi, 2002; Radkowski, et al., 2007;
Smith, et al., 2002; Woolf, et al., 2008) (1+; 1+; 1+; 1-; 1++; 1+;
1+)
Change the ice every 4 hours (Kullenberg, et al., 2006) (1+)
Recommendation 3.4
Regular assessment to evaluate the effectiveness of cryotherapy in pain relief
Supporting evidences:
The effectiveness of cryotherapy in reducing pain sensation and
should be assessed to optimize the pain management in order to
promote the rehabilitation and improve the quality of life.
(Kullenberg, et al., 2006; Morsi, 2002; Woolf, et al., 2008) (1+; 1-;

Chapter 4: Evidence Based Practice Protocol
44
1+)
Recommendation 3.5
Regular assessment to prevent the undesired complications
Supporting evidences:
Cold related complication, e.g. frostbite (thermal skin injury),
transient nerve palsy, wound dehiscence and deep vein thrombosis,
should be observed to prevent extra pain or discomfort and
decrease the quality of life. (Gibbons, et al., 2001; Kullenberg, et
al., 2006; Morsi, 2002; Radkowski, et al., 2007; Smith, et al., 2002;
Woolf, et al., 2008) (1+; 1+; 1-; 1++; 1+; 1+)
4. Middle Postoperative Stage:
Recommendation 4.1
Disconnect the cryocuff system with the cuff remained on the affected knee
during mobilization
Supporting evidences:
To unplug the system and keep the cuff remained on to provide
continuous compression cryotherapy during mobilization.
(Holmström & Härdin, 2005) (1+)

Chapter 4: Evidence Based Practice Protocol
45
5. Late Postoperative Stage:
Recommendation 5.1
Apply intermitted ice pack regimen on affected knee three to six times daily
and for 15 to 20 minutes in each time after removal of cryocuff in the
remaining length of stay
Supporting evidences:
Cryotherapy by cryocuff has less nighttimes’ pain on the
postoperative day 2 compared with intermitted ice bag therapy.
Otherwise, there is no significance difference in pain control
between continuous cryotherapy and intermitted ice bag therapy
in the following time. Thus, intermitted ice pack regimen would
spend less labour intensive to manage and have less complication.
(Smith, et al., 2002; Woolf, et al., 2008) (1+; 1+)
4.7 Conclusion
Since the proposed protocol is developed with reference to the relevant, up
to date and high qualified research studies, it is believed that the evidence-based
recommendations in the new protocol can effectively reduce the postoperative
pain and local swelling for patients after TKR as well as ameliorate their quality
of life in order to maximize their benefits.

Chapter 5: Implementation Plan
46
CHAPTER 5
IMPLEMENTATION PLAN
After developing the new protocol, the next step is to establish the
implementation plan. A pilot study is necessary to test its feasibility and
transferability before a larger-scale implementation. To ensure the protocol to be
carried out smoothly and efficiently, a good communication plan is required in
advance (Melnyk & Fineout-Overholt, 2005). In this chapter, a communication
plan and a pilot study will be discussed to develop the implementation plan.
5.1 Communication Plan
Gaining approval and support from the stakeholders is the key essential
factors to the success of the new implementation plan. Therefore, a well-planned
communication plan is important at the beginning.
5.1.1 Identifying Stakeholders
Before developing the communication plan, the stakeholders of the protocol
that will be affected by the innovation should be identified. They are:
1. Decision makers, such as the Chief of Service (COS), Departmental
Operational Manager (DOM), Ward Manager (WM), Nursing Officers
(NOs) and Advanced Practice Nurses (APNs).
2. Project team including one APN (for support) and three registered

Chapter 5: Implementation Plan
47
nurses (one is the coordinator)
3. Nurses in the target wards
4. Orthopaedic doctors
5. Allied health professionals, such as physiotherapists and occupational
therapists
5.1.2 Communication Plan with Stakeholders
According to the Iowa Model, the organization support from the top to the
bottom is important for implementing and sustaining the innovation (Melnyk &
Fineout-Overholt, 2005; Polit & Beck, 2008). It is because the managerial support
is a key factor in promoting the change. Thus, the communicating sequences
should be in the order of 1 to 5 presented as above.
5.1.2.1 Communication with Decision Makers
The decision makers play an important role in starting the innovation.
Therefore, gaining their approval and support is the best begun. Firstly, the
coordinator of the project team will be responsible for communicating with the
ward manager, nursing officers and advance practice nurses. The increasing
operation rate of TKR as well as the needs and advantages of introducing the new
practice are presented to them with relevant research findings, critique and
synthesis that discussed in Chapter 1 and 2 before. Besides, the implementation

Chapter 5: Implementation Plan
48
potential such as feasibility, transferability and cost-benefits in Chapter 3 will be
showed to persuade their support. Eventually, they approved the innovation and
agreed to discuss it in the senior staff meeting.
The next step is to communicate with the Chief of Service and
Departmental Operational Manager. A PowerPoint will be prepared for the senior
staff meeting. The PowerPoint are the summary of the dissertation which focus on
the evidence-based findings from the researches, advantages of the innovation,
implementation potential and plan, the budget, time plan (see Appendix 9) as well
as the evaluation plan. Finally, they approve the evidence-based practice and
agree to implement it into the target setting.
5.1.2.2 Communication with Project Team
A project team will be established after the protocol developed. There will
be an advance nurse practice (for support) and three registered nurses (one is the
project coordinator) in the team. The major duties of them are to communicate
with and educate other stakeholders. In addition, they have to monitor the
implement and evaluate the protocol. In view of these, they should understand the
program thoroughly and be well-prepared in advance.
According to Melnyk & Fineout-Overholt (2005), a well preparation is a
key factor to start and sustain a new innovation. Therefore, two training

Chapter 5: Implementation Plan
49
workshops are needed for the project team members before implementing new
protocol. The aims of the workshops are to:
1. discuss the purpose and importance of cryotherapy for patients after
TKR
2. present the protocol contents
3. clarify their roles and responsibilities
4. train the communication, education and troubleshooting skills
5. introduce the implementation and evaluation skills with charts, audit
tool and feedback collection.
Official release to attend the training workshop will be approved by ward
managers, so as to ensure that all members can join the workshops.
1st workshop. It lasts about two hours to introduce the importance of
implementing the new protocol with the support of evidence findings. The
cryotherapy programme and protocol will be presented. Face-to-face
communication is preferred to encourage discussion and question. For further
references, a package will be distributed to all project team members to ensure
they understand the program thoroughly before implementation. The package
includes the summary of:
evidence findings of TKR and its complications

Chapter 5: Implementation Plan
50
advantages of cryotherapy
pilot study
target populations
role and responsibilities of the team members
2nd workshop. This workshop will provide the details of implementation
and evaluation of the protocol. It will last about two to three hours and use
PowerPoint as the main media in this workshop. Feedback, discussion and
question can be raised in-between the presentation. For reinforcement, a package
of the protocol with implementation guide, assessment tools, evaluation tools and
the use of goniometer and cryocuff will be provided to all members. The package
was composed of:
summary of the protocol
time plan of the implementation and evaluation (see Appendix 9)
flow chart of the protocol (see Appendix 8)
measurement, assessment and evaluation tools (see Appendix 10, 11
and 12)
use of goniometer and cryocuff
data collection and analysis methods

Chapter 5: Implementation Plan
51
5.1.2.3 Communication with Nurses in the Target Wards
The compliance and acceptance by the nurses are important factors in the
success of implementation of the protocol. However, most people are reluctant to
change the usual practice and adapt a new protocol, except, it benefit themselves
and other people. Moreover, insufficient awareness and understandings are
another resistance for the implementation. Hence, advantages of implementation
new innovation, such as reduce length of stay and the workload after complication
developed, clarification of misunderstand and uncertainties of the protocol should
be explained to the staff before implementation in order to enhance their
acceptances and interests. In view of this, poster and board as well as briefing and
training can be utilised.
Poster and board. Raising awareness of nurses with evidence-based
findings can promote their change. So, the summary of background, affirming
needs and significance of the evidence-based protocol will be displayed on the
posters and boards to enhance their awareness and interest.
Briefing and training. Six to eight sessions will be required to introduce the
new protocol, measurement tools, assessment tools, evaluation tools,
documentation charting, their roles in protocol explanation to patients, data
collection for evaluation and proper operation procedure of cryocuff. Each session

Chapter 5: Implementation Plan
52
will last for about one to two hours including explanation, question and answer
time.
5.1.2.4 Communication with Orthopaedic Doctors
The cooperation from orthopaedic doctors is also important as they are
responsible for applying the cryocuff immediately after the surgery as well as
prescribing the post operative medication and treatments for patients. The project
team will explain the details of the protocol, including its importance and
significances, advantages of innovation, their roles and implementation strategies
to the orthopaedic doctors in their weekly meeting. In the presentation, there will
be a question and answer session to explain and clarify their concerns in order to
invite their participance as well as enhance their acceptances and cooperations.
5.1.2.5 Communication with Allied Health Professionals
The allied health professionals such as physiotherapists and occupation
therapists are another leading factor to the success of the protocol implementation.
They play important roles in rehabilitation of patient after surgery. Therefore, the
cooperation of them is another hint to increase the compliance of the protocol of
patients. The project team will explain the details of the protocol, its importance
and significances, advantages of innovation, their roles and implementation
strategies to the allied health professionals in their weekly meeting as well. In the

Chapter 5: Implementation Plan
53
meeting, there will be a question and answer session to explain and clarify their
concerns in order to invite their participance as well as enhance their acceptances
and cooperations.
5.2 Pilot Testing
After communication with the stakeholders, based on Polit & Beck (2008),
the next step is to carry out a pilot study. Pilot test is a trial run design and small
scale preliminary study conducted to test the feasibility and transferability of the
protocol. A pilot study is to test the logistics and gather data before a larger-scale
implementation to improve the latter’s quality and efficiency.
5.2.1 Objectives
The objectives of the pilot study are to:
1. test the feasibility and transferability of the protocol
2. assess nurses competency in using the new protocol as well as
measurement, assessment and evaluation tools
3. assess the patients acceptance towards the new developed protocol
4. identify unpredictable problems and barriers of the study and improve
the larger-scale implementation.
5.2.2 Target Setting and Target Population
The target setting and target population of the pilot study are the same as

Chapter 5: Implementation Plan
54
the proposed setting and audiences which described in Chapter 3.1.
5.2.3 Sampling Plan
There are two orthopaedic wards in the target hospital: one is male ward
and another is female ward. Also, three to four suitable cases can recruit weekly in
a ward. As a result, about 30 candidates can be enlisted in four weeks.
5.2.4 Implementation
At the beginning, nurses will explain the content of the protocol thoroughly
to the target patients during admission. After that, the patients will start the
cryotherapy immediately since operation performed according to the new
developed guideline. Postoperative pain sensation will be documented in pain
management record chart (see Appendix 10) at least twice per day. The knee
circumference and range of motion will recorded in knee circumference record
chart and range of motion record chart respectively (see Appendix 11 and 12)
everyday. In between, verbal or written feedbacks and comments from staff and
patients will be collected to monitor the feasibility and transferability of the new
developed guideline. Regular assessment is necessary to measure the staff
competency in using the protocol as well. Finally, a special chop will be stamped
on the last page of clinical management sheet with the content of:

Chapter 5: Implementation Plan
55
This patient has *continued / discontinued to follow the cryotherapy
protocol during hospitalization.
*delete as appropriate
to measure the patients’ acceptance towards the guideline before discharge.
5.2.5 Outcomes to be Measured
The outcomes of the pilot study that should be measured are as followed:
feasibility and transferability of the protocol
nursing competency in using the protocol as well as measurement,
assessment and evaluation tools
patients acceptance towards the new protocol
5.2.6 Data Collection and Analysis
The pilot test will be analysed in terms of outcomes that showed as above.
For the feasibility and transferability of the protocol, feedback from the
stakeholders including nurses, patients, doctors and allied health professionals as
well as the unpredictable problems and barriers which encountered during the test
will be collected for evaluation. For monitoring the nursing competency in using
the protocol and documentation tools, the records will be reviewed to check if the
documents are charted correctly as well as verbal feedback and written evaluation
form from staff will be gathered. Lastly, the continuity of using cryotherapy will

Chapter 5: Implementation Plan
56
be assessed before discharge to check the patients’ acceptance towards the new
developed protocol.
5.2.7 Conclusion
The pilot test is a preliminary study which is essential before
implementation of the new developed protocol. If it shows that the protocol is
feasible and transferable, the confidence of full implementation will be greatly
enhanced. On the other hand, if there are barriers or problems in the pilot study
implementation, amendment and modification may be needed to considerate.
Except this, the support from the decision makers is important for carrying out the
protocol. Hence, a written report should be prepared for the managerial level in
senior staff meeting to report the progress and results of implementation.

