Embed Size (px)
Citation preview

Festschrift for Sir John McMichael 81
ReferencesANON. (1966) Editorial: Toxic bread. J. Amer. med. Ass. 196,
1150.CHUTTARI, H.K., SIDHU, WIG, K.L., GUPTA, D.N., RAMA-
LINGASWAMI, V. (1966) Follow-up study of cases from theDelhi epidemic of infectious hepatitis, 1955-56. Brit. med.J. ii, 676.
KOPELMAN, H., ROBERTSON, M.H., SANDERS, P.G. & ASH, I.(1966a) The Epping Jaundice. Brit. med. J. i, 514.
KOPELMAN, H., SCHEUER, P.J. & WILLIAMS, R. (1966b) Theliver lesion of the Epping Jaundice. Quart. J. Med. 25, 553.
SHERLOCK, S. & WALSHE, V.M. (1946) The post-hepatitissyndrome. Lancet, ii, 482.
The value of praecordial pulsations in the diagnosis ofheart disease
PATRICK MOUNSEYRoyal Postgraduate Medical School, London
PALPATION of the praecordium is as indispensableas auscultation of the heart in clinical examina-tion of the cardiac patient. Indeed, the twoshould be practised simultaneously, checking thetiming of heart sounds and praecordial move-ments in relation to one another. To some ex-tent the introduction of the modern binauralstethoscope with its flexible rubber tubes hasbeen a retrograde step, since this instrument isless suited to simultaneous analysis of praecordialpulsations and heart sounds than was the originalsolid tubular stethoscope invented by Laennec.In the Traite de l'Auscultation Mediate, Laennec(1819) emphasized that his instrument could beused not only to auscultate the heart but alsoto appreciate accurately the cardiac impulse. Heincludes in his book a chapter on the cardiacimpulse and states that a forcible impulse shouldbe regarded as the principle sign of cardiachypertrophy.Improved methods of recording the cardiac
impulse have been slower to develop than hasphonocardiography, although apex cardiographywas one of the earliest methods introduced forrecording the heart beat (Marey, 1878). Apexcardiography suffers from the disadvantage thatit is only a record of the relative displacementof a point in an intercostal space in relation tothe immediately surrounding area of chest wall.In cardiac diagnosis it is often the displacementof a large area of the thoracic cage by themovements of the underlying heart that is im-portant diagnostically, (as in the left parasternallift of right ventricular hypertrophy), and notthe relative movement of a small area in anintercostal space. To record this, an instrumentis required that measures absolute displacement,that is the total movement of the chest wall inF
relation to a fixed point in space. Variousmethods have been used for making this mea-surement, by Dressler in 1937, Eddleman et al.in 1953 and by Beilin & Mounsey in 1962. Wehave called our instrument the impulse cardio-gram and it aims at being a graphic record ofwhat the physician's hand and fingers feel.
The technique of palpating the praecordiumIt is often a good practice when examining the
praecordium to place the whole palm of thehand over the area of the chest that underliesthe heart. In this way, one can imagine that oneis holding the anterior surface of the heart inthe cup of one's hand, thus appreciating bothright and left heart events simultaneously. Careshould be taken, however, not to assume thatpulsations at the apex are always due to the leftventricle, while those in the left parasternal areaare due to the right. Although this state-ment is true probably in about 90% of patients,in the other 10% it is misleading. With greatenlargement of either left or right ventricle therelationship of underlying chambers of the heartto the praecordium are altered (Fig. 1). Thus,with marked left ventricular hypertrophy thischamber may underlie the whole area of prae-cordium from the apex beat to the left sternaledge, the right ventricle being pushed over tothe right. Similarly, with great right ventricularenlargement this chamber forms the apex of theheart, the left ventricle being rotated posteriorly(Deliyannis et al., 1964). It is more accurate,therefore, when describing praecordial pulsationsto relate these to the areas on the chest wallwhere they are felt, rather than to term them'right or left ventricular types' of impulse.
by copyright. on O
ctober 16, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.44.507.81 on 1 January 1968. D
ownloaded from

