Embed Size (px)
Citation preview

1
Evaluation of three standard dietary regimes in the
treatment of
Severe Malnutrition; The “TranSAM study”
An interim analysis
Report written by Sara van Vliet (s2255685) under supervision of Dr R.H. J. Bandsma,
Pediatric Gastroenterologist at the University of Groningen and University Medical Center
Groningen (UMCG) and Dr W.P. Voskuijl, Paediatrician and Senior Lecturer at the
Department of Paediatrics, College of Medicine, Queen Elisabeth Central Hospital (QECH)

2
Summary
Malnutrition is still one of the most devastating co-morbidities in young children. Despite
following treatment protocols for children suffering from severe acute malnutrition (SAM)
based on World Health Organisation (WHO) management guidelines case-fatality rate during
rehabilitation, even in specialized centers, remain up to 30%. The rise in co-morbidities such
as HIV has dramatically altered the epidemiology, case-presentation, pathophysiology, case-
management and outcome of childhood malnutrition. In addition, clinical impression and
recent published and unpublished data from the study Unit, MOYO House, at Department of
Paediatrics & Child Health, Queen Elisabeth Central Hospital (QECH), Blantyre, Malawi,
suggest that case-fatality during rehabilitation of HIV (non-) infected severely malnourished
children has been increasing over time and could be related to a specific phase of treatment,
namely the Transition Phase. There is data from the laboratory in Groningen, studies in
MOYO House, and others that severe malnutrition is associated with a severe impairment in
gut function, leading to deficient uptake of nutrients, especially carbohydrates. This impaired
function can be associated with watery diarrhoea and can ultimately lead to the child’s
demise. There is a lack of data evaluating gut function and optimal nutritional regimen
needed during the Transition Phase in rehabilitating severely, especially HIV infected,
malnourished children. This study aims to evaluate three different, commonly used and well
established WHO/ United Nations International Children's Emergency Fund (UNICEF)
(1999; 2009) dietary treatment protocols in severely malnourished children while admitted to
MOYO house. The Therapeutic Diets either consists of F75 (WHOs low energy, low protein
therapeutic milk) + Ready-to-Use-Therapeutic Food (RUTF), RUTF only, or F100 (WHOs
high energy and high protein therapeutic milk). The design was a randomised controlled
clinical trial.
This report serves as an interim analysis of the first 30 recruitments, looking at stool
frequency, stool consistency, frequency of vomiting, electrolyte disturbances, mortality and
changes in weight to look at the effect of the three different diets. Hypothesised was that the
(too) high carbohydrate content of F75 + RUTF would cause more frequent electrolyte
disturbances and would induce more frequent diarrhoea in a still recovering gastro intestinal
system compared to RUTF only or F100. The analysed results cannot describe a trend. In
addition, no major differences are found between the different diets to break off the study or
change the study design. A bigger sample size will be recruited to use for further analyses.
These outcomes could possibly provide answers in relation to the effect of the different diets.
Ondervoeding is nog steeds een van de meest heftige co-morbiditeiten in jonge kinderen.
Ondanks het volgen van behandelingsprotocollen voor kinderen die lijden aan Severe Acute
Malnutriton (SAM) volgens de richtlijnen van de Wereldgezondheidsorganisatie (WHO)
blijft het sterftecijfer tijdens revalidatie, zelfs in gespecialiseerde centra, nog zo’n 30%. Het
stijgen van co-morbiditeiten zoals HIV heeft de epidemiologie, casus presentatie,
pathofysiologie, beleid en prognose van ondervoeding in kinderen drastisch veranderd.
Bovendien geven ervaringen uit de kliniek en recente gepubliceerde en ongepubliceerde
gegevens uit onze studie locatie, MOYO ward, op de afdeling Pediatric & Child Health in het
Queen Elisabeth Central Hospital (QECH), Blantyre, Malawi, de indruk dat sterfte tijdens
revalidatie van HIV (niet-) besmette ondervoede kinderen na verloop van tijd is toegenomen
en gerelateerd is aan een specifieke fase van de behandeling, de zogenaamde overgangsfase.
Gegevens uit het laboratorium in Groningen en studies uit MOYO ward en andere centra
wijzen erop dat ernstige ondervoeding geassocieerd is met een ernstig verminderd
functioneren van de darm en dysfunctie in de opname van voedingsstoffen, met name van

3
koolhydraten. Deze verminderde functie uit zich in waterige diarree en kan uiteindelijk leiden
tot het sterven van het kind. Er is een gebrek aan kennis over de darm functie en over een
optimaal dieet tijdens de overgangsfase in de behandeling van ernstig, met name HIV
geïnfecteerd, ondervoede kinderen. Deze studie richt zich op het evalueren van drie
verschillende therapeutische diëten, volgens de protocollen van WHO/ United Nations
International Children's Emergency Fund (UNICEF) (1999; 2009), ook in gebruik op MOYO
ward. De diëten bestaan uit het geven van; F75 (een lage energie densiteit, laag eiwitgehalte
therapeutische melk) + Ready-to-Use-Therapeutic-Food (RUTF), alleen RUTF of F100 (hoge
energie densiteit en eiwitrijk therapeutische melk). Het ontwerp van de studie is een
randomised controlled clinical trial.
Dit verslag dient als een interim analyse van de eerste 30 inclusies, kijkend naar stoelgang
(frequentie en consistentie van de ontlasting), braken, elektrolytenstoornissen, mortaliteit en
gewichtsveranderingen om het effect van de drie verschillende diëten te beoordelen. De
hypothese was dat het (te) hoge koolhydraatgehalte van F75 + RUTF, in vergelijking met
alleen RUTF of F100, zou leiden tot meer frequente elektrolytenstoornissen en zou zorgen
voor meer frequente diarree in een nog steeds herstellend gastro-intestinaal systeem. De
geanalyseerde resultaten kunnen geen trend beschrijven. Er zijn geen grote verschillen
gevonden tussen de verschillende diëten die zouden kunnen leiden tot het vroegtijdig
afbreken van de studie of de methodes te veranderen. Een grotere inclusie groep zal worden
gebruikt voor verdere analyses. Deze resultaten zouden inzicht kunnen geven over het effect
van de verschillende diëten.

4
Contents list
Summary 2
1. Introduction 5
1.1 Malawi
1.2 The signs, symptoms and outcome of children with Severe Acute
Malnutrition
1.3 Managing severe malnutrition in children
1.3.1 WHO therapeutic guidelines
1.3.2 Managing severe malnutrition in MOYO nutrition ward,
QECH, Malawi
1.4 The aetiology behind the experienced morbidity and case-fatality
during the rehabilitation of severely malnourished children
1.4.1 Malabsorption/osmotic diarrhoea
1.4.2 Bacteraemia
1.5 Current study
2. Methodology 10
2.1 Preparation
2.1.1 Protocol
2.1.2 Set-up
2.2 Subjects
2.3 Design
2.3.1 Randomisation
2.3.2 Blinding
2.4 Intervention
2.5 Variables, Sampling and Storage
2.6 Analyses
2.7 Outcome variables
2.8 Statistics
3. Results 15
4. Discussion 17
5. Conclusion 19
Acknowledgements 19
References 19
Appendices 23

