Embed Size (px)
Citation preview

Pergamon
0 Clinical Original Contribution
Int. J. Radiation Oncology Biol. Phys., Vol. 30, No. 5, pp. 1083-1090, 1994 Copyright 0 1994 Ekvier Science Ltd Printed in the USA. All rights reserved
0360-3016/94 $6.00 + .OO
03603016(94)00376-9
EVALUATION OF WHOLE ABDOMINAL IRRADIATION IN OVARIAN CARCINOMA WITH A FOUR ORTHOGONAL FIELDS TECHNIQUE
LAURENCE THOMAS,* JACQUES PIGNEUX,* JACQUES CHAUVERGNE,~ EBERHARD STUCIUE,~ EMMANUEL BUSSI&RES,~ ANTONY CHEMIN* AND CLAUDE TOULOUSE§
*Department of Radiation Oncology, +Department of Medical Oncology, *Department of Surgery, “Department of Biostatistics, Fondation Bergon%, Comprehensive Cancer Center, 180, rue de Saint-Gengs, 33076 Bordeaux Cedex, France
Purpose: The purpose of this study is to evaluate the toxicity and the results of ahdominopelvic irradiation with a four orthogonal field’s technique in patients with ovarian carcinoma. Methods and Materials: Between May 1981 and December 1990, 167 patients with ovarian carcinoma have been treated with whole abdominal irradiation: 62 patients with no or minimal residual disease < 2 cm after initial surgery (group 1) and 105 patients with no residual disease or macroscopic residual disease < 2 cm assessed by second-look surgery after incomplete debulking surgery and cisplatin-based polychemotherapy (group 2). Irradiation was performed by a four orthogonal field’s technique. Thirty grays were given with a 25 MV photon beam (1.5 Gy/fraction/day, 20 fractions over 30 days). Boosts were performed in 50 cases (median dose of 15 Gy). Results: With a median follow-up of 68 months, the 5-year actuarial survival rate was 50% in the entire group, -group 1,40% in group 2, and 84% in Tl, 61.5% in T2,38% in T3. Five-year actuarial survival was analyzed according to the residuum: (a) after initial surgery (no residual disease: 70%, residual disease: 36.5%), (b) after second-look surgery: 76% in patients with a negative second look, 66% in patients with microscopic residual disease, 22% in patients with macroscopic residual disease and secondary surgical reduction, and 10% in patients with small unresectable nodules. Nine percent of the patients failed to complete irradiation acute side effects related. Five percent required surgery for bowel obstruction. Conclusion: The abdominopelvic irradiation with this four orthogonal field’s technique was associated with tolerable acute toxicity and a low risk of serious late complications. Similar late results to have been reported whole abdominal irradiation with chemotherapy in patients with negative or microscopic residual disease after surgery. Randomized trials comparing these two adjuvant treatments are warranted.
Ovarian carcinoma, Four orthogonal fields technique, Whole abdominal irradiation.
INTRODUCI’ION
The nature of further treatment following surgery in the management of ovarian carcinoma is still controversial.
In 1980, Dembo and Delclos have published the results of a randomized study comparing pelvic radiation therapy alone or with chlorambucil and abdominopelvic radio- therapy in patients who had minimal residual disease after primary surgery. They concluded that whole abdominal irradiation was curative for patients Stage Ib, II, III with small residuum ( 12- 14).
At the same time, the use of cisplatin containing che- motherapy extended because of excellent response rates in advanced ovarian disease (7, 10,37). It raised the ques- tion of the real benefit of whole abdominal irradiation in the treatment of ovarian carcinoma. To answer this ques- tion, in 1982 a multicenter trial in French Centers was initiated. In this trial, the patients with no residual disease or minimal residual disease < 2 cm after initial surgery,
were randomized to receive abdominopelvic irradiation or adjuvant cisplatin based chemotherapy. The patients with residual disease after initial surgery received cisplatin based chemotherapy (two regimens were randomized). Then, they underwent second-look laparotomy and the patients with no residual disease or disease x 2 cm were randomized to receive abdominopelvic irradiation or chemotherapy. We used in this trial an original open field technique with four orthogonal fields. From these data, all our patients are treated according to this technique.
We report here the acute and late toxicity of this tech- nique and the results.
METHODS AND MATERIALS
Patients From May 198 1 through December 1990, 167 patients
with ovarian carcinoma have been treated with whole ab-
Reprint requests to: Laurence Thomas, M.D. Accepted for publication 1 July 1994.
