Embed Size (px)
Citation preview

Evaluation of Left Ventricular Enlargement as a Marker of Early Disease
in Familial Dilated Cardiomyopathy
Running title: Fatkin et al.; Early Disease in Familial Dilated Cardiomyopathy
Diane Fatkin, MD1,3,4; Thomas Yeoh, MB BS, PhD1; Christopher S. Hayward, MD3,4;
Victoria Benson, MSc2; Angela Sheu, MB BS1; Zara Richmond, BSc, Grad Dip Gen Couns1;
Michael P. Feneley, MD2,3,4; Anne M. Keogh, MD2,3,4; Peter S. Macdonald, MB BS, PhD2,4
1Molecular Cardiology Division, 2Cardiac Physiology and Transplantation Division, Victor
Chang Cardiac Research Institute; 3Cardiology Department, St Vincent’s Hospital; and 4Faculty of Medicine, University of New South Wales, Sydney, New South Wales, Australia.
Corresponding author:
Diane Fatkin, MD
Victor Chang Cardiac Research Institute,
Lowy Packer Building, 405 Liverpool St,
PO Box 699, Darlinghurst NSW 2010
Australia
Phone: 61-2-9295 8618
Fax: 61-2-9295 8601
Email: [email protected]
Journal Subject Codes: [89] Genetics of cardiovascular disease
MMMMMMMMMMMMMMMMMMMMMMMacacacacaccacacacacacacaccacacacacacacaaaa dodododododododododododododododododododododddoddd nanananananananaanananananananaannannnnaldldldldldldldldldldldldldldldlddldldlldddldd, , ,,,,,,,,, MBMBMBMBMBMBMBMBMBMMBMBMBMBMBMBMBMBMBBMBM
i
R a
c e
ioooololololology Divivivivivisisisisisioioioon,n,n,n,n, 2CaCaCaCaCardrdrdrdrdiaiaiaiaac ccc PhPhPhysysysyy iolologyyyyy a aa aandnnndn TTTTTrarararaansnsnsnsnsplpp ananananantatatatatatititititionnonnon D DD DDivivivivivis
Reesesesesesearaaa ch IIIIInssnsnn tiituuteee; 3CaCaCaCaCardddddioioioiiolololoologygygygygy Depepararararartmtttmtmeeentt,t SSt ViVV ncncncncncent’t’tt ss sss HoHH spspspita
cine, Universrsrsrrsititititity y y yy ofofofofof N N NNNewewewewew S S S SSouououououttttth hh hh WaWaWaWaaleleleleles,sss SSSSSydydydydydneneneneney,y,y,y,y, N N NNNewewewewew S outh Walettt
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
2
Abstract:
Background – Echocardiographic screening of families with dilated cardiomyopathy (DCM)
has identified a subgroup of asymptomatic relatives with left ventricular enlargement (LVE).
The prognostic significance of LVE in this setting is incompletely understood.
Methods and Results - We evaluated 457 asymptomatic relatives in 128 DCM families and
identified 110 individuals (24%) with LVE. Serial echocardiograms in 72 untreated LVE
relatives showed that 9 individuals (13%) developed DCM over 10 to 152 months (median
52). Thirty LVE relatives and 30 age- and sex-matched healthy control subjects were
evaluated using 2-dimensional and M-mode echocardiography, tissue Doppler imaging, non-
invasive pressure-volume assessment, exercise stress echocardiography, and brain natriuretic
peptide levels. LVE relatives showed mild defects of systolic and diastolic left ventricular
function with normal filling pressures and exercise-induced increments in systolic contraction
in most cases. Left ventricular dimensions and fractional shortening most effectively
differentiated LVE relatives from controls, with other functional indices lacking additive
discriminative value. In a receiver operating characteristics analysis, the area under the curve
for left ventricular end-diastolic diameter (LVEDD, %predicted) was 0.96 (P<0.001).
LVEDD (%predicted) >116%, or LVEDD (%predicted) 112-116% + fractional shortening
<29% had high sensitivity (100%) and specificity (93%) for LVE relatives and identified 8 of
9 progressors.
Conclusions –LVE is a common finding in asymptomatic relatives in DCM families and can
be a marker of pre-clinical cardiomyopathy. Assessment of left ventricular size and
contractile function is required for differentiating between pathological and physiological
causes of LVE and may help to identify those at risk of disease progression.
Key words: dilated cardiomyopathy, echocardiography, diagnosis, early disease.
ogogogogogogogogoggogogoogogogggogoggoggrararararaararrararararararararaarr phphphphphphphphphphphphphphphphphphphphhphphhpp y,y,y,y,y,y,y,y,y,y,y,y,y,yyy,y,yyyyyy,y a a aaaa aaa a aaa aaaaaandndndndndndndndndndnnndndndndnnnnd b bbbbbbbbbbbbbbbbbbrarararararararararrararararararararrrar iiiiiiiiiiiii
nd diiiasasasasasasasasasasasasasasasasasaasasstototototototototototototototototottot lilililiilililiililiiliiliilililiiiccccccccccccccccccccc leleleleleleleleleleleleleleleleleftftftftfftftftftftftftftfftftftftftfttftft vvvvvey
r i
eft ns v
V
y
rmmmmaaala fillingggg p preeeeessssssururururureseseseses aaa aandndndndnd eeexeeeeerccisee-indndndndnducucucucucededededed iiiincncncccrerererr memememementntntntnts s ss s ininininin s s sssysysysysystotototooli
eft veeeeentntntttririririricuulalalll rr diddidd mmem nsnssssioioioons aaaaandndnddnd ff ffrara ttctctioioioonanananan ll lll shshshshhororororortteteet niniiiinnngn mmmost tt efeffffefeffef tcttcttiv
VEVVEE rr relelatatativivvvveseses f f frororom m m cococontntntntrororolslsls, , , , , wiwiwiw thththtt o o othththererer f ffunununu ctctctc ioioioonananan l l ll inininndidididicececec s ss lalall ckckininggg
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
3
Dilated cardiomyopathy (DCM) is a common cause of heart failure and a significant health
and economic burden. There is increasing evidence of a substantial heritable component to
DCM and at least 20-35% individuals with “idiopathic” DCM have familial disease.1,2 Nearly
40 chromosomal loci and disease genes have been identified to date.3 Pre-symptomatic
diagnosis of early disease provides an opportunity for preventative intervention but reliable
methods for detection of individuals at risk are required. Ideally, family genotyping would
enable genotype-positive individuals to be identified before the onset of symptoms. Because
of the costs and time involved in screening large numbers of genes and the low yield (<30%)
of finding mutations, genotype results are not available for most families. Hence, assessment
of the clinical phenotype remains a cornerstone of family management.
Systematic echocardiographic screening of asymptomatic relatives in DCM families
has identified a subgroup of individuals who have abnormalities of left ventricular (LV) size
or function that do not fulfill criteria for DCM.4-8 Isolated LV enlargement (LVE) has been
observed most frequently with a lesser number of individuals having normal LV size and
depressed fractional shortening (dFS). It has been proposed that these echocardiographic
changes represent pre-clinical stages of disease. At least one third of cases do have latent
cardiomyopathy, indicated by myocardial histological changes, reduced maximal exercise
oxygen consumption, or cardiac autoantibodies.5,9-12 However, LVE may also result from
unrelated pathologies or physiological variation, particularly in young, fit individuals
engaged in competitive sporting activity. Differentiating family members with true early
DCM from those with “athlete’s heart” poses a major challenge with significant management
implications.
The major objective of this study was to evaluate the natural history of LVE and the
role of various indices for assessment of myocardial function. We used diagnostic techniques
that have been proposed to be more sensitive or specific indicators of LV functional defects
gegegegegegegegegeegegeggegegeeegeegegemememememememememememeemememememememeemementntntnntntntnntntntntnntnnntnntnn . ... ......
c relllllllllllllllllatataatatatatatatatatatattatatatataattiviiviiviviviviviviviiviviviviviviviviveseseseseeseseseseseseseseesessesseess iiiiiiiiiiiiiiiiinnnnnnnnnnnnnnnnn DCDDDDDDDDDDDDDDDDDDDDDDg p g y p
u a
d E
e
g p g y p
ubububbubggrgg oup ofofofoff i i ii dndndddivivivivividididididuauauauaualslslssls w ww wwhohohhoh hhhhhaavee aabnbnbnnnororororormammamam liiliititiitieseseseses of f f ff leleleleleftftftftft v v v v venenenentrtrtrtrtriciciciciculuuuu a
do nooooott t fufufufufullflll ililililill l crcrcrritiitii erererria fffffororororo DCMCMCMCMCM.4-84-84-84-84 IIIsososolalallalatetetetetedddd d LVLVLVLVLV eeeenllnlllaaara gegegemmmentntnt ( (((LVLVLVLVLVEEE
eqeeqequeueuentntntlylyyyy w w wititiith h h h a aa leleessssssserererer n n numumumummbebebeerrrr ooof f ff inininndididivivivvidududuualala s s s hahahaavivivv ngngnggg n n nnororormamamall LVLVVLV rrr
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