5
1. Introduction
Severe Acute Malnutrition (SAM) is still one of the most devastating conditions in young
children, affecting nearly 20 million worldwide and causes an estimated 2 million to die
every year [1,2,3]. What is more, undernutrition is estimated to be indirectly responsible for
over a third (35%) of the global child mortality [4]. Despite WHO’s Therapeutic Guideline,
case-fatality rates (CFR) during rehabilitation, even in specialized centres, remain high, up to
30% [5,6,7,8]. This exceeds targets such as those based on WHO treatment guidelines which
claim that CFRs should be as low as 5% [9].
1.1 Malawi
Malawi is one of the world’s poorest countries ranking 170 out of 187 countries with
comparable data on the Human Development Index (HDI) [10]. This index represents a
combined measure of three basic dimensions of human development; health, education and
income. Malawi’s health system is frequently hit by crises in the delivery of essential
medicines, understaffed clinics and erratic drug supplies. The UK charity Oxfam reported
that only 9% of local health facilities (54 out of 585) had the full Essential Health Package
list of drugs for treating 11 common diseases in 2012. Additionally, they reported that clinics
often run out of basic antibiotics, HIV test kits and insecticide-treated mosquito nets, and
many facilities have very low stocks of vaccines [11].
50.7 % of the country’s population live under the poverty line with the poorest residing in the
rural northern and southern parts of the country [12]. The agriculture sector, the most
important sector in the economy, is often hit by crises (e.g. crop failure, increase of prices)
causing Malawi to experience frequent food shortages. The Malawi Vulnerability Assessment
Committee (MVAC), based on their results of a post-harvest food security assessment,
predicted that in the April 2012 to March 2013 consumption period, 1.63 million people in 15
mainly southern districts would be unable to adequately access food in order to meet their
basic food needs [13]. The latest estimation of malnutrition (weight/age) in % of children
under five in Malawi is 13.8. The prevalence of undernourishment in the population is 27.0%
[14].
1.2 The signs, symptoms and outcome of children with Severe Acute Malnutrition
Malnutrition can be classified as mild, moderate and severe based on anthropometry,
biochemistry and clinical assessment [15]. Clinically, SAM in children aged 6-60 months
presents itself into different forms. Firstly, the meagre child is wasted (Marasmus), as defined
by low weight-for-height ≤ -3 Z-scores or a mid-upper-arm circumference of <11.5 cm
(WHO growth standards) [16]. Quite different is the clinical manifestation of kwashiorkor,
as defined by low-weight-for-age (60 to 80 % of expected weight) and nutritionally induced
bilateral oedema. Accompanying features include a fatty liver and hepatomegaly, sparse and
discoloured hair, “flaky paint” rash over the skin, anorexia and metabolic disturbances [9].
SAM impairs the immune system causing children suffering from SAM to have a lower
immune response. Children with SAM have a tripled risk of dying from pneumonia, measles,
or diarrhoea [4,17]. They also have a higher risk of acquiring tuberculosis [18]. There are
several studies investigating underlying mechanisms in the development of the immune
system in children suffering from SAM. Protein and zinc deficiency in young infants
contributes to thymus atrophy and dysfunction. Impaired T-cell maturation is associated with

6
a poor nutritional status of the child [19,20,21]. Children with SAM are also more prone to
get severely ill from more common and ‘harmless’ childhood diseases. Frequent illness in a
child with SAM further demises their nutritional status and locks the child in a vicious circle
of recurring illness and discordant growth. Another important co-morbidity in children with
SAM is the human immunodeficiency virus (HIV). HIV has had a major impact on the
epidemiology, case-presentation, pathophysiology, case-management and outcome of
childhood malnutrition [22]. It is estimated that 2.1 million children worldwide are living
with HIV of which 90% live in sub-Saharan Africa [23]. The HIV infection can compromise
the nutritional status of these children early on in their lives [24]. In a systematic review and
meta-analysis of HIV prevalence and mortality among children treated for SAM in sub-
Saharan Africa in which 17 studies (4891 children) were included, the average prevalence of
HIV infection was 29.2%. Children with HIV and SAM were significantly more likely to die
than those children who were HIV sero-negative (HIV–ve) [25].
1.3 Managing severe malnutrition in children
1.3.1 WHO therapeutic guidelines
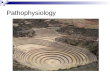
Inpatient treatment of severely malnourished children are based on WHO’s Therapeutic
Guidelines [9,26,27] and is staged into three phases, instructed by the WHO 10-step plan
(figure X); firstly the Stabilisation and Resuscitation 1st Phase, in which children are
resuscitated and metabolically stabilised on a maintenance diet of F75 (WHOs low energy,
low protein therapeutic milk of 75 kcal/kg/day) (step 1-7). This phase will usually last 2-7
days and is focussed on stabilising the child by carefully re-feeding and treating and
identifying life-threatening problems e.g. to avoid the child acquiring the so-called ‘refeeding
syndrome’; a critical state in which the child suffers from electrolyte disturbances and cardiac
failure If appetite is regained and, in the case of kwashiorkor, oedema is starting to resolve,
children are put on a diet containing a higher energy and protein concentration (F100) in what
is called the Transition or 2nd
Phase. Finally, if the child remains well and its appetite allows
ad-libitum feeding the rehabilitation is concluded in the 3rd
Rehabilitation Phase of Rapid
Catch-up Growth with high-energy diet of RUTF (Ready-to-Use-Therapeutic Food). This
stage of the treatment can be done at home.
Table 1: WHO 10-step plan for the management of SAM, adapted from WHO [15].

7
1.3.2 Managing severe malnutrition in MOYO nutrition ward, QECH, Malawi
MOYO nutrition ward treats their inpatients using the above mentioned WHO guidelines and
according to National Malawi guidelines [28]. Clinical experience applying National Malawi
guidelines and annually treating between 1250-2500 severely malnourished children on the
ward point towards a number of unresolved issues regarding peak case fatality rates found.
The mortality rate is high [29] and appears to be increasing over time [30,31]. This could be
associated with several changes of the inpatient feeding protocols on MOYO ward:
- From 2002-5, guidelines for initial care followed WHO 1999 relatively closely with an
‘stabilization phase’ using ‘F75’ milk followed by a minimum of 2 days ‘transition phase
feeding’ using ‘F100’ milk.
- From 2005, ready-to-use therapeutic foods (RUTF) began to be introduced into the diet
during and after transition phase.
- From 2006, the transition phase diet was standardised following guidelines elsewhere: F100
milk was replaced by introduction of RUTF.
- From 2008, the transition phase diet reverted to a more traditional F100-based regime. This
however took time to implement [32], with audit showing that many patients from 2008-10
were still being managed following 2006 guidelines [33].
Retrospective analyses of ward data revealed an increased mortality in children who
transitioned to RUTF (15%) compared to F100 (11%) odds ratio 1.38 (95% CI 1.04 to 1.82)
p<0.00113 (unpublished observations).
However, this increased mortality can also be associated with the increasing clinical
complexity of the patients admitted to the ward [34]. It is difficult to separate the contribution
of changing patient profile from the clinical/feeding interventions which have also changed
over time. Furthermore, watery diarrhoea is observed and appears to be associated with a
substantially higher mortality [33,35]. Cases of circulatory failure are also observed resulting
from either hypo-volaemia induced by the above diarrhoea, or fluid overload following
therapeutic correction; both are presently not very well guided by therapeutic guidelines.
What is more, several nutritional units in the region have experienced a peak in mortality in
the transitional phase (from a F75 stabilization diet to a higher energy diet) [31, unpublished
observations]. All these contributing factors need to be disentangled. Up to date, there is no
published data available prospectively evaluating the different strategies in the transition
phase for inpatient treatment of severely malnourished children.
1.4 The aetiology behind the experienced morbidity and case-fatality during the
rehabilitation of severely malnourished children
1.4.1 Malabsorption/osmotic diarrhoea
Previous studies have shown that severe malnutrition is associated with a severe impairment
in gut function, leading to deficient uptake of nutrients, especially carbohydrates. The
carbohydrate sources of RUTF and F100 consist of a mixture of malto-dextrin, sucrose and
lactose. Sucrose, consisting of glucose and fructose, is a disaccharide, which needs to be
hydrolysed by a disaccharidase before intestinal absorption is possible. Older studies from
Jamaica [36] and South-Africa [37] as well as, limited histological evidence [38,39,40] has
shown impaired absorption of disaccharides and various degrees of villous atrophy in
children with kwashiorkor which could account for the decreased disaccharide absorption
found in these children. Whereas absorption of glucose across the apical membrane is
mediated by the sodium-dependent glucose transporter (SGLT-1), the absorption of fructose
mainly takes place through GLUT-5 [41]. The maximum capacity of healthy intestine to
absorb fructose is limited [42]. Recent human studies have indicated that its absorption can
be improved if glucose and fructose are consumed simultaneously [43,44]. In children with