Chapter 6: Evaluation Plan
57
CHAPTER 6
EVALUATION PLAN
When the pilot study results support the full implementation of the
cryotherapy protocol, it is time to develop an evaluation plan systematically. In
this chapter, a comprehensive evaluation plan will be presented.
6.1 Outcome to be Achieved
The first step of developing an evaluation plan is to determine which
outcomes should be achieved. The outcomes could be divided into two parts: (1)
Primary outcomes and (2) Secondary outcomes. In this protocol, the primary
outcome is the patients’ outcomes including the postoperative pain sensation, knee
circumference and ROM. The secondary outcomes are the patients’ acceptance,
nurses’ competency in using the protocol and documentation tools as well as
system outcome.
6.1.1 Primary Outcomes
As presented, the main objectives of the protocol are to reduce the
postoperative pain, knee swelling and improve ROM of knee for patients after
TKR. Therefore, the intensity of pain, knee circumferences and its ROM are the
primary outcomes to be measured for determining the effectiveness of the
protocol.

Chapter 6: Evaluation Plan
58
The intensity of pain will be measured by Pain Management Record Chart
which is designed by the target hospital (see Appendix 10). About four studies
described the use of Visual Analogue Scale (VAS) as pain assessment tools in their
researches (Holmström & Härdin, 2005; Kullenberg, et al., 2006; Morsi, 2002;
Woolf, et al., 2008). The Numerical Rating Scale (NRS) and Faces Pain Scale
Revised (FPS-R) that used in the target settings are similar to the the VAS used in
the studies. Both NRS and VAS use rating scale to represent the pain. They use a
horizontal line with 0 to 10 marked from left to right equally and respectively. 0
indicate as no pain and 10 indicate as the worst possible pain. The main
differences are the patients rate their pain on a scale by number from 0 to 10
verbally on NRS, while the patients mark a point on the line to measure their pain
visually on VAS. For FPS-R, it will be used for patients who are unable to use
NRS. It also similar to VAS to rate their pain from no pain on the left-most face to
the worst pain on the right-most face visually and then score the chosen face from
0 to 10. Therefore, it is feasible to use the Pain Management Record Chart as a
pain measurement tool in the proposed setting.
For knee swellling, knee grith will be measured in both intervention group
and control group to evaluate the outcome. The circumfernce in mm at mid-patella
with the knee in maximum extension will be recorded on the Knee

Chapter 6: Evaluation Plan
59
Circumferences Record Chart (see Appendix 11) at the same time in everyday to
minimize the bias. 50% of the studies that mentioned about knee swelling used
this methods to evaluate their outcomes (Holmström & Härdin, 2005) as well.
Thus, it is a workable measurement to evaluate the outcome of knee swelling in
the target wards.
Only one study mentioned the measurement method of ROM in details
(Holmström & Härdin, 2005), whereas others studies just presented with
measuring time or measurement tools briefly (Kullenberg, et al., 2006; Morsi,
2002; Radkowski et al., 2007; Smith, et al., 2002). Holmström & Härdin (2005)
suggested to measure at a standard reference points on sitting position with a
goniometer and recorded as maximum active and passive extension and flexion.
The results can record in the self-developed record chart (see Appendix 12). This
method is transferable to the target settings for measuring the ROM of knee.
6.1.2 Secondary Outcomes
Patients’ acceptance, nurses’ competency in using the protocol and
documentation tools as well as system outcomes are the secondary outcomes to be
achieved.
Patients’ acceptance towards the protocol is important for implementation.
Although cryotherapy is a safe practice in reducing pain and swelling, there is still

Chapter 6: Evaluation Plan
60
risk of complication developed. Holmström & Härdin (2005) reported one patient
requested to take off the cryocuff during implementing the cryotherapy and one
patient had cold sensation but able to continue the treatment. Kullenberg, et al.
(2006) showed one patient developed deep vein thrombosis and one patient had
superficial infection of unknown reason in the cryotherapy group. In view of this,
nurses should explain the content of the protocol thoroughly to the target patients
before. Also, a special chop will be stamped on the last page of clinical
management sheet with the content of:
This patient has *continued / discontinued to follow the cryotherapy
protocol during hospitalization.
*delete as appropriate
to monitor their acceptances towards the new developed guideline.
Moreover, good documentation will enhance the data collection and
analysis in order to facilitate the evaluation process. Therefore, the documentation
records will be reviewed regularly. Verbal feedback and written evaluation form
will be gathered to synthesize the comment.
Material and non-material costs used in the implementation period will be
recorded for evaluation. The material costs include the paperwork and
documentary equipment, e.g. document charts and chops; cryotherapy items, e.g.

Chapter 6: Evaluation Plan
61
cryocuff with temperature control, ice maker, tap water, plastic bags, electricity,
etc; medication costs; measuring items, e.g. goniometer and measuring tape; as
well as the non-material costs involve the staff cost per hour that spent on training;
cost for complication development and prolonged length of stay.
6.2 Nature and Number of Clients
The second step is to determine the nature and number of clients to be
involved in the evaluation plan.
6.2.1 The Nature of the Clients to be Involved
The nature of the clients can be referred to the target audiences mentioned
in Chapter 3.1.2, that is all patients who have undergone TKR in two orthopaedic
wards in a public hospital from Hospital Authority, except: (1) those who have
contraindication to cold therapy, (2) cognitive not intact to follow instructions and
(3) patient who are reluctant to apply the cryotherapy at the postoperative stages.
6.2.2 The Number of the Clients to be Involved
Before determining the number of the clients to be involved, the main
outcomes and the evaluation objectives of the guideline should be identified. The
main outcome is to reduce the postoperative pain, knee swelling and improve the
ROM for patients after TKR. The evaluation purpose is to determine the effective
of the guideline in reducing the pain and swelling by comparing with the

Chapter 6: Evaluation Plan
62
intervention group and control group. Hence, two-sample t-test should be used as
the method of analysis.
The sample size will be obtained by the web software which developed by
Lenth (2006-9). Four main components should be calculated or adjusted before
estimating the sample size: (1) standard deviation, (2) power, (3) true difference of
means and (4) ρ-value. The data for sample size calculation can be adapted from
the seven relevant studies (Gibbons, et al., 2001; Holmström & Härdin, 2005;
Kullenberg, et al., 2006; Morsi, 2002; Radkowski et al., 2007; Smith, et al., 2002;
Woolf, et al., 2008).
According to those studies, for the postoperative pain, the standard
deviation is 1.32 in the intervention group whereas 1.6 in the control group. The
true average difference of means that computed is 0.82. The power will be set to
0.8 as that is the customary standard for power. Based on Pilot and Beck (2008),
there is 20% risk of committing Type II error if the power to be fixed as 0.8. The
ρ-value will be set as 0.05 to have a significance result. Hence, the sample size of
51 candidates in each group is figured out. With the application of attrition rate
about 10%, 64 patients are needed in each group.
There are only two studies had discussed about the result of knee swelling
(Holmström & Härdin, 2005; Smith, et al., 2002). So, the data will be generated

Chapter 6: Evaluation Plan
63
from them. The standard deviation is 16 mm in the intervention group and 20 mm
in the control group. The true average difference is 8.5 mm. The power will be set
to 0.8 and ρ-value is 0.05. As a result, 72 cases are estimated for each group.
Counting with about 10% attrition rate, 80 patients are required in each group.
For calculating the sample size in ROM, four studies are involved
(Holmström & Härdin, 2005; Kullenberg, et al., 2006; Morsi, 2002; Smith, et al.,
2002). The standard deviation will be set to 13.95° in intervention group and
12.91° in control group. The true average difference is 8.42°. The power will be
equal to 0.8 and ρ-value is 0.05. By Lenth (2006-9), a sample size of 41 per group
is estimated. Due to about 10% attrition rate, 45 cases are necessary in each
group.
To conclude, about 80 patients are required for both intervention group and
control group in the evaluation plan. Since there are about three to four cases
admitted for scheduled TKR each week in each ward, at least 20 weeks are needed
to recruit enough candidates and 22 weeks for data collection.
6.3 Time and Frequency of Taking Measurements
The next step is to determine when and how often to take the measurement
of the primary and secondary outcomes.

