Embed Size (px)
Citation preview

Abstract of dissertation entitled
“Evidence Based Guideline of Prone Positioning for Adult Patients
with Acute Respiratory Distress Syndrome in Intensive Care Unit”
Submitted by
Wong Sze Lok Rebecca
for the degree of Master of Nursing
at The University of Hong Kong
in August 2014
Acute respiratory distress syndrome (ARDS) is a life-threatening condition commonly
seen in critically ill patients. Direct treatment against ARDS which supports the respiratory
system and treats the underlying cause is limited. Furthermore, it may cause
ventilator-induced lung injury when given high doses of oxygen and continued breathing
pressure (Ricard, Dreyfuss & Saumon, 2003). Several researches have found a simple, safe
and inexpensive prone positioning, which improves oxygenation and effectively benefited on
the survival of ARDS patients.
The objectives of this dissertation are (1) to perform a systematic review for a critical
appraisal of the current evidence on prone positioning to improve respiratory status for the
patients with ARDS, (2) to develop an evidence-based guideline and assess the
implementation potential, and (3) to develop an implementation and evaluation plan for

translating the guideline to an adult ICU of a public hospital in Hong Kong.
In order to identify studies that compared prone positioning with the standard practice,
a systematic search was performed with the use of three electronic databases, namely
PubMed (1997-2013), Medline (ProQuest, 1991-2013) and CINAHL (EBSCO host,
1991-2013). 183 articles were identified, and nine randomized controlled trail studies met the
inclusion criteria. The quality of these selected studies was critiqued by using the Scottish
Intercollegiate Guidelines Network. Seven of the selected studies were graded as high quality.
An early, continuous and prolonged prone positioning was concluded beneficial to patient
outcomes with high statistical significance. There were oxygenation improvements, as well as
reduction in both incidences of pneumonia and mortality rate.
The implementation potential includes the transferability, feasibility and
cost-effectiveness of the innovation to the target setting and audience in the local ICU. An
evidence-based guideline of prone positioning for ARDS patients is developed and is
proposed to translate into practice. The implementation plan includes a communication plan
with stakeholders and a pilot test. The guideline will be revised after a six-month pilot trial.
The outcomes of patients, healthcare providers and system will be evaluated after
implementation. The primary outcome of the innovation is oxygenation. According to
previous studies, a 40mmHg increase in ventilation/perfusion ratio at Day 4 of the
intervention will be considered as clinically effective.

Evidence Based Guideline of Prone Positioning for Adult Patients
with Acute Respiratory Distress Syndrome in Intensive Care Unit
by
Wong Sze Lok Rebecca
BSc (HONS) Nursing. H.K.P.U.; RN. H.K.
A dissertation submitted in partial fulfillment of the requirements for
the degree of Master of Nursing
at The University of Hong Kong
August 2014

i
Declaration
I declare that this dissertation and the research work represents my own work, except
where due acknowledgement is made, and that it has not been previously included in a thesis,
dissertation or report submitted to this University or to any other institution for a degree,
diploma or other qualifications.
Signed………………………………………..
Wong Sze Lok Rebecca
ii
Acknowledgements
I would like to express my deepest gratitude to my supervisor, Dr. Athena Hong, for
her continuous kind guidance and support on my dissertation over the past two years. She has
inspired me with valuable ideas, suggestions and criticisms. I would not have finished my
dissertation without her inspiration and guidance.
I would also like to extend my gratitude to the hard working staff members of Master
of Nursing Studies, for their kindness and patience. Last but not the least, I would like to
thank my family and friends for their unconditional love and support throughout my studies.
Their words of encouragement helped me to keep on going even when times are low.
iii
Table of Contents
Declaration………………………………………………………………………………………… i
Acknowledgements………………………………………………………………………………… ii
Table of Contents………………………………………………………………………………….. iii
Lists of Appendices………………………………………………………………………………... vii
List of Abbreviations………………………………………………………………...................... viii
Chapter 1 Introduction
1.1 Background………………………………………........................................... 1
1.2 Affirming the Needs………………………..……………………...........……. 2
1.2.1 Incidence and prognosis of ARDS………………………………..…… 2
1.2.1 Statistics of ARDS in Hong Kong…………………………………....... 3
1.2.3 Current practice of prone positioning……………………………........ 4
1.3 Research Question, Objectives, Significance……………………………….. 4
1.3.1 Research question…………………………………..………………….. 4
1.3.2 Setting objectives………………………………………………….......... 5
1.3.3 Significance……………………………………..………………............. 5
Chapter 2 Critical Appraisal
2.1 Search Strategies……………………………………………………………... 7
2.1.1 Search methodology……………………………………….………….... 7
2.1.2 Keywords……………………………………………..……..……..…… 7
2.1.3 Selection criteria………………………………………………....….…. 8
2.1.3.1 The inclusion criteria……………………………………………..... 8
2.1.3.2 The exclusion criteria…………………………..………………...... 8
2.1.4 Data extraction……………………………………………..……….….. 8
2.2 Appraisal Strategies………………………………………………………….. 9
2.3 Appraisal Results………………………………………………......……….... 9
2.3.1 Searching results……………………………………………..……….... 9
2.3.2 Overview of the selected studies………………………………………. 10
2.3.3 Randomization and concealment allocation ……………….………… 10
2.3.4 Blinding…………………………………………………………….…… 11
2.3.5 Baseline characteristics………………………………………......….… 11
2.3.6 Data collection………………………………………..……………..….. 11
2.3.7 Power calculation……………………………………….……………… 12
iv
2.3.8 Application of the studies………………………………..………….…. 12
2.3.9 Summary of quality appraisal…………………………..…………...... 13
2.4 Summary and Synthesis of Findings…………………………………..……. 13
2.4.1 Study characteristics………………………………………………...…. 13
2.4.2 Subjects’ characteristics……………………………………..………… 14
2.4.3 Intervention……………………………………………….…………..... 16
2.4.4 Control/ comparison………………………………………………...…. 16
2.4.5 Outcome measures and effect size……………………………..……… 17
2.4.5.1 Participants’ ventilation…………………………………..………... 17
2.4.5.2 Incidence of pneumonia………………………………………........ 18
2.4.5.3 Rate of mortality………………………………………………...….. 18
2.4.5.4 Adverse events……………………………...………………………. 19
2.4.6 Data synthesis and implication...…………………………..………….. 20
2.4.6.1 Participants’ ventilation…………………………………….…...…. 20
2.4.6.2 Incidence of pneumonia………………………………………….... 21
2.4.6.3 Rate of mortality…………………………………………………..... 21
2.4.6.4 Adverse events…………………………………………...…………. 22
Chapter 3 Implementation Potential
3.1 Transferability of the Innovation……………….......................…………..... 24
3.1.1 Target setting/ audience ……………………………….....………….… 24
3.1.1.1 Fitness of the setting………………………………………….....…. 24
3.1.1.2 Characteristics of target population……………………………...... 25
3.1.2 Philosophy of care…………………………………………..………...... 25
3.1.3 Benefit sufficient patients…………………………….…....................... 26
3.1.4 Time frame for implementation and evaluation ……..………..…….. 26
3.2 Feasibility of Implementation …………….………………….……………... 27
3.2.1 Freedom to implement and terminate the innovation……….…….… 27
3.2.2 Interference with current staff practice…………………………..…... 27
3.2.3 Organization climate…………………………………..………...…….. 28
3.2.4 Collaboration among departments……………………….………….... 28
3.2.5 Skills training ……………….……………………………..……..…..... 29
3.2.6 Equipment for implementation and evaluation ……………....……... 29
3.3 Cost-Benefit Ratio of the Innovation………………………………….……. 31
3.3.1 Patient’s potential risks and benefits……………………………..…... 31
3.3.2 Potential risks and benefits towards staff and the setting……............ 31
3.3.3 Potential risks of maintaining current practice……............................ 32
3.3.4 Potential material and non-material costs for implementation…....... 32

v
Chapter 4 Developing an Evidence Based Practice Guideline
4.1 Title of the Evidence-Based Practice Guideline……………..……………... 33
4.2 Aim of the Guideline…………………………...…….…….……………….... 33
4.3 Objectives of the Guideline………………………………………………….. 33
4.4 Target Population……………………………………………………......…… 33
4.5 Target Users of the Guideline……………………………...………………... 34
4.6 Grading Scheme of the Guideline…………………………………………… 34
4.7 Practice Recommendations….……………………..……………...………… 34
4.7.1 Assessment……………………………………………………..……….. 34
4.7.2 Initiation and implementation of prone positioning…………………. 35
4.7.3 Monitoring and evaluation……………………………...………...…… 35
4.7.4 Termination …………………………………….……………....……… 36
Chapter 5 Implementation Plan
5.1 Communication Plan with Potential Stakeholders........................................ 37
5.1.1 Identification of the stakeholders………………………………..……. 37
5.1.2 The process of communication plan and implementation strategies.. 38
5.1.2.1 Initiating the proposed innovation………...………..…………....... 38
5.1.2.2 Guiding the proposed innovation………….……………………..... 39
5.1.2.3 Sustaining the proposed innovation………...……………............... 41
5.2 Pilot Study to Try Out the Guideline……..…………………………………. 41
5.2.1 The objectives of pilot study……………………………..……………. 41
5.2.2 Patient recruitment of pilot study….………….….………….…..…… 42
5.2.3 The new evidence based guideline of prone positioning…….….......... 42
5.2.4 Data collection for patient, staff and system outcomes……………… 42
5.2.5 Evaluation of pilot study……………………………..…….….............. 43
Chapter 6 Evaluation Plan
6.1 Identify Outcomes to be Achieved……………………...……………..…...... 44
6.1.1 Patient outcomes………………………….………..……………..….... 44
6.1.2 Healthcare provider outcomes………..…………...…….………….…. 45
6.1.3 System outcomes……………………...……………..…………………. 45
6.2 Nature and Number of Clients to be Involved………………..…………..... 45
6.3 Data Collection, Time and Frequency of Taking Measurements…............. 46
6.4 Data Analysis……………………………………………….……………..….. 48
6.5 Criteria of an Effective the Guideline…………………………………...….. 48

vi
Chapter 7 Conclusion 50
References……………………………………………………..…………….…………... 51
Appendices…………………………………………………………..………….……..… 57
vii
Lists of Appendices
Appendix 1
Search Strategies …...……………………………………………..……………..
57
Appendix 2
Table of Evidence…………………………………………………..…………….
58
Appendix 3
Critical Appraisal of Each Study by SIGN.………..……………………………..
67
Appendix 4
Summary of Critical Appraisal…………………………………………………...
76
Appendix 5
Grades of Recommendations……………………………………………...……..
77
Appendix 6
Cost-benefit Ratio for the Innovation…..……………..……………….…………
78
Appendix 7
Recommendations of the Innovation…...…..………...………………...……...…
79
Appendix 8
Flow of Communication………………………………………………………….
83
Appendix 9
Evaluation Questionnaire of Journal Club……………………………..…….…..
84
Appendix 10
Evaluation Questionnaire of Training Workshop…………………………...……
85
Appendix 11
Evaluation Questionnaire of Pilot Study…………...……………………….……
86

viii
List of Abbreviations
ABG
ACs
ALI
APNs
Arterial blood gas
Associated Consultants
Acute lung injury
Advanced Practice Nurses
ARDS Acute respiratory distress syndrome
ARF Acute respiratory failure
BAL Bronchoalveolar lavage
BMI Body mass index
CI
COS
DOM
EBP
Confidence interval
Chief of Service
Department Operation Manager
Evidence based practice
FiO2 Fraction of inspired oxygen
HR Hazard ratio
ICU Intensive care unit
ISS Injury severity score
LIS Lung injury score
LOS
MOs
Length of stay
Medical Officers
MV
NC
Mechanical ventilation
Nurse Consultant
NIV Noninvasive ventilation
ns Not significance
PaCO2 Partial pressure of arterial carbon dioxide
PaO2 Partial pressure of arterial oxygen
PaO2/FiO2 ratio
PCAs
Ventilation/perfusion ratio
Patient Care Assistants
PEEP Positive end-expiratory pressure
PP Prone position,
RCT Randomized controlled trial
RR Relative risk
SAPS II Simplified Acute Physiology Score II
SIGN Scottish Intercollegiate Guidelines Network
SOFA
Sequential Organ Failure Assessment

ix
SPSS
UP
The Statistical Package for Social Science
Upright position
VAP Ventilator-associated pneumonia
VC
WCC
WM
Volume control
White cell count
Ward Manager

1
Chapter 1
Introduction
1.1 Background
Acute respiratory distress syndrome (ARDS) is commonly developed in critically ill
patients. It is a serious and life-threatening condition. The lungs suffer from severe
widespread injury, which results in insufficient oxygen from getting to the lungs and into the
bloodstream (Matthay, Ware & Zimmerman, 2012). According to the Bernard et al. (1994),
the American-European Consensus Conference characterized three clinical features of ARDS:
1) bilateral lung infiltrates on the chest radiograph; 2) severe hypoxemia with
ventilation/perfusion (PaO2/FiO2) ratio less than 200mmHg, irresponsive of positive end
expiratory pressure (PEEP) level; 3) no sign of left arterial hypertension or pulmonary
capillary wedge pressure is less than 18mmHg. Besides, the Berlin definition (2012)
classified the severity of ARDS with the basis on the degree of hypoxemia: mild (200mmHg<
PaO2/FiO2≦300mmHg), moderate (100mmHg < PaO2/FiO2≦200mmHg), and severe
(PaO2/FiO2< 100mmHg).
The onset of ARDS is acute and sudden. It usually develops over 4 to 48 hours and
lasts for days, even weeks (Sharma, 2010). The occurrence of ARDS depends on several
factors. The common causes of ARDS are bacterial or viral pneumonia, such as H1N1
influenza, sepsis due to non-pulmonary infection, aspiration of gastric contents into lungs and

2
major trauma. Once people develop ARDS, they become severe dyspnea and cyanosis. At
worst, mechanical ventilation is required for respiratory failure. The function of other organ
deteriorates quickly due to insufficient oxygen supply. As a result, these patients are at high
risk of death if appropriate treatments are not carried out immediately.
Patients with ARDS in the intensive care unit (ICU) are very critical. Direct treatment
against ARDS that supports the respiratory system and treats the underlying cause is limited.
Respiratory support mainly focuses on mechanical ventilation which aims to give high doses
of oxygen and continued breathing pressure. It may cause ventilator-induced lung injury by
over-distention and eventually worsens the function of the lungs (Ricard, Dreyfuss &
Saumon, 2003). Other than mechanical ventilation, prone positioning is one of the most
effective and safe supportive treatment for ARDS patients. However, it is rarely used in the
ICU.
1.2 Affirming the Needs
1.2.1 Incidence and prognosis of ARDS
A few statistical reports have shown most episodes of ARDS are associated with
common causes or predisposing conditions. 10% to 15% of all ICU patients and up to 20% of
mechanically ventilated patients developed ARDS in the United States (Frutos-Vivar, Nin &
Esteban, 2004). Studies conducted by Rubenfeld et al. (2005) noted the incidence of acute
lung injury (ALI) was 79 people per 100,000 populations per year, whereas 59 people per

3
100,000 populations met the criteria of ARDS. However, the most common cause of death for
ARDS was closely related to the number of organ systems involved. About 15% to 30%
mortality resulted from respiratory failure alone, whereas up to 80 % mortality involved three
or more organ failures. The crude mortality rate of ARDS was high, ranging from 34% to
58%, which increased with advancing age as well (Sharma, 2010). In Iceland, the length of
ICU stay for ARDS patients was about 21 days and the hospital stay was 39 days
(Sigvaldason et al, 2006). With the high mortality rate and long recovery period of ARDS
patients, it created a major consequence to the health care system. Fortunately, recent
researches have shown that applying an early, continuous and prolonged prone positioning to
severe ARDS patients led to a 20% decrease in the mortality rate (Guerin et al., 2013).
Voggenreiter et al. (2005) also suggested that the prevalence rate of ARDS was decreased by
prone positioning.
1.2.2 Statistics of ARDS in Hong Kong
In Hong Kong, pneumonia and septicemia were the third and the eighth leading cause
of death in 2011 (The Department of Health, 2012). Roughly estimated by clinical experience,
about 70% of patients were diagnosed with bacterial or viral pneumonia or sepsis in the target
ICU. The ICU admission rate of patients with pneumonia increased sharply especially during
flu season. These patients were high at risk to develop ARDS. However, there was no
statistical record of ARDS incidences in the target setting.

4
1.2.3 Current practice of prone positioning
Although many researchers has proved that prone positioning is effective in improving
oxygenation for up to 70% of patients with ARDS (Albert et al., 1987; Blanch et al., 1997;
Chatte et al., 1997; Lamm et al., 1994; Pelosi, et la., 1998), it is not used as the primary
treatment strategy in the current clinical practice. It is usually considered as a final rescue
maneuver that acts as the last chance to the patients, when the mechanical ventilation setting
reaches the maximum level and fails to maintain good oxygenation. It is comparatively late to
start prone positioning. The initiation, duration and frequency of prone positioning are
prescribed based on clinical judgments of Medical Officers (MOs). The intermittent and short
duration of prone positioning is usually prescribed. However, there is a lack of standardized
guidelines and training of prone positioning for ARDS patients in existing practice. Nurses
are unfamiliar with the technique of prone positioning. With the proposed guideline, it
provides nurses with knowledge of when to start the procedure, recommended duration of
prone positioning, the proper technique of prone positioning and the following consistent
nursing care.
1.3 Research Question, Objectives, Significance
1.3.1 Research question
A clinical question was formulated: How does prone positioning affect the respiratory
status of adult ARDS patients in compared to supine positioning in terms of safety and

5
effectiveness.
1.3.2 Setting objectives
The objectives of this translation nursing research were:
1) To review the evidence on the effectiveness of prone positioning among ARDS
patients in improving oxygenation, secondary to the patients’ survival rate.
2) To appraise, summarize and synthesize the selected research findings.
3) To develop evidence based prone positioning guidelines for adult ARDS patients
in the ICU.
4) To establish an implementation and evaluation plan for the proposed guidelines.
1.3.3 Significance
As mentioned before, the proposed prone positioning is a simple, safe and inexpensive
treatment for ARDS patients. It leads to better oxygenation by enhancing the recruitment of
collapsed alveoli in the dorsal lung regions (Guerin et al., 1999; Lamm et al., 1994; Pappert et
al., 1994). Therefore, an improvement of gaseous exchange is resulted from minimized heart
compression force to the lungs (Albert & Hubmayr, 2000).
Prone positioning facilitates patients with ARDS in ventilating oxygen that is less toxic
and lower in concentration. The pressure of inflation is also reduced, which prevents
ventilator-induced lung injuries and delays multi-organ failure. Hence, the prognosis and
outcomes of patients are greatly improved.