8
severe malnutrition, villous atrophy and limited disaccharidase activity, the intake of
carbohydrates could exceed the intestinal carbohydrate absorptive capacity. Severe glucose
malabsorption was also found in kwashiorkor and hypo-albuminaemic marasmus patients
using a double label glucose technique. In addition, children who showed most severe
glucose malabsorption appeared to develop diarrhoea and/or vomiting [45].
Water absorption in the intestine is dependent on the absorption of solutes. Unabsorbed
nutrients, in this case carbohydrates, will cause osmotic diarrhoea in the malnourished child.
This watery diarrhoea can lead to electrolyte disturbances, dehydration (child becomes
hypovolaemic) and ultimately death. There is local evidence from MOYO house and other
studies supporting this hypothesis [45,46,47]. A study from Nigeria electrolyte disturbances
in children with protein energy malnutrition suffering from diarrhoea showed especially a
high rate of metabolic acidosis (low serum pH and high serum HCO3-) and hypokalaemia
[48].
1.4.2 Bacteraemia
The bacterial infection in severely malnourished children related to immunosuppression can
also be associated with the gut through loss of the protective mucosal barrier [49]. Children
with severe malnutrition are shown to have a higher prevalence of gut barrier dysfunction
[50] and Escherichia coli bacteraemia [51]. What is more, in the severely malnourished a
higher mortality rate from invasive bacterial infection was found than in well- nourished
children with bacteraemia (39% versus 12%) [52]. A recent study investigated the role of the
gut microbiome as a causal factor in kwashiorkor patients and identified that the combination
of Malawian diet and kwashiorkor microbiome in recipient mice produced marked weight
loss, accompanied by distress in amino acid, carbohydrate, and intermediary metabolism that
were only transiently improved with administering RUTF [53].

9
1.5 Current study
To date, there is a lack of data evaluating gut function, intestinal microbial flora, and optimal
nutritional regimen needed during the Transition Phase in rehabilitating severely, especially
HIV infected, malnourished children. New insights could have important implications for the
development of new dietary protocols in the treatment of malnutrition, potentially decreasing
the occurrence of the often fatal diarrhoea during rehabilitation and greatly benefit this
patient group.
This research, set up as a randomised controlled clinical trial, aims to evaluate the outcome,
especially in relation to a child’s gut function, of three different, commonly used dietary
treatment protocols during the Transition Phase (consisting either of F75 + RUTF, RUTF
only, or F100). F75 consists of 65 energy % carbohydrates compared to F100 40% and RUTF
32%. As caloric intake is increased during the transition phase we hypothesize that the (too)
high carbohydrate content of F75 + RUTF is associated with more frequent electrolyte
disturbances and will induce more frequent diarrhoea in a still recovering gastro intestinal
system compared to RUTF only or F100.
In this research, I was responsible for set-up of the study and an interim analysis. This report
will show the interim analysis on the first 30 study inclusions, looking at the effect of the
different diets through analysis of stool consistency, frequency, electrolyte disturbances and
weight loss and/or gain. Any great significant differences found between the diets could lead
to breaking off or changing the study design. Any trends described could provide more
insight.
Research Question: What is the effect of three commonly used transition-phase diets on
clinical outcomes in children being treated for severe acute malnutrition?

10
2. Methodology
2.1 Preparation
Given the nature of the research and research setting, ample time was allocated for
preparation and on-the-ground set-up of workspace, including training of staff and a proof
run of the study. These activities were performed under supervision and aided by my local
supervisor, Dr. Voskuijl.
2.1.1 Protocol
Firstly, the protocol needed to be re-written as change in ward practice and practices in the
international community became apparent; a third arm was added, the “RUTF only” arm, as
was learned that multiple other institutions provide RUTF as the basal nutritional source
during the transition phase and only add F75 if children don’t take enough calories from
RUTF. Providing F75 while adding RUTF had been a common practice at MOYO, the
nutrition rehabilitation unit of Queen Elisabeth Central Hospital during the transition phase.
Both diets are in theory consistent with the recommended WHO protocol but are essentially
different; adding a third arm would greatly strengthen the clinical relevance of the study.
Furthermore, the non-malnourished control group was dropped so as to simplify the protocol
and reduce the need for blood sampling. Though these controls would have been ideal given
the scarcity of normal range reference data, the advantage was outweighed by the
disadvantage in terms of extra blood sampling for control-children. In addition, involving
healthy controls in a study remains an issue in receiving consent from the ethical committee.
Lastly, the protocol was updated with new case definitions of severe acute malnutrition in
accordance with WHO guidelines. For this, I performed a small survey in the paediatric
Accident and Emergency department, assessing the children admitted on their weight, height
and MUAC (mid-upper arm circumference) and found that children were easier diagnosed
with malnutrition using the WHO standard than when using the (older) National Center for
Health Statistics (NCHS)references.
This was in accordance with the literature comparing these standards on a larger scale and
concluding that definition of malnutrition using WHO standards would lead to a higher
disease burden, particularly for severe wasting, than using the NHCS references [54].
2.1.2 Set-up
I investigated practice on the ward and ensured that the study protocol and interventions were
in line with current practices and that these practices were carried out in a similar manner by
all the staff and caregivers. For this, we introduced the use of the ‘MOYO slide chart’ on the
ward to assess children’s nutritional status [55].
Secondly, I certified my workspace, creating space on the ward and finding a lab and
adequate equipment to process and analyse my samples. I gathered all the materials needed
for sampling, processing and storage (including arranging a dependable -80o C freezer to
store samples until shipment to the Netherlands).
Lastly, I had to recruit and instruct staff to help with patient recruitment and sampling. I
recruited five MOYO staff nurses.

11
2.2 Subjects
Inclusion criteria
Children, aged between 6 and 60 months, admitted to MOYO House and diagnosed as
kwashiorkor, and/or marasmus were included after informed consent was given by their
guardian (for consent form in English see appendix A). Both HIV positive and negative
children were included in the study.
Exclusion criteria
Severely malnourished HIV infected children who were MOYO readmissions within the past
year or who were already on anti-retroviral-therapy were excluded. Children that presented
with a PCV of less than 15%, severe hemodynamic instability or severe neurological
symptoms were also excluded. Children whose HIV status was unknown due to their carer
declining the routinely offered test were also excluded.
Subjects were screened for eligibility on admission to MOYO House and written informed
consent was requested soon after.
Study children who developed persisting diarrhoea during their transition phase and/or
hypovolaemia were monitored more closely. After reversing to their initial therapeutic diet
F75, these patients were checked frequently for fluid & electrolyte balance. Furthermore,
their circulatory state was carefully documented: if compromised they received standard
clinical care.
2.3 Design
This is an open label randomized controlled trial of three standard dietary regimes which are
already in widespread clinical use: two of which are currently in use on MOYO; the third of
which is a variation of how to eat the same basic diet (see 2.4).
2.3.1 Randomisation
Patients were randomised on HIV status and were randomly allocated a feed. The
randomization sequence was computer generated by a colleague from the Malawi Liverpool
Welcome trust (MLW) who was not involved in front line fieldwork.
Allocation concealment was achieved by inserting group labels/feeding instructions into
sealed, sequentially numbered opaque envelopes. At the moment when patients were ready to
begin a transition phase diet, they were asked to draw the next numbered envelope from the
assigned pile; the envelope was opened to show their assigned group. The feed was also
written on the patient’s ‘food ticket’ to help both the carer to remember the correct group and
also to help the MOYO ward kitchen to give the correct feed at all times.
2.3.2 Blinding
This was an open label trial – given the nature of the intervention, it was not be possible to
blind the subjects to their group. For the same reason, it was not possible to blind staff doing
clinical assessment. The investigators analysing samples in the Netherlands will however be
blind to a patient’s group.
2.4 Intervention
Patients began the study once they achieved standard criteria to move from phase 1 to the
transition phase, according to the WHO guidelines [20]. This was after return of their appetite
and, in case of children with kwashiorkor, improvement of oedema.

