-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
1/25
1 | K e n n e t h D . E s p i n o
Evaluation Of The Infant
or Child with
Congenital Heart Disease
Maria Dolores B. Victor, MD., FPCC
HISTORY & PHYSICAL EXAMINATION
COMPREHENSIVE HISTORY
Perinatal Period
Infancy
Older Child
Selected Aspects of History Taking:
Gestational and Natal History
Infections, medications, excessive smoking or alcoholintake
during pregnancy
Birth weight
Postnatal (or Past ) History
Weight gain, development, and feeding pattern
Cyanosis, cyanotic spells, and squatting
Tachypnea, dyspnea, puffy eyelids
Frequency of respiratory infection
Exercise intolerance
Selected Aspects of History Taking:
Postnatal HistoryHeart murmurChest painJoint symptomsNeurologic
symptomsMedications
Family HistoryHereditary diseasesCHDRheumatic feverSudden
unexpected deathDM, HPN, arteriosclerotic heart disease
HISTORY & PHYSICAL EXAMINATION
CLINICAL PRESENTATIONa. Cyanosis
b. Heart Failure
-feeding difficulties
-poor growth
-exercise intolerance
-respiratory distress
c. Chest Pain
d. Extracardiac Congenital Malformation
e. Early Coronary Disease
Physical Examination:
Inspection:
General Appearance and nutritional state
-is the child in distress, well nourished or
undernourished
Chromosomal Abnormalities
-obvious chromosomal abnormalities known to
be associated with certain CHD should benoted
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
2/25
2 | K e n n e t h D . E s p i n o
Physical Examination:
Color
- cyanotic, pale, or jaundiced
- arterial saturation is usually 85 % or lowerbefore cyanosis is
detectable
- Central cyanosis
- peripheral cyanosis
- differential cyanosis manifested by bluelower extremities and
pink upper
extremities
Physical Examination:
Clubbing
-long-standing desaturation usually longerthan 6 months
- appears earliest and most noticeably in
the thumb
Respiratory rate, dyspnea, retraction
-tachypnea, along with tacchycardia is theearliest sign of
left-sided heart failure
Physical ExaminationPalpation:
Peripheral pulses
- pulse rate and note any irregularities
- the right and left arm and an arm and aleg should be
compared.
Weak leg pulses and strong arm pulsessuggests COA
Bounding pulses are seen PDA, AR
Weak pulses are found in cardiac failure
or circulatory shock
Physical Examination
Chest
-Apical impulse
-Hyperactive precordium
-Substernal thrust: RV enlargement
-Apical heave:lv hypertrophy
-Thrills: palpable equivalent of murmurs
Physical Examination
BP measurement
- The width of cuff should be 40 50% of the
circumference of the arm- Cuffs that are too narrow overestimate
the
true BP, cuffs that are too wide underestimate the true
pressure
- The pressure in the leg is about 10 mmhghigher than in the
arms
AUSCULTATION
Heart Sounds
S2- physiologic split vs widely split
S1 S3
S2 S4
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
3/25
3 | K e n n e t h D . E s p i n o
Ejection Clicks
Murmurs- described as to:
a. Intensity Grades I-VI (systolic)
Grades I-IV (diastolic)
b. Timing- Pansystolic
Diastolic
Continuous
c. Location
d. Radiation
e. Pitch
Friction Rubs
AUSCULTATION CLINICAL PRESENTATION
CYANOSIS
MURMUR
HEART FAILURE
LABORATORY EVALUATION
Hematologic tests
Arterial Blood Gas/ Pulse Oximetry
Chest Roentgenogram
Electrocardiography
Echocardiography
Stress testing
Cardiac Cath and Angiography
LABORATORY EXAMINATION
I. HEMATOLOGIC DATA
Hematocrit anemia
Polycythemia (HCT >65 vol%)
Blood culture
Serum electrolytes
Acute Phase Reactants
ASO titer
Arterial Blood Gases
LABORATORY EXAMINATION
Il. RADIOLOGIC ASSESSMENT
Chest Roentgenogram
Postero-AnteriorLateral
Cardiac size and shape and location of apex
Pulmonary vascular markings
