Embed Size (px)
Citation preview
COPYRIGHT © 2004 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
Evaluation of Morton’s Theory of Second Metatarsal Hypertrophy
BY BRETT R. GREBING, MD, AND MICHAEL J. COUGHLIN, MD
Investigation performed at Treasure Valley Hospital, Boise, Idaho
Background: Originally introduced by Morton, the concept of hypertrophy of the medial cortex and the entire shaftof the second metatarsal as an objective sign of increased mobility of the first ray has not been subjected to muchscrutiny. The goal of the current study was to assess the clinical relevance and reliability of radiographic measures of hyper-trophy of the second metatarsal in relation to mobility of the first ray, pes planus, and tightness of the gastrocnemius-soleus in both control subjects and patients with diagnosed disorders of the forefoot.
Methods: Four study groups of forty-three subjects each were evaluated. The cohort included an asymptomatic con-trol group as well as three groups made up of patients with symptoms and a diagnosis of hallux valgus, hallux rigidus,or interdigital neuroma. Mobility of the first ray (as measured with a device and method described by Klaue et al.),arch height, and ankle dorsiflexion were measured on physical examination. Plain weight-bearing radiographs and pre-viously established equations were used to determine hypertrophy and the length of the second metatarsal, and thehallux valgus and first-second intermetatarsal angles were measured on plain radiographs as well.
Results: There was no significant difference between the control and symptomatic groups with regard to the valuesfor hypertrophy of the second metatarsal. The patients with hallux valgus deformity had significantly greater mobilityof the first ray (p < 0.001) compared with the controls. No correlation was found between values for hypertrophy ofthe second metatarsal and mobility of the first ray, the length of the first metatarsal, pes planus, or restricted ankledorsiflexion. No correlation was found between mobility of the first ray and either pes planus or restricted ankle dorsi-flexion. A weak correlation (r = 0.4) was noted between increased mobility of the first ray and the hallux valgus angle.
Conclusions: Our findings do not support Morton’s concept that medial cortical hypertrophy and increased shaftwidth of the second metatarsal are associated with increased mobility of the first ray or relative shortness of the firstmetatarsal. In addition, hypertrophy of the second metatarsal was not associated with either pes planus or restrictedankle dorsiflexion. We found the practice of using hypertrophy of the second metatarsal as an indicator of mobility ofthe first ray to be unreliable, and thus we consider it to be an inappropriate indication for arthrodesis of the firstmetatarsocuneiform joint in the treatment of hallux valgus deformity.
Level of Evidence: Diagnostic study, Level IV-1 (case-control study). See Instructions to Authors for a complete de-scription of levels of evidence.
he concept of hypermobility of the first ray was intro-duced by Morton1, who suggested that, as a result ofeither dorsal extension of the first metatarsal or a short
first metatarsal2, the first ray becomes ineffective and non-functional as a weight-bearing structure. It was Lapidus3-5,however, who suggested that increased mobility of the meta-tarsocuneiform joint was a cause of hallux valgus. Mortonclaimed that hypermobility was characterized by increasedmotion of the first ray on clinical examination1, but he thoughtthat the most notable structural feature associated with hy-permobility of the first ray was hypertrophy of the secondmetatarsal bone6. Morton2 also suggested that the symptomsassociated with interdigital neuromas were probably causedby instability of the first metatarsal. Others have speculatedthat hallux rigidus is associated with instability of the first ray
as well7-10. Furthermore, Morton and others have linked pesplanus to a short first metatarsal1,6,11,12, hypermobility of thefirst ray1,6,11,12, and a contracture of the gastrocnemius or Achil-les tendon1,2,12.
While other authors have questioned the associationbetween hypermobility of the first ray and cortical hypertro-phy of the second metatarsal in normal subjects13 and in thosewith hallux valgus14, the concept of medial cortical hyper-trophy of the second metatarsal as an objective finding asso-ciated with a hypermobile hallux valgus deformity has beenaccepted with few or no supporting objective data in a num-ber of reports11,12,15-19.
Our goal in the current study was to assess the clinicalrelevance and reliability of radiographic measurements of thelength, width, and cortical thickness of the second metatarsal
T

TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 86-A · NU M B E R 7 · JU LY 2004EV A LU A T ION OF MOR TON’S THEOR Y OF SECOND ME T A T A R S A L HY P ER T ROPHY
in relation to mobility of the first ray,pes planus, and tightness of the gastroc-nemius and soleus in both normal, as-ymptomatic subjects and those with adiagnosis of hallux valgus, hallux rigi-dus, or interdigital neuroma.
Materials and MethodsApproval
ll subjects participating in this studyreceived a thorough explanation of
the risks and benefits of inclusion andgave informed consent. Approval fromthe institutional review board was ob-tained prior to the start of this study.
Inclusion CriteriaSubjects were selected for inclusion inone of four different study groups. Onlyone foot of each patient was included.The control group was composed initiallyof ten patients who had been treated fora corn on the fifth toe of the contralateralfoot but had no symptoms or previousinjury or surgery in the normal foot. Thestudy was then expanded to include anadditional thirty-three asymptomatic volun-teers who also had never had any symp-toms, injury, or treatment of the foot.These subjects were recruited from hospi-tal staff employees on a random basis.
The three other study groups in-cluded subjects with a diagnosis of hal-lux valgus, hallux rigidus, or interdigitalneuroma who presented to the office ofthe senior author (M.J.C.) for manage-ment. Each subject had only one of thethree forefoot diagnoses.
Subjects were enrolled consecu-tively if they met the criteria for inclu-sion in one of the three study groups,
but they were matched for gender. Tobe included in the study, a subject witha diagnosis of hallux valgus had to have
a moderate or severe clinical deformitywith a radiographic finding of halluxvalgus of ≥25°20. All subjects were can-
A
TABLE I Demographic Data
Group*
Entire CohortControl Hallux Valgus Hallux Rigidus Neuroma
Mean age (range) (yr) 46 (20-78) 53 (24-74) 54 (30-78) 49 (20-76) 50 (20-78)
Female† 88% (38) 88% (38) 88% (38) 88% (38) 88% (152)
Male† 12% (5) 12% (5) 12% (5) 12% (5) 12% (20)
Side†
Right 47% (20) 53% (23) 63% (27) 44% (19) 52% (89)
Left 53% (23) 47% (20) 37% (16) 56% (24) 48% (83)
*There were forty-three subjects in each group and 172 subjects in the entire cohort. †The values are given as the percentages of feet withthe number of feet in parentheses.
Fig. 1-A
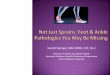
Harris mat imprint demonstrating a normal arch (Fig. 1-A) and pes planus (Fig. 1-B).
MFA = midline foot axis, a line drawn from the middle of the second toe imprint to the
center of the heel imprint.
Fig. 1-B
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 86-A · NU M B E R 7 · JU LY 2004EV A LU A T ION OF MOR TON’S THEOR Y OF SECOND ME T A T A R S A L HY P ER T ROPHY
didates for operative treatment, but the evaluation was com-pleted prior to any surgical intervention.
A subject with a diagnosis of hallux rigidus was includedin the study only if the disorder was Grade 2 or 3 as deter-mined on both clinical and radiographic examination21. Allpatients were candidates for operative treatment, but the eval-uation was completed before any surgical intervention.
To be included in the study, subjects with a diagnosisof interdigital neuroma had to have classic neuroma symp-toms22 and to have undergone surgical treatment with intra-operative and pathologic confirmation of the diagnosis. Thesepatients were evaluated after the index surgery, but all mea-surements pertaining to this study were made on their pre-operative radiographs.
Demographic Data (Table I)The average age of the entire cohort was fifty years (range,twenty to seventy-eight years). The four groups were matchedfor gender; 88% of the subjects in each were women.