12
The three therapeutic diets to be tested during the transition phase were:
1. A High Energy Therapeutic Regime based on F100 milk: in an iso-volumetric amount to
F75 phase 1 milk.
2. A High Energy Therapeutic Regime of RUTF supplemented with F75 milk. Caregivers
started a feed by giving ready-to-use therapeutic foods as much as was tolerated by the child
(up to a maximum of 135 kcal/kg/d) and then followed by giving F75 - to ensure a minimum
intake of 100 kcal/kg/d. The amount of ready-to-use therapeutic foods was increased over 2-3
days until the full requirement of ready-to-use therapeutic foods was taken by the child. F75
was then stopped.
3. A High Energy Therapeutic Regime of RUTF only. Caregivers started a feed by giving
ready-to-use therapeutic foods as much as was tolerated by the child (up to a maximum of
135 kcal/kg/d) but with water and not routinely followed with F75. The amount of ready-to-
use therapeutic foods was increased over 2-3 days until the full requirement of ready-to-use
therapeutic foods was taken by the child. If a child was unable to eat his/her RUTF, they were
moved back a phase to f75 milk alone.
Table 2: Different carbohydrate loads for every diet
CHOa (g)
provided by:
135 kcal F100 135 kcal RUTF 100 kcal F75 + 35 kcal
RUTF
Sucrose 2.34 6.50 2.58
Lactose 8.83 3.25 3.31
Dextrine maltose 2.34 0.00 13.00
Other CHO 0.00 0.88 0.23
Total 13.5 10.6 19.1 aCHO: Carbohydrates
As noted, diet 1 and 2 were both already in use in MOYO House; diet 2 was a variation of
diet 3.
The duration of the study, commencing when at the end of phase 1 the child was transitioned
to the high energy diet, was for the full duration of transition phase. Case fatality, catch-up
growth and failure was recorded for every child until the child was found fit for discharge
from MOYO House.
2.5 Variables, Sampling and Storage
Diets and appetite
Amount and route of administration of feeding was recorded daily. Appetite was recorded
with every feed (by asking caregiver), as was refusal to complete any feed. Patients were
allowed to change from the transition phase to phase 2 if they had been clinically well during
the transition phase and continued to have a good appetite.
Anthropometry and clinical signs of malnutrition
Twice daily weights were taken, and daily assessment of the measure of oedema, hydration
state and capillary refill time, and other routinely collected clinical signs related to
malnutrition. For full list of variables see the questionnaires in appendix B.
Blood sampling
A total of 3 blood samples was taken throughout the study. The first sample was taken on
admission to MOYO House. A second sample was taken while the child was still receiving
F75, just before entering the transition phase. The third sample was taken on day 3 in the
transition phase. Blood was centrifuged and plasma was used to perform electrolyte and

13
bloodgas testing and analyses. A fraction was stored at -80o C until further analysis.
Electrolytes were determined immediately; if there were of therapeutic value they were used
to adjust therapy. Per sample 2.5 ml of blood was drawn keeping the total volume over the
child’s entire test period below 8 ml.
Excreta sampling
A faecal and urine sample, to asses (mal) absorption of the nutrients, were taken on the same
days as the analytic blood sampling. Part of the faecal sample was stored at -80o C until
analysis. Stool frequency and consistency were noted daily.
See appendix C for a case report form (CRF).
2.6 Analyses
As recruitment is on-going and the data set is not completed interim analyses were done on
the first 30 recruitment (of which 25 received the intervention).
The change in weight between the day before and after the diet (day 3) and the weight at the
end of the diet (day 3) were analysed. Weight, amount of feeding, anorexia, route of feeding,
duration on phase 1 and on the transition phase, duration until time of discharge (and death)
and other clinical signs related to malnutrition were entered into a database. The majority of
these other variables will be analysed on the complete sample group.
Plasma electrolytes (glucose/lactate, sodium, potassium, bicarbonate- concentrations), and pH
were determined locally for all time points. This report looked at plasma disturbances in
potassium, bicarbonate and pH, by looking at the difference between the day before and after
(day 3) of the diet, and the end values of the diet (day 3). The other electrolytes will be
analysed for the complete sample group.
Future analyses of the plasma, stool and urine samples that were collected and stored in the
freezer will be performed at the end of the recruitment, when all the samples have been
shipped to the Netherlands. Plasma and urine will be used to measure excretion of 8-
hydroxydeoxyguanosine (8-OhdG) corrected for creatinine excretion as a measure of DNA
oxidative damage. In addition, plasma citrulline concentrations will be determined as a
reflection of enterocyte mass. These analyses will be performed in the Netherlands since
these analyses cannot be conducted in Malawi. Albumin concentration will be determined in
Groningen as well. Faeces pH was determined locally. Faeces will be analysed to determine
alpha 1-antitrypsin and elastase content as a measure of protein loss and pancreatic function,
respectively. In addition, microbiomal analyses of the faecal flora will be performed using
16S rRNA pyrosequencing. These last two faecal samples will be analysed in the Netherlands
since these analyses cannot be conducted in Malawi.
After analysis, all biochemical parameters will be entered in a database.
2.7 Outcome variables
The outcome variables of this report were:
1. Frequency of diarrhoea
2. Frequency of vomiting
3. Electrolyte disturbances (in potassium, bicarbonate and blood pH)

14
4. Recovery rate expressed in incremental weight/kg bodyweight/per day.
5. Mortality
Variables of the complete sample load will be divided into primary and secondary variables
and will include:
Primary Outcome Variable:
1.Fecal pH (on fresh material; determined in Blantyre, BLZ).
Secondary Outcome Variables:
1.Electrolyte disturbances
2.Recovery rate expressed in incremental weight/kg bodyweight/per day
3.Morbidity and clinical signs; assessed every day by a standardized form during the entire
admission period
4.Urinary excretion of 8-hydroxydeoxyguanosine (8-OhdG) corrected for creatinine
excretion, as a measure of DNA oxidative damage (determined in Groningen)
5.Plasma 8-hydroxydeoxyguanosine (8-OhdG) (determined in Groningen)
6.Plasma citrulline concentrations, as a reflection of enterocyte mass (determined in
Groningen)
7.Fecal excretion of elastase and alpha 1-antitrypsin (determined in Groningen)
8.Analysis of fecal microbiota (determined in Groningen).
2.8 Statistics
The calculated sample size is 15 participants per group. An additional 3 participants per
group will be included to account for loss of follow up, inability to obtain blood samples and
other technical issues. Since HIV positive and negative children are to be analysed separately,
a total of 18 (patients) x 3 (groups) x 2 (HIV groups) = 108 patients will be recruited. The
sample size was calculated for faecal pH and reducing substances, which is the most
important primary outcome measure as it most directly reflects carbohydrate malabsorption.
Based on recent glucose absorption data, 45% of malnourished patients suffered from severe
glucose malabsorption that is expected to be associated with osmotic diarrhoea. RUTF in
combination with F75 was the most often used practice during the period this study was
performed. We aim for an improvement of 30% in carbohydrate malabsorption of treatment
1 (F100) compared to 2 (F75+ RUTF) in this pilot study. Using α=0.05 and 80% power, with
an expected sigma of 13% an N of 15 per arm was calculated.
This report will conduct an interim analysis of the first 30 recruitments (of which 27 received
the intervention). Since patients are randomly recruited, HIV positive and negative children
were not balanced between the different groups. The differences between the HIV positive
and negative children will therefore not be incorporated in this interim analysis. Furthermore,
the results of this analysis will not be considered conclusive but serve as indicator for
possible trends and/or significant differences in outcome between the groups to amend or
discontinue the study.