Associated lung and thoracic anomalies
views
LABORATORY EXAMINATION
CXR:
1. Boot-shaped heart tetralogy of fallot
2. Egg-shaped heart transposition ofgreat arteries
3. Snowman sign total anomalouspulmonary venous return
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
4/25
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
5/25
5 | K e n n e t h D . E s p i n o
CONGENITAL HEART
DISEASE
EPIDEMIOLOGY & GENETIC BASIS
Prevalence: 0.5-0.8% of live births
2-3/1000 neonates : symptomatic withheart diseases in 1st year
of life
Diagnosis established in:
40-50% by 1 week old
50-60% by 1 month old
Relative Frequency of Major CHDs
LESIONS % OF ALL
LESIONS
VSD 25-30
ASD 2, PDA 6-8
Coarctation of Aorta, PS
Tetralogy of Fallot
d-Transposition of Great Arteries
5-7
3-5
Aortic Stenosis 4-7
TAPVR, Tricuspid Atresia,
Single Ventricle, Double Outlet RV
1-2
ETIOLOGYUNKNOWN in most CHDs
Multifactorial (genetic & environmental)
Chromosomal abnormalities
Trisomy 21, 13 & 18
Turner Syndrome
2-4% - associated with knownenvironmental or adverse
maternalconditions and teratogenic influences
Etiology:
The cause of most CHD is unknown
Genetic factors- Marfans,Noonans,conotruncal defects
(TOF,DORV,TA,PVA)
Chrosomal abnormality- trisomy 18( 90%),trisomy 21 ( 50 % )
Environmental or adverse maternalconditions- DM, SLE, congenital
rubella
Drugs- lithium, thalidomide,ethanol
Gender differences
GENETIC COUNSELLING
Probability of cardiac malformationoccurring in subsequent
children
A child with CHD ? 2-6% incidence ofCHD for a 2nd pregnancy
2 First-degree relatives with CHD, risk fora subsequent child
may reach 20-30%;CHD similar to 1st child
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
6/25
6 | K e n n e t h D . E s p i n o
Fetal circulation
Differs from adult circulation in severalways:
1.In adults, gas exchange occurs in thelungs.
In the fetus, the placenta provides theexchange of gases and
nutrients
2.Parallel circulation
3.3 unique features: ductus venosus,foramen ovale, ductus
arteriosus
Changes in Circulation after Birth1. Interruption of the
umbilical cords results in:
a) An increase in systemic vascular resistance
b) Closure of ductus venosus
2. Lung expansion results in:
a) Reduction of pulmonary vascular resistanceincrease in
pulmonary blood flow, fall in PA
pressure
b) Functional closure in foramen ovale-closed by the 3rd mo of
life
c) Closure of Patent Ductus Arteriosus
II. Chest Radiograph Findings
Pulmonary vascular markings or
pulmonary blood flow
a. Increased
b. Normal
c. Decreased
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
7/25
7 | K e n n e t h D . E s p i n o
SYSTEMATIC APPROACH
III. Electrocardiogram
a. Right Ventricular
b. Left Ventricular
c. Biventricular
IV. Echocardiography
Hypertrophy
ACYANOTIC CONGENITAL HEARTLESIONS
A. Lesions Resulting in IncreasedVolume Load
B. Lesions Resulting in IncreasedPressure Work
A. LESIONS RESULTING IN INCREASED VOLUME LOAD
1. LEFT-to-RIGHT SHUNTING
ASD
VSD
AVSD
PDA
A. LESIONS RESULTING IN INCREASED VOLUME LOAD
PATHOPHYSIOLOGY
Communication between the systemic or
pulmonary side of circulation? shunting
of fully oxygenated blood back into the
lungs.
A. LESIONS RESULTING IN INCREASED VOLUME LOAD
Direction and magnitude of shunt across the
communication depend on:
a. Size of defect
b. Relative systemic and pulmonarypressure and vascular
resistance
A. LESIONS RESULTING IN INCREASED VOLUME LOAD
COMPLICATIONS
a. Heart Failure
b. Infective Endocarditis
c. Eisenmenger Syndrome
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
8/25
8 | K e n n e t h D . E s p i n o
Ventricular Septal Defect
Prevalence: most common form of CHD and accounts for 25% of
alldefects.
