Embed Size (px)
Citation preview

The Egyptian Journal of Radiology and Nuclear Medicine (2013) 44, 563–572
Egyptian Society of Radiology and Nuclear Medicine
The Egyptian Journal of Radiology andNuclearMedicine
www.elsevier.com/locate/ejrnmwww.sciencedirect.com
ORIGINAL ARTICLE
Evaluation of median nerve in children with type1
diabetes using ultrasonographic imaging and
electrophysiology
Rania Refaata,*, Abeer Maghawry Abdelhameed
a, Nancy Samir Elbarbary
b,
Rana Ahmed El-Hilaly c
a Department of Radiodiagnosis, Ain Shams University, Cairo, Egyptb Department of Pediatrics, Pediatric Endocrinology and Diabetes Unit, Ain Shams University, Cairo, Egyptc Department of Physical Medicine, Rheumatology and Rehabilitation, Ain Shams University, Cairo, Egypt
Received 12 November 2012; accepted 4 June 2013Available online 3 July 2013
*
E-
Pe
N
03
ht
KEYWORDS
Ultrasonography (US);
Nerve conduction study
(NCS);
Children type1 diabetes
(T1DM);
Cross-sectional area (CSA)
of median nerve
Corresponding author. Tel.:mail address: raniarefaat_19
er review under responsibility
uclear Medicine.
Production an
78-603X � 2013 Production
tp://dx.doi.org/10.1016/j.ejrn
+2 010077@hotm
of Egyp
d hostin
and host
m.2013.0
Abstract Background: Diabetic peripheral neuropathy (DPN) is a worldwide costly complication
of diabetes.
Objective: To evaluate the relationship between the sonographically measured cross-sectional area
(CSA) of the median nerve and nerve conduction study (NCS) in children with type1 diabetes
(T1DM) complaining of DPN.
Material and methods: Forty childrenwithT1DMand20age-matchedhealthy subjectswere enrolled
in this study.Thediabetic childrenweredivided into2groups (without andwithDPN).All participants
underwent NCS and sonographic measurement of CSA for the median nerve in the carpal tunnel.
Results: TheCSA of themedian nerve in children withDPNwas higher than that in the control subjects
yetwithnosignificantdifferencewiththatofchildrenwithoutDPN.TheincreasedmediannerveCSAinthe
carpal tunnel was considerably correlated with the median nerve motor latency and duration of diabetes,
nevertheless, with no correlation with median nerve motor conduction velocity (MNCV).
Conclusion: Sonographic measurement of CSA of the median nerve in the carpal tunnel serves as a good
discriminator for diabetic children from healthy individuals. Moreover, it has significant positive correla-
tion with duration of disease and the nerve motor latency.� 2013 Production and hosting by Elsevier B.V. on behalf of Egyptian Society of Radiology and Nuclear
Medicine.
5285089.ail.com (R. Refaat).
tian Society of Radiology and
g by Elsevier
ing by Elsevier B.V. on behalf of Egyptian Society of Radiology and Nuclear Medicine.
6.002

564 R. Refaat et al.
1. Introduction
The World Health Organization estimates that more than 220million people worldwide have diabetes mellitus (DM) (1).
Furthermore, International Diabetes Federation states 78,000children develop T1DM every year (2).
Diabetic neuropathy is recognized as the most common
clinical picture of nervous system disorders caused by DM(3) and is considered the most common type of neuropathies.It affects patients with both type1 and type2 diabetes, but itprogresses more rapidly and its manifestations are more severe
in T1DM (4). Earlier observations and population-based co-hort studies have shown that 66% of patients who haveT1DM develop some form of neuropathy (5).
For the evaluation of peripheral neuropathy (PN), physi-cians traditionally relied primarily on information gained froman accurate clinical history, a thorough physical examination
and electrodiagnostic testing with NCS (6,7). However, suchdiagnostic tests and studies do not provide spatial informationregarding the nerve and the surrounding structures (8). Ultra-
sonography (US) provides a rapid, cheap and non invasivemethod for the examination of the soft tissue structures ofthe wrist as it easily detects the median nerve which is locateddeep to the retinaculum (9).
A sophisticated search revealed a limited knowledge of dia-betic peripheral neuropathy (DPN) in children and a largelyvariable reported prevalence of PN in different studies of pedi-
atric patients with T1DM. Moreover, these children are moreprone to complications because of the early onset of diabetesand accordingly, to assure them of a better life style through
early detection and proper management of the complicationsof the PN.
Thus, our hypothesis is to demonstrate the relationship be-
tween the sonographically measured CSA of the median nervein children with T1DM complaining of DPN and the results ofNCS.
2. Materials and methods
We conducted the study on 40 eligible consecutive patientswith type1 diabetes [10 males, 30 females (mean age
15.2 ± 2.9 years; range: 7–18 years)] recruited from the regularattendants of the Pediatric Diabetes Clinic, Children’s Hospi-tal between June 2011 and January 2012. These patients were
included in the order that they showed up in the diabetes clinic.To be eligible for the study patients had to satisfy the fol-
lowing criteria: (1) children with T1DM, who are able to per-
form all neurological examinations and tests and (2) havingdiabetes for more than five years. We divided the diabetic chil-dren into 2 groups; children with and without diabetic periph-eral neuropathy (DPN). DPN was diagnosed on the basis of
sensory symptoms in the form of bilateral tingling and numb-ness which started a few months ago. Complete history takingwas performed including age, diabetes duration, complications
and insulin regimen for the 40 diabetic patients.Full clinical neurological examination was done to confirm
peripheral neuropathy if present. We adopted the simple rapid
bedside neuropathy disability score (NDS) as a screening toolfor DPN (10). The NDS was derived from the examination ofvibration perception (by means of a 128-Hz tuning fork), pin-
prick and temperature perceptions in the great toe and the
presence or absence of ankle reflexes. The sensory modalitieswere scored as either present (0) or reduced or absent (1) foreach leg. This means that ‘‘reduced’’ was scored as (1) indicat-
ing involvement of the nerve. Ankle reflexes were scored asnormal (0), present with reinforcement (1) or absent (2) foreach leg. The total maximal abnormal score was 10. A score
above 2 was defined as clinical DPN (11).Exclusion of neuropathies other than DPN was considered.
