Embed Size (px)
DESCRIPTION
General introduction to electrophysiology concepts and procedures.
Citation preview

Introduction to ELECTROPHYSIOLOGY
What Are They DOING Over There?!

Basic Principles
Electrophysiology: the study of electrical activity in the body
Three main activities in the EP lab:◦EP Studies◦Device Implants◦Catheter Ablation

Basic Principles
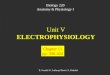
Anatomy of the Cardiac Electrical System
◦SA Node◦AV Node◦His Bundle◦Bundle Branches◦Purkinje Fibers
*Remember: The heart has several levels of backup pacing in place.

Basic Principles

Basic Principles
Normal path of conduction
SA Node AV Node His Bundle Bundle Branches Purkinje Fibers
Start the Heart Animation.url

Basic Principles
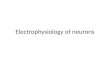
Cardiac Action Potential

Basic Principles
Cardiac Action Potential

Basic Principles
Abnormal Heart Rhythms
◦Bradycardia Failure to generate impulse Failure to propagate impulse
◦Tachycardia Automatic- seen in acutely ill patients Reentry Circuits- most common (SVTs, VT) Triggered

Basic Principles
Treatment of Arrhythmias
Drug Therapy
◦Class I through 5 Antiarrhythmics◦Watch out for proarrhythmia!◦Drug toxicity
***Only use antiarrhythmic drugs for patients with significant symptoms or life threatening arrhythmias.

Basic Principles
Non-pharmacologic Therapies
◦Reverse underlying cause Example: hypokalemia
◦Surgery PCI/CAB for ischemia
◦Devices Pacemaker for bradycardia
◦Ablation Can cure certain tachycardias

EP Studies
INTRODUCTION TO EP STUDIES
An EP study is performed by doing two things:
◦Recording
◦Pacing
That’s it! Diagnosis depends on speed of conduction through the system, direction of impulses, and any
arrhythmias induced.

EP Studies
Indications for EP Study
◦Syncope◦Palpitations◦Documented tachycardia◦Suspected SA or AV node disease◦Risk assessment for Sudden Cardiac Death
(SCD)

EP Studies
Electrode Catheters
◦Can use femoral, subclavian, or IJ access
◦Typically use 5.5 and 6 French sheaths for diagnostic studies
◦Similar to temporary pacing catheters, but with more electrodes near the tip
◦Different shapes for different areas of the heart

EP Studies

EP Studies
Electrode Catheters
◦A basic study will use two.
◦More complex studies (SVT studies) will use more.
***Multiple catheters in multiple locations can track the speed and direction of electrical impulses across the heart.

EP Studies
ECG versus EGM◦Surface ECG is a total of all the electrical
activity across the heart
◦EGM = Intracardiac Electrogram Records only the activity of a localized area, i.e.
between electrodes on the catheters
Faster sweep speed used (typically 100mm/sec)

EP Studies
Intracardiac Electrograms (EGMs)

EP Studies
Intracardiac Electrograms
These deflections represent rapid myocardial depolarization only.
Therefore, we do not see the slower conduction through the SA and AV nodes. Remember the different action potentials of
muscles cells versus nodal cells.

EP Studies
By manipulating the electrode catheters, pacing can be performed from virtually any area of the heart.
◦Premature impulses are delivered by the EP MD with precise timing and patterns.
This is called Programmed Stimulation. A stimulator computer program is used to create
the patterns for pacing.

EP Studies
Programmed stimulation can be used to:
◦Measure SA node and AV node function
◦Measure refractory periods of nodes and myocardium
◦Induce and terminate Ventricular Tachycardia
This can determine which patients receive an ICD implant.

Evaluation of SA Node
Sa Node = Pacemaker of the Heart
◦Comma- shaped
◦Located near SVC
◦Has sympathetic (“fight”) and parasympathetic (“flight”) innervation
*SA Node disease is the most common cause of bradycardia.

Evaluation of SA Node
Types of SA Node Disease:
◦Intermittent or sustained bradycardia
◦Sudden SA Node arrest
◦Periods of bradycardia with tachycardia Brady-Tachy Syndrome
*If significant symptoms are present, these conditions are termed Sick Sinus Syndrome.

Evaluation of SA Node
Symptoms of SA Node Disease
◦Lightheadedness
◦Dizziness
◦Presyncope
◦Syncope

Evaluation of SA Node
Causes of SA Node Disease:
◦Fibrosis
◦SA Nodal artery disease
◦Cardiac Trauma
◦Cardiac inflammatory/infiltrative disease
◦Thyroid disorders

Evaluation of SA Node
Measurement of SA Node Function in EP Lab
◦Sinus node recovery time (SNRT) Based on overdrive suppression
◦Sino-atrial conduction time (SACT) Exit block

Evaluation of AV Node
AV Node = Rate Regulator of the Heart
◦Located on interatrial septum, near TV
◦Has mostly parasympathetic innervation
*AV Node disease is the second major cause of bradycardia.

Evaluation of AV Node
The major question with AV Node disease is: “Does the patient need a pacemaker?”
◦This depends on:
Symptoms
Site of conduction block
Degree of conduction block

Evaluation of AV Node
Symptoms are the same as SA Node disease:
◦Lightheadedness
◦Dizziness
◦Presyncope
◦Syncope

Evaluation of AV Node
Site of AV Block:
General Rule:
Block located in AV Node = no PPM
Block located below AV Node = PPM

Evaluation of AV Node
Degree of AV Block
General Rule:
If 1st Degree = no PPM
If 2nd Degree = maybe PPM
If 3rd Degree = PPM

HIS Bundle
His Bundle = Conductor to Ventricles
◦Compact bundle of Purkinje fibers arising after AV node
◦Rapid conduction through the fibrous AV skeleton
◦Divides into Right and Left Bundle branches
◦If patient has disease in His Bundle, a PPM may be indicated.