Physical ExaminationAll physical examinations and radiographic measurementswere performed by the junior author (B.R.G.).
Tightness of the Achilles Tendon (Examination of Ankle Dorsiflexion)
Each patient was examined in a seated position (with the
knee flexed and extended), with attention focused on tight-ness of the gastrocnemius-soleus muscle (restricted ankledorsiflexion). Care was taken to ensure that the foot was heldin a neutral position (with the talonavicular joint reduced toeliminate transverse tarsal or subtalar motion)23,24 with re-spect to the forefoot and hindfoot during assessment of thegastrocnemius-soleus. Ankle joint motion was measured witha hinged goniometer (with 5° increments) placed on the lat-eral aspect of the foot and ankle and with the fibula and theplantar-lateral border of the foot used as landmarks for eachlimb of the goniometer. A right angle was considered to bethe neutral position.
Harris Mat Studies
Harris mat pressure studies were performed for all patients inorder to assess arch height, not to specifically document in-dividual pressure areas. Patients were asked to stand 18 in (46cm) from the Harris mat and to then step forward, placing thefoot onto the center of the prepared mat, and to continuewalking forward beyond the mat, leaving an imprint of thefoot and the hallux24-26 (Fig. 1).
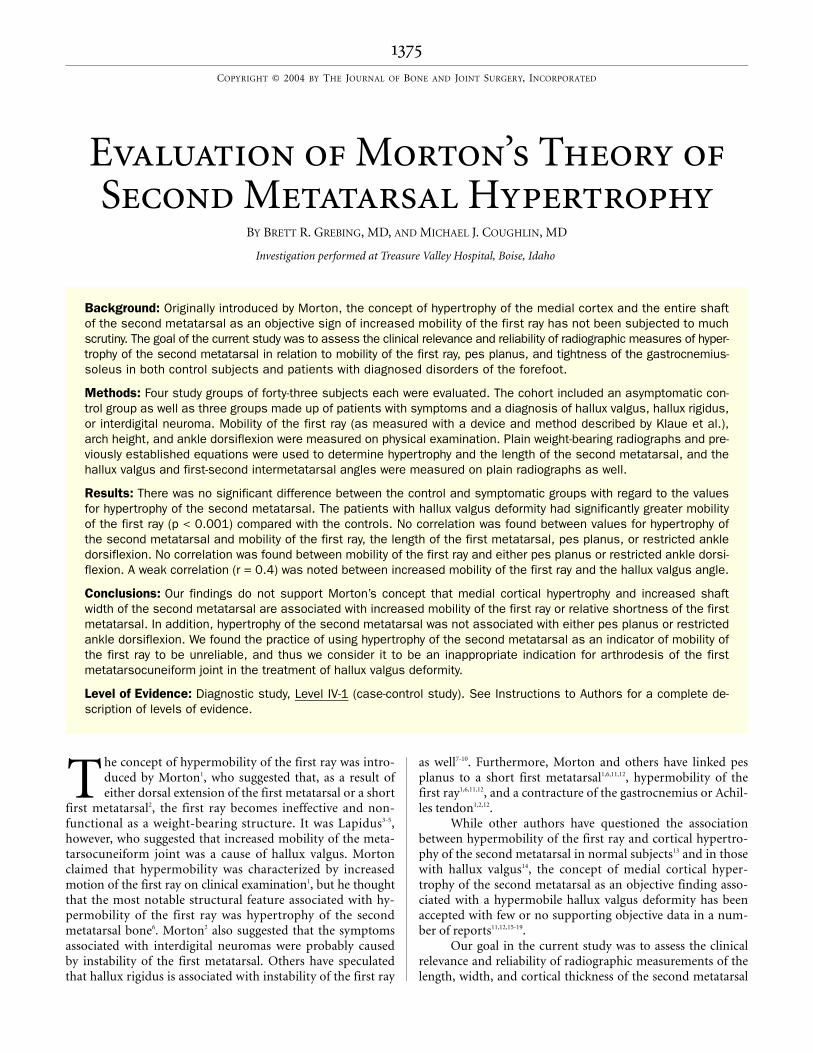
Mobility of the First Ray
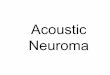
Mobility of the first ray was measured in all patients with useof the device and method described by Klaue et al.27. A mea-surement of ≤9 mm of excursion with use of the device is con-sidered normal for the first ray27 (Fig. 2).
Fig. 2
Klaue’s device27 used to measure mobility of the first ray.
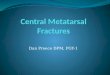
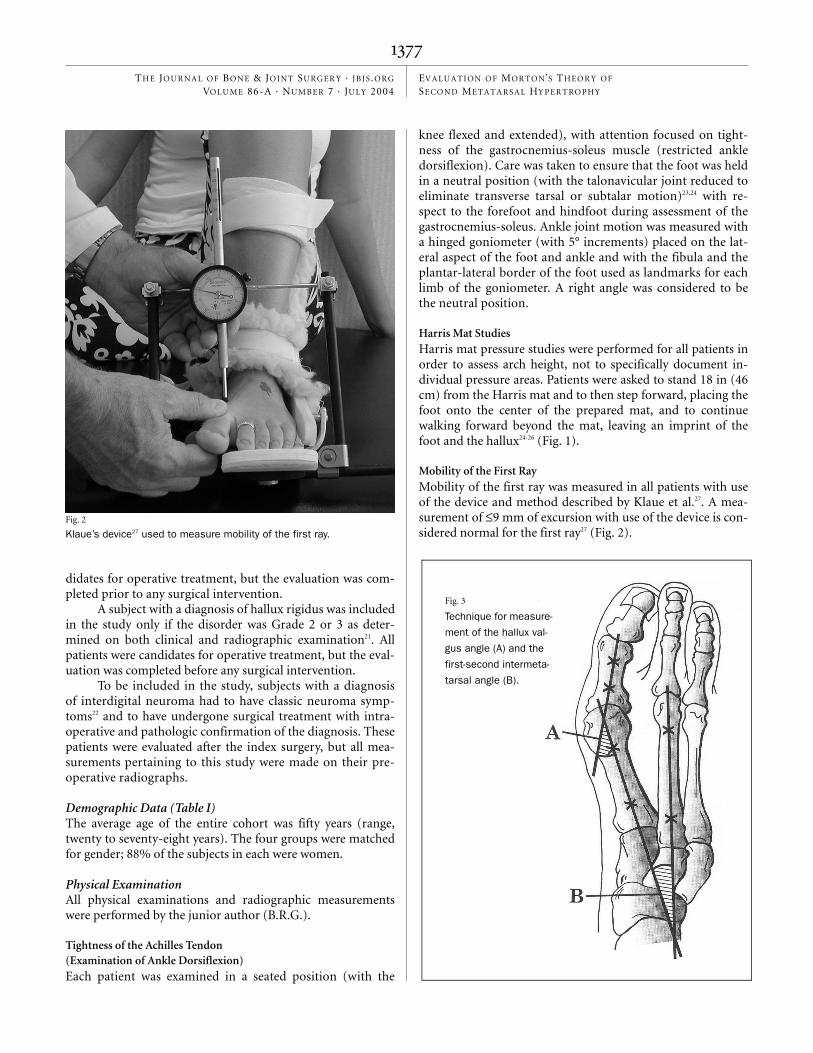
Fig. 3
Technique for measure-
ment of the hallux val-
gus angle (A) and the
first-second intermeta-
tarsal angle (B).

TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 86-A · NU M B E R 7 · JU LY 2004EV A LU A T ION OF MOR TON’S THEOR Y OF SECOND ME T A T A R S A L HY P ER T ROPHY
Radiographic ExaminationAngular Measurements
Standardized anteroposterior weight-bearing radiographs weremade and reviewed for all subjects. The hallux valgus angle (nor-mal, ≤15°) and the first-second intermetatarsal angle (normal,≤9°) were measured according to the guidelines set forth bythe American Orthopaedic Foot and Ankle Society on Angu-lar Measurements20 (Fig. 3).
Measurement of the Length of the First Metatarsal
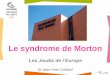
The length of the first metatarsal was measured and comparedwith that of the second metatarsal (metatarsal protrusion dis-tance) on the anteroposterior radiograph. Length measure-ments within 1 mm of each other were considered to be equal.Both Morton’s method2 and the technique used by Hardy andClapham26 (arc measurements) (Fig. 4) were used, in order tocompare the results in our studies with those in previous stud-ies. According to Hardy and Clapham, Morton’s techniquedoes not allow for measurement changes in the length of thefirst metatarsal due to angular malalignment (hallux valgusand metatarsus primus varus). The arc technique of measure-
ment allows for variation in the angle of the first metatarsal.
Measurement of Cortical Thickness
Electronic digital slide calipers (catalog #721 A-6/150; L.S.Starrett, Athol, Massachusetts) were used to measure all corti-cal and metatarsal widths. The calipers have a measuring errorof 0.03 mm.
Morton’s Ratio of Metatarsal Width2
The width of the second metatarsal in comparison with that ofthe lateral three lesser metatarsals was measured on the an-teroposterior radiograph at both (1) the junction of the proxi-mal and middle thirds of each of the lateral four metatarsalsand (2) across the neck of each of these metatarsals. The for-mula described by Morton2 was used to create a ratio withwhich to compare the relative widths of the second metatar-sals (Fig. 5).
Morton’s Ratio of Cortical Thickness2
At the midpart of the diaphysis of all four lateral metatarsals,the entire width of the shaft and the width of the medullary
Fig. 4-A
The technique for measurement of the lengths of the first and second metatarsals with use of transverse lines as described by Morton2
(Fig. 4-A) and with the arc technique described by Hardy and Clapham26 (Fig. 4-B). TN = talonavicular joint, and CC = calcaneocuboid joint.
Fig. 4-B
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 86-A · NU M B E R 7 · JU LY 2004EV A LU A T ION OF MOR TON’S THEOR Y OF SECOND ME T A T A R S A L HY P ER T ROPHY
canal were measured. The individual cortical thickness wasthen calculated, as described by Morton2, by subtracting themedullary width from the shaft width. A ratio was calculatedfrom these values in an attempt to eliminate variability thatmight occur as a result of the differences in the sizes or ages ofthe subjects (Fig. 5).
Technique of Prieskorn et al.13
At the midpart of the diaphysis of the second metatarsal, theentire width of the shaft, the width of the medullary canal,and the medial cortical width were measured. Ratios (medialcortical width to medullary canal width and medial corticalwidth to shaft width) were then calculated in order to obtain
a standardized value regardless of foot size (Fig. 6).
Statistical AnalysisStatistical analysis was performed with use of Instat software(Graphpad, San Diego, California). Comparisons among thefour groups were performed with one-way analysis of vari-ance. Significant differences identified with analysis of vari-ance were evaluated with the Dunn multiple-comparisonstest. Significance was determined by a p value of <0.05. ThePearson correlation matrix was used to assess correlation be-tween variables for all samples. Coefficient values (r values)closer to one indicate strong correlation, whereas values closerto zero indicate weak or no correlation.
TABLE II Radiographic Data
Group
Control Hallux Valgus Hallux Rigidus Neuroma
Hallux valgus angle
Mean (range) (deg) 10.6 (4-15) 34.6 (25-55) 11.0 (3-24) 10.3 (0-19)
Difference compared with control (p value) <0.001 >0.05 >0.05
1st-2nd intermetatarsal angle
Mean (range) (deg) 8.1 (3-13) 15.4 (10-23) 9.0 (4-13) 8.9 (3-16)
Difference compared with control (p value) <0.001 >0.05 >0.05
Short 1st metatarsal (% [no.] of feet)
As measured with transverse lines2 53% (23/43) 63% (27/43) 47% (20/43) 67% (29/43)
As measured with arc method26 30% (13/43) 5% (2/43) 14% (6/43) 37% (16/43)
Cortical thickness of 2nd metatarsal
Mean (range) (mm) 3.0 (1.8-4.5) 3.1 (2.0-4.9) 3.3 (2.0-4.3) 2.9 (1.6-4.0)
Difference compared with control (p value [95% confidence interval])
0.07 (2.9-3.3) 0.07 (3.1-3.4) 0.07 (2.8-3.1)
Midshaft thickness of 2nd metatarsal
Mean (range) (mm) 8.1 (7.0-11.5) 8.3 (6.5-10.8) 8.5 (7.0-10.5) 8.2 (7.0-10.2)
Difference compared with control (p value [95% confidence interval])
0.15 (8.1-8.6) 0.15 (8.3-8.8) 0.15 (7.9-8.5)
Morton’s ratio for cortical thickness2
Mean (range) 1.3 (0.99-1.56) 1.4 (0.99-2.02) 1.4 (0.95-1.78) 1.4 (1.00-2.12)
Difference compared with control (p value [95% confidence interval])
0.18 (1.3-1.5) 0.18 (1.3-1.4) 0.18 (1.4-1.5)
Morton’s ratio for shaft thickness2
Mean (range) 1.1 (0.90-1.30) 1.1 (0.95-1.40) 1.2 (0.97-1.39) 1.2 (0.93-1.40)
Difference compared with control (p value [95% confidence interval])
0.20 (1.1-1.2) 0.20 (1.1-1.2) 0.20 (1.1-1.2)
Ratio of Prieskorn et al. (MCT/IMT*)13
Mean (range) 1.1 (0.47-2.38) 1.0 (0.55-1.56) 1.1 (0.40-2.32) 1.0 (0.40-2.33)
Difference compared with control (p value [95% confidence interval])
0.64 (0.9-1.2) 0.64 (1.0-1.2) 0.64 (0.9-1.2)
Ratio of Prieskorn et al. (MCT/ST*)13
Mean (range) 0.37 (0.25-0.51) 0.37 (0.27-0.52) 0.38 (0.24-0.49) 0.36 (0.20-0.50)
Difference compared with control (p value [95% confidence interval])
0.40 (0.35-0.39) 0.40 (0.36-0.40) 0.40 (0.34-0.38)
*MCT = medial cortical thickness of the second metatarsal, IMT = intramedullary thickness of the second metatarsal, and ST = thickness ofthe entire shaft of the second metatarsal.

TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 86-A · NU M B E R 7 · JU LY 2004EV A LU A T ION OF MOR TON’S THEOR Y OF SECOND ME T A T A R S A L HY P ER T ROPHY
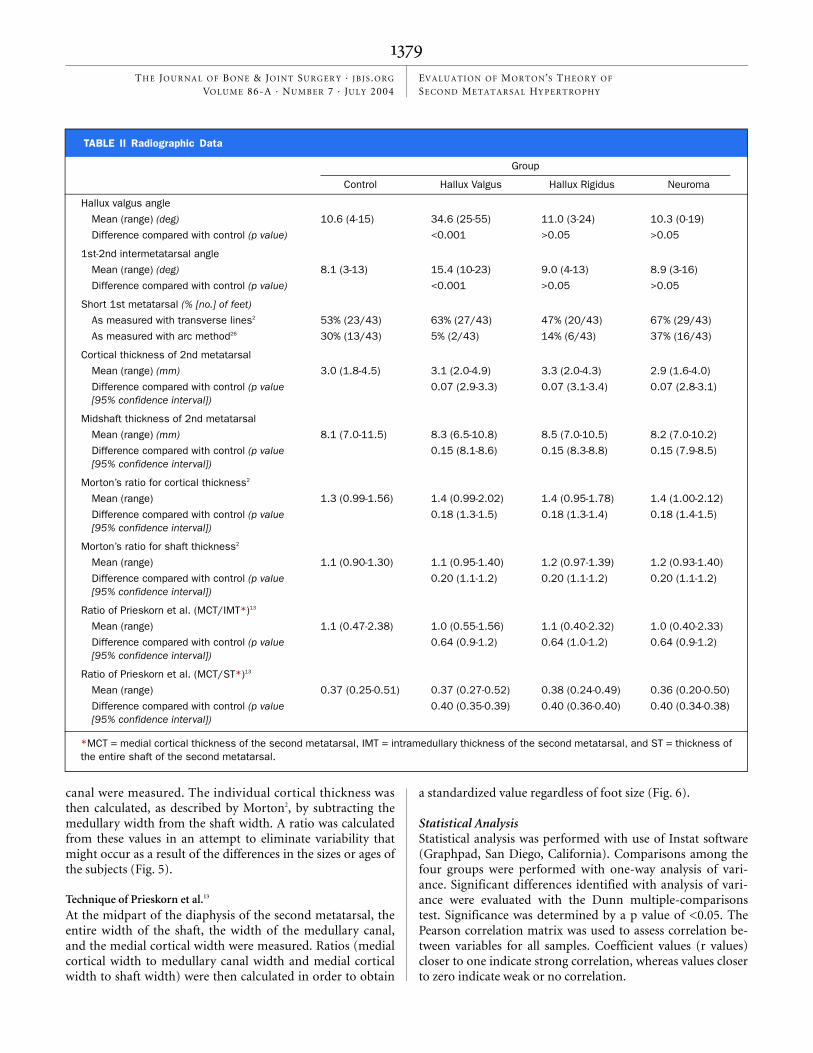
ResultsRadiographic Measurements (Table II)Angular Measurements
he average hallux valgus angle was 34.6° (range, 25° to55°) and the average first-second intermetatarsal angle
was 15.4° (range, 10° to 23°) in the hallux valgus group. Thehallux valgus group differed significantly from the other threegroups with regard to both the hallux valgus angle (p < 0.001)and the first-second intermetatarsal angle (p < 0.001).
Length of First Metatarsal
With use of Morton’s transverse line technique2 to measure the
first metatarsal protrusion distance, 53% (twenty-three) of theforty-three first metatarsals in the control group were foundto be shorter than the second metatarsal. With use of the arcmethod of measurement26, 30% (thirteen) of the first metatar-sals were found to be shorter than the second metatarsal.
When used in the other three groups, the Morton andarc techniques provided distinctly different values, with amarked reduction in the prevalence of short first metatarsalswhen the arc technique was employed. In the hallux valgusgroup, 63% of the first metatarsals were determined to beshort with use of the Morton technique whereas only 5% werenoted to be shorter when the arc technique was used. In theentire cohort, 58% (ninety-nine) of the 172 feet were found tohave a short first metatarsal when measured with Morton’stechnique, whereas 22% (thirty-seven) were found to have ashort first metatarsal when measured with the arc technique.
Cortical Thickness
The average medial cortical thickness of the second meta-tarsal shaft was 3.0 mm in the control group, 3.1 mm in thehallux valgus group, 3.3 mm in the hallux rigidus group, and
T
Fig. 5
With Morton’s technique2, the width of the second metatarsal is quanti-
fied in comparison with that of the three other lesser metatarsals. The
width of the shaft is measured both at the junction of the proximal and
middle thirds (a) of each of the lateral four metatarsals and across the
neck (b) of each of the metatarsals. In order to eliminate variability due
to differences in the sizes and ages of individuals, a ratio of the four
lateral metatarsals is created with the formula:
where I = calculated ratio, II = second metatarsal, III = third metatar-
sal, IV = fourth metatarsal, and V = fifth metatarsal.
Morton quantified cortical thickness2 by measuring the width of
the midpart of the shaft of each of the lateral four metatarsals and
subtracting the intramedullary width (IMT). A ratio is calculated to elim-
inate variability due to differences in the sizes and ages of subjects
with the formula:
where I = calculated ratio, II = second metatarsal, III = third metatar-
sal, IV = fourth metatarsal, V = fifth metatarsal, s = width of the shaft,
and m = width of the intramedullary canal.
(a+b)III(a+b) + IV(a+b) + V(a+b)
3--------------------------------------------------------------------[ ]⁄ I=
(s-m)III(s-m) + IV(s-m) + V(s-m)
3------------------------------------------------------------------[ ]⁄ I=
Fig. 6
With the technique of Prieskorn et al.13, the medial cortical thickness of
the second metatarsal (MCT), the intramedullary thickness of the sec-
ond metatarsal (IMT), and the thickness of the entire shaft (ST) are all
measured at the midpart of the shaft. Two ratios are then established
to evaluate and standardize the medial cortical thickness of the sec-
ond metatarsal for variability in the sizes of the subjects. The medial
cortical thickness is divided by the intramedullary cortical thickness
(MCT/IMT), and the medial cortical thickness is also divided by the en-
tire shaft thickness (MCT/ST).
TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 86-A · NU M B E R 7 · JU LY 2004EV A LU A T ION OF MOR TON’S THEOR Y OF SECOND ME T A T A R S A L HY P ER T ROPHY
2.9 mm in the neuroma group. The differences between thecontrol and the other three groups were not significant. Also,there was no significant difference among the four groupswith regard to the midshaft width of the second metatarsal,the ratios obtained from Morton’s equations for shaft andcortical thickness of the metatarsals, or the values obtainedwith Prieskorn’s equations for medial cortical thickness of themetatarsals (Table III).