15
3. Results
At their time of transition, the first 30 patients were randomly allocated a diet. This resulted
in a F100 N=11, F75+ RUTF N=7 and RUTF only N=9 group. The demographic
characteristics of the study sample are summarised in the table below.
Table 3: Demographic characteristics of study sample divided by diet F100 F75+ RUTF RUTF only
Count Column N %
Count Column N %
Count Column N %
Male gender freqa (%) 3(27.3) 2(28.6) 4(44.4)
Age (months), mean (SDb) 28(18.74) 22(7.07) 21(10.83)
Weight, mean(SD) 7.77(2.01) 8.04(2.14) 6.86(1.60)
pH serum beforec diet, mean(SD) 7.39(0.10) 7.42(0.15) 7.47(0.11)
Potassiumd before diet, mean(SD) 4.5(0.59) 4.62(0.68) 4.16(0.28)
Bicarbonated before diet, mean(SD) 22.3(3.74) 23.2(6.98) 23.4(2.18)
Breastfeeding (months), mean(SD) 16.3(6.65) 17.1(8.40) 12.6(4.58)
HIV test positive, freq (%) 3(27.3) 2(28.6) 1(11.1)
Bilateral oedema, freq (%)
8(72.7) 5(71.4) 7(77.8)
MUACe
(cm) freq (%) 12.0(1.84) 12.2(2.12) 11.8(1.90)
afreq: frequency
bSD: standard deviation
cbefore: day before start transition feed
delectrolytes were measured in serum in mmol/L
eMUAC: mid-upper-arm circumference
The study sample was dominantly female. The mean age across the groups did not differ
greatly, with a mean age of 28, 22 and 21 months. The mean pH at the start of the diet was
lowest in the F100 group and highest in the RUTF only group. The mean starting potassium
levels were similar across the groups and the lowest in the RUTF only group. The mean
HCO3- levels were also similar across the groups with the greatest variance within the F75+
RUTF group. In total there were 6 HIV positive children, of which most (N=3) in the F100
group. Most of the study sample (N=20) had bilateral oedema. In each group the majority of
patients had bilateral oedema.

16
Because of the small sample size, no normal distribution was expected. This was later
verified by testing one of the variables. A non-parametric test (the Kruskal-Wallis) was used
to give the following results;
Table 4: Outcome variables of study sample divided by diet
aHCO3-: Bicarbonate
No differences were found between the different groups as the results shown above were not
significant. I will describe them nevertheless, so I can refer to them in the discussion
following.
With the therapeutic diet of F75+RUTF children there was a tendency to have less diarrhoea
than the other two diets. However, this is not significant (p=.176). In addition this group also
had the highest rate of normal stool (p=.664). Most diarrhoea was seen in the F100 group, in
which the maximum frequency was also the highest. There was no significant difference
between the groups in vomiting frequency (p=.339). Most vomiting was seen in the RUTF
only group. The least vomiting was seen in the F100. The weight difference across all the
groups was very little, but most gain was seen in the F75+ RUTF group. The RUTF group
showed the highest rate of overall weight loss and the least weight gain. The weight of the
F100 group showed the least weight change. These results are not significant (p=.562). The
pH difference in the F100 group was the highest and showed the most gain compared to the
other groups. The F75+ RUTF group showed the most overall loss in pH compared to the
other groups. This is not significant (p=.507). The highest potassium difference was seen in
the F75+ RUTF group with no loss across the whole group. The RUTF only group had the
highest rate of overall potassium loss. These results are not significant (p= .179). The HCO3-
difference was the highest in the F75+ RUTF group, with the most loss overall compared to
the other groups. In the F100 group there was only loss of HCO3-. This is not significant
(p=.634). The pH after the diet was overall highest in the F100 group and lowest in the RUTF
only group. These results are not significant (p=.688). The average potassium levels after diet
were in the normal range. The mean was highest in the F75+ RUTF group. The lowest
Therapeutic diets
F100 F75+ RUTF RUTF only p value
Mean (Min-Max)SD Mean (Min-Max)SD Mean (Min-Max)SD
Clinical data
Freq watery/loose stool
7.89(0.00-19.00)5.49 3.14(0.00-7.00)3.08 4.78(0.00-17.00)5.74 .176
Freq normal stool 3.11(0.00-10.00)3.89 4.57(0.00-11.00)4.61 2.33(0.00-7.00)2.69 .664
Freq vomiting 0.11(0.00-1.00)0.33 0.43(0.00-1.00)0.53 2.56(0.00-11.00)4.10 .339
Weight difference after diet
0.00(-0.28-0.18)0.16 0.01(-0.30-0.32)0.19 -0.10(-0.38-0.11)0.17 .562
Biochemical data
pH difference after diet 0.06(-0.02-0.20)0.10 -0.03(-0.17-0.19)0.15 -0.02(-0.35-0.10)0.17 .507
Potassium difference after diet
0.68(0.00-1.00)0.47 0.75(0.00-1.20)0.57 -0.06(-1.40-0.70)0.81 .179
HCO3-a difference
after diet -1.13(-2.30--0.50)0.81 -2.58(-6.90-3.00)4.22 -0.76(-3.00-2.20)2.17 .634
pH after diet 7.47(7.30-7.72)0.16 7.41(7.31-7.62)0.13 7.41(7.22-7.51)0.09 .688
Potassium after diet 4.76(2.90-7.00)1.46 5.04(4.00-5.70)0.70 4.17(2.60-4.90)0.82 .279
HCO3-a after diet 21.98(15.60-30.00)4.53 19.68(17.10-22.80)2.33 18.98(11.70-23.90)3.61 .407

17
average potassium was found in the RUTF only group, where the minimum was also lowest.
These results are not significant (p=.279). Lastly, the HCO3- after the diet was highest in the
F100 group and lowest in the RUTF only group. This is not significant (p= .407).
Mortality in all the groups was 0. No data are yet available for the duration of the transition
phase and the time of recovery.
4. Discussion
For this report we analysed stool frequency, stool consistency, frequency of vomiting,
electrolyte disturbances, mortality and changes in weight to study the effect of three
commonly used transition-phase diets on clinical outcomes in children being treated for
severe acute malnutrition. We hypothesised that children receiving the F75+ RUTF diet
would experience the highest rate of diarrhoea, electrolyte disturbances and weight loss. In
this interim analysis, no large differences were found between the groups that would lead to
breaking off the study or changing the study design.
There were no significant differences between the diets. This can most likely be explained by
the fact that this study sample (N=27) - namely, the children that received the diet - was much
smaller than the calculated sample size (N=108). In this sample size an individual difference
within a group was more likely to be responsible for the differences seen between the three
groups, more so than the difference of the group as whole.
Taking these individual differences into account, we can first take a look at the frequency of
watery diarrhoea. This variable had a trend to be higher in the F100 group. This group had a
patient with a frequency of 19. This individual will greatly increase the mean of the small
group as a whole, compared to the other groups. In a greater sample size, we expect these
children to be distributed across the groups. In addition, the F100 group had more
recruitments than the other groups; a higher frequency of stool could already be expected. It
is therefore difficult to attribute the high frequency to the diet alone. Useful in the analysis of
diarrhoea frequency would be to take into account the carbohydrate absorption and /or losses
through analysing stool and blood samples on reducing substances and carbohydrate
absorption, respectively. These analyses will be included in the next report.
The impact of an individual can also be seen in the frequency of vomiting. In the RUTF only
group one child vomited 11 times. As these results are not significant, no relation can be
defined between the diet and the vomiting. However, one could suggest that carbohydrate
malbsorption in the diets explained the vomiting seen in the children. Nausea and vomiting
have been described in fructose malabsorption [56] and the RUTF only group had the highest
sucrose load compared to the other diets. But the symptoms could also be attributed to the
taste and/or consistency of the feed. RUTF is a dry, sweet paste that can be difficult to
swallow for small children, especially those who are HIV positive and suffer from
oesophageal thrush [57].
Looking at changes in weight across the groups from before and three days into the diet, we
can see they did not differ much from each other. The RUTF only group experienced a slight
more overall weight loss compared to the other two groups, although this was not significant.
Children are expected to recover lost weight in the transition phase and ‘catch- up growth’
until they are ready for discharge [15]. The weight losses seen in our results could be

