-
7/29/2019 Congenital Heart
1/23
STUDY OF PEDIATRIC CONGENITAL CARDIAC
MALFORMATIONS BY ECHOCARDIOGRAPHY
-
7/29/2019 Congenital Heart
2/23
-
7/29/2019 Congenital Heart
3/23
-
7/29/2019 Congenital Heart
4/23
ANATOMICAL CLASSIF ICATIONThe ventricular septum may be
dividedinto a small membranous portion{Perimembranous defects are
mostcommon (70%)}, and a large muscularportion. The muscular septum
has three
components: the inlet septum, thetrabecular septum (also simply
calledmuscular septum), and the outlet(infundibular or conal)
septum. Thetrabecular septum is further divided
into anterior, posterior, middle, andapical portions.
-
7/29/2019 Congenital Heart
5/23
Echocardiography
Two-dimensional and Doppler echo studies can identifythe number,
size, and exact location of the defect;estimate PA pressure by
using the modified Bernoulli
equation; identify other associated defects; andestimate the
magnitude of the shunt. Because theventricular septum is a large,
complex structure,examination for a VSD should be carried out in
a
systematic manner to be able to specify the exactlocation and
size of the defect. When possible, morethan one view should be
obtained, preferably acombination of the long- and short-axis
views.
-
7/29/2019 Congenital Heart
6/23
In patients with VSD right ventricular pressure can bedetermined
noninvasively by subtracting the VSD-gradient from the systolic
blood pressure. Using astand-alone continuous-wave Doppler the
VSD-gradient may be underestimated due to a large angletheta caused
by the various VSD locations and theoften atypical VSD-jet
directions. Therefore Color-Doppler was used to visualize the
VSD-jet and to align(angle less than 15 degrees) the
continuous-waveDoppler beam.
-
7/29/2019 Congenital Heart
7/23
Transducer position: leftsternal edge; 2nd 4thintercostal
space
Marker dot direction: pointstowards right shoulder
-
7/29/2019 Congenital Heart
8/23
Apical 4-Chamber View (AP4CH)Transducer position: apexof
heart
Marker dot direction:points towards leftshoulder
The AP5CH view isobtained from this view
by slight anteriorangulation of thetransducer towards thechest
wall. The LVOT canthen be visualised
-
7/29/2019 Congenital Heart
9/23
Apical 4-Chamber View (AP4CH
-
7/29/2019 Congenital Heart
10/23
SubCostal 4 Chamber View(SC4CH)
Transducer position:apex of the heart
Marker dot direction:
points towards leftside of neck (450anticlockwise fromAP4CH
view)
Good for assessment
ofLV anterior wall
LV inferior wall
-
7/29/2019 Congenital Heart
11/23
Doppler echocardiographyDoppler echocardiography is a method
fordetecting the direction and velocity ofmoving blood within the
heart.
Pulsed Wave (PW) useful for low
flow e.g. MV flow- measure specific bloodflow by placing the
sampling volume at theregion of enters
Continuous Wave (CW) useful for highvelocity flow e.g aortic
stenosis
Color Flow (CF) Different colors are used todesignate the
direction of blood flow. red isflow toward, and blue is flow away
fromthe transducer with turbulent flow shownas a mosaic
pattern.
-
7/29/2019 Congenital Heart
12/23
Continuous Dopplerwill measure allvelocities along theultrasound
beam: Thebeam is transmittedcontinuously, and thereceived echoes
aresampled continuously
with no range gating.
-
7/29/2019 Congenital Heart
13/23
CF DopplerCF Doppler is a pulsed wave signal with a color
valueassigned to the received signal, which is superimposedon a 2D
image. A higher frequency flow toward thetransducer is expressed in
shades of red and lowerfrequency f low away from the transducer in
shades ofblue.
CF can be used in the diagnosis of abnormal blood flowbetween
two structures including ventricular septaldefects (VSD)
-
7/29/2019 Congenital Heart
14/23
In the image on the lower panel , CFDoppler confirms abnormal
blood f lowthrough the defect.
-
7/29/2019 Congenital Heart
15/23
Echocardiographic profile in ventricular septal defect
Ventricular septal defect
(subaortic) seen from
parasternal long axis
viewParasternal long axisview showing aorta
(Ao), left atrium (LA),
left ventricle (LV) and a
small perimembranous
(subaortic) ventricular
septal defect. Mitral
valve is in the open
position and the aortic
valve in the closed
position.
-
7/29/2019 Congenital Heart
16/23
VSD Jet visualised by colour flow mapping (colour
Doppler)
Colour sector inparasternal long axisview shows the
mosaic(multi-coloured) VSD jet
across theperimembranous VSDfrom the left ventricle tothe right
ventricle. It is ahigh velocity jet becausethe VSD is
restrictive.The neck of the jetalmost corresponds tothe size of the
VSD. VSDjet is seen in a systolicframe.
-
7/29/2019 Congenital Heart
17/23
Continuous wave Doppler interrogation of VSD jet
VSD jet can be picked up in parasternallong axis or short axis
view, guided bycolor Doppler. It may also be picked upfrom the
apical four chamber view, butthe allignment may not be good.
Pulsed Doppler cannot measure the jetvelocity as it is much
higher than theNyquist limit of the pulsed Dopplersystem. Hence
continuous waveDoppler is used for interrogation ofthe VSD jet. The
interventriculargradient is calculated using theBernoulli equation.
A highinterventricular gradient indicates thatthe VSD is
restrictive. A low gradientindicates unrestrictive VSD andpulmonary
hypertension.
-
7/29/2019 Congenital Heart
18/23
Medium sized ventricular septaldefect in peri-membranous
locationseen from the apical five chamber
view. RV: right ventricle; LV: leftventricle; VSD: ventricular
septaldefect; Ao: aorta; RA: right atrium;LA: left atrium; IVS:
interventricularseptum. There is aneurysm of theinteverventricular
septum covering
the VSD, leaving a small gap. TheVSD jet passes through this
smalldefect which is restrictive (below).
-
7/29/2019 Congenital Heart
19/23
-
7/29/2019 Congenital Heart
20/23
-
7/29/2019 Congenital Heart
21/23
VSD jet documented by
Doppler interrogation,showing an interventriculargradient of
61.5 mm Hg,which suggests that the defectis restrictive. Actual
gradientmay be even more as this jet
has an incomplete envelope.
-
7/29/2019 Congenital Heart
22/23
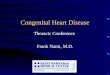
LVRA shunt in perimembranous VSD across STL fenestration
the jet from the left ventricle to the right ventricle across
the
perimembranous VSD
parasternal short axis
view of flow from the
left ventricule to right
ventricle, in theclassical location of a
perimembranous VSD.
-
7/29/2019 Congenital Heart
23/23