4
than standard assessment by 2-dimensional and M-mode echocardiography, including tissue
Doppler imaging,13 non-invasive determination of the preload recruitable stroke work
(PRSW) relationship,14-16 exercise stress echocardiography,17 and plasma levels of brain
natriuretic peptide (BNP).18 Our data confirm the prognostic significance of LVE as a marker
of early disease in familial DCM and suggest a practical approach to the investigation of
asymptomatic family members.
Materials and methods
Subjects
Probands from 128 kindreds with suspected familial DCM were identified from St Vincent’s
Hospital and by physician referral (Table 1). Family members aged >16 years were invited to
undergo clinical evaluation, 12-lead electrocardiography and transthoracic echocardiography.
M-mode echocardiographic dimensions were corrected for age and body surface area
according to Henry’s formula,19 with LV end-diastolic diameter (LVEDD) expressed as a
percentage of predicted diameter as follows: predicted LVEDD = (45.3 x body surface
area0.3) - (0.03 x age) - 7.2. DCM was defined as LVEDD (%predicted) >112% and LV
fractional shortening (LVFS) < 25%. Familial DCM was defined as DCM in 2 or more first-
degree relatives that was unexplained by other inherited cardiac or systemic disorders. In
asymptomatic relatives, LVE was defined as LVEDD (% predicted) >112%, and dFS was
defined as LVFS <25% .5,8,12 A group of 30 healthy volunteers who had no history of
cardiovascular disease comprised a control group. All subjects provided informed written
consent and protocols were approved by the institutional Human Research Ethics Committee.
Longitudinal observational study
identntntntnttntntntntntntntntntntntntttifififififififififififffififififififififffieieieieieieieieieieieieieieieeieiei ddddddddddddddddddddddd frfrfrfrfrfrfrfrfrfrfrfrfrfrffrfrfromomomomomomomomomomomomomomomomomomoom Sp
p ician . e
e c
d
p
phhhhhyysyy ician rererereefefff rrrrrrrrrralalalalal (((((TaTaTaTaTablblblblbleeee e 1)1)1)1)1 . FaFaFaFF miilly mmmmmemememmmbebebbb rsrsrs aaaaaggged ddd d >1>1>1>1>16 6 6 6 6 yeyeyeyeararararars ssss wwweww
evalululululuatatatatatioioiioion,n 1112-222 lleleadaa eeeeeleleeleectrooocacacacaarrrrrdidididd ogogograraphphphphphy yy y y aaanaa dddd d tttrrtrananstss hohohohh rararaciiicc ececchohhhhoc
didiogogograraraphphhhhicicici d ddimimimmenenensisisis onononons s s weweweweererere c c ccorororrererectctctedededd f f forororr a a a gegegegeg a a andndndnd b bbbododoody y y yy ssusurfrfacacace eee
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

5
Relatives were followed with serial echocardiograms. For relatives who had been screened
prior to study recruitment, the follow-up period was taken from the first available
echocardiogram. The duration of follow-up was determined as the time to disease
progression, or commencement of treatment for DCM prophylaxis, or the most recent
echocardiogram. Disease progression was defined by a new onset of contractile dysfunction
(LVFS <25%) or worsening of contractile dysfunction (if baseline LVFS <25%).
Phenotype assessment
Transthoracic echocardiography was performed according to American Society for
Echocardiography guidelines. In addition to LVEDD (%predicted) >112%, two alternative
methods for assessment of LV size were evaluated. LV dilatation was defined by LVEDD
greater than 2.7 cm / body surface area (expressed as m2) (NHLBI standard)20, or LVEDD
above height- and sex-adjusted 95th and 97.5th percentile limits (Framingham standard).21
Peak velocity of early (E) and late (A) diastolic filling, and isovolumic contraction and
relaxation times were measured from mitral inflow velocities, while ejection time was
measured from LV outflow velocity tracings. The myocardial performance index (MPI)
index was derived using the isovolumic contraction, isovolumic relaxation and ejection
times.22 Systolic (S), early (E') and late (A') diastolic myocardial tissue Doppler velocities
were recorded at the septal and lateral margins of the mitral annulus. The PRSW relationship
was determined from non-invasive peripheral arterial pressure waveforms and
echocardiographically-derived on-line LV volume23 using the linear regression equation:
stroke work=MW (end-diastolic volume -VW), where MW is the slope and VW is the volume
axis intercept.14-16 Data were obtained at rest and with variable preload induced by the
Valsalva manoeuvre. Exercise stress echocardiography was performed using the Bruce
protocol. LV end-diastolic and end-systolic areas were measured in the short-axis view at rest
eeeeeeeeeeeeeeeeed)d)d)d)d)d)d)d)d)dd)d)d)dddd)d)d)d)d)) >>>>> >>>>>>>>>>>>>>>>>1111111111111111111111111111111111111111 2%2%2%2%2%2%2%2%22%%2%2%2%2%2%%%2%%%%%, , ,,, , , ,,,,,,,,,,, twtwtwwwtwtwwtwtwwwtwwtwtwtwwwwooo o o o o ooooooo oooooo aaaaaaaaaaaaa
n waaaaaaaaaaaaaaaaasssssssssssssssss deddededededdedededdedededededededededddefififififififififififififififififififififiifinenneneneneneneneneenenenenennnennn dddddddddddddddddddddd bybbbbbbbbbbbby
c r
d n
e o
y
cmmm mm / body ssssururuuu fafafafafacececeee aa aaarererererea (e(e(e(e(expxpxpresssssss edd as mmmmm22222))) )) (N(N(N(N(NHLHLHLHLHLBIBBB ssssstatatattandndndndndarararard)d)d)d)d)202020202 , or
d sexxxxx-adadadadadjjjujj ststt dededed 99955555th andndndndnd 97.777 555ththththth ppperercecentntntnttilililille e lilililil mimimimimitttststs ( ( (FFrFrFFrammmininini ghhhhhamamm s sttattat n
eeeearararlyly ( (E)E)))) a a andndndn l l llatatateee (A(A(A(A(A) ) ) dididid asasasasstototolilililic c c fifififillllllinininng,g,g,, a a aandndndn i i sososoovovovolululuumimimmiic c c c cococontntntrararactctctioioo
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

6
and immediately following peak exercise. NT-pro BNP levels were measured in plasma
samples by electrochemiluminescence using the Elecsys II proBNP immunoassay (Roche
Diagnostics).
Statistical analysis
Differences between progressors and non-progressors, and between LVE cases and controls,
were evaluated using maximum likelihood repeated measures linear or logistic regression,
accounting for the clustering within families (Stata 10, StataCorp LP, Texas, TX). The
clustering within families was modeled using a random effect that was assumed to be
independent and identically normally distributed with mean zero and constant variance.
Receiver operating characteristic (ROC) analysis was performed using PASW Statistics 18
(IBM Corp., Somers, NY). A two-tail P value < 0.05 was considered statistically significant.
Data are reported as mean ± SD.
Results
Prevalence and outcome of asymptomatic echocardiographic changes
Four hundred fifty-seven asymptomatic relatives from 128 DCM families were evaluated
(Figure 1, Table 1). Eighteen relatives (4%) had unsuspected DCM and were commenced on
treatment. One hundred-fifteen relatives (25%) from 54 families had echocardiographic
changes, with LVE in 110 relatives and dFS in 5 relatives. One hundred-five relatives (100
LVE, 5 dFS) were followed prospectively over 10 to 202 months (median 55) with 16
individuals (15%; 15 LVE, 1 dFS) developing DCM. Seventy-four relatives (72 LVE, 2 dFS)
had serial echocardiograms available during periods in which they received no cardiovascular
medications. Thirty-seven individuals (LVE 34, dFS 3) were on treatment for some or all of
o o o oo oo o oo o o o oooo ananananananananananananananananananaand ddddddddd dddddddddddd cococococococococoococococoocococoocooconsnsnsnsnsnsnsnsnnsnsnsnsnsnsnnsssssstatatatatatatatatataatatatataatattat ntntttntntnttntntnttntnnnnt vv v vvvv vvv vvvvvvvvvvaaaaaaaaaaaaaaaa
d usiiiiiiiiingngngngngngngngngngngngngngngngngngngngg PPPPPPPPPPPPPPPPPPPPASASASASASASASASASASASASASASASASAASASASAASASASWWWWWWWWWWWWWWWWWWWWWWWW StSSSSSSg ( ) y p g
m , NY y
d
g ( ) y p g
meeeersrsrr , NY).))) AAAAA ttwowowowowo-t-t-t-t-taiaiaiaiail llll P P P PP vavavavavalululue << 0.005 wwwwwasasasasas c c cononnsisisisidedededd reeeeed d ddd stststststatatataatisiisisistititititicacacacacallllll y
d as mmmmmeaeaeaeaean ± ±±± SDSDSDSDD.
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