18
explained by the losses through stool/vomiting but they don’t have to be alarming as the
children with bilateral oedema could still be losing weight as their oedema resolves. After all,
in all the groups a majority of children started out with bilateral oedema. Moreover, great
weight gain could not be expected in the course of three days. In terms of overall weight
gain1, more weight gain could be expected for the RUTF diet. RUTF has a > 5 energy density
compared to F100 but it has a similar ratio of nutrients to energy (in RUTF the skim milk
used in F100 is replaced by peanut butter) [58]. The higher energy density of RUTF could
have consequences for the duration of stay (or recovery rate) of a child as protocols advise
that discharge in most instances is based on a percentage weight gain (after loss of oedema)
of 15% and this can be adjusted up to 20% weight gain depending on the local situation [16].
Lastly, the electrolyte disturbances seen between the different groups; again, these results
were not significant. Looking at individual cases (minimums), low bicarbonate and potassium
levels at the end of the intervention were seen in all groups. All the groups regained a pH
within normal range (7.35-7.45) at the end of the diet. The F100 group started out with the
lowest mean blood pH (most acidotic) and overall gained the most in pH after the diet. The
mechanism behind hypokalaemia in malnourished patients is still unclear but it is associated
with diarrhoea. According to Agarwal et all [59] the diarrhoea does not necessary disturb the
absorptive mechanisms of potassium but fecal potassium losses are increased in diarrhoeal
diseases by unabsorbed anions (which obligate potassium), by electrochemical gradients
secondary to active chloride secretion, and probably by secondary hyperaldosteronism2. The
same study argues that it’s the potassium losses through this reduced net absorption of
potassium in diarrhoea rather than loss of muscle mass because of malnutrition that causes
hypokalaemia. If this is true, one would expect the diet with the highest rates of diarrhoea to
have the lowest potassium levels. This is the case in our results; F100 and RUTF had the
lowest potassium levels. Due to no significance, it is difficult to be firm on the case.
The results of this interim analysis are not significant enough to describe a trend, give definite
answers or provide informed recommendations on which diet to use during the transition
phase in the treatment of children with SAM. A bigger sample size and more samples that
reflect carbohydrate (mal)absorption are needed for this, as the powercalculation advised.
In addition, in analyses to come, being able to differentiate between the HIV positive and
HIV negative children in the bigger sample would be interesting, as HIV is known to
complicate the child’s recovery. What is more, up till now, no patients were seen to perish
during the different transition diets. If this trend continues, important will be to look at the
rate of recovery of the patients; how are they faring on the different diets? How long is their
duration of stay? For this, including the other (clinical questionnaire) variables in the analyses
will be essential. The outcome of these analyses could not only provide more definite
answers in relation to the effect of the different diets and inform the team in MOYO House
(and WHO) but also formulate further collaborative studies to possibly change (the current as
observed inadequate) rehabilitation regimes.
Alternatively, one could decide to take a closer look at the phase I (F75) diet; all the children
that passed away in this study sample died during this phase. Or the timing of transition;
1 This was difficult to record for this study sample because they were put on a different diet after the last
samples were taken, if clinically preferred. 2 Hyperaldosteronism is a medical condition in which the adrenal gland produces too much aldosterone, a
steroid hormone responsible for the secretion of potassium in the distal tubule and collecting duct of the kidneys.

19
perhaps patients are transitioned too early because they ‘cry’ for more food although their
body cannot yet take the food. Maybe even consider including a (protocolised) phase in
between phase I and II; this is already informal practice on MOYO ward by the slow
introduction of RUTF.
Overall, more recruitment is needed to determine the effect of the different transition diets.
But interesting is to think about possible implications for inpatient care in the case that the
hypothesis of F75+RUTF causing the most complications would be true. As stated before, the
high energy density of RUTF could also provide higher recovery rates and decrease patients’
duration of stay. In an underdeveloped country like Malawi, where health centres and staff
are scarce, these are important issues to consider. The rapid deterioration of a child with
SAM in any phase does not have to be fatal if they are closely monitored. But this issue
cannot be fully dealt with without facing the vast problems of a third world hospital setting.
5. Conclusion
No major differences came out of the interim analysis to suggest changing or breaking off the
study. No trends could yet be described to provide more insight. Recommended is to wait till
recruitment and sampling is finalised and perform analyses on a bigger sample size. These
results could possibly provide more definite answers in relation to the effect of the three
different diets used in the transition phase.
Acknowledgements
I want to thank both my supervisors, Dr. Robert Bandsma, from Groningen and Dr. Wieger
Voskuijl, on the ground, for sharing their knowledge and giving me unconditional support,
guidance and responsibility while conducting a study in a challenging research setting. In
addition, I want to thank the head of department of the paediatric department at QECH, Dr
Neil Kennedy, for allowing us to perform our study in the department. I also thank the Moyo
staff nurses for their hard work, sharing of experience and support throughout. This also goes
for George Fudzulani, lab technician at the department and Praise Kafulatila, lab archiver at
the MLW. Lastly, I want to thank the children and their guardians in Moyo ward for their
patience, strength and invaluable cooperation.
References [1] Li Liu et all for the Child Health Epidemiology Reference Group (CHERG) of WHO and
UNICEF. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with
time trends since 2000. The Lancet 2012; 379(9832): 2151-2161.
[2] Pelletier D.L. Frongillo E.A. Jr. Habicht J.P. Epidemiologic evidence for a potentiating effect of malnutrition
on child mortality. Am J Public Health 1993. 83(8):1130-3.
[3] UNICEF WWSa. Joint Statement on Community-Based Management of
Severe Acute Malnutrition. UNICEF publications. 2007. ISBN: 978-92-806-4147-9.
Available: http://www.unicef.org/nutrition/index_39468.html. Accessed 2013, 07 March.
[4] Black R.E. Allen L.H. Bhutta Z.A. et al. Maternal and child undernutrition: global and regional exposures
and health consequences. Lancet 2008;371(9608):243-60.
[5] Heikens G.T. Bunn J. Amadi B. Manary M. Chhagan M. Berkley J.A. et al. Case management of HIV-
infected severely malnourished children: challenges in the area of highest prevalence. Lancet 2008; 371
(9620):1305-7.
[6] Heikens G.T. How can we improve the care of severely malnourished children in Africa? PLoS Med. 2007;
4(2): e45.

