Embed Size (px)
Citation preview

Evaluation of the toricimplantable collamer lens forsimultaneous treatment ofmyopia and astigmatismExpert Rev. Med. Devices 12(1), 25–39 (2015)
Marianne O Price*1
and Francis W Price Jr2
1Cornea Research Foundation of
America, 9002 N. Meridian St, Suite
212, Indianapolis, IN 46260, USA2Price Vision Group, Indianapolis, IN,
USA
*Author for correspondence:
Tel.: +1 317 814 2990
Fax: +1 317 814 2806
Myopic astigmatism is a prevalent condition that can be treated with spectacles, contactlenses, or laser refractive surgery. However, these treatment options have functionallimitations at higher levels of refractive error. The toric implantable collamer lens is designedto treat a broad range of refractive error, generally up to -18 diopters with +1 to +6 dioptersof astigmatism. Approval for a more limited treatment range of up to 15 diopters of myopiawith +1 to +4 diopters of astigmatism is being sought in the US, where this device has notyet received marketing approval. Surgical correction of high-myopic astigmatism can belife-altering and allow people to participate in activities that were not previously feasiblebecause of visual limitations. The toric implantable collamer lens is implanted behind the irisand in front of the natural crystalline lens. With earlier lens designs, it was necessary tocreate an iridectomy or iridotomy to prevent pupillary block. The newest toric implantablecollamer lens model has a small central hole that is not visually noticeable. This eliminates theneed to create a hole in the iris, thereby enhancing the safety of the procedure.
KEYWORDS: astigmatism • keratoconus • myopia • pellucid marginal degeneration • phakic intraocular lens
Myopic astigmatism: prevalence &treatment optionsThe prevalence of myopia has been increasingand currently exceeds 40% in adolescents andadults in the US and surpasses 70% in teenagehigh school students in Singapore [1,2]. Higherlevels of myopia are associated with higher lev-els of education, more time spent on nearwork and less time spent outdoors. Approxi-mately one-third of myopes also have at least1 diopter of astigmatism [3].
The treatment options for myopic astigma-tism include spectacles, contact lenses, and sur-gical vision correction (BOX 1). While spectaclesare quite safe, many do not care for the appear-ance, functional limitations, poor peripheralvision, thick edges, and chromatic aberrationswith higher myopic corrections. Furthermore,spectacles that correct myopia reduce the appar-ent image size by approximately 2% per diopterof correction [4]. This means that for someonewho requires a 10 diopter myopic correction,
spectacles cause a 20% reduction in image size,reducing the ability to discern fine detail.
Contact lenses are a popular treatmentoption, but many people are contact lensintolerant because of dry eyes or because ofliving or working in dusty, dry, or pollutedconditions. Moreover, the use of contact lensesdepends upon access to a high quality sourceof potable water for hand and lens cleaning.Even with good water quality, the risk of eyeinfections is increased with contact lens use,particularly with overnight wear.
Neither contact lenses nor glasses are com-patible with certain activities, such as watersports. Also, contact lenses both move androtate on the eye with every blink [5]. This cancause visual distortions and glare that increasewith the amount of astigmatism correction.Finally, those with high myopic astigmatismcan have significant residual distortion withglasses or fluctuating vision with contacts andmay prefer a permanent surgical solution thatminimizes visual distortion.
informahealthcare.com 10.1586/17434440.2015.984685 � 2015 Informa UK Ltd ISSN 1743-4440 25
Device Profile
Exp
ert R
evie
w o
f M
edic
al D
evic
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
02/
01/1
5Fo
r pe
rson
al u
se o
nly.

Box 1. Summary of competing technologies in the field.
Spectacles
• Strengths:
– Safe and readily adjustable means of vision correction
• Weaknesses:
– Alters appearance and may not be considered esthetically appealing
– Not compatible with certain activities such as water sports
– Reduces image size in proportion to the amount of myopic correction
– For high levels of correction, the edges of the spectacles can become very thick and cause visual distortion
Contact lenses
• Strengths:
– More esthetically appealing than spectacles
– Cause less image minimization than spectacles for myopic correction
• Weaknesses:
– Many people cannot tolerate contact lenses because of dry eyes or because they live or work in dusty, dry, or polluted conditions
– Contact lenses move with each blink which can result in significant visual fluctuation with astigmatism correction, particularly
in the better-tolerated soft lenses
– The risks of eye infections are substantially increased in contact lens wearers, particularly with overnight use or in areas of the
world with sanitation challenges
Laser refractive surgery
• Strengths:
– Modern lasers provide very predictable and stable corrections in the low to moderate range of refractive error
– Avoids the risks associated with intraocular procedures
• Weaknesses:
– Approximately 10% of those with refractive error are not candidates for laser vision correction because of insufficient corneal
thickness or concerns about corneal biomechanical stability
– Predictability and stability decline at high levels of correction
– Dry eye symptoms can be exacerbated because corneal nerves are severed and require time to regenerate.
– Removal of corneal tissue is irreversible.
– Complicates lens calculations when future cataract surgery is needed
Iris-supported phakic intraocular lens
• Strengths:
– Reversible by removing the implanted lens
– Preserves accommodation and corneal architecture.
• Weaknesses:
– Has the inherent risks of an intraocular procedure
– Considered more surgically challenging than placement of a toric implantable collamer lens
– The Artisan/Verisyse model is rigid and requires a 5–6 mm incision for implantation and a second incision of equal size in a
different location for later removal in conjunction with cataract surgery
– The flexible Artiflex/Veriflex model may be less stable with trauma and has been associated with pigment dispersion
– The nontoric Verisyse is the only model approved for use in the US
Refractive lens exchange
• Strengths:
– Effective for treating moderate to severe refractive error, especially in the presbyopic age group
• Weaknesses:
– Current intraocular lens designs cannot restore accommodation to the level provided by the natural, crystalline lens
– Refractive lens exchange increases the risk of retinal detachment in highly myopic eyes especially in younger patients (<50 years old)
Device Profile Price & Price Jr
26 Expert Rev. Med. Devices 12(1), (2015)
Exp
ert R
evie
w o
f M
edic
al D
evic
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
02/
01/1
5Fo
r pe
rson
al u
se o
nly.

Refractive surgical correction can take three basicapproaches: reshaping the cornea, replacing the crystalline lens,or implanting an intraocular lens (IOL) while leaving the crys-talline lens intact. The cornea can be reshaped with ablative orincisional procedures. The most common ablative procedure islaser in situ keratomileusis (LASIK). A flap (typically80–130 mm thick) is created and lifted, anterior stromal tissueis selectively ablated with an excimer laser, and the flap is laidback in place to speed visual recovery and minimize discom-fort. In contrast, with surface ablation procedures, such as pho-torefractive keratectomy (PRK), tissue is selectively ablatedfrom the corneal surface with or without prior removal of thecorneal epithelium. Corneal ablation procedures require suffi-cient corneal biomechanical stability and thickness to correctthe refractive error without destabilizing the cornea [6].
The cornea can also be reshaped by making incisions to selec-tively weaken certain areas. Incisional procedures, known asastigmatic keratotomy or limbal relaxing incisions, were tradi-tionally performed manually with a blade. While they can nowbe performed more reliably with a femtosecond laser [7], anyincisional reshaping severs collagen lamellae and is inherentlynot as predictable or stable as ablative reshaping of the cornea.
Lens replacement is an excellent option for older adults whohave lost much of their accommodative amplitude and alreadyhave, or may soon develop, cataracts. On the other hand,implanting a phakic IOL (pIOL), while leaving the patient’snatural crystalline lens in place, is preferable for preservingaccommodation in younger adults [8].
Phakic IOLs (pIOL) come in three fundamental designs(angle-supported, iris-fixated, and posterior chamber), whichtake different approaches to securing the lens in the eye [8,9].While surgeons generally consider anterior chamber angle-supported lenses to be the easiest to implant, over the years aseries of angle-supported lens designs have been associated withcorneal decompensation and removed from the market. Incontrast, current iris-supported and posterior chamber phakicIOL designs have been in continuous use for over 15 yearsworldwide.
Description of evidenceThe purpose of this review is to evaluate the efficacy of theVisian toric implantable collamer lens (TICL, Staar Surgical,Monrovia, CA, USA) for treatment of myopic astigmatism.The term ‘collamer’ refers to the lens material, which is acopolymer of hydroxyethyl methacrylate and porcine collagen.
Using the search terms ‘toric’ and ‘collamer’ 58 English-language articles describing use of the TICL were identified inthe PubMed database run by the US National Library ofMedicine. Of these, two reported outcomes from a prospectiverandomized study comparing the TICL with PRK [10,11], onewas a prospective multicenter clinical trial [12], 20 were caseseries for treatment of myopic astigmatism [13–32], 11 werecase series for treatment of keratoconus or other specialindications [33–43], 3 were review articles [44–47], 13 were casereports (£3 cases), and 4 were nonclinical studies or analyses.
Four retrospective case series reported combined efficacy out-comes from myopic and toric ICL implantations [47–50]. Of these,two reported combined safety outcomes, which we included inthe safety analysis, because the myopic and toric lens designs areso similar. Whenever it appeared that the cases in multiplereports from the same center may have substantially overlapped,we selected the publication with the longest follow-up or themost comprehensive set of cases to feature in this review.
We begin by describing the TICL and then present efficacyand safety data for treatment of myopic astigmatism. We nextconsider how the TICL compares with other surgical options.Finally, we assess therapeutic uses of the TICL for treating myo-pic astigmatism in patients with keratoconus or pellucid mar-ginal degeneration, following cataract extraction and intra-ocularlens implantation, and following penetrating keratoplasty.
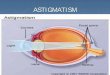
Visian toric implantable collamer lensThe TICL is a one-piece plate-haptic pIOL (FIGURE 1) that ispositioned between the iris and crystalline lens (FIGURE 2). Theoptic is 6 mm in diameter and the lens comes in four lengths(12.1, 12.6, 13.2, and 13.7 mm when packaged in balancedsalt solution) to accommodate different eye sizes. The design of
Iris
Ciliary process Zonules
Cornea
Sulcus
Crystalline lens
TICL
Figure 2. Diagram showing the placement of the toricimplantable collamer lens (in blue) behind the iris and infront of the crystalline lens.Reprinted with Staar Surgical‘s permission from the presentationmade to the Ophthalmic Devices Panel on March 14, 2014 [73].
Flexiblefootplate
Flexiblefootplates
Optic diameter
Lens lengthHaptic
Optic
Figure 1. Diagram of the toric implantable collamer lens.Reprinted with Staar Surgical’s permission from the presentationmade to the Ophthalmic Devices Panel on March 14, 2014 [73].
Evaluation of the TICL for simultaneous treatment of myopia & astigmatism Device Profile
informahealthcare.com 27
Exp
ert R
evie
w o
f M
edic
al D
evic
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
02/
01/1
5Fo
r pe
rson
al u
se o
nly.