6
In order to carrying out prone positioning, ICU health care professionals’ training is
required particularly in proper and safe positioning of patients, tubes and catheters during
position changes. The role of nurses is essential in performing and monitoring prone
positioning. Familiarization of the etiology of ARDS and recognition of the need for a prompt
and proper prone positioning not only improves the patients’ prognosis, it also helps to
maintain a good nursing standard.
For institution consideration, neither extra material nor manpower is needed to perform
the proposed intervention. Medical expenses would be reduced greatly due to less oxygen
used in prone positioning.

7
Chapter 2
Critical Appraisal
The searching strategies for relevant studies with regard to prone positioning among
ARDS patients in ICU were described in this chapter. The findings and data from the studies
were extracted and summarized in the table of evidence. Critical appraisal and quality
assessments were discussed together with summary and synthesis of available data.
2.1 Search Strategies
2.1.1 Search methodology
A systematic search was performed from 1st June 2013 to 15
th August 2013 with the use
of PubMed (1997-2013), Medline (ProQuest, 1991-2013) and CINAHL (EBSCO host,
1991-2013). Other electronic databases such as the British Nursing Index and Google scholar,
and reference lists of the selected studies were also used in the search. However, the studies
were all duplicated. Hence, only the search results in PubMed, Medline and CINAHL were
presented.
2.1.2Keywords
The keywords were categorized into three groups: population, intervention and
outcome. “ARDS patients”, “acute respiratory distress”, “acute respiratory distress
syndrome”, “acute respiratory failure” and “early acute respiratory distress syndrome” were
searched under population; “prone position”, “prone positioning”, and “prone position
8
ventilation” were searched under intervention; “oxygenation”, “oxygen saturation”, “oxygen
consumption” and “ventilation perfusion ratio” were searched under outcome. All selected
studies were in English language and there was no restriction on the year and types of
publication.
2.1.3 Selection criteria
In order to select the appropriate and relevant articles, a number of selection criteria
were established:
2.1.3.1 The inclusion criteria
Randomized controlled trial (RCT) studies focusing on prone positioning intervention
in compared to supine positioning in the ICU were included. Study participants should be 18
years old or above and diagnosed with ARDS. The participants should be intubated and
received mechanical ventilation. The outcome of the studies should be related to the patient’s
respiratory status.
2.1.3.2 The exclusion criteria
Studies conducted on infants or children were excluded. Outpatient population was
excluded in this searching strategy. Studies without a full text were also excluded.
The details of the searching strategies and results were presented in Appendix 1.
2.1.4 Data extraction
Studies were retrieved according to the inclusion criteria, and then excluded if within
9
the exclusion criteria. Nine studies were extracted from the results. The data from these
studies were summarized in the table of evidence, which was developed by the Scottish
Intercollegiate Guidelines Network (SIGN) (2012). The data were categorized into several
components: author(s) and year of publication, study type, level of evidence, participant
characteristics, intervention(s), comparison/control, outcome measures and effect size. The
table of evidence was presented in Appendix 2.
2.2 Appraisal Strategies
A number of methodologies were described in order to appraise the research evidence
critically and to grade the recommendation based on the level of evidence. With the use of
methodology checklist from the Scottish Intercollegiate Guidelines Network (SIGN, 2012),
the quality of nine selected studies was critiqued. The checklists for critical appraisal of the
nine selected studies were presented in Appendices 3 & 4. The details of grading system
developed by SIGN were shown in Appendix 5.
2.3 Appraisal Results
2.3.1 Searching results
A total of 952 articles were retrieved on 15th
August, 2013 from three databases. After
screening the titles and abstracts, there were 183 potential articles related to the topic. 32
articles were considered as eligible studies with RCT studies screening. Six articles were
excluded, as the studies populations were infants and children. Seven articles were excluded,

10
as the full texts were not available. Three articles were further excluded after the conduction
of observation prospective studies. Three articles were excluded, as the outcome measures of
the studies were not related to the respiratory status of the population. Two articles were
excluded, as prone position was not the only compared intervention in the study. One article
was excluded as it was written in German. Another article was excluded as it was a pilot
study. In the end, nine articles met the selection criteria and were included in this review.
2.3.2 Overview of the selected studies
As discussed above, nine RCT studies in total were selected after systematic search.
The critical appraisal table of the studies was presented in Appendices 3 & 4. In general, all
studies had set an appropriate and focused research question that clearly stated the target
population, the intervention and the outcome measures. The questions of all studies were
similar to research question proposed.
2.3.3 Randomization and concealment allocation
Seven studies carried out good randomization by computer generated system
(Fernandez et al., 2008; Guerin et al., 2004; Guerin et al., 2013; Mancebo et al., 2006) or
centralized telephone system operated on a 24-hours-a day, 7-days-a-week basis and were
based on a permuted-block algorithm (Gattinoni et al., 2001; Taccone et al., 2009;
Voggenreiter et al., 2005). Only two studies mentioned randomization was done without any
method descriptions (Papazian et al., 2005; Robak et al., 2011). All participants were well
11
allocated into certain groups by opaque, sealed envelopes or central allocation.
2.3.4 Blinding
For prone positioning ventilation studies, it was impossible to blind either participants
or health care professionals due to their active involvement in the intervention. Therefore, six
selected studies did not describe any blinding process. Guerin et al. (2004) claimed that
neither data collectors nor outcome assessors were not blinded in their study; only two studies
blinded the investigators (Taccone et al., 2009) and outcome assessors (Guerin et al., 2013).
2.3.5 Baseline characteristics
In terms of the baseline characteristics of the participants between groups, three studies
showed p-value with insignificant results (Fernandez et al., 2008; Mancebo et al., 2006;
Voggenreiter et al., 2005). Taccone et al.’s study (2009) showed the characteristics of the
participants without statistical description. The rest of the five studies described the details of
baseline characteristics without presenting the p-value and claimed no statistical difference
between intervention and control groups. In addition, the primary outcome measures used
were clearly stated in all studies, the only difference between the groups was prone
positioning.
2.3.6 Data collection
The data from the groups were collected in the same way at the same period of time, in
order to minimize performance bias. The outcomes among the selected studies were

12
measured by blood test, chest radiography, ventilator setting, bronchoalveolar lavage (BAL),
physiological variables and biochemical variables etc. They were all standard, valid and
reliable methods.
2.3.7 Power calculation
The method of statistical analysis was stated clearly in all studies. The dropout rate was
low with the range of 0 to 8.7% in most of the studies. Three studies did not describe any
dropouts (Gattinoni et al., 2001; Papazian et al., 2005; Robak et al., 2011). The intention to
treat analysis was eventually carried out in six studies (Gattinoni et al., 2001; Guerin et al.,
2004; Guerin et al., 2013; Mancebo et al., 2006; Taccone et al., 2009; Voggenreiter et al.,
2005). Other studies counted in all participants for intention to treat analysis because none of
them were lost from the follow-up. Four studies were limited by small sample size, the
findings resulted in a low statistical power (Fernandez et al., 2008; Gattinoni et al., 2001;
Mancebo et al., 2006; Voggenreiter et al., 2005).
2.3.8 Application of the studies
Seven studies carried out the research in multi-centres, the exceptions being studies of
Papazian et al. (2005) and Robak et al. (2011). The overall effects of the nine studies were
due to the prone positioning. Since all the selected studies were performed in the ICU, the
study population was similar to that in the target setting without racial consideration. Hence,
the findings of the selected studies were generalized and directly applicable to the targeted

13
patients.
2.3.9 Summary of quality appraisal
According to the SIGN appraisal checklist for RCT, the quality of the selected studies
rated from 1++ to 1- (SIGN, 2012). One was identified as high quality (Guerin et al., 2013),
six studies were identified as acceptable (Fernandez et al., 2008; Gattinoni et al., 2001;
Guerin et al., 2004; Mancebo et al., 2006; Taccone et al., 2009; Voggenreiter et al., 2005) and
two studies were identified as low quality (Papazian et al., 2005; Robak et al., 2011). The
parentage of criteria fulfilled ranged from 58% to 100%. Those studies identified as low
quality contained poor randomization description; no blinding was performed and poor
intention to treat analysis.
2.4 Summary and Synthesis of Findings
Data from the selected studies were categorized and summarized in the table of
evidence (Appendix 2). The synthesis of the findings was discussed below.
2.4.1 Study characteristics
The nine selected studies were all RCTs. The studies were published from 2001 to 2013.
Two studies were conducted in France (Guerin et al., 2004; Papazian et al., 2005). The others
were conducted in Germany, Italy, Switzerland, Spain, Mexico and Austria (Fernandez et al.,
2008; Gattinoni et al., 2001; Guerin et al., 2013; Mancebo et al., 2006; Robak et al.,
2011;Taccone et al., 2009; Voggenreiter et al., 2005). No local study was retrieved. Seven

14
studies were conducted in a multi-centre design with the range of 2 to 30 ICU centres.
(Fernandez et al., 2008; Gattinoni et al., 2001; Guerin et al., 2004; Guerin et al., 2013;
Mancebo et al., 2006; Taccone et al., 2009; Voggenreiter et al., 2005 ). The rest of the studies
were a single centre design conducted in a medical ICU.
2.4.2 Subjects’ characteristics
2184 participants in total enrolled in the nine studies. The number of participants in
each study ranged from 20 (Robak et al., 2011) to 791(Guerin et al., 2004). 1126 participants
in total were randomized to receive prone positioning. Participants in five studies were
diagnosed with ARDS by the definition of the American-European Consensus Conference
(Fernandez et al., 2008; Guerin et al., 2013; Mancebo et al., 2006; Papazian et al., 2005;
Taccone et al., 2009). The other three studies included participants with either ALI or ARDS
(Gattinoni et al., 2001; Voggenreiter et al., 2005; Robak et al., 2011), whereas Voggenreiter et
al.’s study (2005) mainly focused on trauma patients. Besides, the largest study enrolled
participants with acute hypoxemia respiratory failure including 51% ALI or ARDS and 7%
acute cardiogenic pulmonary edema (Guerin et al., 2004). Patients in all studies were
intubated and required mechanical ventilation.
About 40% to 83% were male ranging from 42 to 67 year olds. Simplified Acute
Physiology Score II (SAPS II) of participants was calculated in eight studies, the exception
being Voggenreiter et al. one (2005). The SAPS II mean ranged from 38.3 to 52, where higher

15
scores indicated greater severity of symptoms (SAPS II range: 0-164). Five studies carried
out a Sequential Organ Failure Assessment (SOFA) score to the participants with a mean
score of 6.8 to 12, where higher scores indicated more organ failure (SOFA score range: 0-24)
(Fernandez et al., 2008; Guerin et al., 2013; Papazian et al., 2005; Taccone et al., 2009;
Voggenreiter et al., 2005). In terms of the ARDS causes, 18% to 75% of the participants had
pneumonia, 3% to 23.5% of ARDS participants were associated with sepsis, whereas 3% to
36% participants were triggered by aspiration (Guerin et al., 2013; Gattinoni et al., 2001;
Mancebo et al., 2006; Papazian et al., 2005; Robak et al., 2011; Taccone et al., 2009;
Voggenreiter et al., 2005).
Arterial blood gas measurements were performed in all studies at the time of inclusion,
mean PaO2/ FiO2 ratio of participants ranged from 100 (Guerin et al., 2013) to 155.5
(Fernandez et al., 2008), mean partial pressure of arterial oxygen (PaO2) was 80 mmHg
(Guerin et al., 2013) to 116.5mmHg (Mancebo et al., 2006) and mean partial pressure of
arterial carbon dioxide (PaCO2) ranged from 37 mmHg (Voggenreiter et al., 2005) to 57
mmHg (Robak et al., 2011). When it comes to the initial ventilator settings, the fraction of
inspired oxygen (FiO2) mean ranged from 0.49 (Voggenreiter et al., 2005) to 0.82 (Mancebo
et al., 2006), while the PEEP mean ranged from 7.7 (Guerin et al., 2004) to 13.2 (Fernandez
et al., 2008).

16
2.4.3 Intervention
At the beginning of the intervention, participants in two studies received prone
positioning ventilation within an hour after randomization (Guerin et al., 2013; Mancebo et
al., 2006). Whereas the other studies, the intervention started within two to three days after
diagnosis (Fernandez et al., 2008; Guerin et al., 2004; Taccone et al., 2009). Mancebo et al.
(2006) concluded the time between diagnosis and randomization in prone positioning group
was 0.89 day. The mean time between trauma diagnosis and the beginning of intervention in
Voggenreiter et al.’s study (2005) was the longest. An average of five days were spent to
allocate participants into different group.
Participants received prone positioning ventilation for 7 to 20 hours per day. Two
studies continued prone positioning in a specific period (Papazian et al., 2005; Robak et al.,
2011), whereas the others continued the intervention until clinical improvement was reached.
The intervention period ranged from a day (Papazian et al., 2005; Robak et al., 2011) to ten
days (Gattinoni et al., 2001; Mancebo et al., 2006). One study combined upright and prone
positions to compare with supine position (Robak et al., 2011).
2.4.4 Control/ Comparison
In the comparison group, participants remained supine positioning ventilation in most
of the studies. Two studies assigned participants in comparison group to stay in semi
recumbent position (Guerin et al., 2004; Guerin et al., 2013). The use of high-frequency
17
oscillation was considered as an additional therapy that was applied to all participants
(Papazian et al., 2005). Lung protective ventilation was applied except in the studies of
Gattinoni et al. (2001) and Guerin et al. (2004). Crossover was strictly prohibited in two
studies (Robak et al., 2011; Voggenreiter et al., 2005), while two other studies allowed
crossover (Gattinoni et al., 2001; Mancebo et al., 2006), the rest allowed crossover only as a
rescue measure.
2.4.5 Outcome measures and effect size
2.4.5.1 Participants’ ventilation
Eight out of nine selected studies measured the PaO2/FiO2 ratio of the participants.
There was a significant increase in PaO2/FiO2 ratio in prone positioning among these eight
studies. These increased findings were +75 at Day 3(p=0.009) (Fernandez et al., 2008); +18.4
(p= 0.02) (Gattinoni et al., 2001); p<0.001 (Guerin et al., 2004); +15 at Day 3 (p<0.05) and
+22 at Day 5 (p< 0.001) (Guerin et al., 2013); +39 (p<0.005) (Mancebo et al., 2006); +79
(p<0.0001) and +101 (p<0.001) (Papazian et al., 2005); +56 (p<0.05) and +55 (p<0.001)
(Robak et al., 2011) and +44.1 at Day 4 (p=0.03) (Voggenreiter et al., 2005). Study of
Fernandez et al. (2008) showed the largest increase of the PaO2/FiO2 ratio, while Robak et
al.‘s study (2011) showed the shortest period (two hours after implementation) with a
significant increase. Besides, three studies have found a significant reduction of PEEP used
among the intervention group. This reduction showed statistical significance at Day 3 (Guerin

18
et al., 2013) and Day 4 (Mancebo et al., 2006; Voggenreiter et al., 2005) with p-value less
than 0.05, equal to 0.048 and 0.009 respectively. In addition, Mancebo et al. (2006) found
there was a drop with 2 cmH2O of PEEP in intervention group. When it comes to FiO2 used,
two studies showed a significant decrease in prone positioning (Guerin et al., 2013; Mancebo
et al., 2006). This reduction protected participants from oxygen toxicity. With the
improvement of PaO2/FiO2 ratio, reduction of PEEP and FiO2 used, the number of
participants in prone position who had extubated successfully at Day 90 was significantly
higher than those in supine position (p<0.001) (Guerin et al., 2013).
2.4.5.2 Incidence of pneumonia
Only two studies measured the incidence of pneumonia during the implementation.
Voggenreiter et al. (2005) found that the prevalence of pneumonia in prone position group
was significantly lower than those in supine position by 27% (p=0.048). Another study
showed a significant reduction of 3.5 % in ventilator-acquired pneumonia (VAP) in
intervention group (p= 0.045) (Guerin et al., 2004).
2.4.5.3 Rate of mortality
Seven studies measured mortality rate of the participants as one of the outcomes.
However, the measurement periods of mortality were different. Gattinoni et al. (2001)
concluded a 3.9% reduction at Day 10 in prone positioning group (p=0.65). There was a 15%
decrease (p=0.3) in 60-day mortality in prone position in Fernandez et al.’s study (2008). Two

19
studies measured 28-day and 90-day mortality. These findings in prone positioning were
-0.9% (p=0.77) and -1.1% (p=0.74) respectively (Guerin et al., 2004), while -16.8% (p<0.001)
and -17.4% (p<0.001) respectively in Guerin et al.’s study (2013). Mancebo et al.’s study in
2006 showed the ICU mortality of participants in prone positioning had a 15% absolute and
25% relative decrease compared with those ventilated supine (p=0.12), they also measured
the hospital mortality with 12% reduction in prone positioning (p= 0.27). The mortality
decreased 11 % in intervention group with p-value equal to 0.27 (Voggenreiter et al., 2005).
Taccone et al. (2009) noted 28-day and 180-day mortality of moderate ARDS participants in
intervention group were +3% (p=0.62) and -1.3% (p=0.85) respectively, while for severe
ARDS participants, the rates were -8.3% (p=0.631) and -10.5% (p=0.19) respectively. This
showed that the mortality of severe ARDS participants had a greater decrease than those
suffered from moderate ARDS. Although the mortality of ARDS in prone positioning reduced
in most of the studies, the statistical significance did not reach. Only the study of Guerin et al.
(2013) presented a significant reduction in 28-day and 90-day mortalities.
2.4.5.4 Adverse events
Main complications related to prone positioning included pressure sore formation,
device displacement such as endotracheal tube and venous access, hemodynamic instability,
arrhythmia and edema. Four studies concluded the occurrence of the adverse events resulted
from prone positioning was insignificant (Gattinoni et al., 2001; Guerin et al., 2013; Mancebo