20
[7] Heikens G.T, Manary M. Wasting disease in African children: the challenges ahead. Malawi Med J. 2009;
21(3): 101-5.
[8] Heikens G.T, Manary M. 75 years of Kwashiorkor in Africa. Malawi Med J. 2009; 21(3): 96-98.
[9] World Health Organization. Management of severe malnutrition: a manual for physicians and other senior
health workers. Geneva: World Health Organization 1999. ISBN 9241545119.
[10] International Human Development Indicators. Malawi: Country Profile: Human Development Indicators.
2013. Available: http://hdrstats.undp.org/en/countries/profiles/MWI.html. Accessed 2013, 13 March.
[11] IRIN. Malawi’s never-ending drug shortage problem. IRIN Humanitarian news and analysis. Feb 19, 2013.
Available: http://www.irinnews.org/Report/97503/Malawi-s-never-ending-drug-shortage-problem. Accessed
2013, 13 March.
[12] Carlton C. Lewin J. Malnutrition in Malawi: is permaculture the solution? Guardian Professional, March
13, 2013. Available: http://www.guardian.co.uk/global-development-professionals-
network/2013/mar/13/malnutrition-malawi-permaculture. Accessed 2013, 15 March.
[13] Reliefweb. Malawi Food Security Update July 2012. Available: http://reliefweb.int/report/malawi/malawi-
food-security-update-july-2012. Accessed 2013, 15 March.
[14] Trading Economics. Malnutrition prevalence; weight for age (% of children under 5) in Malawi. 2012.
Available http://www.tradingeconomics.com/malawi/malnutrition-prevalence-weight-for-age-percent-of-
children-under-5-wb-data.html. Accessed 2013, 16 March.
[15] Picot J. Hartwell D. Harris P. Mendes D. Clegg A.J. Takeda A. The effectiveness of interventions to treat
severe acute malnutrition in young children: a systematic review. Health Technol Assess 2012; 16(19).
[16] World Health Organization and United Nations Children’s Fund. WHO child growth
standards and the identification of severe acute malnutrition in infants and children. A joint
statement by the World Health Organization and the United Nations Children’s Fund. Geneva: World Health
Organization 2009. Available:
http://www.who.int/nutrition/publications/severemalnutrition/9789241598163_eng.pdf.
Accessed 2013 March 07.
[17] Iyer S.S. Chatraw J.H. Tan W.G. Wherry E.J. Becker T.C. et al. Protein energy malnutrition impairs
homeostatic proliferation of memory CD8 T cells. J Immunol. 2012; 188: 77–84.
[18] Jaganath D. Mupere E. Childhood Tuberculosis and Malnutrition. The Journal of Infectious Diseases 2012;
206:1809–1815.
[19] Savino W. Dardenne M. Velloso L.A. Dayse Silva-Barbosa S. The thymus is a common target in
malnutrition and infection. Br J Nutr 2007; 98:S11–6.
[20] Ngom P.T. Collinson A.C. Pido-Lopez J. Henson S.M. Prentice A.M. Aspinall R. Improved thymic
function in exclusively breastfed infants is associated with higher interleukin 7 concentrations in their mothers’
breast milk. Am J Clin Nutr 2004; 80:722-728.
[21] Rogero M.M. Tirapegui J. Vinolo M.A. et al. Dietary glutamine supplementation increases the activity of
peritoneal macrophages and hemopoiesis in early-weaned mice inoculated with Mycobacterium bovis bacillus
Calmette-Guerin. J Nutr 2008; 138:1343-1348.
[22] Heikens G.T. Bunn J. Amadi B. Manary M. Chhagan M. Berkley J.A. et al. Case management of HIV-
infected severely malnourished children: challenges in the area of highest prevalence. Lancet. 2008; 371(9620):
1305-1307.
[23] World Health Organization, Department of Child and Adolescent Health and Development (CAH) and
HIV/AIDS. WHO recommendations on the management of diarrhoea and pneumonia in HIV-infected infants
and children: integrated management of childhood illness (IMCI). Geneva: World Health Organization; 2010.
ISBN 9789241548083.
[24] Rollins N. Guidelines for an integrated approach to the nutritional care of HIV-infected
children (6 months–14 years). Geneva: World Health Organization; 2009. ISBN 9789241597524.
[25] Fergusson P. Tomkins A. HIV prevalence and mortality among children undergoing treatment for severe
acute malnutrition in sub-Saharan Africa: a systematic review and metaanalysis. Trans R Soc Trop Med Hyg
2009;103:541-548.
[26] Ashworth A. Khanum S. Jackson A. Schofield C. Guidelines for the inpatient treatment of severely
malnourished children. Geneva: World Health Organization; 2003. ISBN 9241546093.
[27] World Health Organization, Department of Child and Adolescent Health and Development. Management of
the Child with a Serious Infection or Severe Malnutrition – Guidelines for Care at the First-Referral Level in
Developing Countries. (IMCI Integrated Management of Childhood Illness). Geneva: World Health
Organization; 2000. ISBN 9241545313.
[28] Interim Guidelines for the Management of Acute Malnutrtion through Community Based Therapeutic Care.
Government of Malawi. 2007.

21
[29] Kerac M. Bunn J. Seal A. Thindwa M. Tomkins A. Sadler K. et al. Probiotics and prebiotics for severe
acute malnutrition (PRONUT study): a double-blind efficacy randomised controlled trial in Malawi. Lancet.
2009; 374(9684): 136-144.
[30] Akahane K. MSc Project (UCL) Comparison of two different inpatient feeding protocols for severely
malnourished children at a sentinel hospital in Malawi: A secondary data analysis. 2011.
[31] Kerac M. Akahane K. Blencowe H. Seal A. Collins S. Phiri A. et al. Inpatient feeding for children with
complicated Severe Acute Malnutrition: audit of Ready-to-Use Food vs. F100 milk in transition phase. Abstract
and Lecture presentation, CAPGAN (Commonwealth Association of Paediatric Gastroenterology & Nutrition)
Conference, London, UK, July 21st to 23rd http://capgan.org/meeting2011prog.html. 2011. Accessed 2012
September 17.
[32] Department of Paediatrics & Child Health QECH, Blantyre, College of Medicine. Protocols for the
Management of Common Childhood Illnesses in Malawi. Blantyre: Second Edition, 2011.
[33] Lim S. Does the choice of feeding regimen for severe acute malnutrition affect the onset of diarrhoea in
paediatric patients? A retrospective case-notes study from a nutritional rehabilitation unit in Blantyre, Malawi
(Student Project); 2011.
[34] Zinser E. Have there been any changes in the causes of mortality with different re-feeding regimens in the
malnourished paediatric population in a large tertiary referral centre in Malawi? (Student Project); 2011.
[35] Maitland K. Berkley J.A. Shebbe M. Peshu N. English M. Newton C.R. Children with severe malnutrition:
can those at highest risk of death be identified with the WHO protocol? PLoS Med. 2006; 3(12): e500.
[36] James W.P. Intestinal absorption in protein-calorie malnutrition. Lancet 1968;1(7538):333-335.
[37] Bowie M.D. Barbezat G.O. Hansen J.D. Carbohydrate absorption in malnourished children. Am J Clin Nutr
1967; 20(2):89-97.
[38] Stanfield J.P. Hutt M.S. Tunnicliffe R. Intestinal biopsy in kwashiorkor. Lancet 1965; 2(7411): 519-523.
[39]Schneider R.E. Viteri F.E. Morphological aspects of the duodeno-jejunal mucosa in protein-calorie
malnourished children and during recovery. Am J Clin Nutr 1972; 25(10): 1092-1102.
[40] Sullivan P.B. Marsh M.N. Mirakian R. Hill S.M. Milla P.J. Neale G. Chronic diarrhea and malnutrition--
histology of the small intestinal lesion. J Pediatr GastroEnterol. Nutr. 1991; 12(2):195-203.
[41] Douard V. Ferraris R.P. Regulation of the fructose transporter GLUT5 in health and disease. Am J Physiol
Endocrinol Metab. 2008; 295(2): e227-237
[42] Rao S.S. Attaluri A. Anderson L. Stumbo P. Ability of the normal human small intestine to absorb fructose:
evaluation by breath testing. Clin. Gastroenterology Hepatology 2007; 5(8): 959-963.
[43] Jentjens R.L. Moseley L. Waring R.H. Harding L.K. Jeukendrup A.E. Oxidation of combined ingestion of
glucose and fructose during exercise. J Appl Physiol. 2004; 96(4): 1277-1284.
[44] Rowlands D.S. Thorburn M.S. Thorp R.M. Broadbent S. Shi X. Effect of graded fructose congestion with
maltodextrin on exogenous 14C-fructose and 13C-glucose oxidation efficiency and high-intensity cycling
performance. J Appl Physiol. 2008; 104(6): 1709-1719.
[45] Bandsma R.H. Spoelstra M.N. Mari A. Mendel M. van Rheenen P.F. Senga E. et al. Impaired Glucose
Absorption in Children with Severe Malnutrition. J Pediatr. 2011; 158(2):282-287.
[46] Bandsma R.H. Mendel M. Spoelstra M.N. Reijngoud D.J. Boer T. Stellaard F. et al. Mechanisms behind
decreased endogenous glucose production in malnourished children. Pediatr Res. 2010; 68(5): 423-8.
[47] Talbert A. Thuo N. Karisa J. Chesaro C. Ohuma E. Ignas J. et al. Diarrhoea complicating severe acute
malnutrition in Kenyan children: a prospective descriptive study of risk factors and outcome. PloS one. 2012;
7(6): e38321.
[48]Odey F.A. et all. Hypokalaemia in children hospitalised for diarrhoea and malnutrition in Calabar, Nigeria.
Niger Postgrad Med J. 2010; 17(1):19-22.
[49] Brewster D.R. Manary M.J. Menzies I.S. O’Loughlin E.V. Henry R.L. Intestinal permeability in
kwashiorkor. Arch Dis Child 1997; 76: 236-241.
[50] Welsh F.K. et all. Gut barrier function in malnourished patients. Gut. 1998;42(3):396-401.
[51] Berkley J.A. Lowe B.S. Mwangi I. Williams T. Bauni E. et al. Bacteremia among children admitted to a
rural hospital in Kenya. N Engl J Med 2005; 352: 39-47.
[52] Brewster D.R. Critical appraisal of the management of severe malnutrition: 3. Complications. J Paediatr
Child Health 2006; 42: 583–593.
[53] Smith et all. Gut Microbiomes of Malawian Twin Pairs Discordant for Kwashiorkor. Science 2013;
339(6119): 548-554.
[54] Kerac, M.et all. Prevalence of wasting among under 6-month-old infants in developing countries and
implications of new case definitions using WHO growth standards: a secondary data analysis. Arch Dis Child
2011; 96:1008-1013.
[55] Sikorski et all. Preliminary evaluation of the Moyo chart—a novel, low-cost, weight-for-height slide chart
for the improved assessment of nutritional status in children.Transactions of the Royal Society of Tropical
Medicine and Hygiene 2010; 104: 743-745.

