Embed Size (px)
Citation preview

EVIDENCE-BASED DIGITAL HEALTH
Michael Bergen
02/22/2019

DISCLOSURE
• ( I have no disclosures )

PURPOSE
• Identify "clinically valid” digital health devices that can be
recommended/purchased by Duke Health for patients as it rolls out digital health
platforms

AIMS
• To evaluate the state of evidence-based literature describing the use of
digital health devices
• To identify problems and limitations of the current state of evidence-
based literature describing these devices
• To, hopefully, identify one or several devices that meet minimum
requirements to be safely recommended to Duke's patient population in
the following categories:

METRIC DEVICE
Glucometer
Sphygmomanometer
Watch
Scale
ECG
Thermometer
Glucose
Blood Pressure
Fitness, Heart Rate
Weight
Heart rhythm
Temperature

FDA MEDICAL DEVICE REGULATION 1
• The Medical Device Amendments of 1976 to the Federal Food, Drug and Cosmetic Act
(FDC Act)
• Class I (47%) – These devices present minimal potential for harm to the user (enema kits and elastic
bandages). 47% of medical devices fall under this category
• 95% of these are exempt from the regulatory process.
• Class II (43%) – higher risk than Class I; must undergo special controls (powered wheelchairs, some
pregnancy test kits).
• Must submit a 501(k) demonstrating “substantial equivalence” to a predicate device
• Class III (10%) – usually sustain or support life, are implanted, or present potential unreasonable risk of
illness or injury (implantable pacemakers, breast implants)
• Must submit a Premarket Approval (PMA) - valid scientific evidence collected from human clinical
trials showing the device is safe and effective for its intended use

GLUCOSE
• Why?
• 2019 American Diabetes Association recommendations2
• “Most patients using intensive insulin regimens … should assess glucose levels using self-monitoring of
blood glucose (or continuous glucose monitoring) …”
• “self-monitoring of blood glucose may help to guide treatment decisions and/or self-management for
patients taking less frequent insulin injections”
• “ensure that patients receive ongoing instruction and regular evaluation of technique, results, and their
ability to use data from self-monitoring of blood glucose to adjust therapy. Similarly, continuous glucose
monitoring use requires robust and ongoing diabetes education, training, and support”
• Evidence:
• IDD: evidence clearly supports SMBG (lower A1C, rates of daytime/nocturnal hypoglycemia)3
• NIDD: “A key consideration is that performing SMBG alone does not lower blood glucose levels. To be useful, the
information must be integrated into clinical and self-management plans."
• “Nearly 1 in 6 non-insulin-treated patients practiced SMBG without either the patient or physician using the
results”4

GLUCOSE
• Glucose Meter Accuracy2
• International Organization for Standardization (ISO 15197:2013)
• FDA standard (Class II)
• "In the U.S., currently marketed monitors must meet the standard under which they were approved, which may not be the
current standard.”2
• "Moreover, the monitoring of current accuracy is left to the manufacturer and not routinely checked by an independent source.”2
Association AD. Diabetes Technology: Standards of Medical Care in Diabetes—2019. Diabetes Care. 2019;42(Supplement 1):S71-S80.

GLUCOSE
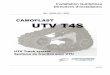
• The Diabetes Technology Society Blood Glucose Monitoring System Surveillance Program5
• 18 BGM’s representing 90% of products obtained by consumers from 2013-2015
• (only 6 of the top 18 glucose meters met the accuracy standard)
Klonoff DC, Parkes JL, Kovatchev BP,
et al. Investigation of the Accuracy of
18 Marketed Blood Glucose Monitors.
Diabetes Care. 2018;41(8):1681-1688.

GLUCOSE
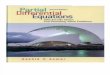
• Comparative Accuracy of 17 Point-of-Care Glucose Meters6

GLUCOSE
Ekhlaspour L, Mondesir D, Lautsch N, et al. Comparative Accuracy of 17
Point-of-Care Glucose Meters. J Diabetes Sci Technol. 2017;11(3):558-566.