the TICL is similar to that of the spherical implantable col-lamer lens (ICL), which has been in commercial use for20 years. The principal differences between the ICL and TICLare that the TICL has a toric surface on the anterior side ofthe optic with marks to facilitate surgical alignment of the toriccorrection with the patient’s axis of astigmatism.
The TICL is inserted through a temporal 3.0-mm incisionwith a micro-injector and allowed to unfold slowly in the ante-rior chamber with the horizontal meridian of the lens alignedwith the horizontal meridian of the eye. An ICL manipulator isused to position each flexible footplate in the ciliary sulcus
between the iris and the crystalline lens. The TICL is thenrotated up to 22-degrees from the horizontal meridian to alignthe toric correction with the patient’s axis of astigmatism [8].Each TICL comes with a guide demonstrating the amount anddirection of rotation required to correct the refractive cylinderin the designated eye (FIGURE 3). To control for potential cyclo-torsion when the patient is in a supine position, the surgeontypically marks the axis with the patient upright before surgery.
Traditionally, the surgeon had to create a peripheral laseriridotomy or two surgical peripheral iridectomies beforeimplanting the lens to prevent pupillary block [8–43]. Shimizu,in cooperation with Staar Surgical, developed an ICL with acentral 0.36 mm diameter hole, which obviates the need for aniridotomy or iridectomy without causing visual disturbances [51].The Centraflow ICL (model V4C) has the CE Mark and isavailable internationally; a premarket approval application hasnot been submitted yet in the US.
The TICL is generally designed to correct myopia rangingfrom -3.00D to -18.00D with cylinder of +1.00D to +6.00D,although approved treatment ranges vary by region [52]. It alsois used to reduce myopic astigmatism in patients whose refrac-tions exceed these ranges.
The TICL has been available commercially since 2002. It hasthe CE Mark and is available in over 60 countries. According tothe manufacturer, over 110,000 TICLs have been implantedglobally. In the US, the ICL received marketing approval fromthe Food and Drug Administration in 2008. A premarketapproval application for the TICL has been submitted for cor-rection of manifest refraction spherical equivalent from -3 to -15 diopters (or reduction of spherical equivalent up to -20 diop-ters) with cylinder of 1 to 4 diopters in adults (21–45 years old).
EfficacyRefractive predictability
A prospective, multicenter clinical trial of the TICL was initi-ated in the US in 2002. Designed to evaluate efficacy, thisstudy enrolled 210 eyes and followed subjects for one year [12].
The refractive predictability was impressive. The mean mani-fest refractive spherical equivalent (MRSE) improved from -9.36 D before TICL implantation to 0.05 D afterwards andthe mean cylinder improved from 1.93D preoperatively to0.51D postoperatively [12]. At the 1-week postoperative exam,77% of eyes were within ± 0.5D and 97% were within ±1 Dof the intended manifest refraction and these levels were main-tained over the 1-year study duration [12].
The excellent predictability achieved over a wide range ofspherical equivalent refractions is illustrated in FIGURE 4. Therefractive outcomes in other studies have echoed the findingsin the multicenter clinical trial, with 53–95% of treated eyesfalling within ± 0.5D of the intended MRSE (TABLE 1A & B)
[13–31,33–36].
Refractive stability
The TICL had excellent postoperative refractive stability inthe published studies. For example, in the multicenter clinical
20
15
10
5
0
0 5 10
R2 = 0.97
Attempted MRSE
Ach
ieve
d M
RS
E c
han
ge
15 20
Figure 4. The achieved versus the attempted manifestrefraction spherical equivalent change with use of the toricimplantable collamer lens for treatment of myopicastigmatism [10].Reprinted with Staar Surgical’s permission from the presentationmade to the Ophthalmic Devices Panel on March 14, 2014 [73].
Preoperative data –12.0Sph Cyl Axis
2.5 75862.0–12.5Lens label data X003
Rotate lens clockwise 11° after horizontal implantation
Axis ofastigmatism
90
270
90
90 60
30
60
3018
0 0
150
120
18011°
150
120
0
Figure 3. Toric implantable collamer lens implantationorientation diagram.Reprinted with Staar Surgical’s permission from the presentationmade to the Ophtalmic Devices Panel on March 14, 2014 [73].
Device Profile Price & Price Jr
28 Expert Rev. Med. Devices 12(1), (2015)
Exp
ert R
evie
w o
f M
edic
al D
evic
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
02/
01/1
5Fo
r pe
rson
al u
se o
nly.

Table
1A.Reportedefficacy
outcomeswiththetoricim
plantable
collamerlensforthetreatm
entofmyopic
astigmatism
.Thestudiesare
orderedfrom
thelongest
tothesh
ortest
follow
up.
Study(Year)
Eyes
Patients
Follow
up
(months)
Pre
MRSE
Mean±SD
Post
MRSE
Mean±SD
Pre
Cyl
Mean±SD
Post
Cyl
Mean±SD
Within
0.5
DMRSE
(%)
Within
1.0
DMRSE
(%)
Mean
Efficacy
Index
Postop
UCVA
‡Preop
BCVA
(%)
Ref.
Kam
iyaetal.(2013)
50
28
36
-9.47±2.91
-0.22±0.37
-2.23±1.09
-0.49±0.41
82
98
0.94
NR
[13]
Sarietal.(2013)
34
20
36
-10.56±3.36†
-0.41±0.50
-2.74±0.87
-0.51±0.36
53
82
NR
NR
[14]
Haseg
awaetal.(2012)
[15]
Low
cyl
168
NR
12
-9.15±3.02
0.37±0.98
-0.95±0.22
-0.29±0.32
NR
NR
NR
NR
Med
ium
cyl
141
NR
12
-9.19±2.33
-0.39±0.37
-1.91±039
-0.39±0.35
NR
NR
NR
NR
Highcyl
29
NR
12
-9.34±3.38
0.42±0.44
-3.5
±0.56
-0.47±0.34
NR
NR
NR
NR
San
ders
etal.(2007)
210
124
12
-9.36±2.66
0.05±0.46
1.93±0.84
0.51±0.48
77
97
NR
77
[12]
Pothireddyetal.
(2012)
110
65
12
-10.0
02.3
±1.1
0.4
±0.6
NR
85
1.04
NR
[16]
Alfonso
etal.(2013)
81
53
12
-6.62±2.84
-0.15±0.36
-3.09±1.18
NR
82
98
0.98
32
[17]
Bhikooetal.(2010)
77
42
12
-8.84±2.24
-0.63±0.51
2.38±1.19
0.44±0.56
82
92
NR
90
[18]
Alfonso
etal.(2010)
55
38
12
-4.65±3.02†
NR
-3.02±0.79
NR
95
100
1.08
91
[19]
Mertensetal.(2008)
43
23
12
-7.29±3.4
-0.17±0.40
-2.62±0.97
-0.20±0.43
77
98
1.05
72
[20]
Alfonso
etal.(2014)
35
20
12
-5.46±4.17†
-0.04±0.16
-3.14±1.19
-.029±0.42
97
100
1.01
77
[21]
Choietal.(2011)
29
20
12
-10.58±3.42
-0.32±0.41
3.6
±1.39
0.39±0.67
NR
NR
1.14
38
[22]
Alfonso
etal.(2010)
15
12
12
-4.41±1.27
-0.31±0.42
-4.85±0.83
-0.55±0.52
70
NR
0.9
NR
[23]
Shengetal.(2012)
54
29
9-12.08±4.22
-0.41±0.61
-1.88±1.49
0.39±0.61
82
89
NR
NR
[24]
Parketal.(2009)
30
20
8-10.63±2.83
0.04±0.64
2.43±1.24
0.73±0.47
70
93
NR
90
[25]
Eliesetal.(2010)
63
36
6-10.71±3.55
NR
3.60
NR
83
94
NR
NR
[26]
Changetal.(2009)
44
29
6-13.18±2.41
0.00±0.42
2.64±0.91
0.59±0.51
83
97
NR
69
[27]
Liuetal.(2013)
33
21
6-11.55±3.52
-0.68±0.36
-2.48±0.91
-0.50±0.19
64
91
1.09
82
[28]
Leeetal.(2011)
30
18
6-9.80±2.49
-0.09±0.38
-2.47±0.66
-0.44±0.44
NR
NR
1.16
NR
[29]
Kam
iyaetal.(2008)
30
18
6-10.8
±2.4
-0.13±0.18
2.1
±0.8
0.47±0.4
NR
100
0.87
NR
[30]
Hashem
etal.(2009)
35
19
3-7.61±4.02
-0.14±0.38
2.8
±1.45
0.63±0.75
NR
NR
NR
NR
[31]
†Data
issphere
ratherthanMRSE.
Cyl:Refractivecylinder
indiopters
(D);MeanEfficiency
Index:Ratio
ofpostoperative
uncorrectedvisual
acuity(UCVA)to
preoperative
best-correctedvisual
acuity(BCVA);MRSE:Man
ifest
refractionsphericalequivalentin
diopters
(D);NR:Notreported;SD
:Standarddeviation.
Evaluation of the TICL for simultaneous treatment of myopia & astigmatism Device Profile
informahealthcare.com 29
Exp
ert R
evie
w o
f M
edic
al D
evic
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
02/
01/1
5Fo
r pe
rson
al u
se o
nly.