This includes the following: patients with other significant
chronic diseases (renal, liver and thyroid diseases) and othersystemic diseases that affect the central nervous system. Inaddition, history of familial neuropathy, other neurologicaldiseases, alcohol consumption, medications and exposure to
toxins (known to cause neuropathy), patients with mentalretardation or psychiatric diseases were excluded. Anthropo-metric measures; weight in kg, height in cm and body mass in-
dex (BMI); were calculated as weight in kilograms divided bysquare of height in meters, which were measured and recorded.
Other microvascular complications were screened including
diabetic retinopathy (DR) that was diagnosed by doing com-plete ocular examination and indirect ophthalmoscopy. Fur-ther urinary albumin excretion was measured by the
immuno-turbidimetric method for the detection of diabeticnephropathy. The kit used was from SERA-PAK (Bayer Cor-poration, Bendict Ave., Tarrytown, NY, USA). The result wasexpressed as albumin to creatinine ratio (ACR) in urine to
avoid diurnal variation in albumin excretion. Urinary creati-nine was estimated on Synchron C·7 (Beckman InstrumentsInc., Brea., CA, USA). Venous blood samples were obtained
in the morning from all patients after an overnight fast. A2 ml blood sample was drawn from peripheral veins undercomplete aseptic conditions. The tube was placed on EDTA
for the direct assay of HbA1c. The average of HbA1c measure-ments was determined and calculated for each patient (fourdeterminations per year) with an average length of three
months between each HbA1c measurement.For comparison, we enrolled 20 age-matched healthy sub-
jects (12 males and 8 females) with no obvious medical disor-der and not receiving any medication who served as a control
group. This group included children recruited from the sameregion as the case subjects; most were classmates or acquain-tances of the case subjects. They were age–BMI – matched
healthy individuals with a mean age of 13.9 ± 3.3 years; range:7–17 years. We studied a total of 120 upper limbs in all 60 sub-jects who underwent median NCS and sonographic measure-
ment of the median nerve CSA about 5 cm proximal to thewrist (in the carpal tunnel). These investigations were doneconcurrently in the same day.
The study protocol was approved by the Committee of Eth-
ics and the parents of all study participants; the patients andthe control subjects gave their written informed consent.
2.1. Sonographic measurement of the median nerve cross-sectional area (CSA)
Sonographic examination was performed unbiased to patient’s
history and NCS results using a Philips HD11 Revision 1.0.9imaging system with an L12-3 linear array probe and a B modereal time apparatus. The examiners had a board-certified
license and more than 10 years of experience. Patients wereseated in a chair with arms extended, hands resting in a

Fig. 1b Normal sonographic appearance of transverse scan of
the median nerve (MN) in the wrist of a child of the control group;
showing multiple hypoechoic bands corresponding to neuronal
fascicles which are separated by hyperechoic lines that correspond
to the epineurium.
Fig. 1c Normal transverse scan of the median nerve (MN) in the
wrist of a child of the control group; showing its normal elliptic
outline.
Evaluation of median nerve in children with type1 diabetes using ultrasonographic imaging and electrophysiology 565
horizontal supine position on the examination couch andfingers semiextended (12). We performed longitudinal(Fig. 1a) and transverse scans of the median nerve about
5 cm proximal to the wrist (in the carpal tunnel).We traced the median nerve through its course as follows. It
crosses superficially to the brachial artery at the mid-humerus
to lie on its medial side. The nerve enters the forearm betweenthe heads of pronator teres, the deeper of which separates itfrom the ulnar artery, while, at the wrist, the median nerve be-
comes superficial on the ulnar side of flexor carpi radialis, ex-actly in the midline (13). Accordingly, advanced sonographictechniques such as color Doppler and power Doppler imagingwere used in this study in order to identify the median nerve in
children with poor sonographic images.The normal appearance of the peripheral nerve should be
readily recognized as it consists of multiple hypoechoic bands
corresponding to neuronal fascicles, which are separated byhyperechoic lines that correspond to the epineurium(Fig. 1b) (14). The median nerve lies within the carpal tunnel
just to the radial side of the superficial row of flexor digitorumtendons. On transverse sonograms, the nerve appears elliptic inoutline (Fig. 1c) (9).
We measured median nerve CSA at the inner border of thethin hyperechoic rim of the nerve (perineurium) using the man-ual tracing technique (Fig. 1d) as according to Hammer et al.(15), this method of measurement of median nerve CSA yields
the most correct CSA. The weight of the probe was also ap-plied without additional pressure.
Fig. 1d Measurement of the median nerve (MN) CSA in the
wrist at the inner border of the thin hyperechoic rim of the nerve
(perineurium) using the manual tracing technique in a child of the
control group being 0.039 cm2.
2.2. Nerve conduction study
The nerve conduction study was performed with conventionalprocedure using the Schwarzer Topaz machine, Germany.
NCS was done on both median nerves measuring the motornerve conduction velocity (MNCV) and the motor latencyfrom the elbow to the wrist joint in a room with ambient tem-
perature of 25 �C and skin surface temperature between 31 �Cand 33 �C. The pick up (active) electrode was placed on theprominence of abductor pollicis brevis muscle. The referencewas placed on the distal phalanx of the thumb. The ground
electrode was placed between the active and the stimulator.The distal stimulation was applied 8 cm proximal to the activeelectrode and is placed between the flexor carpi radialis and
palmaris longus tendons. The proximal stimulation was ap-plied in the medial aspect of the antecubital fossa just lateralto the brachial artery.
Fig. 1a Normal sonographic appearance of longitudinal scan of
the median nerve (MN) in the wrist of a child of the control group.
2.3. Statistical analysis
SPSS statistics (V. 19.0, IBM Corp., USA, 2010) was used fordata analysis. Data were expressed as Mean ± SD for quanti-tative parametric measures and both number and percentagefor categorized data. For comparison between two indepen-
dent mean groups for parametric data, Student’s t test wasused, while, Wilcoxon Rank Sum test was used for comparisonbetween two independent groups for non-parametric data.
Additionally, Ranked Spearman’s correlation test was appliedto study the possible association between each of the two vari-ables among each group for non-parametric data. Chi-square
test was applied, as well, to study the association between eachof the two variables or comparison between two independentgroups as regards the categorized data.