1083
1084 I. J. Radiation Oncology 0 Biology 0 Physics
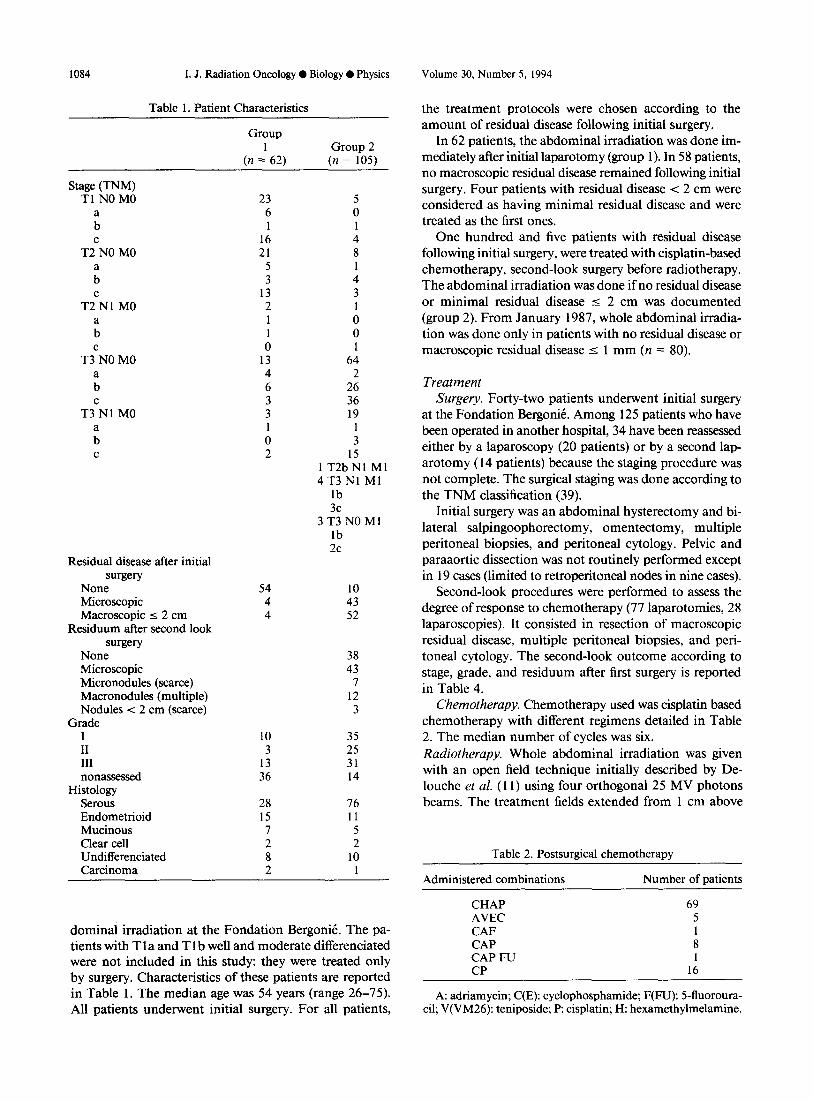
Table 1. Patient Characteristics
Group
(n =’ 62) Group 2
(n = 105)
Stage (TNM) Tl NO MO
:
T2CN0 MO
:
T2CNl MO
:
T3CN0 MO
:
T3CN1 MO
: C
Residual disease after initial surgery
None Microscopic Macroscopic 5 2 cm
Residuum after second look surgery
None Microscopic Micronodules (scarce) Macronodules (multiple) Nodules < 2 cm (scarce)
Grade
iI III nonassessed
Histology Serous Endometrioid Mutinous Clear cell Undifferentiated Carcinoma
23 5 6 0
16 21
5 3
13 2 1 1 0
13 4 6 3 3
0 2
54 10 4 43 4 52
10 35 3 25
13 31 36 14
28 15 I 2 8 2
4 8
4 3
0 0
64 2
26 36 19
1 3
15 1 T2b Nl Ml 4T3Nl Ml
lb 3c
3T3NOMl lb 2c
38 43
7 12 3
76 11 5 2
10
dominal irradiation at the Fondation Bergon& The pa- tients with T 1 a and T 1 b well and moderate differentiated were not included in this study: they were treated only by surgery. Characteristics of these patients are reported in Table 1. The median age was 54 years (range 26-75). All patients underwent initial surgery. For all patients,
Volume 30, Number 5, 1994
the treatment protocols were chosen according to the amount of residual disease following initial surgery.
In 62 patients, the abdominal irradiation was done im- mediately after initial laparotomy (group 1). In 58 patients, no macroscopic residual disease remained following initial surgery. Four patients with residual disease < 2 cm were considered as having minimal residual disease and were treated as the first ones.
One hundred and five patients with residual disease following initial surgery, were treated with cisplatin-based chemotherapy, second-look surgery before radiotherapy. The abdominal irradiation was done if no residual disease or minimal residual disease 5 2 cm was documented (group 2). From January 1987, whole abdominal irradia- tion was done only in patients with no residual disease or macroscopic residual disease s 1 mm (n = 80).
Treatment Surgery. Forty-two patients underwent initial surgery
at the Fondation Bergonit. Among 125 patients who have been operated in another hospital, 34 have been reassessed either by a laparoscopy (20 patients) or by a second lap- arotomy (14 patients) because the staging procedure was not complete. The surgical staging was done according to the TNM classification (39).
Initial surgery was an abdominal hysterectomy and bi- lateral salpingoophorectomy, omentectomy, multiple peritoneal biopsies, and peritoneal cytology. Pelvic and paraaortic dissection was not routinely performed except in 19 cases (limited to retroperitoneal nodes in nine cases).