trial, the mean MRSE changed by only 0.01 diopter between1 week and 1 year postoperatively (FIGURE 5). Likewise themean refractive cylinder changed by only 0.02 dioptersbetween 1 week and 1 year postoperatively (FIGURE 6). In3-year studies, Kamiya et al. found that mean MRSEchanged by -0.15 diopters and mean refractive cylinderchanged by 0.04 diopters between 1 month and 3 yearspostoperatively [13], and Sari et al. found no significantchange in refractive sphere or cylinder between 1 and 3 yearsafter TICL implantation (p = 0.99) [14]. Of course, somerefractive shift is expected with eventual aging and develop-ment of cataracts.
Visual outcomes
The visual outcomes were as impressive as the refractive out-comes in the US clinical trial. Postoperatively, 77% of treatedeyes had uncorrected visual acuity (UCVA) that equaled orexceeded the preoperative best spectacle corrected visual acuity(BSCVA) [12]. At 1 year, UCVA was ‡20/20 in 83% of treatedeyes and ‡20/40 in 96% [12]. The mean improvement inBSCVA was 0.88 lines, with 19% of the eyes gaining ‡2 linesof vision and 2% losing ‡2 lines of vision between the preop-erative and 1-year postoperative exams [12]. The visual out-comes in subsequent clinical studies echoed these findings(TABLE 1) [13–31,33–36].
SafetyThe TICL had a favorable Safety Index (ratio of postopera-tive BSCVA to preoperative BSCVA) in the publishedstudies (TABLE 2). Reported complication rates were low, withthe most frequent being axis misalignment or lens rotation(treated by repositioning the lens), cataract formation (whenvisually significant, treated by removing the TICL, extractingthe cataract, and implanting a posterior chamber IOL), andimproper lens sizing/vault (corrected by exchanging the lens).These are enumerated in TABLE 2 and discussed in greaterdetail in subsequent sections.Topical anesthesia can be used for TICL implantation
thereby avoiding complications associated with general or localanesthesia. Intraocular infection or inflammation is an uncom-mon but serious risk with any surgical procedure. Amongthe 1899 cases listed in TABLE 2 was one reported case ofendophthalmitis and one case of toxic anterior segment syn-drome [47]. A few cases of transient intraocular pressure eleva-tion were reported after the laser iridotomy and/or after thelens implantation.A few complaints of serious glare were noted in association
with the iridotomies or iridectomies. Also, pupillary block canoccur if the iridotomies or iridectomies are not patent, but thiscomplication was not reported in the reviewed TICL studies.As noted earlier, a newer TICL design with a small centralhole (Centraflow model) obviates the need for an iridotomy oriridectomy and eliminates concerns about pupillary block orglare from holes created in the iris [51]. The small central holedoes not significantly affect vision or optical quality of myopicT
able
1B.Reportedefficacy
outcomeswiththetoricim
plantable
collamerlensforthetreatm
entofkeratoco
nusorpellucidmarginal
degeneration.Thestudiesare
orderedfrom
longest
tosh
ortest
follow
up.
Study(Year)
Eyes
Patients
Follow
up
(months)
Pre
MRSE
Mean±SD
Post
MRSE
Mean±SD
Pre
Cyl
Mean±SD
Post
Cyl
Mean±SD
Within
0.5
DMRSE
(%)
Within
1.0
DMRSE
(%)
Mean
efficacy
index
Postop
UCVA
‡Preop
BCVA
(%)
Ref.
Camoriano
etal.(2012)
10
524
-6.71±0.9
-0.58±0.1
NR
NR
70
90
NR
NR
[36]
Alfonso
etal.
(2010)
30
21
12
-5.38±3.26
-0.08±0.37
-3.48±1.24
0.41±0.61
87
100
1.07
NR
[33]
Hashemian
etal.(2013)
22
14
6-4.98±2.63
-0.33±0.51
-2.77±0.99
-1.23±0.65
68
91
1.24
NR
[34]
Kamiyaet
al.
(2011)
27
14
6-10.11±2.46
0.10±0.43
-3.03±1.58
-0.56±0.74
85
96
1.01
NR
[35]
†Data
issphererather
than
MRSE.
Cyl:Refractivecylinder
indiopters
(D);MeanEfficiency
Index:Ratio
ofpostoperative
uncorrectedvisual
acuity(UCVA)to
preoperativebest-correctedvisual
acuity(BCVA);MRSE:Man
ifestrefractionsphericalequivalentin
diopters
(D);NR:Notreported
;SD:Standarddeviation.
Device Profile Price & Price Jr
30 Expert Rev. Med. Devices 12(1), (2015)
Exp
ert R
evie
w o
f M
edic
al D
evic
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
02/
01/1
5Fo
r pe
rson
al u
se o
nly.