The probability of error (p value) at 0.05 was consideredsignificant, while, at 0.01 and 0.001 was considered highlysignificant. To obtain the most sensitive and specific cut-offvalue for the sonographically measured CSA of the median

566 R. Refaat et al.
nerve, Diagnostic Validity Test was used and ROC wasconstructed. AUC was calculated to evaluate the most discrim-inating markers between the compared groups.
3. Results
Demographic data for the diabetic children and the control
individuals were recorded as shown in Table 1. There wereno significant differences in age, height, weight and BMI be-tween the diabetic children and the healthy subjects.
Patients with type1 diabetes were 10 males and 30 females.It is not surprising that in this series, there is a predominanceof females (75%) in T1DM cohort. It was previously reported
that unlike many other autoimmune diseases, where femalesare more at risk of disease, T1DM subgroups have a similargender distribution when diagnosed under age 15 with
T1DM. However, a minor male excess in incidence has beenreported in Europe and in populations of European originand as light female excess in populations of African or Asianorigin (16).
The included patients used human insulin in a dose rangingfrom 0.5 to 2.5 IU/kg/day with a mean of 1.8 ± 0.38 IU/kg/day; all of them were on intensive insulin therapy. 28 patients
were on preprandial injections of short-acting insulin andintermediate acting insulin (isophane NPH insulin) and 12 pa-tients were on long acting insulin analog (insulin glargine –
Aventis Pharma) at bedtime and preprandial short acting insu-lin analog. Of the 40 patients who were enrolled in the study,13 patients (32.5%) exhibited diabetic nephropathy in the formof microalbuminuria with a mean range of 90 ± 57.4 (mg/l)
and none had macroalbuminuria. 4 patients had bothnephropathy and peripheral neuropathy (10%). None of theenrolled patients had diabetic retinopathy.
By using Pearson Chi-Square test, there was a significantdifference (p = 0.024) between ratio of females to males inchildren without and with diabetic peripheral neuropathy
(DPN). Children without DPN group comprised of 14 females(70%) and 6 males (30%) and children with DPN group com-prised of 16 females (80%) and 4 males (20%), while, control
individuals comprised of 8 females (40%) and 12 males (60%).The sonographically measured CSA and the NCS results
for the diabetic children and the healthy subjects are shownin Table 2.
Comparison between control individuals versus childrenwithout DPN, control individuals versus children with DPNand children without DPN versus children with DPN concern-
ing the mean value of median nerve CSA, the mean value ofmedian nerve motor latency and the mean value of median
Table 1 Detailed demographic data of the study subjects.
Variable Control individuals
n 20
Sex, male/female 12/8
Age, y ± SD 13.9 ± 3.3
Height, cm ± SD 158 ± 6.5
Weight, kg ± SD 55.2 ± 11.2
Body mass index ± SD 20.1 ± 2.7
Duration of diabetes, y ± SD NA
NA, not applicable; SD, standard deviation.
nerve motor nerve conduction velocity (MNCV) were done.The results are summarized in Table 3 according to the valueof the probability of error (p value) to express the significance
of the difference between the compared groups.The mean median nerve CSA in the control individuals
showed statistically highly significant difference (p = 0) com-
pared to that of children without (Fig. 2) and with DPN(Fig. 3) as it was 0.043 versus 0.072 cm2 and 0.073 cm2 respec-tively. There was no statistical significance (p= 0.828) be-
tween mean median nerve CSA of children without DPNand that of children with DPN being 0.072 cm2 versus0.073 cm2.
The mean value of median nerve motor latency in the con-
trol individuals showed statistically highly significant differ-ence compared to that of children without (p= 0.001) andwith DPN (p= 0.005) as it was 2.96 ms versus 3.4 ms and
3.5 ms respectively. There was no statistical significance(p = 0.747) between the mean value of median nerve motor la-tency of children without DPN and that of children with DPN
being 3.4 ms versus 3.5 ms.The mean value of median nerve MNCV in the control
individuals showed statistically no significant difference
(p = 0.085) compared to that of children without DPN andstatistically significant difference (p = 0.016) compared to thatof children with DPN as it was 54.6 m/s versus 52.9 m/s and54.6 m/s versus 51.5 m/s respectively. There was no statistical
significance (p = 0.312) between the mean value of mediannerve MNCV of children without DPN and that of childrenwith DPN being 52.9 m/s versus 51.5 m/s.