Chapter 6: Evaluation Plan
64
6.3.1 Primary Outcomes
The aims of the new protocol are to reduce the postoperative pain, knee
swelling and increase the ROM. Thus, the measurements should be taken after
operation. The intensity of pain will be measured at least twice daily which set by
the pain assessment protocol in the target hospital. The frequency of assessment
can be increased if patients’ pain intensity is aggravated. Besides, the pain
assessment should be done after intervention implemented in order to evaluate the
effectiveness of the interventions. For the knee swelling, bilateral knee girths will
be recorded at the same time every day until discharge in order to minimize the
bias. Because of the ward practice, it is be usually measured around seven o’clock
every morning by nurses. Nurses are required to check the ROM of knee at the
same time every day as well in virtue of keeping consistence. To be convenience,
it will be measured with knee swelling measurement.
6.3.2 Secondary Outcomes
The patient’s acceptance towards the new guideline can be measured before
discharge. The cryotherapy team members can calculate the number of people
who accept using cryotherapy after the surgery for evaluating the acceptance rate
of the protocol. For nurses’ competency in using the guideline and documentation
tools, verbal feedback and comments will be collected at any time after
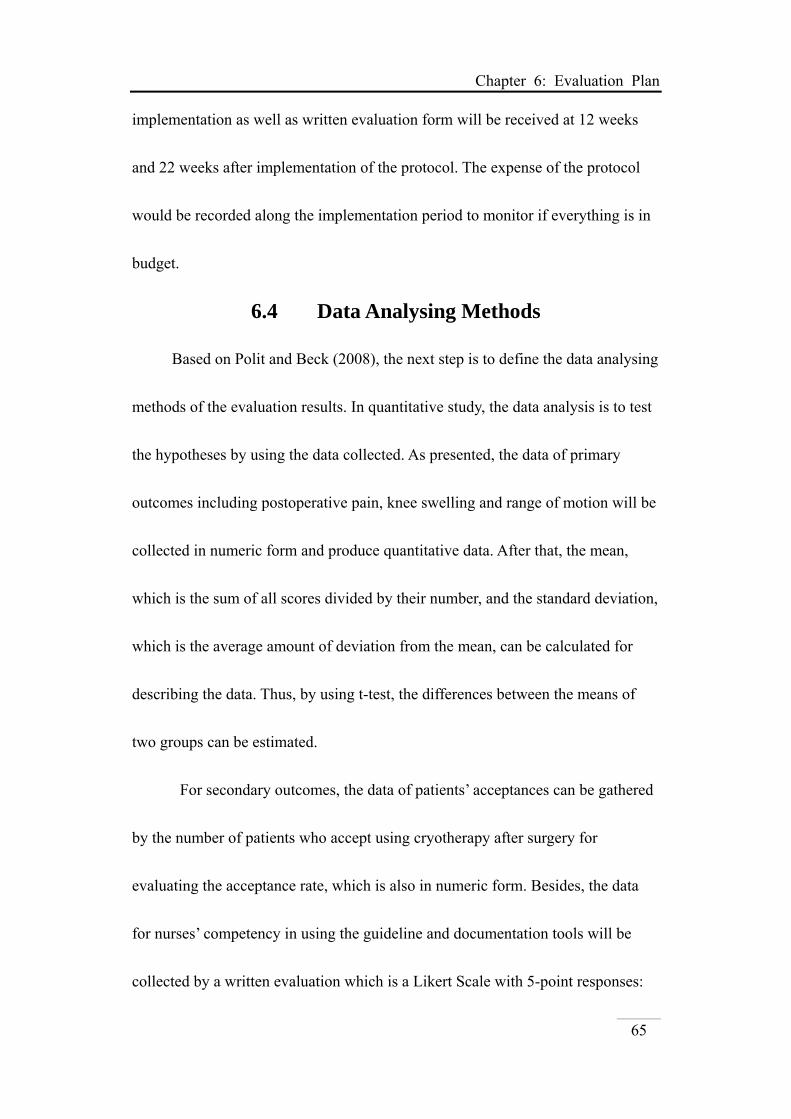
Chapter 6: Evaluation Plan
65
implementation as well as written evaluation form will be received at 12 weeks
and 22 weeks after implementation of the protocol. The expense of the protocol
would be recorded along the implementation period to monitor if everything is in
budget.
6.4 Data Analysing Methods
Based on Polit and Beck (2008), the next step is to define the data analysing
methods of the evaluation results. In quantitative study, the data analysis is to test
the hypotheses by using the data collected. As presented, the data of primary
outcomes including postoperative pain, knee swelling and range of motion will be
collected in numeric form and produce quantitative data. After that, the mean,
which is the sum of all scores divided by their number, and the standard deviation,
which is the average amount of deviation from the mean, can be calculated for
describing the data. Thus, by using t-test, the differences between the means of
two groups can be estimated.
For secondary outcomes, the data of patients’ acceptances can be gathered
by the number of patients who accept using cryotherapy after surgery for
evaluating the acceptance rate, which is also in numeric form. Besides, the data
for nurses’ competency in using the guideline and documentation tools will be
collected by a written evaluation which is a Likert Scale with 5-point responses:

Chapter 6: Evaluation Plan
66
(1) strongly agree, (2) agree, (3) neutral, (4) disagree and (5) strongly disagree.
Each response will have a numerical value for data analysis. Therefore, they can
be interpreted by using t-test as well. Finally, to analyse the cost-effectiveness,
comparison between the material and non-material costs used in implementing the
new protocol as well as the cost of continuing current practice such as the
medication expense, treatment cost after complication developed and cost of
prolonged length of stay will be performed for evaluation. The net balance can
reveal the advantages of implementing the new protocol.
6.5 Effectiveness of the Protocol
The last step is to evaluate the effectiveness of the protocol. Since the main
objectives of the guideline are to reduce the postoperative pain, knee swelling and
improve ROM for patients after TKR, the primary outcomes have the first priority
to determine the effectiveness of the protocol. However, the patients’ acceptances
towards the protocol and the nurses’ competency in using the protocol will affect
the results of evaluation. So, the secondary outcomes are also important. In view
of this, the new protocol will be considered as effective if the results can achieve
the following bases:
1. For postoperative pain, as the average mean difference among the literatures
is about 0.82 (Gibbons, et al., 2001; Holmström & Härdin, 2005; Kullenberg,

Chapter 6: Evaluation Plan
67
et al., 2006; Morsi, 2002; Radkowski et al., 2007; Smith, et al., 2002; Woolf,
et al., 2008), it can be considered as effective if the mean differences of pain
score reduce at least 1 which compared with the control group.
2. For knee swelling, only two studies are presented about these results
(Holmström & Härdin, 2005; Smith, et al., 2002). The true average
difference of the knee girth is about 8.5mm. Therefore, the new guideline
will be effective in reducing knee swelling if the knee circumferences can
reduce at least 10 mm which compared with that of control group.
3. For the ROM of knee, the true average difference among the four studies is
8.42° (Holmström & Härdin, 2005; Kullenberg, et al., 2006; Morsi, 2002;
Smith, et al., 2002). Hence, the protocol will be reflected as effective if ROM
in intervention group larger 10° than that in control group.
4. For patients’ acceptance, by observation, nearly all patients accept to use
cryocuff in other knee surgery. Therefore, for conservative estimation, it will
be effective if there are at least 80% of patients who follow the cryotherapy
guideline during hospitalization.
5. As shown, nurses play an important role in implementing the new guideline;
therefore, their competencies are also need to be considered for an effective
protocol. Accordingly, if positive feeling and feedback towards the new

Chapter 6: Evaluation Plan
68
guideline are collected as well as good documentation and regular review
performed by nurses, the protocol can be decided as effective.
6.6 Conclusion
To sum up, the effectiveness of the guideline is determined by the primary
outcomes and secondary outcomes. Thus, the guideline is effective and can be
applied to the proposed setting in a long period of time if positive outcomes are
leaded. On the other hand, if negative outcomes are generated, the guideline may
have to be amended. However, the guideline is developed from updated and high
quality studies. Therefore, it believed that it will be effective.

Chapter 7: Summary
69
CHATPER 7
SUMMARY
According to the reviewed study, cryotherapy is suggested as a safe,
economical and efficient method in managing the postoperative pain, knee
swelling and ROM for patients after TKR. However, cryotherapy is not
performed as a common practice in most places such as the proposed settings. In
this regard, a systematic, critical and evidence based guideline of the related issue
has been conducted. The relevant evidences which transferred from the reviewed
study are used to establish the protocol for patients in the proposed settings with
well-designed implementation and evaluation plan suggested. It is hoped that the
new developed guidelines is beneficial to patients after TKR in an orthopaedics
settings in order to preserve patients’ quality of life and relieve healthcares’
burdens.

Appendices
70
APPENDICES
Appendix 1: Table of Electronic Databases
Keyword(s) MEDLINE
(Ovid) (1948 – 2011)
BNI (Ovid)
(1994 – 2011)
BNIA (Ovid)
(1985 – 2011)
CINAHL Plus
(EBSCOhost)
PubMed (NCBI)
Cochrane Library (WOL)
(1) Total Knee Arthroplasty 20520 28 33 (2) Total Knee Replacement 10318 245 252 (3) Cryotherapy 6452 26 28 (4) Cold therapy 3160 7 10 (5) Pain 395920 6117 8035 (6) (1) or (2) 21012 269 280 (7) (3) or (4) 6499 32 37 (8) (5) and (6) and (7) 20 0 0 (9) (6) and (7) 2 2 (10) (1) and (3) and (5) 6
19 5
(11) (1) and (4) and (5) 4 5 (12) (2) and (3) and (5) 2
12 4
(13) (2) and (4) and (5) 4 6 (14) Limited (8) to English and publication year
from 2001 to current 10
(15) Limited (9) to publication year from 2001 to current
2 2

Appendices
71
Keyword(s) MEDLINE
(Ovid) (1948 – 2011)
BNI (Ovid)
(1994 – 2011)
BNIA (Ovid)
(1985 – 2011)
CINAHL Plus
(EBSCOhost)
PubMed (NCBI)
Cochrane Library (WOL)
(16) Limited (10) to English and publication year from 2001 to current
4
(17) Limited (11) to English and publication year from 2001 to current
2
(18) Limited (12) to English and publication year from 2001 to current
2
(19) Limited (13) to English and publication year from 2001 to current
2
(20) Limited (10) and (11) to English and published in the past ten years
10
(21) Limited (12) and (13) to English and published in the past ten years
8
Related to the topic (by a quick look on title only) 10 2 2 3 10 1 Related to the topic and belong to controlled trials (by looking at the abstract and the text)
5 1 1 1 5 0
From reference lists 1 Total number of studies 7

Appendices
72
Appendix 2: Tables of Evidences
Bibliographic Citation
Study Type
& Ev Lv.
Number of Patients
Patient Characteristics Intervention Comparison Length of
follow upOutcome Measures Effect Size
1. Gibbons, et al. (2001)
RCT 1+
Total: 60 Cryo/Cuff: 30 patients Robert Jones: 30 patients
Cryo/Cuff: - Age: 70 yrs old - Sex ratio M/F:
11/19 - Osteoarthritis: 25 - Rheumatoid
arthritis: 5 - Knee score: 37 - Function Score: 47- Mean blood loss:
720 ml - Patients
transfused: 6 Robert Jones: - Age: 71 yrs old - Sex ratio M/F:
14/16 - Osteoarthritis: 27 - Rheumatoid
arthritis: 3 - Knee score: 40 - Function Score: 39- Mean blood loss:
1200 ml - Patients
transfused: 7
Cold compression dressing: - Placed over a single
layer of crepe and Velband immediately after OT
- Layer removed by PT once back to ward
- Cryo/Cuff with inflatable cuff place on the knee and attached at the back with Velcreo straps
- Cuff filled with ice water via a tube attached to ice bucket
- Cuff with compression and cold therapy, last to 60 mins
- No CPM - Physiotherapy same
as control gp - Minimum 6 hrs
during the day until discharge
Modified Robert Jones bandage: - Firm
compression in 3 layers Velband and crepe, which remained in place for 48 hrs
- No CPM - Physiotherapy
same as intervention gp
Pre-op to 10 days after OT
Before OT: - Pain scores
by visual analogue scale (0-100)
After OT: - Amount of
morphine used via PCA for the first 48hrs
- Amount of oral analgesic used up to 10 days
- Pain Scores recorded on alt. days after physiother-apy at the end of afternoon
Range of motion: - Cryo-cuff gp: 5° – 82° - Robert Jones gp: 3° – 78° - P > 0.05 Pain scores: Cryo-cuff gp: - Pre-op: 60+ - Day 1: 60+ - Day 3: 30+ - Day 5: 40+ - Day 7: 30+ - Day 9: 20+ Robert Jones gp: - Pre-op: 70+ - Day 1: 60+ - Day 3: 40+ - Day 5: 40+ - Day 7: 40+ - Day 9: 30+ - P > 0.05 Analgesia: Cryo-cuff gp: - morphine used:
0.65 mg/kg/48hrs - Oral analgesia: 44 doses Robert Jones gp: - morphine used:
0.6 mg/kg/48hrs - Oral analgesia: 40 doses - P > 0.05 Complication: - No recorded complication
General Comment: There is no statically significant different between 2 groups in range of motion, pain scores and need for analgesic.