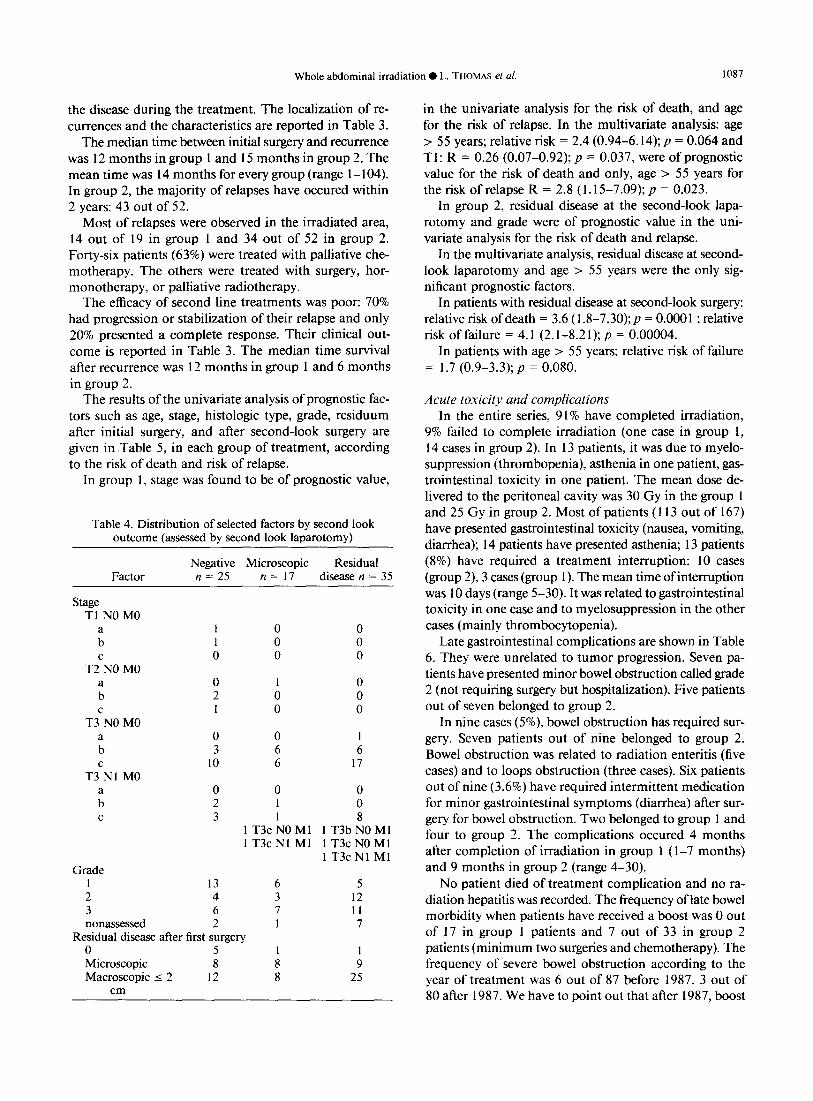
Second-look procedures were performed to assess the degree of response to chemotherapy (77 laparotomies, 28 laparoscopies). It consisted in resection of macroscopic residual disease, multiple peritoneal biopsies, and peri- toneal cytology. The second-look outcome according to stage, grade, and residuum after first surgery is reported in Table 4.
Chemotherapy. Chemotherapy used was cisplatin based chemotherapy with different regimens detailed in Table 2. The median number of cycles was six. Radiotherapy. Whole abdominal irradiation was given with an open field technique initially described by De- louche et al. (11) using four orthogonal 25 MV photons beams. The treatment fields extended from 1 cm above
Table 2. Postsurgical chemotherapy
Administered combinations Number of patients
CHAP 69 AVEC 5 CAF 1 CAP 8 CAP FU 1 CP 16
A: adriamycin; C(E): cyclophosphamide; F(FU): 5-fluoroura- cil; V(VM26): teniposide; P: cisplatin; H: hexamethylmelamine.
Whole abdominal irradiation 0 L. THOMAS et al. 1085
the diaphragms to below the peritoneal reflections. For the anterior and posterior fields, a liver shield was made for the right liver only. Its shape ensured an adequate irradiation of the right hemidiaphragm, the paraaortic area, and the right paracolic gutter. A posterior renal shield was set at the beginning of irradiation.
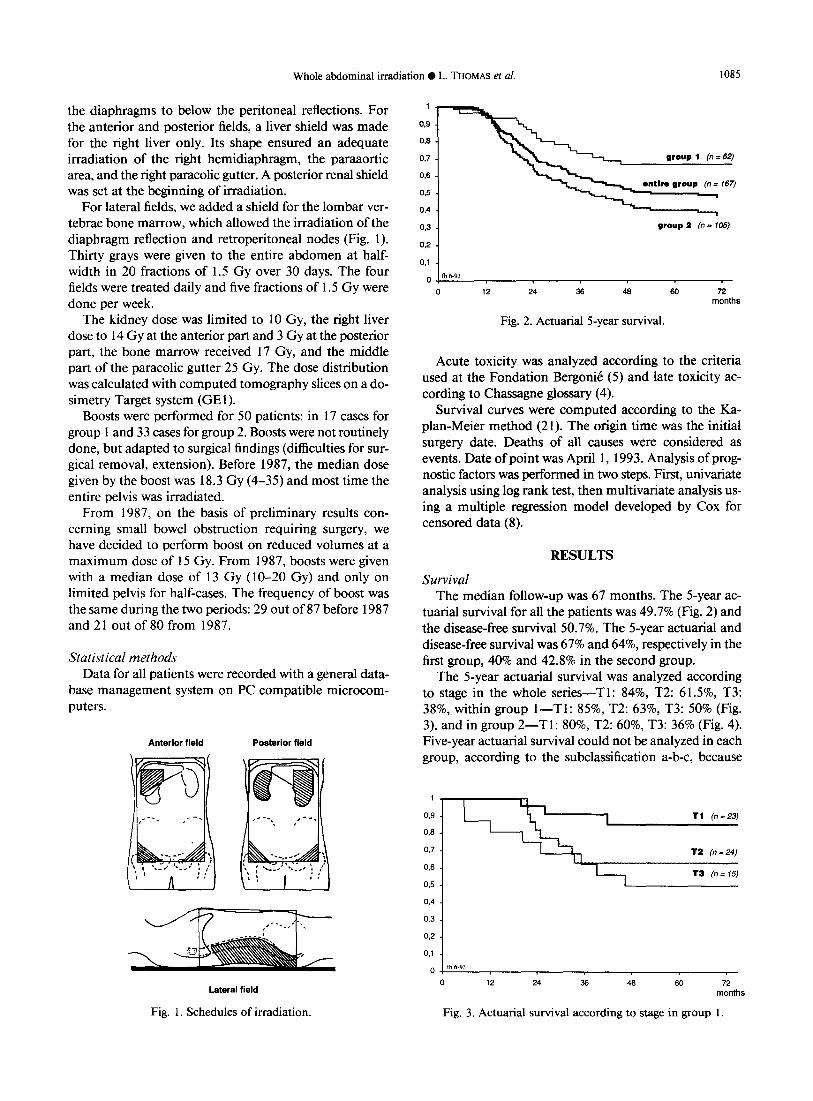
For lateral fields, we added a shield for the lombar ver- tebrae bone marrow, which allowed the irradiation of the diaphragm reflection and retroperitoneal nodes (Fig. 1). Thirty grays were given to the entire abdomen at half- width in 20 fractions of 1.5 Gy over 30 days. The four fields were treated daily and five fractions of 1.5 Gy were done per week.