lenses [51,53,54]. The Centraflow model has the CE Mark but isnot approved for use in the US.
Lens position, alignment & rotational stability
Adequate correction of refractive cylinder depends upon theproper centration and alignment of the toric axis when the lensis initially implanted as well as subsequent lens stability andlack of rotation. The lens was repositioned in 1.5% of the casesshown in TABLE 2. The most common reason was lens misalign-ment or decentration noted on the first postoperative day(1.1%) [12–18,20,22,26,34,47]. Spontaneous lens rotation requiringrepositioning was reported in six cases (0.3%) [13,15,27,31], and intwo cases (0.1%) a subsequent traumatic injury caused the lensposition to change, requiring repositioning [13]. Thus the datasuggests that the TICL has a high degree of rotational stability.
Several methods have been used to assess axis alignmentand rotational stability. In a series of 54 eyes implantedwith a TICL, Sheng et al. found from anterior chamberphotographs that the mean absolute value of the differencebetween the intended and achieved cylinder axis position was6.96 ± 8.37 degrees (range 0–40 degrees) [24]. Hashem et al.used an OPD-Scan II (Nidek Co Ltd, Gamagori, Japan) toassess the axis alignment and rotational stability of the TICL in35 eyes with the aid of refractive wavefront maps that displayedthe refractive power of the eye after subtracting the refractivepower of the anterior corneal surface [31]. They found that themean absolute value of the difference between the measuredaxis and the planned axis was 3.36 ± 2.50 degrees [31]. Furthercomparing measurements taken at successive postoperativeexams, they found that the mean absolute value of axis mis-alignment was 2.90 ± 2.11 degrees between the 1-day and1-month exams and 2.68 ± 2.11 degrees between 1-day and3-month exams in 34 of 35 treated eyes [31]. However in oneeye significant axis rotation was noted at the 3-month examand was correlated with an increase in manifest cylinder from0.50D at the 1-month exam to 3.75D at the 3-monthexam [31]. The misalignment was corrected by repositioningthe lens.
As demonstrated in this case, axis misalignment of 15 degreesor more reduces the intended cylinder correction by at least50%, and with axis misalignment of 30 degrees there is noreduction in the magnitude of the original cylinder. Therefore,the overall stability of the manifest cylinder outcomes overtime in multiple studies suggests that the TICL is rotationallystable in the vast majority of cases.
Sanders et al. prospectively assessed axis alignment at con-secutive postoperative examinations by slit lamp examinationand detected minimal axis change between one exam andthe next in most eyes, with observed changes generally fall-ing within the range of precision of the measurement pro-cess [12]. In 13 incidences where the recorded axis varied15 degrees or more between subsequent exams, the changedid not correlate with the manifest refraction, suggesting anerror in the axis measurement rather than a true shift inaxis [12].
Lens sizing & vault
The TICL is provided in four different lengths (12.1, 12.6,13.2, and 13.7 mm when packaged in balanced salt solution).The length of the TICL relative to the diameter of the ciliarysulcus determines its clearance over the crystalline lens, whichis called ‘vault’. The package labeling says the optimal range ofvault is 0.1 to 1 mm. Inadequate lens clearance can lead toanterior subcapsular cataract, whereas excessive vault can causeiris pigment dispersion or angle closure glaucoma. In the stud-ies summarized in TABLE 2, visually significant cataract was theprimary reason for lens removal and inadequate vault was theprimary reason for lens exchange.
Among the cases of anterior subcapsular cataract formationnoted in TABLE 2, most were judged to be trace and not visuallysignificant [12–16]. Those considered visually significant weretreated by removing the TICL in conjunction with cataract sur-gery. Few studies reported any complications associated with
10
–1–2–3
Mean MRSE ± 1 SD
–4–5–6–7M
RS
E, D
Pre-op 1 wk
–9.38
0.02 0.13 0.13 0.11 0.03
1 mo 3 mo 6 mo 12 mo
–9–8
–10–11–12–13
Figure 5. The stability of the manifest refractive sphericalequivalent reported as mean and standard deviation indiopters following treatment with the toric implantablecollamer lens [10].mo: Month; wk: Week.Reprinted with Staar Surgical’s permission from the presentationmade to the Ophthalmic Devices Panel on March 14, 2014 [73].
0.50
3.0
2.5
2.0
1.5
1.0
0.5
0.0Pre-op 1 wk
0.50
Mean diopter ± 1 SD
Man
ifes
t re
frac
tive
cyl
ind
er, D
0.52 0.520.45
1 mo 3 mo 6 mo 12 mo
1.95
Figure 6. The stability of the manifest refractive cylinderreported as mean and standard deviation in dioptersfollowing treatment with the toric implantable collamerlens [10].mo: Month; wk: Week.Reprinted with Staar Surgical’s permission from the presentationmade to the Ophthalmic Devices Panel on March 14, 2014 [73].
Evaluation of the TICL for simultaneous treatment of myopia & astigmatism Device Profile
informahealthcare.com 31
Exp
ert R
evie
w o
f M
edic
al D
evic
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
02/
01/1
5Fo
r pe
rson
al u
se o
nly.

Table
2.Publish
edsafety
outcomeswiththetoricim
plantable
collamerlens.
Within
each
treatm
entindication(m
yopic
astigmatism
or
keratoco
nus/pellucidmarginaldegeneration),thestudiesare
orderedfrom
thelongest
tothesh
ortest
follow
up.Thelast
twostudies
reportedsafety
outcomeswithboth
toricandnontoricim
plantable
collamerlens.
Myopic
astigmatism
Eyes
Length
of
follow
up
(months)
Mean
Safety
Index
%losing2or
more
lines
BCVA
Lens
reposition
(eyes)
Anterior
subcapsu
lar
cataract
(eyes)
Lensremoval
(eyes)
Lens
exch
ange
(eyes)
Endothelial
cellloss
(%)
Ref.
Kamiyaetal.
(2013)
50
36
1.16
06
4NR
NR
2.3
[13]
Sarietal.(2013)
34
36
NR
NR
32
NR
NR
8.7
[14]
Hasegaw
aetal.
(2012)
338
12
NR
NR
31
NR
10
[15]
Sanders
etal.
(2007)
210
12
NR
1.6
16
31
NR
[12]
Pothired
dyet
al.
(2012)
110
12
†0.9
11
1NR
10.3
[16]
Alfonso
etal.
(2013)
81
12
1.12
02
0NR
NR
NR
[17]
Bhikooetal.
(2010)
77
12
NR
NR
10
11
NR
[18]
Alfonso
etal.
(2010)
55
12
1.13
NR
00
0NR
NR
[19]
Mertensetal.
(2008)
43
12
1.14
2.4
10
0NR
NR
[20]
Alfonso
etal.
(2014)
35
12
1.08
00
00
04.4
[21]
Choiet
al.
(2011)
29
12
1.19
NR
10
NR
NR
NR
[22]
Alfonso
etal.
(2010)
15
12
1.07
NR
00
NR
NR
NR
[23]
Shengetal.
(2012)
54
9NR
0NR
0NR
23.5
[24]
Park
etal.(2009)
30
8NR
NR
00
NR
1NR
[25]
Eliesetal.(2010)
63
6NR
02
NR
NR
NR
NR
[26]
Changetal.
(2009)
44
6NR
02
00
011.0
[27]
Liuetal.(2013)
33
61.25
00
NR
NR
NR
NR
[28]
†Thereportedsafety
index
appearedto
havebeencalculatedincorrectlybasedonthedata.
BCVA:Best-correctedvisual
acuity;
MeanSafety
Index:ratioofpostoperative
BCVAto
preoperative
BCVA(in
Decim
alnotation).
Device Profile Price & Price Jr
32 Expert Rev. Med. Devices 12(1), (2015)
Exp
ert R
evie
w o
f M
edic
al D
evic
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
02/
01/1
5Fo
r pe
rson
al u
se o
nly.

Table
2.Publish
edsafety
outcomeswiththetoricim
plantable
collamerlens.
Within
each
treatm
entindication(m
yopic
astigmatism
or
keratoco
nus/pellucidmarginaldegeneration),thestudiesare
orderedfrom
thelongest
tothesh
ortest
follow
up.Thelast
twostudies
reportedsafety
outcomeswithboth
toricandnontoricim
plantable
collamerlens(cont.).
Myopic
astigmatism
Eyes
Length
of
follow
up
(months)
Mean
Safety
Index
%losing2or
more
lines
BCVA
Lens
reposition
(eyes)
Anterior
subcapsu
lar
cataract
(eyes)
Lensremoval
(eyes)
Lens
exch
ange
(eyes)
Endothelial
cellloss
(%)
Ref.
Leeetal.(2011)
30
61.28
1.28
00
00
NR
[29]
Kamiyaetal.
(2008)
30
61.28
NR
00
00
NR
[30]
Hashem
etal.
(2009)
35
3NR
NR
1NR
NR
NR
NR
[31]
Keratoco
nus/pellucid
Camorianoetal.
(2012)
10
24
NR
00
00
1NR
[36]
Alfonso
etal.
(2010)
30
12
1.16
00
NR
00
2.6
[33]
Hashemianetal.
(2013)
22
61.4
02
00
0NR
[34]
Kamiyaetal.
(2011)
27
61.12
00
0NR
NR
4.4
[35]
TICLandICL
Gomez-Baster
etal.(2014)
349
48
1.2
3.1
30
11
NR
[47]
Gonzalez-Lopez
etal.(2012)
100
11.16
00
00
0NR
[48]
†Th
ereported
safety
index
appearedto
havebeencalculatedincorrectlybasedonthedata.
BCVA:Best-corrected
visual
acuity;
MeanSafety
Index:
ratioofpostoperative
BCVAto
preoperative
BCVA(in
Decimalnotation).
Evaluation of the TICL for simultaneous treatment of myopia & astigmatism Device Profile
informahealthcare.com 33
Exp
ert R
evie
w o
f M
edic
al D
evic
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
02/
01/1
5Fo
r pe
rson
al u
se o
nly.