Appendices
73
Bibliographic Citation
Study Type& Ev Lv.
Number of Patients
Patient Characteristics Intervention Comparison
Length of
follow up
Outcome Measures Effect Size
2. Holmström & Härdin (2005)
RCT1+
Total: 60 Cryo: 23 EDA: 21 Control: 17
Cryo: - Age: 68 yrs
old - Sex ratio
M/F: 9/14 - Weight: 75 kg- VAS at rest: 1- VAS on
motion: 5 - Function
(ISK): 12 EDA: - Age: 75 yrs
old - Sex ratio
M/F: 6/15 - Weight: 77 kg- VAS at rest: 1- VAS on
motion: 5 - Function
(ISK): 15 Control: - Age: 72 yrs
old - Sex ratio
M/F: 6/11 - Weight: 77 kg- VAS at rest:
1.5 - VAS on
motion: 4 - Function
(ISK): 13
- All patients received traditional analgesics: paracetamol 500mg, dextropropoxyfene 50 and 100mg, supplementary morphine, oral 5mg and IV 5mg/ml when required
- Rehabilitation started on Day 1
Pre-op to 6 weeks after TKR
Pain: VAS (0-10) - At rest and on motion - Every 24hrs - From end of surgery to
Day 6-7 - Recorded by
physiotherapist, nurse or patient if discharged before observation time
- Consumption of injectable and oral morphine from surgery to Days 6-7 was summarized every 24 hrs
Range of motion: standard reference points on sitting position with a goniometer and recorded as max active and passive extension and flexion - Measured on pre-op,
Day 7 and Week 6 with same tools
Knee girth: circumference in mm at mid-patella with the knee in max extension - Measured on pre-op,
Day 7 and Week 6 with same tools
Pain at rest: VAS Pre D1 D2 D3 D4 D5 D6 D7 W6
1 1 3+ 2+ 1+ 1+ 1+ 1 0+ 0+ 2 1 2+ 2+ 1 1+ 1+ 1 1+ 0+ 3 1+ 3 2+ 1 2+ 2 2 2 1
Pain on motion: VAS Pre D1 D2 D3 D4 D5 D6 D7 W6
1 5 5+ 5 4 3+ 3+ 2+ 2 1+ 2 5 4 4+ 4 3+ 2+ 2+ 2+ 1+ 3 4+ 5+ 4+ 3 4 4+ 3 3+ 1+
1 = Cryo/Cuff; 2 = EDA; 3 = Control Morphine requested:
Day 1 - Cryo: 13.4mg (100%) (P=0.028) - EDA: 7.5mg (65%) (P < 0.001) - Control: 20.8mg (100%) - Different between Cryo and EDA is not significance Day 2 - Cryo: 3.9mg - EDA: 3.2mg - Control: 6.3mg - Different not significance
Total used in first 3 days: - Cryo: 18.7mg - EDA: 14.2mg - Control: 28.4mg - Different between EDA and Control was significance (P=0.005) - EDA: ↑ slightly after 48hrs - Cryo: constantly ↓ pain curve even after removal of the cryocuff and no
morphine is needed after Day 4 - Other groups continuously request until Day 7 Swelling: - No significant differences in swelling. (mild ↓ swelling by cryocuff
compared with EDA and control gp) Range of motion: - No significant difference in passive or active ROM - At 6 weeks, passive and active ROM was similar to pre-op ROM Complication: - Cryo: required to removal of the cryocuff before 48 hrs: 1 patient .felt cold but retained the cryotherapy: 1 patient - EDA: ↓ sensibility in both leg: 3 patients totally paralyzed in both leg: 1 patient anaesthetized in the other leg: 1 patient require to remove before 48 hrs: 1 patient
Cryo/Cuff: - Applied immediately after
skin closure and before release of the tourniquet.
- Cooling system with an insulated cuff strapped to the front of the knee
- Ice water temperature: 10°C – 15°C
- An automatic device with continuous chilling and pulsing compression of 30mmHg in intervals 30sec
- Treatment continuous for 48hr
- Ice water changed every 6 hrs or more often if melted
- At mobilization, system was unplugged and cuff remained on
EDA: - 2.5 to 5 mg/ml of
bupivacaine was administered into epidural space
- continuous administration for 48 hrs
General Comment:
Both Cryo/Cuff and EDA was significantly reduced in morphine used compared with the control group. No significant difference between groups was noted in subjective pain, swelling, ROM and function. Cryo/Cuff seems to be a risk-free, well-tolerated, little competence-demanding alternative to EDA in the postoperative pain management.

Appendices
74
Bibliographic Citation
Study Type & Ev Lv.
Number of Patients
Patient Characteristics Intervention Comparison Length of
follow upOutcome Measures Effect Size
3. Kullenberg, et al. (2006)
RCT1+
Total: 86 Cold compression: 45 EDA (Standard): 41
Cold compression: - Age: 68.1
yrs old - Sex ratio
M/F: 1.35/1 EDA: - Age: 68.9
yrs old - Sex ratio
M/F: 1.43/1
Cold compression: - The cryocuff
was applied after tourniquet deflated
- The cryocuff, covered the anterior part of the knee, leaves patella and popliteal space free of pressure
- For 3 days after TKR
- Rechilling every 60 mins by nursing staff for 3 days
- Ice was changed every 4 hrs
EDA (Standard): - Epidural
analgesia with ropivacain till D3
- Then, IV NSAID drugs and opioids
Pre-op to 3 weeks after TKR
Pain: Visual analogue scale - Recorded by
nurse and PT during motion
- Total consumption of analgesics in relation to patient body weight
- Analyzed by Wilcoxon signed rank test
Range of motion: - Flexion and
extension recorded by PT at D1, at discharge and 3 weeks post- operatively
- Analyzed by paired t test
1 2 Pain: (VAS) D1 2.1±1.0 2.2±0.8 D3 0.8±0.9 1.2±0.7 During exercise
3.4±1.5 2.3±1.7
Pain (mg morphine/kg/24hr)
0.37±0.11 0.43±0.05
ROM: D1 50.4±8 51.4±11.1 At discharge
75.1±10.5 62.9±12.8 (P=0.0019)
3 weeks post-op
98.9±9.4 87.6±7.8 (P=0.0045)
Completed rehab
4.3±1.1 5.6±1.2 (P=0.002)
1 = Cold compression group 2 = EDA (Standard) group Complication: Cryo: - DVT: 1 patient - Superficial soft tissue infection of
unclear origin: 1 patient - Request removal of cold compression: 1
patient EDA - DVT: 1 patient
General Comment: Combined cold compression therapy controls pain (use less analgesics), improves ROM, and may speed up the time for mobilization.
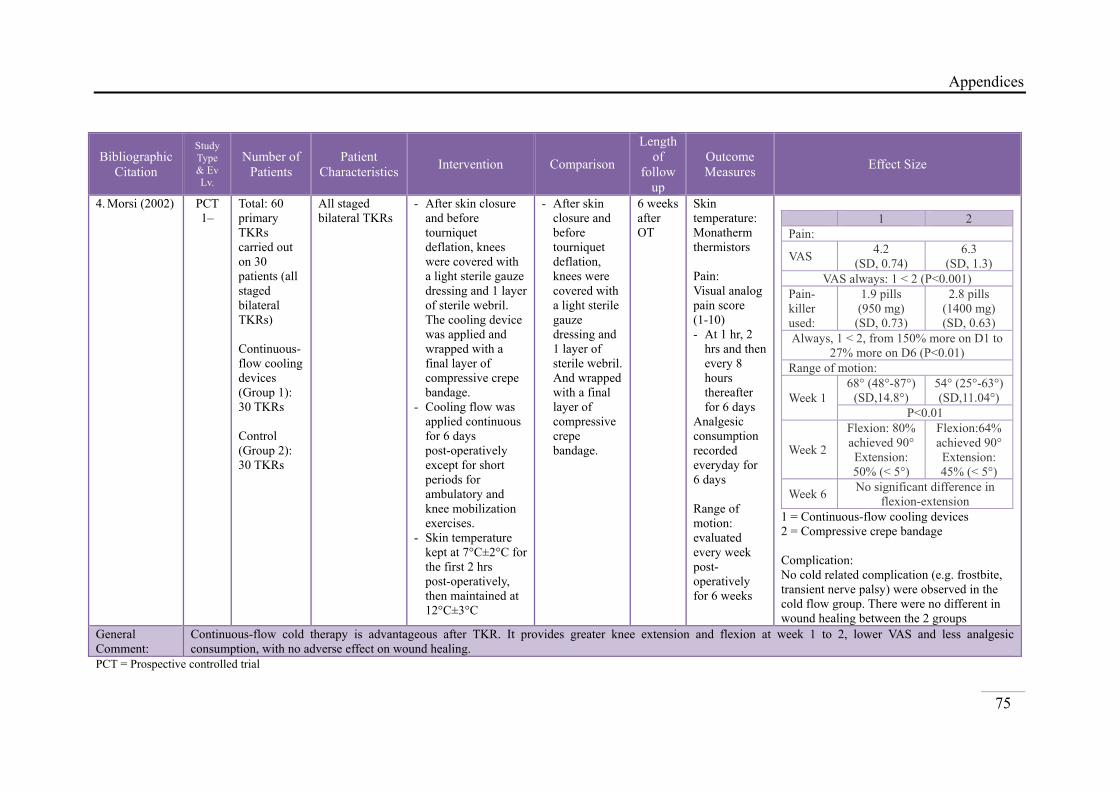
Appendices
75
Bibliographic Citation
Study Type & Ev Lv.
Number of Patients
Patient Characteristics Intervention Comparison
Length of
follow up
Outcome Measures Effect Size
4. Morsi (2002) PCT1–
Total: 60 primary TKRs carried out on 30 patients (all staged bilateral TKRs) Continuous-flow cooling devices (Group 1): 30 TKRs Control (Group 2): 30 TKRs
All staged bilateral TKRs
- After skin closure and before tourniquet deflation, knees were covered with a light sterile gauze dressing and 1 layer of sterile webril. The cooling device was applied and wrapped with a final layer of compressive crepe bandage.
- Cooling flow was applied continuous for 6 days post-operatively except for short periods for ambulatory and knee mobilization exercises.
- Skin temperature kept at 7°C±2°C for the first 2 hrs post-operatively, then maintained at 12°C±3°C
- After skin closure and before tourniquet deflation, knees were covered with a light sterile gauze dressing and 1 layer of sterile webril. And wrapped with a final layer of compressive crepe bandage.
6 weeks after OT
Skin temperature: Monatherm thermistors Pain: Visual analog pain score (1-10) - At 1 hr, 2
hrs and then every 8 hours thereafter for 6 days
Analgesic consumption recorded everyday for 6 days Range of motion: evaluated every week post- operatively for 6 weeks
1 2 Pain:
VAS 4.2 (SD, 0.74)
6.3 (SD, 1.3)
VAS always: 1 < 2 (P<0.001) Pain- killer used:
1.9 pills (950 mg)
(SD, 0.73)
2.8 pills (1400 mg) (SD, 0.63)
Always, 1 < 2, from 150% more on D1 to 27% more on D6 (P<0.01)
Range of motion:
Week 168° (48°-87°)
(SD,14.8°) 54° (25°-63°) (SD,11.04°)
P<0.01
Week 2
Flexion: 80% achieved 90°Extension: 50% (< 5°)
Flexion:64% achieved 90° Extension: 45% (< 5°)
Week 6 No significant difference in flexion-extension
1 = Continuous-flow cooling devices 2 = Compressive crepe bandage Complication: No cold related complication (e.g. frostbite, transient nerve palsy) were observed in the cold flow group. There were no different in wound healing between the 2 groups
General Comment:
Continuous-flow cold therapy is advantageous after TKR. It provides greater knee extension and flexion at week 1 to 2, lower VAS and less analgesic consumption, with no adverse effect on wound healing.
PCT = Prospective controlled trial

Appendices
76
Bibliographic Citation
Study Type & Ev Lv.
Number of
Patients Patient Characteristics Intervention Comparison
Length of follow
up
Outcome Measures Effect Size
5. Radkowski, et al. (2007)
RCT1++
Total: 64 patients 45°F group: 28 patients 75°F group: 36 patients
45°F (N=28)
p Value
Mean age (SD)
63.7 (±10.4) 0.269
BMI (SD) 32.6 (±5.5) 0.173
Female 46% 0.124Race 0.107African American 3.6%
Caucasian 89.3% Right side 36% 0.939IKDC score 33.5 0.884Range (Lin, et al.) of motion
101° 0.713
75°F
(N=36) p
ValueMean age (SD)
66.9 (±10.4) 0.269
BMI (SD) 30.7 (±5.1) 0.173
Female 64% 0.124Race 0.107African American 16.7%
Caucasian 80.6% Right side 44% 0.939IKDC score 33.8 0.884Range (Lin, et al.) of motion
103° 0.713
IKDC = International Knee Documentation Committee
All is the same except the temperature of cuff from cryotherapy device is 45°F
All is the same except the temperature of cuff from cryotherapy device is 75°F
From OT day to Day 30
Skin temperature: temperature probes placed on the skin surface (Omega Temperature Logger, Omega Engineering Inc., Stamford, CT) All patients were evaluated in the postoperative period by the same research nurse. Pain: Verbal analog scale (0-10), narcotic consumption Self-reported knee function: IKDC Passive knee ROM: using a hand goniometer by PT
Pain: VAS 45°F 75°F
D1 6.0 5.5 D3 7.1 6.3 D30 6.2 6.5
P = 0.4 No differences in the average pain score between two groups Opioid consumption
45°F 75°F p value D1 7.1% 5.6% 0.961 D3 46.4% 25% 0.111
No differences observed in the postoperative Opioid consumption between the two groups No differences in early postoperative ROM between two groups No differences in patients’ self-reported postoperative functional scores between two groups Complication: No incidences of wound dehiscence or nerve palsies.
General Comment:
With the colder 45°F cryotherapy temperature following TKR, no improvement was observed in the short-term postoperative narcotic consumption and pain scores, ROM and self-reported knee function. No adverse effects were reported with the cryotherapy treatment.