The kidney dose was limited to 10 Gy, the right liver dose to 14 Gy at the anterior part and 3 Gy at the posterior part, the bone marrow received 17 Gy, and the middle part of the paracolic gutter 25 Gy. The dose distribution was calculated with computed tomography slices on a do- simetry Target system (GEl).
Boosts were performed for 50 patients: in 17 cases for group 1 and 33 cases for group 2. Boosts were not routinely done, but adapted to surgical findings (difficulties for sur- gical removal, extension). Before 1987, the median dose given by the boost was 18.3 Gy (4-35) and most time the entire pelvis was irradiated.
From 1987, on the basis of preliminary results con- cerning small bowel obstruction requiring surgery, we have decided to perform boost on reduced volumes at a maximum dose of 15 Gy. From 1987, boosts were given with a median dose of 13 Gy (lo-20 Gy) and only on limited pelvis for half-cases. The frequency of boost was the same during the two periods: 29 out of 87 before 1987 and 21 out of 80 from 1987.
Statistical methods Data for all patients were recorded with a general data-
base management system on PC compatible microcom- puters.
Anterior field Posterior field
Lateral field
Fig. 1. Schedules of irradiation.
03
03
0,7
0,6
0.5
0.4
0,3
0,2
0.1
0 m 6-93
0 12 24 36 48 60 72 months
Fig. 2. Actuarial 5-year survival.
Acute toxicity was analyzed according to the criteria used at the Fondation Bergonit? (5) and late toxicity ac- cording to Chassagne glossary (4).
Survival curves were computed according to the Ka- plan-Meier method (21). The origin time was the initial surgery date. Deaths of all causes were considered as events. Date of point was April 1, 1993. Analysis of prog- nostic factors was performed in two steps. First, univariate analysis using log rank test, then multivariate analysis us- ing a multiple regression model developed by Cox for censored data (8).
RESULTS
Survival The median follow-up was 67 months. The 5-year ac-
tuarial survival for all the patients was 49.7% (Fig. 2) and the disease-free survival 50.7%. The 5-year actuarial and disease-free survival was 67% and 64%, respectively in the first group, 40% and 42.8% in the second group.
The 5-year actuarial survival was analyzed according to stage in the whole series-Tl: 84%, T2: 6 1.5%, T3: 38%, within group I-Tl: 85%, T2: 63%, T3: 50% (Fig. 3), and in group 2-Tl: 80%, T2: 60%, T3: 36% (Fig. 4). Five-year actuarial survival could not be analyzed in each group, according to the subclassification a-b-c, because
I Tl (n=23)
0,7 - t2 (n=24)
0.6 - T3 (n= 15)
0,5 -
0,4 - 0.3 -
0,2 -
0.1 -
0, m 6.93
0 12 24 36 46 60 72 months
Fig. 3. Actuarial survival according to stage in group 1.

1086
1 -
03 - 0.8 -
Or7 -
0.6 -
03 -
0.4 -
03 -
0.2 -
0.1 -
0, m 6-w
0
I. J. Radiation Oncology 0 Biology 0 Physics
Ti (ll=5)
T2 (II = 10)
24 36 46 60 72
months
Fig. 4. Actuarial survival according to stage in group 2.
the subset of patients in each category was too small, ex- cept in group 2 for T3b: 4 1% and for T3c: 30%.
The 5-year actuarial survival was analyzed according to histological types in the entire group: serous (43.6%), other types (59.6%).
Five-year survival was analyzed according to grading, but we have to point out that the number of grade 2 was small (grade 1: 62%, grade 2: 24%, grade 3: 38%).
Analyzed according to the residuum following initial surgery, the 5-year actuarial survival was: with residual disease 36.5%, and with no residual disease 70% (Fig. 5). According to the size of residual disease at second-look laparotomy (Fig. 6), the 5-year actuarial survival in pa- tients with negative second look was: 76%, with micro- scopic residual disease: 60% (positive cytology or positive random biopsies). In patients with a macroscopic positive second-look laparotomy even after debulking, the 5-year actuarial survival was 22% and 10% with small residual unresectable nodules.
The 5-year recurrence and metastasis rates in patients with negative second-look surgery, were 30% and 15%, respectively. The 5-year recurrence and metastasis rates
006 -
0,5 -
0,4 _
03 -
0,2 -
0,l - b6.93
0,
0 12 24 36 46 60 72
months
Fig. 5. Actuarial survival according to tumor rest at initial sur- gery.
Volume 30, Number 5, 1994
o rn6-93
0 12 24 36 46 60 72 monl
Fig. 6. Actuarial survival according to residual disease at second look laparotomy.
in patients with microscopic residual disease at second- look laparotomy were 35% and 14%, respectively, and in patients with macroscopic disease, even after debulking, 80% and 57%, respectively.
We have observed 73 recurrences in the whole series: 21 (group l), 52 (group 2).
Five patients in group 2 have presented progression of
Table 3. Recurrences
Group 1 Group 2 (2 1 out of 62) (52 out of 105)
Stage T Tl 6123
T2 8123 T3 7116
N Nl 1 M Ml 0
Grade 1 2 2 1 3 8 nonassessed 10
Site Regional 14 Metastasis 4 Associated 3
(regional + metastasis)
Residual disease (initial surgery)
None 18 Residual 3
Residuum (second look laparotomy)
None Microscopic Macroscopic
Outcome Dead from cancer 17 Dead (other cause) 1 Alive with cancer 1 Alive 2
115 3110
48190 12 5
13 18 16 5
34 6
12
5 47
12 28 12
46 2 4
Whole abdominal irradiation 0 L. THOMAS et al. 1087
the disease during the treatment. The localization of re- currences and the characteristics are reported in Table 3.