20
et al., 2006; Voggenreiter et al., 2005). Gattinoni et al. (2001) found there was a statistical
insignificance in the complications except the occurrence of pressure sore in prone
positioning. It was a 0.8 increase in the number of new or worsening pressure sore with
p-value equal to 0.004. Taccone et al. (2009) claimed that the incidence of the adverse events
such as the increased of sedation and paralyzing drugs, hemodynamic instability and
displacement of devices were significantly higher in intervention group (+18.2%, p<0.001).
Finally, Guerin et al. (2004) found prone positioning significantly increased the incidence of
selective intubation, endotracheal tube obstruction and pressure sores with p=0.01, p=0.002
and p=0.005 respectively.
2.4.6 Data synthesis and implication
From the data mentioned above, prone positioning benefited ARDS participants in
oxygenation improvement, decreases in pneumonia rate and possibly mortality rate. It was
concluded that the disease severity of the participants varied in the early studies (Gattinoni et
al., 2001; Guerin et al., 2004; Voggenreiter et al., 2005). They recruited patients with acute
respiratory failure including both ALI and ARDS. The duration of prone positioning
performed was relatively shorter. Less than 12 hours/day were spent for the intervention
intermittently and did not use lung protective ventilation.
2.4.6.1 Participants’ ventilation
There was a trend to perform prone positioning at early stage that within 48 hours after
21
diagnosis in recent studies (Fernandez et al., 2008; Guerin et al., 2013; Mancebo et al., 2006).
The most recent studies only recruited patients with similar severity of ARDS. Prolonged
prone positioning was performed more than 17 hours/day. Patients were only turned to supine
position for a few hours to carry out daily nursing care or medical treatment. Prone
positioning was continued every day until significant improvement in oxygenation. A
significant clinical improvement was found within three days of implementation period
(Fernandez et al., 2008). Besides, patients ventilated with recent protective lung ventilation
prevented them from ventilator-induced lung injury.
2.4.6.2 Incidence of pneumonia
Since two studies concluded the incidence of pneumonia showed a significant drop
with prone position (Guerin et al., 2004; Voggenreiter et al., 2005), it might be related to the
drainage effect of secretions when patients remained at prone position, aspirations could be
prevented.
2.4.6.3 Rate of mortality
When it comes to the effect in mortality, the findings of the studies were inconclusive.
Although there was a decrease in mortality in prone position, the statistical significance did
not meet. It may be due to a small sample size in four studies (Fernandez et al., 2008;
Gattinoni et al., 2001; Mancebo et al., 2006; Voggenreiter et al., 2005), in which two studies
were stopped prematurely due to medical contraindications of prone positioning, shortened

22
period of enrollment (Fernandez et al., 2008) and unwillingness of caregivers (Mancebo et
al., 2006). The large spectrum of disease severity among the selected patients resulted in the
unclear influence of mortality (Gattinoni et al., 2001; Guerin et al., 2004; Voggenreiter et al.,
2005). Besides, the cause of ARDS mortality was mainly related to multi-organ failure rather
than respiratory failure alone. Taccone et al. (2009) allowed a 72-hour enrollment period that
might explain insignificant result. It violated the principle of early intervention, led to more
effective outcome (Mancebo et al., 2006). At last, Guerin et al. (2013) carried out the study
with sufficient sample of ARDS patients and early implemented prolonged prone positioning
with lung protective ventilation, led a significant decrease of mortality.
2.4.6.4 Adverse events
For the adverse events of the prone positioning, there were insignificant results among
most of the studies. Gattinoni et al. (2001) found incidence of pressure sore significantly
increased in prone positioning, it was explained by late enrollment of the ARDS patients that
nearly 25% of them had pressure sore at entry and a lack of protective measures done. The
use of cushions or protective pads in recent studies reduced the incidence of prevent pressure
sores effectively (Mancebo et al., 2006; Robak et al., 2011; Guerin et al., 2013). The increase
of selective intubation, endotracheal tube obstruction and devices displacement might relate
to the unfamiliar technique turning procedure (Guerin et al., 2004). In fact, the adverse events
of prone positioning were reversible and preventable; the use of appropriate tuning guidelines

23
and nursing care protocol could minimize the occurrence of the complications.
In conclusion, prone positioning is a simple, safe and cheap supportive treatment. A
number of benefits for ARDS patients showed in oxygenation improvement, pneumonia and
mortality reductions after the review of studies. It should be implemented early within 48
hours after diagnosis (Fernandez et al., 2008; Guerin et al., 2013; Mancebo et al., 2006). The
duration of prone positioning should be prolonged at least 17 hours per day (Fernandez et al.,
2008; Guerin et al., 2013; Mancebo et al., 2006; Taccone et al., 2009) and it should continue
the treatment every day until clinical improvement noted (Guerin et al., 2013). Besides, lung
protective ventilation should be performed. Appropriate turning guidelines and nursing care
protocol can prevent several complications of prone positioning.

24
Chapter 3
Implementation Potential
In previous chapters, prone positioning has been proved as an effective measure of
oxygenation improvement for the patients with ARDS. With the consideration of the potential
benefits, the innovation will be transferred to ICU of a public hospital in Hong Kong. The
target audience and setting, transferability, feasibility and cost-benefit ratio of the innovation
will be considered before actual transfer.
3.1 Transferability of the Innovation
3.1.1 Target setting/ audience
The evidence-based guideline of prone positioning will be proposed in the ICU of a
public hospital. A total of eight beds are served and the average bed occupancy rate is about
80%. The target setting provides services to those adult patients with different types of
critically ill diagnosis including medical illness (30%), surgical illness (36%), orthopedic
illness (12%) or ear, nose and throat illness (22%) based on the statistics from the target
setting in 2012.
3.1.1.1 Fitness of the setting
None of the selected studies was conducted in Hong Kong, which may have racial
barrier when transferring the innovation to Hong Kong audience. However, all selected
studies were carried out in ICU and the patients in the studies suffered from ARDS. The

25
clinical settings in the selected studies are similar to the target setting. The transferability of
prone positioning is still high.
3.1.1.2 Characteristics of target population
The target audience will be the adult patients who receive mechanical ventilation and
develop ARDS after ICU admission. The eligible patients in the selected studies are similar
characteristics to the target audience in terms of diagnosis and treatment of the disease.
Patients in most of the selected studies mainly have pneumonia and sepsis, which are the
common diagnosis in the target setting (Gattinoni et al., 2001; Guerin et al., 2013; Mancebo
et al., 2006; Papazian et al., 2005; Robak et al., 2011; Taccone et al., 2009; Voggenreiter et al.,
2005). There is no geographic barrier in selecting appropriate clinical setting and audience.
Hence, the innovation is suitable for the target setting.
3.1.2 Philosophy of care
‘Helping people stay healthy’ is the mission of Hospital Authority (Hospital Authority,
2013). As health care professionals, we have an important responsibility of not only giving
life-saving treatment to our patients, but also assisting them to regain their health and stay
healthy. The service goal of target setting is to provide patients with the safe, high-quality and
evidence-based services for their best possible outcomes. The philosophy of innovation is to
improve ventilation when patients have life-threatening ARDS. It further reduces the
mortality rate by 17% regarding to Guerin et al.’s study (2013). Using the evidence-based

26
guideline of prone positioning in the target setting, the prognosis among patients will be
improved. Therefore, the philosophy of the innovation achieves the missions of both Hospital
Authority and the target setting.
3.1.3 Benefit sufficient patients
The innovation will benefit patients who have ARDS and require mechanical
ventilation. Based on the annual admission rate of the target setting in 2012, around 400
patients admitted to the target setting and about 40% of them were diagnosed with pneumonia
or sepsis. However, not all of these patients reached the criteria of the proposed innovation. It
is estimated that 100 of patients will benefit from the proposed innovation every year. The
number of target audience is increasing due to the increased severity of pneumonia that is
associated with Human Swine Influenza or Avian Influenza (H7N9) these years (WHO,
2013).
3.1.4 Time frame for implementation and evaluation
A pilot study of the innovation will be commenced in the target setting. The duration
will last for six months for implementation and evaluation. Prone positioning will be
implemented on the day of ARDS diagnosis and will be continued until patients’ ventilation
is improved. It will last at least 4 days for every eligible patient (Guerin et al., 2013) and the
evaluation will be conducted every day in order to find out any barrier of the innovation. The
mortality rate of the target audience will be evaluated one month after the implementation

27
(Guerin et al., 2004; Taccone et al., 2009; Guerin et al., 2013).
3.2 Feasibility of Implementation
3.2.1 Freedom to implement and terminate the innovation
Primary nursing practice has been promoted for more than six years in the target setting.
Each primary nurse is responsible for one to two patients. Hence, nurses have autonomy to
make decision by following the evidence-based guideline together with their clinical
judgment. They will have the freedom to implement the innovation after gaining the approval
from the Department Operation Manager (DOM). If the adverse events occur, nurses will
notice, report and terminate the innovation immediately.
3.2.2 Interference with current staff practice
As prone positioning is a new innovation, it requires more manpower to implement
comparing with the standard turning procedure especially for the patients who have different
central venous accesses, tracheal tube and monitoring instruments. During each turning, at
least five staffs are involved and it usually takes five to ten minutes for the process (De Jong
et al., 2013; Mancebo et al., 2006). Since the total bed number is small, there are about ten
health care providers including nurses and Patient Care Assistants (PCAs) are on duty during
day shift, nearly 50% of them will assist for prone positioning and it will create minor
interference to the current setting. As the procedure is not time-consuming, it should be
implemented in the morning duty in order to ensure sufficient manpower and minimize the

28
interference made.
3.2.3 Organization climate
Evidence-based practice (EBP) of nursing practice is positively supported within the
target setting. Under the leadership of a DOM, Nurse Consultant (NC) and Advanced Practice
Nurses (APNs) play an important role in project co-ordination and implementation. In order
to implement this innovation, monthly journal club and weekly nursing grand round are the
prefect communication channels between NC, APNs and nurses to share updated research
findings and nursing care. Knowledge of the new innovation will be reinforced during the
group sharing.
Besides, nurses can express their concerns and barriers that they encounter in ward
meeting. Their feedback enhances the evaluation and modification of the innovation.
3.2.4 Collaboration among departments
As the innovation is being implemented, the collaboration among the health care
providers within or outside the department is extremely crucial. The proposed innovation will
be introduced to MOs first who are responsible for making a precise diagnosis of ARDS,
holding patient’s head during the proning process and further weaning the ventilator setting.
If the patient does not coordinate with the mechanical ventilation after prone positioning,
nurses will discuss with MOs in order to seek for sedation or paralyzing agents to the
patients.

29
The innovation needs to gain collaboration with laboratory and x-ray department in
order to evaluate the outcomes. For example, regular blood taking, culture testing from
endotracheal aspirates and chest x-ray will show any oxygenation improvement or presence
of chest infection. The laboratory and x-ray department are unlikely oppose the innovation
since there is no extra investigation which interferes their daily function.
3.2.5 Skills training
Staff training will be conducted before the guideline implementation. After the research
findings sharing in journal club and nursing grand round, a one-hour workshop will be held to
reinforce the specific technique of prone positioning. PCAs will be instructed to be the
assistants in the proning process. Nurses will supervise and ensure PCAs to stand at correct
position. Nurses will also assist in proper positioning to ensure patient’s safety such as
securing all life-saving materials throughout the process.
Besides, nurses will be taught about the monitoring and adverse events of prone
positioning. Shift assessment of the patient’s skin integrity will be done to elevate any
formation of pressure sore. Poor nurses’ turning technique will be one of the barriers
concerned. Department audit team in order to review the nursing practice and maintain the
standard of care will conduct an audit of prone positioning.
3.2.6 Equipment for implementation and evaluation
Comparing with the standard turning position, there will be no extra pillow used in

30
prone positioning. Three pillows will be placed under the shoulders, the pelvis and shins in
order to reduce the restriction of the chest and abdominal movements (Guerin et al., 2004;
Guerin et al., 2013; Mancebo et al., 2006; Robak et al., 2011). Besides, a manufactured prone
headrest will be purchased in order to protect and support patient’s head and face. Since this
device is reusable, two prone headrests will be required in the target setting.
The clinical measuring tools for outcome evaluation are available. For the
measurement of oxygenation and chest infection, continuous patient’s pulse oximetry
monitoring, arterial blood gas analysis, patient’s clinical signs, ventilator setting and chest
radiography should be recorded routinely (Fernandez et al., 2008; Gattinoni et al., 2001;
Guerin et al., 2004; Guerin et al., 2013; Mancebo et al., 2006; Papazian et al., 2005; Robak et
al., 2011; Taccone et al., 2009; Voggenreiter et al., 2005). Daily blood test for clotting profile,
complete blood count, renal and liver function helps to monitor patient’s non-pulmonary
system failure (Gattinoni et al., 2001; Voggenreiter et al., 2005). Adverse events including
presence, site and severity of pressure sore, hemodynamic instability, unplanned extubation
or blockage of endotracheal tube should also be documented. Finally, the duration and
number of prone positioning and the mortality rate should be recorded for the efficacy of the
innovation.
31
3.3 Cost-Benefit Ratio of the Innovation
3.3.1 Patient’s potential risks and benefits
Although prone positioning is cost-effective, patients may encounter adverse events
such as facial edema and pressure sore formation. Also, devices such as central venous access
and tracheal tube may be displaced during the turning process. Since the selected studies
showed no significant results in adverse events, using protective pads and strengthening
nursing observation and their turning technique can solve them. Once patients develop
hemodynamic instability or arrhythmia, the innovation should be terminated.
Prone positioning improves patient’s oxygenation, so the ventilator setting can be
further weaned. The use of oxygen becomes less that prevents the occurrence of barotrauma
as well. The rate of VAP can be reduced by the drainage effect of secretions. Finally, the
mortality rate of ARDS patients can be decreased.
3.3.2 Potential risks and benefits towards staff and the setting
Prone positioning requires teamwork from different parties including MOs, nurses, and
PCAs. Team building will be encouraged through the cooperation. The workload of nurses
will not become heavier because the pressure sore observation and vital signs monitoring are
the same as current practice. Nurses will gain new knowledge and proning technique as well.
Staff development, morale and satisfaction will be enhanced if the innovation succeeds to
save patients’ lives.

32
3.3.3 Potential risks of maintaining current practices
The current treatment of ARDS only depends on the clinical judgment of MOs, patients
keep supine position and are turned laterally every two hours, and there is no formal
guideline of prone positioning for nurses and MOs. As a result, patients with ARDS will
ventilate difficultly, the ventilator setting and the chance of developing barotrauma will be
increased. The prognosis of the patients cannot be improved if the current practice is
maintained.
3.3.4 Potential material and non- material costs for implementation
As mentioned above, prone positioning is simple and the equipment needed is minimal.
Most equipment including pillows, routine laboratory tests and chest radiograph service are
available in the target setting. Only two extra manufactured prone headrests will be purchased
and no addition maintenance cost will be needed. Training workshop reduces nurses’ stress
related to unfamiliar tuning technique. However, extra time for nurse training is required. The
training handout will be uploaded to the department website. No extra printing cost will be
spent except a new guideline will be printed out and kept as reference in the target setting.
The cost in the long run prone positioning not only is minimal, it also saves much cost of the
outcome. The details of cost calculation are attached in Appendix 6.
In conclusion, prone positioning can be implemented in the target setting with limited
barriers after concerning the transferability, feasibility and cost-benefit ratio.

33
Chapter 4
Developing an Evidence Based Practice Guideline
An evidence-based guideline of prone positioning is established according to the
evidence from the selected studies in previous chapters.
4.1 Title of the Evidence-Based Practice Guideline
Evidence based guideline of prone positioning for adult patients with acute respiratory
distress syndrome in intensive care unit.
4.2 Aim of the Guideline
The aim of the innovation is to facilitate ventilation among ARDS patients by
increasing their oxygenation. It further decreases the prevalence of VAP and improves the
survival rate of patients.
4.3 Objectives of the Guideline
The objectives of this guideline are:
- To formulate clinical instructions for prone positioning based on the best evidence
based practice research,
- To strengthen nurses’ awareness and competence in performing prone positioning,
- To enhance nurses’ knowledge in prone positioning in evidence based approach.
4.4 Target Population
Patients who are 18 years old or above and suffer from ARDS.

34
4.5 Target Users of the Guideline
All nurses are working in Intensive Care Unit.
4.6 Grading Scheme of the Guideline
Regarding to “SIGN 50: a guideline developer’s handbook” (SIGN, 2012), the levels of
evidence are rated from 1++ to 4 and the grades of recommendation are presented as Grade A
to Grade D (Appendix 5).
4.7 Practice Recommendations
A number of recommendations for prone positioning are concluded based on the
evidences from nine selected studies. They are presented into four categories: (1) Assessment;
(2) Initiation and implementation of prone positioning; (3) Monitoring and evaluation and (4)
Termination (Appendix 7).
4.7.1 Assessment
Recommendation 1.1 (Grade A)
Patients who have severe hypoxemia with PaO2/FiO2 ratio < 150mmHg, FiO2 ≥ 0.6
and PEEP ≥ 5cm of water and require MV are benefit from prone positioning.
Recommendation 1.2 (Grade A)
Patients are contraindicated for prone positioning if they have cerebral edema with
elevated intracranial pressure >30mmHg and cerebral perfusion pressure <60mmHg, unstable
fractures of pelvic, femur or spine, severe hemodynamic instability, pregnancy and elevated

35
intra-abdominal pressure.
4.7.2 Initiation and implementation of prone positioning
Recommendation 2.1 (Grade A)
Prone positioning should be initiated within 36 hours upon ARDS diagnosis.
Recommendation 2.2 (Grade A)
The duration of prone positioning should be at least 17hours/day.
Recommendation 2.3 (Grade A)
Prone positioning should be continued at least 4 days.
Recommendation 2.4 (Grade A)
Protective lung ventilation should be applied during prone positioning.
Recommendation 2.5 (Grade A)
Protective pads should support patients’ forehead, chest, knees and iliac crests during
prone positioning.
Recommendation 2.6 (Grade A)
Patients’ heads and necks should be turned laterally every two hours during prone
positioning.
4.7.3 Monitoring and evaluation
Recommendation 3.1 (Grade A)
Physiological variables of patients should be continuously monitored and documented

36
just before prone positioning, 1 hour after prone positioning, just before turning back to
supine position and 4 hours later.
Recommendation 3.2 (Grade A)
Nurse should monitor and record the presence of VAP.
Recommendation 3.3 (Grade A)
Patients’ skin integrity should be observed every shift.
4.7.4 Termination
Recommendation 4.1 (Grade A)
Prone positioning should be terminated if patients’ oxygenation improves or
deteriorates and major complication occurs.