7
the follow-up period, including 6 LVE relatives who crossed over from the no-treatment
group.
Natural history of LVE
The natural history of LVE was further evaluated in the subgroup of 72 relatives who were
followed in the absence of treatment (“natural history” cohort, Figure 1). Nine relatives
(13%) showed disease progression over follow-up periods ranging from 10 to 152 months
(median 52), including one 17 year-old male who developed DCM requiring heart
transplantation. Baseline clinical and echocardiographic parameters were compared between
those who progressed and those who did not (Table 2). “Progressors” were relatively younger
than “non-progressors”, however the mean age at DCM diagnosis in family members of
progressors (42 ± 16 years, n=37) was similar to the study probands overall (Table 1). Our
findings are in keeping with recent data suggesting that screening of asymptomatic family
members can identify at-risk individuals at an earlier stage of disease. 24 There were no
differences in mean values for LVEDD, LVEDD (%predicted) or LVESD at study entry
between progressors and non-progressors.
Assessment of LV dilation
Previous studies of early disease have focussed on individuals with and without LVE within
families and the extent to which similar changes might be present in healthy control subjects
has not been considered. To better characterise the LVE phenotype, we studied 30
consecutive LVE relatives who agreed to undergo further more detailed echo evaluation and
30 age- and sex-matched control subjects. None of these LVE relatives was a progressor. By
design, all LVE subjects had LVEDD (%predicted) >112%, but unexpectedly, 11 of 30
healthy controls also fell within this range. A higher cut-off, >118%, proposed by Baig and
ssosososososososososososossosososososososorsrsrsrsrsrsrsrsrsrsrsrsrsrsrssrsrsrssr ” weweweweweweweweeweweweweweweeewwwwwwww rererererererererererererereerererrere rrrrr rr r r rrrelelelelelelelelelellelleleelelelatatatatatatatatatatatatatataatatataaata iiiiiiiiiiiiiiii
is innnnnnnnnnnnnnn fffffffffffffffffffffffamamamamamamamamamamamamamamamamamamaa ilililiilililililililililililililillilililyyyyyyyyyyyyyyyyyyyy mmememememmememememmmememememmemm m, g g y
± b
e t
n w
, g g y
± 1616666 years, n=n=nnn 3737373737) ) ) )) wawawawawassss s sisisisisimimimimm lalallar to tthhe ssssstututututudydydydydy pprororobababababandndnddds ss ss ovvvvverereereralallalall l l ll (T(T(T(T(Tabaaa
eepininininingg g wiwwww thhhhh r reececceenennt dadadadaatatataaa sugggggggegeg ssssstitittit ngngng tt thahahhahatttt t scscscscscreeeeenenenenenininini g g g g offfff aa asssympmpttototomamat
nnnntitifyfy aa at-t-t-ririririr sksksksk i i indndndndiviviividididi uauauaualslslsls a a aat t t t t ananan e e earararlililiererer s s statatatagegegegeg o o o f f f ff dididiseseseasasase.e.e.e 24 T T Thehererere w ww w
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

8
colleagues5 had greater stringency, identifying 23 LVE relatives and 2 controls. In a ROC
analysis, the area under the curve (AUC) for LVEDD (% predicted) was 0.96 (P<0.001,
Figure 2). LVEDD (% predicted) >116% gave the highest sensitivity (0.93) and specificity
(0.93) and was found in 28 relatives and 2 controls.
We compared LVEDD (% predicted) with two alternative methods for normalization
of LV size.20,21 The NHLBI standard identified 21 LVE relatives and 13 control subjects,
while the Framingham standard identified 24 LVE relatives and 2 controls at the 95th
percentile and 19 LVE relatives and 1 control at the 97.5th percentile. The AUC for the
NHLBI and Framingham 95th percentile standards were 0.75 (P=0.001) and 0.95 (P<0.001),
respectively (Figure 2). These data indicate that LVEDD (% predicted) and the Framingham
standards are superior to the NHBLI standard and have similar efficacy overall. Of the
criteria evaluated, LVEDD (% predicted) >116% most effectively differentiated family
members and controls.
Comparison of LV function in LVE relatives and control subjects
To determine whether pre-clinical defects of myocardial function are present in LVE
relatives, a range of parameters were evaluated and compared with control subjects (Table 3).
At rest, LVE relatives had increased end-diastolic and end-systolic LV dimensions and lower
LVFS, as well as lower peak E wave velocities, lower peak and longer time to peak S wave
velocities, and higher MPI index. Although there was a trend towards lower slope (Mw) and
higher intercept (Vw) of the PRSW relationship in LVE relatives, both of which are indices
of reduced contractility,14-16 there was a substantial scatter of data and the differences with
control subjects did not achieve statistical significance. With exercise stress, LVE relatives
achieved comparable peak heart rates but had lower systolic blood pressure and shorter
exercise duration. LV cross-sectional areas before and after exercise were increased in LVE
dididididididididididididdidididididididictctctccttctctctctctctcttctctctctccc ededededededededededededededededededededdededd) ))))) )))) ) ) ))))))))) ananananananananaananananananaannnnnnd dddddddd ddd dddddddd ththhhthththhhhthhthththhthe ee e ee ee e eee ee e eeeee FFFFFFFFFFFFFFFF
efficaaaaaaaaaaaaaaaaaacycycycycycycycycycycycycycycycycycycyccc ooooooooooooooooooovevevevevevevevevevevevevvevevveveevvev rararararararaarararaaaarrararaarallllllllllllllllllllllllllllllllllllll Op y
d d
n
p y
d, LLLVLL EDD DD (%(%(%(%( ppppprererereredididididictctctctctededededed) )))) > > >1111166%6% mmosososososttt t efefefefeffefffef ctcctivivivivvelee y y y y y dididdid fffffffffferererererenenenenntititititiatatatatatedeeee
ntrolslslslsls.
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
9
relatives but the relative increment in fractional area change at peak exercise was equivalent
to control subjects. Five LVE relatives and 2 control subjects had BNP levels that were
higher than those of an age- and sex-determined reference range, but there were no
differences in mean levels between the groups.
Predictive value of echocardiographic indices
The sensitivity and specificity of indices of systolic and diastolic LV function were assessed
by comparing the numbers of LVE relatives and control subjects who had values lying
outside a limit defined ± 2 SD of the mean values in control subjects. Individual parameters
had only weak to moderate sensitivity but generally high specificity (Table 4). The cut-off
value for LVEDD (%predicted) >122% defined by this method was less sensitive than
LVEDD (%predicted) >116%. The combined criteria of LVEDD (%predicted) >116%, or
LVEDD (%predicted) 112-116% + LVFS <29 identified all 30 LVE (100%) relatives and 2
control subjects (sensitivity 100%, specificity 93%). Addition of other parameters had no
incremental value for identifying LVE relatives. In the natural history cohort, 61 individuals
met these criteria, including 8 of the 9 progressors.
Discussion
Here we find that LVE is common in asymptomatic relatives and that 1 in 10 individuals with
LVE will progress to DCM within a 5-year period. LVE is also present in many normal
individuals, highlighting the need for criteria to distinguish between pathological and
physiological LV dilatation. Our natural history data indicate that LVE alone incompletely
identifies progressors and that assessment of LV size and contractile function is required for
risk stratification. While a variety of techniques for detecting pre-clinical cardiomyopathy
ciciciciciciciciciciciciccicicicicicicicitytytytytyytytytytytytytytytytytyytytyyyyy (((( ((( ( ( ((( ( ( (((( ( ((((TaTaTaTaTaTaTaTaTaaTaaTTTTaTaTTaaaaTT blblblblblblblblbblblblblblblbbllllle e e eee e e e eee e e ee eee e 4)4)4)4)4)4)4)4)4)4)4)4)4)44)44)4 . . . TThTThTTTTTTTThTThTThTTTT
was leleleleleleleleleleleleleleleleleeeeeesssssssssssssssssssssssssssssssssssss sssssssssssssssssseneneneneneneneneneneneeneneneneneneeenene sisisisisiisisisisisisisisiisiissiiititititittitititittititititittitititit vevvv( p ) y
>
( r
( p ) y
ccccteeeed) >11116%6%6%6%6%. ThThThThThee eee cococococombmbmbmbmbininini ededded ccriterriaaaaa ooo oof fff f LVLVLVLVLVEDEDEDDEDD DDDD (%(%(%(%(%prprrrrededededediciciicicteteteteted)d)d)d)d) >
cted)d)d)d)d) 11111121211 -111116161616% %%%% + +++ LVLVLVLVLVFFSFFF <<<<<2929292929 iii iddededd tntntifffffieeieeeddd dd aaalaa l llll 3030303030 LLLLLVEVEVEEVE (1(1(1(11000000%)%)%)%)) r rele
(sesesensnsnsititivivitititii y y y yy 1010100%0%0%, ,,,, spspspsppececece ififificicccititity y y yy 939393%)%)%)%)%). . AdAdAdA dididiitititionononn oo of f f f otototheheheheer r r r papapapp rararamememeteteterrrr
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