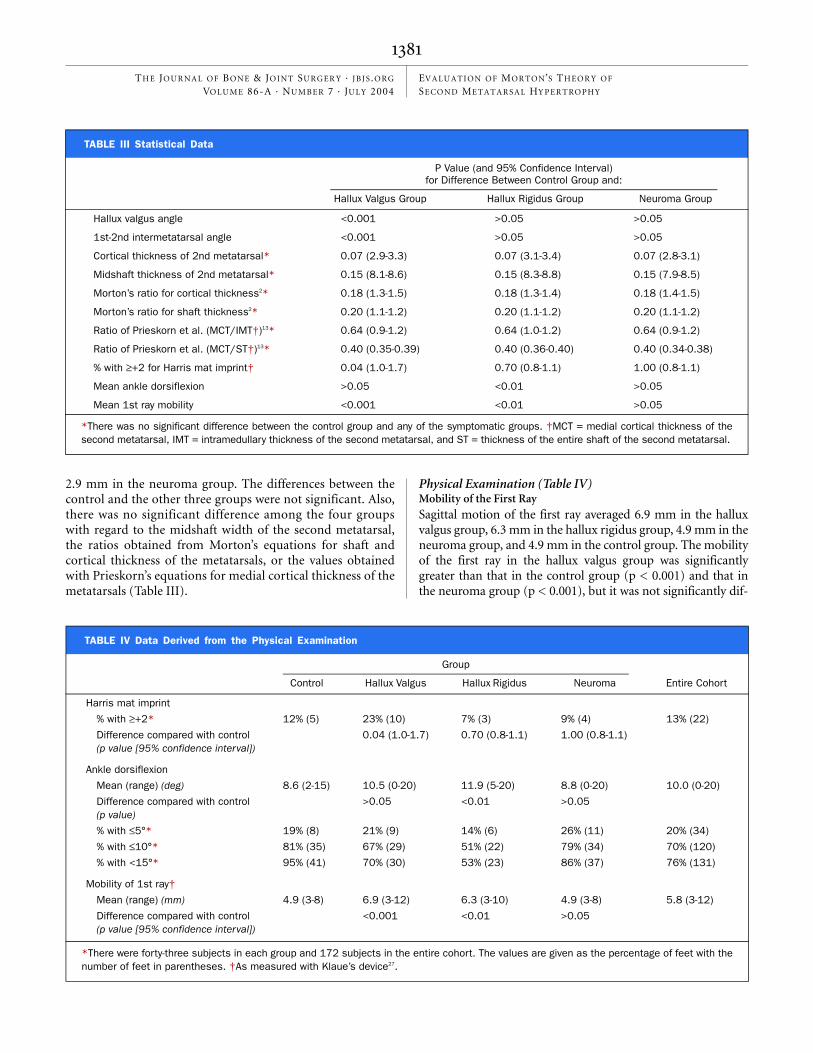
Physical Examination (Table IV)Mobility of the First Ray
Sagittal motion of the first ray averaged 6.9 mm in the halluxvalgus group, 6.3 mm in the hallux rigidus group, 4.9 mm in theneuroma group, and 4.9 mm in the control group. The mobilityof the first ray in the hallux valgus group was significantlygreater than that in the control group (p < 0.001) and that inthe neuroma group (p < 0.001), but it was not significantly dif-
TABLE IV Data Derived from the Physical Examination
Group
Entire CohortControl Hallux Valgus Hallux Rigidus Neuroma
Harris mat imprint
% with ≥+2* 12% (5) 23% (10) 7% (3) 9% (4) 13% (22)
Difference compared with control (p value [95% confidence interval])
0.04 (1.0-1.7) 0.70 (0.8-1.1) 1.00 (0.8-1.1)
Ankle dorsiflexion
Mean (range) (deg) 8.6 (2-15) 10.5 (0-20) 11.9 (5-20) 8.8 (0-20) 10.0 (0-20)
Difference compared with control (p value)
>0.05 <0.01 >0.05
% with ≤5°* 19% (8) 21% (9) 14% (6) 26% (11) 20% (34)
% with ≤10°* 81% (35) 67% (29) 51% (22) 79% (34) 70% (120)
% with <15°* 95% (41) 70% (30) 53% (23) 86% (37) 76% (131)
Mobility of 1st ray†
Mean (range) (mm) 4.9 (3-8) 6.9 (3-12) 6.3 (3-10) 4.9 (3-8) 5.8 (3-12)
Difference compared with control (p value [95% confidence interval])
<0.001 <0.01 >0.05
*There were forty-three subjects in each group and 172 subjects in the entire cohort. The values are given as the percentage of feet with thenumber of feet in parentheses. †As measured with Klaue’s device27.
TABLE III Statistical Data
P Value (and 95% Confidence Interval) for Difference Between Control Group and:
Hallux Valgus Group Hallux Rigidus Group Neuroma Group
Hallux valgus angle <0.001 >0.05 >0.05
1st-2nd intermetatarsal angle <0.001 >0.05 >0.05
Cortical thickness of 2nd metatarsal* 0.07 (2.9-3.3) 0.07 (3.1-3.4) 0.07 (2.8-3.1)
Midshaft thickness of 2nd metatarsal* 0.15 (8.1-8.6) 0.15 (8.3-8.8) 0.15 (7.9-8.5)
Morton’s ratio for cortical thickness2* 0.18 (1.3-1.5) 0.18 (1.3-1.4) 0.18 (1.4-1.5)
Morton’s ratio for shaft thickness2* 0.20 (1.1-1.2) 0.20 (1.1-1.2) 0.20 (1.1-1.2)
Ratio of Prieskorn et al. (MCT/IMT†)13* 0.64 (0.9-1.2) 0.64 (1.0-1.2) 0.64 (0.9-1.2)
Ratio of Prieskorn et al. (MCT/ST†)13* 0.40 (0.35-0.39) 0.40 (0.36-0.40) 0.40 (0.34-0.38)
% with ≥+2 for Harris mat imprint† 0.04 (1.0-1.7) 0.70 (0.8-1.1) 1.00 (0.8-1.1)
Mean ankle dorsiflexion >0.05 <0.01 >0.05
Mean 1st ray mobility <0.001 <0.01 >0.05
*There was no significant difference between the control group and any of the symptomatic groups. †MCT = medial cortical thickness of thesecond metatarsal, IMT = intramedullary thickness of the second metatarsal, and ST = thickness of the entire shaft of the second metatarsal.

TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 86-A · NU M B E R 7 · JU LY 2004EV A LU A T ION OF MOR TON’S THEOR Y OF SECOND ME T A T A R S A L HY P ER T ROPHY
ferent from that in the hallux rigidus group (p > 0.05). The mo-bility of the first ray in the hallux rigidus group was alsosignificantly increased compared with that in the control group(p < 0.01) and that in the neuroma group (p < 0.001). Therewas no significant difference between the control and neuromagroups with regard to mobility of the first ray (p > 0.05).
Contracture of the Achilles Tendon
In the evaluation of tightness of the gastrocnemius and soleus,no group was found to have <5° of dorsiflexion on average.Both the hallux valgus and the hallux rigidus group had, onaverage, >10° of ankle dorsiflexion. The hallux rigidus grouphad the greatest ankle dorsiflexion, with an average of 11.9°,which was significantly greater than the values in the control(p < 0.01) and neuroma groups (p < 0.01) but not signifi-cantly greater than the value in the hallux valgus group (p >0.05). The control group had the lowest average ankle dorsi-flexion (8.6°): 19% (eight) of the forty-three subjects in thatgroup had ≤5° of ankle dorsiflexion; 81% (thirty-five), ≤10°;and 95% (forty-one), <15°. Of the entire cohort of 172 sub-jects, 20% (thirty-four) exhibited ankle dorsiflexion of ≤5°;70% (120), ≤10°; and 76% (131), <15°.
Pes Planus
The Harris mat studies demonstrated that a low arch (pesplanus) was significantly more common in the hallux valgusgroup than it was in the control group (p = 0.04), hallux rigi-dus group (p = 0.01), or neuroma group (p = 0.02). Of thesubjects with hallux valgus, 23% (ten) had moderate or severepes planus deformity (a grade of +2 or greater for the Harrismat imprint). There was no significant difference among theother three groups (p > 0.05).
We analyzed the relationship between pes planus and ashort first ray as measured with the arc technique, and wefound that only five (23%) of the twenty-two subjects withmoderate or severe pes planus deformity had a short firstmetatarsal. We also found that only six (27%) of the twenty-two feet with moderate or severe pes planus demonstratedincreased mobility of the first ray (>9 mm of motion as mea-sured with Klaue’s device). Three (14%) of the twenty-two pa-tients with moderate or severe pes planus had both a shortfirst metatarsal and increased mobility of the first ray.