excessive vault. One reported pigment dispersion (prevalence8%) [18], and one reported a case of iridocorneal touch causedby excessive vault that was treated by replacing the lens with asmaller model [12].
Lindland et al. evaluated changes in ICL and TICL vaultunder different lighting conditions and found that theICL and TICL behaved similarly [55]. The mean vault was0.33 ± 0.17 mm in mesopic conditions, and in photopic con-ditions the vault decreased by -0.04 ± 0.06 mm [55]. This wasnot a clinically significant change relative to the recom-mended range of vault that is well-tolerated.
In another study, Lindland et al. assessed whether vaultchanges with accommodation and did not detect a significantdifference [56]. However, they did note a tendency toward lowervault in older patients. This is consistent with the increase inthe thickness of the human crystalline lens with age. In theirseries of 77 eyes followed for an average of 5 years (range 1–7 years), 10 eyes developed anterior subcapsular cataract [51].One case was surgically induced and five were associated withlens touch. Interestingly, they had two eyes with apparent lenstouch that did not develop anterior subcapsular cataract [56].
In most studies, the horizontal corneal diameter was mea-sured with calipers or a topographic device to select the appro-priate lens length. However, studies have shown poorcorrespondence between external measurements and the inter-nal dimensions of the eye [8]. Although direct measurement ofthe ciliary sulcus diameter with ultrasound biomicroscopy isless commonly performed, studies suggest it can reduce theincidence of inadequate or excessive vault [57,58].
Endothelial cell loss
The endothelial cells lining the inner surface of the cornea areessential for maintaining appropriate corneal hydration andclarity. These cells have limited regenerative capability andslowly decline in density with age. Intraocular surgery can causeimmediate and/or chronic corneal endothelial cell loss.
Reported endothelial cell loss following TICL implantationis shown in TABLE 2, with the longest follow up being 3 years.These results are comparable to the cell loss measured in stud-ies with the non-toric ICL, for example the 3-year US clinicaltrial [59]. Only a few studies have evaluated longer-term endo-thelial cell loss. Alfonso et al. reported cumulative cell loss of7.7% at 5 years and Igarashi et al. reported cumulative cell lossof 6.2% with 8-year follow-up after ICL implantation [60,61].
Conservatively extrapolating from available pIOL data, theAmerican National Standards Institute has estimated the long-term cell loss following implantation of a pIOL and issuedguidelines for the minimum preoperative endothelial cell den-sity a candidate should have based on age at the time of lensimplantation [ANSI Z80.13–2007 (R2012)]. In a post-approval ICL study conducted in the US, a subset of eyes(about 6% of those with data) experienced cell loss at a higherrate than the rest of the cohort through 7 years, while furthermeasurements taken after 10 years in several of these eyesshowed a decrease in the rate of cell loss [62]. No factors could
be identified which differentiated the small group with greatercell loss from the rest of the cohort [62]. All of the eyes in theUS study had laser iridotomies, which some studies suggestmay be associated with chronic long-term endothelial cell lossin some eyes [63,64]. The newer Centraflow TICL model elimi-nates the need for an iridotomy or iridectomy, so it will beinteresting to see how the long-term endothelial cell loss datacompares with this lens model.
TICL versus other treatment optionsTICL versus laser refractive surgery
Some patients are not considered candidates for laser refractiveprocedures because of limited corneal thickness and/or ques-tionable corneal biomechanical stability. Furthermore, thepredictability of laser refractive outcomes declines at high levelsof correction, whereas the TICL has excellent refractivepredictability over a wide range of MRSE and cylinder(FIGURE 4).
The better predictability of the TICL for higher levels ofastigmatism was demonstrated nicely in a retrospective analysisof 338 eyes implanted with a TICL versus 196 eyes treatedwith LASIK (MEL 80, Carl Zeiss), in which Hasegawa et al.segregated the eyes by the degree of preoperative manifest cylin-der (low £1.25D, medium 1.5–2.75D, or high >3D) [15]. Thepredictability in correcting cylinder was comparable for the twotreatments in the low cylinder range [15]. In the moderate cylin-der range, 91 versus 79% corrected within 0.5D of the mani-fest refractive cylinder for LASIK and TICL, respectively [15].In contrast, in the high cylinder range the TICL was more pre-dictable (53 vs 72% corrected within 0.5D of the attemptedcylinder correction for LASIK vs TICL, respectively) [15]. Ofnote, the preoperative MRSE was significantly more myopic inthe TICL eyes (mean -9.3D vs ~-5D in the LASIK eyes),because the TICL can treat high myopia more predictably thanLASIK without concerns about corneal thickness. Postoperativesurgical interventions were more common after LASIK: theTICL axis was repositioned in three eyes (0.89%), whereas8.8% of the LASIK eyes were retreated within 1 year [15].
Schallhorn et al. conducted a randomized prospective studythat enrolled 46 subjects with moderate to high myopia [10].Half of the subjects (23 subjects, 43 eyes) received a TICL andthe other half (23 subjects, 45 eyes) had conventional PRK per-formed with a VISX Star S3 laser followed by application ofmitomycin C. At 1-year, UCVA was significantly better in theTICL group: the rate of 20/20 or better vision was 97 vs 82%(p = 0.033) and the rate of 20/12.5 or better vision was 47 ver-sus 9% (p < 0.001) in the TICL and PRK groups, respec-tively [10]. Also, mean BSCVA was 1 line better with the TICL(-0.17 ± 0.06 vs -0.09 ± 0.08, p < 0.001), and a significantlyhigher proportion of the TICL eyes realized an improvementof 1 or more lines in BSCVA (95 vs 39% in the PRK group,p < 0.001) [10]. The TICL had better predictability (attemptedvs achieved correction), and those who received the TICL per-formed significantly better on certain measures in a night driv-ing simulation test [11].
Device Profile Price & Price Jr
34 Expert Rev. Med. Devices 12(1), (2015)
Exp
ert R
evie
w o
f M
edic
al D
evic
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
02/
01/1
5Fo
r pe
rson
al u
se o
nly.

Kamiya et al. compared TICL implantation in 30 eyes(18 patients) with wavefront-guided LASIK (Technolas 217z,Bausch & Lomb) in 24 eyes (17 patients) to correct high myo-pic astigmatism [30]. Although the preoperative mean MRSE,manifest cylinder and UCVA were all significantly worse in theTICL group (MRSE: -10.8 ± 2.4 vs -7.9 ± 1.5D, p < 0.001;manifest cylinder: 2.1 ± 0.8 vs 1.3 ± 0.4, p = 0.004), a higherpercentage of TICL eyes ended up within ± 0.5D of theattempted MRSE correction (100 vs 71%) [30]. Also, the safetyand efficacy indices were higher in the TICL group (safetyindex 1.28 ± 0.25 vs 1.01 ± 0.16 and efficacy index 0.87 ±0.15 vs 0.83 ± 0.23) [30].
TICL versus ICL plus LASIK
The ICL became available over a decade before the TICL.During that time interval, high myopic astigmatism could betreated with a spherical ICL followed by excimer laser treat-ment several months later in what was termed a ‘bioptics’approach by Zaldivar et al. [65].
Alfonso et al. retrospectively compared 81 TICL eyes with83 bioptics eyes [17]. At 1 year, 81.5% of the TICL eyes versus94% of the bioptics eyes were within ±0.5D of the attemptedspherical equivalent correction [17]. The safety index was com-parable in both groups while efficacy was higher in the biopticsgroup [17]. Choi et al. compared 29 TICL eyes and 26 biopticseyes at one year and found that the visual and refractive out-comes and safety and efficacy indices were similar in bothgroups [22]. Perez-Vives et al. used an adaptive optics visualsimulator to simulate the vision after TICL implantation andafter a bioptics procedure for treatment of moderate- and high-myopic astigmatism [66]. Visual acuity at different contrasts andcontrast sensitivity at 10, 20, and 25 cycles degree (-1) weremeasured for 3- and 5-mm pupils. Significant differencesbetween treatments were most prevalent in the high-myopicastigmatism group and with the larger (5-mm) pupil size [66].In all cases in which a significant difference was detected, thesimulated visual acuity and contrast sensitivity were better withthe TICL than with the bioptics approach [66]. Compared witha bioptics approach, some obvious advantages of TICL implan-tation are that it’s removable, it maintains the corneal architec-ture, and it precludes a second surgical procedure with theinherent risks and costs.
TICL versus toric iris-supported pIOL
Lee et al. retrospectively compared outcomes of TICL implan-tation in 30 eyes of 18 patients with outcomes of the toriciris-supported Artisan lens (Ophtec BV, Groningen, the Neth-erlands) in 31 eyes of 22 patients [29]. Preoperatively, the twogroups were comparable in age (mean 29 years), UCVA (mean1.66 LogMAR), BSCVA (mean 0.025 LogMAR), mean spheri-cal equivalent (-10D), and mean manifest cylinder (-2.5D). At1, 3 and 6 months postop, BSCVA and spherical equivalentwere comparable in both groups [29]. However, manifest cylin-der power was significantly better in the TICL group at onemonth, because the foldable TICL was inserted through a
3-mm temporal corneal incision whereas the rigid Artisan lensrequired a larger 6.1–6.3 mm sclero-corneal incision that wasclosed with sutures [29]. Six months after lens implantation,UCVA was approximately one line better in the TICL group(-0.04 ± 0.08 vs 0.03 ± 0.06, p = 0.021) [29].
A newer, foldable, iris-supported pIOL, the Artiflex (Ophtec),can be inserted through a 3.2-mm incision, more similar to theTICL. The use of a smaller incision can speed healing and reducesurgically induced astigmatism and higher order aberrations. In aEuropean multicenter study, the toric Artiflex had excellentrefractive predictability: 82% of treated eyes were within ±0.5Dof the intended refraction [67]. The most common complicationwas pigment and nonpigment precipitates (15 and 12%, respec-tively). Also, 2 eyes (1.7%) lost two or more lines of BSCVAbecause synechiae developed postoperatively.
Enclavation of iris tissue between the claws of the hapticsshould ensure rotational stability in the absence of postopera-tive trauma. However, it requires a bi-manual technique, whichcan be more challenging than implantation of a posteriorchamber pIOL.
Therapeutic indicationsKeratoconus & pellucid marginal degeneration
The TICL has been used effectively, either alone or in combi-nation with other treatments, for patients with keratoconus orpellucid marginal degeneration (PMD), conditions in whichthe cornea thins and bulges resulting in myopicastigmatism [33–36]. Clinically significant keratoconus has aprevalence of approximately 1 in 2000 people.
Appropriate candidates for TICL implantation alone arecontact lens intolerant patients with early or mild keratoconusor PMD, little to no central corneal scarring and minimalirregular astigmatism. It is also important to determine that therefraction has remained stable for at least 2 years to help ensurethat the surgical correction will continue to be appropriateover time.
Good results have been obtained using a 2-stage procedurein patients with progressive keratoconus or PMD, as evidencedby a changing refraction and corneal topography [37,39]. First,the cornea is stabilized by collagen cross-linking and severalmonths later a TICL is implanted to correct the refractiveerror.
Patients with more advanced keratoconus or PMD and poorBSCVA because of irregular astigmatism have been treated suc-cessfully with a 3-stage procedure [38,40]. Intracorneal ring seg-ments are implanted to regularize the corneal shape andimprove BSCVA, and collagen cross-linking is used to stabilizethe cornea. Finally, a TICL is implanted to correct the residualmyopic astigmatism (TABLE 1).
Following corneal transplantation
Refractive outcomes are unpredictable after penetrating kerato-plasty. Many patients end up with myopia, as well as regularand irregular astigmatism, and 10–15% may have to use ahard contact lens to provide a more regular surface to the eye
Evaluation of the TICL for simultaneous treatment of myopia & astigmatism Device Profile
informahealthcare.com 35
Exp
ert R
evie
w o
f M
edic
al D
evic
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
02/
01/1
5Fo
r pe
rson
al u
se o
nly.