10
have been proposed, standard 2-dimensional and M-mode echocardiography is an effective
screening method for detection of early disease. These findings have implications for the
clinical screening and follow-up of asymptomatic relatives in DCM families.
The prevalence and natural history of LVE have been evaluated in several studies.4-
8,12 In the largest series to date, Mahon and colleagues8 screened 767 asymptomatic relatives
of 189 DCM probands and found 140 relatives (18%) with abnormal echocardiograms,
including 119 relatives with LVE and 21 relatives with dFS. Eight of the 107 LVE relatives
(8%) who were followed prospectively developed DCM over a median 53-month period. In
our cohort of 457 asymptomatic relatives in 128 DCM families, we found 115 of 457
asymptomatic relatives relatives (25%) with abnormal echocardiograms, most of whom
(n=110) had LVE. Nine of 72 untreated LVE individuals (13%) progressed to DCM over a
median 52-month period. Our data are concordant with those of Mahon et al. and show that a
clinically-significant number of asymptomatic relatives will deteriorate within 5 years after
LVE is detected.
Given its prognostic significance, the reliability of methods used to define LVE is
paramount. Diagnosis of LV dilatation based on a laboratory reference range for LVEDD (eg.
>56 mm) is relatively insensitive, particularly in women, and several different normalization
formulae have been proposed, that take into account factors such as age, sex, height, and
body surface area.19-21 Normalization of LVEDD to BSA using the Henry formula has been
recommended for clinical practice. 25 We selected LVEDD (%predicted) >112% since this is
a frequently-used criterion for LV dilatation and permits direct comparison with other early
disease studies, including that of Mahon et al. 5,8,12 Baig and colleagues5 suggested that
LVEDD (%predicted) >118% might be a better predictor of relatives at risk of developing
DCM, while Hershberger and colleagues26 concluded that the Framingham standard was
superior to LVEDD (%predicted) >112% or the NHLBI standard for detecting LVE. We
iiiiiiiiiiiiiiiogoogogogogogogogogogogogogogogogogogogogoggggrararaarararararararaararrararararaaaar msmsmsmsmsmsmsmsmsmsmsmsmmmmmsmmsmmmsmmmm ,, ,, , , ,,,, ,,,, momomomomomomomomomommmomomomomommmm sttstststststststststtstsststst o o o oo o o ooo oooo o oooooffffffffffffffff
progggggggggggggggggrerererererererererererererererererererressssssssssssssssssssssssssssssssededededededededededededededededdededededdeddd tttttttttttttttttoooooooooooooooooooo DCDDDDDDDDDDDDDDDD( ) p g
h riod. d
ca
( ) p g
h peeriod. OuOuOuuOurr dadadadadatatatatata aa aaarerererere ccccconononononcccordrdrdrddaantt wiwiiiiththththth ttttthohohohohosesee oo ooof f ff f MaMaMaaahohohohohon nnn n etetetetet a a aaal.llll aa aaandnnn
canttttt nnn numumumumumbeerr ofofofff a asysysysympmmpmpmptotototot maaaaatiiititic cc rerelallall tititit veveveveessss s wiwiwiwiwillllll d ddddetette ererioiiorararatetetet wwititi hihihihiinn 5 5555
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

11
concur with these findings but also show that LVEDD (%predicted) >116% gives even better
discrimination between family members and control subjects.
Our natural history data do not support a direct relationship between LV size and
disease progression in all cases, and some progressors had an only mild LVE together with
LV systolic dysfunction at the initial screening study. These differences in primary
manifestations of disease are likely to be explained at least in part, by the underlying family
gene mutation, and demonstrate that LV size and function need to be incorporated into risk
assessment. A number of non-invasive techniques for detection of early myocardial
dysfunction in familial DCM have been reported5,9-12 but a comprehensive comparative
analysis has not been performed. Our echocardiographic studies provide insights into
myocardial performance in LVE relatives as well as the sensitivity and specificity of various
functional parameters.
The majority of LVE relatives had LVFS values that were within a “normal”
reference range, however the mean LVFS was significantly lower than in control subjects.
LVE relatives had a lower mitral S wave velocity, prolonged time to peak S wave velocity
and higher MPI index, consistent with mild defects of LV systolic function. Indices of
diastolic function were similar in LVE relatives and control subjects, with no augmentation
of atrial contraction or rapid early filling that is characteristically seen in patients with
established DCM and elevated LV filling pressure. The low mitral inflow E wave velocity
suggests normal LV filling pressure, consistent with normal levels of BNP in the majority of
individuals. Despite the baseline impairment of systolic function, as well as higher chamber
volumes and heart rates, LVE relatives were able to partially compensate functionally to
maintain cardiac output with exercise and achieved similar increments in systolic contraction
and maximum heart rates to those in control subjects, explaining their lack of symptoms.
pppppppppppppppppppppprororororoorororororororororororoororovivivivivivivvivivivivvivivivivivivivivviviidededededededededededeededddddedddedd ii iiiiiiiiiiiiinsnsnsnsnsnsnsnsnsnsnnsnsnsnsnsnsnsnn igigigigigigigigiggggiggiggghthththththththththththththththththhthhth sssssssssssssssss
ity aaaaaaaaaaaaaaandndndndndndndndddndndndndndndndndndndndnnd sssssssssssssssspepepepepepepepepepepepepepepepeepeepepeeeeciciciciciciciciciciciciciciciiicic fifififfifififififififififfififififififificicccccccccccc ty p
e
ri ve d m
h l
y p
etetetete eeree s.
rity oooof fff LVLVLVLL E EEE rereelallall titittitives ssss hahahahh d LVLVLVLVLVFSFSFSFSFS v valallueuueueuesss thththththattttt www wwereree wiwiiiithththththiiniii aa “ “““nonon rmrm
hhhoowoweeveverererrr t t thehehehe m m meaeaean n n LVLVLVLVFSFSFSS w w wwwasasass s s siiigngngngg ififificiciccanananntltlttly y y yy loloooowewewer rr ththththanananan i iin n n cococontntntrororol
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

12
However, the peak pulse pressure, rate-pressure product, and exercise duration were
relatively reduced, consistent with blunting of peak myocardial work capacity.
While statistically significant differences between groups were found for many of the
functional parameters evaluated, there was a substantial scatter of data and overlap between
LVE relatives and control subjects. To derive some practical guidelines for the investigation
of individual family members, we determined the sensitivity and specificity of various
parameters using data dichotomized ± 2 SD from mean values in control subject. In this
analysis, individual factors had low-to-moderate sensitivity and sensitivity. Surprisingly, the
simple measures of LV dimensions and LVFS were more discriminative than the tissue
Doppler and exercise echo parameters. Most of the individuals with abnormal tissue Doppler
and exercise echo parameters were already identified by changes in LV dimensions and
LVFS, and there was no incremental value for including these factors. Selecting individuals
with more severe LV dilatation, (LVEDD (%predicted) >116%), or an intermediate extent of
LV dilatation together with LVFS less than 2SD from the control mean (LVEDD
(%predicted) 112-116% + LVFS <29%), gave a very high sensitivity (100.0%) and
specificity (93.3%) for differentiating LVE relatives from control subjects, and identified 8 of
the 9 progressors in the natural history study. These observations suggest that asymptomatic
relatives that meet these criteria have a high likelihood of having early disease and warrant
close-follow-up. In relatives with LVEDD (%predicted) 112-116% + LVFS >29%, some
may be genotype-positive and too young to show signs of disease, while others may in fact be
genotype-negative.
Identification of LVE relatives at greatest risk of progression remains a challenge.
Although useful for detecting early disease, LVEDD (%predicted) >116% or LVEDD
(%predicted) 112-116% + LVFS <29% had a positive predictive value of only 13% within a
5-year period. LVEDD and LVESD are independent predictors of congestive heart failure in
wiwiwwwiwiwwiwiwwiwiwwiwiwiwwwiwww thththththhthtthththththththththhth aa aa aaa a a aaaa aaaaaaaabnbnbnbnbnbnbnbnbnnbnbnbnbnbnbnbnbnbnbnnb orororororororoorororororororoororrrrmamamamamamamamamammamamamammammmm lllllllllllll l titititititititititititititititittitisssssssssssssssss
s in LLLLLLLLLLLLLLLLLLLLLLLVVVVVVVVVVVVVVVVVVVVVVV didididiidididididididididididididiididd memememememememememememememememmemmemmmmm nnsnsnsnsnnsnnsnnnsnsnsnsnsnnsnn iop y y g
s no i .
e i
g D
p y y g
wawawawwas no inccccrererrr memmemementntntntntalalalalal vv vvvalalalalalueueueueue f ff forrrrr ii inccluudididididingngngngng ttttthehehhh sesese fffffaaactooooorrrrsr . SeSeSSeS lelelelelectcctctc inininining
e LV VVVV dididiiilalalalalataatititt ononn, (L(L(L((LVEVEVEVEEDDDDDD (((((%p%p%p%p%predddddicicteteted))d)d)d) > >>>>1111111116%6%6%6%6%),),),), o oor ananan ii iiinttnttteerer ememem dddidd
geeeeththererer w witititti h h h h LVLVLVFSFSFS l lllesesesss ss s ththththananannn 2 2 2SDSDSDS f fffrororom mm thththe e e cocococ ntntntn rororol l ll mememeananana ( ( ( ((LVLVLVEDEDEDDDDD
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