Appendices
77
Bibliographic Citation
Study Type& Ev Lv.
Number of Patients
Patient Characteristics Intervention Comparison
Length of
follow up
Outcome Measures Effect Size
6. Smith, et al. (2002)
RCT 1+
Total: 84 patients Compression Bandage Group (Woolf, et al.): 40 Cold Therapy Group (Brander & Stulberg): 44
CB: - Mean age
(SD): 72yr (7.1)
- Weight kg (SD): 78.5kg (19)
- M/F: 21/19 CT: - Mean age
(SD): 72.1yr (7.8)
- Weight kg (SD): 77.4kg (12)
- M/F: 21/23
CT: - The pressure
bandage was removed 6 hours postoperatively and cold therapy via the cryo-pad machine was initiated.
- Cryo-pad was placed directly over but not around the incision site.
- Cryo-therapy machine was set to infuse the pad with cold water between 2°C and 5°C for 15 mins and then deflated for 15 mins.
- The pad machine was removed after 24 hours of use and follow CB routine (applying ice packs three times per day for 15 mins for the next 24 – 48 hours.
CB: - The
bandage was left intact for 24 hours before its removal.
- Ice in plastic bags wrapped in a linen towel was then applied to the wound site three times per day for 15 mins for the next 24 to 48 hours.
Pain: Visual analog scale (1-10) Pain: measure analgesia use, especially opiate used. Knee flexion and swelling: by PT at approximately the same time each day.
Variable (measure) Compression Bandage Significance Mean (SD) Range P =
Swelling pre-op (mm) 410 (38) 380-540 0.294 Swelling 24 hr (mm) 439 (36) 385-522 0.837 Swelling 48 hr (mm) 445 (38) 381-505 0.512 Flexion pre-op (∞) 75.8 (15.4) 40-100 0.443 Flexion 24 hr (∞) 83.6 (12.9) 60-115 0.384 Flexion 48 hr (∞) 86.6 (12.3) 50-112 0.950 Pain D1 (1-10) 4.2 (2.0) 1-10 0.320 Pain D2 (1-10) 4.8 (1.9) 1-8 0.720 Pain D3 (1-10) 3.5 (1.9) 1-8 0.665 Opiates (mg/kg/48hrs) 0.32 (0.29) 0-0.99 0.245
Variable (measure) Cold Therapy Significance
Mean (SD) Range P = Swelling pre-op (mm) 412 (34) 365-490 0.294 Swelling 24 hr (mm) 438 (33) 373-490 0.837 Swelling 48 hr (mm) 439 (26) 393-485 0.512 Flexion pre-op (∞) 71.7 (15.8) 45-115 0.443 Flexion 24 hr (∞) 81.3 (11.8) 60-115 0.384 Flexion 48 hr (∞) 84.9 (13.4) 60-120 0.950 Pain D1 (1-10) 4.3 (1.8) 1-9 0.320 Pain D2 (1-10) 4.3 (2.0) 1-9 0.720 Pain D3 (1-10) 4.2 (1.8) 1-8 0.665 Opiates (mg/kg/48hrs) 0.422 (0.31) 0-1.01 0.245
Complication: no complication reported in this study Cost effectiveness and potential risk: CB: - Intact for 24 – 48 hrs. Cost: US$3 – 5 - Nursing activities: observing for ooze and regular circulation checks - 1 or 2 nursing hours be absorbed over 24 hours CT: - Potential risk: incidents of discomfort, blisters and occasionally
compartment syndrome - Cost: cyro machine: US$250
ice maker: US$1000 single use pads: US$25 each
- Nursing activities: equipment setup, maintenance of ice supply to the machine and removal and cleaning of the machine
- 1 and 2 hours work in addition to routine observations and care.General Comment:
No difference between the two management techniques for pain scores and swelling in the first 48 hours of the postoperative period. A cost benefit analysis showed the compression bandaging is cheaper and less labor intensive to manage than the cold therapy.

Appendices
78
Bibliographic Citation
Study Type & Ev Lv.
Number of Patients
Patient Characteristics Intervention Comparison Length of
follow up Outcome Measures Effect Size
7. Woolf, et al. (2008)
RCT1+
Total: 60 patients, 7 of them excluded → 53 patients Continuous temperature-controlled cryotherapy system (CTC): 24 patients Ice pack regimen (Ice therapy): 29 patients
- Mean patient age: 42.5 years (range: 14 – 73 years old)
- Women were significantly older (47.2 vs. 37.7 yrs old, P<0.05)
- No significant differences (P=0.77) in general personality trait.
- ↑% in CTC underwent more severe surgical procedure (38.5% vs. 26.7% in ice therapy) (P=0.35)
- Knee stability: 71.5% (Ice therapy) vs. 100% (CTC) reported instability (P=0.03)
CTC: - The sterile cooling
bladder was applied over the Webril, and a layer of sterile biascut stockinette was wrapped around the knee.
- Patients were instructed to fill cooler with ice prior to sleep and allow the device to operate through the night for the first 4 days.
- Patients then were instructed to use the device at their own discretion whenever experiencing pain during the remaining 10 days.
Ice therapy: - Apply an
ice pack plus compressive dressing to the affected knee for 20 mins every 2 hours while awake for the first 4 days
- Use the ice pack at their own discretion whenever pain was experienced at night or during the remaining 10 days of the protocol
Post-op Day 2 to Day 14
Pain: 5-point verbal analog rating scale
Pain Intensity Score (95% CI) Ice Therapy CTC
D2 2.95 (2.41-3.48) 2.64 (2.25-3.02) D5 2.15 (1.63-2.27) 2.23 (1.76-2.69) D8 1.90 (1.35-2.44) 2.20 (1.63-2.78) D11 1.46 (1.01-1.91) 1.66 (1.06-2.25) D14 1.60 (0.91-2.28) 1.15 (0.72-1.57)
Pain intensity: mild (did not awaken) - 35.7% in CTC vs. 5.9% in ice
therapy (P=0.04) - % of CTC with night pain which
disrupted their sleep < Ice therapy (significant on Day 2 only)
- No patient in either groups
developed thermal skin injury, infection, nerve palsy or deep venous thrombosis.
General Comment:
There is no difference in pain intensity for any of the follow up days. However, the percentage of patients with nighttimes’ pain that disrupted their sleep was significantly lower on the second postoperative day for the continuous cryotherapy group compared with the ice therapy group. It showed modest benefit in continuous flow, temperature-controlled cryotherapy device versus ice therapy for early nighttimes’ pain control and improved quality of life following routine outpatient knee arthroscopy procedure, with less risk of thermal injury.

Appendices
79
Appendix 3: Levels of Evidences
1++ High quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low risk of
bias
1+ Well-conducted meta-analyses, systematic reviews, or RCTs with a low risk of bias
1- Meta-analyses, systematic reviews, or RCTs with a high risk of bias
2++ High quality systematic reviews of case control or cohort or studies
High quality case control or cohort studies with a very low risk of confounding or bias and
a high probability that the relationship is causal
2+ Well-conducted case control or cohort studies with a low risk of confounding or bias and a
moderate probability that the relationship is causal
2- Case control or cohort studies with a high risk of confounding or bias and a significant risk
that the relationship is not causal
3 Non-analytic studies, e.g. case reports, case series
4 Expert opinion
Appendix 4: Grades of Recommendations
At least one meta-analysis, systematic review, or RCT rated as 1++, and directly applicable to the target population; or A body of evidence consisting principally of studies rated as 1+, directly applicable to the target population, and demonstrating overall consistency of results
A body of evidence including studies rated as 2++, directly applicable to the target population, and demonstrating overall consistency of results; orExtrapolated evidence from studies rated as 1++ or 1+
A body of evidence including studies rated as 2+, directly applicable to the target population and demonstrating overall consistency of results; or Extrapolated evidence from studies rated as 2++
Evidence level 3 or 4; or Extrapolated evidence from studies rated as 2+
Good Practices Points
Recommended best practice based on the clinical experience of the guideline development group

S 1.
SEIn
1
1
1
1
1
1
1
1
I G N M
GibbonsCryothereplacem25(4), 2
ECTION 1:n a well condu
.1 The stud
and clea
.2 The assi
treatmen
.3 An adeq
is used
.4 Subjects
‘blind’ a
.5 The trea
are simi
.6 The only
groups i
investig
.7 All relev
measure
reliable
.8 What pe
or cluste
treatmen
dropped
complet
App
Methodolog
s, C. E. R., Serapy compament: A pro50-252. : INTERNAucted RCT stu
dy addresses a
arly focused q
ignment of su
nt groups is ra
quate concealm
s and investig
about treatmen
atment and co
ilar at the start
y difference b
is the treatmen
gation
vant outcome
ed in a standar
way
ercentage of th
ers recruited i
nt arm of the s
d out before th
ted?
pendix 5: T
gy Checkli
Solan, M. Cared with Rspective ran
AL VALIDITudy…
an appropriate
question.
ubjects to
andomised
ment method
gators are kept
nt allocation
ntrol groups
t of the trial
between
nt under
s are
rd, valid and
he individuals
nto each
study
he study was
Table of Crit
ist 2: Cont
C., Ricketts,Robert Jonesndomized tr
TY This crite
e Adequ
addre
Not rep
Not add
t Not add
Well co
Well co
Well co
s Not add
tical Apprai
trolled Tri
, D. M., & Ps bandage afrial. Interna
erion is: R
uately
essed
P
in
ported T
“r
d
dressed N
m
dressed N
th
overed S
ch
st
overed U
su
gr
A
w
O
overed T
u
dressed N
isals
ials
Patterson, Mfter total kn
ational Orth
Remarks:
PICO were add
n a clear forma
The study only
randomized”,
escribed.
No detail of co
method is desc
No detail of bin
he study.
imilar patient
haracteristics
tudy.
Using the same
urgical techniq
roups.
A tourniquet an
which attached
OT was used in
The outcome m
sed are standa
No detail descr
Appendic
80
M. (2001). nee hopaedics,
dressed, but no
at.
y stated
but no details
oncealment
cribed.
nding stated in
ts’
shown in the
e prosthesis an
que in both
nd surgical dra
d for 48 hrs aft
n all cases.
measurements
ard and reliabl
ribed.
ces
0
ot
s
n
nd
ain
fter
le.