22
[56] Shepherd S.J. et all. Fructose Malabsorption and Symptoms of Irritable Bowel Syndrome: Guidelines for
Effective Dietary Management. J Am Diet Assoc. 2006;106:1631-1639.
[57] Management of Malnutrition in Children Under Five Years. Mother and Child Nutrtion 2013. Available:
http://motherchildnutrition.org/malnutrition-management/info/rutf-plumpy-nut.html. Accessed: 2013,12 April.
[58] Diop E.H.I. et all. Comparison of the efficacy of a solid ready-to-use food and a liquid, milk-based diet for
the rehabilitation of severely malnourished children: a randomized trial. Am J Clin Nutr 2003;78:302-307.
[59] Agarwall R. et all. Pathophysiology of potassium absorption and secretion by the human intestine.
Gastroenterology 1994;107(2):548-571.

23
Appendix A: Consent form English
Appendix Consent Form Parent or Guardian
Research Topic: The effect of different nutritional regimens in the treatment of severe acute malnutrition Malnutrition makes the body weaker and less able to fight infections. Malnutrition also causes the gut to work less well. The gut is where food is taken up by the body. We are conducting a study to compare the results of three different diets in malnourished children.
To obtain the answers to our questions, your child will receive one of three possible diets after we have seen some improvement on the diet the child is receiving at this moment. These diets are the same as we already use to treat malnutrition in children. To obtain a better idea on what diet is better for children with malnutrition, we need to take 3 times some blood from your child. Taking the blood will give some mild pain for the child and the parent should not worry. The total amount of blood we will take is less than two teaspoons and will not have any effect on your child. We will also take some urine and feces to analyse what the effects are of the two different diets. All this information will help us to give even better care to children with malnutrition in the future. You are free to participate or not, and this will not influence the way your child is cared for here at the hospital. If you do not understand any part of this consent form, please inform the investigator so that further explanation can be given. Please feel free to call Dr Wieger Voskuijl: Department of Paediatrics & Child Health QECH; cell 09966 04638, Sara van Vliet, Department of Paediatrics & Child Health QECH; cell 09968613 19. If you have any issues regarding your rights to participate in this study, please contact the chairman of Ethics Committee whose contact are as follows: Lucinda Manda-Taylor College of Medicine, P/Bag 360, Blantyre, University of Malawi 01871911
____________________________ I have understood the above information and I voluntarily agree/disagree to participate in this research. Name of Child Date Signature OR Right Thumbprint Name of Interviewer Signature

24
Appendix B: Questionnaires for clinical assessment
INFORMATION TO BE TAKEN ON ADMISSION - Enrollment in TranSAM
General information
Patient study number:
Patient’s name:
Patient DOB (d -mm-yyyy):
HIMS:
Guardian’s (preferably Mom’s) name:
Guardian (preferably Mom’s) DOB (d-mm-yyyy):
Patient’s Address:
Date of admission (d-m-y):
Nutritional diagnosis on admission
Weight (in kg)
MUAC (in cm))
Length (in cm)
Weight/Height (in SD below the mean)
Presence of oedema (0/+/++/+++)
For how long has the child been breastfed?
Which complementary diet is the child taking
presently?
Anorexia (nr. days):
Co-Morbidity:
Reactive/non-Reactive (R/NR):
Duration of illness before admission (in weeks):
Main complaint:
Duration, if any, of oedema before admission
(in weeks):
Diarrhoea in preceding days (nr. days):
Nr. of diarrhoea (‘episodes’) in last 3 months:
Vomiting (nr. of days):

25
CLINICAL ASSESMENT TO BE TAKEN DAILY (8:00 AM and 4:00 PM)
-Clinical assessment in TranSAM DAY date: DAY date: DAY date: AM PM AM PM AM PM
Weight (kg)
Appetite (Poor/Fair/Good/Excellent)
Finishing feeds (Y/N)
Stool consistency (Normal/Loose/ Watery/Bloody)
Stool frequency AM = Since sunrise/last 24 hours
PM = Since midday
Number of vomits (last 24 hours)
Losses compensated (Good/Fair/Poor/Absent)
Presence of oedema 0/+/++/+++
Hydration status (Dehydrated N=0, mild=1, moderate=2, severe=3)
IV rehydration Y/N (if Y, specify)
Capillary Refill Time (in seconds)
Temperature (in degrees Celsius)
Chest auscultation (Crepitations Y/N)
Saturation (%)
Respiratory rate (per minute)
Heart rate (per minute)
Liver size (in cm) (Enlarged = > 2cm, Y/N)

26
Appendix C: Case report form (sample 1)
SAMPLE 1
Code Parameter Tube Fluid Tube Cupjes Total
Glucose NA
whole blood
0,5 ml
Lactate NA
whole blood
Sodium NA
whole blood
Potassium NA
whole blood
Chloric acid NA
whole blood
Ph NA
whole blood
A1 8-OhdG serum (rood) plasma 0,5 ml 200 microliter 0,5 ml
8-OhdG serum (rood) plasma 0,5 ml
200 microliter 0,5 ml
Citrulline serum (rood) plasma 0,5 ml
200 microliter 0,5 ml
B1 Albumin EDTA (paars) plasma 0,25 ml 200 microliter 0,25 ml
2,25 ml
U1 8-OhdG Eppendorf cup urine 0,5 ml 0,5 ml 0,5 ml
F1 Elastase Eppendorf cup faeces 1 g 1 g 1 g
Elastase Eppendorf cup faeces 1 g 1 g 1 g
Microbioma Eppendorf cup faeces
250 mg 250 mg 250 mg
Alpha 1 antitrypsine pot faeces 5 g 5 g 5 g
Ph Eppendorf cup faeces 1 g 1 g 1 g
Total amount blood: 2,25 ml
Total amount urine: 0,5 ml
Total amount faeces 8,25 g