13
a community-based population27 but we found no differences in the mean LVEDD or LVFS
between progressors and non-progressors at their baseline evaluation. Most of the diagnostic
indices evaluated in the case-control study were not included in the natural history study, and
hence we are unable to exclude the possibility that some of these may have a role in risk
stratification or serial patient monitoring. Continued evaluation of markers of early disease is
required and techniques such as cine magnetic resonance imaging may have a role in
detecting and monitoring preclinical LV dysfunction.28
A limitation of our study is the small number of genotyped individuals and we cannot
exclude the possible confounding effects of inclusion of some relatives with non-genetic
causes of LVE. Since mutations in known disease genes are present in a minority (<25%) of
DCM families,3 the practical reality is that most physicians are required to assess family
members who have unknown genotypes. Even if the genotype is known, there will be diverse
underlying molecular defects, unique individual profiles of background genetic and
environmental factors, and relatives are likely to be screened at varying temporal stages of
the disease process. Hence, a functional classification of early disease may be more
clinically-useful than genotype per se.
These observations highlight the importance of clinical screening of asymptomatic
relatives in DCM families and of ongoing follow-up for those with LVE. Accurate
identification of high-risk subgroups within LVE cohorts will not only have implications for
individual patient management, but will also help to define a target study group for clinical
trials. The ultimate goal of detection of early disease is preventative intervention but there are
currently no data to support either pharmacological treatment or wait-and-see approaches for
pre-symptomatic family members. Prospective studies are urgently required to determine the
most effective agents and optimal timing of prophylactic therapy.
seseseseeseseseseesesesseseseeeeeesentntnntntnttntntntnntntntntntntntnn iiiii iii iiiiiiiiinnnnnnnnnnnnnnnnnnnn aaaaaaaa aaaaaaaa mm m m m mmmmm m m mm mmmmmmmininininininininininiinninininiiinororororrorororrorororororororooorrrititititititititititititititititiitityyyyyyyyyyyyyyyyy
requiiiiiiiiiiiiiiiiirerererererererererererererererererreedddddddddddddddddddddd tototototototototototototoototototoottoo aaaaaaaaaaaaaaaasssssssssssssssssssssssssssssssssseeeeeseeeeeee sp y p y q
v nkno f e s w
cul a
c l
p y p y q
vvvevv unknownwnwnwwn g ggggenenenenenotototototypypypypypesesesss.. . EvEvEEvE ennnnn i f ththe gegggg nononononotyttytt pepepe iiiiis knnnnnowowowowown,n,n,n,n, ttttthehehehehererererere w
cularrrrr d ddddefefefefefecctststt , ,,,, ununu iiqiqiqi ue ii indndndndn ividididididuauauauaualllll prprpr fofofffilililii eeeese ooooofff bababababackckkckgrgrgrrg ouuundndnddd ggenenetetettticiiiic a
ctctctorororsss, aa andndndndn r r releleelatatativiviviveseses a a aarererer l l likikkikelelely y y yy tototo b bbbe ee scscscrererereenenenedede a a aat tt vavavaryryryyyininiinng g g gg tetetempmpmporororalaal
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

14
Acknowledgments: We thank M. Law for statistical advice and analysis; F. Ali, O.
Baddeley, H.Crotty, and J. Hansen for clinical investigations; and K. Alford, D. Amos, J.
Atherton, B. Bastian, F. Bates, M. Cooper, G. Carroll, T. Carruthers, G. Connor, G. Cranney,
R. Cranswick, L. Davis, B. Freedman, J. French, P. French, D. Guy, D. Hammill, D. Hayes,
P. Hayes, D. Kuchar, G. Lane, J. Leitch, S. May, D. Mumford, L. Pressley, D. Richmond, P.
Robinson, S. Roy, C. Semsarian, J. Silberberg, C. Thorburn, P. Thompson, E. Vogl, B.
Walker, for proband referrals.
Funding Sources: This work was supported by the National Health and Medical Research
Council of Australia, Canberra (grant numbers 354400, 404808), National Heart Foundation
(grant number G00S0736), St Vincent’s Clinic Foundation, Sylvia and Charles Viertel
Charitable Foundation, and a Pfizer Cardiovascular Lipid Research Grant (to TY).
Conflict of Interest Disclosures: None.
References:
1. Lee DS, Pencina MJ, Benjamin EJ, Wang TJ, Levy D, O’Donnell CJ, Nam BH, Larson
MG, D’Agostino RB, Vasan RS. Association of parental heart failure with risk of heart
failure in offspring. N Engl J Med. 2006;355:138-147.
2. Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D, Arnett D, Moss AJ,
Seidman CE, Young JB. Contemporary definitions and classification of the
cardiomyopathies. Circulation. 2006;113;1807-1816.
3. Fatkin D, Otway R, Richmond Z. Genetics of dilated cardiomyopathy. Heart Fail Clin.
2010;6:129-140.
4. Zachara E, Caforio AL, Carboni GP, Pellegrini A, Pompili A, del Porto G, Sciarra A,
Bosman C, Boldrini R, Prati PL, McKenna WJ. Familial aggregation of idiopathic
dilated cardiomyopathy: clinical features and pedigree analysis in 14 families. Br Heart
J. 1993;69:129-135.
encina MJ, l CJ, Nam
ostino RB Vasan RS Association of parental heart failure with
encina MJ, BeBeBeBeBenjnjnjnjnjamamammminininii EEEEEJ,J,J,J,J, W W W W Wananananang g g g g TJTJTJJJ, , , ,, LeLLLL vyvyvyvyvy D D D D D, , , O’O’O’O’O’DoDoDoDoDonnnnnnnnnneeelee l CJ, Nam
osoostitinono RRBB VVasasanan RRSS AAssssocociaiatitionon ooff paparerentntalal hheaeartrt ffaiailulurere wwitithhh
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