Pathology:
A VSD may be classified into 4:
1. Perimembranous- most common
2. Outlet defects- accoutn for 5-7%; also called supracristal,
conal,
subpulmonary or subarterial
3. Inlet defects- account for 5-8%
4. Trabecular defects-accoutn for 5-20%; may be central,
apical,margin
VSD
Clinical manifestations:
History:
1.with small VSD, the patient is asymptomatic
2.Moderate to large VSD, delayed growth and
development, decreased exercise tolerance,repeated pulmonary
infections, and CHF arerelatively common
3.With history of cyanosis and decreased level ofactivity may be
present
VSDPhysical Examination:
1. Infants with small VSDs are well developed.
2. Infants and children with large VSDs may havepoor weight gain
or show signs of CHF
3. A sytolic thrill may be present Precordial andhyperactivity
are present with arge VSD.
4. murmur: regurgitant or pansystolic at LLSB
VSDLaboratory Diagnosis
Electrocardiogram
1.With small VSD, the ECG is normal
2.With moderate VSD, LVH and occasionalLAH may seen
3.With large VSD, the ECG shows combinedventricular
hypertrophy
VSD
X-ray studies:
Small VSD: normal
Moderate-large VSD:
1. Cardiomegaly of varying degrees andinvolves LV and RV.
2. Pulmonary vascular marking !nereas
VSD
Natural History:
1. Spontaneous closure occurs in 30-50% of pxs withmembranous
and muscular VSDs during first 2 years of life.
2. CHF in infants with large VSD, but usually not until 6-8
weeksof age
3. PVOD may begin to develop as early as 6-12 mos of age inpxs
with large VSDs.
4. Infundibular stenosis may develop in some infants with
largedefects
5. Aortic insufficiency may develop in pxs with supracristal
VSD
6. Infective endocarditis rarely occurs
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
9/25
9 | K e n n e t h D . E s p i n o
VSD
Management:
1.Medical
-Treatment of CHF, if it develops, with digoxin and
diuretics
-No .Exercise restriction is required in the absence ofpulmonary
hypertension
-Maintenance of .Blood oral hygiene and antibiotic
prophylaxis against infective
Endocarditis
VSD
Management:
2. surgical
If growth cannot be improved, the VSDshould be operated on
within the first 6months of life
Surgery is NOT indicated for small VSD
Atrial Septal Defect
Prevalence: occurs as an isolated anomaly in 6-8% more common
infemales
Pathology:
1. Three types exist- secundum defect, primum defect, sinus
venosus
defect. A PFO does not ordinarily produce shunting and is
notconsidered an ASD.
2. Ostium secundum is the most common accounting for 50-70 % of
allasds . the delefect located at site of fossa ovalis allowing
left-to-riflhtshunting of blood from left atrium to right atrium.
Anomalouspulmonary venous return is present in 10% of cases.
ASD
3. ostium secundum defects occur in about30% of all ASDs,
including those thatoccur as part of AVSD. Isolated ostium
primum ASD occurs in 15% of all ASDs
4. Sinus Venosus Defect-occurs in about10.5 of all ASDs, most
commonly loactedat the entry of superior vena cava into RA.
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
10/25
10 | K e n n e t h D . E s p i n o
ASD
Clinical Manifestations:
History: Infants and asymptomatic; subtle failure may be present
inyounger children; in older children varying degrees of
exerciseintolerance.
PE:
1. Relatively slender body built is typical
2. A widely split and fixed S2
3. A grade 2-3/6 systolic ejection murmur at LUSB secondary to
relativePS
*no murmur, only if blood pass to pulmonic valve.
ASD
Laboratory Diagnosis:
A. X-ray studies
1. Cardiomegaly with enlargement of the RA and RV
2.A prominent pulmonary artery segment and increasedpulmonary
vascular markings
B. Electrocardiogram
Right axis deviation and mild right ventricular hypertrophyor
right bundle branch block
ASDC. Echocardiography
- Diagnostic
- Indirect signs of left to right shunt RVenlargement and RA
enlargement, dilatedPA, paradoxical motion
ofinterventricutarseptum
D. Cardiac catheterization
ASDNatural History:
1. Spontaneous closure in about 40 % in the first 4 years of
life
2. Most children remain active and asymptomatic.
3. If a large defect is untreated.CHF and pulmonary
hypertension develop in their 20s and 30s
4. With or without surgery, atrial arrhythmias may occur
5. Infective endocarditis does not occur in isolated ASDs.
ASD
Treatment:
1. Non-surgical closure
Devices that can be delivered through cardiaccatheterization
2. Surgical closure -indications: QpQs of > 1.5:1
-age: 3 to 4 years of age
-procedure: open heart surgery
-mortality: < 1%
-complications: CVA, arrhythmias
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
11/25
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
12/25
12 | K e n n e t h D . E s p i n o
1
3
2
4
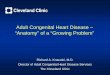
1. Atrial septal defect, primum type.
2. Inlet (type III) ventricular septal defect.
3. Cleft and deformity of tricuspid valve.
4. Cleft and deformity of mitral valve.
Complete Atrio-Ventricular Canal DefectA. LESIONS RESULTING IN
INCREASED VOLUME LOAD
2. REGURGITANT LESIONS
Mitral Regurgitation
Ebstein Anomaly
Pulmonary Regurgitation
Aortic Regurgitation
VSD
2 days old
6 months old
7 years old
1
2
Ebstein's Anomaly of the Tricuspid Valve from birth to 7 years
of age
A. LESIONS RESULTING IN INCREASED VOLUME LOAD
3. CARDIOMYOPATHIES
Viral
Metabolic
Genetic Defects
B. LESIONS RESULTING IN INCREASED PRESSURE
WORK
PATHOPHYSIOLOGY:
Obstruction to normal blood flow
1. Obstruction to Ventricular Outflow
Valvular PS
Valvular AS
Coarctation of Aorta
Pulmonary Stenosis
Prevalence:
Pathology
1. PS may be valvular, subvalvular (infundibular )
supravalvular
2. In valvular PS the valve is thickened, with fused orabsent
commissures.
3. Dysplastic valves are frequently seen with Noonanssyndrome
isolated infundibular PS is rare, usually seen
in TOF
4. Supravalvular PS is occasionally seen with rubellaWilliams
syndrome
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
13/25
13 | K e n n e t h D . E s p i n o
PS
History:
1. Children with mild PS are completelyasymptomatic. Exertional
dyspnea andeasy fatigability may be present in pts with
moderately severe cases.
2. Newborns with critical PS feed poorly, aretachypneic, and may
be cyanotic
PSPhysical Examination:
1. Most patients are acyanotic and well developed.Newborns with
critical PS are cyanotic and techypneic.
2. A right ventricular tap and systolic thrill may be
present
3. A systolic ejection click is present with valvular PS. TheS2
may split widely, and the P2 may be diminishintensity. An
ejection-type systolic murmur is best
audible at ULSB. The louder and longer the murmur, themore
severe the stenosis is.
PSECG:
1. Normal in mild cases
2. Right axis deviation and RVH are present Inmoderate. The
degree of RVH on ECGcorrelates with severity of PS
3. Right atrial hypertrophy and RVH with strainmay be seen with
severe PS
4. Neonates with critical PS may show LVHbecause of a
hypoplastic RV
PSStudies:
1. Heart size is usually normal, but the main PAsegment is
prominent
2. Pulmonary vascular markings are usuallynormal but may
decrease with severe PS.
3. In neonates with critical PS, lung fields areoligemic with
varying degree of cardiomegaly.
Echocardiography
PS
Treatment
A. Medical:
1. Restriction of activity not necessary except incases of
severe PS
2. Antibiotic prophylaxis against SBE
3. Balloon valvuloplasty is the procedure of choice
4. Newborns with critical PS: prostaglandin infusion;balloon
valvuloplasty
PS
B. Surgical:
1. Children with valvular PS in whom balloonvalvuloplasty is
unsuccessful.
2. Other types of obstruction (infundibular,
anomalous RV muscle) with significant pressuregradient also
require surgery
3. If balloon valvuloplasty is unsuccessful orunavailable,
infants with critical PS requiresurgery on an urgent basis
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
14/25
14 | K e n n e t h D . E s p i n o
Aortic Stenosis
Prevalence: accounts for 5%; M > F
Pathology:
1.Stenosis may be valvular, subvalvular. supravalvular
2. Valvular AS may be caused by bicuspid AV, unicuspidAV, or
stenosis of tricuspid AV. (Bicuspid AV is the most
common form)
3. Supravalvular AS is an annular constriction above AV;often
associated with Williams syndrome
4. Subvalvular, AS may result from simple diaphragm or
from long tunnel-like fibromuscular narrowing of LVoutflow
tract
ASHistory:
1. Most children with mild to moderate AS areasymptomatic.
Occasionally, exerciseintolerance may be present
2. Exertional chest pain, easy fatigability, orsyncope may occur
with severe obstruction
3. Infants with critical AS may develop CHF withinfirst few
weeks to months of life.