37
Chapter 5
Implementation Plan
In previous chapters, an evidence-based guideline of prone positioning for adult
patients with ARDS is developed. A well-designed implementation schedule which includes a
clear communication plan with all stakeholders, staff training and a pilot study will be carried
out in the target ICU of a local public hospital in order to examine the effectiveness of
guideline.
5.1 Communication Plan with Potential Stakeholders
5.1.1 Identification of the stakeholders
A good communication among the stakeholders is crucial to the success of the
innovation implementation. For the prone positioning guideline, the potential stakeholders are
involved the administrators, managerial staffs, frontline staffs, supporting groups, patients
with ARDS and their relatives.
The administrators include Chief of Service (COS), DOM and Ward Manager (WM)
who are very important in approving the pilot study and the implementation of the proposed
guideline. They also provide financial support and other resources for the implementation.
The managerial staffs include Associated Consultants (ACs), NC and APNs who are
responsible for promoting evidence based practice in the target setting, monitoring and
managing the outcomes of the proposed guideline.
38
MOs, nurses and PCAs are the frontline staffs who are responsible for the patients in
prone position. MOs and nurses are responsible for the initiation and termination of the
innovation. Nurses also provide ongoing assessment and monitoring for the patients. PCAs
need to assist the nurses during proning procedure.
Supporting groups involve the staffs from laboratory and x-ray department. They are
required to provide efficient and precise laboratory tests and chest radiograph for the outcome
measurement.
5.1.2 The process of communication plan and implementation strategies
As mentioned above, a specific communication strategy will be developed to
appropriate stakeholders to gain their support. A core group of the proposed innovation will
be formed which consists of the proposer, one AC, one APN and two nurses from the target
setting. It will spend about two weeks to invite certain staffs to become core members. The
proposer will introduce the proposed guideline to the team via informal discussion.
Information regarding the affirming needs and significance of the change in current practice
and the evidence of prone positioning from the literature will be presented. When the core
group is formed, core members will approach different parties separately to promote the
innovation.
5.1.2.1 Initiating the proposed innovation
In order to obtain the approval and financial support in the target setting, a formal
39
meeting with the administrators will be held by core members. During the meeting, core
members will present the current practice, the changing needs and the significance of prone
positioning through PowerPoint and written proposal. The new prone positioning guideline
together with the current evidences will be introduced as well to provide a clear view of the
benefits for both patients and clinical setting. The details of the proposed innovation such as
the implementation potential, potential barriers, required resources and manpower will be
discussed. Several meetings will be held to receive their opinions, answer and further explain
their concerns. The estimated time of communication is about a month until the approval
gained.
5.1.2.2 Guiding the proposed innovation
After receiving the approval and resources, core members will promote the proposed
guideline to the other stakeholders in the next one and a half months.
The frontline staffs play an important role to implement the proposed guideline. For
instance, ACs and MOs are required to interpret the x-ray film, provide a precise diagnosis
for ARDS patient and treatments such as ventilator setting adjustment and medication
prescription. Information about the significance and benefits of prone positioning will be
promoted in a one-hour conference. Besides, the details of the guideline will be sent to their
internal e-mail accounts for reference.
For nurses’ training, a one-hour journal club will be held to explain the importance of

40
prone positioning by briefly sharing the research findings. Core members will introduce the
new evidence-based guideline and emphasize the nursing care such as continuous monitoring
and adverse events assessment of prone positioning. The PowerPoint presented in the journal
club will be posted on department website in the hospital intranet. A ‘read and sign’ approach
will be conducted to confirm all nurses recognize the new innovation before implementation
and the copy of the guideline will be kept in every bedside for reference.
As a special technique is required in proning procedure, a one-hour intensive workshop
will be organized every week to reinforce staffs’ skills. The workshop consists of hands-on
practice and return demonstration. Ten nurses will be trained each session and three sessions
will be needed to train up all nurses in the target department. During the training workshop,
the aims and evidence of proposed guideline will be emphasized again to facilitate their
compliance. Using ‘train-the-trainers’ method, all APNs and senior nurses will participate in
the workshop first and become the role models in the future. A guideline with photos about
the proning technique will be kept in the prone positioning folder.
PCAs and other supporting groups will bear comparatively less responsibilities in
implementation. PCAs will follow nurses’ instructions to perform proper proning preparation
and procedure. Since there will be no extra laboratory test nor x-ray for the innovation
evaluation, the guideline will be sent to the department heads via internal e-mail. Patients
recruited in the innovation are remained unconscious; a clear poster will be posted on the
41
notice board to promote the change to their relatives (Appendix 8).
5.2.1.3 Sustaining the proposed innovation
To ensure the success of the change, core members together with NC and all APNs will
provide with ongoing supports and knowledge, which can help to motivate the frontline staffs
to maintain the practice. APNs will monitor nurses’ compliance with the guideline and
patients’ outcomes through daily assessment. Audit team of the department will carry out
nursing audit every three months to evaluate nurses’ skills and care for patients in prone
position. Frontline staffs will give their feedbacks and express their difficulties in the
workshop, monthly ward meeting and weekly nursing grand round. After collecting their
feedbacks, core members will modify the guideline with updated evidence continuously.
5.2 Pilot Study to Try Out the Guideline
5.2.1 The objectives of pilot study
A six-month pilot study will be carried out in the target ICU before full implementation
for the following objectives: (1) to examine the feasibility of prone positioning for ARDS
patients in target ICU; (2) to collect data on outcome measures; (3) to monitor the
acceptability and the compliance with the proposed guideline among the frontline staffs and
patients; (4) to identify potential problems and difficulties during implementation; (5) to
revise the guideline including logistics and operational cost.
Besides, ethical approval is gained from the Hospital Research Ethic Committee before

42
its start. Nurses will explain the information regarding the pilot study to the patients and their
relatives, and obtain their informed consents at the same time.
5.2.2 Patient recruitment of pilot study
Patient recruitment criteria in the pilot study will be the same as the proposed guideline
mentioned and convenient sampling will be used. It is estimated that 15 eligible patients will
be recruited. APNs and core members will screen the eligible patients and seek ACs’ approval
to proceed to the innovation. They will also review the logistics of patient recruitment in
order to identify any difficulty and modify the strategies. With their experiences, nurses will
be trained to be competent in patient selection.
5.2.3 The new evidence based guideline of prone positioning
In the pilot study, nurses will provide prone positioning to the eligible patients. Nurses
with assistance of core members will do continuous assessment and monitoring of the
patients. Besides, they will document ventilator settings, laboratory results and any adverse
events, which show compliance of patients objectively.
5.2.4 Data collection for patient, staff and system outcomes
Oxygenation, which measures PaO2/FiO2 ratio, is considered as primary outcome.
Data including the laboratory results, ventilator settings and respiratory status of patients will
be recorded by nurses. Since patients are unconscious during prone positioning, their
compliance with the innovation will be reflected by objective adverse events such as
43
worsening ventilation. Patient progress review will be done by core members daily to
evaluate the outcomes.
To ensure sufficient knowledge and skills of nurses before the pilot study, those who
participated in the journal club and training workshops should complete the questionnaires at
the end of each session respectively (Appendices 9 & 10). Core members will receive their
comments and revise the training method in a short period. The compliance of nurses will be
assessed through their daily assessment and documentation. Besides, they will complete a
questionnaire, which evaluates their acceptance and job satisfaction at the end of the pilot
study (Appendix 11). Their concerns and difficulties encountered are very useful in revising
the guideline.
For the system outcome, the cost and material used in the pilot study will be estimated
for the budget plan of actual implementation.
5.2.5 Evaluation of pilot study
After collecting and analyzing the data from patients’ objective parameters,
questionnaires and feedbacks, the preliminary outcomes will be evaluated. The weakness and
limitations will be identified and discussed in the formal meeting among the core group. Core
members will review the proposed innovation and share the successful cases to the
stakeholders before the actual implementation.

44
Chapter 6
Evaluation Plan
The evaluation plan is established to assess the effectiveness and feasibility of
proposed guideline in the target ICU. Outcomes of the innovation will be identified and
evaluated after the full implementation. The results will be presented to the stakeholders in
order to determine whether the change is worthwhile to continue in the future.
6.1 Identify Outcomes to be Achieved
The outcomes of the proposed guideline consist of patient outcomes, healthcare
provider outcomes and system outcomes.
6.1.1 Patient outcomes
Clinical benefits of the innovation are primary focus of the patient outcomes. The
purpose of prone positioning is to enhance oxygenation for patients who suffered from ARDS.
Hence, the primary outcome is oxygenation. As previous chapter mentioned, PaO2/FiO2 ratio
was measured in the nine reviewed studies. When PaO2/FiO2 ratio increases significantly,
the guideline is considered as effective. PaO2/FiO2 ratio recorded during the implementation
will compare with the baseline information.
The secondary outcomes are the prevalence of VAP, the mortality rate and the presence
of adverse events.

45
6.1.2 Healthcare provider outcomes
In order to initiate and sustain the change successfully, the cooperation among the MOs,
nurses and PCAs is crucial. Since healthcare providers especially nurses are required certain
knowledge and specific technique to perform prone positioning, their implementation skills
and knowledge will be assessed. Besides, their job satisfaction, compliance with the guideline
and level of competence to implement the innovation will also be measured.
6.1.3 System outcomes
System outcome is an essential consideration for administrators whether approve for
the continuity of the innovation or not. For prone positioning guideline, cost-effectiveness
and manpower will be evaluated as well. The expenditures of the new materials, such as
manufactured prone headrests will be compared with the material used in usual practice.
Besides, the cost spent on holding the journal club or training workshop, paperwork such as
questionnaires and audit forms, and oxygen used in one patient will be counted. The
difference will be analyzed to show cost effectiveness.
6.2 Nature and Number of Clients to be Involved
The proposed innovation involves the ICU patients and frontline staffs. Patients who
are admitted to the ICU are under MV within 36 hours and suffer from ARDS with
PaO2/FiO2 ratio <150mmHg, FiO2 ≥ 0.6 and PEEP ≥5cm water. Those who have cerebral
edema, unstable fracture of pelvic, femur or spine, severe hemodynamic instability,

46
pregnancy or elevated intra-abdominal pressure are excluded due to patient safety and ethical
consideration.
Convenient sampling will be performed in patient recruitment. The sample size is
based on the primary outcome. Three reviewed studies were chosen for the calculation
(Fernandez et al., 2008; Robak et al., 2011; Voggenreiter et al., 2005). These studies showed
an increase of PiO2/FiO2 between 39mmHg and 75mmHg. Hence, an average 50mmHg
increase of PiO2/FiO2 is applied in the online sample size calculator (Lenth, 2006-9). Paired
t-test is performed. By taking a power of 80% at a significance level of 0.05, the estimated
patient number is 32.
For the frontline staffs, there are 23 registered nurses, seven APNs, three ACs, three
MOs and five PCAs in the target ICU are evaluated.
6.3 Data Collection, Time and Frequency of Taking Measurements
Patients’ demographic data, the cause of ARDS, ventilator settings, time from
intubation will be recorded when they are eligible to receive prone positioning. The results of
arterial blood gas (ABG), SOFA score (Vincent et al., 1996), SAPS II (Le Gall et al., 1993)
and time at first prone session started will be documented as baseline information. When the
innovation is started, patients’ physiological data including ABG, pulse oximetry and
ventilator setting are measured routinely before prone positioning, one hour after prone
positioning, before turning back to supine position and four hours later.

47
Chest radiography, blood for total white cell count (WCC) and tracheal aspirates for
microbiology test are taken routinely under MOs’ clinical judgment for diagnosis of VAP. The
positive findings are recorded. Whenever there is any adverse event, the reason of termination,
the duration and number of prone session should be documented as well. The mortality rate
will be monitored 28 days after prone positioning according to Guerin et al.’s study (2013).
These data are obtained from patient’s progress documentation.
Questionnaires using Five-Level Likert Scale design (Likert, 1932) are used to evaluate
healthcare provider outcomes. Healthcare staffs should complete the questionnaires before
and after the journal club and training workshops to evaluate their skills and knowledge
(Appendices 9 & 10). Besides, another set of questionnaire (Appendix 11) is completed every
three months so that the job satisfaction and the level of competence are assessed. The
department audit team evaluates the compliance of nurses to the proposed guideline every
three months. Healthcare staffs are allowed to express their concerns and difficulties directly
in weekly nursing grand round and monthly ward meeting.
At the end of the implementation period, core members can calculate the
cost-effectiveness and manpower. The cost will be reviewed annually, and a final report with
expenditures analysis will be submitted to the administrators.

48
6.4 Data Analysis
Data analysis of outcomes will be carried out by the Statistical Package for Social
Science (SPSS). Descriptive statistics will be used to summarize the characteristics of
patients, which include demographic data, the cause of ARDS, ventilator settings, time from
intubation, SOFA score and SAPS II.
A two-tailed paired t-test will be used to analyze the change of oxygenation and
adverse events at pre and post prone positioning. The results will be presented as mean±
standard deviation. Statistical significance will be set as p<0.05.The prevalence of VAP and
mortality rate will be analyzed by performing a two-tailed z-test for one proportion. The data
will be compared to the baseline statistics.
For healthcare provider outcomes analysis, quantitative data from the questionnaires
will be analyzed by paired t-test and presented as mean±standard deviation. The main idea of
qualitative data obtained from the questionnaires and the meetings will be grouped into key
theme. Different views and experiences will be identified in each key theme and their
structural meanings will be explored.
6.5 Criteria of an Effective the Guideline
The guideline of prone positioning is considered as effective if the primary outcome is
achieved. In the review studies, PaO2/FiO2 ratio was reported to significantly increase by
21mmHg to 75mmHg at Day 4 after prone positioning (Fernandez et al., 2008; Guerin et al.,

49
2004; Guerin et al., 2013; Mancebo et al., 2006; Voggenreiter et al., 2005). Hence, the clinical
effectiveness for this study is quantified as a 40mmHg increase in PaO2/FiO2 ratio at Day 4
of the intervention.
For other secondary outcomes, the expected clinical effectiveness is quantified based
on the reviewed studies. The prevalence of VAP was reduced by 3.5% to 27% (Guerin et al.,
2004; Voggenreiter et al., 2005) and so a 15% reduction is regarded as effective. The
mortality rate was dropped by 8.3% to 16.8% at Day 28 after prone positioning (Fernandez et
al., 2008; Guerin et al., 2013; Robak et al., 2011; Voggenreiter et al., 2005). Hence, a 12%
drop in mortality at Day 28 is regarded as effective. For adverse events, since insignificant
results showed in four reviewed studies (Gattinoni et al., 2001; Guerin et al., 2013; Mancebo
et al., 2006; Voggenreiter et al., 2005), no significant result in adverse events is regarded as
effective.
With regards to the healthcare provider outcomes, job satisfaction, level of competence,
knowledge and skills are expected more than 70% to be graded at least three or above out of
five after implementation. The attendance of the journal club or workshop should be more
than 80%.
For the system outcome, the actual expenditures are expected not exceed the funding
by the department. Manpower and materials are expected to be sufficient during
implementation.

50
Chapter 7
Conclusion
ARDS is common and life-threatening condition developed in critically ill patients. It
is found prone positioning is a simple, safe and inexpensive method to improve oxygenation
and benefit on survival among ARDS patients. A systematic search was done, nine
randomized controlled trials were selected and critical appraised. After summarizing and
synthesizing the evidence, an early, continuous and prolonged prone positioning was proved
effective and was translated to the practice.
Considering the implementation potential including the transferability, the feasibility
and cost-effectiveness of the innovation to the target setting and audience in local ICU, an
evidence-based guideline of prone positioning for ARDS patients is developed.
Implementation plan requires an effective communication strategy to different
stakeholders. Besides, staff training towards the guideline and a six-month pilot study will be
carried out to test the feasibility before full implementation.
The outcomes of patients, healthcare providers and system will be evaluated after
implementation. The primary outcome of the innovation is oxygenation. A 40mmHg increase
in PaO2/FiO2 at Day 4 of the intervention will be regarded as effective.

51
References
Albert, R. & Hubmayr, R. (2000). The prone position eliminates compression of lungs by the
heart. American Journal of Respiratory Critical Care Medicine, 161, 1660-1665.
Albert, R.K., Leasa, D., Sanderson, M., Robertson, H.T. & Hlastala, M.P. (1987). The prone
position improves arterial oxygenation and reduces shunt in olei-acid-induced acute
lung injury. American Review of Respiratory Disease, 135, 628-633.
Bernard, G.F., Artigas, A., Brigham, K.L., Carlet, J., Falke, K., Hudson, L. et al. (1994).
Report of the American-European consensus conference on ARDS: definitions,
mechanisms, relevant outcomes and clinical trial coordination. American Journal of
Respiratory of Critical Care Medicine, 149, 818-824.
Blanch, L., Mancebo, J., Perez, M., Martinez, M., Mas, A., Betbese, A.J. et al. (1997). Short
term effects of prone position in critically ill patients with acute respiratory distress
syndrome. Intensive Care Medicine, 23, 1033-1039.
Chatte, G., Sab, J.M., Dubois, J.M., Sirodot, M., Gaussorgues, P. & Robert, D. (1997). Prone
position in mechanically ventilated patients with severe acute respiratory failure.
American Journal of Respiratory Critical Care Medicine, 155,473-478.
De Jong, A., Molinari, N., Sebbane, M., Prades, A., Futier, E., Jung, B. et al. (2013).
Feasibility and effectiveness of prone position in morbidly obese patients with ARDS.
Chest, 143 (6), 1554-1561.
52
Fernandez, R., Trenchs, X., Klamburg, J., Castedo, J., Serrano, J.M., Besso, G. et al. (2008).
Prone positioning in acute respiratory distress syndrome: a multicenter randomized
clinical trial. Intensive Care Medicine, 34, 1487-1491.
Frutos-Vivar, F., Nin, N. & Esteban, A. (2004). Epidemiology of acute lung injury and acute
respiratory distress syndrome. Current Opinion Critical Care, 10, 1-6.
Gattinoni, L., Tognoni, G., Pesenti, A., Taccone, P., Mascheroni, D., Labarta, V. et al. (2001).
Effect of prone positioning on the survival of patients with acute respiratory failure.
The New England Journal of Medicine, 345(8), 568-573.
Guerin, C., Badet, M., Rosell, S., Heyer, L., Sab, J.M., Langevin, B. et al. (1999). Effects of
prone position on alveolar recruitment and oxygenation in acute lung injury. Intensive
Care Medicine, 25, 1222-1230.
Guerin, C., Gailard, S., Lemasson, S., Ayzac, L., Girard, R., Beuret, P. et al. (2004). Effects of
systematic prone positioning in hypoxemic acute respiratory failure. JAMA, 292(19),
2379-2387.
Guerin, C., Reignier, J., Richard, J.C., Beuret, P., Gacouin, A., Boulain, T. et al. (2013). Prone
positioning in severe acute respiratory distress syndrome. The New England Journal of
Medicine, 368 (23), 2159-2168.
53
Hospital Authority. (2013). Vision, Mission and Values. Retrieved from 20 May, 2013, from
http://www.ha.org.hk/visitor/ha_visitor_index.asp?Content_ID=10009&Lang=ENG&D
imension=100&Parent_ID=10004&Ver=HTML
Lamm, W.J.E., Graham, M, M & Albert, R.K. (1994). Mechanism by which the prone
position improves oxygenation in acute lung injury. American Journal of Respiratory
Critical Care Medicine, 150, 184-193.
Le Gall, J.R., Lemeshow, S. & Saulnier, F. (1993). A new simplified acute physiology score
(SAPS II) based on a European/ North American multicenter study. JAMA, 270(24),
2957-2963.
Lenth, R.V. (2006-9). Java Applets for Power and Sample Size [Computer software].
Retrieved May 9, 2014, from http://homepage.cs.uiowa.edu/~rlenth/Power/
Likert, R. (1932). A technique for the measurement of attitude. Archives of Psychology, 140,
1-55.
Mancebo, J., Fernandez, R., Blanch, L., Rialp, G., Gordo, F., Ferrer, M. et al. (2006). A
multicenter trial of prolonged prone ventilation in severe acute respiratory distress
syndrome. American Journal of Respiratory and Critical Care Medicine, 173,
1233-1239.
Matthay, M.A., Ware, L.B. & Zimmerman, G.A. (2012). The acute respiratory distress
syndrome. The Journal of Clinical Investigation, 122(8), 2731-2740.
54
Papazian, L., Gainnier, M., Marin, V., Donati, S., Arnal, J.M., Demory, D. et al. (2005).
Comparison of prone positioning and high-frequency oscillatory ventilation in patients
with acute respiratory distress syndrome. Critical Care Medicine, 33(10), 2162-2171.
Pappert, D., Rossaint, R., Slama, K., Gruning, T. & Falke, K.J. (1994). Influence of
positioning on ventilation-perfusion relationships in severe adult respiratory distress
syndrome. Chest, 106, 1511-1516.
Pelosi, P., Tubiolo, D., Mascheroni, D., Vicardi, P., Crotti, S., Valenza, F. et al. (1998). Effects
of the prone position on respiratory mechanics and gas exchange during acute lung
injury. American Journal of Respiratory Critical Care Medicine, 157, 387-393.
Ricard, J-D., Dreyfuss, D. & Saumon, G. (2003). Ventilator-induced lung injury. European
Respiratory Journal, 22, Supp 42, 2s-9s.
Robak, O., Schellongowski, P., Bojic, A., Laczika, K., Locker, G.J. & Staudinger, T. (2011).
Short-term effects of combining upright and prone positions in patients with ARDS: a
prospective randomized study. Critical Care, 15.
Rubenfeld, G.D., Caldewell, E., Peabody, E., Weaver, J., Martin, D.P., Neff, M. et al. (2005).
Incidence and outcomes of acute lung injury. The New England Journal of Medicine,
353, 1685-1693.