There was a non significant difference between childrenwithout DPN (p = 0.14) and those with DPN (p= 0.549)regarding the mean value of HbA1c and duration of diabetes,
yet the values of HbA1c were higher in children with DPN.In the group of children without DPN, the mean median
nerve motor latency for both wrists had no correlation with
duration of diabetes (r= 0.327; p = 0.159) and HbA1c(r = 0.148; p = 0.534). The mean median nerve MNCV forboth wrists had no correlation with duration of diabetes(r = �0.375; p= 0.103) and a highly significant negative cor-
relation with HbA1c (r= �0.626; p = 0.003). The mean med-ian nerve CSA for both wrists had no correlation withduration of diabetes (r = �0.111; p = 0.642) and no correla-
tion with HbA1c (r= 0.399; p = 0.082).In the group of children with DPN, the mean median nerve
motor latency for both wrists had no correlation with the dura-
tion of diabetes (r= 0.163; p = 0.494) and HbA1c (r= 0;p= 1). The mean median nerve MNCV for both wrists hada highly significant negative correlation with duration of dia-
Children without DPN Children with DPN
20 20
6/14 4/16
15.9 ± 2.7 14.6 ± 3.5
162 ± 4.5 151.5 ± 8.8
63.2 ± 9.2 50.4 ± 18.8
24 ± 3.2 21.7 ± 7.2
8.6 ± 3.8 8.5 ± 3.7
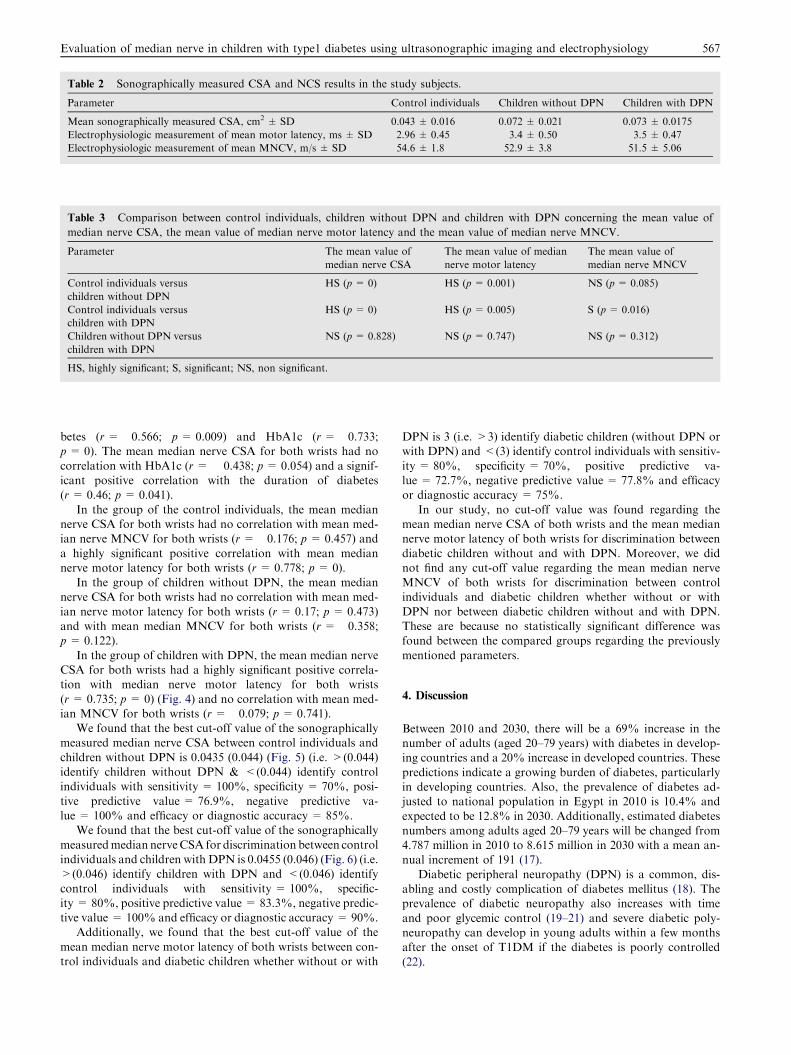
Table 2 Sonographically measured CSA and NCS results in the study subjects.
Parameter Control individuals Children without DPN Children with DPN
Mean sonographically measured CSA, cm2 ± SD 0.043 ± 0.016 0.072 ± 0.021 0.073 ± 0.0175
Electrophysiologic measurement of mean motor latency, ms ± SD 2.96 ± 0.45 3.4 ± 0.50 3.5 ± 0.47
Electrophysiologic measurement of mean MNCV, m/s ± SD 54.6 ± 1.8 52.9 ± 3.8 51.5 ± 5.06
Table 3 Comparison between control individuals, children without DPN and children with DPN concerning the mean value of
median nerve CSA, the mean value of median nerve motor latency and the mean value of median nerve MNCV.
Parameter The mean value of
median nerve CSA
The mean value of median
nerve motor latency
The mean value of
median nerve MNCV
Control individuals versus
children without DPN
HS (p= 0) HS (p = 0.001) NS (p= 0.085)
Control individuals versus
children with DPN
HS (p= 0) HS (p = 0.005) S (p= 0.016)
Children without DPN versus
children with DPN
NS (p= 0.828) NS (p = 0.747) NS (p= 0.312)
HS, highly significant; S, significant; NS, non significant.
Evaluation of median nerve in children with type1 diabetes using ultrasonographic imaging and electrophysiology 567
betes (r= �0.566; p= 0.009) and HbA1c (r= �0.733;p = 0). The mean median nerve CSA for both wrists had no
correlation with HbA1c (r= � 0.438; p= 0.054) and a signif-icant positive correlation with the duration of diabetes(r= 0.46; p = 0.041).
In the group of the control individuals, the mean mediannerve CSA for both wrists had no correlation with mean med-ian nerve MNCV for both wrists (r= �0.176; p = 0.457) and
a highly significant positive correlation with mean mediannerve motor latency for both wrists (r= 0.778; p= 0).
In the group of children without DPN, the mean mediannerve CSA for both wrists had no correlation with mean med-
ian nerve motor latency for both wrists (r= 0.17; p = 0.473)and with mean median MNCV for both wrists (r = �0.358;p = 0.122).
In the group of children with DPN, the mean median nerveCSA for both wrists had a highly significant positive correla-tion with median nerve motor latency for both wrists
(r= 0.735; p = 0) (Fig. 4) and no correlation with mean med-ian MNCV for both wrists (r= �0.079; p= 0.741).
We found that the best cut-off value of the sonographicallymeasured median nerve CSA between control individuals and
children without DPN is 0.0435 (0.044) (Fig. 5) (i.e. >(0.044)identify children without DPN & <(0.044) identify controlindividuals with sensitivity = 100%, specificity = 70%, posi-
tive predictive value = 76.9%, negative predictive va-lue = 100% and efficacy or diagnostic accuracy = 85%.
We found that the best cut-off value of the sonographically
measuredmedian nerveCSA for discrimination between controlindividuals and children with DPN is 0.0455 (0.046) (Fig. 6) (i.e.>(0.046) identify children with DPN and <(0.046) identify
control individuals with sensitivity = 100%, specific-ity = 80%, positive predictive value = 83.3%, negative predic-tive value = 100% and efficacy or diagnostic accuracy = 90%.
Additionally, we found that the best cut-off value of the
mean median nerve motor latency of both wrists between con-trol individuals and diabetic children whether without or with
DPN is 3 (i.e. >3) identify diabetic children (without DPN orwith DPN) and <(3) identify control individuals with sensitiv-
ity = 80%, specificity = 70%, positive predictive va-lue = 72.7%, negative predictive value = 77.8% and efficacyor diagnostic accuracy = 75%.