ASECG: normal in mild cases. LVH with or without strain
pattern may be present in severe cases.
X-ray studies:
1. Heart size is usually normal, but a dilated ascending
aorta or prominent aortic knob may be seen with valvularAS.
2. Significant cardiomegaly does not develop unles CHF
occurs.
3. Newborns with critical AS show generalized
cardiomegaly with pulmonary venous congestion.
AS
Natural history:
1. Chest pain, syncope, and even sudden death may occurwith
severe AS
2. Heart failure occurs with severe AS during the newborn
period or later in adult life3. A significant increase in PG
frequently occurs with
growth
4. The stenosis may worsen with aging as a result of
calcification
5. SBE occurs in approximately 4%
AS
Management:
Medical:
1. Maintenance of good oral hygiene and antibiotic
prophylaxis2. Children with mod-severe AS should not
perform sustained, strenuous physical activities
3. For critically ill-newboms with CHF, inotropics,diuretics and
prostaglandin should be started
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
15/25
15 | K e n n e t h D . E s p i n o
AS
Balloon valvuloplasty- indicated for childrenwith mod-severe AS,
and in symptomaticneonates
Surgical treatment- reserved for valves thatare not amenable to
balloon therapy
1. Surgical valvotomy
2. Aortic valve replacement
1
1) Valvular Stenosis
with a bicuspid
aortic valve
RV
LA
RA
Severe Aortic Stenosis in an infant
Coarctation of Aorta
Prevalence: occurs in 5-7 % of all lesions; M>F
-May occur at any point; but most common justbelow the origin of
left subclavian artery (98%)
- May be a feature of Turner's(30%)
- Associated with bicuspid AV, mitral valveabnormalities, and
subaortic stenosis (Shonecomplex)
COA
Asymptomatic children:
1.Normal growth and development
2.Arterial pulses in the leg are either absent orweak and
delayed. There is hypertension in thearm
3.A systolic thrill present at parasternal notch,ejection click
is frequently audible whichoriginates from bicuspid AV. A short
systolicmurmur can be heard at URSB and mid or lower
left sternal border
COA
X-ray studies:
-infants with severe COA, marked cardiomegalyand pulmonary edema
are present
-in children, heart size maybe normal or slightlyenlarged,
dilatation of ascending aorta, ribnotching in older children
COA
ECG:
-Normal or rightward QRS axis and RVH in most infantswith severe
COA
-LVH is seen in older children; maybe normal in 20%
ofpatients
Echocardiography:
- Will show the site and extent of COA
- Will demonstrate associated abnormalities like bicuspidAV, MV
abnormalities, PDA
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
16/25
16 | K e n n e t h D . E s p i n o
1. Coarctation of the aorta,
distal to the left
subclavian artery
2. Severe aortic stenosis
1
2
Coarctation of the Aorta with severe aortic stenosis in an
infantB. LESIONS RESULTING IN INCREASED PRESSURE
WORK
2. Obstruction to Ventricular Inflow
Tricuscupid Stenosis
Mitral StenosisCor Triatriatum
B. LESIONS RESULTING IN INCREASED PRESSURE
WORK
COMPLICATIONS
Heart Failure
Total Circulatory Collapse
Cyanosis
Systemic Hypertension
CYANOTIC CONGENITAL HEART LESIONS
Divided according to Pathophysiology:
PULMONARY BLOOD FLOW (PBF)
a. Decreased PBF
b. Increased PBF
A. DECREASED PBF
TOF
Pulmonary Atresia with Intact Ventricular
Septum
Tricuspid Atresia
TAPVC with Obstruction
A. DECREASED PBF
Included in these LESIONS are:
1. Obstruction to PBF
2. Pathway by which VENOUS BLOODcan shunt from R? L and
enter
systemic circulation (PFO, ASD,VSD)
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
17/25
17 | K e n n e t h D . E s p i n o
Tetralogy Of FallotPrevalence: occurs in 5 7 % of all CHD
- Most common cyanotic heart defect seen inchildren beyond
infancy
Pathology:
1. Consists of 4 abnormalities: large VSD,right ventricular
outflow tract obstruction,
RVH, overriding of the aorta.2. The pulmonary annulus and MPA is
often
small.