The median time between initial surgery and recurrence was 12 months in group 1 and 15 months in group 2. The mean time was 14 months for every group (range 1- 104). In group 2, the majority of relapses have occured within 2 years: 43 out of 52.
Most of relapses were observed in the irradiated area, 14 out of 19 in group 1 and 34 out of 52 in group 2. Forty-six patients (63%) were treated with palliative che- motherapy. The others were treated with surgery, hor- monotherapy, or palliative radiotherapy.
The efficacy of second line treatments was poor: 70% had progression or stabilization of their relapse and only 20% presented a complete response. Their clinical out- come is reported in Table 3. The median time survival after recurrence was 12 months in group 1 and 6 months in group 2.
The results of the univariate analysis of prognostic fac- tors such as age, stage, histologic type, grade, residuum after initial surgery, and after second-look surgery are given in Table 5, in each group of treatment, according to the risk of death and risk of relapse.
In group 1, stage was found to be of prognostic value,
Table 4. Distribution of selected factors by second look outcome (assessed by second look laparotomy)
Factor Negative Microscopic Residual n = 25 n= 17 disease n = 35
Stage Tl NO MO
:
T2CN0 MO
;
T3CN0 MO a b C
T3 NI MO
: C
Grade
0
0 2 1
0 0 1 3 6 6
10 6 17
0 2 3
13 6 5 4 3 12 6 7 11 2 1 7
0 0 0 0 0 0
:, 0 0
0 0
0 0 1 0 1 8
1 T3cNOMl 1 T3bNOMl 1 T3cNl Ml 1 T3cNOMl
1 T3c Nl Ml
Residual disease after first surgery 0 5 1 1 Microscopic 8 8 9 Macroscopic 5 2 12 8 25
cm
in the univariate analysis for the risk of death, and age for the risk of relapse. In the multivariate analysis: age > 55 years; relative risk = 2.4 (0.94-6.14); p = 0.064 and Tl: R = 0.26 (0.07-0.92); p = 0.037, were of prognostic value for the risk of death and only, age > 55 years for the risk of relapse R = 2.8 (1.15-7.09); p = 0.023.
In group 2, residual disease at the second-look lapa- rotomy and grade were of prognostic value in the uni- variate analysis for the risk of death and relapse.
In the multivariate analysis, residual disease at second- look laparotomy and age > 55 years were the only sig- nificant prognostic factors.
In patients with residual disease at second-look surgery: relative risk of death = 3.6 (1.8-7.30); p = 0.0001 ; relative risk of failure = 4.1 (2.1-8.21); p = 0.00004.
In patients with age > 55 years: relative risk of failure = 1.7 (0.9-3.3); p = 0.080.
Acute toxicity and complications In the entire series, 9 1% have completed irradiation,
9% failed to complete irradiation (one case in group 1, 14 cases in group 2). In 13 patients, it was due to myelo- suppression (thrombopenia), asthenia in one patient, gas- trointestinal toxicity in one patient. The mean dose de- livered to the peritoneal cavity was 30 Gy in the group 1 and 25 Gy in group 2. Most of patients (113 out of 167) have presented gastrointestinal toxicity (nausea, vomiting, diarrhea); 14 patients have presented asthenia; 13 patients (8%) have required a treatment interruption: 10 cases (group 2), 3 cases (group 1). The mean time of interruption was 10 days (range 5-30). It was related to gastrointestinal toxicity in one case and to myelosuppression in the other cases (mainly thrombocytopenia).
Late gastrointestinal complications are shown in Table 6. They were unrelated to tumor progression. Seven pa- tients have presented minor bowel obstruction called grade 2 (not requiring surgery but hospitalization). Five patients out of seven belonged to group 2.
In nine cases (5%) bowel obstruction has required sur- gery. Seven patients out of nine belonged to group 2. Bowel obstruction was related to radiation enteritis (five cases) and to loops obstruction (three cases). Six patients out of nine (3.6%) have required intermittent medication for minor gastrointestinal symptoms (diarrhea) after sur- gery for bowel obstruction. Two belonged to group 1 and four to group 2. The complications occured 4 months after completion of irradiation in group 1 (l-7 months) and 9 months in group 2 (range 4-30).
No patient died of treatment complication and no ra- diation hepatitis was recorded. The frequency of late bowel morbidity when patients have received a boost was 0 out of 17 in group 1 patients and 7 out of 33 in group 2 patients (minimum two surgeries and chemotherapy). The frequency of severe bowel obstruction according to the year of treatment was 6 out of 87 before 1987, 3 out of 80 after 1987. We have to point out that after 1987, boost

1088 I. J. Radiation Oncology 0 Biology 0 Physics Volume 30, Number 5, 1994
Table 5. Prognostic factors analysis
Prognostic Factor
Age > 55
Stage Tl vs.T2+T3
Tl +T2vs.T3 Histology
Serous vs. others Grade
Residual disease after initial surgery 0 + micro/macro
Residual disease after second look laparotomy
Group 1 Group 2
Risk of Risk of Risk of Risk of death relapse death relapse
p = 0.0563 p = 0.0189 p = 0.1312 p = 0.0764 S
p = 0.0169 p = 0.23 p = 0.6949 p = 0.66 S
p = 0.0879 p = 0.27 p = 0.1148 p = 0.10
p = 0.2180 p = 0.93 p = 0.3624 p = 0.95 p = 0.40 p = 0.15 p = 0.04 p = 0.037
S S p = 0.06 p = 0.34 p = 0.1159 p = 0.11
- - p = 0.0005 p = 0.0001
SL SL
were performed on reduced volumes at a maximum dose level of 15 Gy.