55
Scottish Intercollegiate Guideline Network (SIGN). (2012). SIGN 50: A Guideline
Developer’s Handbook. Retrieved March 22, 2013, from
http://www.sign.ac.uk/methodology/checklists.html#
Sharma, S. (2010). Acute respiratory distress syndrome. Clinical Evidence. Retrieved August
8, 2013, from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3217743/pdf/2010-1511.pdf
Sigvaldason, K., Thomormar, K., Bergmann, J.B., Reynisson, K., Magnusdottir, H.,
Stefansson, P.S. et al. (2006). The incidence and mortality of ARDS in Icelandic
intensive care units 1988-1997. Laeknabladid, 92, 201-207.
Taccone, P., Pesenti, A., Latini, R., Polli, F., Vagginelli, F., Mietto, C. et al. (2009). Prone
positioning in patients with moderate and severe acute respiratory distress syndrome.
JAMA, 302(18), 1977-1984.
The ARDS definition task force. (2012). Acute respiratory distress syndrome: the Berlin
definition. JAMA, 307(23), 2526-2533.
The Department of Health. (2012). Public Health & Epidemiology Bulletin. Hong Kong :The
Department of Health.
Vincent, J.L., Moreno, R., Takala, J. et al. (1996). The SOFA (Sepsis-Related Organ Failure
Assessment) score to describe organ dysfunction/failure. Intensive Care Medicine,
22(7), 707-710.

56
Voggenreiter, G., Aufmkolk, M., Stiletto, R.J., Baacke, M.G., Waydhas, C., Ose, C et al.
(2005). Prone positioning improves oxygenation in post-traumatic lung injury- a
prospective randomized trial. The Journal of Trauma, 59(2), 333-343.
World Health Organization. (2013). Avian Influenza A (H&N9)virus. Retrieved December 10,
2013,from
http://www.who.int/influenza/human_animal_interface/influenza_h7n9/en/index.html

57
Appendix 1 Search Strategies
PubMed (1997-2013), Medline (ProQuest, 1991-2013, CINAHL (EBSCO host, 1991-2013)
Database
# Keyword search Pubmed Medline
(ProQuest)
CINAHL
(EBSCO host)
1 ARDS patients OR acute respiratory distress
OR acute respiratory distress syndrome OR
acute respiratory failure OR early acute
respiratory distress syndrome
36,989 14,193 4,071
2 Prone position OR prone positioning OR
prone position ventilation
45,359 49,029 837
3 Oxygenation OR oxygen consumption OR
oxygen saturation OR ventilation perfusion
ratio OR breathing
372,093 101,362 1582
4 #1 AND #2 AND #3 510 282 160
5 Subtotal 952
6 #1 AND #2 AND #3 (RCT) 33 20 44
7 Articles remained after screening title,
abstract and full paper
10 5 5
8 Articles remained after removal of duplicated
with other databases
6 3 0
9
Articles from references of eligible studies 0
Studies met the selection criteria 9
Systematic searching was performed in August, 2013

58
Appendix 2 Table of Evidence
1 Gattinoni, L., Tognoni, G., Pesenti, A., Taccone, P., Mascheroni, D., Labarta, V. et al. (2001). Effect of prone positioning on the survival of
patients with acute respiratory failure. The New England Journal of Medicine, 345(8), 568-573. Citation Study
type
Evidence
level
Patient characteristics Intervention(s) Comparison
/ Control
Outcome measures Effect size
Gattinoni
et al.,
2001
RCT 1+ ARDS or ALI patients who were received MV
from December 1996 to October 1999 in Italy
and Switzerland.
Age: mean 58
Male: 70%
BMI: not mentioned
SAPS II: mean 40, SOFA: not mentioned
ALI: 6%, ARDS: 94%
Pneumonia:48 %, Aspiration: 3%,
Sepsis: 9.3% Trauma: 2.3 %, Other:12%
PaO2/ FiO2 ratio: mean 127
PEEP, cm H2O: mean 9.6
FiO2: mean 0.73
PaO2, mmHg: mean 87
PaCO2, mmHg: mean 45
Prone position for
a mean of 7 h/day
for a period of 10
days
(n=152)
Supine
position
(n=152)
Primary outcome:
1) Mortality at 10 days,
2) the time of discharge
from ICU, and 6 months
after randomization.
Secondary outcome:
3) Improvement of
respiratory failure
4) Improvement of organ
dysfunction at 10 days.
5) No. of new/ worsening
sore
6) Complication ( tracheal
tube displacement, loss of
venous access, accidental
extubation, facial edema)
1) -3.9% (21.1% vs.
25%, RR= 0.84,
95%CI= 0.56-1.27,
p=0.65)
2) ns
3) PaO2/ FiO2 ratio
+18.4 (63 vs. 44.6,
p=0.02)
4) ns
5) +0.8 (2.7vs. 1.9,
p=0.004)
6) ns

59
2 Guerin, C., Gailard, S., Lemasson, S., Ayzac, L., Girard, R., Beuret,. P. et al. (2004). Effects of systematic prone positioning in hypoxemic
acute respiratory failure. JAMA, 292(19), 2379-2387.
Citation Study
type
Evidence
level
Patient characteristics Intervention(s) Comparison/
Control
Outcome measures Effect size
Guerin et
al., 2004
RCT 1+ Adult patients with hypoxemic
ARF who were intubated over
48 hours were receiving MV
from December 1998 to
December 2002 in France.
Age: mean 62
Male: 75%
BMI: 26.2
SAPS II : mean 46
PaO2/ FiO2 ratio: mean 153
PEEP, cm H2O: mean 7.7
PaCO2, mmHg: mean 44
Prone position for
median of 8h/day for a
median of 4 days
(n=413)
Mean time between
ICU admission and
randomization was 58h.
Mean time between
randomization and first
prone session was 4.3h.
Supine position with
30° angle
(n=378)
Allow cross over to
prone position with
PaO2/ FiO2 ratio
<100 for more than
12 hours or <60 for
more than 1 hour,
both receiving pure
oxygen.
Primary outcome:
1) Mortality at 28 days
Secondary outcome:
2) Mortality at 90 days
3) Incidence of VAP
4) Duration of MV
5) PaO2/FiO2 ratio
6) Complication
(selective
intubation,
endotracheal tube
obstruction,
pressure sore)
1) -0.9 % ( 31.5% vs. 32.4%,
RR= 0.97,
95% CI= 0.79-1.19,
p= 0.77)
2) – 1.1% (42.2%vs. 43.3%,
RR= 0.98,
95% CI: 0.84-1.13, p= 0.74)
3) -3.5% (20.6% vs. 24.1%,
p=0.045)
4) ns
5) p=<0.001
6) p=0.01, p=0.002, p=0.005
No protective lung ventilation
Crossover was allowed only in cases of
life-threatening hypoxemia.

60
3 Papazian, L., Gainnier, M., Marin, V., Donati, S., Arnal, J.M., Demory, D. et al. (2005). Comparison of prone positioning and
high-frequency oscillatory ventilation in patients with acute respiratory distress syndrome. Critical Care Medicine, 33(10), 2162-2171. Citation Study
type
Evidence
level
Patient characteristics Intervention(s) Comparison/
Control
Outcome measures Effect size
Papazian
et al.,
2005
RCT 1- Adult patients with ARDS
received MV in France
Age: mean 51
Male :59%
BMI: not mentioned
SAPS II score: mean 41
SOFA: mean 9.5
ARDS due to pneumonia:40%
Sepsis: 13%, Aspiration: 36%
PaO2/FiO2 ratio: mean 103
PEEP, cm H2O: mean 11
FiO2: mean 0.72
PaO2, mmHg: not mentioned
PaCO2, mmHg: mean not
mentioned
After an optimizations period (supine-CV)
of 12 hours using conventional lung
protective mechanical ventilation, patients
were assigned to following groups:
1) PaO2/FiO2 ratio
2) Hemodynamic
variables and
gaseous
exchange
1) Group A vs. supine-CV(baseline)
+79 (217 vs. 138, p<0.0001)
Group B vs. supine-CV
+101 (227 vs. 126, p<0.0001 )
Group C vs. supine-CV : ns
2) Prone position group reduced the
venous admixture than supine group.
(p<0.05).
Group A:
Conventional
lung-protective
mechanical ventilation in
prone position
(prone-CV) for 12 hours
(n=13)
Group B:
HFOV in prone position
for 12 hours
(prone-HFOV) (n=13)
Group C:
HFOV in
supine position
for 12 hours
(supine-HFOV)
(n=13)

61
4 Voggenreiter, G., Aufmkolk, M., Stiletto, R.J., Baacke, M.G., Waydhas, C., Ose, C et al. (2005). Prone positioning improves oxygenation in
post-traumatic lung injury- a prospective randomized trial. The Journal of Trauma, 59(2), 333-343. Citation Study
type
Evidence
level
Patient characteristics Intervention(s) Comparison
/ Control
Outcome measures Length
of
study
Effect size
Voggenreiter
et al., 2005
RCT 1+ Multiple trauma adult patients
associated with ALI or ARDS
who received MV from
September 1999 to September
2001in Germany.
Age: mean 42
Male: 83%
BMI: not mentioned
ISS: mean 37, SOFA Score: 12
ALI: 55%, ARDS: 45%
Pneumonia:18 %, Sepsis: 3%
PaO2/ FiO2 ratio: mean 222
PEEP, cm H2O: mean 12
FiO2: mean 0.49
PaO2, mmHg: mean 104
PaCO2, mmHg: mean 37
Prone position during
nighttime until PaO2/
FiO2 ratio >300 in prone
and supine 48 hours.
Prone position was
applied for a mean of
11h/ day.
(n=21)
Supine
position
(n=19)
Primary outcome:
1) Duration of MV
Secondary outcome:
2) Days with ARDS
and ALI
3) Days with LIS >=2
4) PaO2/ FiO2 ratio
5) Sepsis,
6) Prevalence of
pneumonia
7) Prevalence of ARDS
8) Mortality
9) Complication
( pressure sore,
edema, tracheal tube
displacement,
arrhythmia)
10) PEEP Day 4
11) Packed cell
transfusion
12) Use of antibiotic and
paralyzing agent
90days 1) ns
2) ARDS: ns
ALI: -3 days (8 vs. 11,
p= 0.03)
3) ns
4) +44.1 (71.8 vs. 27.7,
p=0.03 in first 4 days )
5) ns
6) -27% (62% vs. 89%,
p=0.048)
7) -6 (6 vs. 12, p=0.03)
8) -11% (5% vs. 16%,
p=0.27), due to small
sample size.
9) ns
10) p<0.009
11) -18.7 (9.5 vs. 28.2 unit
p=0.05)
12) ns.
The mean time between trauma and
entrance into the study was 5 days.
No crossover was allowed.
Protective lung ventilation was applied.
No PEEP algorithm protocol.

62
5 Mancebo, J., Fernandez, R., Blanch, L., Rialp, G., Gordo, F., Ferrer, M. et al. (2006). A multicenter trial of prolonged prone ventilation in
severe acute respiratory distress syndrome. American Journal of Respiratory and Critical Care Medicine, 173, 1233-1239. Citation Study
type
Evidence
level
Patient characteristics Intervention(s) Comparison/
Control
Outcome measures Effect size
Mancebo
et al.,
2006
RCT 1+ Severe ARDS patients as defined
by the American-European
Consensus Conference from
December 1998 to September 2002
in Spain and Mexico.
Age: mean 54
Male: 58%
BMI: not mentioned
SAPS II: mean 41
SOFA: not mentioned
ARDS due to pneumonia:50.7 %
Aspiration: 11%, Sepsis: 23.5%
Trauma: 2.2 %, Other: 12.5%
PaO2/ FiO2 ratio: mean 146.5
PEEP, cm H2O: mean 8.5
FiO2: mean 0.82
PaO2, mmHg: mean 116.5
PaCO2, mmHg: mean 44
Prone position within
1h after randomization
until weaning
oxygenation threshold
was reached, then
turned to supine for up
to 4 hours each
morning.
Prone position was
applied for a mean of
17h/ day with average
10 day.
(n=80)
Supine position
(n=62)
Primary outcome:
1) ICU mortality
Secondary outcome:
2) Hospital mortality
3) Associated
complications
( edema,
conjunctival
hemorrhage and
pressure sore)
4) Length of stay
5) PaO2/ FiO2 ratio
6) FiO2
Day 4
7) Plateau pressure,
8) PEEP
1) -15% absolute, -25% relative
(43% vs. 58%, p=0.12) (due
to higher severity score in
prone group)
2) -12 % (50 vs. 62, p=0.27)
3) ns
4) ns
5) Day 4
+39 (215 vs. 176, p<0.005)
6) Day 4
-10 % (52%vs.62%, p<0.001)
7) -3 (31 vs. 28 cm H2O,
p=0.01)
8) -2 (11vs. 9 cm H2O,
p= 0.048)
Time between ARDS diagnosis and
randomization was 1.04 day in supine group
and 0.89 day in prone group.
Crossover was allowed.
Protective lung ventilation was applied.

63
6 Fernandez, R., Trenchs, X., Klamburg, J., Castedo, J., Serrano, J.M., Besso, G. et al. (2008). Prone positioning in acute respiratory distress
syndrome: a multicenter randomized clinical trial. Intensive Care Medicine, 34, 1487-1491. Citation Study
type
Evidence
level
Patient characteristics Intervention(s) Comparison/
Control
Outcome measures Effect size
Fernandez
et al.,
2008
RCT 1+ ARDS patients as defined by the
American- European Consensus
Conference in September 2003 in
Spain.
Age: mean 54.6
Male: 63%
BMI: not mentioned
SAPS II: mean 38.3
SOFA: mean 9.25
Lung Injury score: mean 3.1
PaO2/ FiO2 ratio: mean 155.5
PEEP, cm H2O: mean 13.2
FiO2: mean 0.75
PaO2, mmHg: mean 112.4
PaCO2, mmHg: mean 49.4
Prone position maintained
up to 20h/day within 48h
after diagnosis. Then,
turned supine when
oxygenation improved for
longer than 12h. (i.e.
PaO2/ FiO2 ratio higher
than 250 at PEEP of 8cm
H2O or lower.
(n=21)
Supine position
(n=19)
Primary outcome:
1) PaO2/ FiO2 ratio
2) 60-day mortality.
Secondary outcome:
3) Length of mechanical
ventilation
4) Length of ICU stay
5) Use of vasoactive
drug and sedation
1) + 75 on Day 3 (234±85 vs.
159±78, p=0.009).
2) -15% (38% vs. 53%), but no
significant difference due to
small sample size.
3) -3.8 day ( 11.9 vs. 15.7,
p=0.5)
4) -2.8day ( 14.7 vs. 17.5,
p=0.5)
5) ns Protective lung ventilation was applied
Crossover was allowed only in cases of
life-threatening hypoxemia after 6h in position
selected.