3. The aortic arch is right-sided in 20 %
TOF
The degree of right ventricular outflowobstruction determines
the timing ofonset of symptoms, the severity ofcyanosis, and the
degree of RVH
When the obstruction is mild, thepatient may not be visibly
cyanotic
( pink TOF )
TOFHistory:1. A heart murmur is usually audible at birth
2. Most patients are symptomatic withcyanosis at birth or
shortly thereafter.Dyspnea on exertion,squatting, or hypoxicspells
develop later, even in mildly cyanoticinfants
3. Infants with acyanotic TOF maybeasymptomatic or may show
signs of CHF
TOFECG: RAD and RVH
CXR: heart size is normal or smaller thannormal, the pulmonary
vascularmarkings are decreased
-a concave MPA segment withupturned apex (boot-shaped or coeuren
sabot)
-RAE and right aortic arch
TOF
Echo: establishes the diagnosis, extentof aortic override,
location and degreeof pulmonary obstruction, size ofproximal branch
pulmonary arteries
Angiography: best demonstrates theanatomy of pulmonary
arteries
TOFNatural History:
1. Infants with acyanotic TOF graduallybecome cyanotic
2. Polycythemia develops
3. Development of relative iron-deficiencystate
4. Hypoxic spells
5. Growth retardation
6. Brain abscess and cerebrovascularaccidents
7. SBE
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
18/25
18 | K e n n e t h D . E s p i n o
Pulmonary Atresia with Intact
Septum- The pulmonary valve is atretic, ventricular
septum is intact
- No egress of blood from the RV
- RA pressures increases and blood shunts viathe foramen ovale
into the LA
- These pts may have sinusoidal channelswithin the RV
- An interatrial communication and PDAare necessary for the pt
to survive
PA with Intact Septum
CM:
-severe cyanosis and tachypnea are seenin distressed infants
-S2 is single, heart murmur is usuallyabsent, but soft murmur of
PDA or TRmaybe audible
-inadequate interatrial communicationcauses hepatomagaly
PA with Intact Septum
ECG: QRS axis 0 90 degrees, RAE,LVH
CXR: heart size maybe normal or large,resulting from RAE.
Pulmonary
vascular markings are decreasedEcho: useful in estimating th
RV
dimensions, size of TV, sinusoidalchannels which are of
prognostic value
PA with Intact Septum
Treatment:
-infusion of Prostaglandin
-aortopulmonary shunt
-radiofrequency ablation catheterfollowed by balloon
valvuloplasty
-Fontan procedure
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
19/25
19 | K e n n e t h D . E s p i n o
Tricuspid Valve AtresiaPrevalence: accounts for 1 2 % of CHD
Pathology:
1. TV is absent, and the RV is hypoplastic.Associated defects
such as ASD, VSD anPDA are necessary for survival
2. TVA is usually classified according to thepresence or absence
of PS and TGA. Thegreat arteries are normally related in about70%
and transposed in 30%
TVACM:
1. Cyanosis usually evident at birth
2. A systolic thrill is rarely whenassociated with PS
3. S2 is single, a ger 2-3/6 regurgitantsystolic murmur of VSD
is noted atLLSB
4. Hepatomegaly may indicate aninadequate interatrial
communicationor CHF
TVAECG: LAD , LVHCXR: heart size maybe normal or slightly
increased. Pulmonary vascularitydecreases in most patients,
although itmay increase with TVA/TGA
Echo: establishes the diagnosis;absence of tricuspid orifice,
small RV,large LV, associated abnormalities
TVATreatment:
- Prostaglandin infusion
- Atrial septostomy
- Aortopulmonary shunt procedure
- Bidirectional Glenn Shunt- Fontan procedure
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
20/25
20 | K e n n e t h D . E s p i n o
A. DECREASED PBF
Degree of cyanosis depend on:
a. Degree of obstruction to PBF:
MILD vs SEVERE
b. When the ductus arteriosus closes
A. DECREASED PBF
COMPLICATIONS
Hypercyanotic, TET, Spells
Shock
Infective Endocarditis
Cerebrovascular accidents
Brain abscess
B. INCREASED PBF
Not associated with obstruction to PBF
Cyanosis caused by either
a. Abnormal ventricular-arterial connectionsb. Total mixing of
systemic venous and
pulmonary venous blood within the heart
ABNORMAL VENTRICULO-ARTERIAL
CONNECTIONS
Transposition of Great Arteries (TGA)
Systemic blood? RA? RV? Aorta? Body
Oxygenated blood? pulmonary veins?LA? LV? pulmonary artery?