Bundle Branches
Bundle Branches = Coordinators of Ventricular Contraction
◦Left Bundle Branch divides into two: anterior and posterior
All end as Purkinje fibers, which rapidly spread the impulse to all ventricular muscle◦Order of contraction: septum apex lateral
walls base

Bundle Branches
Any delay in impulse conduction in or below the bundle branches = Interventricular Conduction Delay (ICVD)◦Can disrupt normal ventricular contraction
ICVD leads to wide QRS on surface ECG
If delay is significant and leads to heart failure, Cardiac Resynchronization Therapy (CRT) may be indicated.

Bundle Branches
Take Note:
◦If performing a right heart cath on a patient, be prepared if they have existing LBBB:
Swan catheters may hit the Right Bundle Branch, causing Right Bundle Branch Block.
Patient would then have complete heart block and need a temporary pacing wire.

Device Therapy
Three kinds of implants in the EP Lab:
◦Permanent pacemakers (PPM)
◦Implantable Cardioverter-Defibrillators (ICDs)
◦Cardiac Resynchronization Therapy (CRT) devices

Device Therapy
Implanted Devices
◦Most are implanted in the pectoral region
◦Can have one, two, or three leads
◦Can be programmed in a variety of ways, to suit each individual patient

Device Therapy
Permanent Pacemakers
◦Indications for use include:
Symptomatic Sinus Bradycardia AV Conduction Disease Cardioneurogenic Syncope Bradycardia-induced VT Significant Ventricular Dysfunction with wide QRS

Device Therapy
Parts of a Pacemaker
◦Generator- contains the circuitry, computer memory, and battery Typical PPM weighs about an ounce (10cc)
◦Leads- usually inserted through venous system to heart Can be active (screwed into heart muscle) or
passive (distal tines catch onto heart tissue)

Temporary Pacers◦Settings:
Rate
mA (current flow)
Sensitivity: more sensitivity = less pacing less sensitivity = more pacing
asynchronous = pacing regardless of what heart is doing

Device Therapy
Implantable Cardioverter-Defibrillators
◦Indications for use include:
Sustained VT/VF EF < or equal to 35%, Class II/III HF Prior MI with EF < or equal to 30%, Class I HF EF < 40, NSVT, inducible VT
Every 3 minutes someone dies from SCA in the USA.

Device Therapy
Parts of an ICD
◦Generator weighs more that PPM, due to addition of a capacitor Weighs about 3 ounces (36cc) Capacitor stores energy needed for shocks
◦RV lead is designed to deliver shocks to convert VT/VF- looks different from a PPM lead under fluoro

Device Therapy
Cardiac Resynchronization Therapy
◦Indications for use include: Class III/IV heart failure Dilated or ischemic cardiomyopathy QRS interval > or equal to 120ms EF < or equal to 35%
Vast majority of patients fitting this criteria also qualify for ICD therapy.
CRT can improve EF up to 10-15%.

Device Therapy
Parts of a CRT device
◦Generator weighs about
◦Requires placement of an LV lead in coronary sinus Successful transvenous placement in ~95% of
patients Other 5% would need surgical placement

Cardiac Ablation
Ablation: destruction of arrhythmia- causing heart tissue
◦Can be curative, eliminating need for antiarrhytmic drugs or surgery
◦Success rates vary according to arrhythmia, with some over 90%.
◦Major complications occur in about 3% of patients.

Cardiac Ablation
How it works:◦Ablation catheter is inserted (usually through
femoral vein) to heart, along with electrode catheters for recording.
◦Electrical activity is recorded, and abnormal rhythms are tracked.
◦Ablation catheter is placed at area of arrhythmia, and energy is applied to destroy tissue.
◦Pt is monitored for any further signs of arrhythmia before leaving EP lab.

Cardiac Ablation
Indications for Catheter Ablation:
◦Symptomatic SVT due to AVNRT, WPW, unifocal atrial tachycardia, and atrial flutter.
◦Atrial fib with lifestyle-limiting symptoms, after inefficacy/intolerance of at least one antiarrhythmic drug.
◦Symptomatic VT.

Cardiac Ablation
Energy Sources:◦Direct current: in the early days, the ablation
catheter was connected to an external defibrillator Greater than 250J could be delivered inside the
heart, heating catheter tip to thousands of degrees Celsius
Blood was instantly vaporized, causing rise in pressure and flash of light
Created lesions up to 4cm2, with ragged edges Only used to ablate His bundle, with 85% success
rate (complications were suprisingly low).

Cardiac Ablation
Radiofrequency (RF) energy:
◦Most commonly used ◦Same as bovie machines in OR◦Much lower voltage than direct current- no
explosions◦Creates smaller, discrete lesions◦No muscle or nerve stimulation- no general
anesthesia needed

Cardiac Ablation
Complications of Ablation:
◦Complete heart block◦Cardiac perforation and tamponade◦Creating MR/TR◦Embolism/stroke◦Pulmonary vein stenosis◦Coronary artery lesions

Current challenges in EP:
◦Atrial Fib ablation- making it safer and more effective, with less procedure time
◦Optimizing CRT therapy◦Getting ICD therapy to more patients who
qualify

References
R. Fogoros. Electrophysiologic Testing, 4th ed.
Medtronic.comStiffler, J. The Diagnostic EP Study.
Healthworks www.skillstat.comEllenbogen and Wood. Cardiac Pacing &
ICDs, 5th ed.Eprewards.com