64
7 Taccone, P., Pesenti, A., Latini, R., Polli, F., Vagginelli, F., Mietto, C. et al. (2009). Prone positioning in patients with moderate and severe
acute respiratory distress syndrome. JAMA, 302(18), 1977-1984. Citation Study
type
Evidence
level
Patient characteristics Intervention(s) Comparison/
Control
Outcome measures Effect size
Taccone
et al.,
2009
RCT 1+ ARDS patients as defined by
American-European Consensus
Conference criteria in Italy and Spain
from February 2004 to June 2008;
Age: mean 60
Male: 71.3%
BMI: 25.3
SAPS II: mean 41
SOFA: mean 6.8
ARDS due to pneumonia: 59.1 %
Aspiration: 6.4%, Sepsis: 4.7%
Trauma: 1.8 %, Other: 23.4%
PaO2/ FiO2 ratio: mean 113
PEEP, cm H2O: mean 10
FiO2: mean 0.72
PaO2, mmHg: not mentioned.
PaCO2, mmHg: mean 46.5
Prone position after
diagnosed ARDS within
72 hours until the
resolution of acute
respiratory failure or end
of the 28-day study
period.
average 8 sessions per
patient, mean duration per
session was 18 hours
(n= 168)
Supine position
(n= 174)
Primary outcome
1) Mortality at day 28
Secondary outcome
2) Mortality at day 180
3) SOFA score at day 28
4) Ventilator free days
5) Complication (use of
sedation, muscle
paralysis,
hemodynamic
instability or device
displacement
Moderate ARDS:
1) +3% (25.5 vs. 22.5%,
RR=1.04, 95%CI=
0.89-1.22, p= 0.62)
2) -1.3% (42.6% vs. 43.9%,
RR= 0.98, 95%CI=
0.76-1.25, p= 0.85)
3) ns
4) ns
Severe ARDS:
1) -8.3% (37.8% vs. 46.1%,
RR=0.87, 95%CI=
0.66-1.14, p= 0.631)
2) -10.5% (52.7% vs. 63.2%,
RR=0.78, 95%CI=
0.53-1.14, p= 0.19)
3) ns
4) ns
5) 18.2% (94.6% vs. 76.4%,
p<0.001)
Protective lung ventilation was applied.
Crossover was allowed only as a rescue
measure.
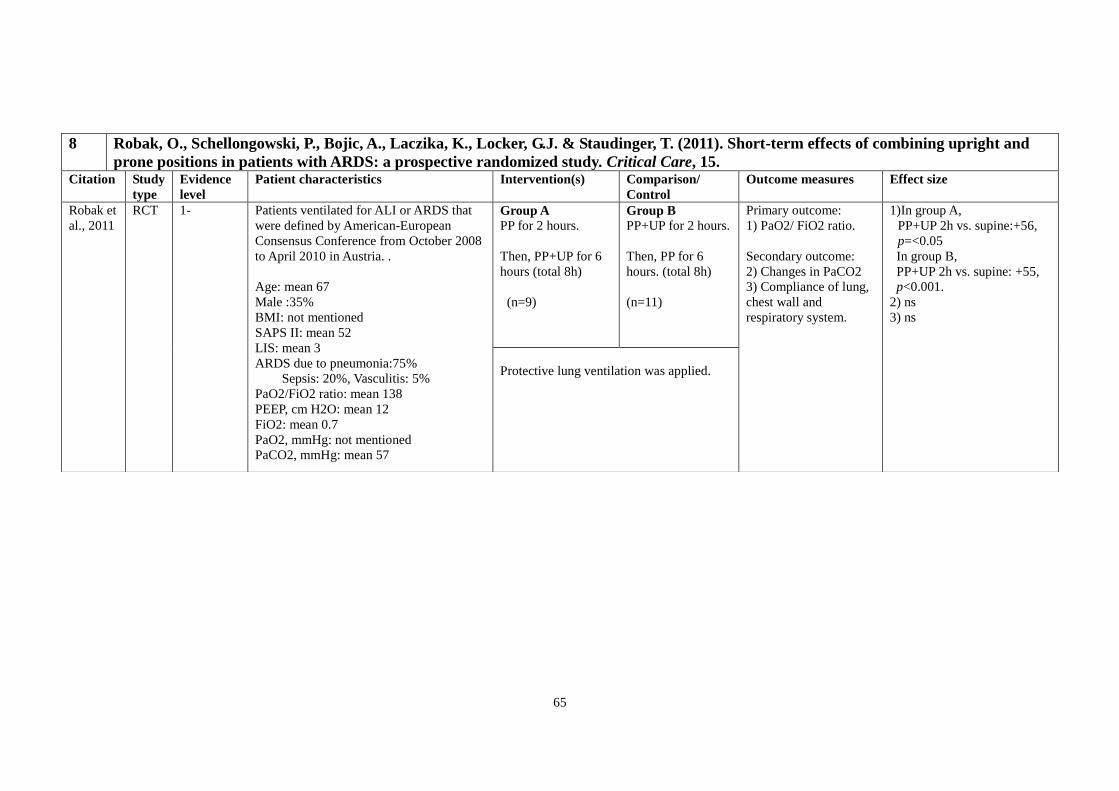
65
8 Robak, O., Schellongowski, P., Bojic, A., Laczika, K., Locker, G.J. & Staudinger, T. (2011). Short-term effects of combining upright and
prone positions in patients with ARDS: a prospective randomized study. Critical Care, 15. Citation Study
type
Evidence
level
Patient characteristics Intervention(s) Comparison/
Control
Outcome measures Effect size
Robak et
al., 2011
RCT 1- Patients ventilated for ALI or ARDS that
were defined by American-European
Consensus Conference from October 2008
to April 2010 in Austria. .
Age: mean 67
Male :35%
BMI: not mentioned
SAPS II: mean 52
LIS: mean 3
ARDS due to pneumonia:75%
Sepsis: 20%, Vasculitis: 5%
PaO2/FiO2 ratio: mean 138
PEEP, cm H2O: mean 12
FiO2: mean 0.7
PaO2, mmHg: not mentioned
PaCO2, mmHg: mean 57
Group A
PP for 2 hours.
Then, PP+UP for 6
hours (total 8h)
(n=9)
Group B
PP+UP for 2 hours.
Then, PP for 6
hours. (total 8h)
(n=11)
Primary outcome:
1) PaO2/ FiO2 ratio.
Secondary outcome:
2) Changes in PaCO2
3) Compliance of lung,
chest wall and
respiratory system.
1)In group A,
PP+UP 2h vs. supine:+56,
p=<0.05
In group B,
PP+UP 2h vs. supine: +55,
p<0.001.
2) ns
3) ns
Protective lung ventilation was applied.

66
9 Guerin, C., Reignier, J., Richard, J.C., Beuret, P., Gacouin, A., Boulain, T. et al. (2013). Prone positioning in severe acute respiratory
distress syndrome. The New England Journal of Medicine, 368 (23), 2159-2168. Citation Study
type
Evidence
level
Patient characteristics Intervention(s) Comparison/
Control
Outcome measures Effect size
Guerin
et al.,
2013
RCT 1++ ARDS patients as defined by
American-European
Consensus Conference criteria
in France and Spain from
January 2008 to July 2011;
MV for ARDS <36 hrs;
Severe ARDS
Age: mean 59
Male : 68.2%
BMI: mean 28.5
SAPS II: mean 46
SOFA: mean 10
ARDS due to
pneumonia:60.3%
PaO2/FiO2 ratio: mean 100
PEEP, cm H2O: mean 10
FiO2: mean 0.79
PaO2, mmHg: mean 80
PaCO2, mmHg: mean 51
Prone position with guidelines within
first hour after randomization until
improvement in oxygenation.
.
(First prone within 55mins after
randomization, average 4 sessions per
patient, mean duration per session
was 17 hours.)
(n=237)
Supine group
remained in a
semi-recumbent
position.
(n=229)
Primary outcome
1) Mortality at day 28
Secondary outcome
2) Mortality at day 90
3) Successful extubation
rate at day 90
4) LOS in ICU at day 90
5) Complications
6) Use of NIV
7) Tracheotomy rate
8) PaO2/FiO2
9) PEEP
10) FiO2
1) -16.8% (16% vs.
32.8%, HR= 0.39,
p<0.001)
2) –17.4% (23.6% vs.
41%, HR= 0.44,
p<0.001)
3) +20.5% (80.5% vs.
65%, HR= 0.45,
p < 0.001)
4) p=0.05, ns
5) p=0.85, ns
6) p> 0.05, ns
7) p>0.05, ns
8) Day 3 +15
(172vs.157, p<0.05)
Day 5 +22
(179vs. 157, p<0.01)
9) Day 3 -0.7, p<0.05
Day5 -0.8, p<0.05
10) Day 3 -0.05, p<0.01
Day 5 -0.07, p<0.01
MV in VC mode with constant inspiratory flow, with
tidal volume targeted at 6ml/kg and PEEP level selected
from a PEEP-FiO2 table.
Protective lung ventilation was applied.
Crossover was allowed only as a rescue measure.
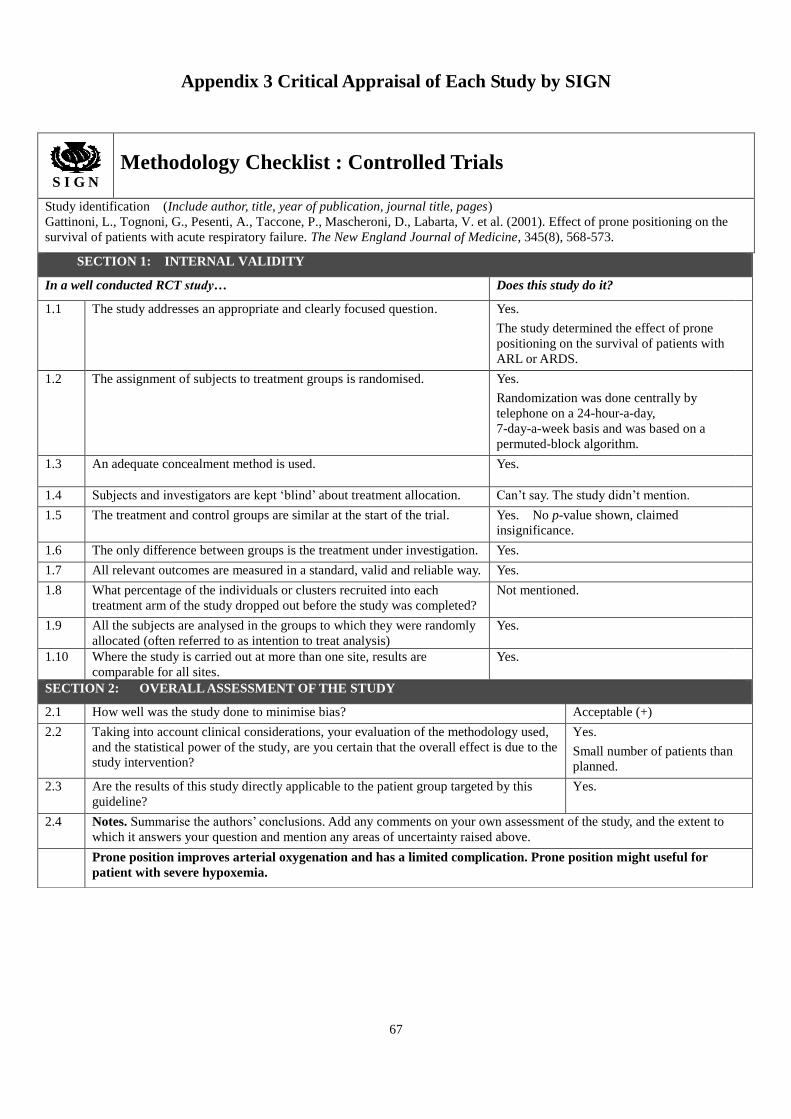
67
Appendix 3 Critical Appraisal of Each Study by SIGN
S I G N
Methodology Checklist : Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Gattinoni, L., Tognoni, G., Pesenti, A., Taccone, P., Mascheroni, D., Labarta, V. et al. (2001). Effect of prone positioning on the
survival of patients with acute respiratory failure. The New England Journal of Medicine, 345(8), 568-573.
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
Yes.
The study determined the effect of prone
positioning on the survival of patients with
ARL or ARDS.
1.2 The assignment of subjects to treatment groups is randomised.
Yes.
Randomization was done centrally by
telephone on a 24-hour-a-day,
7-day-a-week basis and was based on a
permuted-block algorithm.
1.3 An adequate concealment method is used.
Yes.
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation. Can’t say. The study didn’t mention.
1.5 The treatment and control groups are similar at the start of the trial. Yes. No p-value shown, claimed
insignificance.
1.6 The only difference between groups is the treatment under investigation. Yes.
1.7 All relevant outcomes are measured in a standard, valid and reliable way. Yes.
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was completed?
Not mentioned.
1.9 All the subjects are analysed in the groups to which they were randomly
allocated (often referred to as intention to treat analysis)
Yes.
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias? Acceptable (+)
2.2 Taking into account clinical considerations, your evaluation of the methodology used,
and the statistical power of the study, are you certain that the overall effect is due to the
study intervention?
Yes.
Small number of patients than
planned.
2.3 Are the results of this study directly applicable to the patient group targeted by this
guideline?
Yes.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to
which it answers your question and mention any areas of uncertainty raised above.
Prone position improves arterial oxygenation and has a limited complication. Prone position might useful for
patient with severe hypoxemia.
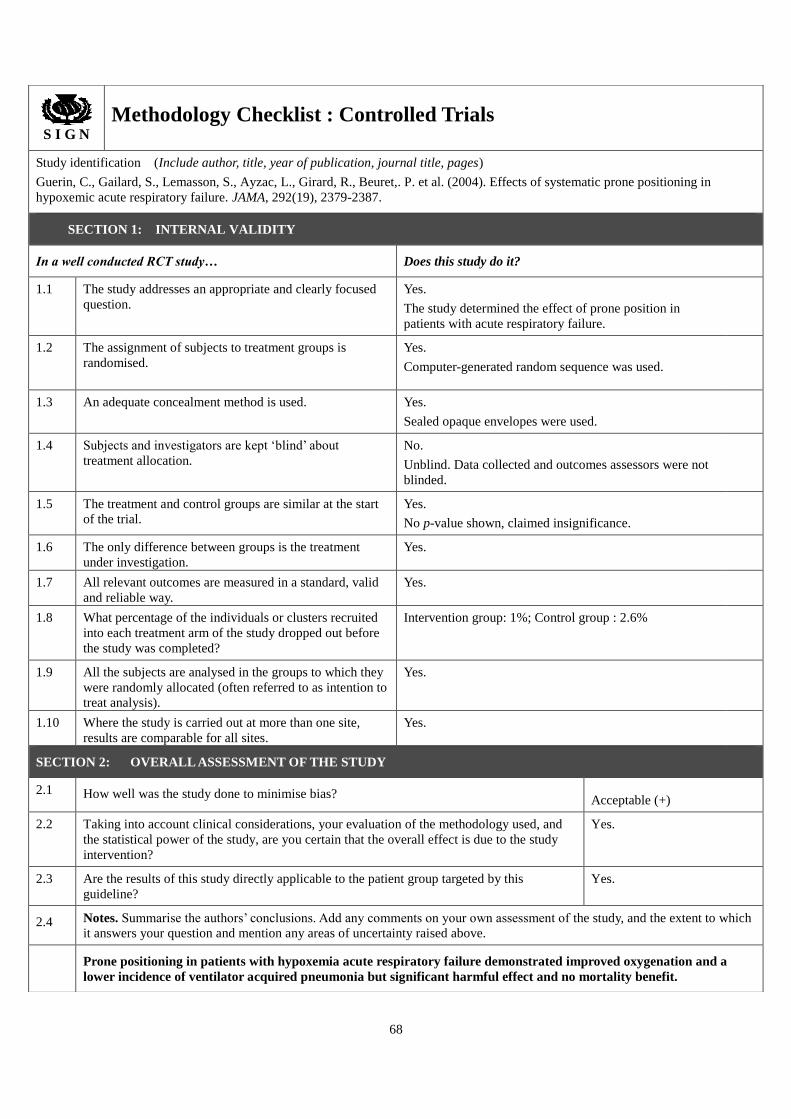
68
S I G N
Methodology Checklist : Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Guerin, C., Gailard, S., Lemasson, S., Ayzac, L., Girard, R., Beuret,. P. et al. (2004). Effects of systematic prone positioning in
hypoxemic acute respiratory failure. JAMA, 292(19), 2379-2387.
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused
question.
Yes.
The study determined the effect of prone position in
patients with acute respiratory failure.
1.2 The assignment of subjects to treatment groups is
randomised.
Yes.
Computer-generated random sequence was used.
1.3 An adequate concealment method is used.
Yes.
Sealed opaque envelopes were used.
1.4 Subjects and investigators are kept ‘blind’ about
treatment allocation.
No.
Unblind. Data collected and outcomes assessors were not
blinded.
1.5 The treatment and control groups are similar at the start
of the trial.
Yes.
No p-value shown, claimed insignificance.
1.6 The only difference between groups is the treatment
under investigation.
Yes.
1.7 All relevant outcomes are measured in a standard, valid
and reliable way.
Yes.
1.8 What percentage of the individuals or clusters recruited
into each treatment arm of the study dropped out before
the study was completed?
Intervention group: 1%; Control group : 2.6%
1.9 All the subjects are analysed in the groups to which they
were randomly allocated (often referred to as intention to
treat analysis).
Yes.
1.10 Where the study is carried out at more than one site,
results are comparable for all sites.
Yes.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias? Acceptable (+)
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and
the statistical power of the study, are you certain that the overall effect is due to the study
intervention?
Yes.
2.3 Are the results of this study directly applicable to the patient group targeted by this
guideline?
Yes.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which
it answers your question and mention any areas of uncertainty raised above.
Prone positioning in patients with hypoxemia acute respiratory failure demonstrated improved oxygenation and a
lower incidence of ventilator acquired pneumonia but significant harmful effect and no mortality benefit.

69
S I G N
Methodology Checklist : Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Papazian, L., Gainnier, M., Marin, V., Donati, S., Arnal, J.M., Demory, D. et al. (2005). Comparison of prone positioning and
high-frequency oscillatory ventilation in patients with acute respiratory distress syndrome. Critical Care Medicine, 33(10), 2162-2171.
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused
question.
Yes.
The study was to compare the effects of prone position, HROV,
and their combination on gas exchange in severe ARDS
patients.
1.2 The assignment of subjects to treatment groups is
randomised.
Can’t say.
Randomization mentioned without method specified
1.3 An adequate concealment method is used.
Yes.
Opaque, sealed envelopes were used.
1.4 Subjects and investigators are kept ‘blind’ about
treatment allocation.
Can’t say. Not mentioned.
1.5 The treatment and control groups are similar at the start
of the trial.
Yes. No p-value shown, claimed insignificance.
1.6 The only difference between groups is the treatment
under investigation.
Yes.
1.7 All relevant outcomes are measured in a standard, valid
and reliable way.
Yes.
1.8 What percentage of the individuals or clusters recruited
into each treatment arm of the study dropped out before
the study was completed?
Not mentioned.
1.9 All the subjects are analysed in the groups to which
they were randomly allocated (often referred to as
intention to treat analysis).
Does not apply.
All the subjects were analyzed as no drop out was mentioned.
1.10 Where the study is carried out at more than one site,
results are comparable for all sites.
Does not apply.
This is a single-centered study carried out in a medical ICU.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias? Low quality (-)
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the
statistical power of the study, are you certain that the overall effect is due to the study
intervention?
Yes
Not clear randomization.
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline? Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which
it answers your question and mention any areas of uncertainty raised above.
In ARDS patients, HFOV in the supine position does not improve oxygenation and reduces lung inflammation,
prone-HFOV produced improvement in oxygenation in oxygenation that was similar to that of prone-CV but was
higher BALF indexes of inflammation.

70
S I G N
Methodology Checklist : Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Voggenreiter, G., Aufmkolk, M., Stiletto, R.J., Baacke, M.G., Waydhas, C., Ose, C et al. (2005). Prone positioning improves
oxygenation in post-traumatic lung injury- a prospective randomized trial. The Journal of Trauma, 59(2), 333-343.
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused
question.
Yes.
The study determined the effect of prone positioning
on the duration of mechanical ventilation in multiple
trauma patients with ALI or ARDS.
1.2 The assignment of subjects to treatment groups is randomised.
Yes.
Randomization was done centrally by telephone on a
24-hour-a-day, 7-day-a-week basis and was based on
a permuted-block algorithm.
1.3 An adequate concealment method is used.
Yes.
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
Can’t say. The study didn’t mention.
1.5 The treatment and control groups are similar at the start of the
trial.
Yes. p-value > 0.05
1.6 The only difference between groups is the treatment under
investigation.
Yes.
1.7 All relevant outcomes are measured in a standard, valid and
reliable way.
Yes.
1.8 What percentage of the individuals or clusters recruited into
each treatment arm of the study dropped out before the study
was completed?
0%
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat
analysis).
Yes.
1.10 Where the study is carried out at more than one site, results
are comparable for all sites.
Yes.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias? Acceptable (+)
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the
statistical power of the study, are you certain that the overall effect is due to the study
intervention?
Yes.
Small sample size.
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline? Yes.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to
which it answers your question and mention any areas of uncertainty raised above.
Intermittent prone positioning did not reduce the duration of mechanical ventilation with limited number of
patients. Oxygenation improved significantly over first 4 days of treatment, the prevalence of ARDS and
pneumonia was reduced.