lungs
Survival depends on fetal pathways
(PFO, PDA and VSD)
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
21/25
21 | K e n n e t h D . E s p i n o
TGA-Defects that permit mixing of the twocirculations ( ASD/PFO,
VSD, PDA )are necessary for survival.
-Half of patients with tga do not haveassociated defect other
than pfo orsmall pda simple tga
-VSD is present in about half of thesepatients
-The clinical presentation varies inrelation to presence or
absence of
associated defects
TGA with Intact SeptumCM:1. Cyanosis and tachypnea are
always
present
2. Hypoxemia is usually severe
-the condition is a medical emergency; earlydiagnosis and
appropriate treatment canavert the development of hypoxemia
ofsevere hypoxemia and acidosis, which leadto death
TGA with Intact Septum
PE:
1. Moderate to severe cyanosis, in large,male newborns
2. Infant is tachypneic but withoutretractions unless CHF
supervenes
3. S2 is single and loud. Murmurs maybeabsent, or a soft
systolic ejectionmurmur
TGA with Intact Septum
Laboratory Studies:
-severe arterial hypoxemia with or withoutacidosis
-hypoglycemia and hypocalcemia
ECG: RAD, RVHCXR: cardiomegaly with increased
pulmonary vascularity
egg-shaped cardiac silhoutte
Echo: diagnostic
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
22/25
22 | K e n n e t h D . E s p i n o
TGA with Intact SeptumTreatment:
1. Prostaglandin to improveoxygenation
2. Maintain normothermia, correction of
acidosis and hypoglycemia3. Atrial septostomy- performed in
all
patients in whom delay in operation isnecessary
TGA with Intact SeptumArterial switch operation ( Jatene )
- Surgical treatment of choice
- Usually performed within the first 2weeks of life
- Restores the normal physiologicrelationships of systemic
andpulmonary blood flow
- Survival rate is 90 95 %
TOTAL MIXING LESIONS
Common Atrium or Ventricle
Total Abnomalous Pulmonary Venous
Return (TAPVR)
Truncus Arteriosus
Total Anomalous Pulmonary VenousReturn
Prevalence: accounts for 1-2 % of CHD
Pathology:
1. No direct communication exists between
pulmonary veins and the LA2. Defect maybe divided into 4
types:
a. Supracardiac: accounts for 50 %; pulmonaryveins drain into
right SVC via the leftvertical vein and innominate vein
TAPVRb. Cardiac: accounts for 20 %; common
pulmonary vein drains into the coronarysinus or directly into
the RA
c. Infracardiac: common pulmonary vein
into the portal vein, hepatic vein, orIVC; most commonly
associated withobstruction
d. Mixed type
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
23/25
23 | K e n n e t h D . E s p i n o
LV
RV
AO
LA
RPA
VenousConfluence
VenousConfluence
AO
RPA
VerticalVein
VerticalVein
Right
Pulmonary Veins
InnominateVein
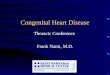
2
Total Anomalous Pulmonary Venous Return to the Innominate
Vein
TAPVR
CM:A.Without pulmonary venous obstruction
1. CHF with growth retardation and frequentrespiratory
infections
2. History of mild cyanosis from birth
3. Precordial bulge with hyperactive RV
4. S2 is widely split and fixed, P2 isaccentuated
5. A gr 2-3/6 systolic ejection murmur atULSB
TAPVRECG: RAE, RVH
CXR:
1. Moderate to marked cardiomegalywith increased pulmonary
vascularmarkings
2. snowman sign or figure of eightmaybe seen in supracardiac
type
Truncus Arteriosus- Single arterial trunk arises from the
heart and supplies the systemic,pulmonary and coronary
circulations
- A VSD is always present and is directlybelow the truncus
- A right aortic arch is present in 30 %
- Di George syndrome present in 33 %
- 4 types
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
24/25
24 | K e n n e t h D . E s p i n o
TA
- Clinical picture varies with age,
depending on level of pulmonary
vascular resistance
- In newborn period: signs of heart failureare usually absent;