15
5. Baig MK, Goldman JH, Caforio AL, Coonar AS, Keeling PJ, McKenna WJ. Familial
dilated cardiomyopathy: cardiac abnormalities are common in asymptomatic relatives
and may represent early disease. J Am Coll Cardiol. 1998;31:195-201.
6. Crispell KA, Wray A, Ni H, Nauman DJ, Hershberger RE. Clinical profiles of four
large pedigrees with familial dilated cardiomyopathy. Preliminary recommendations for
clinical practice. J Am Coll Cardiol. 1999;34:837-847.
7. Michels VV, Olson TM, Miller FA, Ballman KV, Rosales AG, Driscoll DJ. Frequency
of development of idiopathic dilated cardiomyopathy among relatives of patients with
idiopathic dilated cardiomyopathy. Am J Cardiol. 2003;91:1389-1392.
8. Mahon NG, Murphy RT, MacRae CA, Caforio AL, Elliott PM, McKenna WJ.
Echocardiographic evaluation in asymptomatic relatives of patients with dilated
cardiomyopathy reveals preclinical disease. Ann Intern Med. 2005;143:108-115.
9. McKenna CJ, Sugrue DD, Kwon HM, Sangiorgi G, Carlson PJ, Mahon N, McCann
HA, Edwards WD, Holmes DR, Schwartz RS. Histopathologic changes in
asymptomatic relatives of patients with idiopathic dilated cardiomyopathy. Am J
Cardiol. 1999;83:281-283.
10. Mahon NG, Sharma S, Elliott PM, Baig MK, Norman MW, Barbeyto S, McKenna WJ.
Abnormal cardiopulmonary exercise variables in asymptomatic relatives of patients
with dilated cardiomyopathy who have left ventricular enlargement. Heart.
2000;83:511-517.
11. Mahon NG, Madden BP, Caforio AL, Elliott PM, Haven AJ, Keogh BE, Davies MJ,
McKenna WJ. Immunohistologic evidence of myocardial disease in apparently healthy
relatives of patients with dilated cardiomyopathy. J Am Coll Cardiol. 2002;39:455-462.
t ttt ttttt PMPMPMPMPMPMPMPMPMPMPMMPMPMPMPMPMPMPMPMMPMP , , ,, ,,, , ,,,,, ,,,, McMcMcMcMcMcMcMccMcMcMcMcMcMcMccMMMMMMMM KeKeKeKeKeKeKeKeKeKeKKKeKeKeKeKeKeKKK nnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnna a aa aaaaaaaaaaaaaaa WWWWWWWWWW
f patitititititititititiitititiiittititiienenenenenenenenenenenenenenenenenennee tstststststststststststststststststsss wwwwwwwwwwwwwwwwwwwwwwwitiititititittitititititititiititttti hhhhhhhhhhhhhhhhhhhhhhh diddddddg p y p p
p 8
CJ, , ,
r
g p y p p
patatatatathhyhh reveaaaaalsllsl pppppreeeeeclclclclclinininininicicicicicalalalalal dddddisiii eaaaaasse. AnAnAnn nnn n InInInInInteteteteternrnn MM M MMedee . 202020202 0505050505;1;1;1;1;14343434343:1:1:1:1:108000
CJ, SuSuSuSS grgrgrgrg ueee DDDDD,D,D,DD KK KKKwooooonnnnn HMHMHMHMHM, SaSaSaSaSangngngioiorgrggrggii ii G,G,G,G,G, CC CCCarararararlslslsl onononn PPPPPJJ,JJJ MMMMMahhahhhonononn NNNNN,
rdddsss WDWDWD, HoHoHolmlmeseses D D DR,R,R,, S SSSchchhchwawawaww rtrtrtz zz RSRSS. HiHiHiH stststs opopopppatatathohohohh lolooogigiggg c c c chchcc ananangegegesss inin
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

16
12. Caforio AL, Mahon NG, Baig MK, Tona F, Murphy RT, Elliott PM, McKenna WJ.
Prospective familial assessment in dilated cardiomyopathy. Cardiac autoantibodies
predict disease development in asymptomatic relatives. Circulation. 2007;115:76-83.
13. Matsumura Y, Elliott PM, Mahon NG, Virdee MS, Doi Y, McKenna WJ. Familial
dilated cardiomyopathy: assessment of left ventricular systolic and diastolic function
using Doppler tissue imaging in asymptomatic relatives with left ventricular
enlargement. Heart. 2006;92:405-406.
14. Karunanithi MK, Feneley MP. Single beat determination of preload recruitable stroke
work relationship: derivation and evaluation in conscious dogs. J Am Coll Cardiol.
2000;35:502-513.
15. Hayward CS, Kalnins WV, Kelly RP. Gender-related differences in left ventricular
chamber function. Cardiovasc Res. 2001;49:340-350.
16. Mandarino WA, Pinsky MR, Gorcsan J 3rd. Assessment of left ventricular contractile
state by preload-adjusted maximal power using echocardiographic automated border
detection. J Am Coll Cardiol. 1998;31:861-868.
17. Sakata K, Ino H, Fujino N, Nagata M, Uchiyama K, Hayashi K, Konno T, Inoue M,
Kato H, Sakamoto Y, Tsubokawa T, Yamagishi M. Exercise-induced systolic
dysfunction in patients with non-obstructive hypertrophic cardiomyopathy and
mutations in the cardiac troponin genes. Heart. 2008;94:1282-1287.
18. McDonagh TA, Robb SD, Murdoch DR, Morton JJ, Ford I, Morrison CE, Tunstall-
Pedoe H, McMurray JJ, Dargie HJ. Biochemical detection of left ventricular systolic
dysfunction. Lancet. 1998;351:9-13.
19. Henry WL, Gardin JM, Ware JH. Echocardiographic measurements in normal subjects
from infancy to old age. Circulation. 1980;62:1054-1061.
erenccccccccccccccccceseseseseseseseseseseseseseseseseseseseee iiiiiiiiiiiiiiiiiiiinnnnnnnnnnnnnnnnnnn leleleleleleleleleleleleleleelelelelllll ftftftftftftfftftftftftftftftftftftft vvvvvvvvvvveny
u
e t
y
uncncncnncttittt on. CaCaCaaardrdrddrdiooooovavavaaascscscscsc RR R RReseseseses.. . 202020202 010101011;4; 99:34344440-0-00-0 35353535350.0.000
WAWAWAAA, PiPiPiPiPinssskykykykyky MMMMMRRR,RR GGGGGorororororcsannnnn J JJJJ 33 333rdrdrdrdrd. AAsAAA sesesesesesssssssssmemememem ntntntntnt oooff ff lelll ftftftftft vv veeentrtrtriciculullulararar
eeeloloadad aa-adjdjdjjdjusususteteted d dd mamamaxiximamamam l l popopopooweweweer r r usususining gg ecececechohooocacacac rdrdrdrr ioiooogrgrgrgg apapapapphihic c c auauautototomamaamattt
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
17
20. Manolio TA. Baughman KL, Rodeheffer R, Pearson TA, Bristow JD, Michels VV,
Abelmann WH, Harlan WR. Prevalence and etiology of idiopathic dilated
cardiomyopathy (summary of a National Heart, Lung and Blood Institute Workshop).
Am J Cardiol. 1992;69:1458-1466.
21. Vasan RS, Larson MG, Levy D, Evans JC, Benjamin EJ. Distribution and
categorization of echocardiographic measurements in relation to reference limits. The
Framingham Heart Study: formulation of a height- and sex-specific classification and
its prospective validation. Circulation. 1997;96:1863-1873.
22. Tei C, Ling LH, Hodge DO, Bailey KR, Oh JK, Rodeheffer RJ, Tajik AJ, Seward AJ.
New index of combined systolic and diastolic myocardial performance: a simple and
reproducible measure of cardiac function – a study in normals and dilated
cardiomyopathy. J Cardiol. 1995;26:357-366.
23. Gorcsan J. Load-independent indices of left ventricular function using automated
border detection. Echocardiography.1999;16:63-76.
24. Moretti M, Merlo M, Barbati G, Di Lenarda A, Brun F, Pinamonti B, Gregori D,
Mestroni L, Sinagra G. Prognostic impact of familial screening in dilated
cardiomyopathy. Eur J Heart Fail. 2010;12:922-927.
25. Feigenbaum H. Appendix: Echocardiographic measurements and normal values. In:
Feigenbaum H, ed. Echocardiography. 5th ed. Philadelphia:Williams and Wilkins;
1994:658-683.
26. Hershberger RE, Ni H, Crispell KA. Familial dilated cardiomyopathy:
echocardiographic diagnostic criteria for classification of family members as affected. J
Card Fail. 1999;5:203-212.
pepepepepepepepepepepepeppepepeppepepepepep rfrfrfrfrfrfrfrfrfrfrfrfrfrfffffrffororororororoororororoorororororooorooro mamamamamamamamaamamamamamamamaammmmmmmmancncncncncncnccncncncncncncncncncnccnn e:e:e:e:e:e:e:e:e:eee:ee aaa aaaaaaa aaaaaaaaaaaa ssssssssssssssss
mals ananananananananananananananannanananannddddddddddddddddddddd didididididididididididididididididididdiididiilalalalalalalalalalalalalalalalalalal tetetettetetetetetetetetetetteteteteteedddddddddddddddddy
p
L t ce o
e
y
patatatatathhyhh . J CaCaCaaardrdrdr ioioioioiolllll.. 1919191919959595995;2;2;2;2;26:6:6:66 353535357-7-7-77 36666.
Loaaaddd-dd ininininindededdd pepependndndddenenennt ininininndididididices ofofoffof l lllleffeffft tttt veveventntntnntririririricucucucuculaaaaarrrrr fufufuf ncncncctiiiiiononon usiiingngng aaautututo
ecccctitiononon. EcEcEcchohohohocacacardrdddioioiogrgrgrgrg apapapapphyhyhyyy.1.1.19999999999;9;9;16166:6:6:63-3-3 7676766.
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