DISCUSSION
For patients with ovarian carcinoma, surgical treatment is not sufficient in the great majority of cases. The type of further treatment is still controversial. In our study we
Table 6. Gastrointestinal toxicity
Group 1 Group 2
Number of
patients
Subobstruction
Bowel obstruction Grade 2 Grade 3
Gastrointestinal symptoms
Grade 1
Grade 2
Bowel obstruction Grade 2 Grade 3
Subobstruction Grade 2
Gastrointestinal symptoms
Grade I
Grade 2
1 3 4 16
1 2 3 2 7 9
0 1 6
1 4
treated conservatively treated surgically
bowel obstruction incomplete treated conservatively
toxicity treated with medication In group 1, stage and age were prognostic in the uni- during less than one month variate analysis and in the multivariate analysis: risk of
treatment necessary more than one death = 2.4 in patients with age > 55 years and 0.26 in month patients presenting T 1.
have treated 167 patients with abdominopelvic irradiation either after surgery alone (group 1) or after chemotherapy and second-look surgery (group 2). Our results (5-year actuarial survival of 67% in group 1 and 40% in group 2) are similar to those reported by many authors with ab- dominopelvic irradiation (13, 23, 25, 27, 40).
We have to point out that the tolerance of four or- thogonal fields technique was good: only 9% of patients have failed to complete irradiation ( 1 case in group 1, 14 cases in group 2) mainly due to myelosuppression (thrombocytopenia). In the majority of reported data, 30% of patients had a definitive irradiation interruption due to a clinical or hematological toxicity ( 1, 16, 19). Severe small bowel obstruction requiring surgery were observed in nine patients (5%). Higher rates of complications have been reported in the literature especially after chemo- therapy (3, 17, 19, 36, 41).
The frequency of late bowel morbidity was high (7 out of 33) in group 2 patients (two surgeries + chemotherapy) who have received a boost. This is in agreement with other authors findings (36,40, 41).
Some factors have been found to be prognostic: age, stage, histology, grade, residual disease after initial and second-look surgery (1,6,9, 13, 16,20,24,28, 34,40,42).
In our series, these factors were studied in an univariate and multivariate analysis in each group of patients. Re- sidual disease after initial surgery was not found as prog- nostic. The fact that this criteria was chosen as the basis of treatment selection could explain why it did not appear when it was analyzed in each group.

Whole abdominal irradiation 0 L. THOMAS et al. 1089
In early stages, controversial results about adjuvant treatment after inital surgery have been reported even in randomized trials (12, 22, 35). This could be explained by the fact that the surgical staging procedures could be different or incomplete. We have to point out with Young, Trimbos, and Monga (30, 38, 42) the importance of a comprehensive surgical staging necessary to select appro- priate additional therapy if necessary. Its lack has a sig- nificant impact on final stage.
The value of abdominopelvic irradiation is difficult to assess because of controversial results given by random- ized trials (12, 22, 35) and excellent results gained in ret- rospective studies with no adjuvant treatment after surgery alone (5year actuarial survival: 94% for stage Ic (30) or with cisplatin polychemotherapy (5-year actuarial sur- vival: 93.3% for Tl-T2 (15, 31-33).
In advanced ovarian carcinoma, our results seem bene- ficial if whole abdominal irradiation is applied to micro- scopic or no residual disease at the second-look laparot- omy (5-year actuarial survival of 76% with negative second look, 60% with microscopic residual disease. The same findings (5-year actuarial survival between 67% and 50%) have been reported by Franchin, Haie, and others (3, 16, 19, 20).
In these patients, the multivariate analysis shows that the amount of residual disease at the second-look lapa- rotomy is a high predictor of survival. Risk of death: 3.7; risk of relapse: 4.1. In patients with residual disease at
second-look laparotomy, the same findings have been re- ported by Haie (20) and Lippman (26).
However, the value of abdominopelvic irradiation is difficult to assess: Menczer (28,29) has obtained excellent results with intraperitoneal chemotherapy (5-year actu- arial survival 75%) and others in the same conditions have gained 5-year survival between 49% and 83% with no ad- juvant treatment after second-look laparotomy (9, 18,34).
Even in randomized trials the results after second look are controversial. Bruzzone has shown the superiority of cisplatin chemotherapy over whole abdominal irradiation (2), and an unpublished data from French Cancer Centers has shown no differences between the two modalities.
CONCLUSION
On the basis of our results, we can conclude that ab- dominopelvic irradiation using the four orthogonal fields technique is associated with tolerable acute toxicity and a low risk of serious late complications.
Abdominopelvic irradiation seems valuable in the management of ovarian carcinoma when there is no mac- roscopic residual disease left after initial surgery or at the second-look procedure.