In our study, no cut-off value was found regarding themean median nerve CSA of both wrists and the mean mediannerve motor latency of both wrists for discrimination between
diabetic children without and with DPN. Moreover, we didnot find any cut-off value regarding the mean median nerveMNCV of both wrists for discrimination between controlindividuals and diabetic children whether without or with
DPN nor between diabetic children without and with DPN.These are because no statistically significant difference wasfound between the compared groups regarding the previously
mentioned parameters.
4. Discussion
Between 2010 and 2030, there will be a 69% increase in thenumber of adults (aged 20–79 years) with diabetes in develop-ing countries and a 20% increase in developed countries. These
predictions indicate a growing burden of diabetes, particularlyin developing countries. Also, the prevalence of diabetes ad-justed to national population in Egypt in 2010 is 10.4% and
expected to be 12.8% in 2030. Additionally, estimated diabetesnumbers among adults aged 20–79 years will be changed from4.787 million in 2010 to 8.615 million in 2030 with a mean an-nual increment of 191 (17).
Diabetic peripheral neuropathy (DPN) is a common, dis-abling and costly complication of diabetes mellitus (18). Theprevalence of diabetic neuropathy also increases with time
and poor glycemic control (19–21) and severe diabetic poly-neuropathy can develop in young adults within a few monthsafter the onset of T1DM if the diabetes is poorly controlled
(22).

Fig. 2 The median nerve (MN) CSA in a child without DPN: (A) Transverse scan of the median nerve in the wrist showing the neuronal
fascicles and the epineurium. (B) The sonographically measured CSA at the inner border of the perineurium using the manual tracing
technique was 0.071 cm2.
568 R. Refaat et al.
More than 80% of patients with clinical diabetic neuropa-thy have a distal symmetrical form of the disorder (23,24). Inthis neuropathic pattern, signs and symptoms start and remain
more pronounced in the feet and go on to affect more proximalparts of the lower limbs and eventually the distal parts of theupper limbs (25).
The diagnosis of diabetic neuropathy is based on its charac-teristic symptoms and can be confirmed with NCS (5,26–28).Although, NCS is generally considered to be the most sensitivefor detecting and monitoring DPN, its utilization in patients
with diabetes is low (18). This is presumably because theNCS is time-consuming, slightly invasive and generally notwell tolerated for repeated evaluations (29).
Sonographic examinations can be performed to assessperipheral nerves and have already been used for the evalua-tion of disorders of the peripheral nervous system (30–36). Ad-
vances in ultrasound technology have made it possible toachieve a good spatial resolution for clear evaluation of theperipheral nerves. Wide availability, low cost, non invasive-
ness, being painless and short examination time are the advan-tages of sonography (37). Though, US is operator dependent,it shows high reproducibility after adequate training of theoperators (38).
As sonography is a non invasive method, it can be usedfor the measurement of the nerve CSA providing importantadditional information in patients with suspected neuropa-
thy. Sonographic measurements of the nerve CSA include
two methods: the indirect method (ellipsoid formula) (CSA(mm2) = major axis · minor axis · p · l/4) and the directmethod (tracing) (36). Recently, Aleman et al. (39) reported
that sonography for median nerve CSA measurements werereproducible either by tracing or by indirect method when astandardized sonographic examination protocol was used.
We used the direct method (tracing) for the examinationand measured it about 5 cm from the wrist (in the carpaltunnel).
The mechanism of diabetic neuropathy involves the patho-
genesis of damage to the pain mechanism, which is multifacto-rial and includes metabolic disturbances such ashyperglycemia, even impaired glucose tolerance, dyslipidemia,
oxidative and nitrosative stress, growth factor deficiencies,microvascular insufficiency and autoimmune damage to nervefibers (40).
It has been also reported that abnormalities in diabetic neu-ropathy include axonal degeneration in nerve fibers and pri-mary demyelination resulting from Schwann cell dysfunction
(41). Suzuki et al. (42) reported that sorbitol itself and second-ary sodium accumulation caused by an increase in sorbitolmay have been major contributors to the increase in intracellu-lar hydration in a hydrogen 1 nuclear magnetic resonance
study. It has further been hypothesized that in individuals withdiabetes mellitus, the peripheral nerve is swollen because of in-creased water content related to increased aldose reductase
conversion of glucose to sorbitol (43).

Fig. 3 The median nerve (MN) CSA in a child with DPN: (A) Transverse scan of the median nerve in the wrist showing the neuronal
fascicles and the epineurium. (B) The sonographically measured CSA at the inner border of the perineurium using the manual tracing
technique was 0.103 cm2.
Fig. 4 Linear Regression analysis showing a highly significant
positive correlation between the mean CSA of the median nerve
and the mean median nerve motor latency among children with
DPN(r = 0.735; p= 0).
Fig. 5 ROC curve analysis showing the diagnostic performance
of the mean CSA for discriminating patients without DPN from
control individuals, AUC = 0.814.
Evaluation of median nerve in children with type1 diabetes using ultrasonographic imaging and electrophysiology 569
Although, the symptoms of DPN appear bilaterally from
the soles or feet and the wide use of NCS in the diagnosis ofDPN making NCS in the lower limbs to appear more appro-priate for assessing DPN, we performed NCS in the upper
limbs. This is because NCS in the lower limbs is lengthy andaction potentials in the lower limbs sometimes cannot beevoked in patients with advanced DPN. Moreover, Sasaki
et al. (44) and Kohara et al. (45) reported that motor nerveconduction velocity (MNCV) slowing in the upper limbs wassimilar to that in the lower limbs of diabetic patients. Also,
the skin temperature and humidity easily affect the sensorynerve conduction velocity at the time of measurement, so itis often impossible to measure (36).