18
27. Vasan RS, Larson MG, Benjamin EJ, Evans JC, Levy D. Left ventricular dilatation and
the risk of congestive heart failure in people without myocardial infarction. N Engl J
Med. 1997;336:1350-1355.
28. Koikkalainen JR, Antial M, Lotjonen JMP, Heliö T, Lauerma K, Kivistö SM, Sipola P,
Kaartinen MA, Kärkkäinen ST, Reissell E, Kuusisto J, Laakso M, Oresic M, Nieminen
MS, Peuhkurinen KJ. Early familial dilated cardiomyopathy: identification with
determination of disease state parameter from cine MR image data. Radiology.
2008;249:88-96.
Table 1. Characteristics of 128 probands and their families
Clinical Feature No. individuals (%)
Proband demographics: - Males - Age at study entry (years) - Caucasian ethnicity
79 (62%) 42 ± 14
128 (100%) Family phenotype*:
- DCM only - DCM + conduction-system abnormalities - DCM + skeletal muscle involvement†
111 (87%) 16 (13%)
1DCM inheritance pattern‡:
- Autosomal dominant - Possible autosomal dominant or X-linked - X-linked - Autosomal recessive
94 (73%) 27 (21%) 7 (6%) 0 (0%)
Known genotype§ 4
DCM indicates dilated cardiomyopathy. * Classification based on predominant clinical manifestations of affected family members. † Calf tenderness during exercise and raised creatine kinase levels found in two affected individuals in one family. No individuals in any family had clinical signs of skeletal muscle weakness or wasting. Creatine kinase levels were not systematically assessed in all cases. ‡ Presumptive mode of inheritance based on distribution of affected individuals in family pedigrees. § Novel mutations (unpublished) were present in 4 families. Of 23 genotyped family members, 13 individuals were genotype-positive (DCM 3, LVE 5, obligate carrier 1) and 10 individuals were genotype-negative (all phenotypically normal).
a
un ethnicity
%4
128 (100%
a
aphihihiiicscscs:: :
uuuddy e ttntryryryryry ( ( ( (yeyeyeyey arararara s)s)ss) nnn etethnhnicicitityy
79 (62%424242 ±± ± 11 14444
121288 (1(100000%
No. individua
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

19
Table 2. Baseline characteristics of 72 untreated LVE relatives followed prospectively
Parameter No progression Progression P value
Individuals (no. families) 63 (35) 9 (9) -
Males (%) 38 (60.3%) 5 (55.6%) 0.83
Age at study entry (years) 34.4 ± 9.6 27.0 ±7.7 0.03
LVEDD (mm) 56.6 ± 3.3 55.7 ± 3.2 0.44
LVEDD (% predicted) 120.2 ± 5.0 119.3 ± 4.7 0.61
LVESD (mm) 38.1 ± 3.7 38.8 ± 3.3 0.58
LVFS (%) 32.4 ± 5.2 30.2 ± 3.8 0.22
Heart rate (bpm) 65 ± 12 66 ± 9 0.90
Follow-up duration (months) 55.2 ± 27.9 52.6 ± 32.0 0.47
LVEDD indicates left ventricular end-diastolic diameter; LVESD, left ventricular end-
systolic diameter; LVFS, left ventricular fractional shortening.
3333333333333333333330.0.000.00.0.0.000.0.00.00.0000 2 22222 222 2 222222222222 ± ±±±±±±±±± ±±±± ±±±±± ±±± 3.3.3.3.3.3.3.3.33.3.333.3.333 8 8 8 8888 8 8 8888 888 888 88
66666666666666666666 ±±±±±±±±±±±±±±±±±±±±± 9999999999999999999
o
a
oono (monthshshsshs)) ) 55.2.2.222 ± 2277.9 9 9 99 52525222.6.6.666 ±± ±±± 3 33 332.22.22 0 0 0 00
ss llleftftft vennnnntrtrtrtt iciciciculululululararar eeeeendndndndnd-d-d-diaiaiaai stststststoooolililic cc cc dididididiamamamammetetetererererr; ; ; ;; LVLVLVLVLVESESESESESD,D,D,D,D, l l lllefefefefeft t t tt veveveveventntnt iiriculalala
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

20
Table 3. Characteristics of LVE relatives and age- and gender-matched healthy controls
Parameter LVE relatives Control subjects P value
Individuals (no. families) Males (%) Age (years) LVEDD (mm)
30 (20)
17 (57)
39.0 ± 10.9
58.2 ± 3.9
30
17 (57)
39.0 ± 10.9
49.7 ± 3.6
-
-
-
<0.001LVEDD (% predicted) 122.9 ± 6.7 107.3 ± 7.4 <0.001LVESD (mm) 40.2 ± 3.5 30.9 ± 3.7 <0.001LVFS (%) 30.9 ± 4.8 37.8 ± 4.2 <0.001Mitral E (cm/s) 71.7 ± 14.0 84.9 ± 15.6 0.002 Mitral A (cm/s) 55.9 ± 9.6 58.1 ± 12.4 0.42 E/A ratio 1.32 ± 0.33 1.53 ± 0.38 0.07 Myocardial performance index 0.41 ± 0.11 0.28 ± 0.06 <0.001 Mitral S (cm/s) 8.2 ± 2.2 10.3 ± 2.3 <0.001 Time to peak S (cm/s) 0.22 ± 0.07 0.18 ± 0.04 0.01 Mitral E’ (cm/s) 13.4 ± 4.3 15.2 ± 2.9 0.06 Mitral A’ (cm/s) 7.3 ± 1.9 7.6 ± 2.3 0.64 E/E’ ratio 5.8 ± 2.0 5.7 ± 1.2 0.82 Mw (slope) 0.9 ± 0.3 1.0 ± 0.3 0.22 Vw (intercept) 30.3 ± 35.7 21.3 ± 35.6 0.38 End-diastolic area (rest, cm2) 22.7 ± 4.0 18.6 ± 2.9 <0.001 Fractional area change (rest, %) 49.4 ± 5.5 61.4 ± 8.6 <0.001
End-diastolic area (ex vs rest, cm2) -3.6 ± 2.9 -2.9 ± 1.9 0.27 Fractional area (ex vs rest,%) 10.5 ± 11.7 13.6 ± 9.5 0.25
Heart rate (rest, bpm) 67 ± 9 62 ± 10 0.04 Heart rate (maximum, bpm) 175 ± 19 177 ± 12 0.48 Systolic BP (rest, mmHg) 124 ± 12 121 ± 12 0.33 Systolic BP (max, mmHg) 168 ± 12 176 ± 14 0.05 Diastolic BP (rest, mmHg) 79 ± 7 78 ± 9 0.50 Diastolic BP (max, mmHg) 67 ± 6 63 ± 7 0.05 Rate-pressure product† 29326 ± 3601 31209 ± 3208 0.03 Peak pulse pressure (mmHg) 99 ± 10 113 ± 15 0.01 Exercise time (min) 11.6 ± 2.4 14.2 ± 2.9 <0.001 NT-pro BNP (ng/L) 88 ± 121 51 ± 54 0.12
BNP indicates brain natriuretic peptide; BP, blood pressure; LVEDD, left ventricular end-diastolic diameter; LVESD, left ventricular end-systolic diameter; LVFS, left ventricular fractional shortening. * Lateral margin of mitral annulus; data for septal margin are similar (not shown). † maximum heart rate x maximum systolic BP.
1.1.1.1.11.1.11.111.11111.111 535353535353535353535335353535353353535335 ± ±±±±±±± ±±± ±± ± ± ±± ±±±± 00 0000 000 00000 000.3.3.3.3.3.3.3.33.3.3.3.3.3.333338 888888888888888880.2828882828282828282882888288882888 ±±± ±±±±±±±±±±±±±±±±±± 000000000000000000000000.000000000000000000006 666666666666666666666610 333333333333333333333 ±±±±±±±±±±±±±±±±±±±±±± 22222222222222222222 333333333333333333333333
c 0.22 .07 18 ± 0.04
0.3
a (rest cm ) 22 7 ± 4 0 18 6 ± 2 9
cmmmmm/s/s/s/s/s))))) 0.22 ±±±±± 00.07 0.18 ± 0.04 131313133.4 ±± 4.33.33.3 15.55.5.5.222 22 ± ±± ±± 2.2.2.22 9 9 9 9977.33 ±± 1.99999 7 7 777.6.6.6.66 ± 22222.33 55555 888.8 ±±± 2 222.00000 5.77777 ±±±± ± 1.22222 00000.9.9.9.9.9 ± ± ± ± 00000.3.3.33 11111.0.0.0.0.0 ± 0.3
3030303030.3.3.33 ± ± ± 3 3 3335.55.7 7 7 7 212121221.3.3.333 ± ± ±± 3 3 3335.5.5.666 aaa ((rerestst cmcm22222)) 2222 77 ±± 44 00 1188 66 ±± 22 99
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