71
S I G N
Methodology Checklist : Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Mancebo, J., Fernandez, R., Blanch, L., Rialp, G., Gordo, F., Ferrer, M. et al. (2006). A multicenter trial of prolonged prone ventilation
in severe acute respiratory distress syndrome. American Journal of Respiratory and Critical Care Medicine, 173, 1233-1239.
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
Yes.
The study determined whether prone ventilation
can decrease mortality in the course of ARDS.
1.2 The assignment of subjects to treatment groups is randomised. Yes.
Computer-generated random sequence was used.
1.3 An adequate concealment method is used.
Yes.
Sealed opaque envelopes were used.
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation. Can’t say.
The study didn’t mention.
1.5 The treatment and control groups are similar at the start of the trial. Yes.
p-value > 0.05
1.6 The only difference between groups is the treatment under
investigation.
Yes.
1.7 All relevant outcomes are measured in a standard, valid and reliable
way.
Yes.
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
completed?
Intervention group: 2.5%; control group: 3.2%
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).
Yes.
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias? Acceptable (+)
2.2 Taking into account clinical considerations, your evaluation of the methodology
used, and the statistical power of the study, are you certain that the overall effect
is due to the study intervention?
Yes.
The study was stopped due to decreased
patient accrual and was underpowered.
2.3 Are the results of this study directly applicable to the patient group targeted by
this guideline?
Yes.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which
it answers your question and mention any areas of uncertainty raised above.
Prone ventilation is feasible and safe, and may reduce mortality in patient with severe ARDS when it is initiated early
and applied for most of the day. The study conducted a good randomization. Blinding to patient is difficult to proceed.

72
S I G N
Methodology Checklist : Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Fernandez, R., Trenchs, X., Klamburg, J., Castedo, J., Serrano, J.M., Besso, G. et al. (2008). Prone positioning in acute respiratory
distress syndrome: a multicenter randomized clinical trial. Intensive Care Medicine, 34, 1487-1491.
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused
question.
Yes.
The objective of the study was to examine the effect
on survival of prone positioning in ARDS patients.
1.2 The assignment of subjects to treatment groups is randomised.
Yes.
Computer-generated random sequence was used.
1.3 An adequate concealment method is used.
Yes.
Centralized call centre
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
Can’t say. The study didn’t mention.
1.5 The treatment and control groups are similar at the start of the
trial.
Yes.
p-value > 0.05
1.6 The only difference between groups is the treatment under
investigation.
Yes.
1.7 All relevant outcomes are measured in a standard, valid and
reliable way.
Yes.
1.8 What percentage of the individuals or clusters recruited into
each treatment arm of the study dropped out before the study
was completed?
Intervention group: 8.7% ; Control group: 0%
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat
analysis).
No. The study didn’t mention.
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias? Acceptable (+)
2.2 Taking into account clinical considerations, your evaluation of the
methodology used, and the statistical power of the study, are you
certain that the overall effect is due to the study intervention?
Yes.
The study conducted with low recruitment of
patient. Low statistic power due to small sample
size.
2.3 Are the results of this study directly applicable to the patient group
targeted by this guideline?
Yes.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to
which it answers your question and mention any areas of uncertainty raised above.
Early continuous prone positioning benefit on survival in ARDS patients. The study conducted a good
randomization. Blinding to patient is difficult to proceed.

73
S I G N
Methodology Checklist : Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Taccone, P., Pesenti, A., Latini, R., Polli, F., Vagginelli, F., Mietto, C. et al. (2009). Prone positioning in patients with moderate
and severe acute respiratory distress syndrome. JAMA, 302(18), 1977-1984.
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
Yes.
The study assessed the benefits of prone
positioning in patients with moderate and
severe hypoxemia who are affected by ARDS.
1.2 The assignment of subjects to treatment groups is randomised.
Yes.
Computer-generated random sequence was
used.
1.3 An adequate concealment method is used.
Yes.
Allocation was done centrally by telephone on
a 24-hour-a-day, 7-day-a-week basis and was
based on a permuted-block algorithm.
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation. Yes.
Only investigators were blinded.
1.5 The treatment and control groups are similar at the start of the trial. Yes. No p-value shown.
1.6 The only difference between groups is the treatment under
investigation.
Yes
1.7 All relevant outcomes are measured in a standard, valid and reliable
way.
Yes
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
completed?
Intervention group: 1.2%, Control group: 1.1%.
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).
Yes.
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias? Acceptable (+)
2.2 Taking into account clinical considerations, your evaluation of the methodology used,
and the statistical power of the study, are you certain that the overall effect is due to the
study intervention?
Yes.
2.3 Are the results of this study directly applicable to the patient group targeted by this
guideline?
Yes.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to
which it answers your question and mention any areas of uncertainty raised above.
Prone positioning doesn’t provide significant survival benefit in patients with ARDS or in subgroups with moderate
and severe hypoxemia.

74
S I G N
Methodology Checklist : Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Robak, O., Schellongowski, P., Bojic, A., Laczika, K., Locker, G.J. & Staudinger, T. (2011). Short-term effects of combining
upright and prone positions in patients with ARDS: a prospective randomized study. Critical Care, 15.
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
Yes.
The study evaluated the effect of
combining upright and prone position on
gas exchange in patients with ALI or
ARDS.
1.2 The assignment of subjects to treatment groups is randomised.
Can’t say.
Randomization mentioned without method
specified.
1.3 An adequate concealment method is used.
Yes.
Sealed envelopes were used.
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation. Can’t say. Not mentioned.
1.5 The treatment and control groups are similar at the start of the trial. Yes. No p-value shown, claimed
insignificance.
1.6 The only difference between groups is the treatment under investigation. Yes.
1.7 All relevant outcomes are measured in a standard, valid and reliable way. Yes.
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was completed?
Not mentioned.
1.9 All the subjects are analysed in the groups to which they were randomly
allocated (often referred to as intention to treat analysis).
Does not apply.
All the subjects were analyzed as no drop
out was mentioned.
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Does not apply.
This is a single-centered study carried out
in a medical ICU.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias? Low quality (-)
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the
statistical power of the study, are you certain that the overall effect is due to the study
intervention?
Yes.
Not clear
randomization.
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline? Yes.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to
which it answers your question and mention any areas of uncertainty raised above.
Combining the prone position with the upright position with ALI or ARDS patients leads to further improvement
of oxygenation.

75
S I G N
Methodology Checklist : Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Guerin, C., Reignier, J., Richard, J.C., Beuret, P., Gacouin, A., Boulain, T. et al. (2013). Prone positioning in severe acute
respiratory distress syndrome. The New England Journal of Medicine, 368 (23), 2159-2168.
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused
question.
Yes.
They study evaluated the effect of prone position on
outcomes in patients with severe ARDS.
1.2 The assignment of subjects to treatment groups is
randomised.
Yes.
Computer-generated random sequence was used.
1.3 An adequate concealment method is used. Yes.
Centralized web based management system.
1.4 Subjects and investigators are kept ‘blind’ about
treatment allocation.
Yes.
Outcome assessor blinded.
1.5 The treatment and control groups are similar at the start
of the trial.
Yes. No p-value shown, claimed insignificance.
1.6 The only difference between groups is the treatment
under investigation.
Yes
1.7 All relevant outcomes are measured in a standard, valid
and reliable way.
Yes.
1.8 What percentage of the individuals or clusters recruited
into each treatment arm of the study dropped out before
the study was completed?
0%
1.9 All the subjects are analysed in the groups to which they
were randomly allocated (often referred to as intention to
treat analysis).
Yes.
1.10 Where the study is carried out at more than one site,
results are comparable for all sites.
Yes.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias? High quality (++)
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the
statistical power of the study, are you certain that the overall effect is due to the study
intervention?
Yes.
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline? Yes.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to
which it answers your question and mention any areas of uncertainty raised above.
Patients with ARDS and severe hypoxemia can benefit from prone treatment when it is used early and in relatively
long sessions.

76
Appendix 4 Summary of Critical Appraisal
Y=Yes , N=No, CS= Can’t say, NA= Does not apply, NM= Not mentioned
1 Gattinoni
et al 2001
2 Guerin et
al. 2004
3 Papazian
et al, 2005
4
Voggenieter
et al. 2005
5 Mancebo
et al. 2006
6 Fernandez
et al. 2008
7 Taccone et
al 2009
8 Robak et
al. 2011
9 Guerin et
al. 2013
1.1 Y Y Y Y Y Y Y Y Y
1.2 Y Y CS Y Y Y Y CS Y
1.3 Y Y Y Y Y Y Y Y Y
1.4 NM N NM NM NM NM Y NM Y
1.5 Y Y Y Y Y Y Y Y Y
1.6 Y Y Y Y Y Y Y Y Y
1.7 Y Y Y Y Y Y Y Y Y
1.8 NM 1%; 2.6% NM 0% 2.5%; 3.2% 8.7%; 0% 1.2%; 1% NM 0%
1.9 Y Y NA Y Y NM Y NA Y
1.10 Y Y NA Y Y Y Y NA Y
2.1 + + - + + + + - ++
2.2 Y Y Y Y Y Y Y Y Y
2.3 Y Y Y Y Y Y Y Y Y
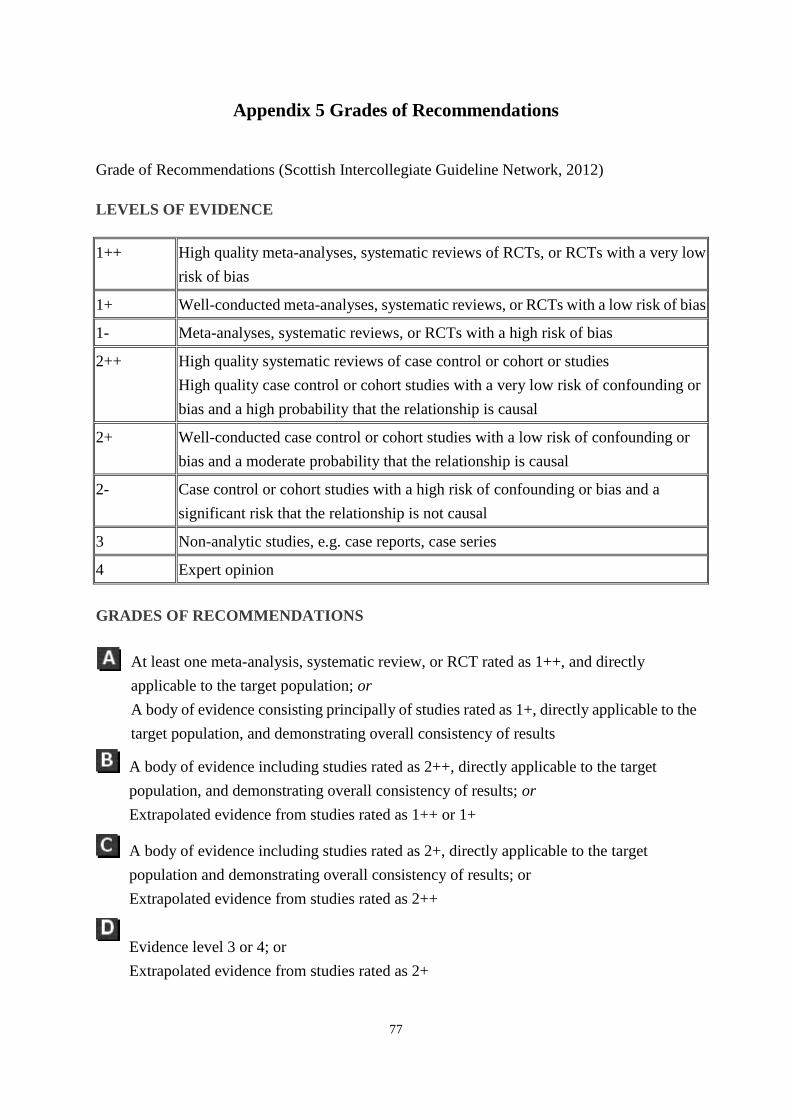
77
Appendix 5 Grades of Recommendations
Grade of Recommendations (Scottish Intercollegiate Guideline Network, 2012)
LEVELS OF EVIDENCE
1++ High quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low
risk of bias
1+ Well-conducted meta-analyses, systematic reviews, or RCTs with a low risk of bias
1- Meta-analyses, systematic reviews, or RCTs with a high risk of bias
2++ High quality systematic reviews of case control or cohort or studies
High quality case control or cohort studies with a very low risk of confounding or
bias and a high probability that the relationship is causal
2+ Well-conducted case control or cohort studies with a low risk of confounding or
bias and a moderate probability that the relationship is causal
2- Case control or cohort studies with a high risk of confounding or bias and a
significant risk that the relationship is not causal
3 Non-analytic studies, e.g. case reports, case series
4 Expert opinion
GRADES OF RECOMMENDATIONS
At least one meta-analysis, systematic review, or RCT rated as 1++, and directly
applicable to the target population; or
A body of evidence consisting principally of studies rated as 1+, directly applicable to the
target population, and demonstrating overall consistency of results
A body of evidence including studies rated as 2++, directly applicable to the target
population, and demonstrating overall consistency of results; or
Extrapolated evidence from studies rated as 1++ or 1+
A body of evidence including studies rated as 2+, directly applicable to the target
population and demonstrating overall consistency of results; or
Extrapolated evidence from studies rated as 2++
Evidence level 3 or 4; or
Extrapolated evidence from studies rated as 2+
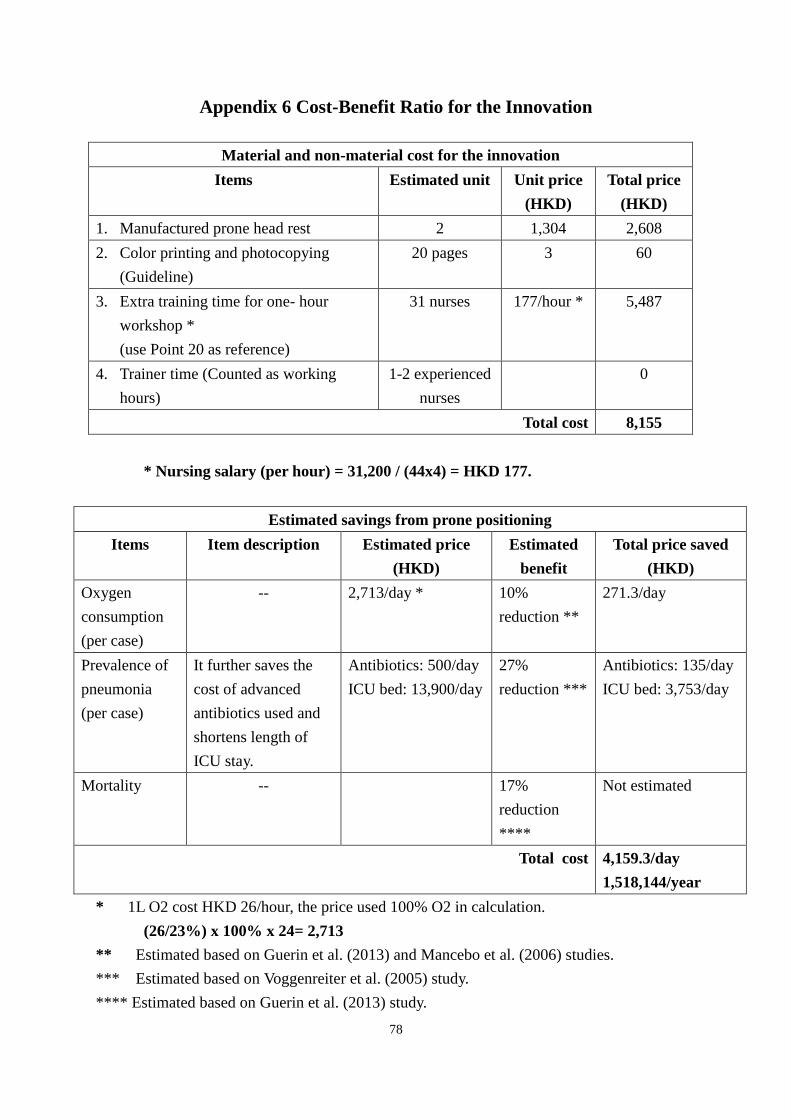
78
Appendix 6 Cost-Benefit Ratio for the Innovation
Material and non-material cost for the innovation
Items Estimated unit Unit price
(HKD)
Total price
(HKD)
1. Manufactured prone head rest 2 1,304 2,608
2. Color printing and photocopying
(Guideline)
20 pages 3 60
3. Extra training time for one- hour
workshop *
(use Point 20 as reference)
31 nurses 177/hour * 5,487
4. Trainer time (Counted as working
hours)
1-2 experienced
nurses
0
Total cost 8,155
* Nursing salary (per hour) = 31,200 / (44x4) = HKD 177.
Estimated savings from prone positioning
Items Item description Estimated price
(HKD)
Estimated
benefit
Total price saved
(HKD)
Oxygen
consumption
(per case)
-- 2,713/day * 10%
reduction **
271.3/day
Prevalence of
pneumonia
(per case)
It further saves the
cost of advanced
antibiotics used and
shortens length of
ICU stay.
Antibiotics: 500/day
ICU bed: 13,900/day
27%
reduction ***
Antibiotics: 135/day
ICU bed: 3,753/day
Mortality -- 17%
reduction
****
Not estimated
Total cost 4,159.3/day
1,518,144/year
* 1L O2 cost HKD 26/hour, the price used 100% O2 in calculation.
(26/23%) x 100% x 24= 2,713
** Estimated based on Guerin et al. (2013) and Mancebo et al. (2006) studies.
*** Estimated based on Voggenreiter et al. (2005) study.
**** Estimated based on Guerin et al. (2013) study.