Mizumoto et al. (46) chose to look at the distal motor la-tency and MNCV because the sensory nerve conduction veloc-ity was not measurable in many hands and therefore appeared
to be an unsuitable parameter. Thus, we carried out motornerve conduction studies only in the upper limbs. This is alsosustained as small myelinated and unmyelinated nerve fibers,
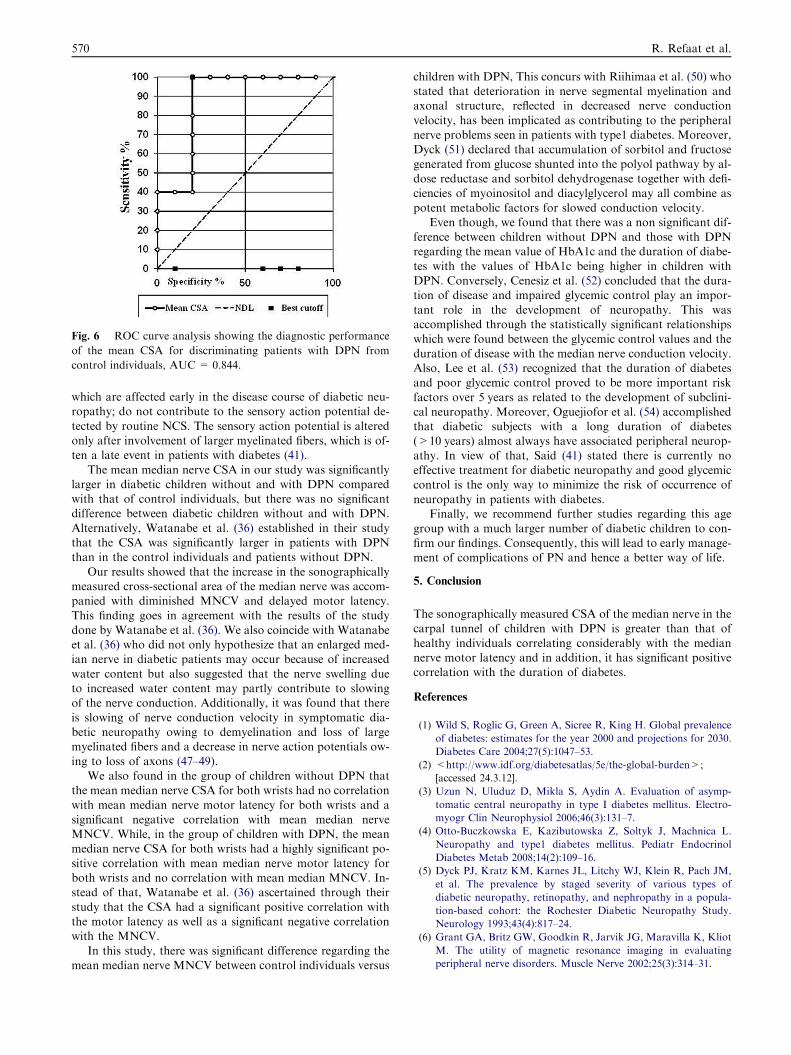
Fig. 6 ROC curve analysis showing the diagnostic performance
of the mean CSA for discriminating patients with DPN from
control individuals, AUC = 0.844.
570 R. Refaat et al.
which are affected early in the disease course of diabetic neu-ropathy; do not contribute to the sensory action potential de-
tected by routine NCS. The sensory action potential is alteredonly after involvement of larger myelinated fibers, which is of-ten a late event in patients with diabetes (41).
The mean median nerve CSA in our study was significantlylarger in diabetic children without and with DPN comparedwith that of control individuals, but there was no significantdifference between diabetic children without and with DPN.
Alternatively, Watanabe et al. (36) established in their studythat the CSA was significantly larger in patients with DPNthan in the control individuals and patients without DPN.
Our results showed that the increase in the sonographicallymeasured cross-sectional area of the median nerve was accom-panied with diminished MNCV and delayed motor latency.
This finding goes in agreement with the results of the studydone by Watanabe et al. (36). We also coincide with Watanabeet al. (36) who did not only hypothesize that an enlarged med-ian nerve in diabetic patients may occur because of increased
water content but also suggested that the nerve swelling dueto increased water content may partly contribute to slowingof the nerve conduction. Additionally, it was found that there
is slowing of nerve conduction velocity in symptomatic dia-betic neuropathy owing to demyelination and loss of largemyelinated fibers and a decrease in nerve action potentials ow-
ing to loss of axons (47–49).We also found in the group of children without DPN that
the mean median nerve CSA for both wrists had no correlation
with mean median nerve motor latency for both wrists and asignificant negative correlation with mean median nerveMNCV. While, in the group of children with DPN, the meanmedian nerve CSA for both wrists had a highly significant po-
sitive correlation with mean median nerve motor latency forboth wrists and no correlation with mean median MNCV. In-stead of that, Watanabe et al. (36) ascertained through their
study that the CSA had a significant positive correlation withthe motor latency as well as a significant negative correlationwith the MNCV.
In this study, there was significant difference regarding themean median nerve MNCV between control individuals versus
children with DPN, This concurs with Riihimaa et al. (50) whostated that deterioration in nerve segmental myelination andaxonal structure, reflected in decreased nerve conduction
velocity, has been implicated as contributing to the peripheralnerve problems seen in patients with type1 diabetes. Moreover,Dyck (51) declared that accumulation of sorbitol and fructose
generated from glucose shunted into the polyol pathway by al-dose reductase and sorbitol dehydrogenase together with defi-ciencies of myoinositol and diacylglycerol may all combine as
potent metabolic factors for slowed conduction velocity.Even though, we found that there was a non significant dif-
ference between children without DPN and those with DPNregarding the mean value of HbA1c and the duration of diabe-
tes with the values of HbA1c being higher in children withDPN. Conversely, Cenesiz et al. (52) concluded that the dura-tion of disease and impaired glycemic control play an impor-
tant role in the development of neuropathy. This wasaccomplished through the statistically significant relationshipswhich were found between the glycemic control values and the
duration of disease with the median nerve conduction velocity.Also, Lee et al. (53) recognized that the duration of diabetesand poor glycemic control proved to be more important risk
factors over 5 years as related to the development of subclini-cal neuropathy. Moreover, Oguejiofor et al. (54) accomplishedthat diabetic subjects with a long duration of diabetes(>10 years) almost always have associated peripheral neurop-
athy. In view of that, Said (41) stated there is currently noeffective treatment for diabetic neuropathy and good glycemiccontrol is the only way to minimize the risk of occurrence of
neuropathy in patients with diabetes.Finally, we recommend further studies regarding this age
group with a much larger number of diabetic children to con-
firm our findings. Consequently, this will lead to early manage-ment of complications of PN and hence a better way of life.