21
Table 4. Discriminative value of echocardiographic variables in 30 LVE relatives and 30
control subjects
Parameter No. LVE
relatives
No.controlsubjects
Sensitivity* Specificity*
LVEDD >56.9 mm 17 0 56.7% 100%
LVEDD (%predicted) >122% 16 0 53.3% 100% LVESD >38.4 mm 20 1 66.7% 96.7% LVFS <29.4% 13 0 43.3% 100% Mitral E <53.6 cm/s 3 2 10.0% 93.3% E/A ratio <0.77 1 0 3.3% 100% Myocardial performance index >0.40 13 0 43.3% 100% Mitral S <5.7 cm/s 4 0 13.3% 100% Time to peak S >0.26cm/s 7 2 23.3% 93.3% Heart rate >82 bpm 3 1 10.0% 96.7% Systolic BP (max, ex)<148 mmHg 0 0 0% 100% Diastolic BP (max, ex) >77 mmHg 1 1 3.3% 96.7% Rate-pressure product <24793 3 1 10.0% 96.7% Peak pulse pressure <83 mmHg 2 0 6.7% 100% Exercise time <8.4 min 2 0 6.7% 100%
BP indicates blood pressure; LVEDD, left ventricular end-diastolic diameter; LVESD, left ventricular end-systolic diameter; LVFS, left ventricular fractional shortening. * Sensitivity and specificity were determined using the numbers of individuals in each group with values outside the mean ± 2SD for the control group.
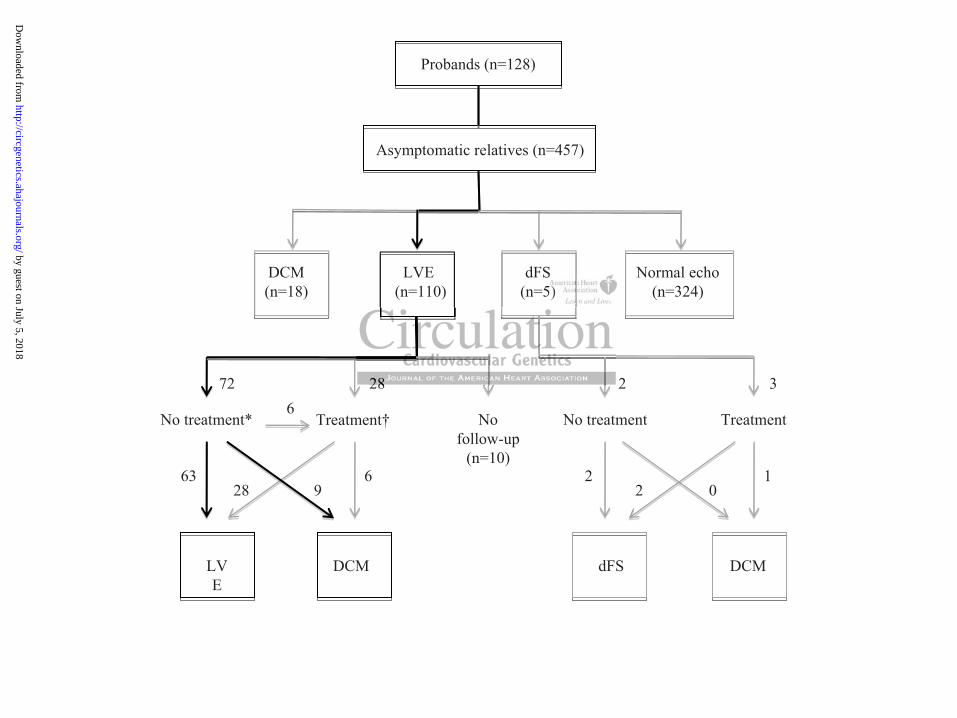
Figure Legends:
Figure 1. Results of baseline screening and follow-up of asymptomatic relatives of patients
with familial dilated cardiomyopathy.
DCM indicates dilated cardiomyopathy; dFS, depressed left ventricular fractional shortening;
LVE, left ventricular enlargement.
* The outcomes of relatives with LVE (n=72) who were not receiving any treatment during
the period between progress echocardiograms (“natural history” cohort) are indicated by the
13131313131331313131313131313131331313131 .3.3.3.3.3.33.3333.3.3.3.3333% % % % %% % % % %%%%% %% %%%%%2323232323232232323232323232323232332332232 33333.3333333333333333%%%%% %%%%%%%%%%%%%%%%%%%101010101010101010101010101010101010001001 0000000000000000000%%%%%%%%%%%%%%%%%%%%%%%%%p
x, 0 % a x) >ou
od pressure; LVEDD left ventricular end diastolic diameter; LV
px, exexexexex)<)<)<)<)<1414141414888 mmmmmm Hg 0 0 0% axxx,xx ex) >77777 m mmmmHmHmHmHmHgggg g 1 1111 111 11 3.3.3.3.3.3%3%3%3%3% oddddducucucucuct <2474444 93993 33 3 1 10000.0.0.00.0% %%ure <8<8<8<8<8333 33 mmHgHgHgHgHg 2 2222 0 6.6666 7%%%%% .4 min 2 2 2 2 2 0 0 0 0 0 6.7%
odd pressure; LLVEVEDDDD lleftft ventt iricullar endd didiasttolilic didiam teter; LVVLV
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

22
black lines. Six of these individuals subsequently crossed over to the treatment group and
underwent further follow-up.
† Cardiovascular medications, including -blockers, angiotensin converting enzyme
inhibitors, calcium antagonists, were administered for various indications (DCM prophylaxis,
hypertension, palpitations, atrial fibrillation) at some time during the follow-up period.
Figure 2. ROC analysis of different methods for assessment of left ventricular dilatation in
asymptomatic relatives and healthy control subjects.
AUC indicates area under the curve; Framingham, criteria based on data from the
Framingham Heart Study, LVEDD differences from 95th percentile values are shown;
NHLBI, criteria formulated by National Heart Lung and Blood Institute expert panel;
LVEDD (%predicted), ratio of actual left ventricular end-diastolic diameter to predicted
diameter, expressed as a percentage; ROC, receiver operating characteristic.
ttttttttttttttttttttilililililiiliililililililililililllilii e ee ee e e e e ee e ee e e eeeeeee vavavavavavavavavavavavavavavavavavavavavavavaavav lululululululululululuuulululluululul eseseseseeseseseseseseseseseesessesessses a a a a aa aaaaaaaaaaaaarerererererererereerererrrere sss ss ss ss sss sssssshhhhhhhhhhhhhhhhhhhh
Institttititttttttttttttuttttutututttututtututtututttuu eeee exeexexexexxxxppepeppepepeeerttttrttttrtrtrttrtrttrtrt py g p p
r
s
y g p p
cccteeed), ratio ofoffff aaaaaccccctututututualalalalal l lefefefefeft tttt veveventttttriicuular eeenee d-d-d-d-d-diddidd aaastototototoliiic dididididiammmmmetetetete ererererr tttttoo ooo pr
sed as a perceceeceentntntage;e;e;e;; RRRRROOOOOC, receivevev r opererrrratatata ing chahahahararr cttteristitic.
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
Asymptomatic relatives (n=457)
Probands (n=128)
DCM(n=18)
LVE(n=110)
dFS(n=5)
Normal echo(n=324)
No treatment* Nofollow-up
(n=10)
DCMLVE
Treatment† No treatment Treatment
DCMdFS
63
72 28
6
6
928 22 1
0
2 3
S5)
2828
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

Richmond, Michael P. Feneley, Anne M. Keogh and Peter S. MacdonaldDiane Fatkin, Thomas Yeoh, Christopher S. Hayward, Victoria Benson, Angela Sheu, Zara
CardiomyopathyEvaluation of Left Ventricular Enlargement as a Marker of Early Disease in Familial Dilated
Print ISSN: 1942-325X. Online ISSN: 1942-3268 Copyright © 2011 American Heart Association, Inc. All rights reserved.
TX 75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas,Circulation: Cardiovascular Genetics
published online June 2, 2011;Circ Cardiovasc Genet.
http://circgenetics.ahajournals.org/content/early/2011/06/02/CIRCGENETICS.110.958918World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circgenetics.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Genetics Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further information aboutnot the Editorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center,Circulation: Cardiovascular Genetics Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on July 5, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from