Appendices
81
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis)
Not addressed No detail described.
1.10 Where the study is carried out at
more than one site, results are
comparable for all sites
Not addressed No detail described.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY 2.1 How well was the study done to minimise bias?
Code ++, +, or −
+
2.2 If coded as +, or − what is the likely direction in which
bias might affect the study results?
No detail of randomizing
method, concealment method
and binding method are
described.
2.3 Taking into account clinical considerations, your
evaluation of the methodology used, and the statistical
power of the study, are you certain that the overall effect
is due to the study intervention?
Yes
2.4 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes
2.5 Notes. There is no statically significant different between 2 groups in range of motion,
pain scores and need for analgesic. That means there is no significant different in cryocuff
and Robert Jones bandage after TKR

S 2.
SEIn
1
1
1
1
1
1
I G N M
HolmstranesthesrandomiJournal
ECTION 1:n a well condu
.1 The stud
and clea
.2 The assi
treatmen
.3 An adeq
is used
.4 Subjects
‘blind’ a
.5 The trea
are simi
.6 The only
groups i
investig
Methodolog
röm, A., & Hsia after kneized and conof Arthropl
: INTERNAucted RCT stu
dy addresses a
arly focused q
ignment of su
nt groups is ra
quate concealm
s and investig
about treatmen
atment and co
ilar at the start
y difference b
is the treatmen
gation
gy Checkli
Härdin, B. Cee unicompantrolled stulasty, 20(3)
AL VALIDITudy…
an appropriate
question.
ubjects to
andomised
ment method
gators are kept
nt allocation
ntrol groups
t of the trial
between
nt under
ist 2: Cont
C. (2005). Cartmental ar
udy of 60 pa, 316-321.TY
This crite
e Well co
Not rep
Not add
t Not add
Well co
Adequ
addre
trolled Tri
Cryo/Cuff crthroplasty:
atients with
erion is: R
overed
ported T
“r
d
dressed N
m
dressed N
th
overed S
ch
st
uately
essed
-
-
-
-
-
-
ials
compared to a prospectia 6-week fo
Remarks:
PICO covered
The study only
randomized”,
escribed.
No detail of co
method is desc
No detail of bin
he study.
imilar patient
haracteristics
tudy.
All patients rece
assessment and
post-op rehabili
All under tourni
different orthop
Same type of pr
different brand.
All are placed su
All are received
analgesics (Para
dextropropoxyfe
and supplement
5 mg and IV 5m
All have the sam
program
Appendic
82
o epidural ive, ollow-up.
d
y stated
but no details
oncealment
cribed.
nding stated in
ts’
shown in the
eive same pre-op
information after
tation.
iquet control by
edic surgeons.
rosthesis used wit
uction drain
d traditional
acetamol 500mg,
fene 50 and 100m
tary morphine (or
mg/ml)
me rehabilitation
ces
2
s
n
r
th
mg,
ral

Appendices
83
1.7 All relevant outcomes are
measured in a standard, valid and
reliable way
Well covered - The outcome measurement
used are standard and
reliable.
1.8 What percentage of the individuals
or clusters recruited into each
treatment arm of the study
dropped out before the study was
completed?
5% - Cryo: 1
- EDA: 2
- Control: 0
- Acceptable as < 20%
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis)
Not addressed No detail described.
1.10 Where the study is carried out at
more than one site, results are
comparable for all sites
Not addressed No detail described.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY 2.1 How well was the study done to minimise bias?
Code ++, +, or −
+
2.2 If coded as +, or − what is the likely direction in which
bias might affect the study results?
No detail of randomizing
method, concealment method
and binding method are
described.
2.3 Taking into account clinical considerations, your
evaluation of the methodology used, and the statistical
power of the study, are you certain that the overall effect
is due to the study intervention?
Yes
2.4 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes
2.5 Notes. Both Cryo/Cuff and EDA was significantly reduced in morphine used compared
with the control group. No significant difference between groups was noted in subjective
pain, swelling, ROM and function. Cryo/Cuff seems to be a risk-free (1 patient totally
paralyzed in both legs and 1 patient anesthetized in the other leg in EDA group),
well-tolerated, little competence-demanding alternative to EDA in the postoperative pain
management.

S 3.
SEIn
1
1
1
1
1
1
I G N M
KullenbcryotherJournal
ECTION 1:n a well condu
.1 The stud
and clea
.2 The assi
treatmen
.3 An adeq
is used
.4 Subjects
‘blind’ a
.5 The trea
are simi
.6 The only
groups i
investig
Methodolog
berg, B., Ylirapy after toof Arthropl
: INTERNAucted RCT stu
dy addresses a
arly focused q
ignment of su
nt groups is ra
quate concealm
s and investig
about treatmen
atment and co
ilar at the start
y difference b
is the treatmen
gation
gy Checkli
ipää, S., Södotal knee artlasty, 21(8)
AL VALIDITudy…
an appropriate
question.
ubjects to
andomised
ment method
gators are kept
nt allocation
ntrol groups
t of the trial
between
nt under
ist 2: Cont
derlund, K.,throplasty: , 1175-1179TY
This crite
e Adequ
addre
Not rep
Well co
t Not add
Adequ
cove
Well co
trolled Tri
, & Resch, Sa prospectiv9.
erion is: R
uately
essed
T
cl
ported T
“r
d
overed U
dressed N
th
uately
ered
S
ch
st
overed P
-
D
-
-
-
-
N
ials
S. (2006). Pve study of
Remarks:
The compariso
learly in the re
The study only
randomized”,
escribed.
Use of sealed e
No detail of bin
he study.
imilar patient
haracteristics
tudy.
Pre-op:
Pre-medicate
sedative and
During surgery
Both groups
anesthesia w
and ropivaca
All knees are
through a mi
incision with
parapatellar a
Use tourniqu
and applied f
Before skin c
haemostasis
using diather
No wound drai
Appendic
84
Postoperativ86 patients
on hasn’t state
esearch questi
y stated
but no details
envelopes
nding stated in
ts’
shown in the
ed with a mild
paracetamol
y:
are under spin
with morphine
ain
e approached
idline anterior
h a medial
arthrotomy
uet (300 mmH
for 75 mins
closure,
was controlle
rmy
in used
ces
4
ve .
d
ion
s
n
d
nal
r
Hg)
d

Appendices
85
1.7 All relevant outcomes are
measured in a standard, valid and
reliable way
Adequately
addressed
The outcome measurements
used are standard and reliable
in pain, but not mentioned in
the device used in ROM
measurement.
1.8 What percentage of the individuals
or clusters recruited into each
treatment arm of the study
dropped out before the study was
completed?
~3.5% - Cold compression: 2
- EDA: 1
- Acceptable as < 20%
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis)
Not addressed No detail described.
1.10 Where the study is carried out at
more than one site, results are
comparable for all sites
Not addressed No detail described.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY 2.1 How well was the study done to minimise bias?
Code ++, +, or −
+
2.2 If coded as +, or − what is the likely direction in which
bias might affect the study results?
No detail of randomizing
method and binding method
are described.
2.3 Taking into account clinical considerations, your
evaluation of the methodology used, and the statistical
power of the study, are you certain that the overall effect
is due to the study intervention?
Yes
2.4 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes
2.5 Notes. Combined cold compression therapy controls pain (use less analgesics), improves
ROM, and may speed up the time for mobilization.

S 4.
SEIn
1
1
1
1
1
1
1
1
I G N M
Morsi, EJournal
ECTION 1:n a well condu
.1 The stud
and clea
.2 The assi
treatmen
.3 An adeq
is used
.4 Subjects
‘blind’ a
.5 The trea
are simi
.6 The only
groups i
investig
.7 All relev
measure
reliable
.8 What pe
or cluste
Methodolog
E. (2002). Cof Arthropl
: INTERNAucted RCT stu
dy addresses a
arly focused q
ignment of su
nt groups is ra
quate concealm
s and investig
about treatmen
atment and co
ilar at the start
y difference b
is the treatmen
gation
vant outcome
ed in a standar
way
ercentage of th
ers recruited i
gy Checkli
Continuous-lasty, 17(6)
AL VALIDITudy…
an appropriate
question.
ubjects to
andomised
ment method
gators are kept
nt allocation
ntrol groups
t of the trial
between
nt under
s are
rd, valid and
he individuals
nto each
ist 2: Cont
flow cold th, 718-722.TY
This crite
e Poorly ad
Not app
Not app
t Not app
Adequ
addre
Well co
Adequ
addre
s Not add
trolled Tri
herapy after
erion is: R
ddressed
plicable It
st
plicable It
st
plicable A
tr
uately
essed
A
pr
st
p
gr
overed -
-
-
-
uately
essed
T
u
in
th
m
dressed N
ials
r total knee
Remarks:
PICO are not
t is a prospecti
tudy without r
t is a prospecti
tudy without r
All patients rec
reatment.
All patients had
rimary osteoa
taged bilateral
atient will be
roup and cont
All compone
cemented.
All patients w
CPM.
The operatio
or under the
the author us
technique.
And same dr
after surgerie
The outcome m
sed are standa
n pain, but not
he device used
measurement.
No detail descr
Appendic
86
arthroplasty
defined clearl
ive control tri
randomized.
ive control tri
randomized.
ceive the same
d advanced
arthrosis and
l TKRs. Every
the treatment
trol group.
ents were
were placed in
on was done by
supervision o
sing the same
ressing applied
es.
measurements
ard and reliabl
t mentioned in
d in ROM
ribed.
ces
6
y.
ly
ial
ial
e
y
n
y
f
d
le
n

Appendices
87
treatment arm of the study
dropped out before the study was
completed?
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis)
Not addressed No detail described.
1.10 Where the study is carried out at
more than one site, results are
comparable for all sites
Not addressed No detail described.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY 2.1 How well was the study done to minimise bias?
Code ++, +, or −
−
2.2 If coded as +, or − what is the likely direction in which
bias might affect the study results?
The studies was not a
randomized controlled trials
2.3 Taking into account clinical considerations, your
evaluation of the methodology used, and the statistical
power of the study, are you certain that the overall effect
is due to the study intervention?
Yes
2.4 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes
2.5 Notes. Continuous-flow cold therapy is advantageous after TKR. It provides greater knee
extension and flexion at week 1 to 2, lower VAS and less analgesic consumption, with no
adverse effect on wound healing.