5. Conclusion
The sonographically measured CSA of the median nerve in thecarpal tunnel of children with DPN is greater than that of
healthy individuals correlating considerably with the mediannerve motor latency and in addition, it has significant positivecorrelation with the duration of diabetes.
References
(1) Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence
of diabetes: estimates for the year 2000 and projections for 2030.
Diabetes Care 2004;27(5):1047–53.
(2) <http://www.idf.org/diabetesatlas/5e/the-global-burden>;
[accessed 24.3.12].
(3) Uzun N, Uluduz D, Mikla S, Aydin A. Evaluation of asymp-
tomatic central neuropathy in type I diabetes mellitus. Electro-
myogr Clin Neurophysiol 2006;46(3):131–7.
(4) Otto-Buczkowska E, Kazibutowska Z, Soltyk J, Machnica L.
Neuropathy and type1 diabetes mellitus. Pediatr Endocrinol
Diabetes Metab 2008;14(2):109–16.
(5) Dyck PJ, Kratz KM, Karnes JL, Litchy WJ, Klein R, Pach JM,
et al. The prevalence by staged severity of various types of
diabetic neuropathy, retinopathy, and nephropathy in a popula-
tion-based cohort: the Rochester Diabetic Neuropathy Study.
Neurology 1993;43(4):817–24.
(6) Grant GA, Britz GW, Goodkin R, Jarvik JG, Maravilla K, Kliot
M. The utility of magnetic resonance imaging in evaluating
peripheral nerve disorders. Muscle Nerve 2002;25(3):314–31.

Evaluation of median nerve in children with type1 diabetes using ultrasonographic imaging and electrophysiology 571
(7) Wein TH, Albers JW. Electrodiagnostic approach to the patient
with suspected peripheral polyneuropathy. Neurol Clin
2002;20(2):503–26.
(8) Beltran J, Rosenberg ZS. Diagnosis of compressive and entrap-
ment neuropathies of the upper extremity: value of MR imaging.
Am J Roentgenol 1994;163(3):525–31.
(9) Lee JC, Healy JC. Normal sonographic anatomy of the wrist and
hand. Radiographics 2005;25(6):1577–90.
(10) Weintrob N, Amitay I, Lilos P, Shalitin S, Lazar L, Josefsberg Z.
Bedside neuropathy disability score compared to quantitative
sensory testing for measurement of diabetic neuropathy in
children, adolescents and young adults with type1 diabetes. J
Diabetes Complications 2007;21(1):13–9.
(11) Young MJ, Boulton AJ, MacLeod AF, Williams DR, Sonksen
PH. A multicentre study of the prevalence of diabetic peripheral
neuropathy in the United Kingdom hospital clinic population.
Diabetologia 1993;36(2):150–4.
(12) Kuo MH, Leong CP, Cheng YF, Chang HW. Static wrist
position associated with least median nerve compression: sono-
graphic evaluation. Am J Phys Med Rehabil 2001;80(4):256–60.
(13) Ellis H. Course and distribution of nerves, The Upper Limb. In:
Clinical Anatomy, A revision and applied anatomy for clinical
student. Blackwell Publishing; 2006. p. 195–6, Part 3.
(14) Watanabe T, Ito H, Sekine A, Katano Y, Nishimura T, Kato Y,
et al. Sonographic evaluation of the peripheral nerve in diabetic
patients: the relationship between nerve conduction studies, echo
intensity and cross-sectional area. J Ultrasound Med
2010;29(5):697–708.
(15) Hammer HB, Hovden IA, Haavardsholm EA, Kvien TK.
Ultrasonography shows increased cross-sectional area of the
median nerve in patients with arthritis and carpal tunnel
syndrome. Rheumatology (Oxford) 2006;45(5):584–8.
(16) Soltesz G, Patterson CC, Dahlquist G. EURODIAB Study
Group Worldwide childhood type 1 diabetes incidence – what can
we learn from epidemiology? Pediatr Diabetes 2007;8(6):6–14.
(17) Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the
prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract
2010;87(1):4–14.
(18) Vinik AI, Emley MS, Megerian JT, Gozani SN. Median and
ulnar nerve conduction measurements in patients with symptoms
of diabetic peripheral neuropathy using the NC-stat system.
Diabetes Technol Ther 2004;6(6):816–24.
(19) Pirart J. Diabetes mellitus and its degenerative complications: a
prospective study of 4400 patients observed between 1947 and
1973. Diabetes Care 1978;1(168–188):253–63.
(20) Diabetes Control and Complications Trial Research Group. The
effect of intensive treatment of diabetes on the development and
progression of long-term complications in insulin-dependent
diabetes mellitus. N Engl J Med 1993;329:977–86.
(21) Martin CL, Albers J, HermanWH, Cleary P, Waberski B, Greene
DA, et al. Neuropathy among the diabetes control and compli-
cations trial cohort 8 years after trial completion. Diabetes Care
2006;29(2):340–4.
(22) Said G, Bigo A, Ameri A, Gayno JP, Elgrably F, Chanson P,
et al. Uncommon early onset neuropathy in diabetic patients. J
Neurol 1998;245(2):61–8.
(23) Palumbo PJ, Elveback LR, Whisnant JP. Neurologic complica-
tions of diabetes mellitus: transient ischemic attack, stroke, and
peripheral neuropathy. Adv Neurol 1978;19:593–601.
(24) De Freitas, Nascimento OJM, Chimelli L, Escada TM, Nevares
MT. Diabetic neuropathy I – concept, epidemiology, classifica-
tion, clinical and electrophysiological aspects. A study of 210
cases (Portuguese). Rev Brasileira Neurol 1992;28:69–73.
(25) Said G. Progressive centripetal degeneration in polyneuropathies
(French). Rev Neurol 1981;137(10):573–88.
(26) Ozaki I, Baba M, Matsunaga M, Takebe K. Deleterious effect of
the carpal tunnel on nerve conduction in diabetic polyneuropathy.
Electromyogr Clin Neurophysiol 1998;28(6):301–6.
(27) Bae JS, Kim BJ. Subclinical diabetic neuropathy with normal
conventional electrophysiological study. J Neurol
2007;254(1):53–9.
(28) Kim WK, Kwon SH, Lee SH, Sunwoo IN. Asymptomatic
electrophysioloogic carpal tunnel syndrome in diabetics: entrap-
ment or polyneuropathy. Yonsei Med J 2000;41(1):123–7.