Therefore, randomized trials after appropriate stratifi- cation are warranted to assess the real value of whole ab- dominal irradiation compared to other adjuvant treatment after initial surgery and second-look procedures.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
Bolis, G.; Zanaboni, F.; Vanoli, P.; Russo, A.; Franchi, M.; Scarfone, G.; Pecorelli, S. The impact of whole-abdomen radiotherapy on survival in advanced ovarian cancer patients with minimal residual disease after chemotherapy. Gynecol. Oncol. 39: 150- 154; 1990. Bruzzone, M.; Repetto, L.; Chiara, S.; Campora, E.; Conte, P. F.; Orsatti, M.; V&ale, V.; Rubagotti, A.; Rosso, R. Che- motherapy vs. radiotherapy in the management of ovarian cancer patients with pathologic complete response or min- imal residual disease at second look. Gynecol. Oncol. 38: 392-395; 1990. Cain, J. M.; Russell, A. H.; Greer, B. E.; Tamimi, H. K.; F&e, D. C. Whole abdomen radiation for minimal residual epithelial ovarian carcinoma after surgical resection and maximal first-line chemotherapy. Gynecol. Oncol. 29: 168- 175; 1988. Chassagne, D. Cancer du co1 u&in: Glossaire ou lexique des complications. Bull. Cancer 67: 1; 1980. Chauvergne, J.; Hoerni, B.; Durand, M. Langage commun dans l’expression des resultats therapeutiques en cancerol- ogie. Bull. Cancer 61:235-244; 1974. Chauvet, B.; Fignon, A.; Calais, G.; Lansac, J.; Le Floch, 0. L’irradiation dans le traitement des adenocarcinomes de I’ovaire. Etude retrospective de quarante-quatre cas. J. Gy- necol. Obstet. Biol. Reprod. 18:526-532; 1989. Conte, P.; Bruzzone, M.; Chiara, S.; Sertoli, M. R.; Daga, M. G.; Rubagotti, A.; Conio, A.; Ruvolo, M.; Rosso, R.; Santi, L.; Carnino, F.; Cottini, M.; Mossetti, C.; Guercio, E.; Gatti, M.; Siliquini, P.N.; Prelato, M. L.; Durando, C.; Giaccone, G.; Calciatti, A.; Farinini, M.; Centonze, M.;
8.
9.
10.
11.
12.
13.
14.
Rugiati, S.; Parodi, G.; Messineo, M.; Storace, A.; Bemar- dini, G.; Misurale, F.; Alessandri, S.; Casini, M.; Ragni, N.; Foglia, G.; Bentivoglio, G.; Pescetto, G. A randomized trial comparing cisplatin plus cyclophosphamide vs. cisplatin, doxorubicin, and cyclophosphamide in advanced ovarian cancer. J. Clin. Oncol. 4:965-97 1; 1986. Cox, D. R. Regression models and life tables (with discus- sion). J. R. Stat. Sot. [B] 34:187-220; 1972. Creasman, W. T.; Gall, S.; Bundy, B. N.; Beecham, J.; Mor- tel, R.; Homesley, H. D. Second-look laparotomy in the patient with minimal residual stage III ovarian cancer (a gynecologic oncology group study). Gynecol. Oncol. 35:378- 382; 1989. Dauplat, J.; Ben Ahmed, S.; Achard, J. L.; De Latour, M.; Legros, M.; Plagne, R. Le cancer Cpithelial de l’ovaire. Ap- ports de l’exptrience d’un centre aux donnees actuelles du pronostic et du traitement. J. Gynecol. Obstet. Biol. Reprod. 19:247-260; 1990, Delouche, G.; Valinta, D.; Bachelot, F.; Rambert, P.; Floiras, J. L.; Gest, J. Radiotherapie des cancers Cpitheliaux de l’ovaire. Irradiation totale de l’abdomen par champs ortho- gonaux. J. Eur. Radiother. 2: 103-l 17; 198 1. Dembo, A. J. Postoperative abdominopelvic irradiation in patients with epithelial cancer of ovary. The Princess Mar- garet Hospital Experience. J. Cancer Res. Clin. Oncol. 107: 9 l-93; 1984. Dembo, A. J. Abdomino-pelvic radiotherapy in ovarian cancer. Cancer 55:2285-2290; 1985. Dembo, A. J. Epithelial ovarian cancer: The role of radio- therapy. Int. J. Radiat. Oncol. Biol. Phys. 22:835-845; 1992.
1090 I. J. Radiation Oncology 0 Biology 0 Physics Volume 30, Number 5, 1994
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
Dottino, P. R.; Plaxe, S. C.; Cohen, C. J. A phase II trial of adjuvant cisplatin and doxorubicin in Stage I epithelial ovarian cancer. Gynecol. Oncol. 43:203-205; 199 1. Franchin, G.; Tumolo, S.; Scarabelli, C.; De Paoli, A.; Boz, G.; Crivellari, D.; Arcicasa, M.; Bortolus, R.; Gobitti, C.; Minatel, E.; Roncadin, M.; Trovo, M. G. Whole abdomen radiation therapy after a short chemotherapy course and second look laparotomy in advanced ovarian cancer. Gy- necol. Oncol. 41:206-211; 1991. Fyles, A. W.; Dembo, A. J.; Bush, R. S.; Levin, W.; Manchul, L. A.; Pringle, J. F.; Rawlings, G. A.; Sturgeon, J. F. G.; Thomas, G. M.; Simm, J. Analysis of complications in pa- tients treated with abdominopelvic radiation therapy for ovarian carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 22: 847-85 1; 1992. Gershenson, D. M.; Copeland, L. J.; Wharton, J. T.; Atkin- son, E. N.; Sneige, N.; Edwards, C. L.; Rutledge, F. N. Prog- nosis of surgically determined complete responders in ad- vanced ovarian cancer. Cancer 55: 1129-1135; 1985. Hacker, N. F.; Berek, J. S.; Bumison, C. M.; Heintz, A. P. M.; Junlard, G. J. F.; Lagasse, L. D. Whole abdominal radiation as salvage therapy for epithelial ovarian cancer. Obstet. Gynecol. 