for best vision. Those who are contact lens intolerant may becandidates for surgical vision correction. Iovieno et al. evaluatedTICL implantation to correct ametropia in seven eyes of sevenkeratoconus post-keratoplasty patients who were unable to wearglasses or contact lenses [42]. Patients gained a mean of eightlines of UCVA going from 1.18 ± 0.4 to 0.2 ± 0.1 [42]. TheMRSE improved from -8.09 ± 3.77 to 0.33 ± 0.54, while themanifest cylinder improved from -4.36 ± 0.75 to 1.74 ±0.84 [42].
Likewise, Alfonso et al. evaluated TICL implantation in15 post-keratoplasty eyes of 15 patients who were unable towear glasses because of anisometropia or contact lenses becauseof dry eye [43]. Laser refractive surgery was contra-indicatedbecause of high myopia and astigmatism with limited baselinecorneal thickness. The mean MRSE improved from -9.80 ±5.88 to -0.95 ± 1.12 [43]. The safety index was 1.58 and nopatient lost more than 1 line of visual acuity [43]. No complica-tions were noted through 2 years of follow up [43].
TICL as a piggy-back lens with a PCIOL
Kojima et al. treated residual myopic astigmatism in a series of8 pseudophakic eyes in 5 patients with piggyback insertion of aTICL [41]. All eyes were corrected within 0.5D of the intendedMRSE and UCVA improved from 20/125 preoperatively to20/30 postoperatively (0.76 ± 0.43 to 0.20 ± 0.46) [41].
ConclusionThe TICL is highly effective for correcting myopic astigmatismand is more predictable and stable than laser refractive surgeryfor correcting high levels of myopia and astigmatism. Further-more, the lens is removable and can provide more functionalvision than spectacles or contact lenses for high myopic astigma-tism. By combining the astigmatic and myopic corrections in thelens implant, patients can have refractive error corrected with asingle surgery instead of requiring either astigmatic incisions orlaser ablative surgeries to be performed on the cornea afterimplantation of a spherical ICL. Reported complication rates arelow, with the most common being repositioning to adjust thetoric alignment, cataract formation, and exchange for a differentlens size. The new Centraflow model further enhances safety byeliminating the need for an iridectomy or iridotomy.
Expert commentary & five-year viewWith any elective procedure, minimizing complications is key.Complications with the TICL are primarily related to lens siz-ing and maintaining appropriate fluid flow across the iris plane.Current methods of mechanically measuring the width of thecornea horizontally, either with calipers or photographic testingdevices, result in appropriate vault most, but not all, the time.Ultrasound devices are not as easy to use, nor as widely avail-able. Improvements in the ease and clarity of imaging the inter-nal anatomy of the eye could further reduce the lowcomplication rate and increase TICL adoption.
The new CentraFlow design with a hole in the center of theoptic maintains appropriate fluid flow, eliminates the risk of
pupillary block, prevents potential inflammation and bleedingassociated with laser iridotomies, and substantially reduces thesurgical complexity, thus facilitating surgeon adoption of theprocedure. Futhermore, from the patient’s perspective, the Cen-traFlowTM eliminates symptoms of glare or double vision fromany iridotomy, either surgical or laser. Currently, the Centra-Flow is only available outside of the US, where it has beenassociated with increasing ICL use.
With optimized lens sizing and the elimination of difficultieswith iridotomies, the TICL is expected to gain in popularity,particularly relative to contact lens wear in young adults,because contact lenses, especially with overnight wear, have asignificant lifetime risk of corneal warpage, hypoxia, scarring,and infections [68–70]. Furthermore, toric contact lenses have thedisadvantage of moving up and down with each blink, andmore importantly of rotating with each blink, causing the astig-matism correction to rotate out of focus [5]. Many doctors donot even try to correct astigmatism with soft contact lensesbecause of this. Outside the US, contact lens use has notreached the same penetration level as in the US, because itrequires access to sanitary conditions for hand washing andcare of the lenses [71]. As a rule, if the tap water is not safe todrink, it is not safe to use for hand washing before inserting acontact lens.
Some expect that as people become accustomed to highquality optics from a lens implant like the TICL, they will bemore likely to choose a refractive lens exchange with removalof the ICL/TICL when they naturally lose their accommodativeability in their 50s and 60s. Interestingly, many surgeonsremark that patients who have had LASIK with good visualresults are more critical of decreased vision from cataracts anddo not delay cataract surgery as long as those who have neverhad eye surgery.
Advantages of using an ICL or TICL in young adults arethat it does not pose wound construction issues during latercataract surgery (as a rigid phakic IOL does), and it does notcomplicate IOL power calculations (as laser refractive surgerydoes). It may become more common to have phakic lensesimplanted while in the mid-twenties to correct refractive errorsand then have them replaced with a multifocal or accommoda-tive IOL when one reaches the 50- to 60-year age range.
Because of increasing regulatory burdens and increasing costsin hospitals and ambulatory surgery centers, lens implant sur-gery may become an in-office procedure performed by highlyskilled surgeons. This has already happened with some plasticsurgery procedures, and laser refractive surgery is typically anin-office procedure.
Information resourcesThe following website summarizes problems with higher pow-ered spectacles: [72].
Financial & competing interests disclosure
MO Price is a consultant to Staar Surgical and owns stock options in
Staar Surgical. FW Price Jr is a consultant to Staar Surgical and
Device Profile Price & Price Jr
36 Expert Rev. Med. Devices 12(1), (2015)
Exp
ert R
evie
w o
f M
edic
al D
evic
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
02/
01/1
5Fo
r pe
rson
al u
se o
nly.