Correlations (Table V)Of all of the variables that were considered, only the hallux
TABLE V Pearson Correlations*
VariablesHallux
Valgus Angle
1st-2nd Intermetatarsal
Angle
Length of 1st
MetatarsalMobility of 1st Ray
Ankle Dorsiflexion
% with ≥+2 for Harris
Mat Imprint
Cortical thickness of 2nd metatarsal
0.1 0.0 0.1 0.1 0.1 0.1
Midshaft thickness of 2nd metatarsal
0.0 −0.1 0.1 −0.1 0.0 0.1
Morton’s ratio for cortical thickness2
0.0 0.0 0.0 0.1 0.1 0.0
Morton’s ratio for shaft thickness2
0.1 0.0 −0.1 0.0 −0.1 0.2
Ratio of Prieskorn et al. (MCT/IMT†)13
−0.1 −0.1 0.0 0.0 0.1 0.0
Ratio of Prieskorn et al. (MCT/ST†)13
0.0 0.0 0.1 0.1 0.2 0.0
Hallux valgus angle 0.8 0.2 0.4 0.1 0.3
1st-2nd intermetatarsal
angle 0.2 0.3 0.1 0.2
Length of 1st metatarsal 0.2 0.1 0.1
Mobility of 1st ray 0.2 0.1
Ankle dorsiflexion 0.1
% with ≥+2 for Harris mat imprint
*Pearson coefficient values (r values) are shown for correlations between each variable. Note the strong correlation between increasing hal-lux valgus angle and increasing first-second intermetatarsal angle, a mild correlation between increasing mobility of the first ray (as mea-sured with Klaue’s device27) and both increasing hallux valgus angle and increasing first-second intermetatarsal angle, and a mild correlationbetween pes planus and both increasing hallux valgus angle and increasing first-second intermetatarsal angle. †MCT = medial cortical thick-ness of the second metatarsal, IMT = intramedullary thickness of the second metatarsal, and ST = thickness of the entire shaft of the sec-ond metatarsal.

TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 86-A · NU M B E R 7 · JU LY 2004EV A LU A T ION OF MOR TON’S THEOR Y OF SECOND ME T A T A R S A L HY P ER T ROPHY
valgus angle and the first-second intermetatarsal angle showeda strong correlation (r = 0.8). No other variables showedstrong correlation across the entire sample. Only a weak corre-lation was noted between pes planus and hallux valgus defor-mity (r = 0.3) and between pes planus and the first-secondintermetatarsal angle (r = 0.2). There was also weak correla-tion between mobility of the first ray and hallux valgus defor-mity (r = 0.4) and between mobility of the first ray and thefirst-second intermetatarsal angle (r = 0.3).
Discussionorton2 based his conclusion that hypertrophy of thesecond metatarsal is a sign of hypermobility of the first
ray on an analysis of 150 subjects who presented with fore-foot pain. Of those patients, fifty-one were diagnosed as hav-ing moderate or severe hypermobility of the first ray. In thecurrent study, we examined 172 subjects, and we assessedonly one foot of each subject. There were forty-three sub-jects in each of four study groups: asymptomatic controls,patients with hallux valgus, patients with hallux rigidus, andpatients with interdigital neuroma. The asymptomatic con-trol group was evaluated for characteristics of the secondmetatarsal and was compared with the groups of symptom-atic patients. A group with interdigital neuroma was included toevaluate Morton’s notion2 that hypermobility of the first rayis associated with development of neuromas, and a groupwith hallux valgus was examined to evaluate Lapidus’s con-tention that hypermobility is associated with hallux valgus3-5.Patients with hallux rigidus were selected as the fourth groupbecause of the implication that hypermobility is also associ-ated with this diagnosis7-10,12.
Morton1 stated that the most notable feature associatedwith hypermobility of the first ray was hypertrophy of the sec-ond metatarsal, which was manifested as either widening ofthe shaft or thickening of the cortex2,6,28. He surmised that thishypertrophy was due to either a short first metatarsal or hy-permobility of the first metatarsal that made the first ray lesseffective as a weight-bearing structure, increasing the weight-bearing burden being shifted onto the lesser metatarsals.Morton hypothesized that the majority of this burden was ab-sorbed by the second metatarsal, resulting in hypertrophy,although he offered no anatomic or statistical proof of hishypothesis2.
Prieskorn et al.13 found no correlation between motionof the first metatarsocuneiform joint and the medial corticalthickness of the second metatarsal in a study of 100 normalfeet. Later, Faber et al.14 reported no significant correlation be-tween mobility of the first metatarsocuneiform joint and theshaft width or medial cortical thickness of the second metatar-sal in ninety-four patients with hallux valgus. In both of thosestudies, the investigators used radiographic techniques to as-sess mobility of the first ray, which was measured in degrees,and those are the only reports on the subject that we couldfind in the literature. Using Klaue’s device, we measured mo-tion of the first ray in millimeters. The technique that Morton2
used early on as well as the technique used later by others13,14,29
to measure metatarsal hypertrophy employed ratios ratherthan absolute values to compensate for varying foot and meta-tarsal sizes. We chose to use both of these techniques in orderto be consistent for comparison purposes.
Our results with the use of Klaue’s device to measuremobility of the first ray confirm the findings in the radio-graphic studies of Prieskorn et al.13 and Faber et al.14, as wefound no correlation between mobility of the first ray andthe length, shaft width, or medial cortical width of the secondmetatarsal. Furthermore, we found no correlation betweenmobility of the first ray and the results of Morton’s two equa-tions for cortical hypertrophy and size. We also found no cor-relation between mobility of the first ray and medial corticalthickness in patients with hallux valgus, hallux rigidus, or in-terdigital neuroma, and there was no significant difference be-tween the values in any of the symptomatic groups and thosein the control group.
Morton1,28 observed unusual shortness of the first meta-tarsal bone when he compared it with the second, and hesuggested that this shortness led to increased pressure be-neath the lesser metatarsals and to excessive pronation. Har-ris and Beath30, however, disputed this notion in their studyof 7167 feet of male military recruits; they observed an equalfrequency of disturbed weight-bearing in feet in which thefirst metatarsal was equal to or longer than the second meta-tarsal and in those with a short first metatarsal. Overall, theyfound that 32% of feet had a short first metatarsal when theyused the arc technique of measurement. The vast majority oftheir subjects with a short first metatarsal had no symptomsor evidence of disturbed weight-bearing. They concludedthat shortness of the first metatarsal relative to the seconddid not mean that the first metatarsal could not readily reachthe ground or that less weight was transmitted through thisbone. Using the same measurement technique, we found anoverall 22% prevalence of feet with a short first metatarsal,which was lower than the prevalence reported by Harris andBeath30.
The relative lengths of the first and second metatarsalscan be measured with different techniques. When metatarsallength is measured with use of arcs intersecting the distal ar-ticular surfaces of the first and second metatarsals26,28, the rela-tive lengths of the metatarsals are not influenced by variationin the intermetatarsal angle or by metatarsus adductus; thus,we prefer this method of measurement. When this techniquewas used in the current study, the prevalence of a short firstmetatarsal was found to be 30% in the control group and 5%in the group with hallux valgus. Morton2 utilized transverselines to quantify metatarsal length and reported various de-grees of shortness of the first metatarsal in 51% (seventy-seven) of his 150 patients with metatarsalgia. In the currentstudy, when metatarsal length was determined with use oftransverse lines, the prevalence of a short first metatarsal in-creased dramatically, from 5% to 63%, in the group with hal-lux valgus and it increased between two and twelvefold in allthree study groups. We believe that Morton’s notion of a highprevalence of a short first metatarsal in patients with metatar-
M

TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 86-A · NU M B E R 7 · JU LY 2004EV A LU A T ION OF MOR TON’S THEOR Y OF SECOND ME T A T A R S A L HY P ER T ROPHY
salgia was largely due to a measurement artifact with his noveltechnique. However, regardless of whether the transverse lineor the arc method was used, we found no correlation betweena short first metatarsal and the shaft width or cortical hyper-trophy of the second metatarsal.
The concept of hypermobility of the first ray was intro-duced by Morton in 19281. While Morton claimed that hyper-mobility of the first ray led to a multitude of foot disorders1,2,he noted that he had been unable to devise a method withwhich to quantify the degree of dorsal hypermobility of thefirst ray2. Recently, attempts have been made to quantify mo-bility of the first ray on the basis of either degrees13,31-33 or milli-meters of either dorsal displacement or total excursion27,34-37.