79
Appendix 7 Recommendations of the Innovation
Recommendation 1.1 (Grade A)
Patients who have severe hypoxemia with PaO2/FiO2 ratio < 150mmHg, FiO2 ≥ 0.6 and
PEEP ≥ 5cm of water and require MV are benefit from prone positioning.
Evidence:
- Patients recruited in the studies met the American-European Consensus Conference
criteria for ARDS that PaO2/FiO2 ratio was equal to or less than 200mmHg. The mean of
PaO2/FiO2 ratio among the patients was below 150mmHg showed a significantly increase in
oxygenation (Fernandez et al., 2008 (1+); Gattinoni et al., 2001 (1+); Mancebo et al., 2006
(1+); Taccone et al., 2009 (1+); Robak et al., 2011 (1-)) and decrease in mortality after prone
positioning (Guerin et al., 2013 (1++)).
Recommendation 1.2 (Grade A)
Patients are contraindicated for prone positioning if they have cerebral edema with
elevated intracranial pressure >30mmHg and cerebral perfusion pressure <60mmHg, unstable
fractures of pelvic, femur or spine, severe hemodynamic instability, pregnancy and elevated
intra-abdominal pressure.
Evidence:
- Patients were excluded in the studies if their clinical condition were contraindicated for
prone positioning. (Fernandez et al., 2008 (1+); Gattinoni et al., 2001 (1+); Guerin et al.,
2004 (1+); Guerin et al., 2013 (1++); Mancebo et al., 2006 (1+); Papazian et al., 2005 (1-);
Robak et al., 2011 (1-); Taccone et al., 2009 (1+); Voggenreiter et al., 2005 (1+)).
Recommendation 2.1 (Grade A)
Prone positioning should be initiated within 36 hours upon ARDS diagnosis.
Evidence:
- Earlier prone positioning could be more effective in reducing incidence of VAP (Guerin
et al., 2004 (1+)), decreasing mortality (Guerin et al., 2013 (1++)), decreasing FiO2
consumption (Mancebo et al., 2006 (1+)) and increasing PaO2/FiO2 ratio (Fernandez et al.,
2008 (1+); Guerin et al., 2004 (1+); Guerin et al., 2013 (1++); Mancebo et al., 2006 (1+);
Papazian et al., 2005 (1-)).
80
Recommendation 2.2 (Grade A)
The duration of prone positioning should be at least 17hours/day.
Evidence:
- Patients experienced a mean prone positioning time was 17 hours/day (Guerin et al., 2013
(1++); Mancebo et al., 2006 (1+)), 18 hours/day (Taccone et al., 2009 (1+)) and 20 hours/day
(Fernandez et al., 2008 (1+)).
- Guerin et al. (2013, 1++) showed 17 hours/day for prone positioning significantly
decreased the mortality rate, increased PaO2/ FiO2 ratio without significant complications.
Recommendation 2.3 (Grade A)
Prone positioning should be continued at least 4 days.
Evidence:
- Prone positioning significantly increased more in PaO2/FiO2 ratio in the first 4 days
(Voggenreiter et al., 2005 (1+)).
- Studies performed prone positioning continuously until oxygenation improvement
(Fernandez et al., 2008 (1+); Gattinoni et al., 2001 (1+); Guerin et al., 2013 (1++); Papazian
et al., 2005 (1-)).
- Guerin et al. (2013, 1++) study continued prone positioning for average 4 ± 4 days per
patient. It improved patients’ oxygenation with PaO2/FiO2 ratio ≥ 150mmHg, PEEP ≤ 10cm
of water and FiO2 ≤ 0.6.
Recommendation 2.4 (Grade A)
Protective lung ventilation should be applied during prone positioning.
Evidence:
- Protective lung ventilation avoided alveolar overdistention and further reduced lung
injury. It also prevented alveolar collapse by maintaining open recruited alveoli (Papazian et
al., 2005 (1-)).
- Tidal volume was kept 6ml/kg of patients’ body weight, the end-inspiratory plateau
pressure ≤ 30cm of water and the respiratory rate of patient should not exceed 35breath/min.
PEEP setting was based on FiO2 requirements (Fernandez et al., 2008 (1+); Guerin et al.,
2013 (1++); Taccone et al., 2009 (1+); Voggenreiter et al., 2005 (1+)).
81
Recommendation 2.5 (Grade A)
Protective pads should support patients’ forehead, chest, knees and iliac crests during prone
positioning.
Evidence:
- With the use of protective pads, the abdominal movement was free and the presence of
pressure sore in prone positioning was statistically insignificant comparing with supine
position. (Guerin et al., 2013 (1++); Mancebo et al., 2006 (1+)).
Recommendation 2.6 (Grade A)
Patients’ heads and necks should be turned laterally every two hours during prone
positioning.
Evidence:
- Guerin et al. (2013, 1++) and Mancebo et al. (2006, 1+) turned patients’ heads and necks
alternatively to right or left in order to minimize the localized pressure successfully.
Recommendation 3.1 (Grade A)
Physiological variables of patients should be continuously monitored and documented just
before prone positioning, 1 hour after prone positioning, just before turning back to supine
position and 4 hours later.
Evidence:
- Blood gas analysis, pulse oximetry and ventilator variables were recorded to measure
oxygenation improvement (Fernandez et al., 2008 (1+); Gattinoni et al., 2001 (1+); Guerin et
al., 2004 (1+); Guerin et al., 2013 (1++); Mancebo et al., 2006 (1+); Papazian et al., 2005 (1-);
Robak et al., 2011 (1-); Taccone et al., 2009 (1+); Voggenreiter et al., 2005 (1+)).
- Continuous monitoring was preferred (Robak et al., 2011 (1-)).
- Biomedical variables used to monitor patients for non-pulmonary system failure such as
hepatic, renal, circulatory and coagulation failure (Gattinoni et al., 2001 (1+); Voggenreiter et
al., 2005 (1+)).
Recommendation 3.2 (Grade A)
Nurse should monitor and record the presence of VAP.
Evidence:
- VAP was detected by the presence of a new radiographic infiltrate, body temperature
greater than 38℃or lower than 36℃, purulent tracheal aspirates and total white cell count
lower than 4,000 × 10³µL or greater than 12,000 × 10³µL (Guerin et al., 2004 (1+);
Voggenreiter et al., 2005 (1+)).
82
Recommendation 3.3 (Grade A)
Patients’ skin integrity should be observed every shift.
Evidence:
- The presence, site and severity of pressure sores were recorded at baseline and daily
during morning assessment (Gattinoni et al., 2001 (1+); Guerin et al., 2004 (1+); Guerin et al.,
2013 (1++); Mancebo et al., 2006 (1+); Voggenreiter et al., 2005 (1+)).
- Pressure sores were classified according to the four stage system of the National Pressure
Ulcers Advisory Panel (Gattinoni et al., 2001 (1+)).
Recommendation 4.1 (Grade A)
Prone positioning should be terminated if patients’ oxygenation improves or deteriorates
and major complication occurs.
Evidence:
- Oxygenation improvement defined as PaO2/FiO2 ratio ≥ 150mmHg with PEEP ≤ 10cm
of water and FiO2 ≤ 0.6. It should be achieved at least 4 hours after turning back to supine
position (Fernandez et al., 2008 (1+); Guerin et al., 2004 (1+); Guerin et al., 2013 (1++);
Mancebo et al., 2006 (1+)).
- PaO2/FiO2 ratio deterioration noted when more than 20% reduction compared with
supine before two consecutive prone days (Guerin et al., 2013 (1++)).
- Major complications included non-scheduled extubation, endotracheal tube obstruction,
major desaturation with SpO2 <85% or PaO2 < 55mmHg for 5 minutes under FiO2=1.0,
hemodynamic instability with heart rate < 30 beats/min for 1 minute, systolic blood pressure
<60 mmHg for more than 5 minutes, cardiac arrest or any other life-threatening reason for
termination (Guerin et al., 2004 (1+); Guerin et al., 2013 (1++); Taccone et al., 2009 (1+)
Voggenreiter et al., 2005 (1+)). This complications directly affected the mortality rate of
patients (Mancebo et al., 2006 (1+)).
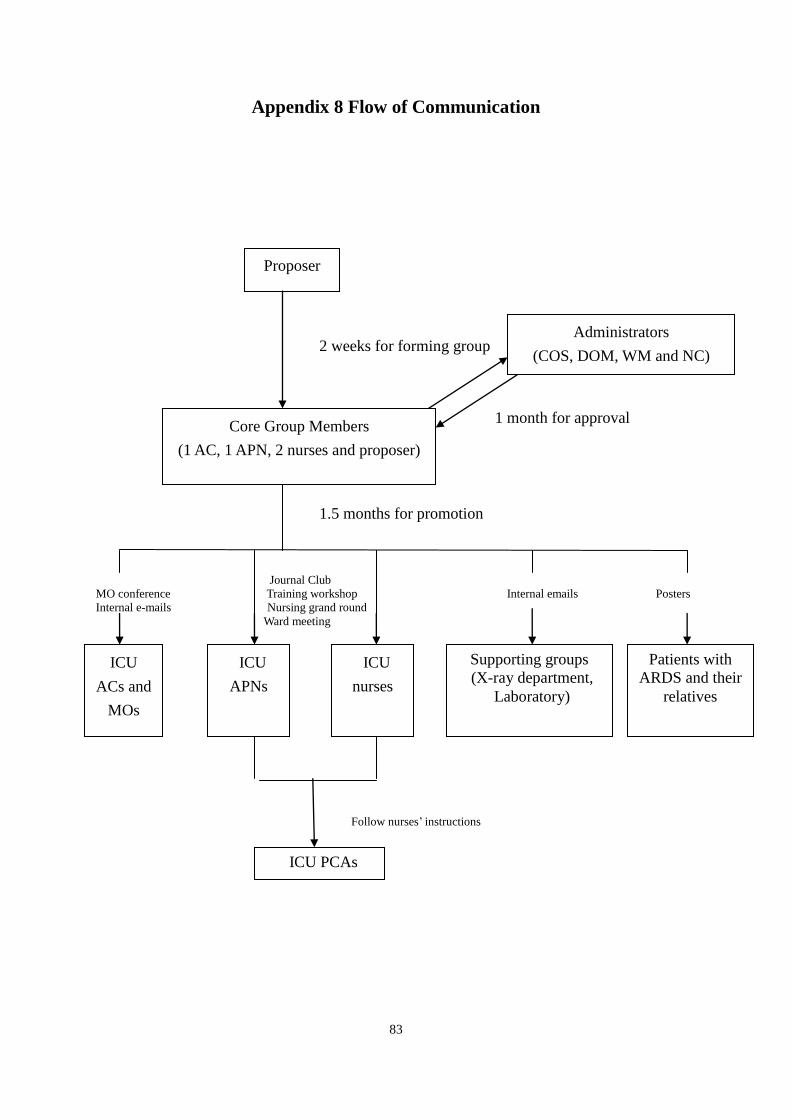
83
Appendix 8 Flow of Communication
2 weeks for forming group
1 month for approval
1.5 months for promotion
Journal Club
MO conference Training workshop Internal emails Posters
Internal e-mails Nursing grand round
Ward meeting
Follow nurses’ instructions
Proposer
Core Group Members
(1 AC, 1 APN, 2 nurses and proposer)
Administrators
(COS, DOM, WM and NC)
ICU
ACs and
MOs
ICU
APNs
ICU
nurses
Supporting groups
(X-ray department,
Laboratory)
ICU PCAs
Patients with
ARDS and their
relatives
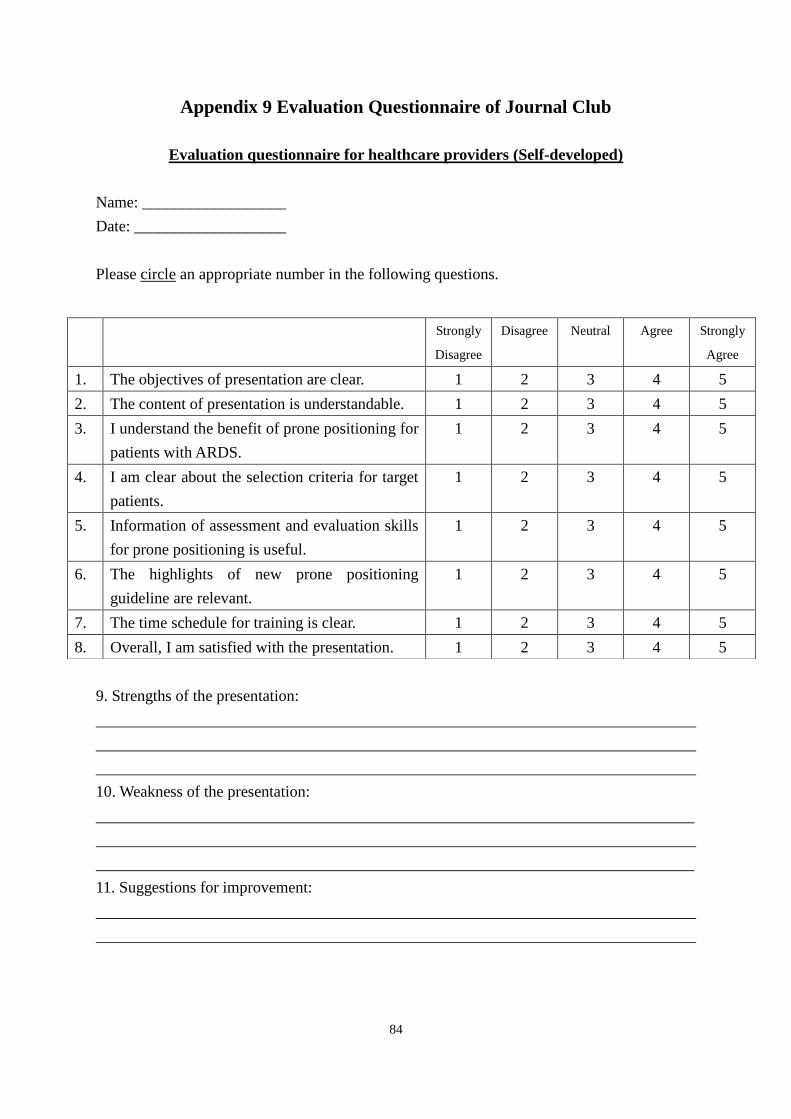
84
Appendix 9 Evaluation Questionnaire of Journal Club
Evaluation questionnaire for healthcare providers (Self-developed)
Name: __________________
Date: ___________________
Please circle an appropriate number in the following questions.
9. Strengths of the presentation:
10. Weakness of the presentation:
11. Suggestions for improvement:
Strongly
Disagree
Disagree Neutral Agree Strongly
Agree
1. The objectives of presentation are clear. 1 2 3 4 5
2. The content of presentation is understandable. 1 2 3 4 5
3. I understand the benefit of prone positioning for
patients with ARDS.
1 2 3 4 5
4. I am clear about the selection criteria for target
patients.
1 2 3 4 5
5. Information of assessment and evaluation skills
for prone positioning is useful.
1 2 3 4 5
6. The highlights of new prone positioning
guideline are relevant.
1 2 3 4 5
7. The time schedule for training is clear. 1 2 3 4 5
8. Overall, I am satisfied with the presentation. 1 2 3 4 5
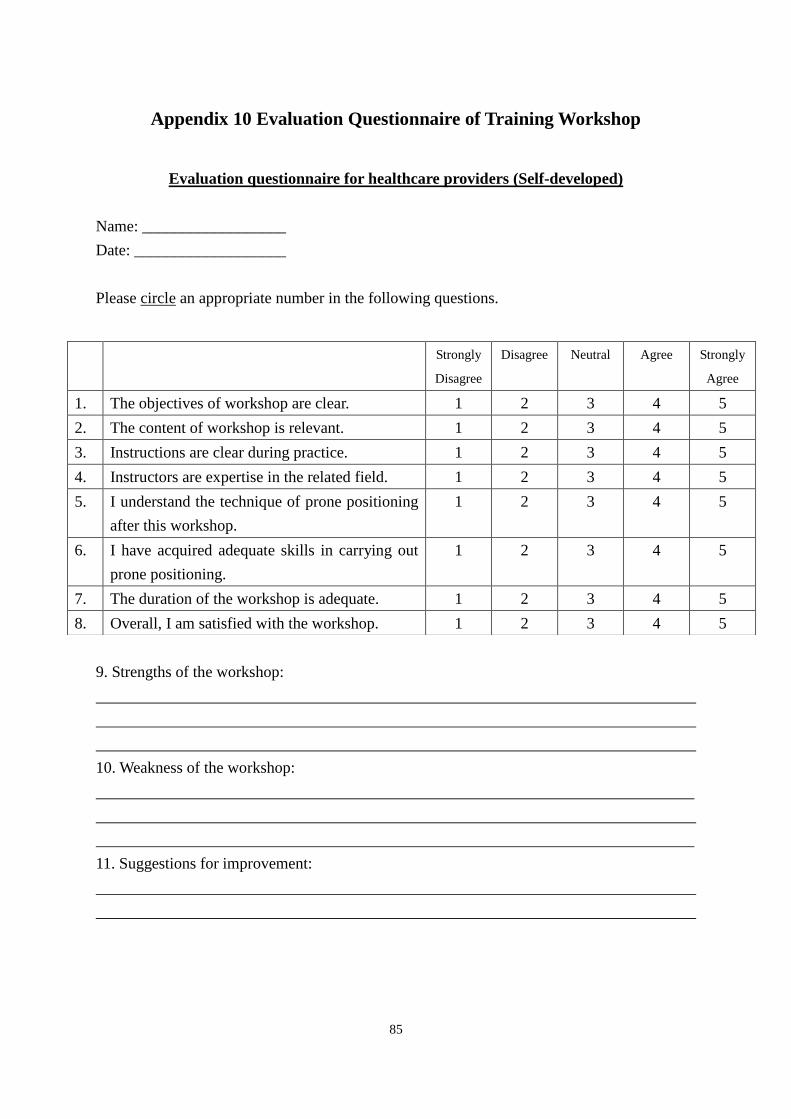
85
Appendix 10 Evaluation Questionnaire of Training Workshop
Evaluation questionnaire for healthcare providers (Self-developed)
Name: __________________
Date: ___________________
Please circle an appropriate number in the following questions.
9. Strengths of the workshop:
10. Weakness of the workshop:
11. Suggestions for improvement:
Strongly
Disagree
Disagree Neutral Agree Strongly
Agree
1. The objectives of workshop are clear. 1 2 3 4 5
2. The content of workshop is relevant. 1 2 3 4 5
3. Instructions are clear during practice. 1 2 3 4 5
4. Instructors are expertise in the related field. 1 2 3 4 5
5. I understand the technique of prone positioning
after this workshop.
1 2 3 4 5
6. I have acquired adequate skills in carrying out
prone positioning.
1 2 3 4 5
7. The duration of the workshop is adequate. 1 2 3 4 5
8. Overall, I am satisfied with the workshop. 1 2 3 4 5
86
Appendix 11 Evaluation Questionnaire of Pilot Study
Evaluation questionnaire for healthcare providers (Self-developed)
Name: __________________
Date: ___________________
Please circle an appropriate number in the following questions.
10. Strengths of the pilot study:
11. Difficulties encountered during the pilot study:
12. Suggestions for improvement:
Strongly
Disagree
Disagree Neutral Agree Strongly
Agree
1. The guideline is easy to carry out. 1 2 3 4 5
2. Time to carry out prone positioning is adequate. 1 2 3 4 5
3. Resources are adequate to implement the
guideline.
1 2 3 4 5
4. Supports are adequate to implement the
guideline.
1 2 3 4 5
5. Patients benefit from prone positioning. 1 2 3 4 5
6. The guideline is feasible to implement for long
term.
1 2 3 4 5
7. I am competent in conducting the guideline. 1 2 3 4 5
8. I am stressful in conducting the guideline. 1 2 3 4 5
9. My job satisfaction is increased by taking part
in the guideline.
1 2 3 4 5
10. I recommend the guideline to other staff. 1 2 3 4 5
11. Overall, the guideline is worth conducting. 1 2 3 4 5





