82 Postgraduate Medical Journal
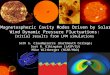
(a) (b) (c)FIG. 1. Superimposed tracings of right (dotted line) and left (solid line) ventricular angiocardiograms of (a)normal subject with functional systolic murmur. The apex beat (black dot) lies 2 cm lateral to the right ven-tricular cavity and overlies the antero-septal ventricular wall. (b) Patient with left ventricular hypertrophy frommitral incompetence. The apex beat (black dot) overlies the antero-lateral wall of the left ventricle; the left para-sternal area overlies its antero-septal ventricular wall. (c) Patient with right ventricular hypertrophy frompulmonary hypertension and ventricular septal defect. The apex beat (black dot) in the fourth intercostal space,7 cm to the left of the mid line, overlies the anterior wall of the right ventricle. The left parasternal area overliesthe more medial portion of the anterior wall of the right ventricle. The interventricular septum lies in thecoronal plane, with the left ventricle rotated posteriorly. (Antero-posterior views.)
The genesis of the cardiac impulse in health anddisease
Angiocardiographic and cinefluoroscopicstudies have shown close correlation between themovements of the heart and the form of thecardiac impulse.
1. The apical impulse in ventricular systoleThe first part of the apical impulse, both in
health and disease, is probably caused by similarmechanisms. In William Harvey's words (1628),'the heart erects and raises itself into a point,so that at this moment it strikes the chest wall
EJECT%ION
;-ATEEJECT!ON j
..T
... W__,~~~ .. i .W_i_W~~
FIG. 2. Left ventricular angiocardiograms (lateral view) of patient with small ventricular septal defect; in diastole(left) and in late systole (right). In line diagram, interrupted lines indicate diastolic, and solid line indicateslate systolic cavity-wall positions. Apical retraction demonstrated in late systole coinciding with retraction inimpulse cardiogram.
by copyright. on O
ctober 16, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.44.507.81 on 1 January 1968. D
ownloaded from

Festschrift for Sir John McMichael 83
..lLY...
LAT EJECT(t
FIG. 3. Left ventricular angiocardiograms (lateral view) of patient with aortic and mitral incompetence; indiastole (left) and in late systole (right). In line diagram, interrupted lines indicate diastolic, and solid lineindicates late systolic cavity-wall positions. Apical portion of heart fails to retract in late systole, thus accountingfor sustained, thrusting apical impulse.
and externally a pulsation can be felt'. It is dur-ing the latter part of systole that the heart be-haves abnormally in the presence of hypertrophy.Whereas in health the anterior wall of the heartretracts from the thoracic cage as the heartempties in late systole (Fig. 2), in left ventricularhypertrophy the antero-apical portion of theheart fails to retract in late systole (Fig. 3), thusgiving rise to the sustained cardiac impulse feltover the praecordium. Studies of the differentmuscle layers of the heart have suggested thatthe cause of this phenomenon is extension of themiddle circular layer of muscle fibres towardthe apex of the heart in the presence of hyper-
Normal heort Hypertrophied heart
Aortatra
~ Aota ~tro
w ~ ~~~~~~~~~~~~~~~~~~~~~~ nrinA
Circular7~~~~~~~~
4 ~~~~~~~~Circular ~
LV LV
Apex Apex
FIG. 4. Schema of forces resulting from contraction ofmiddle circular and of spiral fasciculi of left ventricle.In health, the middle circular fasciculus constricts theupper portion ofthe heart, while the relatively unopposedspiral fibres retract the apex. In left ventricular hyper-trophy the widened middle circular fasciculus extendsfurther toward the apex, thus tending to inhibit theapical retracting action of the spiral fasciculus.
trophy, thus tending to inhibit the apical re-tracting action of the spiral fibres (Fig. 4)(Deliyannis et al., 1964). Other factors, however,probably also contribute to the genesis of thesustained impulse including general increase inheart size and sometimes dilatation as well ashypertrophy.The cause of the sustained impulse in ventri-
cular aneurysm is not far to seek. The aneurys-mal wall which is composed entirely of fibroustissue without any living myocardium, is unableto take part in concentric contraction of theheart and herniates outwards during ventricularsystole (Fig. 5).The marked systolic retraction and diastolic
expansion seen in some cases of constrictivepericarditis is probably related to tethering ofthe inflow and outflow tracts of the ventricles,in annular constrictive pericarditis (Fig. 6). Inthis condition, the anterior wall of the ventriclesis often relatively free from constriction andhence shows exaggerated contraction duringventricular systole and expansion during dia-stole. Ventricular filling is abnormally abruptand forceful due to the high venous filling pres-sure. The marked systolic retraction and largediastolic rapid inflow beat seen in the impulsecardiogram closely reflect the underlying heartwall movements (Mounsey, 1959).
Apical retraction seen in tricuspid incompet-ence is due to a different mechanism, reflectingthe increased stroke output of the dilated rightventricle which is both ejecting blood into thepulmonary artery and regurgitating it through
by copyright. on O
ctober 16, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.44.507.81 on 1 January 1968. D
ownloaded from