Our data are comparable with those in previous reportsin which mobility was measured in millimeters of displace-ment with Klaue’s device27,38. Klaue et al.27 defined a first ray ashypermobile if there was >9 mm of measured motion. Wefound Klaue’s device to be reliable and to provide reproduc-ible measurements of excursion of the first ray when werepeated the measurements on the same individuals. Whilethe applied force is not standardized when this device is used,it is similar in magnitude to that employed in a manualexamination12,18,39. Voellmicke and Deland39 proposed that asimilar level of mobility of the first ray (8 to 10 mm) foundwith a manual examination is indicative of hypermobility.
While the group with hallux valgus in our study diddemonstrate greater mobility of the first ray than did theother three groups, mobility of the first ray did not correlatewith increased medial cortical width of the second metatarsal,increased midshaft width of the second metatarsal, or any ofthe results of the formulas suggested by either Morton2 orPrieskorn et al.13. On the basis of our data, we cannot supportMorton’s theory6 that the most notable structural feature as-sociated with hypermobility of the first ray is hypertrophy ofthe second metatarsal bone.
Hardy and Clapham40 reported a correlation between anincreased hallux valgus angle and the first-second intermeta-tarsal angle, which we found as well.
Lapidus5 (in 1960) and others12,15-18,27,41 believed that hal-lux valgus was associated with hypermobility of the first rayand recommended a metatarsocuneiform arthrodesis. WhileFritz and Prieskorn29 and Faber et al.31 reported no correlationbetween mobility of the first metatarsocuneiform joint andthe magnitude of the first-second intermetatarsal angle, wedid observe a correlation between mobility of the first ray andan increased hallux valgus angle. Only a prospective study onthe treatment of hallux valgus will enable us to evaluate theimportance of this finding.
Morton42 defined normal ankle dorsiflexion as a mini-mum of 15°. In the control group in the current study, 95% ofthe subjects had <15° of ankle dorsiflexion when examinedwith the knee in full extension and the hindfoot in neutral.Using ≤5° of ankle dorsiflexion as a guideline, DiGiovanni etal.43 observed that eight (24%) of thirty-four normal subjectshad restricted dorsiflexion, and when they used ≤10° as aguideline, they found that fifteen (44%) of the normal sub-
jects had restricted dorsiflexion. In the current study, eight(19%) of the forty-three subjects in the control group had an-kle dorsiflexion of ≤5°, thirty-five (81%) had ≤10°, and forty-one (95%) had <15°.
It has been suggested that a gastrocnemius contractureplays a vital biomechanical role in chronic foot and ankleproblems43. While lengthening of the gastrocnemius has beenrecommended for patients with a limitation of dorsiflexion of≥5° who are undergoing surgical treatment for selected footdisorders12, we suggest that since 81% of the subjects in ourcontrol group demonstrated ≤10° of ankle dorsiflexion, thisfinding may not be abnormal.
To be consistent with the evaluation techniques of Mor-ton2 and others24,26,30, we used a foot imprint to determine pesplanus deformity and low arch height. It has been suggestedthat pes planus is often the result of either an anatomicallyshort or a functionally short (hypermobile) first ray6,11. Mor-ton1 concluded that this shortening leads to ineffective weight-bearing by the medial column, pronation of the foot, and adepression of the longitudinal arch as evidenced by the footimprints in his study. Lapidus3 also suggested that there was anassociation between pes planus and hypermobility of the firstray but linked it to medial deviation of the first metatarsal andhallux valgus deformity.
Others24,40, however, have challenged the notion that pesplanus is associated with an ineffective first ray. Harris andBeath24 found that the prevalence of pronation and pes planuswhen the first metatarsal was short was similar to that when itwas long. Hardy and Clapham40 concluded that there was nocorrelation between mobility of the first metatarsocuneiformjoint and pes planus. Neither of these studies, however, in-cluded a statistical analysis of the results, and Harris andBeath24 evaluated only male military recruits.
We found no correlation between pes planus and eithermobility of the first ray or the length of the first metatarsal.Only 23% of individuals with pes planus had a short firstmetatarsal, only 27% of individuals with pes planus dem-onstrated increased mobility of the first ray, and 14% of in-dividuals with pes planus demonstrated both a short firstmetatarsal and increased mobility of the first ray. Our find-ings are in accord with those of Harris and Beath24 and Hardyand Clapham40; thus, we cannot support Morton’s theory thatmobility or shortness of the first ray leads to a pes planusdeformity.
We are not aware of any report on the prevalence of pesplanus and hallux valgus in adult patients. Coughlin25, how-ever, reported that 16% of forty-five adolescent patients withhallux valgus demonstrated pes planus and that flat feet wereno more common in his patients than in the general popu-lation. Our finding of pes planus in 11% of the individuals inour control group supports a previous finding that 10% to20% of the population has an asymptomatic pes planusdeformity24. While there was indeed a higher prevalence ofpes planus in the group with hallux valgus than in the controlgroup in our study, when we examined the entire cohort, wefound only a weak correlation between the hallux valgus an-

TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 86-A · NU M B E R 7 · JU LY 2004EV A LU A T ION OF MOR TON’S THEOR Y OF SECOND ME T A T A R S A L HY P ER T ROPHY
gle and pes planus. This finding may be due to our samplesize; a larger study group may have demonstrated a strongercorrelation.
Morton42 suggested that, in addition to being associatedwith mobility of the first ray, pes planus deformity was associ-ated with a tight Achilles tendon. In the current study, wefound no correlation between pes planus and limited ankledorsiflexion. Morton2 thought that pronation of the foot as aresult of either a tight Achilles tendon or dysfunction of thefirst ray shifted weight laterally onto the forefoot and thatthese stresses were concentrated on the second metatarsal,which resulted in widening of the shaft and thickening of thecortex. We found no association between pes planus and theshaft width or cortical hypertrophy of the second metatarsal.
In conclusion, Morton stressed that a majority of fore-foot problems are related to insufficiency of the first ray andassociated pes planus and Achilles tendon contracture. Heconsidered the most notable evidence of insufficiency of thefirst ray to be hypertrophy and medial cortical thickening ofthe second metatarsal as seen on plain radiographs. Theresults of our investigation demonstrated no significant dif-ference between asymptomatic controls and symptomaticsubjects with hallux valgus, hallux rigidus, or an interdigitalneuroma with regard to hypertrophy or cortical thickness ofthe second metatarsal. In addition, we found no correlationbetween hypertrophy of the second metatarsal and pes pla-
nus, restricted ankle dorsiflexion, mobility of the first ray, orlength of the first ray.
As we found no evidence to support Morton’s theorythat mobility of the first ray is characterized by hypertrophy ofthe second metatarsal, we cannot support the practice of con-sidering cortical hypertrophy of the second metatarsal to be anindication for arthrodesis of the first metatarsocuneiformjoint in the treatment of a hallux valgus deformity. �
NOTE: The authors thank Mary Samson, MS, Denver, Colorado, for her statistical support andexpertise.
References
1. Morton DJ. Hypermobility of the first metatarsal bone: the interlinking factor between metatarsalgia and longitudinal arch strains. J Bone Joint Surg. 1928;10:187-96.
2. Morton DJ. The human foot; its evolution, physiology and functional disorders. New York: Columbia University Press; 1935.
3. Lapidus PW. Operative correction of the metatarsus varus primus in hallux valgus. Surg Gynecol Obstet. 1934;58:183-91.