S 5.
SEIn
1
1
1
1
1
I G N M
Radkow& EaslearthroplAdvance
ECTION 1:n a well condu
.1 The stud
and clea
.2 The assi
treatmen
.3 An adeq
is used
.4 Subjects
‘blind’ a
.5 The trea
are simi
Methodolog
wski, C. A., ey, M. E. (20asty: a proses, 16(2), 67: INTERNAucted RCT stu
dy addresses a
arly focused q
ignment of su
nt groups is ra
quate concealm
s and investig
about treatmen
atment and co
ilar at the start
gy Checkli
Pietrobon, R007). Cryotspective ran7-72.
AL VALIDITudy…
an appropriate
question.
ubjects to
andomised
ment method
gators are kept
nt allocation
ntrol groups
t of the trial
ist 2: Cont
R., Vail, T. therapy tempndomized tri
TY This crite
e Well co
Well co
Well co
t Well co
Well co
trolled Tri
P., Nunley,perature difial. Journal
erion is: R
overed P
overed P
p
co
ra
overed A
an
te
cr
overed T
su
cl
p
an
to
ea
overed S
ch
st
ials
, J. A., 2nd,fferences afof Surgical
Remarks:
PICO was clea
Patient assignm
erformed usin
omputer-gene
andomization.
An administrat
nd concealed
emperature in
ryotherapy de
The patients, p
urgeons, resea
linical epidem
erforming the
nalysis (R.P.)
o the treatmen
ach patient.
imilar patient
haracteristics
tudy.
Appendic
88
, Jain, N. B.fter total knel Orthopaed
arly covered.
ment was
ng
erated blocked
.
tive assistant s
the assigned
each
evice.
articipating
arch nurse and
miologist
e statistical
were all blind
nt assigned to
ts’
shown in the
ces
8
., ee dic
d
set
d
ded

Appendices
89
1.6 The only difference between
groups is the treatment under
investigation
Well covered - Follow the standard surgical
technique used by each of
the participating surgeons.
Surgical protocols between
the surgeons are similar.
- Same dressing applied
- Same cryotherapy devices
used on both group except
difference temperature.
- The cryotherapy device was
used continuously during the
patients’ hospital stay and
discontinued upon
discharge.
1.7 All relevant outcomes are
measured in a standard, valid and
reliable way
Well covered - All patients were evaluated
in the postoperative period
by the same research nurse.
- Pain: VAS, narcotic
consumption
- Self-reported knee function:
IKDC
- Passive knee ROM: using a
hand goniometer by PT
1.8 What percentage of the individuals
or clusters recruited into each
treatment arm of the study
dropped out before the study was
completed?
Not addressed No detail described.
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis)
Not addressed No detail described.
1.10 Where the study is carried out at
more than one site, results are
comparable for all sites
Not addressed No detail described.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY 2.1 How well was the study done to minimise bias? ++

Appendices
90
Code ++, +, or −
2.2 If coded as +, or − what is the likely direction in which
bias might affect the study results?
2.3 Taking into account clinical considerations, your
evaluation of the methodology used, and the statistical
power of the study, are you certain that the overall effect
is due to the study intervention?
Yes
2.4 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes
2.5 Notes. With the colder 45°F cryotherapy temperature following TKR, no improvement
was observed in the short-term postoperative narcotic consumption and pain scores, ROM
and self-reported knee function. No adverse effects were reported with the cryotherapy
treatment.

S 6.
SEIn
1
1
1
1
1
1
1
1
1
I G N M
Smith, Jcontrollepostoper
ECTION 1:n a well condu
.1 The stud
and clea
.2 The assi
treatmen
.3 An adeq
is used
.4 Subjects
‘blind’ a
.5 The trea
are simi
.6 The onl
groups i
investig
.7 All relev
measure
reliable
.8 What pe
or cluste
treatmen
dropped
complet
.9 All thein the gwere ra(often intenti
Methodolog
J., Stevens, ed trial comrative total : INTERNAucted RCT stu
dy addresses a
arly focused q
ignment of su
nt groups is ra
quate concealm
s and investig
about treatmen
atment and co
ilar at the start
y difference b
is the treatmen
gation
vant outcome
ed in a standar
way
ercentage of th
ers recruited i
nt arm of the s
d out before th
ted?
e subjects argroups to wandomly allreferred to on to treat a
gy Checkli
J., Taylor, Mmparing com
knee replacAL VALIDITudy…
an appropriate
question.
ubjects to
andomised
ment method
gators are kept
nt allocation
ntrol groups
t of the trial
between
nt under
s are
rd, valid and
he individuals
nto each
study
he study was
re analysed which they located as analysis)
ist 2: Cont
M., & Tibbempression bacement surgTY
This crite
e Adequ
addre
Well co
Not add
t Not add
Well co
Well co
Adequ
addre
s Not add
Not add
trolled Tri
ey, J. (2002andaging an
gery. Orthop
erion is: R
uately
essed
overed
dressed N
m
dressed N
th
overed S
ch
st
overed O
af
uately
essed
T
u
in
th
m
dressed N
dressed N
ials
2). A randomnd cold therpaedic Nurs
Remarks:
Outcome is no
Randomize by
No detail of co
method is desc
No detail of bin
he study.
imilar patient
haracteristics
tudy.
Only different
fter OT
The outcome m
sed are standa
n pain, but not
he device used
measurement.
No detail descr
No detail descr
Appendic
91
mized, rapy in sing, 2, 61-6
ot stated clear
y coin toss.
oncealment
cribed.
nding stated in
ts’
shown in the
at the first day
measurements
ard and reliabl
t mentioned in
d in ROM
ribed.
ribed.
ces
1
66.
rly
n
y
le
n

Appendices
92
1.10 Where the study is carried out at
more than one site, results are
comparable for all sites
Not addressed No detail described.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY 2.1 How well was the study done to minimise bias?
Code ++, +, or −
+
2.2 If coded as +, or − what is the likely direction in which
bias might affect the study results?
No detail of concealment
method and binding method
are described.
2.3 Taking into account clinical considerations, your
evaluation of the methodology used, and the statistical
power of the study, are you certain that the overall effect
is due to the study intervention?
Yes
2.4 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes
2.5 Notes. No difference between the two management techniques for pain scores and swelling
in the first 48 hours of the postoperative period. A cost benefit analysis showed the
compression bandaging is cheaper and less labor intensive to manage than the cold
therapy.

S 7.
SEIn
1
1
1
1
1
1
1
1
1
I G N M
Woolf, SComparsimple iKnee Su
ECTION 1:n a well condu
.1 The stud
and clea
.2 The assi
treatmen
.3 An adeq
is used
.4 Subjects
‘blind’ a
.5 The trea
are simi
.6 The only
groups i
investig
.7 All relev
measure
reliable
.8 What pe
or cluste
treatmen
dropped
complet
.9 All thein the gwere ra(often intenti
Methodolog
S. K., Barfierison of a coicing regimeurgery, 21(1: INTERNAucted RCT stu
dy addresses a
arly focused q
ignment of su
nt groups is ra
quate concealm
s and investig
about treatmen
atment and co
ilar at the start
y difference b
is the treatmen
gation
vant outcome
ed in a standar
way
ercentage of th
ers recruited i
nt arm of the s
d out before th
ted?
e subjects argroups to wandomly allreferred to on to treat a
gy Checkli
eld, W. R., Montinuous teen following), 15-19.
AL VALIDITudy…
an appropriate
question.
ubjects to
andomised
ment method
gators are kept
nt allocation
ntrol groups
t of the trial
between
nt under
s are
rd, valid and
he individuals
nto each
study
he study was
re analysed which they located as analysis)
ist 2: Cont
Merrill, K. Demperature-g outpatient
TY This crite
e Well co
Adequ
addre
Not add
t Not add
Poorly ad
Adequ
addre
Adequ
addre
s ~11.6
Not add
trolled Tri
D., & McB-controlled ct knee arthr
erion is: R
overed
uately
essed
-
-
-
dressed N
m
dressed N
th
ddressed N
ch
uately
essed
uately
essed
P
67% -
-
-
dressed N
ials
ryde, A. M.cryotherapyroscopy. The
Remarks:
PICO was cle
Randomizatio
record numbe
Even no. → C
Odd no. → Ic
No detail of co
method is desc
No detail of bin
he study.
No specific pat
haracteristics
Pain: 5-points V
- Ice therap
quit or exclud
- CTC: 4 pa
excluded
- Acceptabl
No detail descr
Appendic
93
., Jr. (2008)y device to ae Journal of
early stated
on by hospital
ers
CTC
ce therapy
oncealment
cribed.
nding stated in
tient
described.
VAS
py: 3 patients
ded
atients quit or
le as < 20%
ribed.
ces
3
. a f
l
n
r
Appendices
94
1.10 Where the study is carried out at
more than one site, results are
comparable for all sites
Not applicable In one center only
SECTION 2: OVERALL ASSESSMENT OF THE STUDY 2.1 How well was the study done to minimise bias?
Code ++, +, or −
+
2.2 If coded as +, or − what is the likely direction in which
bias might affect the study results?
No detail of concealment
method, binding method and
patient characteristics are
described.
2.3 Taking into account clinical considerations, your
evaluation of the methodology used, and the statistical
power of the study, are you certain that the overall effect
is due to the study intervention?
Yes
2.4 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes
2.5 Notes. There is no difference in pain intensity for any of the follow up days. However, the
percentage of patients with nighttimes’ pain that disrupted their sleep was significantly
lower on the second postoperative day for the continuous cryotherapy group compared
with the ice therapy group. It showed modest benefit in continuous flow,
temperature-controlled cryotherapy device versus ice therapy for early nighttimes’ pain
control and improved quality of life following routine outpatient knee arthroscopy
procedure, with less risk of thermal injury.

Appendices
95
Appendix 6: Summary of Levels of Evidences
Bibliographic
Citation Study Type
Levels of
Evidence % of criteria fulfilled
1. Gibbons, Solan,
Ricketts, &
Patterson
(2001)
RCT 1 + 40%
2. Holmström &
Härdin (2005) RCT 1 + 50%
3. Kullenberg,
Ylipää,
Söderlund, &
Resch (2006)
RCT 1 + 60%
4. Morsi (2002) PCT 1 – 30%
5. Radkowski, et
al. (2007) RCT 1 ++ 70%
6. Smith, Stevens,
Taylor, &
Tibbey (2002)
RCT 1 + 50%
7. Woolf, et al.
(2008) RCT 1 + 50%

Appendices
96
Appendix 7: Criteria for Evaluating the Implementation Potential of an Innovation under Scrutiny
Transferability of the Findings
1. Will the innovation “fit” in the proposed setting?
2. How similar are the target population in the research and that in the new setting?
3. Is the philosophy of care underlying the innovation fundamentally different from the philosophy prevailing in the
practice setting? How entrenched is the prevailing philosophy?
4. Is there a sufficiently large number of clients in the practice setting who could benefit from the innovation?
5. Will the innovation take too long to implement and evaluate?
Feasibility
1. Will nurses have the freedom to carry out the innovation? Will they have the freedom to terminate the innovation
if it is considered undesirable?
2. Will the implementation of the innovation interfere inordinately with current staff functions?
3. Does the administration support the innovation? Is the organizational climate conducive to research utilization?
4. Is there a fair degree of consensus among the staff and among the administrators that the innovation could be
beneficial and should be tested? Are there major pockets of resistance or uncooperativeness that could undermine
efforts to implement and evaluate the innovation?
5. To what extent will the implementation of the innovation cause friction within the organization? Does the
utilization project have the support and co-operation of department outside the nursing department?
6. Are the skills needed to carry out the utilization project (both the implementation and the clinical evaluation)
available in the nursing staff? If not, how difficult will it be to collaborate with or to secure the assistance of
others with the necessary skills?
7. Does the organization have the equipment and facilities necessary for the innovation? If not, is there a way to
obtain the needed resources?
8. If nursing staff need to be released from other practice activities to learn about and implement the innovation,
what is the likelihood that this will happen?
9. Are appropriate measuring tools available for a clinical evaluation of the innovation?
Cost/Benefit Ratio of the Innovation
1. What are the risks to which clients would be exposed during the implementation of the innovation?
2. What are the potential benefits that could result from the implementation of the innovation?
3. What are the risks of maintaining current practices (i.e. the risks of not trying the innovation)?
4. What are the material costs of implementing the innovation? What are the costs in the short term during
utilization, and what are the costs in the long run, if the change is to be institutionalized?
5. What are the material costs of not implementing the innovation (i.e. could the new procedure result in some
efficiencies that could lower the cost of providing service)?
6. What are the potential non-material costs of implementing the innovation to the organization (e.g. lower staff
morale, staff turnover, and absenteeism)?
7. What are the potential non-material benefits of implementing the innovation (e.g. improved staff morale,
improved staff recruitment)?