minimal cyanosis
- In older infants: pulmonary blood flow isincreased and the
clinical picture isdominated by heart failure
TA
ECG: CVH is present in 70 %
CXR: cardiomegaly with increasedpulmonary vascularity, right
sided archis seen in 30%
Echo: demonstrates a large truncal artery
overriding a large VSD
1
23
Truncus Arteriosus
1. Pulmonary arteries arise from aorta.
2. Truncal valve, occasionally quadracuspid,
stenotic and or insufficient.
Overrides the ventricular septal defect.3. Ventricular septal
defect, large
LV
Truncus
TOTAL MIXING LESIONS
Deoxygenated systemic venous blood andoxygenated blood mix
completely inheart? oxygen saturation equal inpulmonary artery and
aorta
COMPLICATIONS
Cyanosis
Heart failure
OTHER CONGENITAL HEART & VASCULAR
MALFORMATIONS
Anomalies of aortic arch
Anomalous origin of coronary arteries
PULMONARY HYPERTENSION (PH)
1. Primary PH
2. Pulmonary Vascular Disease(Eisenmenger Syndrome)
-
8/14/2019 Evaluation Of The Infant or Child with Congenital
Heart Disease
25/25
*
EISENMENGER SYNDROME
Patients with VSD, blood shunted R? L
2 pulmonary vascular disease
Also seen in patients with ASD, AVSD,
PDA
Present with cyanosis, right heart failure
GENERAL PRINCIPLES OF TREATMENT OF CHD
MILD CHD-
Require NO treatment in most patients,
NO restrictions in physical activity
MODERATE TO SEVERE CHD-
PE modified appropriate to childs physical activitydetermined by
EXERCISE TESTING
Prophylaxis vs Bacterial endocarditis
ex. Dental procedure
Instrumentation of urinary tract
Before lower GI manipulation
GENERAL PRINCIPLES OF TREATMENT OF CHD
MONITOR CYANOTIC PATIENTS
Iron deficiency anemia/ polycythemia
Dehydration avoided
High altitudes and sudden change in thermal
environment be avoided
PHLEBOTOMY IN SYMPTOMATIC PATIENT WITH
POLYCYTHEMIA (Hct >65%)
COUNSEL WOMEN ON RISKS ASSOCIATED WITH
CHILDBEARING
PAROXYSMAL HYPERCYANOTIC ATTACKS(Hypoxic, blue or tet
spells)
A problem during first 2 years of life
Characterized by:
Hyperpnea and restlessness
Increased cyanosis
Gasping respirations
Syncope/ seizures (severe spells)
Generalized weakness sleep
Occur frequently in the morning on awakening
or after vigorous crying
Disappearance of systolic murmur
Procedures To Be Instituted During Spells:
1. Place infant on the abdomen in a
knee- chest position.2. Administer oxygen
3. Inject Morphine SO4 0.2 mg/k
Congenital Heart Disease
ACYANOTIC CHD
1. Lesions Resulting In Increased
Volume Load
1. ASD
2. VSD
3. AVSD
4. PDA
2. Lesions Resulting In IncreasedPressure Load
A. Obstructions To Ventricular Outflow:
1) Valvular Pulmonic Stenosis
2) Valvular Aortic Stenosis,
3) Coarctation Of The Aorta
B. Obstruction To Ventricular Inflow:
1) Tricuspid Stenosis
2) Mitral Stenosis
3) Cor Triatriatum
CYANOTIC CHD
1. Increased Pulmonary Blood
Flow:
1. Transposition of the great vessels
2. Defects with a common atrium or
ventricle,
3. Total Anomalous Pulmonary Venous
Return
4. Truncus Arteriosus
2. Decresed Pulmonary Blood Flow:
1. Tetralogy of Fallot
2. Tricuspid Atresia
3. Various forms of single ventricle with
Pulmonary Stenosis
THE END!