4. Lapidus PW. A quarter of a century of experience with the operative correc-tion of the metatarsus varus primus in hallux valgus. Bull Hosp Joint Dis. 1956;17:404-21.
5. Lapidus PW. The author’s bunion operation from 1931 to 1959. Clin Orthop. 1960;16:119-35.
6. Morton DJ. Significant characteristics of the Neanderthal foot. Natural His-tory. 1926;26:310-14.
7. Bingold AC, Collins DH. Hallux rigidus. J Bone Joint Surg Br. 1950;32:214-22.
8. Kurtz DH, Harrill JC, Kaczander BI, Solomon MG. The Valenti procedure for hallux limitus: a long-term follow-up and analysis. J Foot Ankle Surg. 1999;38:123-30.
9. Jack EA. The aetiology of hallux rigidus. Br J Surg. 1940;27:492-7.
10. Saxena A. The Valenti procedure for hallux limitus/rigidus. J Foot Ankle Surg. 1995;34:485-8.
11. Hansen ST Jr. Hallux valgus surgery. Morton and Lapidus were right! Clin Po-diatr Med Surg. 1996;13:347-54.
12. Hansen ST Jr. Functional reconstruction of the foot and ankle. Philadelphia: Lippincott Williams and Wilkins; 2000. p 22-4, 28-32, 217-9, 222-3.
13. Prieskorn DW, Mann RA, Fritz G. Radiographic assessment of the second metatarsal: measure of first ray hypermobility. Foot Ankle Int. 1996;17:331-3.
14. Faber FW, Kleinrensink GJ, Mulder PG, Verhaar JA. Mobility of the first tar-sometatarsal joint in hallux valgus patients: a radiographic analysis. Foot An-kle Int. 2001;22:965-9.
15. Bednarz PA, Manoli A 2nd. Modified Lapidus procedure for the treatment of
hypermobile hallux valgus. Foot Ankle Int. 2000;21:816-21.
16. Clark HR, Veith RG, Hansen ST Jr. Adolescent bunions treated by the modi-fied Lapidus procedure. Bull Hosp Jt Dis Orthop Inst. 1987;47:109-22.
17. Myerson M, Allon S, McGarvey W. Metatarsocuneiform arthrodesis for man-agement of hallux valgus and metatarsus primus varus. Foot Ankle. 1992;13:107-15.
18. Myerson MS, Badekas A. Hypermobility of the first ray. Foot Ankle Clin. 2000;5:469-84.
19. Sangeorzan BJ, Hansen ST Jr. Modified Lapidus procedure for hallux valgus. Foot Ankle. 1989;9:262-6.
20. Coughlin MJ, Saltzman CL, Nunley JA 2nd. Angular measurements in the evaluation of hallux valgus deformities: a report of the ad hoc committee of the American Orthopaedic Foot and Ankle Society on Angular Measurements. Foot Ankle Int. 2002;23:68-74.
21. Coughlin MJ, Shurnas PS. Hallux rigidus. Grading and long-term results of op-erative treatment. J Bone Joint Surg Am. 2003;85:2072-88.
22. Coughlin MJ, Pinsonneault T. Operative treatment of interdigital neuroma. A long-term follow-up study. J Bone Joint Surg Am. 2001;83:1321-8.
23. Bordelon RL. Surgical and conservative foot care: a unified approach to princi-ples and practice. Thorofare, NJ: Slack; 1988. p 13-4.
24. Harris RI, Beath T. Hypermobile flat-foot with short tendo Achillis. J Bone Joint Surg Am. 1948;30:116-38.
25. Coughlin M. Juvenile hallux valgus: etiology and treatment. Foot Ankle Int. 1995;16:682-97.
26. Hardy RH, Clapham JC. Observations on hallux valgus; based on a controlled series. J Bone Joint Surg Br. 1951;33:376-91.
27. Klaue K, Hansen ST, Masquelet AC. Clinical, quantitative assessment of first tarsometatarsal mobility in the sagittal plane and its relation to hallux valgus deformity. Foot Ankle Int. 1994;15:9-13.
28. Morton D. Metatarsus ativicus. J Bone Joint Surg. 1927;9:531-44.
29. Fritz GR, Prieskorn D. First metatarsocuneiform motion: a radiographic and statistical analysis. Foot Ankle Int. 1995;16:117-23.
30. Harris RI, Beath T. The short first metatarsal. Its incidence and clinical sig-
Brett R. Grebing, MD180 South Third Street, Suite 100, Belleville, IL 62220. E-mail address: [email protected]
Michael J. Coughlin, MD901 North Curtis Road, Suite 503, Boise, ID 83706. E-mail address: [email protected]
The authors did not receive grants or outside funding in support of their research or preparation of this manuscript. They did not receive pay-ments or other benefits or a commitment or agreement to provide such benefits from a commercial entity. No commercial entity paid or directed, or agreed to pay or direct, any benefits to any research fund, foundation, educational institution, or other charitable or nonprofit organization with which the authors are affiliated or associated.

TH E JO U R NA L OF BONE & JOINT SURGER Y · JBJS .ORG
VO LU M E 86-A · NU M B E R 7 · JU LY 2004EV A LU A T ION OF MOR TON’S THEOR Y OF SECOND ME T A T A R S A L HY P ER T ROPHY
nificance. J Bone Joint Surg Am. 1949;31:553-65.
31. Faber FW, Kleinrensink GJ, Verhoog MW, Vijn AH, Snijders CJ, Mulder PG, Verhaar JA. Mobility of the first tarsometatarsal joint in relation to hallux val-gus deformity: anatomical and biomechanical aspects. Foot Ankle Int. 1999;20:651-6.
32. Ito H, Shimizu A, Miyamoto T, Katsura Y, Tanaka K. Clinical significance of increased mobility in the sagittal plane in patients with hallux valgus. Foot An-kle Int. 1999;20:29-32.
33. Wanivenhaus A, Pretterklieber M. First tarsometatarsal joint: anatomical biomechanical study. Foot Ankle. 1989;9:153-7.
34. Glasoe WM, Allen MK, Yack HJ. Measurement of dorsal mobility in the first ray: elimination of fat pad compression as a variable. Foot Ankle Int. 1998;19:542-6.
35. Glasoe WM, Yack HJ, Saltzman CL. The reliability and validity of a first ray measurement device. Foot Ankle Int. 2000;21:240-6.
36. Glasoe WM, Allen MK, Saltzman CL. First ray dorsal mobility in relation to hallux valgus deformity and first intermetatarsal angle. Foot Ankle Int. 2001;22:98-101.
37. Glasoe WM, Allen MK, Saltzman CL, Ludewig PM, Sublett SH. Comparison of two methods used to assess first-ray mobility. Foot Ankle Int. 2002;23:248-52.
38. Coughlin MJ, Shurnas PS. Hallux valgus in men. Part II: first ray mobility after bunionectomy and factors associated with hallux valgus deformity. Foot Ankle Int. 2003;24:73-8.
39. Voellmicke KV, Deland JT. Technique tip: manual examination technique to assess dorsal instability of the first ray. Foot Ankle Int. 2002;23:1040-1.
40. Hardy RH, Clapham JC. Hallux valgus; predisposing anatomical causes. Lan-cet. 1952;1:1180-3.
41. Myerson M. Metatarsocuneiform arthrodesis for treatment of hallux valgus and metatarsus primus varus. Orthopedics. 1990;13:1025-31.
42. Morton DJ. Evolution of the longitudinal arch of the human foot. J Bone Joint Surg. 1924;6:56-90.
43. DiGiovanni CW, Kuo R, Tejwani N, Price R, Hansen ST Jr, Cziernecki J, San-georzan BJ. Isolated gastrocnemius tightness. J Bone Joint Surg Am. 2002;84:962-70.