Appendices
97
Appendix 8: Cryotherapy Protocol Flow Chart
R2.1: Apply cryocuff immediately after surgery
Preoperative Stage:
Intra-operative Stage:
Early Postoperative Stage
Middle Postoperative Stage
Late Postoperative Stage:
R1.1: Use cryocuff as a mean to provide continuous compression cryotherapy
R2.3: Place cryocuff on the anterior part of knee as well as leave patella and popliteal space free of pressure
R2.2: Place the cryocuff on a light dressing wound
Cryocuff Management R3.1: Keep cryocuff continuously on affected knee at least 48 hours
after operation
Regular Assessment
R3.4: To evaluate pain intensity R3.5: To prevent complication
R4.1: Disconnect cryocuff system with the cuff remained on the knee during mobilization
R5.1: Apply intermitted ice pack regimen after removal of cryocuff
R3.2: Keep temp at 7°C – 15°C R3.3: Re-chill regularly
Regular Assessment (R3.4 – R3.5)

Appendices
98
Appendix 9: Gannt Chart of Implementing the Protocol
Week 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 37 39 40 41 42 43 44 45
Preparation:
1. Searching evidences
2. Data summary and synthesis
3. Protocol development
4. Cryotherapy team formation
Pilot Study:
1. Communication with stakeholders
2. Training staff
3. Trial implementation
4. Evaluation and modification
Implementation:
Evaluation:

Appendices
99
Appendix 10: Pain Management Record Chart

Appendices
100
Appendix 10: Pain Management Record Chart (Cont’d)

Appendices
101
Appendix 11: Knee Circumferences Record Chart
Hospital Authority TSEUNG KWAN O HOSPITAL
ORTHOPAEDIC & TRAUMATOLOGY
Knee Circumferences Record Chart
Please Use Block Letter or Affix Label
Hospital No:____________Name:_________________________I.D. No:________Sex:____ Age:____Dept:_____ Team:___ Ward/Bed:__
OT
Day Date Time
Affected Knee (in mm)
(Left / Right)*
Non-Affected Knee (in mm)
(Left / Right)*
Staff
Signature
1
2
3
4
5
6
7
8
9
10
11
12
13
14
* Circle as appropriate

Appendices
102
Appendix 12: Range of Motion Record Chart
Hospital Authority TSEUNG KWAN O HOSPITAL
ORTHOPAEDIC & TRAUMATOLOGY
Range of Motion Record Chart
Please Use Block Letter or Affix Label
Hospital No:____________Name:_________________________ I.D. No:_________ Sex:___ Age:____
Dept:______ Team:____ Ward/Bed:___
OT
Day Date Time
Affected _______(area)
(Left / Right)*
Non-Affected _______(area)
(Left / Right)* Staff
SignatureMax
Active
Extension
Max
Active
Flexion
Max
Passive
Extension
Max
Passive
Flexion
Max
Active
Extension
Max
Active
Flexion
Max
Passive
Extension
Max
Passive
Flexion
1
2
3
4
5
6
7
8
9
10
11
12
13
14
* Circle as appropriate

References
103
REFERENCES
Abramson, D. I., Chu, L. S., Tuck, S., Jr., Lee, S. W., Richardson, G., & Levin, M.
(1966). Effect of tissue temperatures and blood flow on motor nerve
conduction velocity. The Journal of the American Medical Association,
198(10), 1082-1088.
Adie, S., Naylor, J. M., & Harris, I. A. (2010). Cryotherapy after total knee
rrthroplasty: a systematic review and meta-analysis of randomized
controlled trials. Journal of Arthroplasty, 25(5), 709-715.
Barry, S., Wallace, L., & Lamb, S. (2003). Cryotherapy after total knee
replacement: a survey of current practice. Physiotherapy Research
International, 8(3), 111-120.
Bonica, J. J. (1990). The management of pain (2nd ed.). Philadelphia: Lea &
Febiger.
Brander, V., & Stulberg, S. D. (2006). Rehabilitation after hip- and knee-joint
replacement. American Journal of Physical Medicine & Rehabilitation, 85
(Suppl), S98-S118.
Chatap, G., De Sousa, A., Giraud, K., & Vincent, J.-P. (2007). Pain in the elderly:
Prospective study of hyperbaric CO2 cryotherapy (neurocryostimulation).
Joint Bone Spine, 74, 617-621.
References
104
Chou, S. Y., & Liu, H. E. (2008). Comparsion of effectiveness between moist and
dry cryotherapy in reducing discomfort after orthognathic surgery. Journal
of Clinical Nursing, 17, 1735-1741.
Coordinating Committee in Orthopaedics & Traumatology. (2011). Total Knee
Replacement. (PILIC0053E Version1.1). Hong Kong: Hospital Authority.
Crutchfield, J., Zimmerman, L., Nieveen, J., Barnason, S., & Pozehl, B. (1996).
Preoperative and postoperative pain in total knee replacement patients.
Orthopaedic Nursing, 15(2), 65-72.
Department of Pharmacy, TKOH. (July 2011). TKOH Formulary. Tseung Kwan
O Hospital, Hospital Authority. Retrieved 27th December, 2011, from
https://gateway.ha.org.hk/vdesk/index.php3?Z=5,6
Farry, P. J., Prentice, N. G., Hunter, A. C., & Wakelin, C. A. (1980). Ice treatment
of injured ligaments: an experimental model. New Zealand Medical
Journal, 91(651), 12-14.
Gibbons, C. E. R., Solan, M. C., Ricketts, D. M., & Patterson, M. (2001).
Cryotherapy compared with Robert Jones bandage after total knee
replacement: A prospective randomized trial. International Orthopaedics,
25(4), 250-252.
References
105
Grella, R. J. (2008). Continuous passive motion following total knee arthroplasty:
a useful adjunct to early mobilisation? Physical Therapy Reviews, 13(4),
269-279.
Holmström, A., & Härdin, B. C. (2005). Cryo/Cuff compared to epidural
anesthesia after knee unicompartmental arthroplasty: a prospective,
randomized and controlled study of 60 patients with a 6-week follow-up.
Journal of Arthroplasty, 20(3), 316-321.
Hospital Authority. Employee Handbook. Hong Kong: Hospital Authority.
Hospital Authority. (1st July 2002, 30th September 2010). Guidelines for
Specialty Nursing Service: Orthopedic & Traumatological Nursing Care.
Retrieved 3rd December, 2011, from
http://www.ekg.org.hk/html/gateway/index.htm?http://www.ekg.org.hk/ht
ml/gateway/clinical/guidelines.jsp&1
Hospital Authority. (2010). Vision, Mission and Values. Retrieved 3rd December,
2011, from
http://www.ha.org.hk/visitor/ha_visitor_index.asp?Content_ID=10009&La
ng=ENG&Dimension=100&Parent_ID=10

References
106
Kullenberg, B., Ylipää, S., Söderlund, K., & Resch, S. (2006). Postoperative
cryotherapy after total knee arthroplasty: a prospective study of 86 patients.
Journal of Arthroplasty, 21(8), 1175-1179.
Lenth, R. V. (2006-9). Java Applets for Power and Sample Size [Computer
software]. Retrieved 13th May, 2012, from
http://www.stat.uiowa.edu/~rlenth/Power
Lin, C. W., March, L., Crosbie, J., Crawford, R., Graves, S., Naylor, J., et al.
(2009). Maximum recovery after knee replacement--the MARKER study
rationale and protocol. BMC Musculoskeletal Disorders, 10, 69-76.
Lombardi, A. V., Drouillard, P. D., Mallory, T. H., & Vaughn, B. K. (1993). The
efficacy of continuous cold therapy in the postoperative management of
total knee arthroplasty patients. Orthopaedic Transactions, 17(1), 157.
Martin, S. S., Spindler, K. P., Tarter, J. W., & Detwiler, K. B. (2002). Does
cryotherapy affect intraarticular temperature after knee arthroscopy?
Clinical Orthopaedics & Related Research(400), 184-189.
Matsen, F. A., 3rd, Questad, K., & Matsen, A. L. (1975). The effect of local
cooling on postfracture swelling. A controlled study. Clinical
Orthopaedics & Related Research(109), 201-206.

References
107
Melnyk, B. M., & Fineout-Overholt, E. (2005). Evidence-based practice in
nursing & healthcare: A guide to best practice. Philadelphia: Lippincott
Williams & Wilkins.
Morsi, E. (2002). Continuous-flow cold therapy after total knee arthroplasty.
Journal of Arthroplasty, 17(6), 718-722.
Medical Service Development Committee, Hospital Authority. (April 2002).
Hospital Authority Strategy on CPG Development. Retrieved 3rd
December, 2011, from
http://www.ekg.org.hk/html/gateway/tm/cpg/ha-policy.htm
Nadler, S. F., Weingand, K., & Kruse, R. J. (2004). The Physiologic Basis and
Clinical Applications of Cryotherapy and Thermotherapy for the Pain
Practitioner. Pain Physician, 7, 395-399.
Naylor, J., Harmer, A., Fransen, M., Crosbie, J., & Innes, L. (2006). Status of
physiotherapy rehabilitation after total knee replacement in Australia.
Physiotherapy Research International, 11(1), 35-47.
Pearse, E. O., Caldwell, B. F., Lockwood, R. J., & Hollard, J. (2007). Early
mobilisation after conventional knee replacement may reduce the risk of
postoperative venous thromboembolism. Journal of Bone & Joint Surgery
- British Volume, 89(3), 316-322.

References
108
Polit, D. F., & Beck, C. T. (2008). Nursing research: Generating and assessing
evidence for nursing practice (8th ed.). Philadelphia: Lippincott.
Radkowski, C. A., Pietrobon, R., Vail, T. P., Nunley, J. A., 2nd, Jain, N. B., &
Easley, M. E. (2007). Cryotherapy temperature differences after total knee
arthroplasty: a prospective randomized trial. Journal of Surgical
Orthopaedic Advances, 16(2), 67-72.
Schroder, D., & Passler, H. H. (1994). Combination of cold and compression after
knee surgery. A prospective randomized study. Knee Surgery and Sports
Traumatology, 2(3), 158-165.
Scottish Intercollegiate Guidelines Network. (2008). SIGN 50: A Guideline
Developer's Handbook - Annex B: Key to Evidence Statements and
Grades of Recommendations Retrieved 25 May 2011, from
http://www.sign.ac.uk/guidelines/fulltext/50/annexb.html
Scottish Intercollegiate Guidelines Network. (2008). SIGN 50: A Guideline
Developer's Handbook - Annex C: Critical appraisal - Notes and checklists.
Retrieved 25 May 2011, from
http://www.sign.ac.uk/guidelines/fulltext/50/annexc.html

References
109
Scottish Intercollegiate Guidelines Network. (2008). SIGN 50: A Guideline
Developer's Handbook - Annex D: Completed Evidence Table. Retrieved
25 May 2011, from
http://www.sign.ac.uk/guidelines/fulltext/50/compevidence.html
Smith, J., Stevens, J., Taylor, M., & Tibbey, J. (2002). A randomized, controlled
trial comparing compression bandaging and cold therapy in postoperative
total knee replacement surgery. Orthopaedic Nursing, 21(2), 61-66.
Woolf, S. K., Barfield, W. R., Merrill, K. D., & McBryde, A. M., Jr. (2008).
Comparison of a continuous temperature-controlled cryotherapy device to
a simple icing regimen following outpatient knee arthroscopy. The Journal
of Knee Surgery, 21(1), 15-19.
Yan, C. H., Chiu, K. Y., & Ng, F. Y. (2011). Total knee arthroplasty for primary
knee osteoarthritis: changing pattern over the past 10 years. Hong Kong
Medical Journal, 17(1), 20-2





