Ophtec. He owns stock options in Staar Surgical and has received pay-
ment for lectures including services on speakers bureaus from Alcon and
Bausch & Lomb. The authors have no other relevant affiliations or
financial involvement with any organization or entity with a financial
interest in or financial conflict with the subject matter or materials dis-
cussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this
manuscript.
Key issues
• Low to moderate myopic astigmatism can be corrected with spectacles, contact lenses, or laser refractive surgery. The visual quality
provided by these options declines with higher levels of correction. Placing the corrective lens closer to the nodal point of the eye (just
behind the crystalline lens) decreases the aberrations induced by the corrective lens.
• Toric phakic intraocular lenses provide predictable and stable visual correction over a wide range of myopia and astigmatism and
address an important need by allowing people with higher levels of myopic astigmatism to participate in normal activities not previously
accessible because of visual limitations.
• Posterior chamber and iris-supported toric phakic intraocular lens models (manufactured by Staar Surgical and Ophtec, respectively) are
approved for use outside the US and have reasonably long track records. No toric phakic intraocular lenses are approved in the US.
• The toric implantable collamer lens is a posterior chamber lens that is implanted through a small incision using a technique that is
comparatively easy to master. Reported complication rates are low, with the most common being improper lens sizing and vault (treated
by exchanging the lens), cataract formation (if visually significant, treated by lens removal and cataract extraction), and axis misalign-
ment or lens rotation (treated by repositioning the lens).
• The addition of a small central hole in the toric implantable collamer lens has enhanced the safety profile by obviating the need for an
iridotomy or iridectomy and eliminating concerns about pupillary block or glare from holes in the iris. Studies show the small central
hole does not affect the optical quality of the lens.
References
1. Vitale S, Sperduto RD, Ferris FL 3rd.
Increased prevalence of myopia in the
United States between 1971-1972 and
1999-2004. Arch Ophthalmol 2009;
127(12):1632-9
2. Quek TP, Chua CG, Chong CS, et al.
Prevalence of refractive errors in teenage
high school students in Singapore.
Ophthalmic Physiol Opt 2004;24(1):47-55
3. Young G, Sulley A, Hunt C. Prevalence of
astigmatism in relation to soft contact lens
fitting. Eye Contact Lens 2011;37(1):20-5
4. Stevens JD. Astigmatic excimer laser
treatment: theoretical effects of axis
misalignment. Eur J Implant Refract Surg
1994;6:310-18
5. Edrington TB. A literature review: the
impact of rotational stabilization methods
on toric soft contact lens performance. Cont
Lens Anterior Eye 2011;34(3):104-10
6. Condon PI. 2005 ESCRS Ridley Medal
Lecture: will keratectasia be a major
complication for LASIK in the long term? J
Cataract Refract Surg 2006;32(12):2124-32
7. Nagy ZZ. New technology update:
femtosecond laser in cataract surgery. Clin
Ophthalmol 2014;18:8:1157-67
8. Guell JL, Morral M, Kook D, et al. Phakic
intraocular lenses Part 1: historical overview,
current models, selection criteria, and
surgical techniques. J Cataract Refract Surg
2010;36(11):1976-93
9. Kohnen T, Kook D, Morral M, et al.
Phakic intraocular lenses Part 2: results and
complications. J Cataract Refract Surg 2010;
36(12):2168-94
10. Schallhorn S, Tanzer D, Sanders DR, et al.
Randomized prospective comparison of
visian toric implantable collamer lens and
conventional photorefractive keratectomy for
moderate to high myopic astigmatism. J
Refract Surg 2007;23(9):853-67
11. Schallhorn S, Tanzer D, Sanders DR, et al.
Night driving simulation in a randomized
prospective comparison of Visian toric
implantable collamer lens and conventional
PRK for moderate to high myopic
astigmatism. J Refract Surg 2010;26(5):
321-6
12. Sanders DR, Schneider D, Martin R, et al.
Toric Implantable Collamer Lens for
moderate to high myopic astigmatism.
Ophthalmology 2007;114(1):54-61
13. Kamiya K, Shimizu K, Kobashi H, et al.
Three-year follow-up of posterior chamber
toric phakic intraocular lens implantation
for moderate to high myopic astigmatism.
PLoS One 2013;8(2):e56453
14. Sari ES, Pinero DP, Kubaloglu A, et al.
Toric implantable collamer lens for
moderate to high myopic astigmatism:
3-year follow-up. Graefes Arch Clin Exp
Ophthalmol 2013;251(5):1413-22
15. Hasegawa A, Kojima T, Isogai N, et al.
Astigmatism correction: laser in situ
keratomileusis versus posterior chamber
collagen copolymer toric phakic intraocular
lens implantation. J Cataract Refract Surg
2012;38(4):574-81
16. Pothireddy R, Reddy KP, Senthil S, et al.
Posterior chamber toric phakic intraocular
lenses for myopic astigmatism: first
experience in India. J Cataract Refract Surg
2012;38(9):1583-9
17. Alfonso JF, Lisa C, Fernandez-Vega Cueto L,
et al. Comparison of visual and refractive
results of Toric Implantable Collamer Lens
with bioptics for myopic astigmatism.
Graefes Arch Clin Exp Ophthalmol 2013;
251(3):967-75
18. Bhikoo R, Rayner S, Gray T. Toric
implantable collamer lens for patients with
moderate to severe myopic astigmatism:
12-month follow-up. Clin Experiment
Ophthalmol 2010;38(5):467-74
19. Alfonso JF, Fernandez-Vega L, Fernandes P,
et al. Collagen copolymer toric posterior
chamber phakic intraocular lens for myopic
astigmatism: one-year follow-up. J Cataract
Refract Surg 2010;36(4):568-76
20. Mertens EL, Sanders DR, Vitale PN.
Custom-designed toric phakic intraocular
Evaluation of the TICL for simultaneous treatment of myopia & astigmatism Device Profile
informahealthcare.com 37
Exp
ert R
evie
w o
f M
edic
al D
evic
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
02/
01/1
5Fo
r pe
rson
al u
se o
nly.