65:60-66; 1985. Haie, C.; Pejovic-Lenfant, M. H.; George, M.; Michel, G.; Gerbaulet, A.; Prade, M.; Chassagne, D. Whole abdominal irradiation following chemotherapy in patients with minimal residual disease after second look surgery in ovarian carci- noma. Int. J. Radiat. Oncol. Biol. Phys. 17: 15-19; 1989. Kaplan, E.; Meier, P. Non parametric estimation from in- complete observations. J. Am. Statist. Assoc. 53:457-481; 1958. Klaassen, D.; Shelley, W.; Starreveld, A.; Kirk, M.; Boyes, D.; Gerulath, A.; Levitt, M.; Fraser, R.; Carmichael, J.; Methot, Y.; Willan, A. Early stage ovarian cancer: A ran- domized clinical trial comparing whole abdominal radio- therapy, Melphalan, and intraperitoneal chromic phosphate: A National Cancer Institute of Canada Trials Group Report. J. Clin. Oncol. 6:1254-1263; 1988. Leers, W. H.; Kock, H. C. L. V. The evaluation of post- operative irradiation in patients with early stage ovarian cancer. Gynecol. Oncol. 28:4 l-49; 1987. Lentz, S. S.; Cha, S. S.; Wieand, H. S.; Podratz, K. C. Stage I ovarian epithelial carcinoma: Survival analysis following definitive treatment. Gynecol. Oncol. 43: 198-202; 199 1. Lindner, H.; Willich, H.; Atzinger, A. Primary adjuvant whole abdominal irradiation in ovarian carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 19:1203-1206; 1990. Lippman, S.; Alberts, D.; Slymen, D.; Weiner, S.; Aristizabal, S.; Luditch, A.; Davis, J.; Surwit, E. Second-look lapartomy in epithelial ovarian carcinoma. Prognostic factors associated with survival duration. Cancer 61:2571-2577; 1988. Martinez, A.; Shray, M. F.; Howes, A. E.; Bagshaw, M. A. Postoperative radiation therapy for epithelial ovarian cancer: The curative role based on a 24-year experience. J. Clin. Oncol. 3(7):901-911; 1985. Menczer, J.; Ben-Baruch, G.; Modan, M.; Brenner, H. In- traperitoneal cisplatin chemotherapy vs. abdominopelvic irradiation in ovarian carcinoma patients after second look laparotomy. Cancer 63: 1509- 15 13; 1988. Menczer, J.; Ben-Baruch, G.; Rizel, S.; Brenner, H. Intra- peritoneal cisplatin chemotherapy in ovarian carcinoma
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
patients who are clinically in complete remission. Gynecol. Oncol. 461222-225; 1992. Monga, M.; Carmichael, J. A.; Shelley, W. E.; Kirk, M. E.; Krepart, G. V.; Jeffrey, J. F.; Pater, J. L. Surgery without adjuvant chemotherapy for early epithelial ovarian carci- noma after comprehensive surgical staging. Gynecol. Oncol. 43:195-197; 1991. Piver, M. S.; Malfetano, J.; Baker, T. R.; Lele, S. B.; Mar- chetti, D. L. Adjuvant cisplatin-based chemotherapy for stage I ovarian adenocarcinoma: A preliminary report. Gy- necol. Oncol. 35:69-72; 1988. Piver, M. S.; Malfetano, J.; Hempling, R. E.; Baker, T. R.; Driscoll, D. L. Cisplatin-based chemotherapy for stage II ovarian adenocarcinoma: A preliminary report. Gynecol. Oncol. 39:249-252; 1990. Piver, M. S.; Malfetano, J.; Baker, T. R.; Hempling, R. E. Five-year survival for stage IC or stage I grade 3 epithelial ovarian cancer treated with cisplatin-based chemotherapy. Gynecol. Oncol. 46:357-360; 1992. Podczaski, E.; Manetta, A.; Kaminski, P.; Ricelli, A.; Larson, J.; DeGeest, K.; Mortel, R. Survival of patients with ovarian epithelial carcinomas after second look laparotomy. Gy- necol. Oncol. 36:43-47; 1990. Sell, A.; Bertelsen, K.; Andersen, J. E.; Stroyer, I.; Panduros, J. Randomized study of whole-abdomen irradiation vs. pel- vic irradiation plus cyclophosphamide in treatment of early ovarian cancer. Gynecol. Oncol. 37:367-373; 1990. Shray, M.; Martinez, A.; Howes, A.; Podratz, K.; Ballon, S.; Malkasian, G.; Sikic, B. Advanced epithelial cancer: Sal- vage whole abdominal irradiation for patients with recurrent or persistent disease after combination chemotherapy. J. Clin. Oncol. 6:1433-1439; 1988. Thigpen, T. J.; Blessing, J. A.; Vance, R. B.; Lambuth, B. W. Chemotherapy in ovarian carcinoma: Present role and future prospects. Semin. Oncol. 16:(Suppl. 6):58-65; 1989. Trimbos, J. B.; Schueler, J. A.; van der Burg, M.; Her-mans, J. L.; Van Lent, M.; Heintz, A. P. M.; Fleuren, G. J. Watch and wait after careful surgical treatment and staging in well- differentiated early ovarian cancer. Cancer 67:597-602; 1991. TNM classification des tumeurs malignes. 4eme edition, Geneve, Edition UICC; 1988: 118. Van Bunningen, B.; Bouma, J.; Kooijman, C.; Warlam- Rodenhuis, C. C.; Heintz, A. P. M.; Van Lindert, A. Total abdominal irradiation in stage I and II carcinoma of the ovary. Radiother. Oncol. 11:305-310; 1988. Whelan, T. J.; Dembo, A. J.; Bush, R. S.; Sturgeon, J. F. G.; Fine, S.; Pringle, J. F.; Rawlings, G. A.; Thomas, G. M.; Simm, J. Complications of whole abdominal and pelvic radiotherapy following chemotherapy for advanced ovarian cancer. Int. J. Radiat. Oncol. Biol. Phys. 22: 853- 858; 1992. Young, R. C. Initial therapy for early ovarian carcinoma. Cancer 60:2042-2049; 1987. Young, R. C.; Walton, L. A.; Ellenberg, S. S.; Homesley, H. D.; Wilbanks, G. D.; Decker, D. G.; Miller, A.; Park, R.; Major, F., Jr. Adjuvant therapy in stage I and stage II epithelial ovarian cancer: results of two prospective ran- domized trials. N. Engl. J. Med. 322:1021-1027; 1990.