(29) Colak A, Kutlay M, Pekkafali Z, Saracoglu M, Demircan N,
Sims�ek H, et al. Use of sonography in carpal tunnel syndrome
surgery. A prospective study. Neurol Med Chir (Tokyo)
2007;47(3):109–15.
(30) Wiesler ER, Chloros GD, Cartwright MS, Smith BP, Rushing J,
Walker FO. The use of diagnostic ultrasound in carpal tunnel
syndrome. J Hand Surg Am 2006;31(5):726–32.
(31) Abe M. Ultrasound measurement of the median nerve for carpal
tunnel syndrome of the non-handicapped and the handicapped. J
Phys Ther Sci 2004;16:107–14.
(32) Jayaraman S, Naidich TP. The carpal tunnel: ultrasound display
of normal imaging anatomy and pathology. Neuroimaging Clin
N Am 2004;14(1):103–13.
(33) Nakamichi K, Tachibana S. Detection of median nerve enlarge-
ment for the diagnosis of idiopathic carpal tunnel syndrome:
value of multilevel assessment. J Jpn Soc Surg Hand
2003;20:69–71 [in Japanese].
(34) Duncan I, Sullivan P, Lomas F. Sonography in the diagnosis of
carpal tunnel syndrome. Am J Roentgenol 1999;173(3):681–4.
(35) Lee D, Van Holsbeeck MT, Janevski PK, Ganos DL, Ditmars
DM, Darian VB. Diagnosis of carpal tunnel syndrome. Ultra-
sound versus electromyography. Radiol Clin North Am
1999;37(4):859–72.
(36) Watanabe T, Ito H, Morita A, Uno Y, Nishimura T, Kawase H,
et al. Sonographic evaluation of the median nerve in diabetic
patients: comparison with nerve conduction studies. J Ultrasound
Med 2009;28(6):727–34.
(37) Mohammadi A, Afshar AR, Masudi S, Etemadi A. Comparison
of high resolution ultrasonography and nerve conduction study in
the diagnosis of carpal tunnel syndrome: diagnostic value of
median nerve cross-sectional area. Iran J Radiol
2009;6(3):147–52.
(38) Beekman R, Visser LH. Sonography in the diagnosis of carpal
tunnel syndrome: a critical review of the literature. Muscle Nerve
2003;27(1):26–33.
(39) Aleman L, Berna JD, Reus M, Martınez F, Domenech-Ratto G,
Campos M. Reproducibility of sonographic measurements of the
median nerve. J Ultrasound Med 2008;27(2):193–7.
(40) Vinik A. The approach to the management of the patient with
neuropathic pain. J Clin Endocrinol Metab 2010;95(11):4802–11.
(41) Said G. Diabetic neuropathy – a review. Nat Clin Pract Neurol
2007;3(6):331–40.
(42) Suzuki E, Yasuda K, Yasuda K, Miyazaki S, Takeda N, Inouye
H, et al. 1H-NMR analysis of nerve edema in the streptozotocin-
induced diabetic rat. J Lab Clin Med 1994;124(5):627–37.
(43) Lee D, Dauphinee DM. Morphological and functional changes in
the diabetic peripheral nerve: using diagnostic ultrasound and
neurosensory testing to select candidates for nerve decompres-
sion. J Am Podiatr Med Assoc 2005;95(5):433–7.
(44) Sasaki H, Nanjo K, Yamada M, Naka K, Bessho H, Kikuoka H,
et al. Diabetic neuropathy as a heterogeneous syndrome: multi-
variate analysis of clinical and neurological findings. Diabetes Res
Clin Pract 1988;4(3):215–22.
(45) Kohara N, Kimura J, Kaji R, Goto Y, Ishii J, Takiguchi M, et al.
F-wave latency serves as the most reproducible measure in nerve
conduction studies of diabetic polyneuropathy: multicentre anal-
ysis in healthy subjects and patients with diabetic polyneuropathy.
Diabetologia 2000;43(7):915–21.
(46) Mizumoto D, Hashizume H, Senda M, Nagoshi M, Inoue H.
Electrophysiological assessment of the carpal tunnel syndrome in
hemodialysis patients: formula for predicting surgical results. J
Orthop Sci 2008;8(1):8–15.

572 R. Refaat et al.
(47) Behse F, Buchthal F, Carlsen F. Nerve biopsy and conduction
studies in diabetic neuropathy. J Neurol Neurosurg Psychiatry
1977;40(11):1072–82.
(48) Mulder DW, Lambert EH, Bastron JA, Sprague RG. The
neuropathies associated with diabetes: a clinical and electromyo-
graphic study of 103 unselected diabetic patients. Neurology
1961;11(4):275–84.
(49) Daube JR. Electrophysiologic testing in diabetic neuropathy. In:
Dyck PJ, Thomas PK, Asbury AK, Winegrad AI, Porte D,
editors. Diabetic Neuropathy. Philadelphia, PA: WB Saunders;
1987. p. 162–76.
(50) Riihimaa PH, Suominen K, Tolonen U, Jantti V, Knip M,
Tapanainen P. Peripheral nerve function is increasingly impaired
during puberty in adolescents with type1 diabetes. Diabetes Care
2001;24(6):1087–92.
(51) Dyck PJ. Peripheral neuropathy: new concepts and therapy.
Neurol Clin 1992;10:3–6.
(52) Cenesiz F, Tur BS, Tezic T, Gurer Y. Nerve conduction in
children suffering insulin dependent diabetes mellitus. Indian J
Pediatr 2003;70(12):945–51.
(53) Lee S-S, Han H-S, Kim H. A 5-yr follow-up nerve conduction
study for the detection of subclinical diabetic neuropathy in
children with newly diagnosed insulin-dependent diabetes melli-
tus. Pediatric Diabetes 2010;11(8):521–8.
(54) Oguejiofor OC, Odenigbo CU, Oguejiofor CB. Evaluation of the
effect of duration of diabetes mellitus on peripheral neuropathy
using the United Kingdom screening test scoring system, bio-
thesiometry and aesthesiometry. Niger J Clin Pract
2010;13(3):240–7.