Postgraduate Medical Journal
the incompetent tricuspid valve into the rightatrium. Cineradiological studies show a markedseesaw motion of the heart, with inward move-ment of the left cardiac border during systoleand simultaneous outward movement of the rightatrial border. This seesaw cardiac motion isclearly reflected in the movements imparted tothe whole praecordium (Boicourt, Nagle &Mounsey, 1965).
2. The atrial beatIncreased atrial transport function with de-
creased ventricular compliance is probably thebasic abnormality responsible for an augmentedatrial beat associated with ventricular hyper-trophy. In hypertrophic obstructive cardiomyo-pathy, where great ventricular hypertrophy isseen, the major portion of ventricular filling hasbeen shown to take place during atrial systole
FIG. 5. Impulse cardiogram, chest X-ray, cineradiogram left cardiac border, and cross-section of heart atautopsy in patient with cardiac aneurysm. Paradoxical systolic pulsation shown in cineradiogram tracings,accounting for overlying sustained cardiac impulse. Bulging of left cardiac border in chest X-ray. Extensiveinfarct involving whole of lateral wall of left ventricle at autopsy. ECG showing ST elevation and tall T wavesin anterior chest leads.
84by copyright.
on October 16, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.44.507.81 on 1 January 1968. Dow
nloaded from

Festschrift for Sir John McMichael 85
I:
RAI ftVp BEAT~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~............
I~ ~~~~~~~~~..... ............
(P SYSTOLIC RETRACTION~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~......
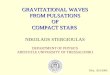
FIG. 6. (a) Annular constrictive pericarditis as seen at operation. Pericardial constriction, (1) in A-V groove,and (2) around base of aorta and pulmonary artery. (b) Praecordial impulse cardiogram (MID P) showingsystolic retraction in constrictive pericarditis. The outward diastolic pulsation is the diastolic rapid inflow beat(DRI beat). The early diastolic sound (EDS) coincides with the steep portion of the upstroke of the DRI beat.Phonocardiogram: PA, MF: pulmonary area, medium frequency. 2' and 2": split second heart sound. LSE, MF:left sternal edge, medium frequency. Electrocardiogram lead 1I.
V 4
ORS
oL
FIG. 7. Superimposed tracings of cineangiocardio-grams of right ventricle in left lateral view, at threepoints during cardiac cycle, indicated in simultaneouselectrocardiogram. Note major increase of ventricularcavity area during downstroke of P wave (-- - line)and beginning of QRS (- - - line), i.e. in atrialsystole and end-diastole.
in cineangiocardiographic studies. This is asso-ciated with a large outward movement of theanterior ventricular wall which in turn causesthe giant atrial beat in the cardiac impulse (Fig.7) (Nagle et al., 1966). In ventricular aneurysm,however, another factor is probably contributingto the large amplitude of the atrial beat, namely
the thin tambour-like quality of the aneurysmalwall.
AcknowledgmentsThe illustrations are reproduced by kind permission of the
Editor of the British Heart Journal, 21, 325 (1959), 24, 409(1962), 26, 396 (1964), 27, 379 (1965), 28, 419 (1966).
ReferencesBEILIN, L. & MOUNSEY, J.P.D. (1962) The left ventricular
impulse in hypertensive heart disease. Brit. Heart J. 24, 409.BoICOURT, O.W., NAGLE, R.E. & MOUNSEY, J.P.D. (1965)The clinical significance of systolic retraction of the apicalimpulse. Brit. Heart J. 27, 379.
DELIYANNIS, A.A., GILLAM, P.M.S., MOUNSEY, J.P.D. &STEINER, R.E. (1964) The cardiac impulse and the motion ofthe heart. Brit. Heart J. 26, 396.
DRESSLER, W. (1937) Pulsations of the wall of the chest.Arch. intern. Med. 60, 662.
EDDLEMAN, E.E., WILLIS, K., REEVES, T.J. & HARRISON, T.R.(1953) The kinetocardiogram. I. Method of recordingpraecordial movements. Circulation, 8, 269.
HARVEY, W. (1628) Exercitatio anatomica de Motu Cordiset Sanguinis in Animalibus. Frankfurt.
LAENNEC (1819) De l'Auscultation Mediate, pp. 206-210.J. A. Brosson, Paris.
MACKENZIE, J. (1908) Diseases of the Heart. Oxford Uni-versity Press.
MAREY, E.J. (1878) La Methode graphique dans les Sciencesexperimentales. Masson, Paris.
MOUNSEY, J.P.D. (1959) Annular constrictive pericarditis.Brit. Heart J. 21, 325.
NAGLE, R.E., BoICOURT, O.W., GILLAM, P.M.S. & MOUNSEY,J.P.D. (1966) Cardiac impulse in hypertrophic obstructivecardiomyopathy. Brit. Heart J. 28, 419.
by copyright. on O
ctober 16, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.44.507.81 on 1 January 1968. D
ownloaded from