GLUCOSE
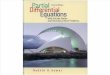
• Contour Next One
• MSRP: $19.99 – strips $0.83
• CONTOUR® DIABETES App compatible with iOS and Android
• 1) Data automatically exported from CONTOUR® DIABETES App to Apple Health via HealthKit integration
• Duke MyChart can periodically query Apple Health for updates
• 2) Data integrates into Glooko, which can be accessed by Epic or MyChart via public API
“Through REST-based APIs, Glooko
has integrated directly with… EPIC”
Glooko API
integrated
into Duke
MyChart app
CONTOUR® DIABETES App

GLUCOSE
• Accu-Chek Nano ($9.99 - strips $0.63)
• Accu-Chek Aviva (~$30 - strips $1.58)
iOS
Android
Glooko API integrated
into Duke MyChart app

GLUCOSE
• Overall
• Assortment of peer-reviewed literature on glucometer accuracy, but no standardized,
independent analysis
• Price is difficult to determine (especially for the test strips) due to variation in
insurance coverage
• Consumers likely turn to consumer reporting sites for help, which are fraught with
bias

BLOOD PRESSURE7
• Why?
• 103 million adults in the US with HTN; ~$131 Billion in costs each year
• Self-measured blood pressure (SMBP) is indicated for HTN, DM, ESRD, and others
• “Masked HTN”: ~ 30% in-office false negative rate
• “White coat HTN”: ~ 35% in-office false positive rate
• SMBP plus usual clinical care > usual clinical care alone7
• SMBP more predictive of all-cause and cardiac mortality than clinic BP
• ”Masked” HTN associated with greater risk of death than sustained HTN

BLOOD PRESSURE
• Cuff validation
• FDA class II
• Validation protocols:
• Improving the accuracy of blood pressure measurement: the influence of the European Society of Hypertension International Protocol (ESH-
IP) for the validation of blood pressure measuring devices and future perspectives (Stergiou et al.)8
• 323 home BP monitors, 12 validated in children, 25 validated in pregnancy
• American Pharmacists Association, American Medical Association (AMA), Association for the Advancement of Medical
Instrumentation (AAMI), American Heart Association (AHA), American Society of Hypertension (ASH), and Canadian
Hypertension Education Program (CHEP)
• Coalition for Accurate Measurement of Blood Pressure (CAMBP) with the intent to develop a publicly available Validated Blood
Pressure Device Listing (VDL) by Nov 2017
• So where is it?

BLOOD PRESSURE
• Target: BP (AMA + AHA)
• Minimum recommended requirements
• Automatic inflation functionality.
• Upper arm cuff (unless the patient’s arm circumference is too large—in which case, use of a wrist device with proper technique is acceptable).
• Large screen for patients with poor eyesight.
• Optional Bluetooth connectivity to allow patients to synchronize with other devices.
• Date and time stamp for review of readings.
• Memory to store at least 30 BP readings.
• Ability to average 2 to 3 blood pressure readings taken over 10 minutes or less if possible.
• Clinically validated device tested for accuracy
• Proper cuff sizing
• Public protocol and data collection system for health systems to join
• https://targetbp.org

BLOOD PRESSURE
• Omron 10 Series (BP786, HEM-7321T-Z)• Validated under the European Society of Hypertension International Protocol9
• $69.99

LIMITATIONS & CHALLENGES
• Sharing devices is not always user-friendly
• Lag between new technology and clinical validation
• Major shortcomings of clinical validation protocol

REFERENCES
1. https://www.fda.gov/medicaldevices/resourcesforyou/consumers/ucm142523.htm
2. Association AD. Diabetes Technology: Standards of Medical Care in Diabetes—2019. Diabetes Care. 2019;42(Supplement 1):S71-S80.
3. Garber AJ. Treat-to-target trials: uses, interpretation and review of concepts. Diabetes Obes Metab. 2014;16(3):193-205
4. Grant RW, Huang ES, Wexler DJ, et al. Patients who self-monitor blood glucose and their unused testing results. Am J ManagCare. 2015;21(2):e119-129.
5. Klonoff DC, Parkes JL, Kovatchev BP, et al. Investigation of the Accuracy of 18 Marketed Blood Glucose Monitors. Diabetes Care. 2018;41(8):1681-1688.
6. Ekhlaspour L, Mondesir D, Lautsch N, et al. Comparative Accuracy of 17 Point-of-Care Glucose Meters. J Diabetes Sci Technol. 2017;11(3):558-566.
7. Banegas JR, Ruilope LM, de la Sierra A, et al. Relationship between Clinic and Ambulatory Blood-Pressure Measurements and Mortality. N Engl J Med. 2018;378(16):1509-1520
8. Stergiou GS, Asmar R, Myers M, et al. Improving the accuracy of blood pressure measurement: the influence of the European Society of Hypertension International Protocol (ESH-IP) for the validation of blood pressure measuring devices and future perspectives. J Hypertens. 2018;36(3):479-487.
9. Belghazi J, El Feghali RN, MoussalemT, Rejdych M, Asmar RG. Validation of four automatic devices for self-measurement of blood pressure according to the International Protocol of the European Society of Hypertension. Vasc Health Risk Manag. 2007;3(4):389-400