lenses to correct high corneal astigmatism. J
Refract Surg 2008;24(5):501-6
21. Alfonso JF, Lisa C, Alfonso-Bartolozzi B,
et al. Collagen copolymer toric phakic
intraocular lens for myopic astigmatism:
one-year follow-up. J Cataract Refract Surg
2014;40(7):1155-62
22. Choi SH, Lee MO, Chung ES, et al.
Comparison of the toric implantable
collamer lens and bioptics for myopic
astigmatism. J Refract Surg 2011;27(2):91-7
23. Alfonso JF, Baamonde B, Madrid-Costa D,
et al. Collagen copolymer toric posterior
chamber phakic intraocular lenses to correct
high myopic astigmatism. J Cataract Refract
Surg 2010;36(8):1349-57
24. Sheng XL, Rong WN, Jia Q, et al.
Outcomes and possible risk factors
associated with axis alignment and rotational
stability after implantation of the Toric
implantable collamer lens for high myopic
astigmatism. Int J Ophthalmol 2012;5(4):
459-65
25. Park SC, Kwun YK, Chung ES, et al.
Postoperative astigmatism and axis stability
after implantation of the STAAR Toric
Implantable Collamer Lens. J Refract Surg
2009;25(5):403-9
26. Elies D, Alonso T, Puig J, et al. Visian toric
implantable collamer lens for correction of
compound myopic astigmatism. J Refract
Surg 2010;26(4):251-8
27. Chang J, Lau S. Toric Implantable
Collamer Lens for high myopic astigmatic
Asian eyes. Ophthalmology 2009;116(12):
2340-7
28. Liu TX, Luo X. Stability of axis and patient
satisfaction after toric implantable collamer
lens implantation for myopic astigmatism.
Pak J Med Sci 2013;29(6):1371-4
29. Lee SY, Kwon HJ, Ahn HS, et al.
Comparison of patient outcomes after
implantation of Visian toric implantable
collamer lens and iris-fixated toric phakic
intraocular lens. Eye 2011;25(11):1409-17
30. Kamiya K, Shimizu K, Igarashi A, et al.
Comparison of collamer toric implantable
contact lens implantation and
wavefront-guided laser in situ keratomileusis
for high myopic astigmatism. J Cataract
Refract Surg 2008;34(10):1687-93
31. Hashem AN, El Danasoury AM,
Anwar HM. Axis alignment and rotational
stability after implantation of the toric
implantable collamer lens for myopic
astigmatism. J Refract Surg 2009;25(10):
S939-43
32. Kamiya K, Shimizu K, Aizawa D, et al.
One-year follow-up of posterior chamber
toric phakic intraocular lens implantation
for moderate to high myopic astigmatism.
Ophthalmology 2010;117(12):2287-94
33. Alfonso JF, Fernandez-Vega L, Lisa C, et al.
Collagen copolymer toric posterior chamber
phakic intraocular lens in eyes with
keratoconus. J Cataract Refract Surg 2010;
36(6):906-16
34. Hashemian SJ, Soleimani M, Foroutan A,
et al. Toric implantable collamer lens for
high myopic astigmatism in keratoconic
patients after six months. Clin Exp Optom
2013;96(2):225-32
35. Kamiya K, Shimizu K, Kobashi H, et al.
Clinical outcomes of posterior chamber
toric phakic intraocular lens implantation
for the correction of high myopic
astigmatism in eyes with keratoconus:
6-month follow-up. Graefes Arch Clin Exp
Ophthalmol 2011;249(7):1073-80
36. Camoriano GD, Aman-Ullah M,
Purba MK, et al. Toric collagen copolymer
phakic intraocular lens to correct myopic
astigmatism in eyes with pellucid marginal
degeneration. J Cataract Refract Surg 2012;
38(2):256-61
37. Shaheen MS, El-Kateb M,
El-Samadouny MA, et al. Evaluation of a
toric implantable collamer lens after corneal
collagen crosslinking in treatment of
early-stage keratoconus: 3-year follow-up.
Cornea 2014;33(5):475-80
38. Dirani A, Fadlallah A, Khoueir Z, et al.
Visian toric ICL implantation after
intracorneal ring segments implantation and
corneal collagen crosslinking in keratoconus.
Eur J Ophthalmol 2014;24(3):338-44
39. Fadlallah A, Dirani A, El Rami H, et al.
Safety and visual outcome of Visian toric
ICL implantation after corneal collagen
cross-linking in keratoconus. J Refract Surg
2013;29(2):84-9
40. Jarade E, Dirani A, Fadlallah A, et al.
Visian toric ICL implantation for residual
refractive errors after ICRS implantation
and corneal collage cross-linking in
keratoconus. J Refract Surg 2013;29(7):444
41. Kojima T, Horai R, Hara S, et al.
Correction of residual refractive error in
pseudophakic eyes with the use of a
secondary piggyback toric Implantable
Collamer Lens. J Refract Surg 2010;26(10):
766-9
42. Iovieno A, Guglielmetti S, Capuano V,
et al. Correction of postkeratoplasty
ametropia in keratoconus patients using a
toric implantable Collamer lens. Eur J
Ophthalmol 2013;23(3):361-7
43. Alfonso JF, Lisa C, Abdelhamid A, et al.
Posterior chamber phakic intraocular lenses
after penetrating keratoplasty. J Cataract
Refract Surg 2009;35(7):1166-73
44. Huang D, Schalhorn SC, Sugar A, et al.
Phakic intraocular lens implantation for the
correction of myopia: a report by the
American Academy of Ophthalmology.
Ophthalmology 2009;116(11):2244-58
45. Espandar L, Meyer J. Keratoconus: overview
and update on treatment. Middle East Afr J
Ophthalmol 2010;17(1):15-20
46. Kummelil MK, Hemamalini MS, Bhagali R,
et al. Toric implantable collamer lens for
keratoconus. Indian J Ophthalmol 2013;
61(8):456-60
47. Gomez-Bastar A, Jaimes M,
Graue-Hernandez EO, et al. Long-term
refractive outcomes of posterior chamber
phakic (spheric and toric implantable
collamer lens) intraocular lens implantation.
Int Ophthalmol 2014;34(3):583-90
48. Gonzalez-Lopez F, Bilbao-Calabuig R,
Mompean B, et al. Intraocular pressure
during the early postoperative period after
100 consecutive implantations of posterior
chamber phakic intraocular lenses with a
central hole. J Cataract Refract Surg 2013;
39(12):1859-63
49. Bamashmus MA, Al-Arabi AH, Alawad MA.
Visual outcomes and patient satisfaction after
implantable collamer lens and Toric
implantable collamer lens correction for
moderate to high myopia and myopic
astigmatism. Saudi Med J 2013;34(9):
913-19
50. Lin H, Yan P, Yu K, et al. Anterior
segment variations after posterior chamber
phakic intraocular lens implantation in
myopic eyes. J Cataract Refract Surg 2013;
39(5):730-8
51. Shimizu K, Kamiya K, Igarashi A, et al.
Early clinical out-comes of implantation of
posterior chamber phakic intraocular lens
with a central hole (Hole ICL) for moderate
to high myopia. Br J Ophthalmol 2012;
96(3):409-12
52. Product information on the Visian toric
implantable collamer lens. Available from:
http://staar.com/products/visian-toric-icl/
53. Shimizu K, Kamiya K, Igarashi A, et al.
Intraindividual comparison of visual
performance after posterior chamber phakic
intraocular lens with and without a central
hole implantation for moderate to high
myopia. Am J Ophthalmol 2012;154(3):
486-94
54. Perez-Vives C, Ferrer-Blasco T,
Madrid-Costa D, et al. Visual quality
Device Profile Price & Price Jr
38 Expert Rev. Med. Devices 12(1), (2015)
Exp
ert R
evie
w o
f M
edic
al D
evic
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
02/
01/1
5Fo
r pe
rson
al u
se o
nly.

comparison of conventional and hole-Visian
implantable collamer lens at different
degrees of decentering. Br J Ophthalmol
2014;98(1):59-64
55. Lindland A, Heger H, Kugelberg M, et al.
Changes in vaulting of myopic and toric
implantable collamer lenses in different
lighting conditions. Acta Ophthalmol 2012;
90(8):788-91
56. Lindland A, Heger H, Kugelberg M, et al.
Vaulting of myopic and toric Implantable
Collamer Lenses during accommodation
measured with Visante optical coherence
tomography. Ophthalmology 2010;117(6):
1245-50
57. Choi KH, Chung SE, Chung TY, et al.
Ultrasound biomicroscopy for determining
Visian implantable contact lens length in
phakic IOL implantation. J Refract Surg
2007;23(4):362-7
58. Dougherty PJ, Rivera RP, Schneider D,
et al. Improving accuracy of phakic
intraocular lens sizing using high-frequency
ultrasound biomicroscopy. J Cataract
Refract Surg 2011;37(1):13-18
59. Sanders DR, Doney K, Poco M. ICL in
Treatment of Myopia Study Group. United
States Food and Drug Administration
clinical trial of the implantable collamer lens
(ICL) for moderate to high myopia:
three-year follow-up. Ophthalmology 2004;
111(9):1683-92
60. Alfonso JF, Baamonde B, Fernandez-Vega L,
et al. Posterior chamber collagen copolymer
phakic intraocular lenses to correct myopia:
five-year follow-up. J Cataract Refract Surg
2011;37(5):873-80
61. Igarashi A, Shimizu K, Kamiya K.
Eight-year follow-up of posterior chamber
phakic intraocular lens implantation for
moderate to high myopia. Am J
Ophthalmol 2014;157(3):532-9
62. Transcript of the Ophthalmic Devices Panel
Meeting held on March 14, 2014. Available
from: www.fda.gov/downloads/
AdvisoryCommittees/
CommitteesMeetingMaterials/
MedicalDevices/
MedicalDevicesAdvisoryCommittee/
OphthalmicDevicesPanel/UCM392476.pdf
[Last accessed on 17 June 2014]
63. Park HY, Lee NY, Park CK, et al.
Long-term changes in endothelial cell
counts after early phacoemulsification versus
peripheral iridotomy using sequential argon:
YAG laser technique in acute primary angle
closure. Graefes Arch Clin Exp Ophthalmol
2012;250(11):1673-80
64. Lim LS, Ho CL, Ang LP, et al. Inferior
corneal decompensation following laser
peripheral iridotomy in the superior iris.
Am J Ophthalmol 2006;142(1):166-8
65. Zaldivar R, Davidorf JM, Oscherow S,
et al. Combined posterior chamber phakic
intraocular lens and laser in situ
keratomileusis: bioptics for extreme myopia.
J Refract Surg 1999;15(3):299-308
66. Perez-Vives C, Domınguez-Vicent A,
Madrid-Costa D, et al. Myopic astigmatism
correction: comparison of a Toric
Implantable Collamer Lens and a bioptics
technique by an adaptive optics visual
simulator. Ophthalmic Physiol Opt 2013;
33(2):114-22
67. Doors M, Budo CJ, Chirstiaans BJ, et al.
Artiflex toric foldable intraocular lens:
short-term results of a prospective European
multicenter study. Am J Ophthalmol 2012;
154(4):730-9
68. Robertson DM, Cavanagh HD. The clinical
and cellular basis of contact lens-related
corneal infections: a review. Clin
Ophthalmol 2008;2(4):907-17
69. Fonn D, Simpson T, Woods J, et al. New
technologies to assess lens-mediated effects
of the cornea. Eye Contact Lens 2007;
33(6 Pt 2):364-70
70. Robertson DM. The effects of silicone
hydrogel lens wear on the corneal
epithelium and risk for microbial keratitis.
Eye Contact Lens 2013;39(1):67-72
71. McMonnies CW. Hand hygiene prior to
contact lens handling is problematical. Cont
Lens Anterior Eye 2012;35(2):65-70
72. High-Powered Lenses and Thickness.
Available from: www.opticampus.com/
cecourse.php?url=high_powered/
73. STAAR� Surgical Visian Toric Implantable
Collamer� Lens PMA Supplement
P030016. Available from: www.fda.gov/
downloads/AdvisoryCommittees/
CommitteesMeetingMaterials/Medical
Devices/MedicalDevicesAdvisoryCommittee/
OphthalmicDevicesPanel/UCM389743.pdf
[Last accessed on 17 June 2014]
Evaluation of the TICL for simultaneous treatment of myopia & astigmatism Device Profile
informahealthcare.com 39
Exp
ert R
evie
w o
f M
edic
al D
evic
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
02/
01/1
5Fo
r pe
rson
al u
se o
nly.

本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具